Contents
What is a grand mal seizure
Grand mal seizure is an older term for generalized tonic-clonic seizure, which is one type of seizure that involves your entire body. Grand mal seizure is the type of seizure most people picture when they think about seizures. The terms seizure, convulsion, or epilepsy are most often associated with generalized tonic-clonic seizures, is what most people think of as a typical epileptic fit.
Having just one grand mal seizure it is not considered to be epilepsy – about half the people who have one grand mal seizure never have another seizure.
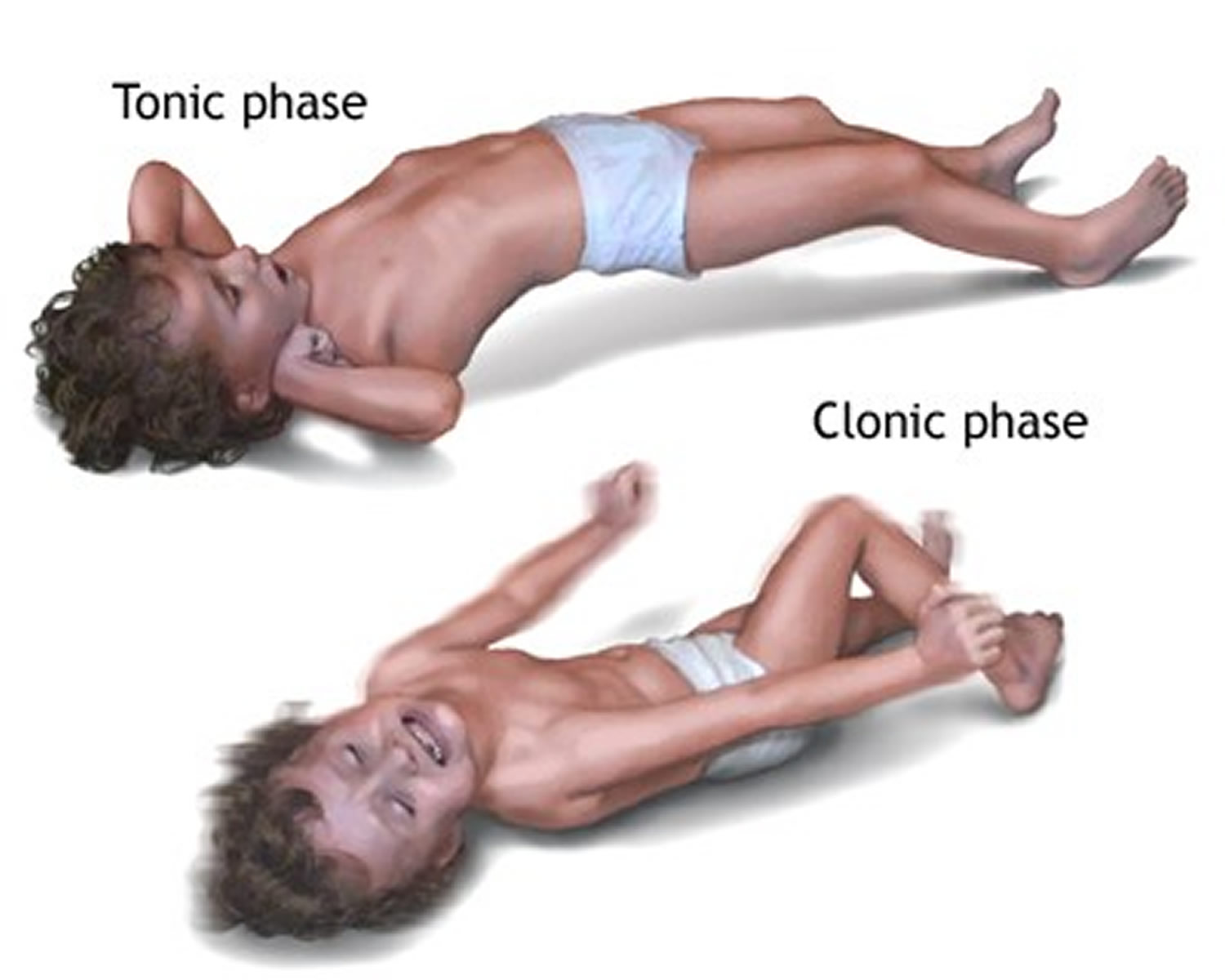
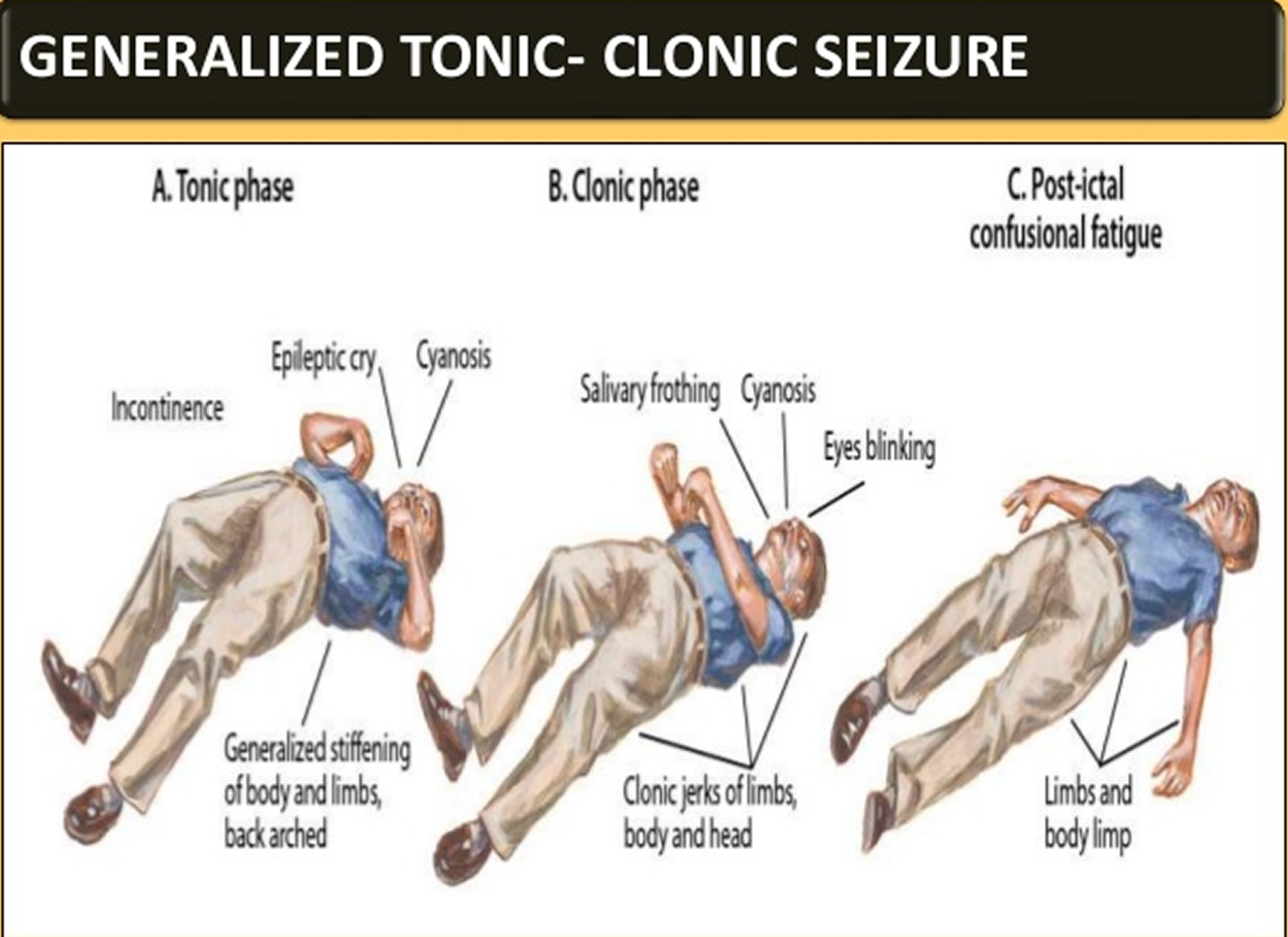
Grand mal seizure happens in two stages – an initial “tonic” stage, shortly followed by a second “clonic” stage:
- Tonic stage – you lose consciousness and your muscles suddenly contract causing your body to become stiff and you may fall to the floor. This phase tends to last about 10 to 20 seconds.
- Clonic stage – your muscles go into rhythmic contractions, alternately flexing and relaxing. Your limbs jerk about, you may lose control of your bladder or bowel, you may bite your tongue or the inside of your cheek, and you might have difficulty breathing. Clonic phase (convulsions) usually last one to two minutes or less.
The following signs and symptoms occur in some but not all people with grand mal seizures:
- A scream. Some people may cry out at the beginning of a seizure.
- Loss of bowel and bladder control. This may happen during or following a seizure.
- Unresponsiveness after convulsions. Unconsciousness may persist for several minutes after the convulsion has ended.
- Confusion. A period of disorientation often follows a grand mal seizure. This is referred to as postictal confusion.
- Fatigue. Sleepiness is common after a grand mal seizure.
- Severe headache. Headaches may occur after a grand mal seizure.
Grand mal seizure begins with a sudden loss of consciousness (tonic stage), the body then becomes stiff followed by jerking of the muscles (clonic stage). Turning red or blue, tongue-biting and loss of bladder control are common.
Figure 1. Grand mal seizure
Grand mal seizure after effects
Confusion, drowsiness, memory loss, headache, agitation and difficulty remembering what happened and feel tired or confused can occur on regaining consciousness. Grand mal seizure normally stops after a few minutes, but some last longer. Most seizures last from 30 seconds to 2 minutes and do not cause lasting harm. However, it is a medical emergency if seizures last longer than 5 minutes or if a person has many seizures and does not wake up between them. Seizures can have many causes, including medicines, high fevers, head injuries and certain diseases. People who have recurring seizures due to a brain disorder have epilepsy.
Many people with grand mal seizures (generalized tonic-clonic seizures) have vision, taste, smell, or sensory changes, hallucinations, or dizziness before the seizure. This is called an aura.
Grand mal seizures may occur in people of any age. Grand mal seizure can occur once (single episode). Or, grand mal seizures can occur as part of a repeated, chronic illness (epilepsy). Some seizures are due to psychological problems (psychogenic).
In terms of epilepsy, epilepsy is not one single condition; rather epilepsy is a range of different chronic neurological disorders in which clusters of nerve cells, or neurons, in the brain sometimes signal abnormally and cause seizures. Epilepsy can be considered a spectrum disorder because of its different causes, different seizure types, its ability to vary in severity and impact from person to person, and its range of co-existing conditions. Epilepsy is a common, long-term brain condition where a person has repeated seizures, and is thought to affect about 2.3 million adults and more than 450,000 children and adolescents in the United States currently live with epilepsy.
In general, a person is not considered to have epilepsy until he or she has had two or more unprovoked grand mal seizures separated by at least 24 hours. In contrast, a provoked seizure is one caused by a known precipitating factor such as a high fever, nervous system infections, acute traumatic brain injury, or fluctuations in blood sugar or electrolyte levels.
Many people who have a grand mal seizure never have another one and don’t need treatment. But someone who has recurrent grand mal seizure may need treatment with daily anti-seizure medications to control and prevent future grand mal seizures.
Grand mal seizure what to do
If you see someone having a seizure or fit, there are some simple things you can do to help. You should call an ambulance if you know it’s their first seizure or it’s lasting longer than 5 minutes.
It might be scary to witness, but don’t panic.
If you’re with someone having a seizure:
- only move them if they’re in danger – such as near a busy road or hot cooker
- cushion their head if they’re on the ground
- loosen any tight clothing around their neck – such as a collar or tie to – aid breathing
- when their convulsions stop, turn them so they’re lying on their side (the recovery position)
- stay with them and talk to them calmly until they recover
- note the time the seizure starts and finishes
If they’re in a wheelchair, put the brakes on and leave any seatbelt or harness on. Support them gently and cushion their head, but don’t try to move them.
- Don’t put anything in their mouth, including your fingers. They shouldn’t have any food or drink until they fully recover.
When to call an ambulance:
Call your local emergency number and ask for an ambulance if:
- it’s the first time someone has had a seizure
- the seizure lasts for more than 5 minutes
- the person doesn’t regain full consciousness, or has several seizures without regaining consciousness
- the person is seriously injured during the seizure
People with epilepsy don’t always need to go to hospital every time they have a seizure.
Some people with epilepsy wear a special bracelet or carry a card to let medical professionals and anyone witnessing a seizure know they have epilepsy.
Figure 2. Recovery position

Seizure first aid
It’s helpful to know what to do if you witness someone having a seizure. If you’re at risk of having seizures in the future, pass this information along to family, friends and co-workers so that they know what to do if you have a seizure.
To help someone during a seizure:
- Carefully roll the person onto one side
- Place something soft under his or her head
- Loosen tight neckwear
- Remove eyeglasses
- Avoid putting your fingers or other objects in the person’s mouth
- Don’t try to restrain someone having a seizure
- Clear away dangerous objects, if the person is moving
- Stay with the person until medical personnel arrive
- Observe the person closely so that you can provide details on what happened
- Time the seizure
- Check for a medical alert bracelet or ID
- Stay calm
When to see a doctor
Seek immediate medical help if any of the following occurs:
- The seizure lasts more than five minutes.
- Breathing or consciousness doesn’t return after the seizure stops.
- A second seizure follows immediately.
- You have a high fever.
- You’re experiencing heat exhaustion.
- You’re pregnant.
- You have diabetes.
- You’ve injured yourself during the seizure.
If you experience a seizure for the first time, seek medical advice.
Lifestyle and home remedies
Here are some steps you can take to help with seizure control:
- Take medication correctly. Don’t adjust the dosage before talking to your doctor. If you feel your medication should be changed, discuss it with your doctor.
- Get enough sleep. Lack of sleep can trigger seizures. Be sure to get adequate rest every night.
- Wear a medical alert bracelet. This will help emergency personnel know how to treat you correctly if you have another seizure.
Personal safety
Seizures don’t usually result in serious injury, but if you have recurrent seizures, injury is a possibility. These steps can help you avoid injury during a seizure:
- Take care near water. Don’t swim alone or relax in a boat without someone nearby.
- Wear a helmet for protection during activities such as bike riding or sports participation.
- Take showers instead of baths, unless someone is near you.
- Modify your furnishings. Pad sharp corners, buy furniture with rounded edges and choose chairs that have arms to keep you from falling off the chair.
- Consider carpet with thick padding to protect you if you do fall.
- Display seizure first-aid tips in a place where people can easily see them. Include any important phone numbers there, too.
Diet therapy
Following a diet that’s high in fat and low in carbohydrates, known as a ketogenic diet or keto diet, can improve seizure control. Variations on a high-fat, low-carbohydrate diet, such as the low glycemic index and modified Atkins diets, though less effective, aren’t as restrictive as the ketogenic diet and may provide benefit.
Grand mal seizure complications
Having a seizure at certain times can lead to circumstances that are dangerous for you or others. You might be at risk of:
- Falling. If you fall during a seizure, you can injure your head or break a bone.
- Drowning. If you have a seizure while swimming or bathing, you’re at risk of accidental drowning.
- Car accidents. A seizure that causes either loss of awareness or control can be dangerous if you’re driving a car or operating other equipment.
- Pregnancy complications. Seizures during pregnancy pose dangers to both mother and baby, and certain anti-epileptic medications increase the risk of birth defects. If you have epilepsy and plan to become pregnant, work with your doctor so that he or she can adjust your medications and monitor your pregnancy, as needed.
- Emotional health issues. People with seizures are more likely to have psychological problems, such as depression and anxiety. Problems may be a result of difficulties dealing with the condition itself as well as medication side effects.
Can you die from a grand mal seizure
You can’t die from a grand mal seizure, but death is probably depending on what you were doing at the time your grand mal seizure occurs. For example, if you were scuba diving alone and have a grand mal seizure – you’re at risk of accidental drowning or you are driving a car or operating heavy equipment and have a grand mal seizure.
Sudden unexpected death in epilepsy (SUDEP)
Epilepsy is common, affecting one in every 200 people. People with epilepsy have a significantly higher mortality than people who do not have epilepsy: the rate of death from any cause in patients with epilepsy is 2-3 times higher than that of the general population.
This increased mortality is due to a variety of causes, such as accidents (trauma, drowning) during seizures, suffocation, suicide, and death due to other conditions (such as brain tumors) that lead to seizures.
The most common single epilepsy related cause of death is Sudden Unexpected Death in Epilepsy (SUDEP). In people with Sudden Unexpected Death in Epilepsy (SUDEP), no cause for death is found at post mortem. The risk of sudden death in people with epilepsy (SUDEP) is estimated to be 24 times greater than for those without epilepsy.
Sudden Unexpected Death in Epilepsy (SUDEP) is diagnosed when there is an unexpected non traumatic (such as head injury) and non drowning death in an individual with epilepsy. It may be witnessed or un-witnessed, and may occur following a seizure or not. It must not occur due to status epilepticus (prolonged seizure that does not respond to medication), inhaling (aspiration) of stomach contents, or any kind of poisoning. To be classified as Sudden Unexpected Death in Epilepsy (SUDEP), there must be no evidence of a cause of death due to drugs or other diseases at post mortem examination. The person does not have to have been known to have a seizure just before their death (although this is often the case), but they must have been diagnosed with epilepsy in the past.
It is important to note that ‘sudden death’ is not the same thing as ‘instantaneous death’. Sudden death is defined as death occurring within an hour of starting to become unwell.
Sudden unexpected death in epilepsy (SUDEP) is the single most important cause of death in people with epilepsy.
The reported incidence of sudden death in epilepsy varies between studies. When studies relate to higher risk groups, SUDEP is found to be a more frequent cause of death than in lower risk groups. In lower risk groups, such as children with epilepsy, the general population, epilepsy registers and autopsy series studies, SUDEP explained from 0-14% of deaths. In contrast, SUDEP explained 29-75% of deaths within studies where subjects were enrolled in drug trials, epilepsy surgery or surgical candidates, epilepsy clinics and registers of patients with refractory epilepsy.
The frequency of SUDEP in community based populations with epilepsy is estimated as between 1:500 and 1:1000 patient years. That is, if 1000 people with epilepsy were monitored for one year, one of those would die of SUDEP. The highest rates of SUDEP (2.2-10 deaths per 1000 patient years) have been found in candidates for epilepsy surgery, those with severe refractory epilepsy, and those who require input from specialist epilepsy referral centres. Intermediate rates (3.4-3.6 deaths per 1000 patient years) have been found in studies including patients with intellectual impairment. Lowest rates (0.35-2.5 deaths per 1000 patient years) have occurred in studies involving children.Studies of epilepsy in the general population found rates of SUDEP to be 0-1.35 deaths per 1000 patient years studied. For those with severe refractory epilepsy, the risk of SUDEP is about 0.5-1% per year.
Risk Factors for Sudden Unexpected Death in Epilepsy (SUDEP)
Many studies have been performed in an attempt to identify risk factors for SUDEP. Though none have been clearly confirmed, some possible risk factors are summarized below:
- Patient related – young adulthood, male gender, alcohol abuse, being in bed
- Seizure related- more frequent seizures, early age at onset of seizures, long duration of epilepsy, grand mal seizures (tonic- clonic seizure type), seizure within previous year, intractable epilepsy.
- Treatment related- taking multiple anti epileptic medications, poor adherence with antiepileptic drugs, surgery, frequently changing the types or dose of medication taken.
Though individual cases of SUDEP are often reported in medical literature, it has proven difficult to study SUDEP in depth. This is because SUDEP is so rare in the general population. Studies into SUDEP have therefore only been on small groups of patients. However, some useful information has been gathered, both from these studies of small groups of patients, and from animal studies.
The majority of people with newly diagnosed epilepsy will not go on to have seizures in the long term, and within this group SUDEP is an extremely rare occurrence. Studies have therefore tended to focus on individuals with more severe forms of epilepsy, who generally have greater representation within specialist clinics, hospital inpatient settings and residential care. The risk of SUDEP is known to be elevated within this population.
In most studies, the age of death due to SUDEP has been between 25-40 years. However, diagnosing SUDEP in older populations can be difficult as other medical conditions are more likely to be present at autopsy. Death may be mistakenly attributed to these other conditions (such as vascular disease), as by definition SUDEP may only be diagnosed if no other cause of death is found.
The frequency of SUDEP in patients with epilepsy is not always related to the type of, or severity, of seizures experienced. Both major and minor seizures have led to SUDEP. This is because the apparent severity of the convulsions on the outside does not necessarily reflect what is happening in the brain – more severe disturbances in brain activity do not always produce larger seizures. Nevertheless, most cases of SUDEP are said to be associated with seizures of the grand mal (generalised tonic-clonic) type, more severe epilepsy, more frequent seizures, and individuals requiring many antiepileptic drugs.
Most cases of SUDEP occur when the person is in bed. SUDEP may therefore be related to sleep. Whether this is due to a difference in the physiology between nocturnal and daytime seizures, or simply due to lack of supervision and help available at the time is unknown.
Sudden Unexpected Death in Epilepsy (SUDEP) diagnosis
SUDEP is diagnosed when an individual with epilepsy dies suddenly, and no cause (such as drowning, trauma, or choking) can be found during post mortem examination. Although a difficult idea for many families to cope with, medical examination of the body of a person who dies in these circumstances is important to rule out other causes of death which may mimic SUDEP, such as a drug overdose or brain hemorrhage. This information is important so that more can be learned about causes of death in epilepsy, including SUDEP, with the hope of preventing deaths in the future.
Sudden Unexpected Death in Epilepsy (SUDEP) treatment
Unfortunately, scientists do not yet know exactly how to prevent or treat SUDEP. Strategies are suggested by experts in the area, who base their suggestions on identifying and minimizing an individual’s possible risk factors for SUDEP. There is not yet a high level of evidence that proves that these strategies work in preventing SUDEP.
It is likely that the risk of SUDEP can be reduced by making sure that seizure control in all patients with epilepsy is as good as possible, though optimization of medical and surgical management. This remains the most important treatment goal in patients with epilepsy. Aggressive treatment of refractory epilepsy (characterized by uncontrolled seizures), with specialist epilepsy center input and consideration of surgery or vagal nerve stimulation is warranted.
Supervision at night, either with a ‘supervisor’ sharing the same room, regular checks throughout the night, or use of a monitoring device has been associated with a decreased risk of SUDEP.
There is some debate as to the best approach in discussing SUDEP with individuals with epilepsy and their families. Given the rare nature of the condition, some clinicians feel outlining the risk of SUDEP will create needless worry for individuals with epilepsy and their relatives. Increasingly however, the importance of identification of high risk individuals, with subsequent education and use of prevention strategies is being promoted clinically and within the literature. Other strategies that have been suggested are identification of seizure precipitants and promoting compliance with treatment.
Grand mal seizure causes
A grand mal seizure (generalized tonic-clonic seizure) is caused by abnormal electrical activity throughout the brain. The brain’s nerve cells normally communicate with each other by sending electrical and chemical signals across the synapses that connect the cells. In people who have seizures, the brain’s usual electrical activity is altered and many nerve cells fire at the same time. Exactly what causes the changes to occur often remains unknown.
Grand mal seizures (generalized tonic-clonic seizures) may occur in people of any age. Grand mal seizure can occur once (single episode). Usually, a grand mal seizure is caused by epilepsy (a chronic seizure condition). But sometimes, grand mal seizures can be triggered by other health problems, such as extremely low blood sugar, a high fever or a stroke. Some seizures are due to psychological problems (psychogenic).
However, grand mal seizures are sometimes caused by underlying health problems, such as:
Injury or infection
- Traumatic head injuries
- Infections, such as encephalitis or meningitis, or a history of such infections
- Injury due to a previous lack of oxygen
- Stroke
Congenital or developmental abnormalities
- Blood vessel malformations in the brain
- Genetic syndromes
- Brain tumors
Metabolic disturbances
- Very low blood levels of glucose, sodium, calcium or magnesium
Withdrawal syndromes
- Using or withdrawing from drugs, including alcohol
Risk factors for grand mal seizures
Risk factors for grand mal seizures include:
- A family history of seizure disorders
- Any injury to the brain from trauma, a stroke, previous infection and other causes
- Sleep deprivation
- Medical problems that affect electrolyte balance
- Illicit drug use
- Heavy alcohol use.
Grand mal seizure symptoms
Many people with grand mal seizures (generalized tonic-clonic seizures) have vision, taste, smell, or sensory changes, hallucinations, or dizziness before the seizure. This is called an aura.
The seizures often result in rigid muscles. This is followed by violent muscle contractions and loss of alertness (consciousness). Other symptoms that occur during the seizure may include:
- Biting the cheek or tongue
- Clenched teeth or jaw
- Loss of urine or stool control (incontinence)
- Stopped breathing or difficulty breathing
- Blue skin color
After the grand mal seizure, the person may have:
- Confusion
- Drowsiness or sleepiness that lasts for 1 hour or longer (called the post-ictal state)
- Loss of memory (amnesia) about the seizure episode
- Headache
- Weakness of 1 side of the body for a few minutes to a few hours following seizure (called Todd paralysis)
Grand mal seizure diagnosis
After a seizure, your doctor will thoroughly review your symptoms and medical history. The doctor will perform a physical exam. This will include a detailed check of the brain and nervous system. Your doctor may order several tests to determine the cause of your seizure and evaluate how likely it is that you’ll have another one.
Tests may include:
- An EEG (electroencephalogram) will be done to check the electrical activity in the brain. In this test, doctors attach electrodes to your scalp with a paste-like substance. The electrodes record the electrical activity of your brain, which shows up as wavy lines on an EEG recording. The EEG may reveal a pattern that tells doctors whether a seizure is likely to occur again. EEG testing may also help your doctor exclude other conditions that mimic epilepsy as a reason for your seizure. People with seizures often have abnormal electrical activity seen on this test. In some cases, the test shows the area in the brain where the seizures start. The brain may appear normal after a seizure or between seizures.
- Blood tests. Your doctor may take a blood sample to check for signs of infections, genetic conditions, blood sugar levels or electrolyte imbalances.
- Lumbar puncture. If your doctor suspects an infection as the cause of a seizure, you may need to have a sample of cerebrospinal fluid removed for testing.
- Computerized tomography (CT) scan. A CT scan uses X-rays to obtain cross-sectional images of your brain. CT scans can reveal abnormalities in your brain that might cause a seizure, such as tumors, bleeding and cysts.
- Magnetic resonance imaging (MRI). An MRI uses powerful magnets and radio waves to create a detailed view of your brain. Your doctor may be able to detect lesions or abnormalities in your brain that could lead to seizures.
- Positron emission tomography (PET). PET scans use a small amount of low-dose radioactive material that’s injected into a vein to help visualize active areas of the brain and detect abnormalities.
- Single-photon emission computerized tomography (SPECT). A SPECT test uses a small amount of low-dose radioactive material that’s injected into a vein to create a detailed, 3-D map of the blood flow activity in your brain that happens during a seizure. Doctors may also conduct a form of a SPECT test called subtraction ictal SPECT coregistered to magnetic resonance imaging (SISCOM), which may provide even more-detailed results.
Figure 3. EEG brain activity
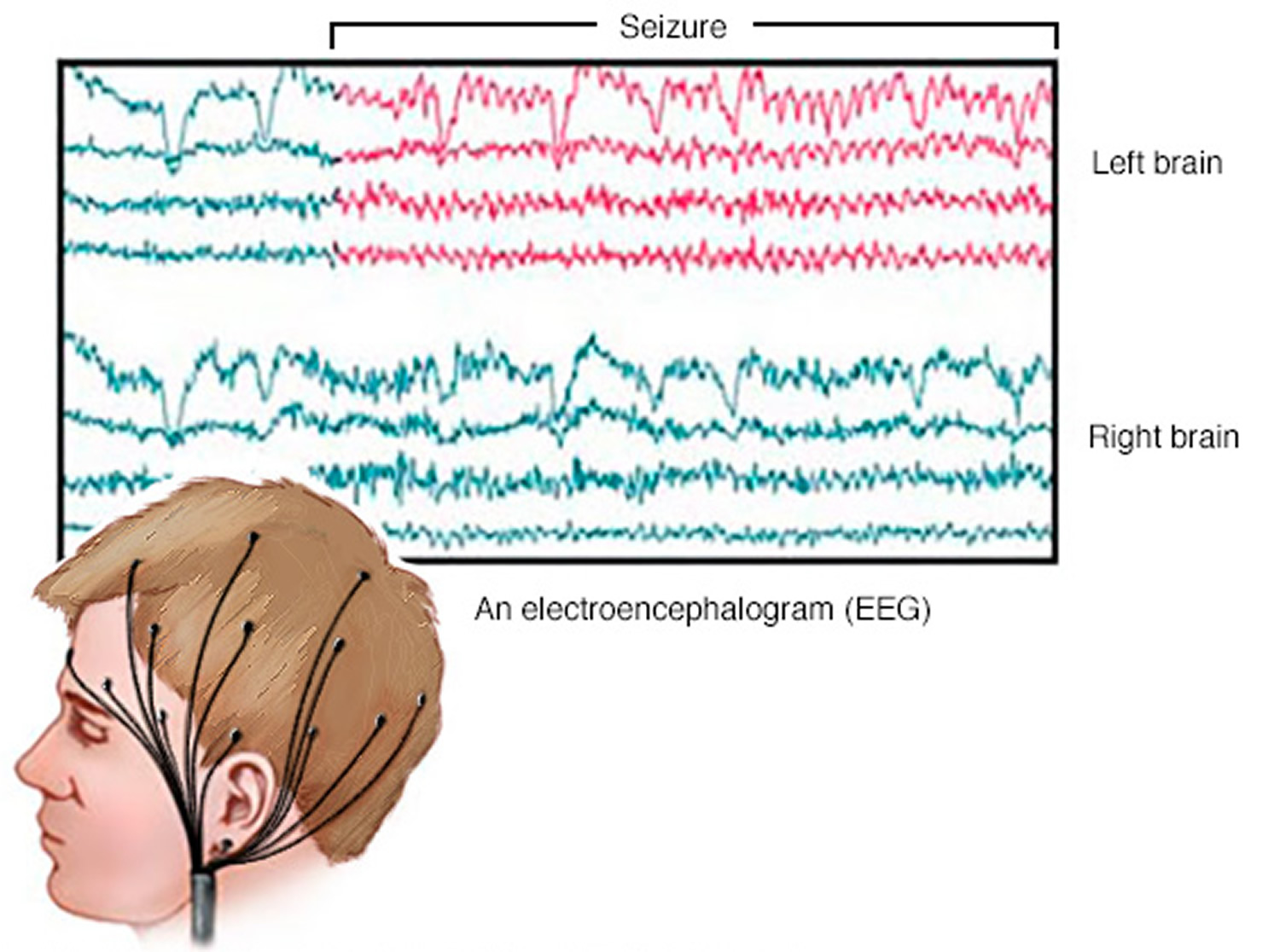
Note: An EEG records the electrical activity of your brain via electrodes affixed to your scalp. EEG results show changes in brain activity that may be useful in diagnosing brain conditions, especially epilepsy and other seizure disorders.
Figure 4. SPECT scans
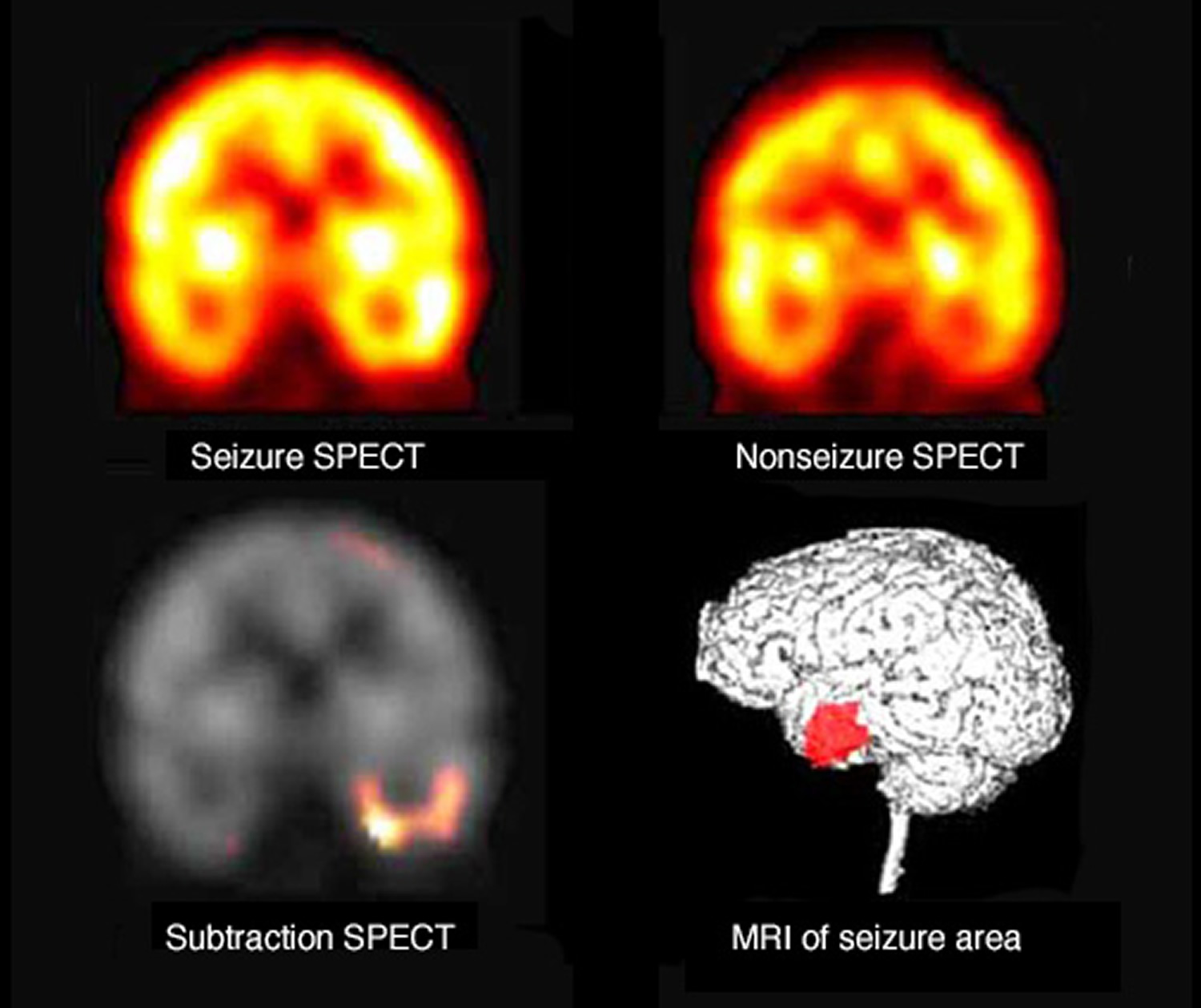
Note: This example shows SPECT scans taken during and between seizures. The differences represent areas where blood flow increased during the seizure. Once identified, that location is fitted onto an MRI image of the brain.
Grand mal seizure treatment
Not everyone who has one grand mal seizure has another one. Because a grand mal seizure can be an isolated incident, your doctor may not start treatment until you’ve had more than one.
Treatment for grand mal seizures includes medicines, changes in lifestyle for adults and children, such as activity and diet, and sometimes surgery. Your doctor can tell you more about these options.
Medications
Many medications are used in the treatment of epilepsy and seizures, including:
- Carbamazepine (Carbatrol, Tegretol, others)
- Phenytoin (Dilantin, Phenytek)
- Valproic acid (Depakene)
- Oxcarbazepine (Oxtellar, Trileptal)
- Lamotrigine (Lamictal)
- Gabapentin (Gralise, Neurontin)
- Topiramate (Topamax)
- Phenobarbital
- Zonisamide (Zonegran)
Finding the right medication and dosage can be challenging. Your doctor likely will first prescribe a single drug at a relatively low dosage, and then increase the dosage gradually until your seizures are well-controlled.
Many people with epilepsy are able to prevent seizures with just one drug, but others need more than one. If you’ve tried two or more single-drug regimens without success, your doctor may recommend trying a combination of two drugs.
To achieve the best seizure control possible, take medications exactly as prescribed. Always call your doctor before adding other prescription medications, over-the-counter drugs or herbal remedies. And never stop taking your medication without talking to your doctor.
Mild side effects of anti-seizure medications can include:
- Fatigue
- Dizziness
- Weight gain
More-troubling side effects that need to be brought to your doctor’s attention immediately include:
- Mood disruption
- Skin rashes
- Loss of coordination
- Speech problems
- Extreme fatigue
In addition, the drug Lamictal has been linked to an increased risk of aseptic meningitis, an inflammation of the protective membranes that cover the brain and spinal cord that’s similar to bacterial meningitis.
Surgery
When anti-seizure medications aren’t effective, other treatments may be an option:
- Surgery. The goal of surgery is to stop seizures from happening. Surgeons locate and remove the area of your brain where seizures begin. Surgery works best for people who have seizures that always originate in the same place in their brains.
- Vagus nerve stimulation. A device implanted underneath the skin of your chest stimulates the vagus nerve in your neck, sending signals to your brain that inhibit seizures. With vagus nerve stimulation, you may still need to take medication, but you may be able to lower the dose.
- Responsive neurostimulation. During responsive neurostimulation, a device implanted on the surface of your brain or within brain tissue can detect seizure activity and deliver an electrical stimulation to the detected area to stop the seizure.
- Deep brain stimulation. Doctors implant electrodes within certain areas of your brain to produce electrical impulses that regulate abnormal brain activity. The electrodes attach to a pacemaker-like device placed under the skin of your chest, which controls the amount of stimulation produced.
Pregnancy and seizures
Women who’ve had previous seizures usually are able to have healthy pregnancies. Birth defects related to certain medications can sometimes occur.
In particular, valproic acid has been associated with cognitive deficits and neural tube defects, such as spina bifida. The American Academy of Neurology recommends that women avoid using valproic acid during pregnancy because of risks to the baby. It’s especially important to avoid valproic acid during the first trimester of pregnancy, if possible.
Discuss these risks with your doctor. Because of the risk of birth defects, and because pregnancy can alter medication levels, preconception planning is particularly important for women who’ve had seizures.
In some cases, it may be appropriate to change the dose of seizure medication before or during pregnancy. Medications may be switched in rare cases.
Contraception and anti-seizure medications
It’s also important to know that some anti-seizure medications can alter the effectiveness of oral contraceptives — a form of birth control — and some oral contraceptives can speed up the absorption of seizure medications. If contraception is a high priority, check with your doctor to evaluate whether your medication interacts with your oral contraceptive, and if other forms of contraception need to be considered.
Coping and support
If you’re living with a seizure disorder, you may feel anxious or stressed about what your future holds. Stress can affect your mental health, so it’s important to talk with your health care provider about your feelings and seek ways you can find help.
At home
Your family can provide much-needed support. Tell them what you know about your seizure disorder. Let them know they can ask you questions, and be open to conversations about their worries. Help them understand your condition by sharing any educational materials or other resources that your health care provider has given you.
At work
Meet with your supervisor and talk about your seizure disorder and how it affects you. Discuss what you need from your supervisor or co-workers if a seizure happens while at work. Consider talking with your co-workers about seizure disorders — you can widen your support system and bring about acceptance and understanding.
You’re not alone
Remember, you don’t have to go it alone. Reach out to family and friends. Ask your health care provider about local support groups or join an online support community. Don’t be afraid to ask for help. Having a strong support system is important to living with any medical condition.





{kind=link}