
Contents
What is ingrown hair
When the tip of hair grows back under the skin and burrows in the uppermost dermis or into the hair follicle, it is known as ingrown hair. An ingrown hair has lost its path to the surface of the skin. Ingrown hair commonly results from shaving, plucking, waxing or threading. Ingrown hair can occur on any body site where hair is shaved or plucked, including armpit, pubic area, and legs. Ingrown hair is also known as shaving rash or razor bumps. Ingrown hair growth within the skin may be asymptomatic initially, but later causes inflammation, swelling and tenderness called razor bumps or shaving bumps (pseudofolliculitis barbae), which is a foreign-body inflammatory reaction surrounding ingrown facial hairs.
Razor bumps is not an infection but rather a “foreign body” reaction, much like the body would react to a splinter of wood in the skin. The condition may be worsened by methods used to achieve a close shave, such as pulling the skin tight while shaving, shaving against the “grain” or direction of hair growth, or using multi-blade razors.
Ingrown hair is due to shaving, particularly close shaving—because the cut hair may retract beneath the skin surface. Ingrown hair can also occur in skin folds and scars. Ingrown hair occurs mainly in people with curly hair, because the curl of the hair means that the sharp pointed end of a recently shaved hair comes out from the skin and re-enters the skin close by causing a foreign body inflammatory reaction.
Ingrown hair is a common condition that results from hair removal. It’s most prevalent in black men who shave facial hair. But ingrown hair can affect anyone who removes hair by shaving, tweezing or waxing.
Ingrown hairs most commonly appear in the beard area, including the chin and cheeks and, especially, the neck. They can appear on the scalp in those who shave their heads. Other common areas for ingrown hairs are the armpits, pubic area and legs.
Often, an ingrown hair improves without treatment. You can avoid ingrown hair by not removing hair. If that’s not an option, you can use hair removal methods that lessen the risk of developing ingrown hairs.
Risk factors for ingrown hairs
Having tightly curled hair is the main risk factor for ingrown hairs.
Complications of ingrown hairs
Chronic ingrown hairs can lead to:
- Bacterial infection (from scratching)
- Skin darkening (hyperpigmentation)
- Permanent scarring (keloids)
- Pseudofolliculitis barbae, also known as razor bumps
What causes ingrown hair
Although the exact mechanisms for ingrowing hair remain unknown, scientists considered that the actions of pulling or extruding the hair might play important roles, because the actions might result in possibility of localized inflammation and swelling around the hair follicle, and/or changing the growing direction of the hair, that made the hair grow inside the skin possible 1). While the hair was growing slowly inside the skin, the inflammation was extending gradually, and the length of lesion may be equal to the length of the ingrowing hair (excluding the hair follicle section). But when the hair follicle is deceased, the hair might move inside the skin. When the hair is growing inside the skin, it may also cause physical stimulation causing possible erythema (redness) which may be an inflammatory reaction stimulated by the hair, and the hair was excluded from the skin as a foreign body.
What does an ingrown hair look like
Figure 1. Hair structure
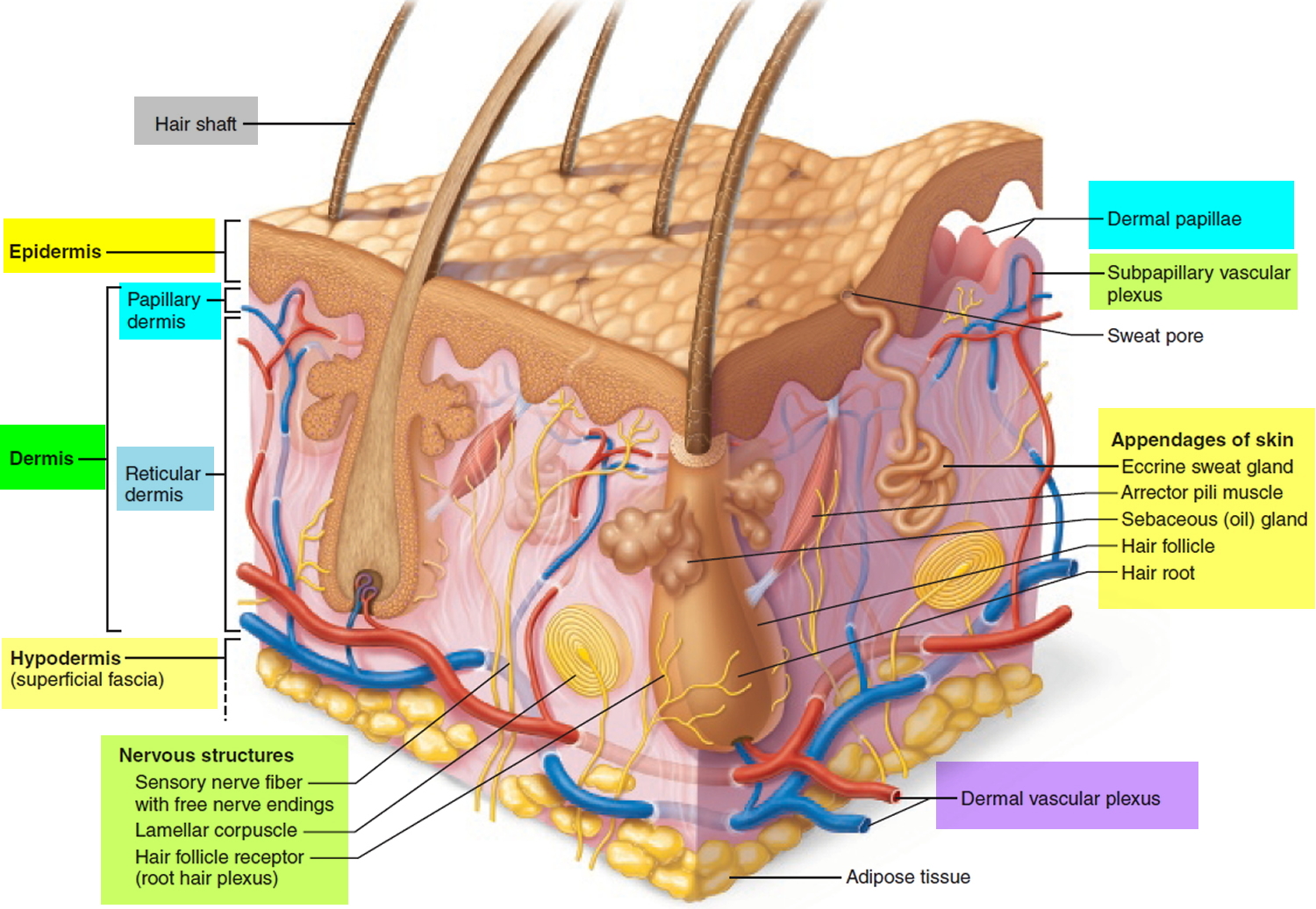
Figure 2. Hair follicle
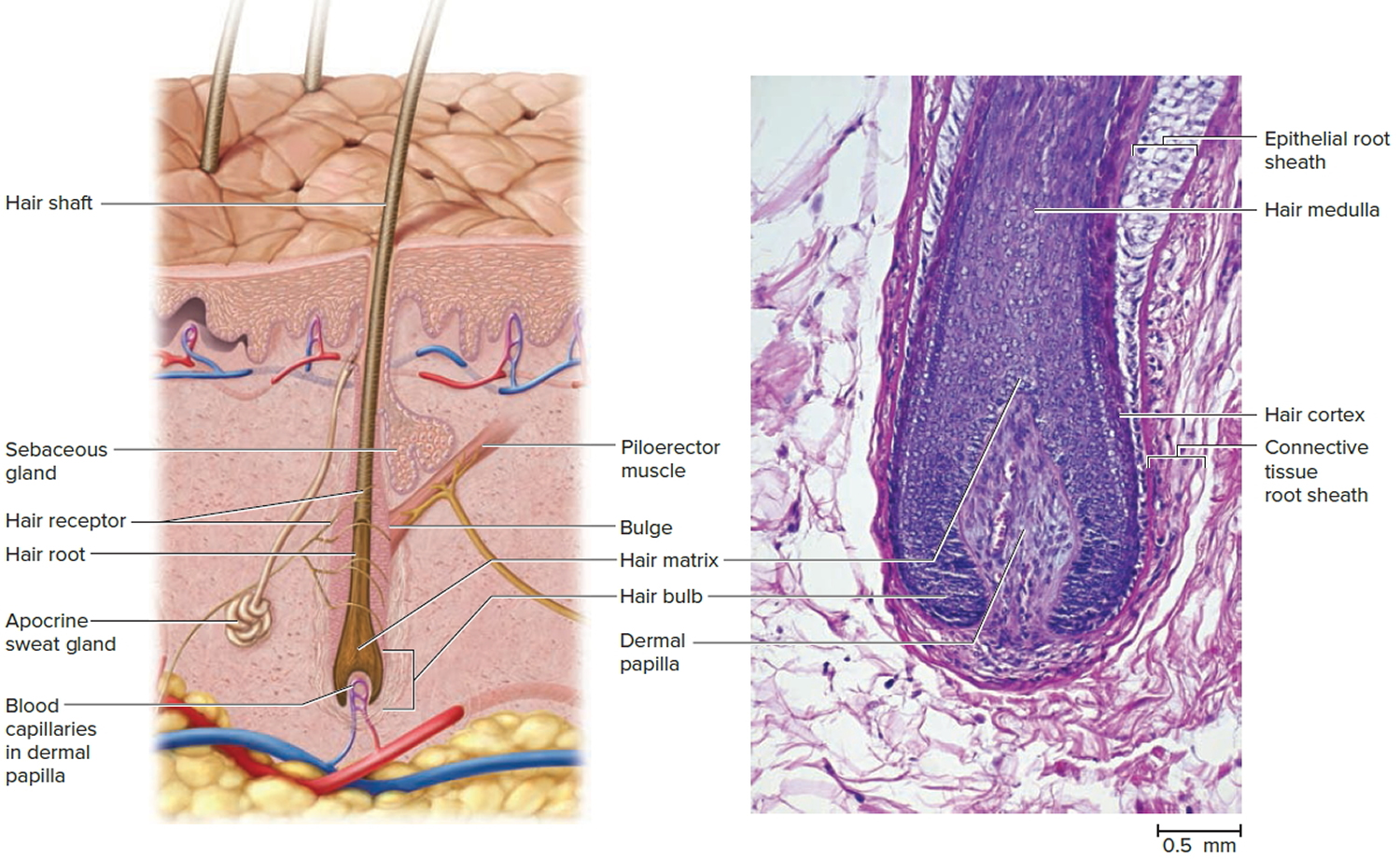
Figure 3. Ingrown hair cyst

Figure 4. Ingrown hair – note multiple pustules in the beard secondary to ingrowing hairs.

Figure 5. Ingrown hair
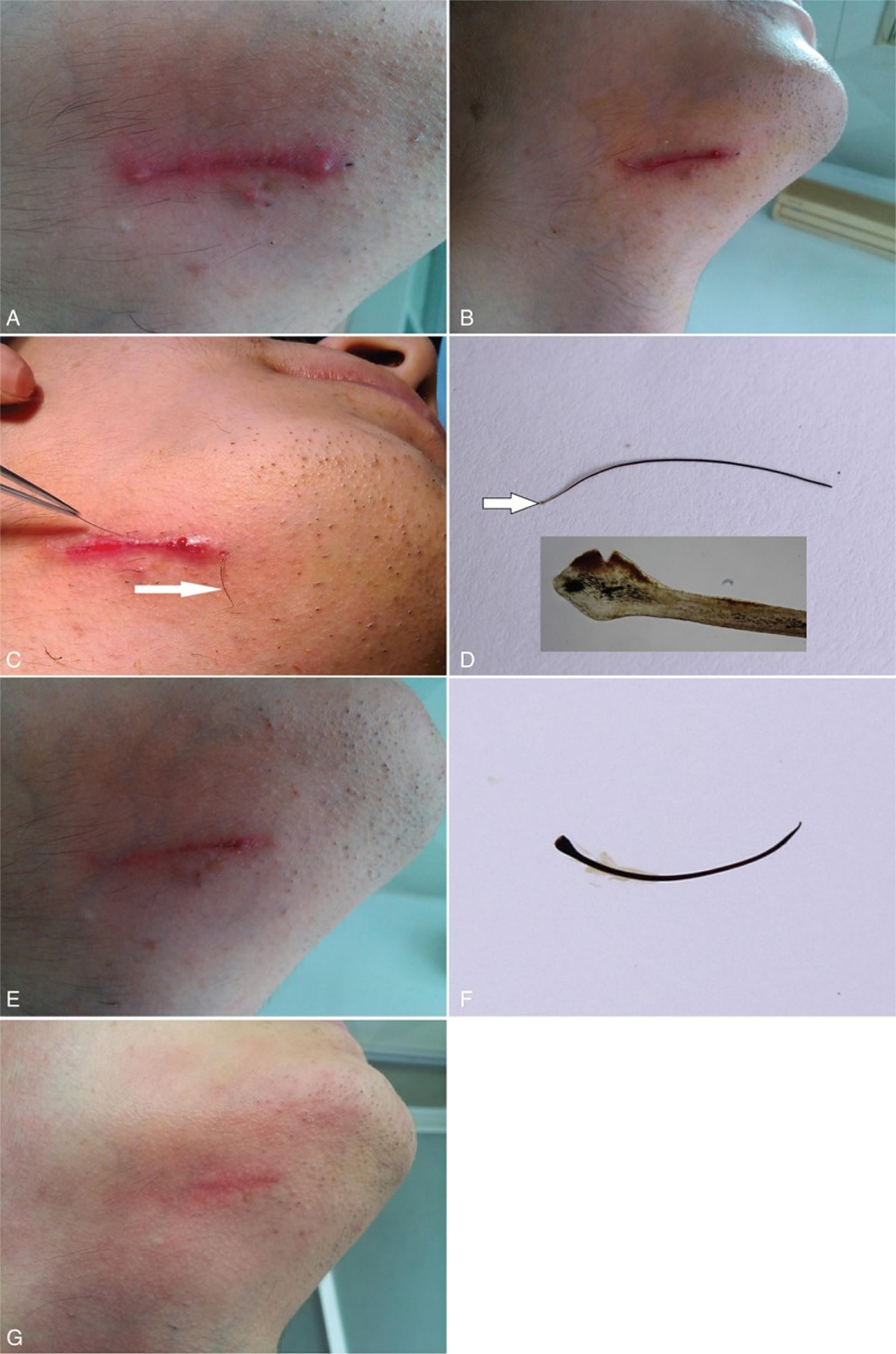
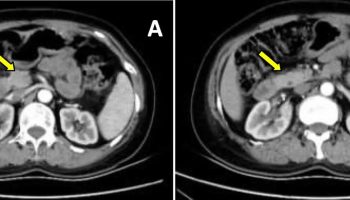
Footnotes: A 4.3-cm-long black linear lesion beneath the skin located on the right chin associated with edematous erythema around and 2 inflammatory papules on both ends of the lesion (A). The folliculitis improved excellently after treatment with topical mupirocin ointment for a week, and a hair shaft with its distal end protruding out of the skin presented on the lesion (B). A hair (grasped by the forceps) (C) with hair follicle (D, the white arrow; the inset showing a closer view of the hair, ×100) is easy pulled out; the second hair shaft (C, the white arrow) with its follicle in skin is pulled out from the skin. A new black linear lesion about 1 cm in length appeared in the skin in the region of prior erythema 2 weeks later after pulling out of the prior beards (E), showing hair shaft with hair follicle (F). Mild erythema left behind in 3 months of follow-up (G).
Ingrown hair prevention
To prevent ingrown hair recurrence, follow a proper shaving regimen long term and consider hair removal. Methods may include:
- If you don’t mind growing your hair, do so. This is curative!
- The chances of having ingrown hairs is greatly reduced if the hairs are kept at least a few millimeters long.
- If shaving is a must, please try the following shaving regimen:
- Apply a warm compress to the area for a few minutes prior to shaving.
- Ensure the skin is well moisturized, for example using a lotion containing glycolic acid to the affected areas. This exfoliates the surface skin cells and reduces the likelihood of new inflamed spots.
- Use a mild exfoliant, such as a extra gentle Buf-Puf facial sponge or loofah or better still a soft bristle (clean) toothbrush. Massage the area that is prone to ingrown hairs prior to shaving. Massage in a circular motion to help release the hairs that have curled inward. Some even use a toothpick to release hairs that have grown back on themselves.
- Cleanse the skin using a polyester skin-cleansing pad or a moisturizing shaving foam.
- Use a shaving gel designed for sensitive skin.
- Do not pull the skin taut when shaving.
- Either use a single blade disposable razor, or use electric hair clippers or a razor with an attachment that leaves the cut hairs long.
- Sterilize metal hair clippers and electric razors using boiling water, and plastic items should be soaked in antiseptic solution.
- Shave in the direction of hair growth (hairs pointing down, shave with a downward stroke). Do not shave against the direction of hair growth. Shaving against “the grain” will worsen the condition. On the neck, shave with the grain in a downward stroke only, never up.
- Take short strokes and do not shave back and forth over the same areas. One or two strokes in each area will suffice. Remember you do not want too close of a shave.
- After shaving, use a Hydrocortisone 1% lotion (available over-the-counter) to soothe any “razor burn” or irritation if needed.
- At night use any medication prescribed by your doctor e.g. Eflornithine cream. Eflornithine hydrochloride applied topically as a cream twice daily is the first agent known to help slow the rate of excessive hair growth. It is marketed under the brand name Vaniqa® and comes as eflornithine hydrochloride 13.9% cream. Eflornithine works by blocking the enzyme ornithine decarboxylase that stimulates hair growth. Eflornithine HCl cream 13.9% has been shown to slow the rate of hair growth in animal and human studies. Studies with eflornithine cream have been limited to treating unwanted hair on the face, around the lips and chin. Eflornithine hydrochloride is available on prescription from a doctor in the United States and elsewhere. Eflornithine HCl cream is very well tolerated. Some women may experience minor and temporary skin irritations including:
- redness
- stinging
- burning
- tingling
- rash
- ingrown hairs (pseudofolliculitis barbae)
- acne
- If skin irritation develops, the Eflornithine HCl cream dose may be reduced to once a day. If irritation continues you should stop using the cream.
- A laser beam can be used to get rid of hair by destroying the hair at its base. This procedure has to be done by a dermatologist (a skin doctor). It is probably the most expensive way to get rid of hair. In the future, it may become a permanent way to remove facial hair. Laser hair removal, especially Nd:YAG and diode lasers, but there is a risk of causing white or dark marks in skin of color.
- Electrolysis is the only permanent way to remove hair. A thin metal probe is inserted in the opening in the skin where the hair grows. An electric current destroys the hair at its base. You may need to get this treatment more than once to get rid of the hair for good. Electrolysis is more expensive. It isn’t done by a doctor. If you have a pacemaker, you can’t use this method.
- Chemical depilatories such as barium sulfide paste and calcium thioglycolate; these can be irritating
- Intense pulsed light (IPL)
How to treat ingrown hair
Medical treatment of ingrown hair inflammation
- Hydrocortisone cream can reduce mild inflammation and itching.
- Topical acne treatments such as benzoyl peroxide and tretinoin are used to suppress follicular hyperkeratosis.
- A combination of tretinoin, low-potency topical corticosteroid, and hydroquinone may be selected to decrease inflammation, hyperkeratosis and pigment production.
- Oral tetracyclines are used to reduce inflammation.
- Photodynamic therapy has been successful.
- Infected ingrown hair are treated with topical or oral anti-staphylococcal antibiotics.
Any plucking should stop. The tip of the hair may be teased out, releasing the hair. Laser hair removal may be a permanent solution for problematic areas.
- Growing your hair is curative.
- Release hairs. Hair releasing is critically important and must be done instead of plucking hairs. Hair releasing means removing the end of any hair buried in papules or pustules. Hair releasing may be done with a toothpick or a needle yourself or by your physician. Use a sterile needle to gently lift embedded hair tips. You may need to release your hairs every two to three days.
- Laser ablation.
- Shave carefully (see prevention above).
- Depilatories may work for some.
Growing hair is curative. Even a short hair is excellent. If this is not possible, various tips may allow for a relatively close shave.
- Use a shaving gel and a sharp razor.
- Don’t pull the skin taut.
- Shave with the direction of hair growth
- Shave each area only once.
- After shaving, apply a soothing after shave or hydrocortisone 1% lotion (available over-the-counter) to soothe any “razor burn” or irritation if needed.
A depilatory may be used, but many find these too irritating.
Laser hair removal may be helpful. For darker-skinned patients, the longer pulsed lasers (e.g. 1064 nm or 810 nm) may be used.
If inflammatory pustules or papules are present, topical benzoyl peroxide or a combination benzoyl peroxide with clindamycin product may be recommended. Topical retinoid every night at bedtime may be helpful, especially if there is post inflammatory hyperpigmentation.
Eflornithine 12% topically twice daily for 16 weeks was shown in one study to work synergistically with laser hair removal 2).
References [ + ]

{kind=link}