Contents
- What is eye infection
- Stye eye infection
- What is Blepharitis ?
- What is Meibomianitis
- What is Periorbital cellulitis
- What is Orbital cellulitis
- What is Dacryoadenitis
- What is Dacryocystitis
- What is Trachoma
- What is Conjunctivitis (Pink Eye) ?
- What Is Bacterial Keratitis ?
- What is Fungal Keratitis ?
- What is Herpes Keratitis ?
- What Is Uveitis ?
- What is Cytomegalovirus Retinitis
- Eye infections from contact lens
- Baby eye infection
What is eye infection
Your eyes can get infections from bacteria, fungi, or viruses. Eye infections can occur in different parts of the eye and can affect just one eye or both.
Eye infections can affect:
- The skin around the eye e.g. Periorbital Cellulitis
- The eyelid e.g. Stye, Chalazion
- The eyelashes e.g. Blepharitis
- The soft tissue, fat and muscles around the eye e.g. Orbital Cellulitis
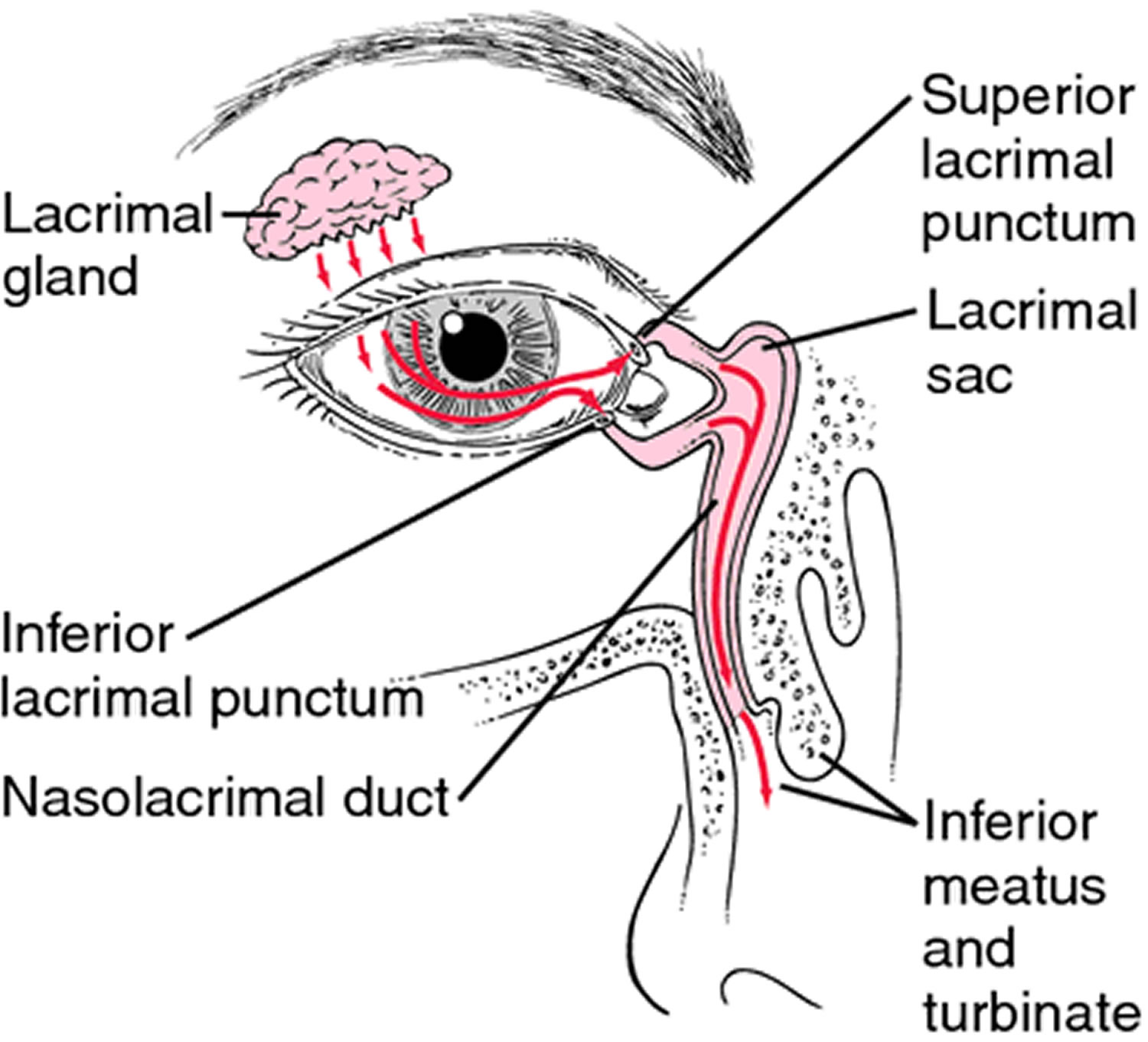
- The lacrimal gland, almond-shaped exocrine gland in each eye, that secrete the aqueous layer of the tear film. They are situated in the upper outer region of each orbit. e.g. Dacryoadenitis
- The tear ducts e.g. Dacryocystitis
- The oil glands in your eyelid (Meibomian glands)
- The cornea e.g. Bacterial, Fungal and Viral Keratitis
- The conjunctiva e.g. Conjunctivitis (Pink Eye), Trachoma
- The iris e.g. Uveitis
- The sclera e.g. Uveitis
- The retina e.g. Cytomegalovirus retinitis.
Two common eye infections are:
- Conjunctivitis – also known as pinkeye. Conjunctivitis is often due to an infection. Children frequently get it, and it is very contagious.
- Stye – a bump on the eyelid that happens when bacteria from your skin get into the hair follicle of an eyelash.
Symptoms of eye infections may include redness, itching, swelling, discharge, pain, or problems with vision. Treatment depends on the cause of the infection and may include compresses, eye drops, creams, or antibiotics.
Figure 1. Human eye
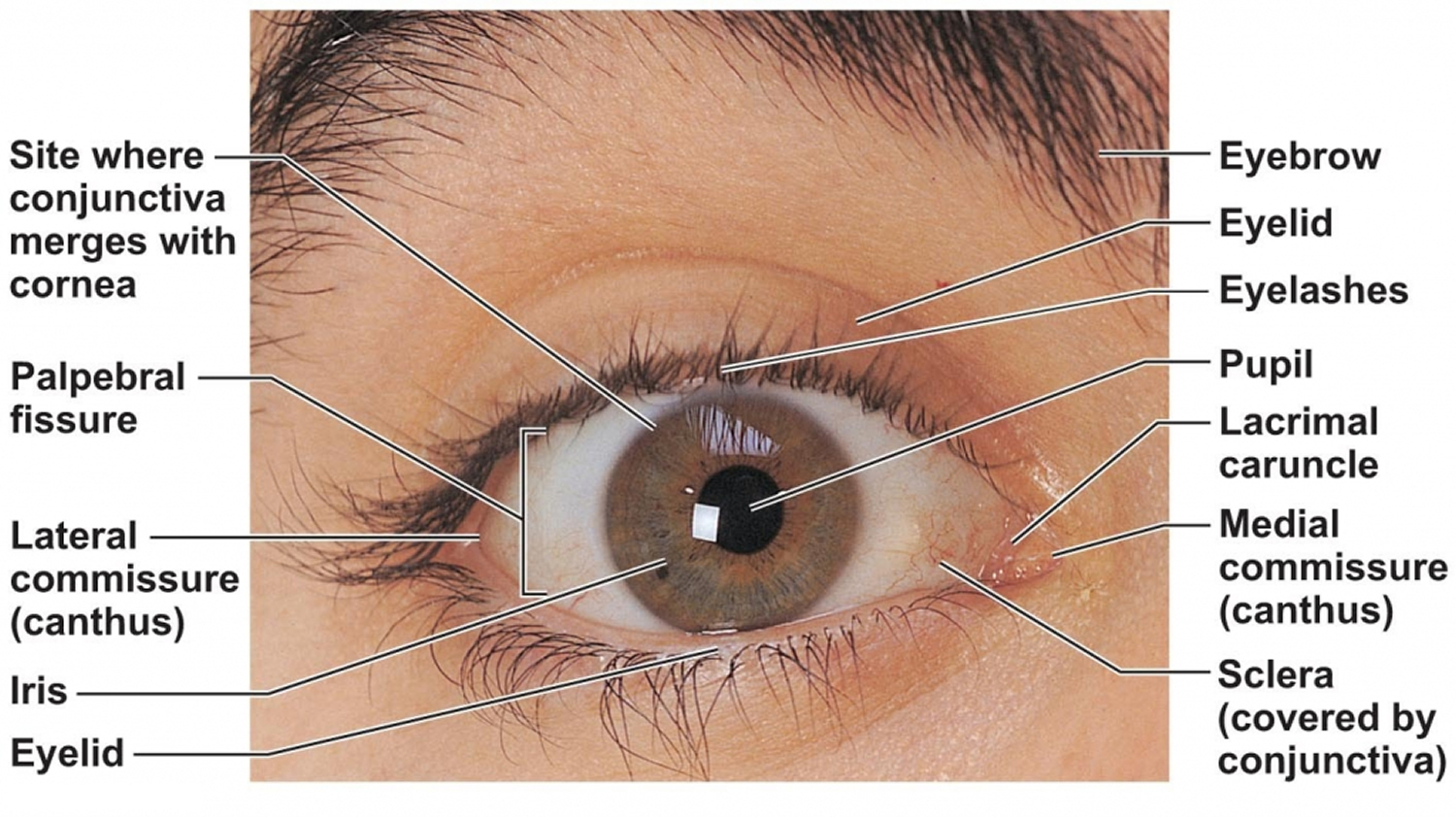
Figure 2. Eye anatomy
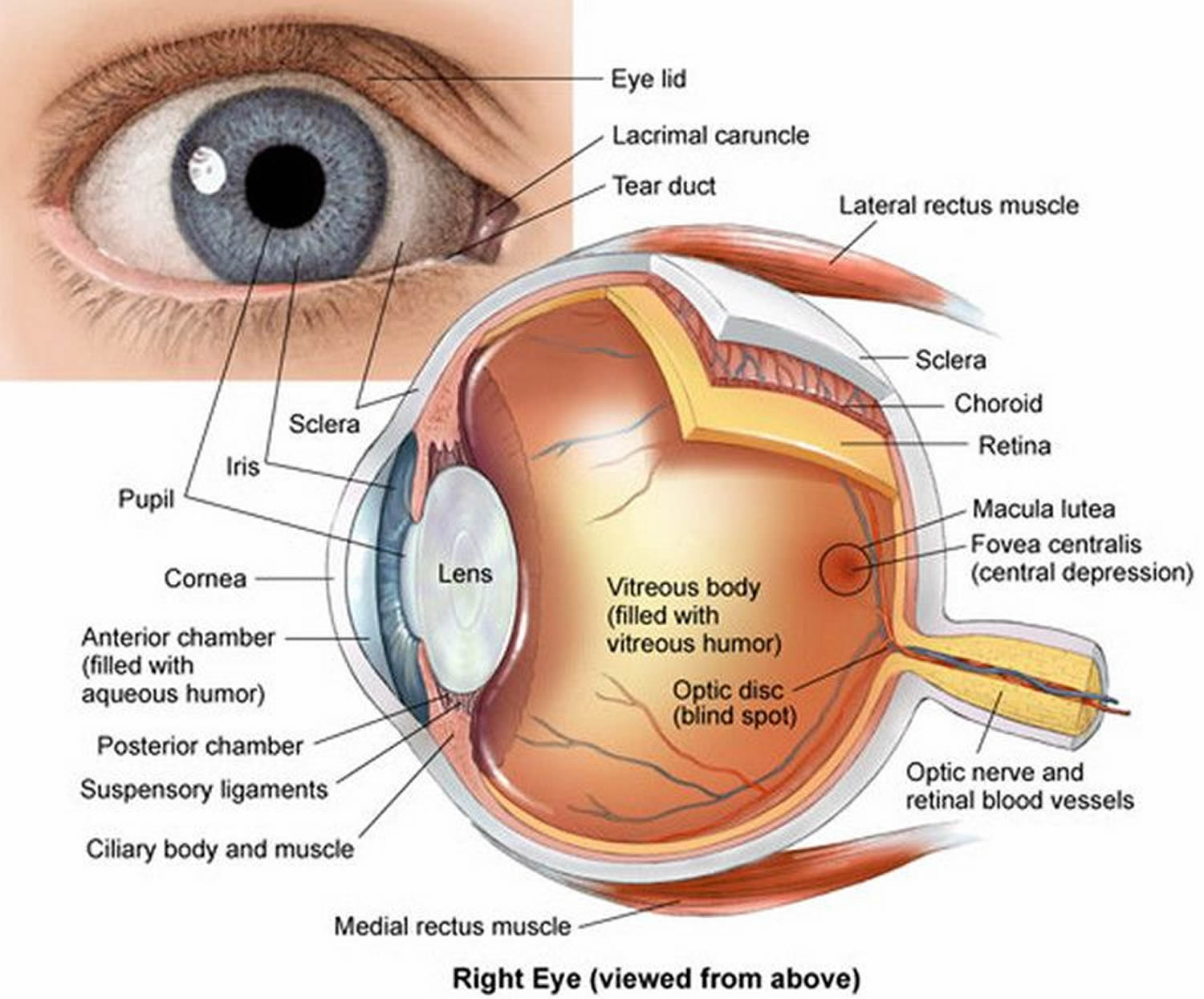
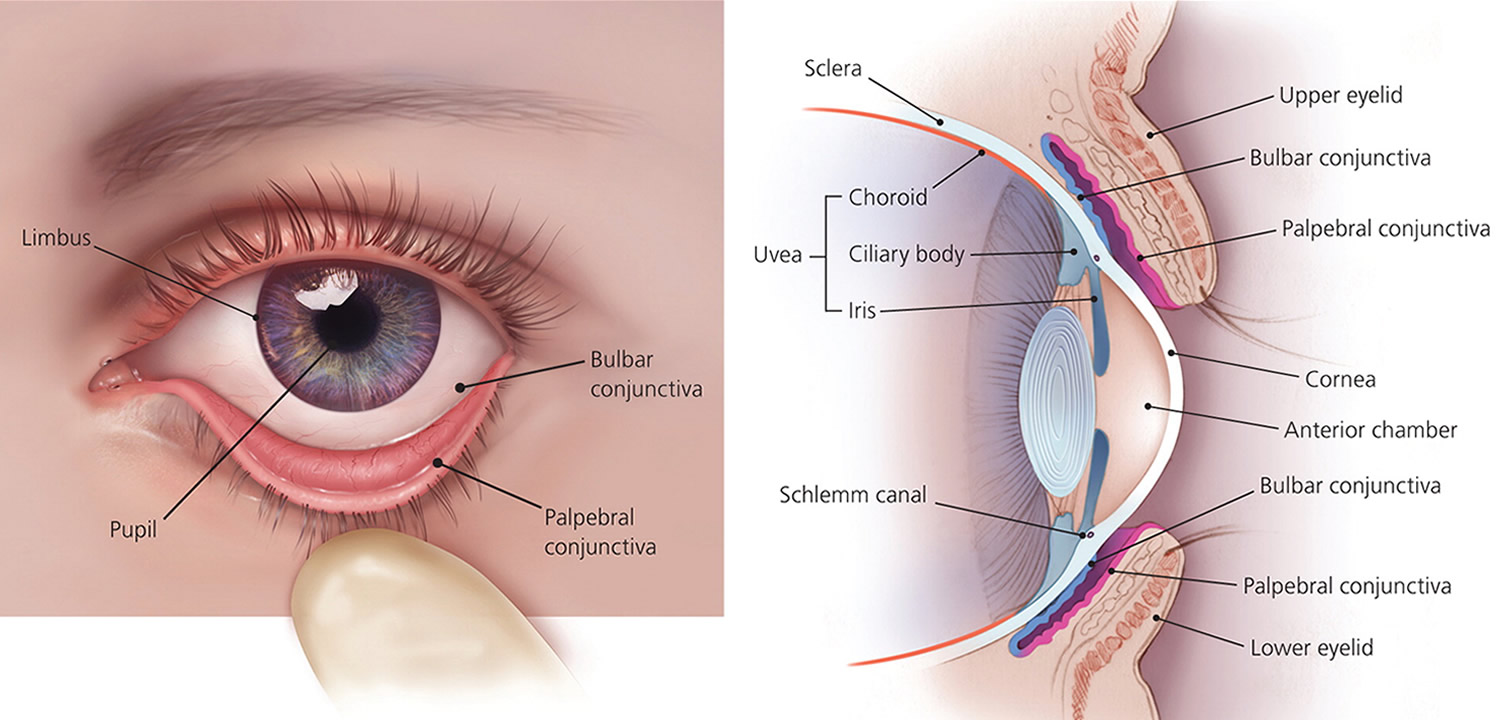
Note: The Uvea is a layer of tissue beneath the white of the eye (sclera). The Uvea has three parts: the iris, which is the colored part of the eye; the choroid layer, which is the layer of blood vessels and connective tissue between the sclera and the retina; and the ciliary body, which secretes the transparent liquid (aqueous humor) into the eye.
Stye eye infection
Although the terms chalazion and stye are often used interchangeably, they are not the same thing 1.
- A stye is an infection of an oil gland in the eyelid. It is like a small abscess or “boil” on the edge of the eyelid.
- A chalazion is a small or large bump on the eye lid caused by a blocked oil gland in the eye.
Both eye conditions often heal on their own. However, see your eye care professional if the bump continues to grow.
What is the difference between a stye and a chalazion ?
- Sometimes it can be difficult to tell the difference between a stye and a chalazion.
A stye is very painful. It often appears at the eyelid’s edge, usually caused by an infected eyelash root. It often swells, sometimes affecting the entire eyelid.
A chalazion is not usually painful. It is a bump that usually develops farther back on the eyelid than a stye. It is caused by a clogged oil gland. Rarely does it make the entire eyelid swell.
What is a stye ?
Hordeolum or stye is an acute, purulent inflammation of the eyelid margin usually caused by obstructed orifices of the sebaceous glands of the eyelid, usually caused by an infected eyelash root commonly caused by bacterial infection of the follicle of the eyelash 2. Stye, which affects sebaceous glands internally or externally, is common. When the meibomian gland in the tarsal plate is affected, internal hordeolum occurs. And when the glands of Zeis or Moll associated with eyelash follicles are affected, external hordeolum, or stye occurs. The onset of hordeolum is usually self limited, and may resolve in about a week with spontaneous drainage of the abscess. When the condition is severe, it can spread to adjacent glands and tissues. Recurrences are very common. As long as an internal hordeolum remains unresolved, it can develop into a chalazion or generalized eyelid cellulitis.
A internal hordeolum is an infection of the internal meibomian (sebaceous) gland, whereas a stye (external hordeolum) is an infection of the external Zeis (sweat) gland 3. These localized masses appear as papules and furuncles located distally at the lid edge 2. They typically resolve spontaneously within a few days or weeks, and warm compresses can help 2. Chronic hordeolum can lead to chalazion 3.
There are two kinds of styes:
- External hordeolum: A stye that begins at the base of your eyelash. Most are caused by an infection in the hair follicle. It might look like a pimple.
- Internal hordeolum: A stye inside your eyelid. Most are caused by an infection in an oil-producing gland in your eyelid.
You can also get a stye if you have blepharitis. This is a condition that makes your eyelids at the base of the eyelashes red and swollen.
When you first get a stye, your eyelid is probably red and tender to the touch. Your eye may also feel sore and scratchy.
Figure 3. A stye is a red, sore lump near the edge of the eyelid

What is a chalazion ?
A chalazion is a swollen bump on the eyelid. It happens when the eyelid’s oil gland clogs up. It may start as an internal hordeolum (stye). At first, you might not know you have a chalazion as there is little or no pain. But as it grows, your eyelid may get red, swollen, and sometimes tender to touch. If the chalazion gets large, it can press on your eye and cause blurry vision. Rarely, the whole eyelid might swell.
More than one chalazion can occur in an eyelid at the same time, and both upper and lower eyelids may be affected 4. A chalazion can occur on one or both eyes.
What causes a chalazion ?
Small glands lining the edge of the eyelids produce oil that helps lubricate the surface of the eye (meibomian glands). When one of these glands becomes blocked, oil backs up inside the gland and forms a bump in the eyelid. If the gland ruptures, the oily materials can irritate the surrounding eyelid skin causing it to become red, swollen and painful.
Why do chalazion occur ?
Usually there is no known underlying cause. However, chronic inflammation of the oil gland openings (blepharitis) predisposes to the development of a chalazion. Persistent blepharitis may result in recurrent chalazia. Blepharitis may be aggravated by poor eyelid hygiene that includes eye rubbing in children. Certain skin types may be more prone to chalazia and blepharitis.
How can chalazia be prevented ?
A consistent daily regimen of eyelid scrubs using baby shampoo or pre-moistened eyelid cleansing wipes can reduce the chances of developing new chalazia. This is especially useful when blepharitis is present. For those with a recurrent problem, regular use of topical or oral antibiotics is sometimes prescribed.
Figure 4. A chalazion is an enlargement of an oil-producing gland in the eyelid.

Chalazion and Stye Symptoms
Stye symptoms can include:
- a very painful red bump along the edge of the eyelid at the base of the eyelashes. It may make the entire eyelid swell
- usually a small pus spot at the center of the bump
- feeling like something is in your eye
- having a scratchy feeling in the eye
- being sensitive to light
- crustiness along the eyelid margin
- tearing in that eye
A chalazion can develop and you might not see any symptoms. When there are symptoms, they can include:
- a bump on the eyelid, sometimes becoming red and swollen. Occasionally it can be tender.
- rarely, an entirely swollen eyelid
- blurry vision, if the chalazion is large enough to press on the eyeball
Who Is at Risk for Chalazia and Styes ?
Anyone can get a stye or chalazion. But you are even more likely to get one if you have:
- Blepharitis, a problem that affects the edge of your eyelid
- Had a stye or chalazion before
- A skin condition, such as acne rosacea or seborrheic dermatitis
- Diabetes or other medical problems
What are the treatment options for stye and chalazion ?
Here are ways to treat your stye or chalazion:
- Warm compresses
Soak a clean washcloth in hot water and hold it to your eyelid for 10–15 minutes at a time, 3–5 times a day. Keep the cloth warm by soaking it in hot water often. For a chalazion, this warm compress helps the clogged oil gland to open and drain. You can help the gland clear itself by gently massaging around the area with your clean finger.
- Antibiotics
Your ophthalmologist may prescribe an antibiotic for an infected stye.
- Steroid shots
If your chalazion is very swollen, your ophthalmologist may give you a steroid shot (cortisone) to reduce the swelling.
- Surgery to drain the area
If your stye or chalazion affects vision or does not go away, you may need to have it drained. This surgery is usually done in the doctor’s office using local anesthesia.
If a stye or chalazion keeps coming back time after time, your ophthalmologist may biopsy it. This is where a tiny piece of tissue is removed and studied. This helps your ophthalmologist check to see if there is a more serious eye problem.
- Do not squeeze or try to pop a stye or chalazion
Doing so could spread the infection into your eyelid. Do not wear eye makeup or contact lenses while you have a stye or chalazion.
What are other treatment options for chalazion ?
Most chalazia resolve by themselves within several days to weeks, but sometimes can take months to completely disappear. Anti-inflammatory eye drops, ointments or an injection into the bump may be needed. Oral antibiotics may be used if the chalazion is associated with bacterial infection of the surrounding eyelid tissues (cellulitis). A large, swollen, or persistent chalazion might require surgical drainage. Although older children and adults can undergo the procedure in a doctor’s office under local anesthesia, general anesthesia is usually necessary to drain chalazia in young children.
What is Blepharitis ?
Blepharitis is when you have bacteria and oily flakes at the base of your eyelashes 5. Blepharitis is inflamed, irritated, itchy, and reddened eyelids or feel like they are burning 6. It most often occurs where the eyelashes grow. Dandruff-like debris builds up at the base of the eyelashes as well. Blepharitis is very common, especially among people who have oily skin, dandruff or dry eyes.
- Blepharitis increases the risk of developing a chalazion or stye.
Figure 5. Blepharitis
What causes blepharitis ?
Everyone has some bacteria on their skin. Some people, however, have more bacteria at the base of their eyelashes than other people. This can cause dandruff-like flakes to form. Also, some people have problems with oil glands in their eyelids (e.g. decrease or breakdown of the normal oils produced by the eyelid) leading to blepharitis.
Blepharitis is more likely to be seen in people with:
- A skin condition called seborrheic. This problem involves the scalp, eyebrows, eyelids, skin behind the ears, and the creases of the nose
- Allergies that affect the eyelashes (less common)
- Excess growth of the bacteria that are normally found on the skin
- Rosacea, which is a skin condition that causes a red rash on the face.
Symptoms of blepharitis
Symptoms include:
- Red, irritated eyelids
- Scales that stick to the base of the eyelashes
- Burning feeling in the eyelids
- Crusting, itching and swelling of the eyelids
You may feel like you have sand or dust in your eye when you blink. Sometimes, the eyelashes may fall out. The eyelids may become scarred if the condition continues long-term.
Exams and Tests for blepharitis
The health care provider can most often make the diagnosis by looking at the eyelids during an eye exam. Special photos of the glands that produce oil for the eyelids can be taken to see if they are healthy or not.
Blepharitis Treatment
Unfortunately there is not a cure for blepharitis, but there are a number of things you can do to help control the symptoms. The outcome is most often good with treatment. You may need to keep the eyelid clean to prevent the problem from coming back. Continuing treatment will ease redness and help make your eyes more comfortable. Treatments include 7:
- Warm compresses
Wet a clean washcloth with warm water and wring it out until somewhat dry. Place the washcloth over your closed eyes for at least 1 minute 8. Wet the washcloth as often as needed so it stays warm. This will help loosen the flakes sticking around your eyelashes. It also helps keep nearby oil glands from clogging.
- Eyelid scrubs
Soak a clean washcloth, cotton swab (Q-tip) applicator, or lint-free pad in warm water. Then use it to gently scrub the base of your eyelashes. Scrub for about 15 seconds.
- Antibiotics
Your ophthalmologist may have you use an antibiotic ointment on your eyes. Put a small amount of ointment on a clean fingertip or a cotton swab (Q-tip). Gently apply the ointment to the base of your eyelashes. Do this just before bedtime, or as your doctor recommends. Your doctor might prescribe an antibiotic medicine for you to take by mouth.
- Eye drops
Artificial tears or steroid eye drops may reduce redness, swelling and dry eye. Your ophthalmologist might prescribe an antibiotic eye drop to help the oil glands work better.
- Skin and eyelid hygiene
It is very important to keep your eyelids, skin and hair clean. This keeps your blepharitis symptoms under control. Carefully wash your eyelashes every day with baby shampoo. Also, wash your hair, scalp and eyebrows with an antibacterial shampoo. There are some new antiseptic sprays you can use on the skin that keep bacteria from growing too much.
Avenova™ by NovaBay (Emeryville, CA) is a prescription eyelid daily hygiene product for use in managing the symptoms associated with anterior and posterior blepharitis. The product contains Neutrox, which is pure 0.01% hypochlorous acid in a normal saline solution. Hypochlorous acid is a naturally occurring substance produced by our white blood cells 9.
The 0.01% hypochlorous eyelid cleanser is indicated for the removal of debris from the lid margin. It is a non-detergent-based product that is suitable for daily eyelid and eyelash hygiene. This eyelid cleanser does not contain surfactants, which can strip oils and dry the skin 10 and cause a dermatitis 11. The product is packaged in a spray bottle and is designed to be applied onto a cotton pad or cotton-tipped applicator, which is wiped along the eyelashes, eyelids, and the periocular skin, as needed.
In vitro testing shows that hypochlorous acid in solution is not only effective against a wide variety of bacteria, but also neutralizes the toxins produced by bacteria 12, known to cause ocular irritation 13. It potentially reduces the bacterial load on the eyelids and has shown broad spectrum anti-microbial activity in vitro.
What is Meibomianitis
Meibomianitis is inflammation of the meibomian glands, a group of oil-releasing (sebaceous) glands in the eyelids 14. These glands have tiny openings to release oils onto the surface of the cornea.
Causes of Meibomianitis
Any condition that increases the oily secretions of the meibomian glands will allow excess oils to build up on the edges of the eyelids 15. This allows for the excess growth of bacteria that are normally present on the skin.
These problems can be caused by allergies, hormone changes during adolescence, or skin conditions such as rosacea and acne.
Meibomianitis is often associated with blepharitis, which can cause a buildup of a dandruff-like substance at the base of the eyelashes.
In some people with meibomianitis, the glands will be plugged so that there is less oil being made for the normal tear film. These people often have symptoms of dry eye.
Prevention of meibomianitis
Keeping your eyelids clean and treating associated skin conditions will help prevent meibomianitis 16.
Symptoms of Meibomianitis
Symptoms include:
- Swelling and redness of eyelid edges
- Symptoms of dry eye
- Slight blurring of vision due to excess oil in tears — most often cleared by blinking
- Frequent styes
Exams and Tests of Meibomianitis
Meibomianitis can be diagnosed by an eye exam. Special tests are not required.
Treatment of Meibomianitis
Standard treatment involves:
- Carefully cleansing the edges of the lids
- Applying moist heat to the affected eye
These treatments will usually reduce symptoms in most cases.
Your health care provider may prescribe an antibiotic ointment to apply to the lid’s edge.
Other treatments may include:
- Having an eye doctor perform meibomian gland expression to help clear the glands of secretions.
- Inserting a small tube (cannula) into each gland opening to wash out thickened oil.
- Taking tetracycline antibiotics for several weeks.
- Using LipiFlow 17, a device that automatically warms the eyelid and helps clear the glands.
- Taking fish oil to improve the flow of oil from the glands.
- Using a medicine containing hypochlorous acid, this is sprayed onto the eyelids. This may be particularly useful in people who have rosacea.
You may also need treatment for general skin conditions such as acne or rosacea.
Outlook (Prognosis) for Meibomianitis
Meibomianitis is not a vision-threatening condition. However, it may be a long-term (chronic) and recurring cause of eye irritation. Many people find the treatments frustrating because results are not often immediate. Treatment, however, will often help reduce symptoms.
What is Periorbital cellulitis
Periorbital cellulitis is an infection of the eyelid or skin around the eye 18.
Figure 6. Periorbital cellulitis

Causes of Periorbital cellulitis
Periorbital cellulitis commonly affects children under 18 months old, though it can occur at any age.
This infection can occur after a scratch, injury, or bug bite around the eye, which allows germs to enter the wound. It can also extend from a nearby site that is infected, such as the sinuses.
Symptoms of Periorbital cellulitis
Symptoms include:
- Redness around the eye or in the white part of the eye
- Swelling of the eyelid, whites of eyes, and surrounding area
This condition does not often affect vision or cause eye pain.
Exams and Tests for Periorbital cellulitis
The health care provider will examine the eye and ask about the symptoms.
Tests that may be ordered include:
- Blood culture
- Blood tests (complete blood count)
- CT scan
- MRI scan
Treatment of Periorbital cellulitis
Antibiotics are given by mouth, by shots, or through a vein (intravenously; IV) to help fight the infection.
Outlook (Prognosis) of Periorbital cellulitis
Periorbital cellulitis almost always improves with treatment. In rare cases, the infection spreads into the eye socket, the tissues that surround the eye, and the eyeball itself. This infection is called orbital cellulitis.
When to see a Medical Professional
See your provider right away if:
- The eye becomes red or swollen
- Symptoms get worse after treatment
- Fever develops along with eye symptoms
- It is difficult or painful to move the eye
- The eye looks like it is sticking (bulging) out
- There are vision changes
What is Orbital cellulitis
Orbital cellulitis is an infection of the fat and muscles around the eye 19. It affects the eyelids, eyebrows, and cheeks. It may begin suddenly or be a result of an infection that gradually becomes worse.
Causes of Orbital cellulitis
Orbital cellulitis is a dangerous infection, which can cause lasting problems. Orbital cellulitis is different than periorbital cellulitis, which is an infection of the eyelid or skin around the eye.
In children, it often starts out as a bacterial sinus infection from Haemophilus influenza. The infection used to be more common in young children, under the age of 7. It is now rare due to a vaccine that helps prevent this infection.
The bacteria Staphylococcus aureus, Streptococcus pneumoniae, and beta-hemolytic streptococci may also cause orbital cellulitis.
- Orbital cellulitis infections in children may get worse very quickly and can lead to blindness. Medical care is needed right away.
Prevention of Orbital cellulitis
Getting scheduled HiB vaccine shots will prevent the infection in most children. Young children who share a household with a person who has this infection may need to take antibiotics to avoid getting sick.
Prompt treatment of a sinus or dental infection may prevent it from spreading and becoming orbital cellulitis.
Figure 7. Orbital cellulitis

Symptoms of Orbital cellulitis
Symptoms may include:
- Painful swelling of upper and lower eyelid, and possibly the eyebrow and cheek
- Bulging eyes
- Decreased vision
- Pain when moving the eye
- Fever, often 102°F (38.8°C) or higher
- General ill feeling
- Difficult eye movements, perhaps with double vision
- Shiny, red or purple eyelid
Exams and Tests for Orbital cellulitis
Tests commonly done include:
- CBC (complete blood count)
- Blood culture
- Spinal tap in affected children who are very sick
Other tests may include:
- X-ray of the sinuses and surrounding area
- CT scan or MRI of the sinuses and orbit
- Culture of eye and nose drainage
- Throat culture
Treatment of Orbital cellulitis
In most cases, a hospital stay is needed. Treatment most often includes antibiotics given through a vein. Surgery may be needed to drain the abscess, or relieve pressure in the space around the eye.
- An orbital cellulitis infection can get worse very quickly. A person with this condition must be checked every few hours.
Outlook (Prognosis) of Orbital cellulitis
With prompt treatment, the person can recover fully.
Possible Complications of Orbital cellulitis
Complications may include:
- Cavernous sinus thrombosis (formation of a blood clot in a cavity at the base of the brain)
- Hearing loss
- Septicemia or blood infection
- Meningitis
- Optic nerve damage and loss of vision
When to see a Medical Professional
- Orbital cellulitis is a medical emergency that needs to be treated right away. See your health care provider if there are signs of eyelid swelling, especially with a fever.
What is Dacryoadenitis
Dacryoadenitis is inflammation of the tear-producing gland (lacrimal gland) 20.
Causes of Dacryoadenitis
Acute dacryoadenitis is most commonly due to viral or bacterial infection 21. Common causes include mumps, Epstein-Barr virus, staphylococcus, and gonococcus.
Chronic dacryoadenitis is most often due to noninfectious inflammatory disorders. Examples include sarcoidosis, thyroid eye disease, and orbital pseudotumor.
Prevention of dacryoadenitis
Mumps can be prevented by getting vaccinated. You can avoid getting infected with gonococcus, the bacteria that cause gonorrhea, by using safe sex practices. Most other causes cannot be prevented.
Symptoms of dacryoadenitis
Symptoms may include:
- Swelling of the outer portion of the upper lid, with possible redness and tenderness
- Pain in the area of swelling
- Excess tearing or discharge
- Swelling of lymph nodes in front of the ear
Exams and Tests for dacryoadenitis
Dacryoadenitis can be diagnosed by an examination of the eyes and lids. Special tests, such as a CT scan may be required to search for the cause. Sometimes a biopsy will be needed to make sure that a tumor of the lacrimal gland is not present.
Treatment of dacryoadenitis
If the cause of dacryoadenitis is a viral condition such as mumps, rest and warm compresses may be enough. In other cases, the treatment depends on the disease that caused dacryoadenitis.
Outlook (Prognosis) of dacryoadenitis
Most people will fully recover from dacryoadenitis 22. For more serious causes, such as sarcoidosis, the outlook depends on the disease that caused this condition.
Possible Complications of dacryoadenitis
Swelling may be severe enough to put pressure on the eye and distort vision. Some people who were first thought to have dacryoadenitis may turn out to have cancer of the lacrimal gland.
What is Dacryocystitis
Dacryocystitis is infection of the tear (lacrimal) sac usually due to a blockage in the tear (nasolacrimal) duct 23. The usual cause is a staphyloccocal or streptococcal species, typically as a consequence of nasolacrimal duct obstruction.
In acute dacryocystitis, the patient presents with pain, redness, and edema around the lacrimal sac. Diagnosis is suspected based on symptoms and signs and when pressure over the lacrimal sac causes reflux of mucoid material through the puncta. Initial treatment is with warm compresses and oral antibiotics for mild cases or IV antibiotics for severe cases. The antibiotic is usually a 1st-generation cephalosporin or penicillinase-resistant synthetic penicillin. If the infection does not respond as expected, consideration should be given to methicillin-resistant Staphylococcus aureus (MRSA), and antibiotics changed accordingly. The abscess can be drained and the antibiotics can be changed based on culture results if the initial antibiotic proves ineffective.
Patients with chronic dacryocystitis usually present with a mass under the medial canthal tendon and chronic conjunctivitis. Definitive treatment for resolved acute dacryocystitis or chronic conjunctivitis is usually surgery that creates a passage between the lacrimal sac and the nasal cavity (dacryocystorhinostomy).
Complications of dacryocystitis
- Fistula formation
- Lacrimal sac abscess
- Orbital cellulitis
- Meningitis
- Cavernous sinus thrombosis
Risk Factors of Dacryocystitis
- Almost always related to nasolacrimal duct obstruction.
- Nasal pathologies like nasal septum deviation, rhinitis and inferior turbinate hypertrophy on the same side.
- Female is also a known risk factor for the development of this infectious condition due to narrow duct diameter.
- The presence of dacryoliths at various levels of the lacrimal drainage system.
- The occurrence of acute dacryocystitis being more prevalent with increasing age.
Causes of Dacryocystitis
Dacryocystitis usually occurs because of obstruction of the nasolacrimal duct 24. The obstruction may be an idiopathic inflammatory stenosis (primary acquired nasolacrimal duct obstruction) or maybe secondary to trauma, infection, inflammation, neoplasm, or mechanical obstruction (secondary acquired lacrimal drainage obstruction). Obstruction of the nasolacrimal duct leads to stagnation of tears in a pathologically closed lacrimal drainage system which can result in dacryocystitis
Symptoms and Signs of Dacryocystitis
Congenital dacryocystitis is a serious disease associated with significant morbidity and mortality. If it is not treated promptly and aggressively, newborn infants can experience orbital cellulitis (because the orbital septum is formed poorly in infants), brain abscess, meningitis, sepsis, and death.
Acquired dacryocystitis can be acute or chronic. Acute dacryocystitis is heralded by the sudden onset of pain and redness in the medial canthal region.
Acute dacryocystitis
- Sudden onset of pain, redness, and edema overlying the lacrimal sac area.
- It is not uncommon for the sac to rupture and fistulize through the skin. This fistula commonly closes after a few days of drainage.
- Conjunctival injection and preseptal cellulitis often occur in conjunction with acute dacryocystitis.
- More serious sequelae of acute dacryocystitis is the extension into the orbit with formation of an abscess and development of orbital cellulitis.
Chronic Dacryocystitis
- Tearing is the most common presentation
- Mattering:
- 1. This is caused by the obstruction of drainage of the mucous layer of the tear film with collection of debris and denuded epithelial cells from the surface of the eye.
- 2. Chronic low grade bacterial infection inside the lacrimal sac.
How is Dacryocystitis Diagnosed
- The diagnosis is clinical in most cases.
- Blood counts may reveal leucocytosis.
- Antineutrophilic cytoplasmic antibody testing may be useful to rule out Wegener’s granulomatosis.
- Imaging is rarely needed. In most cases it may reveal enlargement of the sac or foreign bodies or masses. Post traumatic cases or cases suspected of harboring an occult malignancy, Computer Tomography (CT) scan may be needed.
- Dacryocystography and dacryoscintigraphy are useful to detect anatomical abnormalities.
- Subtraction DCG with a CT scan is also useful in understanding anatomical features of the lacrimal sac and surrounding structures.
- The fluorescein dye disappearance test is useful in the clinic especially in those who cannot be syringed in the clinic. Prolonged retention of the dye usually more than 5 minutes indicates delayed drainage. The Jones test is useful to differentiate a functional block from an anatomical block.
- Nasal endoscopy is useful to rule out hypertrophy of the inferior turbinate, septal deviation and inferior meatal narrowing
Management of dacryocystitis
Management of acute dacryocystitis :
- Application of heat
- Systemic antibiotics
- Percutaneous abscess drainage
- DCR (dacryocystorhinostomy) few weeks after acute infection resolves.
Management of chronic dacryocystitis :
- Definitive treatment is a dacryocystorhinostomy, which can be performed as an external or internal endoscopic procedure. Relative contraindications to an internal endoscopic approach would be possible retained foreign body, dacryoliths, suspicion of tumor, or difficult intraoperative nasal visualization.
What is Trachoma
Trachoma is an infection of the eye caused by bacteria called chlamydia 25. Trachoma is the most common infectious cause of blindness in the world and is due to recurrent ocular infection with Chlamydia trachomatis 26. Trachoma still causes 15% of the world’s blindness 27. Adult inclusion conjunctivitis and neonatal inclusion conjunctivitis are relatively important causes of conjunctivitis in both the developed and the developing world. Other chlamydial subtypes and species can infect humans, and lymphogranuloma venereum, C. psittaci, and C. pneumoniae occasionally have been associated with conjunctivitis 28. Repeat infection with this organism leads to conjunctival inflammation and scarring, trichiasis, and ultimately blinding corneal opacification.
The World Health Organization (WHO) reports trachoma is endemic to more than 50 countries, with most blinding trachoma in Africa 26. An estimated 21 million people are living with active trachoma and another 2.2 million people are blind or severely visually impaired 26. Furthermore, 7.3 million people suffer from trichiasis and are at risk for developing blindness.
Epidemiologic studies have shown active trachoma is most common in young children with the prevalence of active trachoma decreasing with age. The long-term sequelae of trachoma infection, including scarring, trichiasis and corneal opacification in adults relates to their exposure to active trachoma when they were young. The gender distrubtion of active trachoma is similar; however, scarring and trichiasis are more common in women than men because women are more likely to care for young children and have longer exposure to the disease.
Blindness from trachoma is due to recurrent episodes of active infection 26. The initial infection is confined to the conjunctival epithelium and triggers an immune response. Repeat infections with subsequent inflammatory responses results in tissue destruction, scarring, cicatricial entropion with trichiasis, and corneal opacification from lashes rubbing against the cornea.
Causes of Trachoma
Trachoma is caused by four ocular serotypes of Chalmydia trachomatis: A, B, Ba and C. Infection with genital serotypes D to K can cause isolated episodes of ophthalmia neonatorum in infants or inclusion conjunctivitis in adults and do not generally lead to blindness.
The condition occurs around the world. It is most often seen in rural areas of developing countries. Children are often affected. However, the scarring caused by the infection may not be noticed until later in life. The condition is rare in the United States. However, it is more likely to occur in crowded or unclean living conditions.
Trachoma is spread through direct contact with infected eye, nose, or throat fluids. It can also be passed by contact with contaminated objects, such as towels or clothes. Certain flies can also spread the bacteria.
Prevention of Trachoma
Spread of the infection can be limited by washing your hands and face often, keeping clothes clean, and not sharing items such as towels.
Symptoms of Trachoma
Most individuals are asymptomatic or have mild symptoms depending on the level of inflammation. It first appears as inflammation of the tissue lining the eyelids (conjunctivitis, or “pink eye”).
Symptoms begin 5 to 12 days after being exposed to the bacteria. The condition begins slowly. Symptoms, if present, are similar to those seen in any chronic conjunctivitis and include redness, discomfort, tearing, photophobia and muco-purulent discharge. Untreated, this may lead to scarring.
Symptoms may include:
- Cloudy cornea
- Discharge from the eye
- Swelling of lymph nodes just in front of the ears
- Swollen eyelids
- Turned-in eyelashes
Exams and Tests for Trachoma
The health care provider will do an eye exam to look for scarring on the inside of the upper eye lid, redness of the white part of the eyes, and new blood vessel growth into the cornea.
Lab tests are needed to identify the bacteria and make an accurate diagnosis.
The clinical manifestations of trachoma can be divided into findings associated with active disease and those associated with repeat infections.
Active Disease:
- Follicular Conjunctivitis: Follicles are dome-shaped collections of lympoid cells. The center of the follicle is avascular and has blood vessels that surround the round base. These appear as yellow-white elevations and are prominent on the everted upper eyelid in trachoma. Large conjunctival follicles located at the upper margin of the cornea may leave depressions known as ‘Herbert’s pits’ which are pathognomonic for trachoma.
- Papillary Hypertrophy: engorgement of small vessels with edema that can obscure deep tarsal vessels
- Corneal Pannus: vascularization of the upper cornea.
Repeat Infection and Inflammation:
- Conjunctival Scarring: White bands or lines that represent fibrosis
- Cicatricial Entropion and Trichiasis: Fibrotic scar tissue contraction causes the eyelid turning inward and lashes touching the eyeball.
- Corneal Opacification: secondary to repeat corneal irritation from inward turning eyelashes
Grading of Trachoma
The WHO grading system:
- Trachomatous Inflammation (TF): The presence of 5 or more follicles (>0.5 mm) in the upper tarsal conjunctiva
- Trachomatous Inflammation (TI): Inflammatory thickening of the tarsal conjunctiva that obscures more than half of the deep normal vessels
- Trachomatous Scarring (TS): The presence of scarring in the tarsal conjunctiva
- Trachomatous Trichiasis (TT): At least one lash rubs on the eyeball
- Corneal Opacity: Easily visible corneal opacity over the pupil
Treatment of Trachoma
Antibiotics can prevent long-term complications if used early in the infection. In certain cases, eyelid surgery may be needed to prevent long-term scarring, which can lead to blindness if not corrected.
The World Health Organization recommends the ‘SAFE’ strategy for the management of trachoma. This strategy was developed in 1997 by The Alliance for the Global Elimination of Blinding Trachoma by the year 2020 (GET 2020) and utilizes a 4 step approach:
- S: Surgery for Trichiasis
- A: Antibiotics for C. trachomatis infection
- F: Facial cleanliness
- E: Environmental change to improve sanitation and increase access to clean water
Outlook (Prognosis) of Trachoma
Outcomes are very good if treatment is started early before scarring and changes to the eyelids develop.
Possible Complications of Trachoma
If the eyelids become very irritated, the eyelashes may turn in and rub against the cornea. This can cause corneal ulcers, additional scars, vision loss, and possibly, blindness.
What is Conjunctivitis (Pink Eye) ?
Conjunctivitis is often called “pink eye” 29. It happens when the conjunctiva is irritated by an infection or allergies. Your eyes are red and swollen (inflamed), and sometimes they have a sticky discharge. You can have conjunctivitis in one or both eyes. Some types of pink eye are very contagious (easily spread from person to person).
There are four main types of conjunctivitis.
- Viral conjunctivitis is the most common type of pink eye. This conjunctivitis is very contagious and often spreads through schools and other crowded places. It usually causes burning, red eyes with a watery discharge.
- Bacterial conjunctivitis is also very contagious. An infection from bacteria causes this form of pink eye. With bacterial conjunctivitis, you have sore, red eyes with a lot of sticky pus.
- Allergic conjunctivitis is a type of pink eye that comes from an allergic reaction to something. It is not contagious. Allergic pink eye makes your eyes very itchy, red and watery.
- Irritants such as contact lenses and lens solutions, chlorine in a swimming pool, smog or cosmetics may also be an underlying cause of conjunctivitis.
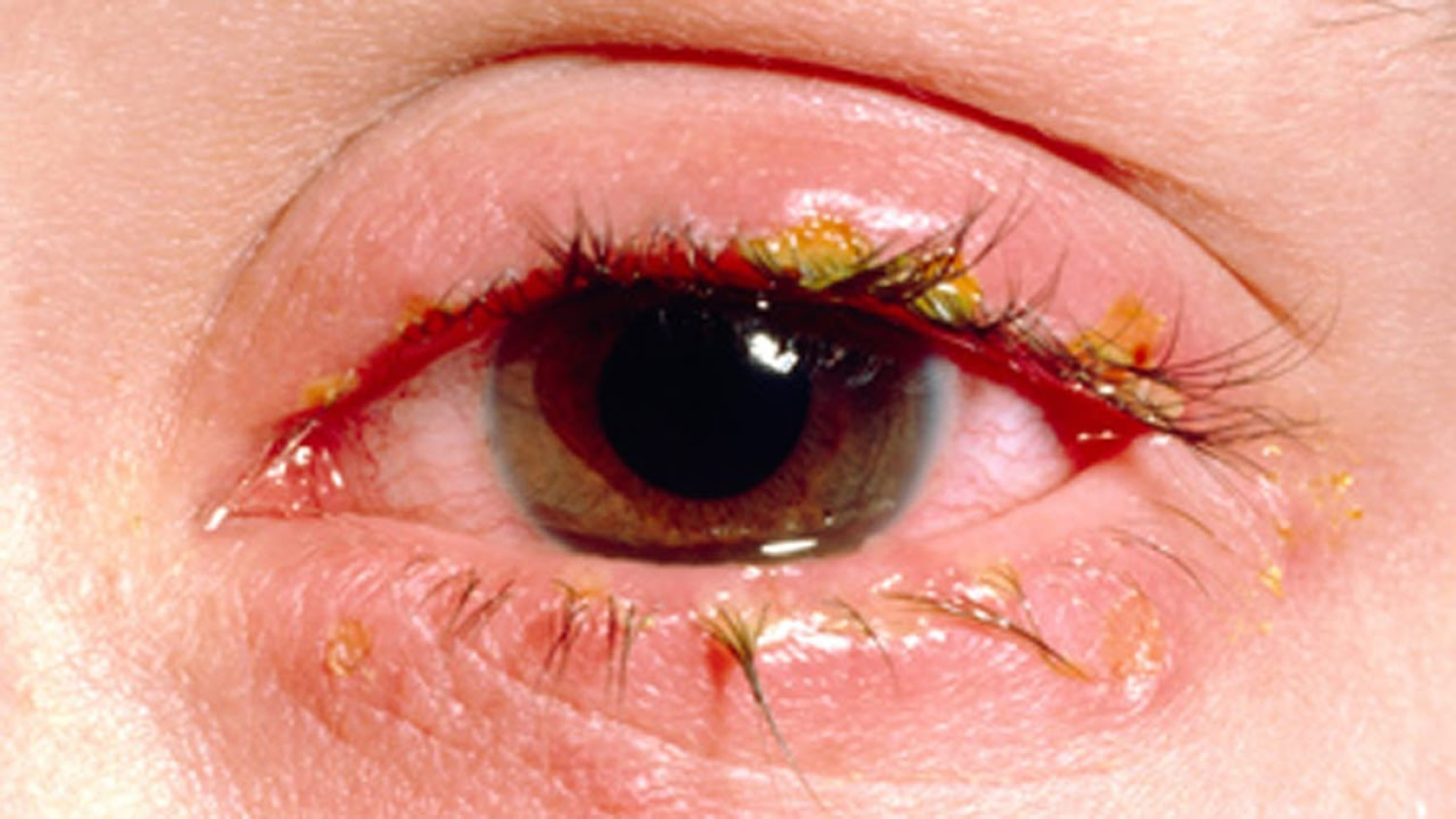
Figure 8. Conjunctivitis (pink eye)

Causes of Pink Eye (Conjunctivitis)
Conjunctivitis is most commonly caused by the same virus that causes the runny nose and sore throat of the common cold.
Bacterial infections cause conjunctivitis that produces lots of sticky pus in the eye. Some bacterial infections, however, may cause little or no discharge. Sometimes the bacteria that cause pink eye are the same that cause strep throat. Both bacterial and viral conjunctivitis are easily spread from person to person.
Sometimes having an allergic reaction to pollen or animals can cause conjunctivitis. So can irritation from cigarette smoke, car fumes, pool chlorine or other toxic substances. The main symptom of allergic pink eye is itchy eyes. Other symptoms include red, burning and tearing eyes and puffy eyelids. Allergic or irritant conjunctivitis is not contagious.
Pink Eye Symptoms
Pink eye symptoms may include 30:
- the feeling that something is in your eye, or a gritty sensation in your eye
- red eyes
- burning eyes
- itchy eyes
- painful eyes (this is usually with the bacterial form)
- watery eyes
- puffy eyelids
- blurry or hazy vision
- being extra sensitive to light
- lots of mucus, pus, or thick yellow discharge from your eye. There can be so much that your eyelashes stick together (usually with bacterial conjunctivitis).
Pink Eye Treatment
Treating your pink eye usually depends on the type of conjunctivitis you have.
If your conjunctivitis is caused by a viral infection, there are no specific treatments 31. Your body fights the virus on its own. Placing a cool, wet washcloth on your eyes can help make them feel more comfortable.
If your pink eye is caused by a bacterial infection, your ophthalmologist may prescribe antibiotic eye drops 31. Antibiotics do not treat an infection caused by a virus or by allergy 31.
If your conjunctivitis is due to allergies, you might be told to use certain eye drops to help with the itchiness and puffiness.
Sometimes conjunctivitis can be caused by a chemical or other substance in your eye. In this case, rinse the eye free of the substance. You might be told to use certain eye drops or ointment for the eyes.
Stop pink eye from spreading
Some conjunctivitis can spread from person to person 31. Follow these tips so you will not infect other people or re-infect yourself.
- Use a clean towel or tissue each time you wipe your face and eyes.
- Wash your hands very often. Always wash them before and after you eat, when you go to the bathroom, or after you sneeze or cough.
- Try not to touch your eyes. If you do, wash your hands right away.
- Bacteria can live in makeup. This can cause pink eye and even a dangerous infection of the cornea. Do not use eye makeup while your eyes are infected.
- Replace your makeup if you have an eye infection. And never share eye makeup with others.
- Make sure to clean your contact lenses exactly as your ophthalmologist recommends.
- If you have conjunctivitis, wash any discharge from around the eyes several times a day.
- Do not use the same eye drop dispenser/bottle for infected and non-infected eyes—even for the same person.
- Avoid sharing articles like towels, blankets, and pillowcases.
- Clean your eyeglasses.
- Clean, store, and replace your contact lenses as instructed by your eye health professional.
- Do not share eye makeup, face makeup, makeup brushes, contact lenses or containers, or eyeglasses.
- Avoid touching or rubbing your eyes.
Conjunctivitis usually goes away on its own within 1–2 weeks. If your symptoms last longer than that, you should see your ophthalmologist. He or she can make sure you don’t have a more serious eye problem.
What Is Bacterial Keratitis ?
Bacterial keratitis is an infection of the cornea 32. The cornea is the clear, dome-shaped window of the front of your eye.
Bacterial keratitis usually develops quickly. Left untreated it can cause blindness.
There are many different bacteria that cause keratitis. The two bacteria most commonly responsible for this type of infection in the U.S. are:
- Staphylococcus aureus
- Pseudomonas aeruginosa
Symptoms of bacterial keratitis may include:
- pain in the eye (often sudden)
- reduced vision
- increased light sensitivity
- excessive tearing
- discharge from your eye
See your doctor or ophthalmologist right away if you have any of these symptoms. This is especially important if they come on suddenly. If not treated, a bacterial keratitis eye infection can lead to blindness. Treatment must start right away to prevent vision loss 32.
Causes of Bacterial Keratitis
The two main causes of bacterial keratitis are:
- contact lens use, especially extended-wear lenses
- eye injury
You risk an infection from contact lenses if you wear them too long or do not take care of them correctly. Proper care of your contacts will lower your risk of developing a keratitis infection.
Prevent Infection With Proper Contact Lens Care
Follow your eye care provider’s instructions to wear, clean and store your contacts. These are some things to keep in mind:
- Wash your hands with soap and water and dry them with a lint-free towel before handling your contacts.
- Minimize contact with water. Remove lenses before going swimming or in a hot tub.
- Do not rinse or store your contacts in water (tap or sterile water).
- Do not put your lenses in your mouth to wet them.
- Do not use saline solution and rewetting drops to disinfect lenses. Neither is an effective or approved disinfectant.
- Follow your eye care professional’s schedule for wearing and replacing your contacts.
- Use the “rub and rinse” method to clean your contacts. Rub your contact lenses with your fingers, then rinse them with solution before soaking. Use this method even if the solution you are using is a “no-rub” variety.
- Rinse the contact lens case with fresh solution — not water. Then leave the empty case open to air dry.
- Keep the contact lens case clean and replace it regularly, at least every three months. Lens cases can be a source of contamination and infection. Do not use cracked or damaged lens cases.
- Do not re-use old solution or “top off” the solution in your lens case.
- Do not transfer contact lens solution into smaller travel-size containers.
- Do not allow the tip of the solution bottle to touch any surface. Keep the bottle tightly closed when not in use.
- Never wear your lenses after storage for 30 or more days without disinfecting them again.
Bacterial Keratitis Treatment
To diagnose bacterial keratitis, your ophthalmologist will discuss your symptoms with you. They may gently scrape the eye to take a small sample and test it for infection.
Bacterial keratitis is usually treated with antibiotic drops. Drops are usually put in frequently. Treatment may also involve steroid drops. You may need to return to your ophthalmologist several times.
If you and your ophthalmologist find and treat bacterial keratitis early, you may preserve your vision. In severe cases decreased vision or blindness may be the result. This is also true if the infection affects the center of the cornea. Sometimes a cornea transplant is needed to restore vision.
What is Fungal Keratitis ?
Fungal keratitis is an infection of the cornea 33. Fungal keratitis can develop quickly from an eye injury or contact lens use. It can cause blindness if it is not treated 33. In some cases, treatment cannot restore vision 33. In these cases, permanent vision impairment or blindness may occur.
There are many different fungi that can infect the cornea such as Fusarium, Aspergillus or Candida.
Keratitis. Keratitis is an infection or inflammation of the cornea.
Superficial keratitis involves the outer layers of the cornea. After this form of keratitis heals, there is usually no scar on the cornea.
Deep keratitis affects deeper layers of the cornea. There can be a scar on the cornea after it heals, which may or may not affect your vision. This will depend on the location of the scar.
Besides fungal keratitis, other types of keratitis include 33:
- Amoebic keratitis, which is an infection with amoeba. It is often caused by Acanthamoeba and usually affects contact lens wearers.
- Bacterial keratitis, which is an infection with bacteria
- Herpes keratitis, which is an infection with herpes simplex or herpes zoster viruses
- Photokeratitis, due to intense ultraviolet (UV) radiation exposure. Examples include snow blindness or welder’s arc eye.
Fungal Keratitis Causes
Fusaria are common fungi found in soil, water, and plants throughout the world 34. They are particularly common in warmer climates. Fungal keratitis can happen after an injury to the cornea involving plant material. One example is getting hit in the eye with a palm branch.
People who have a low immune response can also get fungal keratitis if they come in contact with the fungus. There is also a risk of developing fungal keratitis with contact lens use. Proper use and care of contact lenses can reduce your risk of getting a fungal infection if you wear contacts. Ask your ophthalmologist about proper contact lens care.
Fungal Keratitis Symptoms
Symptoms of fungal keratitis may include 35:
- reduced vision
- pain in the eye (often sudden)
- increased light sensitivity
- tearing
- excessive tearing or discharge from your eye
See your ophthalmologist right away if you experience any of these symptoms. This is especially important if these symptoms come on suddenly. You must start treatment right away to prevent possible blindness.
Fungal Keratitis Treatment
Your ophthalmologist may gently scrape the eye to take a small sample of material. They will test the sample for infection. This test will help diagnose whether your infection is fungal keratitis or bacterial keratitis 36.
Treatment of fungal keratitis usually includes antifungal eye drops and oral medications. If these medicines are not effective, you may need surgery, including corneal transplantation. In some cases, even corneal surgery will not restore vision. In these cases, permanent vision impairment or blindness may occur. That is why it is so important to see your ophthalmologist at the first sign of any ocular infection.
What is Herpes Keratitis ?
Herpes keratitis is a viral infection of the eye caused by the herpes simplex virus (HSV). There are two major types of the virus 37:
- Type I is the most common and primarily infects the face, causing the familiar “cold sore” or “fever blister.”
- Type II is the sexually transmitted form of herpes, infecting the genitals.
While both Type I and Type II herpes can spread to the eye and cause infection, Type I is by far the most frequent cause of eye infections. Infection can be transferred to the eye by touching an active lesion (a cold sore or blister) and then your eye.
Herpes Keratitis Causes
Type I herpes is very contagious and is commonly transmitted by skin contact with someone who has the virus 38. Almost everyone — about 90 percent of the population — is exposed to Type I herpes, usually during childhood Herpes Keratitis Causes. https://www.aao.org/eye-health/diseases/herpes-keratitis-cause.
After the original infection, the virus lies in a dormant state, living in nerve cells of the skin or eye. Reactivation can be triggered in a number of ways, including:
- stress
- sun exposure
- fever
- trauma to the body (such as injury or surgery)
- menstruation
- certain medications
Once herpes simplex is present in the eye, it typically infects the eyelids, conjunctiva and cornea 38. It may also infect the inside of the eye; however, this is much less common.
Herpes Keratitis Symptoms
The symptoms of herpes keratitis may include pain, redness, blurred vision, tearing, discharge and sensitivity to light 39.
If the infection is superficial, involving only the cornea’s outer layer (called the epithelium), it will usually heal without scarring. However, it if involves the deeper layers of cornea (which can happen after time), the infection may lead to scarring of the cornea, loss of vision and sometimes even blindness.
Left untreated, herpes keratitis can severely damage your eye.
Herpes Keratitis Treatment
Treatment of herpes keratitis depends on its severity 40. Mild infection is typically treated with topical and sometimes oral antiviral medication 40. Your ophthalmologist may gently scrape the affected area of the cornea to remove the diseased cells. In case of severe scarring and vision loss, a corneal transplant may be required.
It is very important to consult an ophthalmologist before beginning any treatment, because some medications or eyedrops may actually make the infection worse 40.
There is no complete cure for herpes; once the virus is in the body, you cannot get rid of it 40. However, if you develop herpes keratitis, there are some things you can do to help prevent recurring outbreaks:
- If you have an active cold sore or blister, avoid touching your eyes.
- Steroids can increase the herpes virus in the body. You should not use steroid eye drops unless you are taking an anti-viral medicine as well.
- Stop wearing contact lenses if you keep getting infections.
- See an ophthalmologist immediately if symptoms of ocular herpes return.
What Is Uveitis ?
Uveitis occurs when the middle layer of the eyeball gets inflamed (red and swollen). This layer, called the uvea, has many blood vessels that nourish the eye. Uveitis can damage vital eye tissue, leading to permanent vision loss 41.
Three types of uveitis
There are 3 types of uveitis. They are based on which part of the uvea is affected.
- Swelling of the uvea near the front of the eye is called anterior uveitis. It starts suddenly and symptoms can last up to 8 weeks. Some forms of anterior uveitis are ongoing, while others go away but keep coming back.
- Swelling of the uvea in the middle of the eye is called intermediate uveitis. Symptoms can last for a few weeks to many years. This form can go through cycles of getting better, then getting worse.
- Swelling of the uvea toward the back of the eye is called posterior uveitis. Symptoms can develop gradually and last for many years.
In severe cases, all layers may be involved 41.
Uveitis Causes
Doctors do not always know what causes uveitis. You are more likely to get uveitis if you have or have had 42:
- infections such as shingles virus, herpes simplex virus, syphilis, Lyme disease, and parasites such as toxoplasmosis.
- a systemic inflammatory disease such as inflammatory bowel disease (IBS), rheumatoid arthritis or lupus
- an eye injury
Smoking (cigarettes, cigars or pipes) also increases your risk of getting uveitis.
Uveitis Symptoms
Uveitis can develop suddenly. Symptoms can include 43:
- having a red eye with or without pain
- being very sensitive to bright light
- having blurry vision
- seeing “floaters” (specks or moving clouds in your vision) all of a sudden
See your ophthalmologist right away if you notice any of these symptoms.
Uveitis Diagnosis
Your ophthalmologist will examine the inside of your eye. Since uveitis is often connected with other diseases or conditions, some tests may be needed. They may include a physical exam, blood or skin tests, examination of eye fluids, and imaging tests, such as X-rays 44. Your ophthalmologist may ask about other diseases or health problems you have had.
How is uveitis treated ?
Uveitis needs to be treated right away to prevent lasting problems 44. Ophthalmologists often treat uveitis with eyedrop medicine that reduces inflammation (corticosteroids). They may also use an eye drop to widen (dilate) the pupil, which helps reduce pain and swelling. Sometimes medicine may need to be given by injection (shots) or taken by mouth. Often times, your ophthalmologist will work with a special kind of doctor called a rheumatologist to help treat you.
What is Cytomegalovirus Retinitis
Cytomegalovirus (CMV) retinitis is a viral infection of the retina of the eye resulting in inflammation 45.
A cytomegalovirus infection usually only causes symptoms in people with a weakened immune system. Certain medicines (like cancer therapy) and diseases (such as HIV/AIDS) can cause a weakened immune system.
People with AIDS who have a CD4 count of less than 250 cells/microliter or 250 cells/cubic millimeter should be examined regularly for this condition, even if they do not have symptoms. If you had cytomegalovirus retinitis in the past, ask your provider if you need treatment to prevent its return.
Causes of Cytomegalovirus retinitis
Cytomegalovirus retinitis is caused by a member of a group of herpes-type viruses. Infection with cytomegalovirus is very common. Most people are exposed to cytomegalovirus in their lifetime, but typically only those with weakened immune systems become ill from cytomegalovirus infection.
Serious cytomegalovirus infections can occur in people who have weakened immune systems as a result of:
- HIV/AIDS
- Bone marrow transplant
- Chemotherapy
- Drugs that suppress the immune system
- Organ transplant
Symptoms of Cytomegalovirus retinitis
Some people with cytomegalovirus retinitis have no symptoms.
If there are symptoms, they may include:
- Blind spots
- Blurred vision and other vision problems
- Floaters
Retinitis usually begins in one eye, but often progresses to the other eye. Without treatment, damage to the retina can lead to blindness in 4 to 6 months or less.
Exams and Tests of Cytomegalovirus retinitis
Cytomegalovirus retinitis is diagnosed through an ophthalmologic exam. Dilation of the pupils and ophthalmoscopy will show signs of cytomegalovirus retinitis.
Cytomegalovirus infection can be diagnosed with blood or urine tests that look for substances specific to the infection. A tissue biopsy can detect the viral infection and presence of cytomegalovirus virus particles, but this is rarely done.
Treatment of Cytomegalovirus retinitis
The goal of treatment is to stabilize or restore vision and prevent blindness. Long-term treatment is often needed. Medicines may be given by mouth (orally), through a vein (intravenously), or injected directly into the eye (intraviteously).
Outlook (Prognosis) of Cytomegalovirus retinitis
Even with treatment, the disease can worsen to blindness. This progression may be because the virus becomes resistant to the antiviral drugs so that the drugs are no longer effective, or because the person’s immune system has deteriorated further.
Cytomegalovirus retinitis may also lead to retinal detachment, in which the retina detaches from the back of the eye, causing blindness.
Possible Complications of Cytomegalovirus retinitis
Complications that may result include:
- Kidney impairment (from drugs used to treat the condition)
- Low white blood cell count (from drugs used to treat the condition).
Eye infections from contact lens
Millions of people wear contact lenses safely every day. Contact lenses are the number one choice for many people with vision correction needs. Contact lenses can be used to correct a variety of vision disorders such as Myopia (nearsightedness), Hyperopia (farsightedness), Astigmatism, and Presbyopia (poor focusing with reading material and other near vision tasks). But there is a risk of getting an eye infection from them.
Keratitis is the most common infection from wearing contact lenses 46. It is when the cornea—the clear, front window of the eye — becomes infected. In some cases, it can scar the cornea, affecting your vision. If the cornea is severely scarred, a cornea transplant may be needed to have clear vision again.
- Hygiene is the most critical aspect of successful long-term contact lens wear.
What causes contact lens infections ?
There are a number of things that can cause a contact lens-related infection. Some causes of infection may include:
- using extended-wear lenses
- sleeping in your contact lenses
- having microbes build up under the lens
- infection from herpes virus
- bacteria or fungus
- not keeping lenses or cases clean, or reusing or topping off contact lens solution.
Important Contact Lens Care Tips
- Always wash and thoroughly dry your hands before handling contact lenses.
- Carefully and regularly clean contact lenses as directed by your optometrist. Rub the contact lenses with your fingers and rinse them thoroughly before soaking the lenses overnight in multipurpose solution that completely covers each lens.
- Store lenses in the proper lens storage case, and replace the case at least every three months. Clean the case after each use, and keep it open and dry between cleanings.
- Use only products recommended by your optometrist to clean and disinfect your lenses. Saline solution and rewetting drops do not disinfect lenses.
- Use only fresh solution to clean and store contact lenses. Never reuse old solution. Change the contact lens solution according to the manufacturer’s recommendations, even if you don’t use the lenses daily.
- Always follow the recommended contact lens replacement schedule your optometrist prescribes. Get new lenses when recommended. Don’t try to extend the life of your contacts by wearing them too long. Only keep lenses as long as your prescriber recommends. For example, one-month contact lenses should only be used for 30 days after opening the package.
- Remove contact lenses before swimming or entering a hot tub.
- Follow recommended wearing schedule.
- Do not substitute sterile saline solutions for multi-purpose solutions.
- Rub and rinse your contact lenses as directed by your eye care professional.
- Do not “top-off” the solutions in your case. Always discard all of the leftover contact lens solution after each use. Never reuse any lens solution.
- Clean, rinse and air-dry your lens case each time lenses are removed.
- Do not expose your contact lenses to any water: tap, bottled, distilled, lake or ocean water.
- See your eye care professional if you experience any symptoms of eye irritation or infection.
Contact lens infection symptoms
Symptoms of contact lens-related infections include:
- blurry vision
- unusual redness of the eye
- pain in the eye
- tearing or discharge from the eye
- being extra sensitive to light
- feeling like there is something in your eye
Some contact lens-related eye infections can cause serious vision loss or even blindness. If you have any of these symptoms, is important to see your eye doctor as soon as possible.
Baby eye infection
Neonatal ophthalmia, also called neonatal conjunctivitis, a relatively common illness, is defined as conjunctivitis occurring within the first four weeks of life 47 affecting 1.6% to 12% of all newborns 48. Originally, this term only referred to cases caused by Neisseria gonorrhoeae, but the term currently encompasses any conjunctivitis in this age group. In a newborn baby, serious eye infections may result from exposure to bacteria during passage through the birth canal—which is why all infants are treated with antibiotic eye ointment or drops in the delivery room 49. Such infections must be treated early to prevent serious complications.
Neisseria gonorrhoeae now accounts for <1% of reported cases of neonatal ophthalmia in the United States, while that due to Chlamydia trachomatis ranges from 2% to 40% 50. Other bacteria such as Staphylococcus species, Streptococcus species, Haemophilus species and other Gram-negative bacterial species account for 30% to 50% of cases 51. Much less commonly, neonatal conjunctivitis is caused by viral infections (herpes simplex, adenovirus, enteroviruses). Infectious conjunctivitis must be distinguished from eye discharge secondary to blocked tear ducts and from conjunctivitis due to exposure to chemical or other irritants.
In most instances, neonatal ophthalmia (baby eye infection) is a mild illness. The exception is ophthalmia due to infection with Neisseria gonorrhoeae 51. Without preventive measures, gonococcal ophthalmia occurs in 30% to 50% of infants exposed during delivery 52, 53 and may progress quickly to corneal ulceration, perforation of the globe and permanent visual impairment 54. Infants at increased risk for gonococcal ophthalmia are those whose mothers are at risk for sexually transmitted infections (STIs) 55.
Preventing neonatal conjunctivitis
The Canadian Paediatric Society recommends that ocular prophylaxis with 1% silver nitrate, 0.5% erythromycin ointment, or 1% tetracycline hydrochloride be given to all newborns, including those born by cesarean section, in the first hour after birth 56. It is important to note that routine ocular prophylaxis does not prevent chlamydial neonatal conjunctivitis; and that although gonorrheal neonatal conjunctivitis has become relatively rare with the introduction of ocular prophylaxis, it must continue to be considered, given its high propensity to cause severe ocular destruction and blindness 57.
Erythromycin Ointment
That goo, in most hospitals, is erythromycin ointment, and it serves as a simple, harmless, cost-effective means of preventing blindness 58. The blindness in question results from infection with 1 of 2 sexually transmitted infections, chlamydia (see Trachoma above) and gonorrhea (often people get both at the same time). Both infections can progress rapidly in newborns’ eyes, damaging the clear part over the pupils (corneas) and causing irreversible harm. Men and women can harbor chlamydia and gonorrhea infections without any symptoms. Obstetricians test most women for these infections during their pregnancies and treat them if their tests come back positive, but mothers can still pick up those diseases after their tests come back, so to be safe we treat everyone.
Erythromycin ointment is close to 100% effective in preventing gonorrhea eye infections, but chlamydia infections can still pop up as long as 2 weeks after delivery. When this happens, only oral antibiotics provide effective treatment. Because of the danger from chlamydia, most pediatricians test newborns’ eyes for the disease before prescribing antibiotics. Other eye infections may also threaten a baby’s vision, including herpes simplex virus and Staphylococcus aureus. There are several other reasons a baby might develop eye discharge in the first few weeks of life, including a rare allergic reaction to erythromycin.
Causes of neonatal conjunctivitis (ophthalmia neonatorum)
Causes of ophthalmia neonatorum include the following:
- Chemical
Bacterial
- Chlamydia trachomatis
- Neisseria gonorrhoeae
- Haemophilus species
- Streptococcus pneumoniae
- Staphylococcus aureus
- Staphylococcus epidermidis
- Streptococcus viridans
- Escherichia coli
- Pseudomonas aeruginosa
- Other
Viral
- Adenovirus
- Herpes simplex virus
Chemical conjunctivitis
Chemical conjunctivitis accounts for most cases of neonatal conjunctivitis 59, presenting as a mild, purulent conjunctivitis within the first 24 hours of life. It is most commonly associated with silver nitrate prophylaxis, or secondary to prophylaxis with other agents such as erythromycin or tetracycline 48. Chemical conjunctivitis is a self-limiting condition that does not require any diagnostic tests or treatment 60.
Non–sexually transmitted bacteria
Non–sexually transmitted bacteria account for 30% to 50% of cases of neonatal conjunctivitis 56. The most commonly isolated microorganisms are listed above under causes bacterial. The role of Staphylococcus aureus is unclear, as it is commonly cultured from the eyes of asymptomatic infants 61. Most cases of bacterial neonatal conjunctivitis can be treated with topical antibiotics (aminoglycosides, polymyxin B sulfate–trimethoprim solution, macrolides, or fluoroquinolones) 62. Neonatal conjunctivitis caused by Pseudomonas is rare but can present with eyelid edema, erythema, and purulent discharge causing corneal perforation, endophthalmitis, blindness, and possibly death 59. Presumptive diagnosis can be made from Gram stain results, and a definitive diagnosis is based on conjunctival culture results 59. Systemic antibiotics have poor penetration into the anterior chamber of the eye, and thus both systemic and topical aminoglycoside antibiotics, and occasionally subconjunctival injections, are required for effective treatment. These infants require isolation and assessment by an ophthalmologist 48.
Sexually transmitted bacteria
Chlamydia trachomatis
Sexually transmitted bacteria including Chlamydia trachomatis account for up to 40% of all cases of neonatal conjunctivitis in Canada 48. An infant born vaginally to a mother with chlamydial cervicitis has a 50% to 75% chance of acquiring the bacteria in the nasopharynx, rectum, vagina, or conjunctiva 63. Of neonates with proven exposure to chlamydia, 30% to 50% will develop conjunctivitis 64. The prevalence of chlamydial infections is higher in the spring and summer months 65. The incubation period is typically 1 week after delivery; however, it varies from 5 to 14 days or earlier if membranes ruptured prematurely 66. The clinical manifestations vary from mild conjunctival injection with scant watery discharge to severe mucopurulent discharge with eyelid edema, chemosis, and pseudomembrane formation 67, 64. Loss of vision is very rare. Most cases of chlamydial infections resolve spontaneously without complications, but, if left untreated, superficial corneal vascularization and conjunctival scarring can occur 64. Newborns with conjunctivitis should have specimens of their conjunctiva and pharynx sent for culture. The American Academy of Pediatrics recommends a 14-day course of systemic erythromycin (50 mg/kg/d, divided in 4 doses) 68. Topical therapy is not indicated 64. Erythromycin has a 10% to 20% failure rate and thus some infants will require a second or occasionally a third course of erythromycin 69. Parents should be informed of the potential risk of pyloric stenosis and counseled on monitoring 64. A small study has demonstrated that a short course of oral azithromycin (20 mg/kg once daily for 3 days) might be an effective treatment alternative; however, further studies are needed 70. The infant’s mother and her sexual partners should be treated for chlamydia 57.
Neisseria gonorrhoeae
Neisseria gonorrhoeae accounts for less than 1% of all reported cases of neonatal conjunctivitis in Canada 56. In the absence of adequate prophylaxis, 30% to 42% of infants born by vaginal delivery to infected mothers will develop gonococcal neonatal conjunctivitis 67. The transmission rate is higher in mothers with concomitant chlamydial infection 71. Infants born to mothers with known gonococcal infection should be treated with a single parenteral dose of cefotaxime or ceftriaxone 72. If left untreated, gonorrheal neonatal conjunctivitis can lead to corneal scarring, ulceration, panophthalmitis, and perforation of the globe within 24 hours 72. The disease typically presents with profound chemosis, edema of the eyelids, and abundant purulent discharge that might be blood-tinged from superficial hemorrhage within 2 to 5 days of birth; however, it can manifest up to 2 to 3 weeks after delivery 72. Infants with gonorrheal neonatal conjunctivitis should be hospitalized, treated with frequent irrigation of the conjunctiva and intravenous or intramuscular administration of ceftriaxone (25 to 50 mg/kg, to a maximum dose of 125 mg), and evaluated for disseminated gonococcal disease (eg, arthritis, sepsis, meningitis) 73, 74. The infant’s mother and her sexual partners should be treated for gonorrhea 73.
Viral conjunctivitis
Viral conjunctivitis is most commonly caused by adenovirus and herpes simplex virus 67. Infants with adenovirus neonatal conjunctivitis might present with petechial hemorrhage or occasionally with large subconjunctival hemorrhages 73. Lymphadenopathy is associated with approximately 50% of cases of viral conjunctivitis 73. Infants with conjunctivitis caused by herpes simplex virus might be diagnosed late, as they are commonly treated empirically for chlamydial or gonococcal infection 67. Herpetic lesions on the borders of the eyelids are common and present 6 to 14 days after birth 67. These infants require diagnostic evaluation, including lumbar puncture, and assessment by an ophthalmologist. Treatment includes systemic acyclovir (60 mg/kg in divided doses 3 times a day) for 14 days, coupled with topical ophthalmic solution (ie, 1% trifluridine, 0.1% iododeoxyuridine, or 3% vidarabine) 68, 68.
Eye infections that occur after the newborn period:
These infections may be unsightly, because of the redness of the eye and the yellow discharge that usually accompanies them, and they may make your child uncomfortable, but they are rarely serious. Several different viruses, or bacteria, may cause them. If your pediatrician feels the problem is caused by bacteria, antibiotic eye drops are the usual treatment. Conjunctivitis caused by viruses should not be treated with antibiotics.
If the white of your child’s eye and the inside of his lower lid become red, he probably has a condition called conjunctivitis. Also known as pinkeye, this inflammation, which can be painful and itchy, usually signals an infection, but may be due to other causes, such as an irritation, an allergic reaction, or (rarely) a more serious condition. It’s often accompanied by tearing and discharge, which is the body’s way of trying to heal or remedy the situation.
If your child has a red eye, he needs to see the pediatrician as soon as possible. Eye infections typically last seven to ten days. The doctor will make the diagnosis and prescribe necessary medication if it is indicated. Never put previously opened medication or someone else’s eye medication into your child’s eye. It could cause serious damage.
- Eye infections are very contagious !
Except to administer drops or ointment, you should avoid direct contact with your child’s eyes or drainage from them until the medication has been used for several days and there is evidence of clearing of the redness. Carefully wash your hands before and after touching the area around the infected eye.
- National Eye Institute, Department of Health and Human Services. Eyelid Disorders – Chalazion & Stye. https://www.nei.nih.gov/faqs/eyelid-disorders-chalazion-stye[↩]
- Lindsley K, Nichols JJ, Dickersin K. Interventions for acute internal hordeolum. Cochrane Database Syst Rev. 2013;(4):CD007742.[↩][↩][↩]
- Lederman C, Miller M. Hordeola and chalazia. Pediatr Rev. 1999;20(8):283–284.[↩][↩]
- American Association for Pediatric Ophthalmology and Strabismus. Chalazion. https://aapos.org/terms/conditions/33[↩]
- What Is Blepharitis ? American Academy of Ophthalmology. https://www.aao.org/eye-health/diseases/what-is-blepharitis[↩]
- Blepharitis. Medline Plus, U.S. National Library of Medicine. https://medlineplus.gov/ency/article/001619.htm[↩]
- Blepharitis Treatment. American Academy of Ophthalmology. https://www.aao.org/eye-health/diseases/blepharitis-treatment[↩]
- Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol. 2016;10:1385-1396. PMID: 27555745 www.ncbi.nlm.nih.gov/pubmed/27555745[↩]
- Wang L, Bassiri M, Najafi R, et al. Hypochlorous acid as a potential wound care agent: part I. Stabilized hypochlorous acid: a component of the inorganic armamentarium of innate immunity. J Burns Wounds 2007;6:e5.[↩]
- Sindt CW. Wash away your old hygiene strategy. Lens care insights. Rev Cornea Contact Lenses. May 2014.[↩]
- Welling JD, Mauger TF, Schoenfield LR, Hendershot AJ. Chronic eyelid dermatitis secondary to cocamidopropyl betaine allergy in a patient using baby shampoo eyelid scrubs. JAMA Ophthalmol 2014;132:357-9.[↩]
- Crew JR, Varilla R, Rocas TAI, et al. Treatment of acute necrotizing fasciitis using negative pressure wound therapy and adjunctive neutrophase irrigation under the foam. Wounds 2013;25:272-7.[↩]
- Krader CG. Hypochlorous acid lid cleanser provides novel advantages. Ophthal Times 2014.[↩]
- Meibomianitis. Medline Plus, U.S. National Library of Medicine. https://medlineplus.gov/ency/article/001621.htm[↩]
- Foster CS. The eye in skin and mucous membrane disorders. In: Tasman W, Jaeger EA, eds. Duane’s Ophthalmology. 2013 ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:vol 5, chap 27.[↩]
- Lid hygiene product helps reduce blepharitis, MGD symptoms. Ophthalmology Times. http://ophthalmologytimes.modernmedicine.com/ophthalmologytimes/news/lid-hygiene-product-helps-reduce-blepharitis-mgd-symptoms[↩]
- Lane SS, DuBiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea. 2012;31(4):396-404. PMID: 22222996 www.ncbi.nlm.nih.gov/pubmed/22222996[↩]
- Periorbital cellulitis. Medline Plus, U.S. National Library of Medicine. https://medlineplus.gov/ency/article/000976.htm[↩]
- Orbital cellulitis. Medline Plus, U.S. National Library of Medicine. https://medlineplus.gov/ency/article/001012.htm[↩]
- Dacryoadenitis. Medline Plus, U.S. National Library of Medicine. https://medlineplus.gov/ency/article/001625.htm[↩]
- Durand ML. Periocular infections. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 8th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 118.[↩]
- Karesh JW, On AV, Hirschbein MJ. Noninfectious orbital inflammatory disease. In: Tasman W, Jaeger EA, eds. Duane’s Ophthalmology. 2013 ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:vol 2, chap 35.[↩]
- Dacryocystitis. Merck Manual, Merck Sharp & Dohme Corp. http://www.merckmanuals.com/professional/eye-disorders/eyelid-and-lacrimal-disorders/dacryocystitis[↩]
- Dacryocystitis. EyeWiki, American Academy of Ophthalmology. http://eyewiki.aao.org/Dacryocystitis[↩]
- Trachoma. Medline Plus, U.S. National Library of Medicine . https://medlineplus.gov/ency/article/001486.htm[↩]
- Trachoma. EyeWiki, American Academy of Ophthalmology. http://eyewiki.org/Trachoma[↩][↩][↩][↩]
- Thylefors, B. The World Health Organization’s program for the prevention of blindness. Int Ophthalmol. 1990;14:211–212. https://www.ncbi.nlm.nih.gov/pubmed/2188924[↩]
- Lietman, T., Brooks, D., Moncada, J. et al, Chronic follicular conjunctivitis associated with Chlamydia psittaci or Chlamydia pneumoniae. Clin Infect Dis. 1998;26:1335–1340. https://www.ncbi.nlm.nih.gov/pubmed/9636859[↩]
- American Academy of Ophthalmology. Conjunctivitis: What Is Pink Eye ? https://www.aao.org/eye-health/diseases/pink-eye-conjunctivitis[↩]
- American Academy of Ophthalmology. Conjunctivitis: Pink Eye Symptoms. https://www.aao.org/eye-health/diseases/pink-eye-conjunctivitis-symptoms[↩]
- American Academy of Ophthalmology. Conjunctivitis: Pink Eye Treatment. https://www.aao.org/eye-health/diseases/pink-eye-conjunctivitis-treatment[↩][↩][↩][↩]
- American Academy of Ophthalmology. What Is Bacterial Keratitis ? https://www.aao.org/eye-health/diseases/what-is-bacterial-keratitis[↩][↩]
- American Academy of Ophthalmology. What is Fungal Keratitis ? https://www.aao.org/eye-health/diseases/what-is-fungal-keratitis[↩][↩][↩][↩]
- American Academy of Ophthalmology. Fungal Keratitis Causes. https://www.aao.org/eye-health/diseases/fungal-keratitis-cause[↩]
- American Academy of Ophthalmology. Fungal Keratitis Symptoms. https://www.aao.org/eye-health/diseases/fungal-keratitis-symptoms[↩]
- American Academy of Ophthalmology. Fungal Keratitis Treatment. https://www.aao.org/eye-health/diseases/fungal-keratitis-treatment[↩]
- American Academy of Ophthalmology. What is Herpes Keratitis ? https://www.aao.org/eye-health/diseases/herpes-keratitis[↩]
- American Academy of Ophthalmology. Herpes Keratitis Causes. https://www.aao.org/eye-health/diseases/herpes-keratitis-cause[↩][↩]
- American Academy of Ophthalmology. Herpes Keratitis Symptoms. https://www.aao.org/eye-health/diseases/herpes-keratitis-symptoms[↩]
- American Academy of Ophthalmology. Herpes Keratitis Treatment. https://www.aao.org/eye-health/diseases/herpes-keratitis-treatment[↩][↩][↩][↩]
- American Academy of Ophthalmology. What Is Uveitis ? https://www.aao.org/eye-health/diseases/what-is-uveitis[↩][↩]
- American Academy of Ophthalmology. Uveitis Causes. https://www.aao.org/eye-health/diseases/uveitis-causes[↩]
- American Academy of Ophthalmology. Uveitis Symptoms. https://www.aao.org/eye-health/diseases/uveitis-symptoms[↩]
- American Academy of Ophthalmology. Uveitis Diagnosis. https://www.aao.org/eye-health/diseases/uveitis-diagnosis[↩][↩]
- CMV retinitis. Medline Plus, U.S. National Library of Medicine. https://medlineplus.gov/ency/article/000665.htm[↩]
- Contact Lens-Related Eye Infections. American Academy of Ophthalmology. https://www.aao.org/eye-health/diseases/contact-lens-related-eye-infections[↩]
- American Academy of Pediatrics. Prevention of neonatal ophthalmia. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, editors. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012. pp. 880–2.[↩]
- Diagnosis and management of pediatric conjunctivitis. Teoh DL, Reynolds S. Pediatr Emerg Care. 2003 Feb; 19(1):48-55. https://www.ncbi.nlm.nih.gov/pubmed/12592117/[↩][↩][↩][↩]
- Eye Infections in Infants & Children. Healthy Children, American Academy of Pediatrics. https://www.healthychildren.org/English/health-issues/conditions/eyes/Pages/Eye-Infections.aspx[↩]
- Moore DL, MacDonald NE, Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Preventing ophthalmia neonatorum. The Canadian Journal of Infectious Diseases & Medical Microbiology. 2015;26(3):122-125. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4507834/[↩]
- American Academy of Pediatrics . Prevention of neonatal ophthalmia. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, editors. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012. pp. 880–2.[↩][↩]
- Laga M, Plummer FA, Nzanze H, et al. Epidemiology of ophthalmia neonatorum in Kenya. Lancet. 1986;2(8516):1145–9. https://www.ncbi.nlm.nih.gov/pubmed/2877285[↩]
- Davidson HH, Hill JH, Eastman NJ. Penicillin in the prophylaxis of ophthalmia neonatorum. J Am Med Assoc. 1951;145(14):1052–5. https://www.ncbi.nlm.nih.gov/pubmed/14803306[↩]
- Forbes GB, Forbes GM. Silver nitrate and the eye of the newborn. Credé’s contribution to preventive medicine. Am J Dis Child. 1971;121(1):1–3. https://www.ncbi.nlm.nih.gov/pubmed/5543849[↩]
- U.S. Centers for Disease Control and Prevention Sexually transmitted diseases treatment guidelines, 2010. MMWR. 2010;59(RR-12). https://www.cdc.gov/std/treatment/2010/default.htm[↩]
- Recommendations for the prevention of neonatal ophthalmia. Paediatrics & Child Health. 2002;7(7):480-483. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2795679/[↩][↩][↩]
- Teoh DL, Reynolds S. Diagnosis and management of pediatric conjunctivitis. Pediatr Emerg Care. 2003;19(1):48–55. https://www.ncbi.nlm.nih.gov/pubmed/12592117[↩][↩]
- Erythromycin Ointment. Healthy Children, American Academy of Pediatrics. https://www.healthychildren.org/English/ages-stages/prenatal/delivery-beyond/Pages/Erythromycin-Ointment.aspx[↩]
- Pediatric ocular inflammation. Wagner RS, Aquino M. Immunol Allergy Clin North Am. 2008 Feb; 28(1):169-88, vii. https://www.ncbi.nlm.nih.gov/pubmed/18282551/[↩][↩][↩]
- Ophthalmia neonatorum. Chandler JW, Rapoza PA. Int Ophthalmol Clin. 1990 Winter; 30(1):36-8. https://www.ncbi.nlm.nih.gov/pubmed/2404890/[↩]
- Conjunctivitis: systematic approach to diagnosis and therapy. Thanathanee O, O’Brien TP. Curr Infect Dis Rep. 2011 Apr; 13(2):141-8. https://www.ncbi.nlm.nih.gov/pubmed/21365377/[↩]
- Bacterial conjunctivitis in children: antibacterial treatment options in an era of increasing drug resistance. Pichichero ME. Clin Pediatr (Phila). 2011 Jan; 50(1):7-13. https://www.ncbi.nlm.nih.gov/pubmed/20724317/[↩]
- Rours IG, Hammerschlag MR, Ott A, De Faber TJ, Verbrugh HA, de Groot R, et al. Chlamydia trachomatis as a cause of neonatal conjunctivitis in Dutch infants. Pediatrics. 2008;121(2):e321–6. https://www.ncbi.nlm.nih.gov/pubmed/18245405[↩]
- Hammerschlag MR. Chlamydial and gonococcal infections in infants and children. Clin Infect Dis. 2011;53(Suppl 3):S99–102. https://www.ncbi.nlm.nih.gov/pubmed/22080275[↩][↩][↩][↩][↩]
- Di Bartolomeo S, Mirta DH, Janer M, Rodríguez Fermepin MR, Sauka D, Magariños F, et al. Incidence of Chlamydia trachomatis and other potential pathogens in neonatal conjunctivitis. Int J Infect Dis. 2001;5(3):139–43. https://www.ncbi.nlm.nih.gov/pubmed/11724670[↩]
- Darville T. Chlamydia trachomatis infections in neonates and young children. Semin Pediatr Infect Dis. 2005;16(4):235–44. https://www.ncbi.nlm.nih.gov/pubmed/16210104[↩]
- Zuppa AA, D’Andrea V, Catenazzi P, Scorrano A, Romagnoli C. Ophthalmia neonatorum: what kind of prophylaxis? J Matern Fetal Neonatal Med. 2011;42(6):769–73. https://www.ncbi.nlm.nih.gov/pubmed/21534852[↩][↩][↩][↩][↩]
- American Academy of Pediatrics . Chlamydia trachomatis. In: Pickering LK, editor. Red book: 2012. Report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2012. pp. 276–81.[↩][↩][↩]
- Pichichero ME. Bacterial conjunctivitis in children: antibacterial treatment options in an era of increasing drug resistance. Clin Pediatr (Phila) 2011;50(1):7–13. Epub 2010 Aug 19. https://www.ncbi.nlm.nih.gov/pubmed/20724317[↩]
- Hammerschlag MR, Gelling M, Roblin PM, Kutlin A, Jule JE. Treatment of neonatal chlamydial conjunctivitis with azithromycin. Pediatr Infect Dis J. 1998;17(11):1049–50. https://www.ncbi.nlm.nih.gov/pubmed/9849993[↩]
- Laga M, Plummer FA, Nzanze H, Namaara W, Brunham RC, Ndinya-Achola JO, et al. Epidemiology of ophthalmia neonatorum in Kenya. Lancet. 1986;2(8516):1145–9. https://www.ncbi.nlm.nih.gov/pubmed/2877285[↩]
- Woods CR. Gonococcal infections in neonates and young children. Semin Pediatr Infect Dis. 2005;16(4):258–70. https://www.ncbi.nlm.nih.gov/pubmed/16210106[↩][↩][↩]
- Thanathanee O, O’Brien TP. Conjunctivitis: systematic approach to diagnosis and therapy. Curr Infect Dis Rep. 2011;13(2):141–8. https://www.ncbi.nlm.nih.gov/pubmed/21365377[↩][↩][↩][↩]
- Wagner RS, Aquino M. Pediatric ocular inflammation. Immunol Allergy Clin North Am. 2008;28(1):169–88. https://www.ncbi.nlm.nih.gov/pubmed/18282551[↩]





{kind=link}