Contents
- L-Carnitine
- L-Carnitine function
- L-Carnitine sources
- How much carnitine do I need?
- Carnitine Deficiency
- L-Carnitine uses
- Alzheimer’s disease and dementia
- Cardiovascular disease and peripheral artery disease
- Insulin resistance
- Type 2 diabetes mellitus
- Infertility
- Osteoarthritis
- Athletic performance enhancement
- Weight loss
- Chemotherapy-induced peripheral neuropathy
- Diabetic peripheral neuropathy
- Antiretroviral-related peripheral neuropathy
- End-stage renal disease (ESRD)
- Depression
- Hepatic encephalopathy
- Cancer-related fatigue
- Frailty
- Skeletal muscle wasting
- Muscle cramps
- L-Carnitine dose
- L-Carnitine side effects
L-Carnitine
L-Carnitine, is short for Levocarnitine or Carnitor or vitamin BT or beta-hydroxy-gamma-N-trimethylaminobutyric acid, is an enantiomer (a mirror image of three-dimensional shape) of carnitine 1, 2, 3, 4, 5, 6, 7, 8. Since carnitine was discovered in muscle extracts in 1905 by Gulewitsch and Krimberg in Moscow, Russia 9 and by Kutscher in Germany 10, the term carnitine has always been referred to as L-carnitine. At that time Carnitine was named from the Latin word ‘carnis’ which means ‘flesh’ 11. L-Carnitine appeared to act as a vitamin in the yellow mealworm beetle (Tenebrio molitor) and was therefore termed vitamin BT 5. However, vitamin BT is a misnomer because humans can synthesize L-carnitine. In general, Carnitine is the generic term for several compounds, including L-Carnitine, Acetyl-L-carnitine, and Propionyl-L-carnitine 12. In 1927, the chemical structure of carnitine was identified as beta-hydroxy-gamma-trimethyl-amino-butyric acid 13. In 1955, Fritz reported that muscle extracts added by means of rat liver homogenates effected an increase in palmitate oxidation rate 14. In the same year, Friedman and Fraenkel found the reversible transfer of acetyl groups between carnitine and coenzyme A 15. In 1962, Bremer observed that the formed acetyl-carnitine was an effective supplier of acetyl groups for beta-oxidation in the mitochondria 16. Later that year, Bremer 17 was the first researcher who described the main physiological function of carnitine as carrier for the translocation of long-chain fatty acid from cytoplasmic compartment into mitochondria, where beta-oxidation enzymes are located for energy production. The physiological form of carnitine was identified in 1962 as the L (−) isomer, or L-Carnitine 18.
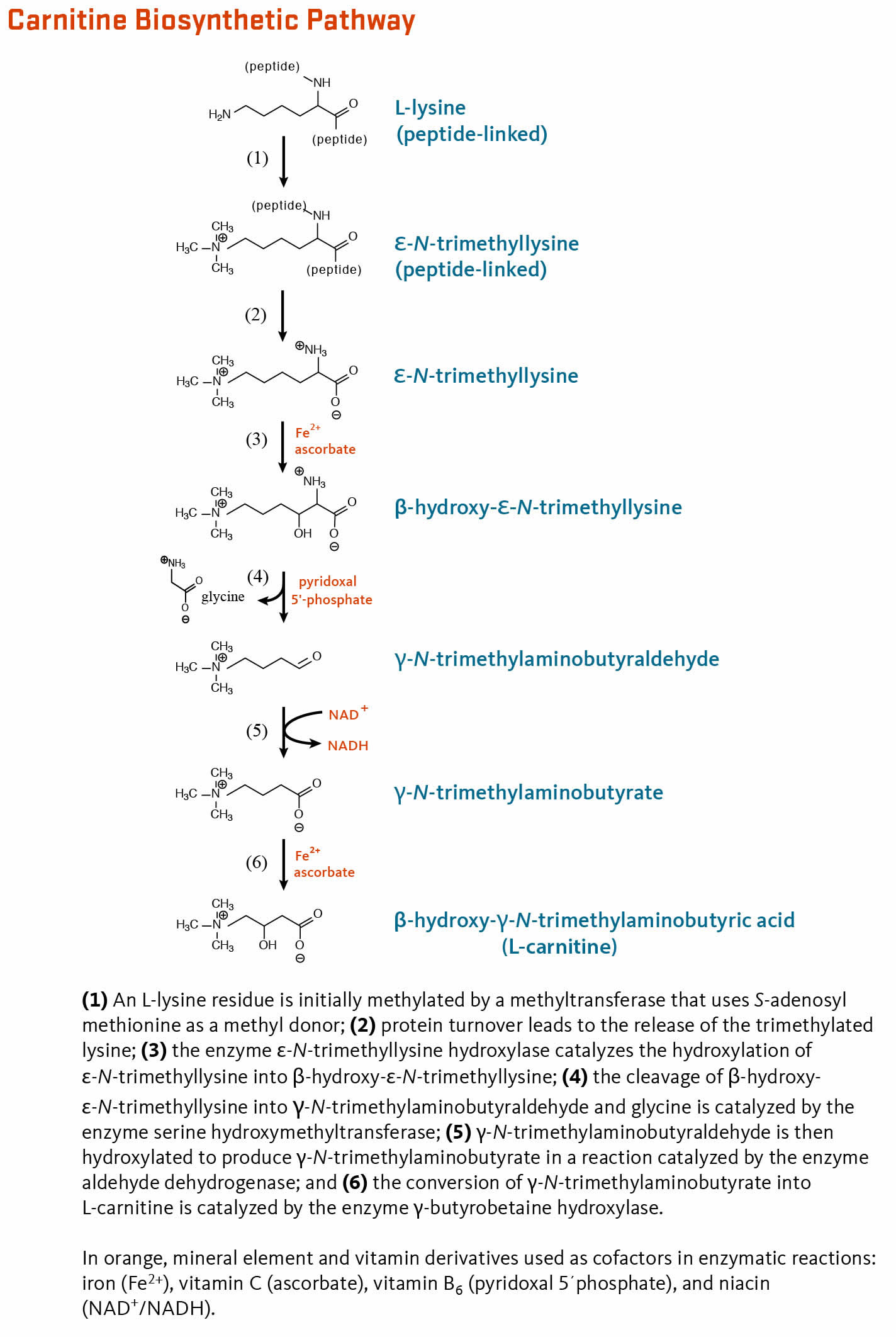
In humans, 25% of the daily L-Carnitine required is produced by your liver, muscle and kidneys from amino acids such as Lysine and Methionine, while the remaining 75% is provided by food intake such as meat, poultry, fish, milk, and some dairy products 19, 20, 21, 22. Four enzymes are involved in endogenous L-carnitine biosynthesis 23. The enzymes are all ubiquitous except for gamma-butyrobetaine hydroxylase which is absent from your heart and skeletal muscle 23. The gamma-butyrobetaine hydroxylase enzyme is highly expressed in your liver, testes, and kidney 24. The rate limiting step in carnitine biosynthesis is the availability of trimethyllysine at the intramitochondrial site of trimethyllysine hydroxylase activity 25.
L-Carnitine is primarily synthesized in your liver and transported via the bloodstream to heart and skeletal muscle, which rely on L-carnitine for fatty acid oxidation yet cannot synthesize it 26. The rate of L-carnitine biosynthesis in humans was studied in strict vegetarians (i.e., in people who consume very little dietary carnitine from meat) and estimated to be 1.2 micromol/kg of body weight/day 27. The rate of L-carnitine synthesis depends on the extent to which peptide-linked lysines are methylated and the rate of protein turnover. There is some indirect evidence to suggest that excess lysine in the diet may increase endogenous L-carnitine synthesis; however, changes in dietary carnitine intake level or in kidney reabsorption do not appear to affect the rate of endogenous L-carnitine synthesis 20.
The normal rate of L-carnitine biosynthesis in humans ranges from 0.16 to 0.48 mg/kg of body weight/day 28. Therefore, a 70 kg (154 1b) person would synthesize between 11 and 34 mg of carnitine per day. This rate of L-carnitine biosynthesis, combined with efficient (95%) L-carnitine reabsorption by your kidneys, is sufficient to prevent L-carnitine deficiency in generally healthy people, including strict vegetarians 29.
The bioavailability of L-carnitine from food can vary depending on dietary composition 23. For example, one study reported that bioavailability of L-carnitine in individuals adapted to low-carnitine diets (i.e., vegetarians) was higher (66%-86%) than in those adapted to high-carnitine diets (i.e., regular red meat eaters; 54%-72%) 30. The remainder is degraded by colonic bacteria.
Under certain conditions (e.g., premature birth or kidney disfunction), the demand for L-carnitine may exceed an individual’s capacity to synthesize it, making it a conditionally essential nutrient 31, 28, 32.
Carnitine plays a critical role in energy production. It is an essential cofactor that helps transport long-chain fatty acids into the mitochondria so that they can be oxidized to produce energy in the form of adenosine triphosphate (ATP) 33, 34. Carnitine also helps transport some toxic compounds out of the mitochondria 34.
Carnitine is concentrated in tissues that oxidize fatty acids as a dietary fuel 12, 35. The vast majority (>99%) of body carnitine is situated in the intracellular compartment. About 95% of total body carnitine is stored in your heart and skeletal muscle. Most of the remainder is stored in your liver and kidney, and circulating plasma contains only about 0.5% of the body’s carnitine 36. Excess plasma carnitine is excreted in urine 37.
The body needs about 15 mg/day of carnitine from a combination of dietary sources and endogenous synthesis 38. Foods of animal origin provide most of the carnitine in American diets. A typical omnivorous diet provides about 24 to 145 mg carnitine daily for a person weighing 165 pounds. In contrast, a vegan diet provides about 1.2 mg carnitine 12. Normal carnitine levels are maintained by balance between dietary intake, endogenous synthesis, and kidney reabsorption. Based on carnitine content in food, bioavailability of dietary carnitine is about 54–86% 39. In the kidney the majority of carnitine (90–99% of filtered load) is reabsorbed until saturation is reached. The renal threshold for carnitine excretion is around 50 micromol/L. The kidneys are very efficient in maintaining normal levels of plasma carnitine by modulating urinary carnitine excretion according to the intake from diet 39.
Healthy children and adults do not need to consume carnitine from food or supplements because the liver and kidneys synthesize sufficient amounts to meet daily needs 40, 41. In 1989, the Food and Nutrition Board (FNB) of the National Academies of Sciences, Engineering, and Medicine concluded that carnitine is not an essential nutrient 42. Therefore, the Food and Nutrition Board (FNB) did not establish Dietary Reference Intakes (DRIs) for carnitine 43.
Endogenous carnitine synthesis does not appear to be affected by dietary carnitine intake or carnitine excretion and is sufficient to meet the carnitine needs of healthy people 12. A person weighing 165 lb who follows a strict vegetarian diet, for example, synthesizes approximately 14.4 mg/day carnitine 12.
Carnitine status is not routinely assessed in clinical practice, but it can be determined by measuring circulating carnitine. The vast majority (>99%) of body carnitine is situated in the intracellular compartment. Circulating carnitine represents only about 0.5% of body carnitine 36. Therefore, normal plasma free carnitine levels are low, ranging between 25–50 micromol/L 44. Normal carnitine levels are variable based on age and gender. In one study of 80 healthy volunteers, mean serum-free carnitine levels in males were 41 micromol/L (range 26.4–53.4) whereas in females the mean was 39 micromol/L (range 19.2–44.5) 45. The same study showed a positive correlation between carnitine levels (free and total) with age, although in males the correlation didn’t reach statistical significance 45.
A plasma free carnitine concentration of 20 micromol/L or less, or a total carnitine concentration of 30 micromol/L or less, is abnormally low 12. The ratio of acyl-L-carnitine ester to free L-carnitine can also be used to assess carnitine status because under normal conditions most carnitine is in the free unesterified form. A ratio of 0.4 or greater in plasma or serum indicates abnormal carnitine metabolism and suggests carnitine insufficiency 12, 46, 47.
Figure 1. L-carnitine chemical structure
Figure 2. Acetyl-L-carnitine and propionyl-L-carnitine chemical structure

Figure 3. L-carnitine biosynthetic pathway
L-Carnitine function
L-Carnitine is formed in your liver from the hydroxylation of gamma butyrobetaine, which is synthesized in your kidneys from lysine and methionine and then transported to other tissues. The activity of gamma butyrobetaine is age dependent, being much lower in newborns than in older children and adults 49. Carnitine plays a critical role in energy production. L-Carnitine is most concentrated in tissues that use fatty acids as their primary fuel, such as skeletal and heart muscle. Carnitine functions to carry long-chain fatty acids obtained from your diet to the energy-producing centers in your muscle cells called the mitochondria, so that they can be oxidized to produce energy in the form of adenosine triphosphate (ATP) 34, 20. Cells need carnitine to bring certain types of fats (fatty acids) into mitochondria, which are within cells. Fatty acids are a major source of energy for your heart and muscles. During periods of fasting, fatty acids become the most important energy source for the heart and other muscles. A deficiency of carnitine results in accumulation of fats in the liver, muscle, and heart.
L-Carnitine is required for mitochondrial beta-oxidation of long-chain fatty acids for energy production in the form of adenosine triphosphate (ATP) 1. Long-chain fatty acids must be esterified to L-carnitine in order to enter the mitochondrial matrix where beta-oxidation occurs (Figure 4 & 5). On the outer mitochondrial membrane, carnitine palmitoyltransferase 1 (CPT1) catalyzes the transfer of medium or long-chain fatty acids esterified to coenzyme A (CoA) to L-carnitine. This reaction is a rate-controlling step for the beta-oxidation of fatty acid 50. A transport protein called carnitine-acylcarnitine translocase (CACT) facilitates the transport of L-carnitine (acylcarnitine) and carnitine-fatty acid complexes across the inner mitochondrial membrane. Carnitine-acylcarnitine translocase (CACT) is part of the carnitine shuttle system, which is essential for moving fats into the mitochondria to produce energy. On the inner mitochondrial membrane, carnitine palmitoyltransferase 2 (CPT-2) catalyzes the transfer of fatty acids from L-carnitine to free coenzyme A (CoA). Fatty acyl-coenzyme A (CoA) is then metabolized through beta-oxidation in the mitochondrial matrix, ultimately yielding propionyl-CoA and acetyl-CoA 20. Carnitine is eventually recycled back to the cytosol (Figure 4 & 5).
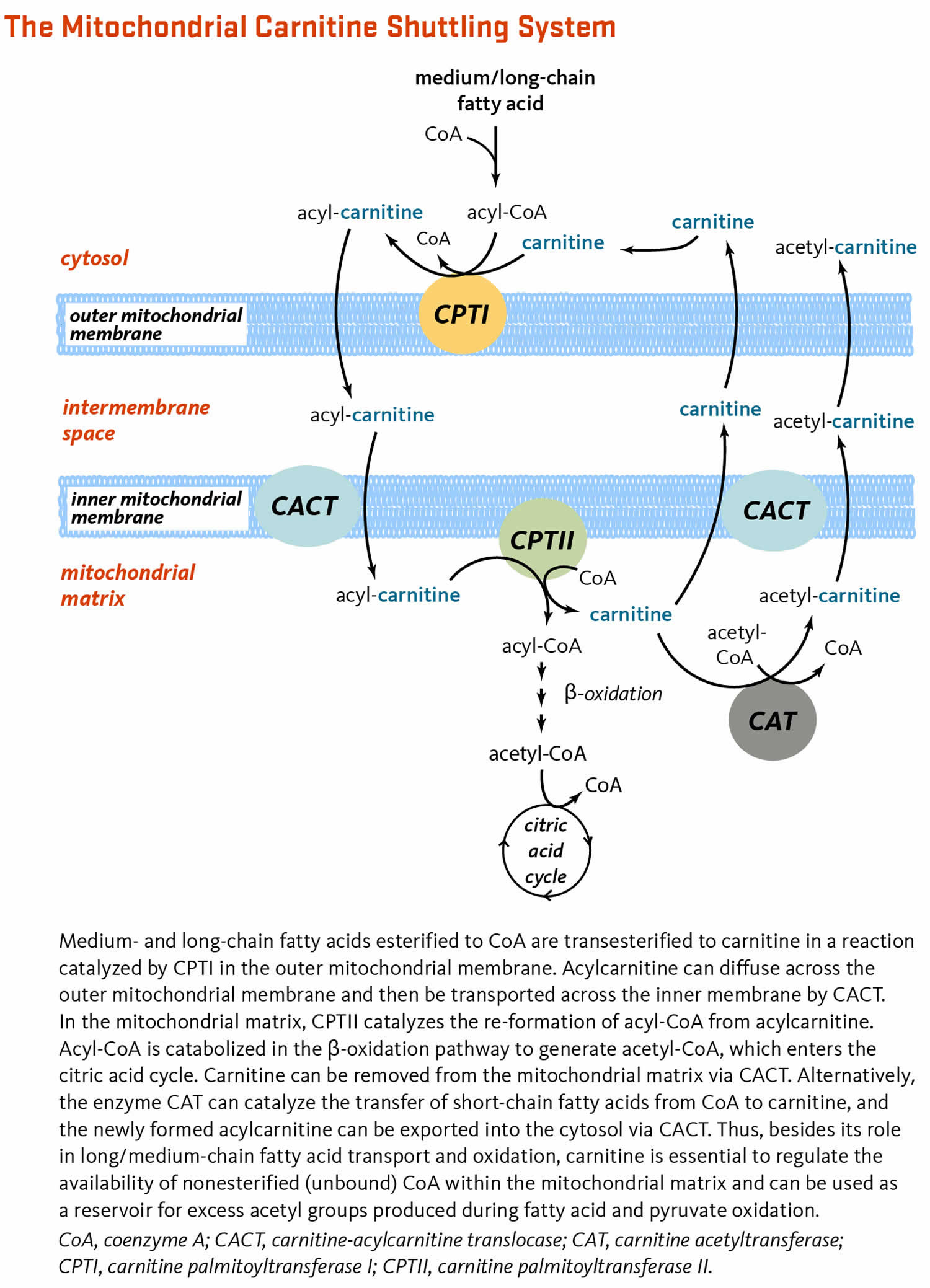
Free nonesterified coenzyme A (CoA) is required as a cofactor for numerous cellular reactions. The flux through pathways that require nonesterified coenzyme A (CoA), such as the oxidation of glucose, may be reduced if all the coenzyme A (CoA) available in a given cell compartment is esterified. Carnitine can increase the availability of nonesterified coenzyme A (CoA) for these other metabolic pathways 1. Within the mitochondrial matrix, carnitine acetyl transferase (CAT) catalyzes the transesterification of short- and medium-chain fatty acids from coenzyme A (CoA) to carnitine (Figure 4 & 5). The resulting acylcarnitine esters (e.g., acetylcarnitine) can remain in the mitochondrial matrix or be exported back into the cytosol via carnitine-acylcarnitine translocase (CACT). Free nonesterified coenzyme A (CoA) can then participate in other reactions, such as the generation of acetyl-CoA from pyruvate in a reaction catalyzed by pyruvate dehydrogenase 51. Acetyl-CoA can then be oxidized to produce energy (ATP) in the citric acid cycle.
In addition to its importance for energy production, L-carnitine was shown to display direct antioxidant properties in test tube study 52. Carnitine also helps transport some toxic compounds out of the mitochondria 34.
Age-related declines in mitochondrial function and increases in mitochondrial oxidant production are thought to be important contributors to the adverse effects of aging 23. Tissue L-carnitine concentrations have been found to decline with age in humans and animals 53. The expression of most proteins involved in the transport of carnitine (organic cation transporter novel 2 [OCTN2]) and the acylcarnitine shuttling system across the mitochondrial membrane (CPT1a, CPT2, and CAT) was also found to be much lower in the white blood cells of healthy older adults than of younger adults 54.
Preclinical studies in rats showed that supplementation with high doses of acetyl-L-carnitine (ALCAR) reversed a number of age-related changes in liver mitochondrial function yet increased liver mitochondrial oxidant production 55. Acetyl-L-carnitine (ALCAR) supplementation in rats has also been found to improve or reverse age-related mitochondrial declines in skeletal and heart muscular function 56, 57. Co-supplementation of aged rats with L-carnitine and alpha-lipoic acid blunted age-related increases in reactive oxygen species (ROS), lipid peroxidation, protein carbonylation, and DNA strand breaks in a variety of tissues (heart, skeletal muscle, and brain) 58, 59, 60, 61, 62, 63, 64, 65, 66, 67. Co-supplementation for three months improved both the number of total and intact mitochondria and mitochondrial ultrastructure of neurons in the hippocampus 59. Although acetyl-L-carnitine (ALCAR) exerts antioxidant activities in rats, it is not known whether taking high doses of acetyl-L-carnitine (ALCAR) will have similar effects in humans 23.
Figure 4. L-Carnitine function
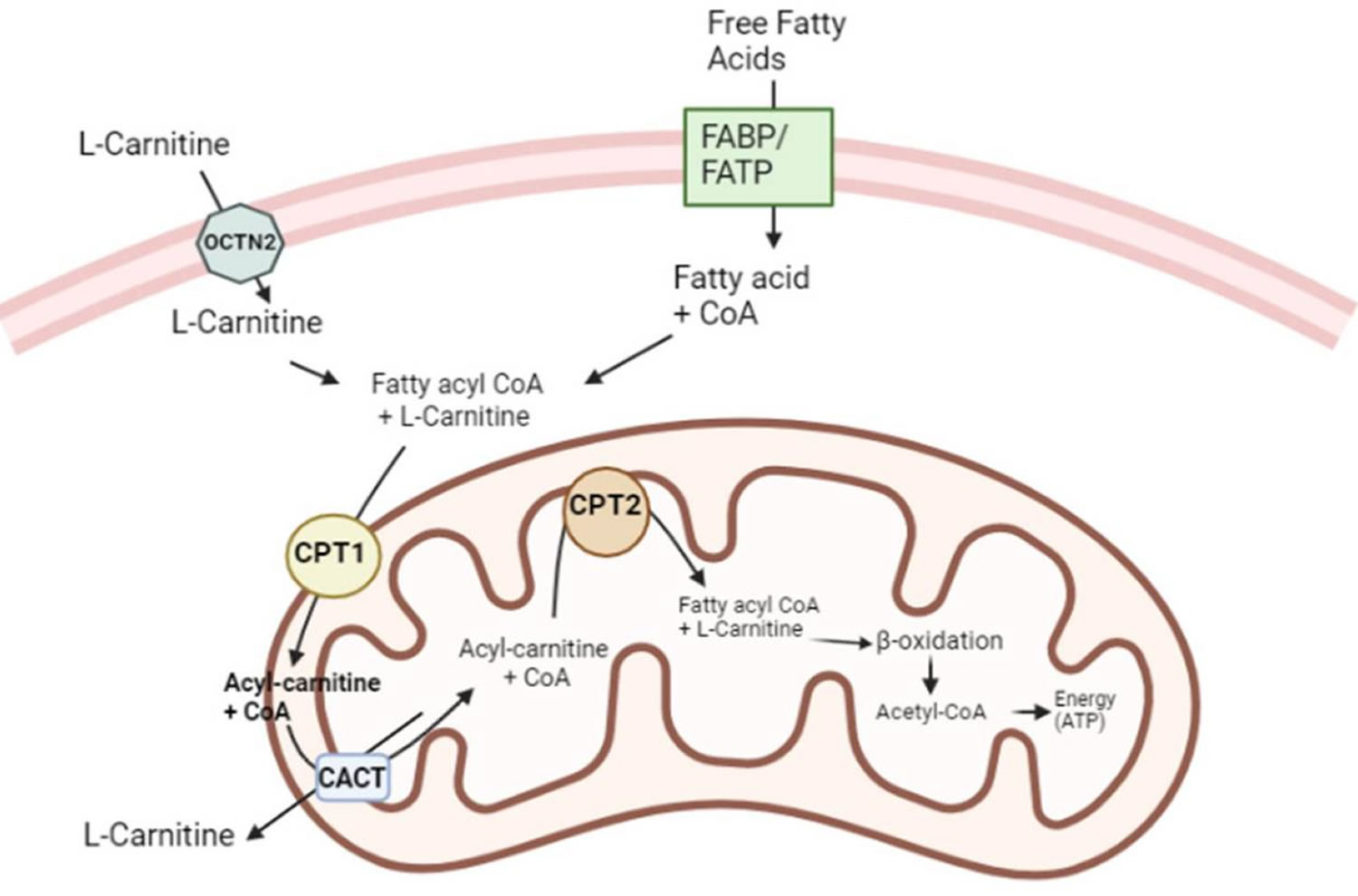
Footnotes: L-Carnitine functions as a cofactor for long-chain fatty acids across the inner mitochondrial membrane. Fatty acids rely on a set of proteins, including transport proteins, to enter the cell. Once inside, long-chain fatty acids bind to coenzyme A (CoA) to form acyl-CoA. However, the impermeability of the mitochondrial membrane to acyl-CoA requires the involvement of L-Carnitine as a shuttle for the transport of fatty acids into the mitochondria. Organic cation transporter novel 2 (OCTN2) facilitates the transport of L-Carnitine into the cell. Subsequently, carnitine palmitoyltransferase 1 (CPT I) enables the transfer of the acyl group from acyl-CoA to carnitine, forming acyl-carnitine. Carnitine-acylcarnitine translocase (CACT) then translocates acyl-carnitine across the inner mitochondrial membrane. Once inside the mitochondria, carnitine palmitoyltransferase 2 (CPT II) cleaves acyl-carnitine, releasing the acyl group, which subsequently binds to coenzyme A (CoA), initiating beta-oxidation. Upon completion of this process, carnitine is transported back to the cytoplasm through the carnitine-acylcarnitine translocase (CACT), allowing for its reuse in subsequent cycles. This intricate transport mechanism involving L-Carnitine is essential for the efficient utilization of fatty acids as an energy source within the mitochondria. It ensures the proper delivery of fatty acids to the site of beta-oxidation, facilitating their effective metabolism and energy production.
[Source 21 ]Figure 5. Mitochondrial carnitine shuttling system
L-Carnitine sources
L-Carnitine is naturally present in many foods especially foods of animal origin especially red meat and is available as a dietary supplement 12. Carnitine is also synthesized in your liver, kidneys, muscle and brain from the amino acids lysine and methionine 68, 31.
Many foods, especially animal foods, naturally contain L-carnitine. These include the following 12, 48, 69:
- Red meat is a good source of carnitine.
- Poultry, fish, and dairy have some carnitine.
- Vegetables, fruits, and grains have very small amounts of carnitine.
Meat, poultry, fish, and dairy products are the richest sources of L-carnitine, while fruit, vegetables, and grains contain relatively little L-carnitine 70. Omnivorous diets have been found to provide 23 to 135 mg/day of L-carnitine for an average 70 kg person, while strict vegetarian diets may provide as little as 1 mg/day for a 70 kg person 26. Between 54% and 86% of L-carnitine from food is absorbed, compared to 5%-25% from oral supplements (0.6-7 g/day) 50, 12. The bioavailability of acetyl-L-carnitine (ALCAR) has not been well studied 71. Non-milk-based infant formulas (e.g., soy formulas) should be fortified so that they contain 11 mg/L of L-carnitine.
Table 1 lists several foods and their approximate carnitine content in milligrams (mg) per serving, based on several small studies.
Data on the carnitine content of specific foods are limited. The U.S. Department of Agriculture’s (USDA’s) FoodData Central does not include the carnitine content of foods.
Table 1. L-Carnitine food sources
| Food | Milligrams (mg) per serving |
|---|---|
| Beef steak, cooked, 3 ounces | 42–122 |
| Ground beef, cooked, 3 ounces | 65–74 |
| Milk, whole, 1 cup | 8 |
| Codfish, cooked, 3 ounces | 3–5 |
| Chicken breast, cooked, 3 ounces | 2–4 |
| Ice cream, ½ cup | 3 |
| Cheese, cheddar, 2 ounces | 2 |
| Whole-wheat bread, 2 slices | 0.2 |
| Asparagus, cooked, ½ cup | 0.1 |
L-carnitine supplements
Carnitine is available in dietary supplements containing only carnitine or a combination of carnitine and other ingredients 70.
Carnitine is available as a supplement in a variety of forms, such as:
- L-carnitine: the most widely available and least expensive.
- Acetyl-L-carnitine (ALCAR): Often used in studies for Alzheimer disease and other brain disorders.
- Propionyl-L-carnitine: Often used in studies for heart disease and peripheral vascular disease.
Avoid D-carnitine supplements. They interfere with the natural form of L-carnitine and and is toxic 48.
In some cases, L-carnitine may be taken by prescription or given intravenously by a health care provider. L-Carnitine is also a drug that is used to treat people with primary carnitine deficiency or systemic primary carnitine deficiency, which is a rare inherited metabolic disorder in which their body does not make enough carnitine and cannot properly process fats into energy particularly during periods without food (fasting) 72, 73. L-Carnitine is also being studied as a way to prevent tissue damage caused by chemotherapy 11.
While bioavailability of L-carnitine from the diet is quite high, absorption from oral L-carnitine supplements is considerably lower 12. Absorption of supplemental L-carnitine is about 14% to 18%, much less than that of dietary L-carnitine 12. The bioavailability of L-carnitine from oral supplements (doses, 0.6 to 7 g) ranges between 5% and 25% of the total dose 74. Less is known regarding the metabolism of the acetylated form of L-carnitine, acetyl-L-carnitine (ALCAR); however, the bioavailability of acetyl-L-carnitine (ALCAR) is thought to be higher than that of L-carnitine. The results of test tube experiments suggested that acetyl-L-carnitine (ALCAR) might be partially hydrolyzed upon intestinal absorption 75. In humans, administration of 2 g/day of acetyl-L-carnitine (ALCAR) for 50 days increased plasma acetyl-L-carnitine (ALCAR) concentrations by 43%, suggesting that either acetyl-L-carnitine (ALCAR) was absorbed without prior hydrolysis or that L-carnitine was re-acetylated in the intestinal absorptive cells (enterocytes) 74.
Intravenous L-carnitine
Intravenous L-carnitine is available by prescription only for the treatment of primary and secondary L-carnitine deficiencies.
Oral L-carnitine
Oral L-carnitine is available by prescription for the treatment of primary and secondary L-carnitine deficiencies. It is also available without a prescription as a nutritional supplement; supplemental doses usually range from 0.5 to 2 g/day.
Acetyl-L-carnitine (ALCAR)
Acetyl-L-carnitine (ALCAR) is available without a prescription as a nutritional supplement. In addition to providing L-carnitine, it provides acetyl groups that may be used in the formation of the neurotransmitter, acetylcholine (ACh). Supplemental doses usually range from 0.5 to 2 g/day 76.
Propionyl-L-carnitine
Propionyl-L-carnitine is not approved by the U.S. Food and Drug Administration (FDA) for use as a drug to prevent or treat any condition. It is, however, available without prescription as a nutritional supplement.
How much carnitine do I need?
The body needs about 15 mg/day of carnitine from a combination of dietary sources and endogenous synthesis 38. Foods of animal origin provide most of the carnitine in American diets. A typical omnivorous diet provides about 24 to 145 mg carnitine daily for a person weighing 165 pounds. In contrast, a vegan diet provides about 1.2 mg carnitine 12.
Endogenous carnitine synthesis does not appear to be affected by dietary carnitine intake or carnitine excretion and is sufficient to meet the carnitine needs of healthy people 12. A person weighing 165 lb who follows a strict vegetarian diet, for example, synthesizes approximately 14.4 mg/day carnitine 12.
Healthy children and adults do not need to consume carnitine from food or supplements because the liver and kidneys synthesize sufficient amounts to meet daily needs 40, 41. In 1989, the Food and Nutrition Board (FNB) of the National Academies of Sciences, Engineering, and Medicine concluded that carnitine is not an essential nutrient 42. Therefore, the Food and Nutrition Board (FNB) did not establish Dietary Reference Intakes (DRIs) for carnitine 43.
Carnitine Deficiency
Nutritional carnitine deficiencies have not been identified in healthy people without metabolic disorders, suggesting that most people can synthesize enough L-carnitine 1. Even strict vegetarians or vegans show no signs of carnitine deficiency despite the fact that most dietary carnitine is derived from animal sources 27. Infants, particularly premature infants, are born with low stores of L-carnitine, which could put them at risk of carnitine deficiency given their rapid rate of growth. One study reported that infants fed carnitine-free, soy-based formulas grew normally and showed no signs of a clinically relevant carnitine deficiency; however, some biochemical measures related to lipid metabolism differed significantly from infants fed the same formula supplemented with L-carnitine 77. Soy-based infant formulas are now fortified with the amount of L-carnitine normally found in human milk 78.
Two types of carnitine deficiency states exist: primary carnitine deficiency and secondary carnitine deficiency. Low carnitine status is generally due to impaired mitochondrial energy metabolism or to carnitine not being efficiently reabsorbed by the kidneys. At present, there is no test that assesses functional carnitine deficiency in humans 20. Regardless of the cause, plasma concentrations of free carnitine ≤20 µmol/L and increased acylcarnitine/free carnitine ratios (≥0.4) are considered abnormal 20.
Primary and secondary carnitine deficiency can be treated with high doses (20–200 mg/kg/day) of L-carnitine supplements 35, 79, 80, 81.
Primary carnitine deficiency
Primary carnitine deficiency also called systemic primary carnitine deficiency (CDSP) is a genetic disorder of the cellular carnitine transporter system that causes a shortage of carnitine within cells 73, 72. Primary carnitine deficiency is caused by mutations in the SLC22A5 gene 73, 72. The SLC22A5 gene provides instructions for making a protein called OCTN2 (organic cation transporter novel 2) that transports carnitine into cells. Cells need carnitine to bring certain types of fats (fatty acids) into mitochondria, which are the energy-producing centers within cells. Fatty acids are a major source of energy for the heart and muscles. During periods of fasting, fatty acids become the most important energy source for the heart and other muscles.
Mutations in the SLC22A5 gene result in an absent or dysfunctional OCTN2 (organic cation transporter novel 2) protein. As a result, there is a shortage (deficiency) of carnitine within cells. Without carnitine, fatty acids cannot enter mitochondria and be used to make energy. Reduced energy production can lead to some of the features of primary carnitine deficiency, such as muscle weakness and hypoglycemia. Fatty acids can also build up in cells and damage the liver, heart, and muscles. This abnormal buildup causes the other signs and symptoms of primary carnitine deficiency.
Primary carnitine deficiency occurs in approximately 1 in 100,000 newborns worldwide 73. Based on newborn screening and reports in medical literature, the prevalence of primary carnitine deficiency in the US is estimated to be 1 in every 50,000 newborns 72. In Japan, primary carnitine deficiency affects 1 in every 40,000 newborns 73.
Primary carnitine deficiency is inherited as an autosomal recessive genetic trait. Recessive genetic disorders occur when an individual inherits two copies of an abnormal gene for the same trait, one from each parent. If an individual inherits one normal gene and one gene for the disease, the person will be a carrier for the disease but will not show symptoms. The risk for two carrier parents to both pass the altered gene and have an affected child is 25% with each pregnancy. The risk to have a child who is a carrier like the parents is 50% with each pregnancy. The chance for a child to receive normal genes from both parents is 25%. The risk is the same for males and females. Parents who are close relatives (consanguineous) have a higher chance than unrelated parents to both carry the same abnormal gene, which increases the risk to have children with a recessive genetic disorder.
Primary carnitine deficiency signs and symptoms typically appear during infancy or early childhood. Primary carnitine deficiency can result in epilepsy and severe brain dysfunction (encephalopathy) in infants; seizures, irregular heartbeat, and breathing problems in adolescents and young adults; and muscle weakness (myopathy), rhabdomyolysis, a weakened and enlarged heart (cardiomyopathy), vomiting, and low blood glucose (hypoglycemia) or sudden death in older people. The severity of this condition varies among affected individuals. Some people with primary carnitine deficiency do not have symptoms (asymptomatic), however, all affected individuals have an increased risk of heart failure, liver disorders, and coma and are at risk for sudden death 73, 72.
Problems related to primary carnitine deficiency can be triggered by periods of fasting or by illnesses such as viral infections. Primary carnitine deficiency is sometimes mistaken for Reye syndrome, a severe disorder that may develop in children who appear to be recovering from viral infections such as chickenpox or flu.
Plasma carnitine levels are extremely reduced in people primary carnitine deficiency. The diagnosis can be confirmed with molecular genetic testing to identify mutations in the SLC22A5 gene. Newborn screening is available to detect low carnitine levels in infants with primary carnitine deficiency.
The main treatment for primary carnitine deficiency is oral L-carnitine 100 to 200 mg/kg daily dose in 3 divided doses, which is very effective if started before organ damage occurs 36, 82, 83. L-carnitine is a fairly safe medication, and few side effects associated with high doses include diarrhea and intestinal discomfort. Additionally, bacterial degradation of unabsorbed oral L-carnitine in the bowel results in trimethylamine, which has a peculiar fishy odor 36, 80. These side effects can be minimized by decrease the L-carnitine dose or treatment with a 7 to 10-day course of oral metronidazole, which could eradicate the intestinal bacterial overgrowth 84.
Maintenance therapy with L-carnitine can improve plasma carnitine levels, and the dose is titrated based on the carnitine plasma levels and also on the response 36. Continued L-carnitine administration prevents hypoglycemic (low blood sugar) episodes as well as cause improvement in myopathic symptoms. The muscle carnitine levels rise slightly (only up to 5% to 10% of controls), due to the abnormal OCTN2 which is unable to increase the uptake of carnitine into the myocyte adequately 85, 86. Carnitine enters mostly by passive diffusion from plasma and via low-affinity transporters, and this modest increase is enough to prevent muscle complications 86.
Acute hypoglycemic (low blood sugar) episodes associated with carnitine deficiency are treated with intravenous 10% dextrose infusion or proper feeding and diet 86, 84, 87 Maintaining normal carnitine levels through supplementation and preventing hypoglycemia (low blood sugar) through frequent feeding and diet can prevent the metabolic, liver, heart, and muscular complications of primary carnitine deficiency 86, 84.
Weakened and enlarged heart (cardiomyopathy), if present, should be managed and treated by a cardiologist.
Secondary carnitine deficiency
Secondary carnitine deficiency may result from either genetic or acquired conditions such as chronic kidney failure (chronic kidney disease) that reduce endogenous carnitine synthesis or increase its excretion or from chronic use of pivalate-containing medications that reduce carnitine absorption or increase its excretion 40, 88.
The following individuals are among those most likely to have inadequate carnitine status and secondary carnitine deficiency.
- Premature infants. Babies born prematurely have high growth demands but have low carnitine stores and an inadequate ability to synthesize carnitine 89, 36. Premature infants may require supplemental carnitine in addition to that supplied in breast milk and fortified infant formula 12. Many enteral and parenteral formulas for premature infants are fortified with L-carnitine to improve lipid metabolism and promote weight gain 12. However, a Cochrane Review of six randomized clinical trials in newborns requiring parenteral nutrition (many of whom were premature) did not support the use of parenteral carnitine to improve lipid utilization or weight gain 90.
- Individuals with secondary carnitine deficiency due to end-stage kidney disease, hemodialysis, or both. Carnitine homeostasis in individuals with kidney diseases can be impaired by reduced synthesis and increased elimination of carnitine by the kidneys. Kidney diseases can also reduce carnitine intake from food because patients often have poor appetite and consume fewer animal products 91. Many patients with end-stage kidney disease, particularly those on hemodialysis, become carnitine insufficient. Low levels of carnitine in blood and muscle stores can contribute to anemia, muscle weakness, fatigue, altered levels of blood fats, and heart disorders. Numerous studies suggest that high doses of supplemental carnitine (often injected) administered to patients on maintenance hemodialysis can correct some or all of these symptoms 92. However, most of these studies had small numbers of participants and were not double-blind clinical trials. The authors of a meta-analysis of these studies concluded that carnitine supplements might help patients manage their anemia but not their blood-lipid profiles, and that the effects of these supplements on exercise capacity and heart disorders were inconclusive 92.
- Genetic defects in the metabolism of amino acids, cholesterol, and fatty acids, such as propionyl-CoA carboxylase deficiency (propionic acidemia) and medium chain acyl-CoA dehydrogenase deficiency 93. Such inherited disorders lead to a buildup of organic acids, which are subsequently removed from the body via urinary excretion of acylcarnitine esters. Increased urinary losses of carnitine can lead to the systemic depletion of carnitine 20.
- A number of inherited mutations in genes involved in carnitine shuttling and fatty acid oxidation pathways do not systematically result in carnitine depletion such that carnitine supplementation may not help mitigate the symptoms but lead to abnormal profiles of acylcarnitine esters in blood 94, 95.
Signs and symptoms of secondary carnitine deficiency include hyperammonemic encephalopathy (malaise, seizures, and decreased consciousness caused by elevated ammonia levels), hypoglycemia, hypoketonemia (low level of ketones in the blood), dicarboxylic aciduria (increased concentrations of dicarboxylic acids in the urine), hyperuricemia (excess uric acid in the blood), muscle weakness, myoglobinuria (excess myoglobin in the urine), cardiomyopathy, and sudden death 91.
Secondary carnitine deficiency can be resolved with high doses (20–200 mg/kg/day) of supplemental carnitine 35, 79, 80, 81.
L-Carnitine uses
The role of supplemental L-carnitine is being investigated for the treatment of Alzheimer’s disease and dementia, cardiovascular disease and peripheral artery disease, insulin resistance and diabetes, infertility, osteoarthritis, athletic performance enhancement, and weight loss. It is important to note that treatment with L-carnitine or acyl-L-carnitine esters (i.e., acetyl-L-carnitine [ALCAR], propionyl-L-carnitine) was generally used as an add-on to standard medical therapy, not in place of it 23. It is also important to consider the fact that the bioavailability of L-carnitine and acylcarnitine derivatives administered orally is low (~10-20%) 23. Intravenous (IV) administration is more likely to increase plasma carnitine concentration, yet homeostatic mechanisms tightly control blood concentration through metabolism and kidney excretion. Up to 90% of 2 g of L-carnitine administered intravenously is excreted into the urine within 12 to 24 hours. Only a fraction of the L-carnitine dose is thought to enter the endogenous carnitine pool — largely found in skeletal muscle 26.
L-carnitine is also added in energy drinks, pre-workout supplements, and a large proportion of other products found at health food stores 96, 97.
Alzheimer’s disease and dementia
Alzheimer’s disease is characterized by the accumulation of plaques and the degeneration of neurons in the brain, including cholinergic neurons involved in memory functions 98. Cholinergic neurons use the neurotransmitter acetylcholine (ACh) 98. Acetylcholine (ACh) is an important neurotransmitter that plays a role in brain functions, such as memory, and body functions, such as muscle contractions to move your muscles. Low levels of acetylcholine are associated with memory issues and muscle disorders. Alzheimer’s disease is often treated by increasing acetylcholine (ACh) levels or preventing its breakdown 99.
Carnitine might be conditionally essential in individuals with Alzheimer’s disease because it may support acetylcholine synthesis and help remove toxic compounds to alleviate mitochondrial dysfunction associated with extensive degeneration of brain structures 31. Therefore, researchers have examined whether acetyl-L-carnitine (ALCAR) supplements benefit individuals with Alzheimer’s disease or other forms of dementia, but studies have had mixed results 31, 100.
In a 2003 meta-analysis of 21 clinical trials, a total of 1,204 adults with mild cognitive impairment or mild Alzheimer’s disease took supplements containing 1.5 to 3.0 g/day acetyl-L-carnitine (ALCAR) or placebo for 3 to 12 months 101. Clinical and psychometric assessment scores were better, and improvements determined by clinicians were greater in supplement users than in the placebo groups 101.
In contrast, a 2003 Cochrane Review of 15 clinical trials (including 13 of those in the meta-analysis described above) had somewhat different findings 100. The clinical trials assessed the effectiveness of 1 to 3 g/day acetyl-L-carnitine (ALCAR) supplementation or placebo over 12 to 52 weeks in participants with mild to moderate dementia or cognitive decline 100. The results showed that acetyl-L-carnitine (ALCAR) supplementation decreased symptom severity at 12 and 24 weeks but not at 52 weeks. Similarly, acetyl-L-carnitine (ALCAR) supplements improved scores on the Mini Mental State Examination at 24 weeks but not at 12 or 52 weeks and had no effect on the severity of dementia, functional ability, or overall clinical global impression scores 100. The authors of the Cochrane Review noted that results from studies conducted more recently were less positive than those from earlier studies; they concluded that the routine clinical use of acetyl-L-carnitine supplements to treat the signs and symptoms of dementia was not justified 100.
The effects of acetyl-L-carnitine (ALCAR) supplements in Alzheimer’s disease and other forms of dementia remain unclear and continue to be an area of active research 102, 103, 31.
Cardiovascular disease and peripheral artery disease
Carnitine plays a role in transporting long-chain fatty acids in the heart (myocardial) mitochondria, where they are metabolized via oxidation for energy. It is also involved in moderating oxidative stress 104, 105 and might decrease markers of inflammation 106. During ischemic events, carnitine prevents fatty acid ester accumulation, which can lead to fatal ventricular arrhythmias 104. For these reasons, researchers are examining whether carnitine affects cardiovascular health.
Clinical trials examining the effects of carnitine supplements on cardiovascular disease have had mixed results. A meta-analysis of 13 clinical trials included a total of 3,629 adults with acute myocardial infarction who took either L-carnitine (from 2.7 g/day for 5 days to 6 g/day for 12 months) or placebo. The study found that L-carnitine significantly reduced rates of all-cause mortality, ventricular arrhythmias, and new-onset angina but did not affect risk of heart failure or myocardial reinfarction 104, 107. The carnitine dose and duration of the clinical trial did not appear to affect outcomes.
Another meta-analysis of 17 clinical trials that included a total of 1,625 adults with chronic heart failure found that 1 g/day to 6 g/day for 7 days to 3 years L-carnitine supplements improved left ventricular ejection fraction by 4.14%, stroke volume by 8.21 mL, and cardiac output by 0.88 L/min compared to routine/conventional treatment 108. These benefits did not vary by supplement dose or study duration. However, L-carnitine did not affect rates of all-cause mortality or performance on a timed walking test 108.
Other research has raised concerns about the negative cardiovascular effects of chronic exposure to carnitine. A 2013 study that included 2,595 adults age 54–71 years undergoing elective heart evaluation found that L-carnitine is metabolized by intestinal microbiota to trimethylamine-N-oxide (TMAO), a proatherogenic substance that is associated with increased cardiovascular disease risk 109. Because of differences in intestinal bacteria composition, omnivorous study participants produced more trimethylamine-N-oxide (TMAO) than vegans or vegetarians after consumption of L-carnitine. The study also found dose-dependent associations between fasting plasma L-carnitine concentrations and risk of coronary artery disease, peripheral artery disease, and cardiovascular disease, but only in participants with concurrently high trimethylamine-N-oxide (TMAO) levels 109.
A 2022 clinical trial also found potentially deleterious outcomes in 157 individuals age 58 to 75 years with metabolic syndrome who received 1 g supplemental L-carnitine or placebo twice a day for 6 months 110. Although the results showed no differences in total plaque volume between groups, total cholesterol and low-density lipoprotein cholesterol levels were higher in participants taking L-carnitine 110. L-carnitine supplementation was also associated with 9.3% greater carotid arterial plaque stenosis in males who ate less red meat and had lower baseline stenosis and total plaque volume than other participants 110.
Peripheral artery disease is a blood vessel disorder usually caused by atherosclerosis and its resulting arterial stenosis and occlusion. Peripheral artery disease is common among older adults, although it is often underdiagnosed 111, 112. Researchers have examined whether propionyl-L-carnitine, an acyl derivative of L-carnitine, mitigates the cramping leg pain of intermittent claudication, the main symptom of peripheral artery disease, but findings from studies have been mixed. A systematic review of three randomized clinical trials compared 234 participants who took 2 g/day oral propionyl-L-carnitine for 4 to 6 months with 222 patients who took placebo 113. In one trial, participants supplemented with propionyl-L-carnitine had improved peak walking times (walking until pain could not be tolerated), self-reported improvements in walking distance and speed, and decreased pain. The other two trials showed no benefit of propionyl-L-carnitine on peak walking time compared with placebo 113.
More research is needed to fully understand the effects of carnitine on cardiovascular health.
Heart attack
Heart attack also called myocardial infarction occurs when an atherosclerotic plaque in a coronary artery ruptures and obstructs the blood supply to the heart muscle, causing injury or damage to the heart. Several clinical trials have explored whether L-carnitine administration immediately after heart attack diagnosis could reduce injury to heart muscle resulting from ischemia and improve clinical outcomes. An early trial in 160 men and women diagnosed with a recent heart attack showed that oral L-carnitine 4 g/day in addition to standard pharmacological treatment for one year significantly reduced mortality and the occurrence of angina attacks compared to the control 114. In another controlled trial in 96 patients, treatment with intravenous L-carnitine (5 g bolus followed by 10 g/day for three days) following a heart attack resulted in lower concentrations of creatine kinase-MB and troponin-1, two markers of cardiac injury 115. However, not all clinical trials have found L-carnitine supplementation to be beneficial after heart attack. For example, in a randomized, double-blind, placebo-controlled trial in 60 participants diagnosed with an acute heart attack, neither mortality nor echocardiographic measures of cardiac function differed between patients treated with intravenous L-carnitine (6 g/day) for seven days followed by oral L-carnitine (3 g/day) for three months and those given a placebo 116. Another randomized placebo-controlled trial in 2,330 patients with acute heart attack, L-carnitine therapy (9 g/day intravenously for five days, then 4 g/day orally for six months) did not affect the risk of heart failure and death six months after heart attack 117.
A 2013 meta-analysis of randomized controlled trials found that L-carnitine therapy in patients who experienced an heart attack reduced the risks of all-cause mortality (-27%; 11 trials; 3,579 participants), ventricular arrhythmias (-65%; five trials; 229 participants), and angina attacks (-40%; 2 trials; 261 participants), but had no effect on the risks of having a subsequent myocardial infarction or developing heart failure 104. Because about 90% of oral L-carnitine supplements is unlikely to be absorbed, one could ask whether the efficacy is equivalent between protocols using both intravenous and oral administration and those using oral administration only 26. This has not been examined in subgroup analyses.
Heart failure
Heart failure is described as the heart’s inability to pump enough blood for all of the body’s needs. In coronary heart disease, accumulation of atherosclerotic plaque in the coronary arteries may prevent heart regions from getting adequate circulation, ultimately resulting in cardiac damage and impaired pumping ability. Heart attack (myocardial infarction) may also damage the heart muscle, which could potentially lead to heart failure. Furthermore, the diminished heart’s capacity to pump blood in cases of dilated cardiomyopathy may lead to heart failure. Because physical exercise increases the demand on the weakened heart, measures of exercise tolerance are frequently used to monitor the severity of heart failure. Echocardiography is also used to determine the left ventricular ejection fraction (LVEF), an objective measure of the heart’s pumping ability. A left ventricular ejection fraction (LVEF) of less than 40% is indicative of systolic heart failure 118.
An abnormal acylcarnitine profile and a high acylcarnitine to free carnitine ratio in the blood of patients with heart failure have been linked to disease severity and poor prognosis 119, 120, 121. Addition of L-carnitine to standard medical therapy for heart failure has been evaluated in several clinical trials. A 2013 meta-analysis of 17 randomized, placebo-controlled studies in a total of 1,625 participants with heart failure found that oral L-carnitine (1.5-6 g/day for seven days to three years) significantly improved several measures of cardiac functional capacity (including exercise tolerance and markers of the left ventricle function), yet had no impact on all-cause mortality 108.
Angina pectoris
Angina pectoris is chest pain that occurs when the coronary blood supply is insufficient to meet the metabolic needs of the heart muscle 122. In a prospective cohort study in over 4,000 participants with suspected angina pectoris, elevated concentrations of certain acylcarnitine intermediates in blood were associated with fatal and non-fatal acute myocardial infarction 123. In early studies, the addition of oral L-carnitine or propionyl-L-carnitine to pharmacologic therapy for chronic stable angina modestly improved exercise tolerance and decreased electrocardiographic signs of ischemia during exercise testing in some angina patients 124, 125, 126. Another early study examined hemodynamic and angiographic variables before, during, and after administering intravenous propionyl-L-carnitine (15 mg/kg body weight) in men with myocardial dysfunction and angina pectoris 127. In this study, propionyl-L-carnitine decreased myocardial ischemia, evidenced by significant reductions in ST-segment depression and left ventricular end-diastolic pressure 127. No recent and/or large-scale studies have been conducted to further examine the potential benefit of L-carnitine or propionyl-L-carnitine in the management of angina pectoris.
Insulin resistance
Insulin resistance plays an important role in the development of type 2 diabetes. Because insulin resistance may be associated with mitochondrial dysfunction and a defect in fatty-acid oxidation in muscle, carnitine supplementation has been studied for its possible effects on insulin resistance and diabetes 128, 129, 130, 131.
A 2023 meta-analysis of 41 randomized clinical trials examined the effects of L-carnitine supplementation on glycemic markers in 2,900 men and women age 18 years and older 132. Most participants had health conditions such as type 2 diabetes, obesity, polycystic ovary syndrome (PCOS) or nonalcoholic fatty liver disease (NAFLD). L-carnitine supplements at doses of 0.25 to 4 g/day for 2 to 52 weeks reduced fasting blood glucose, insulin resistance, and glycosylated hemoglobin (HbA1c) but not serum insulin levels 132.
Other meta-analyses have had a narrower focus, examining only studies in specific populations. A 2017 meta-analysis included five randomized clinical trials (three of which were included in the 2023 meta-analysis described above) in a total of 631 adults with insulin resistance who took 2 or 3 g/day L-carnitine or placebo for 4 weeks to 12 months 133. The L-carnitine improved measures of insulin resistance, and the benefits at 12 months exceeded those at 3 months 133.
A systematic review and meta-analysis of four randomized clinical trials (all of which were included in the 2023 meta-analysis described above) with a total of 284 adults with type 2 diabetes compared the metabolic effects of L-carnitine with those of placebo. The results showed that 2 or 3 g/day L-carnitine for 12 to 52 weeks reduced levels of fasting plasma glucose, total cholesterol, LDL cholesterol, and apolipoproteins B100 and A1 but not triglycerides, lipoprotein (a), or HbA1c.
Additional clinical trials with larger samples are needed to determine whether L-carnitine supplements can reduce the risk of diabetes or the severity of complications.
Type 2 diabetes mellitus
Several small clinical trials have explored whether supplemental L-carnitine could improve glucose tolerance in people with impaired glucose metabolism. A potential benefit of L-carnitine in these patients is based on the fact that it can (i) increase the oxidation of long-chain fatty acids which accumulation may contribute to insulin resistance in skeletal muscle, and (ii) enhance glucose utilization by reducing acyl-CoA concentration within the mitochondrial matrix 134. A meta-analysis of five trials in participants with either impaired fasting glucose, type 2 diabetes mellitus, or nonalcoholic steatohepatitis found evidence of an improvement in insulin resistance with supplemental L-carnitine compared to placebo 133. Another meta-analysis of four randomized, placebo-controlled trials found evidence of a reduction in fasting plasma glucose concentration and no improvement of glycated hemoglobin concentration in subjects with type 2 diabetes mellitus supplemented with acetyl-L-carnitine (ALCAR) 129. A third meta-analysis of 16 trials suggested that supplementation with (acyl)-L-carnitine may reduce fasting blood glucose and glycated hemoglobin concentrations, but not resistance to insulin 135. In a recent double-blind, randomized, placebo-controlled trial, the effect of acetyl-L-carnitine (ALCAR) was examined in 229 participants treated for type 2 diabetes mellitus, hypertension, and dyslipidemia 136. Acetyl-L-carnitine (ALCAR) supplementation 1 g/day for 6 months had no effect on systolic or diastolic blood pressure, markers of kidney function (i.e., glomerular filtration rate and albuminuria), markers of glucose homeostasis (i.e., glucose disposal rate, glycated hemoglobin concentration, and a measure of insulin resistance), and blood lipid profile (i.e., concentrations of triglycerides, lipoprotein (a), LDL-cholesterol, HDL-cholesterol, and total cholesterol) 136.
Infertility
Carnitine might play a role in sperm maturation, sperm motility, and spermatogenesis 137, 21. Carnitine might also reduce oxidative stress, which could improve developing egg (oocyte) growth and maturation in female ovary 138. Therefore, researchers are examining whether supplemental carnitine improves sperm count, concentration, and motility as well as pregnancy rates.
A systematic review and meta-analysis of three randomized clinical trials examined the effects of 1 g/day to 3 g/day L-carnitine or acetyl-L-carnitine (ALCAR) for 2 to 6 months on sperm parameters in 201 men age 20 to 40 years who had infertility 139. Compared to placebo, supplemental carnitine improved sperm motility by 7.84% and morphology by 4.91% but did not affect sperm concentration 139.
A 2022 Cochrane Review assessed the effectiveness of carnitine supplementation on male subfertility (delays in conception due to low sperm concentration) 140. The review included six randomized clinical trials in a total of 1,089 men with subfertility who took 1,000 to 3,000 mg/day carnitine for 8 weeks to 6 months 140. In some trials, carnitine was compared with placebo, whereas in others, it was compared with antioxidants such as vitamin C or vitamin E or a control group that received no treatment. Carnitine supplementation increased sperm motility and concentration at some timepoints (e.g., 3 months) but did not affect rates of live birth or pregnancy 140.
Researchers have also examined whether carnitine might improve ovulation and pregnancy rates in females with polycystic ovary syndrome (PCOS), a condition that commonly causes infertility. In one 26-month randomized controlled trial, 170 women younger than 35 years took clomiphene citrate and either 3 g/day supplemental L-carnitine or placebo from day 3 of their menstrual cycle until the day of their first positive pregnancy test result 141. Individuals in the group taking L-carnitine had 64.4% higher ovulation rates and thicker endometrial tissue (10.1 mm vs. 6.8 mm) than those in the placebo group. In addition, more participants in the L-carnitine group became pregnant than those who took placebo, and they had fewer miscarriages.
In a 3-month randomized controlled trial, 280 women with PCOS received either 3 g L-carnitine or placebo 142, 143. Participants who took L-carnitine supplements had improved menstrual cycle regularity and higher ovulation and pregnancy rates, but miscarriage rates did not differ between the groups 142, 143.
More research is needed to determine whether carnitine supplements affect male infertility or pregnancy rates in women with PCOS.
Osteoarthritis
Some research suggests that carnitine reduces levels of C-reactive protein (CRP), a biomarker of systemic inflammation, and levels of malondialdehyde, a lipid peroxidation product that induces pain and disability in patients with osteoarthritis 144. In addition, levels of acylcarnitines (conjugated carnitine esters) are lower in people with osteoarthritis than in age- and gender-matched healthy individuals 145. For these reasons, investigators are studying whether L-carnitine supplements can relieve osteoarthritis symptoms, but study results have been mixed 144, 146.
A randomized clinical trial examined the anti-inflammatory effects of L-carnitine supplementation for osteoarthritis management in 69 women age 40 to 60 years with mild to moderate osteoarthritis in both knees 147. The women took 250 mg L-carnitine three times a day or placebo for 8 weeks. Serum levels of several inflammation biomarkers and pain scores were lower in the carnitine group than in the placebo group: Interleukin-1-beta levels decreased 5.53%, matrix metalloproteinase-1 levels decreased 9.10%, and the visual analog scale of pain decreased 52.67% 147.
In another randomized clinical trial, 76 women (average age 55 years) with obesity and knee osteoarthritis took 1 g/day L-carnitine or placebo for 12 weeks 144. In comparison with placebo, carnitine did not reduce osteoarthritis pain or stiffness or increase physical function 144.
Larger studies with samples that include both men and women are needed to determine whether carnitine supplementation helps manage osteoarthritis symptoms.
Athletic performance enhancement
Carnitine helps preserve muscle glycogen and promote fat oxidation. Carnitine also spares the use of amino acids as energy sources during exercise, making them potentially available for new protein synthesis 37 and decreases the accumulation of lactate 148. However, research findings on the effectiveness of supplemental carnitine on athletic performance are mixed 37.
One study randomly assigned 14 recreational athletes age 24–28 years with an average body mass index (BMI) of 23 to consume a carbohydrate solution with or without 2.0 g of L-carnitine tartrate twice a day for 24 weeks 149. At the end of the trial, perceived exertion on a cycle ergometer at a workload of 50% and then 80% of maximal oxygen consumption (VO2max, a measure of aerobic fitness and endurance capacity) was lower in the carnitine group (14.0, Borg scale) than in the control group (16.2) 149.
In another study, 24 men age 18–40 years (eight omnivores and 16 vegetarians) took 1 g L-carnitine twice daily for 12 weeks 150. Each participant performed a 60-minute cycling exercise at 75% VO2max at the beginning and end of the trial. Carnitine supplementation had no significant effect on VO2max, blood lactate concentration, skeletal muscle energy metabolism, or physical performance in either the vegetarians or the omnivores. Carnitine supplementation increased skeletal muscle carnitine stores in the vegetarians, but not the omnivores, by approximately 13% 150.
A 2018 comprehensive review summarized the effects of supplemental L-carnitine on exercise performance and recovery in well-trained athletes (age 16–36 years) and recreationally active adults (age 18–50 years) 151. The review included 11 clinical trials (one of which was the trial described above) in a total of 251 well-trained athletes who took 1 to 4 grams L-carnitine or placebo a single time or once or twice daily for up to 6 months 151. L-carnitine supplements reduced lactate levels and heart rate; increased lipid metabolism, VO2max, oxygen consumption, and L-carnitine plasma concentrations; improved performance; and hastened recovery in some of the studies 151. However, L-carnitine supplements did not affect performance or maximal exercise test results in other studies. In 17 studies that included recreationally active adults, a total of 237 participants took 2 g L-carnitine once or 2 to 4 g L-carnitine or placebo once or twice daily for up to 3 months. L-carnitine decreased plasma lactate concentrations, pyruvate concentrations, and muscle soreness and increased VO2max and recovery in some studies. However, in other studies, L-carnitine did not affect lactate, heart rate, VO2max, endurance, performance time, or perceived exertion during exercise.
A systematic review of 11 randomized clinical trials examined the effects of oral L-carnitine supplementation on high- and moderate-intensity exercise performance in a total of 203 physically active and untrained adults age 18 to 46 years 152. Participants took 3 to 4 g/day L-carnitine for 1 week or 1 to 3 g/day for 4 to 24 weeks or placebo (or, in one study also described above, a carbohydrate solution) 152. The studies had mixed results. Some studies found significant improvements in VO2max, peak power, maximum sprinting power, perceived exertion, and number of repetitions and volume lifted in a leg press in the L-carnitine group. However, other studies found no differences in VO2max, fatigue, maximum and average power, or total work on a cycle ergometer. No studies found that L-carnitine supplementation improved moderate-intensity exercise performance.
Overall, the evidence on supplemental carnitine’s effectiveness for performance enhancement is mixed, and additional investigations are needed.
Weight loss
Because carnitine transports fatty acids into the mitochondria and acts as a cofactor for fatty acid oxidation, researchers have proposed using L-carnitine supplements to promote weight loss, often in conjunction with a low-calorie diet, exercise, or prescription weight-loss drugs 153. Weight loss has been a secondary outcome in most studies, and these studies have had inconclusive results.
In a randomized clinical trial in 258 adults age 47–59 years with uncontrolled type 2 diabetes, participants who took 2 g/day L-carnitine plus the prescription medication orlistat (360 mg/day) for 1 year lost more weight (11.3 kg) than those who took orlistat alone (9.5 kg) 154. However, in another randomized clinical trial, 2 g/day L-carnitine alone for 6 months did not affect weight loss in 94 men and women who were overweight (age 43–58 years; BMI range 24.6–29.8) and had newly diagnosed type 2 diabetes 155. A 2016 systematic review and meta-analysis combined the results from nine randomized clinical trials in adults (including the two described above) that assessed carnitine’s effects on weight loss 153. The trials included a total of 911 participants. In eight trials, doses ranged from 1.8 to 4 g/day L-carnitine for 30 to 360 days; in the ninth trial, the dose was 15 mg/kg/day for 182 days. Study participants who took carnitine supplements lost an average of 1.33 kg more weight than those who took a placebo, regardless of the study duration or L-carnitine dose 153.
Larger studies are needed to determine whether carnitine supplementation affects weight loss.
Chemotherapy-induced peripheral neuropathy
A few randomized, double-blind, placebo-controlled trials have examined whether acetyl-L-carnitine (ALCAR) might help prevent or treat chemotherapy-induced peripheral neuropathy. A trial in 150 participants with either ovarian cancer or castration-resistant prostate cancer found no evidence that acetyl-L-carnitine (ALCAR) 1g every 3 days given with the anticancer drug sagopilone for up to six cycles of treatment reduced the overall risk of peripheral neuropathy compared to a placebo 156. However, acetyl-L-carnitine (ALCAR) reduced the risk of high-grade sagopilone-induced neuropathy 156. In contrast, another trial in 409 women with breast cancer found that acetyl-L-carnitine (ALCAR) 3 g/day for 24 weeks increased anticancer drug taxanes-induced peripheral neuropathy and decreased measures of functional status compared to placebo 157. A follow-up study reported that the negative impact of 24-week treatment with acetyl-L-carnitine (ALCAR) was still observed at week 52; however, no differences between acetyl-L-carnitine (ALCAR) and placebo were apparent at week 104 158. Finally, one trial in 239 participants already suffering from chemotherapy-induced peripheral neuropathy reported a reduction in the severity of neuropathic symptoms with acetyl-L-carnitine (ALCAR) 3 g/day for eight weeks compared to placebo 159. Improvements in electrophysiological parameters were also observed with acetyl-L-carnitine (ALCAR) treatment 159.
The results from these trials are conflicting and therefore difficult to interpret. The efficacy of acetyl-L-carnitine (ALCAR) in the prevention and treatment of chemotherapy-induced peripheral neuropathy remains to be established 160.
Diabetic peripheral neuropathy
Peripheral nerve dysfunction occurs in about 50% of people with diabetes mellitus, and chronic neuropathic pain is present in about one-third of people with diabetic peripheral neuropathy 161. Advanced stages of diabetic peripheral neuropathy can lead to recurrent foot ulcers and infections, and eventually amputations 162. A 2019 systematic review 163 identified three placebo-controlled interventions that examined the effect of oral supplementation with acetyl-L-carnitine (ALCAR) 1.5-3.0 g/day for one year in individuals with diabetic peripheral neuropathy 164, 32. Low-quality evidence suggested a lower level of pain with acetyl-L-carnitine (ALCAR), as measured with a visual scale analog. Low-quality evidence from another trial that compared the effect of acetyl-L-carnitine (ALCAR) 1.5 g/day with that of methylcobalamin (a form of vitamin B12) 1.5 mg/day for 24 weeks suggested no difference between treatments regarding the extent of functional disability (using the Neuropathy Disability Scale) or measures of symptom quality and severity (using the Neuropathy Symptom Scale) 165.
The use of certain antiretroviral agents such as nucleoside analogs has been associated with an increased risk of developing peripheral neuropathy in HIV-positive individuals 166, 167. Small, uncontrolled, open-label intervention studies have suggested a beneficial effect of acetyl-L-carnitine (ALCAR) in patients with painful neuropathies. An early uncontrolled study found that 10 out of 16 HIV-positive subjects with painful neuropathy reported improvement after three weeks of intravenous or intramuscular acetyl-L-carnitine (ALCAR) treatment 168. Results from another uncontrolled intervention in 21 HIV-positive patients suggested that long-term (two to four years) oral acetyl-L-carnitine (ALCAR) supplementation 1.5 g/day may be a beneficial adjunct to antiretroviral therapy to improve neuropathic symptoms in some HIV-infected individuals 169, 170. Additionally, two small studies in participants presenting with antiretroviral-induced neuropathy found significant reduction in subjects’ mean pain intensity with oral acetyl-L-carnitine (ALCAR) 1-3 g/day for 4 to 24 weeks, but no effect on objective neurophysiological parameters was found 171, 172.
A double-blind, placebo-controlled trial in 90 HIV-positive patients with symptomatic distal symmetrical polyneuropathy found no benefit of intramuscular injection with 1 g/day of acetyl-L-carnitine (ALCAR) for two weeks in the intention-to-treat analysis, but there was some pain relief in the group of 66 patients who completed the trial 173. Large-scale, controlled studies are needed before any conclusions can be drawn.
End-stage renal disease (ESRD)
L-Carnitine and short/medium-chain acylcarnitine molecules are removed from the circulation during hemodialysis. Both L-carnitine loss into the dialysate and impaired synthesis by the kidneys contribute to a progressive carnitine deficiency in patients with end-stage renal disease (also known as kidney failure or renal failure) undergoing hemodialysis 174. The low clearance of long-chain acylcarnitine molecules leads to a high acylcarnitine-to-L-carnitine ratio that has been associated with a higher risk of cardiovascular mortality 175. Carnitine depletion in patients undergoing hemodialysis may lead to various conditions, such as muscle weakness and fatigue, plasma lipid abnormalities, and refractory anemia.
A 2014 systematic review and meta-analysis of 31 randomized controlled trials in a total of 1,734 patients with end-stage renal disease (kidney failure) found that L-carnitine treatment — administered either orally or intravenously — resulted in reductions of serum C-reactive protein (a marker of inflammation and predictor of mortality in patients undergoing hemodialysis) and LDL-cholesterol, although the latter was not deemed to be clinically relevant 176. There was no effect of L-carnitine on other serum lipids (i.e., total and HDL-cholesterol, triglycerides) and anemia-related indicators (i.e., hemoglobin concentration, hematocrit, albumin, and required dose of recombinant erythropoietin) 176.
The US National Kidney Foundation did not recommend routine administration of L-carnitine to subjects undergoing dialysis yet encouraged the development of trials in patients with select symptoms that do not respond to standard therapy, i.e., persistent muscle cramps or hypotension during dialysis, severe fatigue, skeletal muscle weakness or myopathy, cardiomyopathy, and anemia requiring large doses of erythropoietin 177, 178.
Finally, the use of L-carnitine (10-20 mg/kg body weight given as a slow bolus injection) is approved by the U.S. Food and Drug Administration (FDA) to treat L-carnitine deficiency in subjects with end-stage renal disease undergoing hemodialysis 23.
Depression
A 2018 meta-analysis identified 12 randomized controlled trials, including 791 participants, that examined the effect of acetyl-L-carnitine (ALCAR) on symptoms of depression 179. Evidence from nine trials suggested a reduction in depressive symptoms with acetyl-L-carnitine (ALCAR) 3 g/day for a median 8 weeks compared to a placebo. Three trials that compared acetyl-L-carnitine (ALCAR) treatment 1-3 g/day for 7-12 weeks and antidepressant medications found acetyl-L-carnitine (ALCAR) was as effective as antidepressants in treating depressive symptoms 179. Another meta-analysis of trials that compared the safety profile of antidepressants found evidence of fewer adverse effects, and consequently, better adherence to treatment with acetyl-L-carnitine (ALCAR) compared to placebo and in contrast to classical pharmaceutical agents 180.
Hepatic encephalopathy
Hepatic encephalopathy refers to the occurrence of a spectrum of neuropsychiatric signs or symptoms in individuals with acute or chronic liver disease 181. Subclinical hepatic encephalopathy may not feature any symptoms beyond abnormal behavior on psychometric tests or symptoms that are nonspecific in nature. In contract, overt hepatic encephalopathy can present with disorientation, obvious personality change, inappropriate behavior, somnolence, stupor, confusion, and coma 181. Changes in mental status are thought to be caused by the liver failing to detoxify neurotoxic compounds like ammonia. A 2019 systematic review of five placebo-controlled trials conducted by one group of investigators examined the effect of acetyl-L-carnitine (ALCAR) in 398 participants with cirrhosis and portal hypertension (high blood pressure in the portal vein) and presenting with either subclinical or overt hepatic encephalopathy. acetyl-L-carnitine (ALCAR) was either administered orally (4 g/day for 90 days) in four trials or intravenously (4 g/day for three days) in one trial. Acetyl-L-carnitine (ALCAR) was found to significantly reduce blood ammonium concentration compared to placebo. However, none of the trials reported on serious adverse outcomes, including mortality. Additionally, the evidence was too limited to assess the impact on quality of life or mental and physical fatigue.
Fatigue is not uncommon in people who have undergone chemotherapy and survived cancer, with fatigue symptoms depending on the specific type of cancer and treatment. Cancer-related fatigue can persist well beyond the end of chemotherapy and be associated with cognitive and functional decline, insomnia, depression, and a reduction in the quality of life 182. A 2017 systematic review and meta-analysis identified 12 intervention studies that assessed the effect of L-carnitine or acetyl-L-carnitine (ALCAR) on cancer-related fatigue (reported as a primary or secondary outcome) in cancer survivors 183. Three studies had no control arm, eight studies were open-label, and eight studies included fewer than 100 participants. Overall, only three studies were deemed of good quality. The meta-analysis of these three randomized, double-blind, placebo-controlled trials found no effect of L-carnitine (0.25-4 g/day for 1 week to 3 months) or acetyl-L-carnitine (ALCAR) (3 g/day for 6 months) on the level of cancer-related fatigue 183.
Frailty
Frailty is a syndrome common among geriatric populations and characterized by a functional decline and a loss of independence to perform the activities of daily living. Frailty in individuals may include at least three of the following symptoms: unintentional weight loss, exhaustion (poor endurance), weakness (low grip strength), slowness, and physical inactivity 184. It is believed that early stages of frailty are manageable to interventions that could avert adverse outcomes, including the increased risk of hospitalization and premature death 185. The suggestion that carnitine deficiency may lead to frailty through mitochondrial dysfunction has been examined in one trial 186. This randomized, double-blind, placebo-controlled trial in 58 older adults identified as “pre-frail” found an decrease in a Frailty Index score and an improvement in the hand grip test in individuals supplemented with L-carnitine (1.5 g/day) over 10 weeks but not in those given a placebo 187. However, there was no difference in Frailty Index and hand grip test scores between supplemental L-carnitine and placebo groups.
Skeletal muscle wasting
Loss of skeletal muscle mass also known as sarcopenia is associated with a decrease in muscle strength and occurs with aging 188, as well as in several pathological conditions 189, 190, 191. Based on preclinical studies, it has been suggested that L-carnitine supplementation could limit the imbalance between protein anabolism (synthesis) and catabolism (degradation) that leads to skeletal muscle wasting 134. A randomized, double-blind, placebo-controlled trial in 28 older women (ages, 65-70 years) found no effect of L-carnitine supplementation (1.5 g/day for 24 weeks) on serum pro-inflammatory cytokine concentrations, body mass and composition (lean [fat-free] mass and skeletal muscle mass), or measures of skeletal muscle strength 192. In contrast, a retrospective cohort study in patients with cirrhosis found a reduced rate of skeletal muscle loss over at least six months in those who were administered L-carnitine (N=35; mean dose, 1.02 g/day) compared to those who were not 193. Of note, supplementation with L-carnitine was given in patients with cirrhosis to control hyperammonemia (N=27), to reduce muscle cramps (N=6), or to prevent carnitine deficiency (N=2). One major limitation of this study beyond its retrospective design is that patients who received L-carnitine had a significantly different clinical presentation; in particular, liver dysfunction was significantly more severe in these patients than in those who were not supplemented 193.
Muscle cramps
Muscle cramps are involuntary and painful contractions of skeletal muscles. Two uncontrolled studies conducted in participants with cirrhosis found that L-carnitine supplementation was safe to use at doses of 0.9 to 1.2 g/day for eight weeks 194 and 1 g/day for 24 weeks 195 and might be considered to control the frequency of cramps. However, whether supplemental L-carnitine can be efficacious to limit the incidence of muscle cramps in patients with cirrhosis remains unknown. An open-label, non-randomized trial in 69 patients with either type 1 or type 2 diabetes mellitus found a reduction in the incidence of muscle cramps and an improvement in the quality of life of those prescribed 0.6 g/day of L-carnitine for four months compared to controls 196. In contrast, there is little evidence to date to suggest that supplemental L-carnitine could reduce muscle cramps in patients undergoing hemodialysis 197. Well-designed trials are necessary to examine whether L-carnitine could be helpful in the management of muscle cramps.
L-Carnitine dose
Recommended doses of L-carnitine vary depending on the health condition being treated. The usual L-carnitine dose is between 1 to 3 g per day. In the selected studies, participants were supplemented in a dose ranging from 1 g to 4,5 g per day for either 12 or 24 weeks 198. L-carnitine supplements providing more than 3 g/day of L-carnitine may cause a “fishy” body odor. High doses (5 or more grams per day) may cause diarrhea.
People with the following conditions should talk to their doctor before taking carnitine:
- Peripheral vascular disease
- High blood pressure
- Liver disease from alcoholism (cirrhosis)
- Diabetes
- Kidney disease
- History of seizures
L-Carnitine side effects
In general, L-carnitine appears to be well tolerated; no toxic effects have been reported in relation to intakes of high doses of L-carnitine. L-Carnitine supplementation may cause mild gastrointestinal symptoms, including nausea, vomiting, abdominal cramps, diarrhea and muscle weakness in people with uremia and seizures in those with seizure disorders 83, 199, 200. L-carnitine supplements providing more than 3 g/day may cause a “fishy” body odor due to bacterial degradation of unabsorbed oral L-carnitine in the bowel resulting in trimethylamine, which has a peculiar fishy odor 36, 80.
Acetyl-L-carnitine (ALCAR) has been reported to increase agitation in some Alzheimer’s disease patients 76. Despite claims that L-carnitine or acetyl-L-carnitine (ALCAR) might increase seizures in some individuals with seizure disorders 76, these are not supported by any scientific evidence 201. Only the L-isomer of carnitine is biologically active; the D-isomer may actually compete with L-carnitine for absorption and transport, thereby increasing the risk of L-carnitine deficiency 28. Supplements containing a mixture of the D- and L-isomers (D,L-carnitine) have been associated with muscle weakness in patients with kidney disease. Long-term studies examining the safety of acetyl-L-carnitine (ALCAR) supplementation in pregnant and breast-feeding women are lacking 76.
Some research indicates that intestinal bacteria breakdown unabsorbed carnitine to form trimethylamine-N-oxide (TMAO) and gamma-butyrobetaine, which are proatherogenic substances that are associated with increased risk of cardiovascular disease 109, 202, 203, 204, 109, 110. The increased risk of cardiovascular disease appears to be more pronounced in people who consume meat than in vegans or vegetarians. The implications of these findings are not well understood and require more research.
Drug interactions
Several types of medications have the potential to interact with L-carnitine supplements. A few examples are provided below. People taking these and other medications on a regular basis should discuss their L-carnitine intake with their doctors.
- Pivalate-conjugated antibiotics. Carnitine interacts with pivalate-conjugated antibiotics, such as pivampicillin, that are used to prevent urinary tract infections 205. Pivalic acid combines with L-carnitine and is excreted in the urine as pivaloylcarnitine, thereby increasing L-carnitine losses. Consequently, prolonged use of pivalic acid-containing antibiotics, including pivampicillin, pivmecillinam, pivcephalexin, and cefditoren pivoxil (Spectracef), can lead to secondary L-carnitine deficiency. However, although tissue carnitine levels in people who take these antibiotics may become low enough to limit fatty acid oxidation, no cases of illness due to carnitine deficiency in this population have been described 206, 40, 71.
- Valproic acid and other anticonvulsants. Treatment with the anticonvulsants valproic acid, phenobarbital, phenytoin, and carbamazepine reduces blood levels of carnitine 207, 208, 209, 210. The anticonvulsant valproic acid (Depakene) interferes with L-carnitine biosynthesis in the liver and forms with L-carnitine a valproylcarnitine ester that is excreted in the urine. However, L-carnitine supplements are necessary only in a subset of patients taking valproic acid. Risk factors for L-carnitine deficiency with valproic acid include young age (<2 years), severe neurological problems, use of multiple antiepileptic drugs, poor nutrition, and consumption of a ketogenic diet. In addition, the use of valproic acid with or without other anticonvulsants may cause liver toxicity and increase plasma ammonia concentrations, leading to encephalopathy 209, 211. This toxicity may also occur after acute valproic acid overdoses. Intravenous L-carnitine administration might help treat valproic acid toxicity in children and adults, although the optimal regimen has not been identified 212.
- There is insufficient evidence to suggest that nucleoside analogs used in the treatment of HIV infection (i.e., zidovudine [AZT], didanosine [ddI], zalcitabine [ddC], and stavudine [d4T] or certain cancer chemotherapy agents (i.e., ifosfamide, cisplatin) increase the risk of secondary L-carnitine deficiency.
- Rebouche CJ. Carnitine. In: Shils ME, Shike M, Ross AC, Caballero B, Cousins RJ, eds. Modern Nutrition in Health and Disease. 10th ed. Philadelphia: Lippincott, Williams & Wilkins; 2006:537-544.[↩][↩][↩][↩]
- Flanagan JL, Simmons PA, Vehige J, Willcox MD, Garrett Q. Role of carnitine in disease. Nutr Metab (Lond). 2010 Apr 16;7:30. doi: 10.1186/1743-7075-7-30[↩]
- Rebouche CJ, Paulson DJ. Carnitine metabolism and function in humans. Annu Rev Nutr. 1986;6:41-66. doi: 10.1146/annurev.nu.06.070186.000353[↩]
- Mingorance C, Rodriguez-Rodriguez R, Justo ML, Herrera MD, de Sotomayor MA. Pharmacological effects and clinical applications of propionyl-L-carnitine. Nutr Rev. 2011 May;69(5):279-90. doi: 10.1111/j.1753-4887.2011.00387.x[↩]
- FRAENKEL G, FRIEDMAN S. Carnitine. Vitam Horm. 1957;15:73-118. doi: 10.1016/s0083-6729(08)60508-7[↩][↩]
- Longo N, Amat di San Filippo C, Pasquali M. Disorders of carnitine transport and the carnitine cycle. Am J Med Genet C Semin Med Genet. 2006 May 15;142C(2):77-85. doi: 10.1002/ajmg.c.30087[↩]
- Nakazaki K, Ogawa E, Ishige M, Ishige N, Fuchigami T, Takahashi S. Hypocarnitinemia Observed in an Infant Treated with Short-Term Administration of Antibiotic Containing Pivalic Acid. Tohoku J Exp Med. 2018 Apr;244(4):279-282. doi: 10.1620/tjem.244.279[↩]
- BHATTACHARYYA PK, CARTER HE, FRAENKEL G, WEIDMAN KR. The identity of vitamin BT with carnitine. Arch Biochem Biophys. 1952 Jan;35(1):241-2. doi: 10.1016/s0003-9861(52)80069-4[↩]
- Gulewitsch W., Krimberg R. Zur Kenntunis der extraktionsstoffe der muskeln. 2. Mittei-lung uber das carnitine. Hoppe-Seyler’s Z. Physiol. Chem. 1905;45:326–330.[↩]
- Kutscher F. Uber liebigs fleischextrakt. Mitteilung I. Z. Unters Nahr. Genubm. 1905;10:528–537.[↩]
- Sayed-Ahmed MM. Role of carnitine in cancer chemotherapy-induced multiple organ toxicity. Saudi Pharm J. 2010 Oct;18(4):195-206. doi: 10.1016/j.jsps.2010.07.008[↩][↩][↩]
- Rebouche CJ. Carnitine. In: Ross AC, Caballero B, Cousins RJ, et al., eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2014:252-3.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Tomita M., Senju Y. Uber die aminoverbindungen, welche die Biuretreaktion zeigen. III. Spaltungen der γ-Amino-β-oxybuttersaure in die optisch aktiven komponenten. Hoppe-Seyler’s Z. Physiol. Chem. 1927;169:263–277.[↩]
- Fritz I.B. The effect of muscle extracts on the oxidation of palmitic acid by liver slices and homogenates. Acta Physiol. Scand. 1955;34:367–385. doi: 10.1111/j.1748-1716.1955.tb01256.x[↩]
- Friedman S., Fraenkel G. Reversible enzymatic acetylation of carnitine. Arch. Biochem. Biophys. 1955;51:491–501. doi: 10.1016/0003-9861(55)90515-4[↩]
- BREMER J. Carnitine in intermediary metabolism. Reversible acetylation of carnitine by mitochondria. J Biol Chem. 1962 Jul;237:2228-31. https://www.jbc.org/article/S0021-9258(19)63423-X/pdf[↩]
- BREMER J. Carnitine in intermediary metabolism. The metabolism of fatty acid esters of carnitine by mitochondria. J Biol Chem. 1962 Dec;237:3628-32. https://www.jbc.org/article/S0021-9258(19)84498-8/pdf[↩]
- Kaneko T., Yoshida R. On the absolute configuration of L-carnitine (vitamin BT) Bull. Chem. Soc. Jpn. 1962;35:1153–1155.[↩]
- Tein I., Bukovac S.W., Xie Z.W. Characterization of the human plasmalemmal carnitine transporter in cultured skin fibroblasts. Arch. Biochem. Biophys. 1996;329:145–155. doi: 10.1006/abbi.1996.0203[↩]
- Rebouche CJ. Carnitine. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore; 2014:440-446.[↩][↩][↩][↩][↩][↩][↩]
- Mateus FG, Moreira S, Martins AD, Oliveira PF, Alves MG, Pereira ML. L-Carnitine and Male Fertility: Is Supplementation Beneficial? J Clin Med. 2023 Sep 6;12(18):5796. doi: 10.3390/jcm12185796[↩][↩][↩]
- Johri AM, Heyland DK, Hetu MF, Crawford B, Spence JD. Carnitine therapy for the treatment of metabolic syndrome and cardiovascular disease: evidence and controversies. Nutr Metab Cardiovasc Dis. 2014;24:808–814. doi: 10.1016/j.numecd.2014.03.007[↩]
- L-Carnitine. https://lpi.oregonstate.edu/mic/dietary-factors/L-carnitine[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Rebouche CJ. Ascorbic acid and carnitine biosynthesis. Am J Clin Nutr. 1991 Dec;54(6 Suppl):1147S-1152S. doi: 10.1093/ajcn/54.6.1147s[↩]
- Rebouche C.J., Lehman L.J., Olson L. Epsilon-N-trimethyllysine availability regulates the rate of carnitine biosynthesis in the growing rat. J. Nutr. 1986;116:751–759. doi: 10.1093/jn/116.5.751[↩]
- Evans AM, Fornasini G. Pharmacokinetics of L-carnitine. Clin Pharmacokinet. 2003;42(11):941-67. doi: 10.2165/00003088-200342110-00002[↩][↩][↩][↩]
- Lombard KA, Olson AL, Nelson SE, Rebouche CJ. Carnitine status of lactoovovegetarians and strict vegetarian adults and children. Am J Clin Nutr. 1989 Aug;50(2):301-6. doi: 10.1093/ajcn/50.2.301[↩][↩]
- Seim H, Eichler K, Kleber H. L(-)-Carnitine and its precursor, gamma-butyrobetaine. In: Kramer K, Hoppe P, Packer L, eds. Nutraceuticals in Health and Disease Prevention. New York: Marcel Dekker, Inc.; 2001:217-256.[↩][↩][↩]
- Rebouche CJ. Carnitine. In: Shils ME, Olson JA, Shike M, Ross AC, eds. Nutrition in Health and Disease. 9th ed. Baltimore: Lippincott Williams & Wilkins; 1999:505-512.[↩]
- Rebouche CJ, Chenard CA. Metabolic fate of dietary carnitine in human adults: identification and quantification of urinary and fecal metabolites. J Nutr. 1991 Apr;121(4):539-46. doi: 10.1093/jn/121.4.539[↩]
- Ferreira GC, McKenna MC. L-Carnitine and Acetyl-L-carnitine Roles and Neuroprotection in Developing Brain. Neurochem Res. 2017 Jun;42(6):1661-1675. doi: 10.1007/s11064-017-2288-7[↩][↩][↩][↩][↩]
- De Grandis D, Minardi C. Acetyl-L-carnitine (levacecarnine) in the treatment of diabetic neuropathy. A long-term, randomised, double-blind, placebo-controlled study. Drugs R D. 2002;3(4):223-31. doi: 10.2165/00126839-200203040-00001[↩][↩]
- McGarry J.D., Brown N.F. The mitochondrial carnitine palmitoyltransferase system: From concept to molecular analysis. Eur. J. Biochem. 1997;244:1–14. doi: 10.1111/j.1432-1033.1997.00001.x[↩]
- Belay B, Esteban-Cruciani N, Walsh CA, Kaskel FJ. The use of levo-carnitine in children with renal disease: a review and a call for future studies. Pediatr Nephrol. 2006 Mar;21(3):308-17. doi: 10.1007/s00467-005-2085-4[↩][↩][↩][↩]
- Borum PR. Carnitine. In: Marriott B, Birt DF, Stalling V, Yates A, eds. Present Knowledge in Nutrition, 11th ed. 2020:551-9.[↩][↩][↩]
- Almannai M, Alfadhel M, El-Hattab AW. Carnitine Inborn Errors of Metabolism. Molecules. 2019 Sep 6;24(18):3251. doi: 10.3390/molecules24183251[↩][↩][↩][↩][↩][↩][↩]
- Gnoni A, Longo S, Gnoni GV, Giudetti AM. Carnitine in Human Muscle Bioenergetics: Can Carnitine Supplementation Improve Physical Exercise? Molecules. 2020 Jan 1;25(1):182. doi: 10.3390/molecules25010182[↩][↩][↩]
- Pekala J, Patkowska-Sokoła B, Bodkowski R, Jamroz D, Nowakowski P, Lochyński S, Librowski T. L-carnitine–metabolic functions and meaning in humans life. Curr Drug Metab. 2011 Sep;12(7):667-78. doi: 10.2174/138920011796504536[↩][↩]
- Rebouche C.J. Kinetics, pharmacokinetics, and regulation of L-carnitine and acetyl-L-carnitine metabolism. Ann. N. Y. Acad. Sci. 2004;1033:30–41. doi: 10.1196/annals.1320.003[↩][↩]
- Rebouche CJ. Carnitine. In: Shils ME, Olson JA, Shike M, et al., eds. Modern Nutrition in Health and Disease, 9th ed. New York, NY: Lippincott Williams & Wilkins, 1999:505-12.[↩][↩][↩][↩]
- Alesci S, Manoli I, Costello R, Coates P, Gold PW, et al. Carnitine: lessons from one hundred years of research. Ann NY Acad Sci 2004;1033:ix-xi.[↩][↩]
- National Research Council (US) Subcommittee on the Tenth Edition of the Recommended Dietary Allowances. Recommended Dietary Allowances: 10th Edition. Washington (DC): National Academies Press (US); 1989. Available from: https://www.ncbi.nlm.nih.gov/books/NBK234932[↩][↩]
- National Research Council (US) Subcommittee on the Tenth Edition of the Recommended Dietary Allowances. Recommended Dietary Allowances: 10th Edition. Washington (DC): National Academies Press (US); 1989. 12, Other Substances in Food. Available from: https://www.ncbi.nlm.nih.gov/books/NBK234937[↩][↩]
- Longo N., Frigeni M., Pasquali M. Carnitine transport and fatty acid oxidation. Biochim. Biophys. Acta. 2016;1863:2422–2435. doi: 10.1016/j.bbamcr.2016.01.023[↩]
- Opalka JR, Gellerich FN, Zierz S. Age and sex dependency of carnitine concentration in human serum and skeletal muscle. Clin Chem. 2001 Dec;47(12):2150-3.[↩][↩]
- Coulter DL. Carnitine Deficiency. In: Daroff R, Aminoff M, eds. Encyclopedia of the Neurological Sciences, 2nd ed. Elsevier, 2014:597–99.[↩]
- Ezgu F. Inborn Errors of Metabolism. Adv Clin Chem. 2016;73:195-250. doi: 10.1016/bs.acc.2015.12.001[↩]
- Durazzo A, Lucarini M, Nazhand A, Souto SB, Silva AM, Severino P, Souto EB, Santini A. The Nutraceutical Value of Carnitine and Its Use in Dietary Supplements. Molecules. 2020 May 1;25(9):2127. doi: 10.3390/molecules25092127[↩][↩][↩]
- Borum PR. Carnitine. Annu Rev Nutr. 1983;3:233-59. doi: 10.1146/annurev.nu.03.070183.001313[↩]
- Rebouche CJ. L-carnitine. In: Erdman JWJ, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. ILSI/Wiley-Blackwell; 2012:391-404.[↩][↩]
- McGrane MM. Carbohydrate metabolism–synthesis and oxidation. In: Stipanuk MH, ed. Biochemical and Physiological Aspects of Human Nutrition. Philadelphia: W.B. Saunders Co; 2000:158-210.[↩]
- Solarska K, Lewińska A, Karowicz-Bilińska A, Bartosz G. The antioxidant properties of carnitine in vitro. Cell Mol Biol Lett. 2010;15(1):90-7. doi: 10.2478/s11658-009-0036-y[↩]
- Costell M, O’Connor JE, Grisolía S. Age-dependent decrease of carnitine content in muscle of mice and humans. Biochem Biophys Res Commun. 1989 Jun 30;161(3):1135-43. doi: 10.1016/0006-291x(89)91360-0[↩]
- Karlic H, Lohninger A, Laschan C, Lapin A, Böhmer F, Huemer M, Guthann E, Rappold E, Pfeilstöcker M. Downregulation of carnitine acyltransferases and organic cation transporter OCTN2 in mononuclear cells in healthy elderly and patients with myelodysplastic syndromes. J Mol Med (Berl). 2003 Jul;81(7):435-42. doi: 10.1007/s00109-003-0447-6[↩]
- Hagen TM, Ingersoll RT, Wehr CM, Lykkesfeldt J, Vinarsky V, Bartholomew JC, Song MH, Ames BN. Acetyl-L-carnitine fed to old rats partially restores mitochondrial function and ambulatory activity. Proc Natl Acad Sci U S A. 1998 Aug 4;95(16):9562-6. doi: 10.1073/pnas.95.16.9562[↩]
- Pesce V, Fracasso F, Cassano P, Lezza AM, Cantatore P, Gadaleta MN. Acetyl-L-carnitine supplementation to old rats partially reverts the age-related mitochondrial decay of soleus muscle by activating peroxisome proliferator-activated receptor gamma coactivator-1alpha-dependent mitochondrial biogenesis. Rejuvenation Res. 2010 Apr-Jun;13(2-3):148-51. doi: 10.1089/rej.2009.0955[↩]
- Gómez LA, Heath SH, Hagen TM. Acetyl-L-carnitine supplementation reverses the age-related decline in carnitine palmitoyltransferase 1 (CPT1) activity in interfibrillar mitochondria without changing the L-carnitine content in the rat heart. Mech Ageing Dev. 2012 Feb-Mar;133(2-3):99-106. doi: 10.1016/j.mad.2012.01.007[↩]
- Muthuswamy AD, Vedagiri K, Ganesan M, Chinnakannu P. Oxidative stress-mediated macromolecular damage and dwindle in antioxidant status in aged rat brain regions: role of L-carnitine and DL-alpha-lipoic acid. Clin Chim Acta. 2006 Jun;368(1-2):84-92. doi: 10.1016/j.cca.2005.12.010[↩]
- Aliev G, Liu J, Shenk JC, Fischbach K, Pacheco GJ, Chen SG, Obrenovich ME, Ward WF, Richardson AG, Smith MA, Gasimov E, Perry G, Ames BN. Neuronal mitochondrial amelioration by feeding acetyl-L-carnitine and lipoic acid to aged rats. J Cell Mol Med. 2009 Feb;13(2):320-33. doi: 10.1111/j.1582-4934.2008.00324.x[↩][↩]
- Tamilselvan J, Jayaraman G, Sivarajan K, Panneerselvam C. Age-dependent upregulation of p53 and cytochrome c release and susceptibility to apoptosis in skeletal muscle fiber of aged rats: role of carnitine and lipoic acid. Free Radic Biol Med. 2007 Dec 15;43(12):1656-69. doi: 10.1016/j.freeradbiomed.2007.08.028[↩]
- Sethumadhavan S, Chinnakannu P. L-carnitine and alpha-lipoic acid improve age-associated decline in mitochondrial respiratory chain activity of rat heart muscle. J Gerontol A Biol Sci Med Sci. 2006 Jul;61(7):650-9. doi: 10.1093/gerona/61.7.650[↩]
- Sundaram K, Panneerselvam KS. Oxidative stress and DNA single strand breaks in skeletal muscle of aged rats: role of carnitine and lipoicacid. Biogerontology. 2006 Apr;7(2):111-8. doi: 10.1007/s10522-006-0002-2[↩]
- Sethumadhavan S, Chinnakannu P. Carnitine and lipoic acid alleviates protein oxidation in heart mitochondria during aging process. Biogerontology. 2006 Apr;7(2):101-9. doi: 10.1007/s10522-006-6497-8[↩]
- Savitha S, Sivarajan K, Haripriya D, Kokilavani V, Panneerselvam C. Efficacy of levo carnitine and alpha lipoic acid in ameliorating the decline in mitochondrial enzymes during aging. Clin Nutr. 2005 Oct;24(5):794-800. doi: 10.1016/j.clnu.2005.04.005[↩]
- Savitha S, Panneerselvam C. Mitochondrial membrane damage during aging process in rat heart: potential efficacy of L-carnitine and DL alpha lipoic acid. Mech Ageing Dev. 2006 Apr;127(4):349-55. doi: 10.1016/j.mad.2005.12.004[↩]
- Kumaran S, Subathra M, Balu M, Panneerselvam C. Supplementation of L-carnitine improves mitochondrial enzymes in heart and skeletal muscle of aged rats. Exp Aging Res. 2005 Jan-Mar;31(1):55-67. doi: 10.1080/03610730590882846[↩]
- Kumaran S, Panneerselvam KS, Shila S, Sivarajan K, Panneerselvam C. Age-associated deficit of mitochondrial oxidative phosphorylation in skeletal muscle: role of carnitine and lipoic acid. Mol Cell Biochem. 2005 Dec;280(1-2):83-9. doi: 10.1007/s11010-005-8234-z[↩]
- National Institute of Child Health and Human Development, National Center for Complementary and Alternative Medicine, National Institute of Mental Health, Office of Dietary Supplements, National Institutes of Health. Carnitine: The Science Behind a Conditionally Essential Nutrient. March 25-26, 2004.[↩]
- Carnitine. https://ods.od.nih.gov/factsheets/Carnitine-Consumer[↩]
- Carnitine. https://ods.od.nih.gov/factsheets/Carnitine-HealthProfessional[↩][↩][↩]
- Rebouche CJ. Kinetics, pharmacokinetics, and regulation of L-carnitine and acetyl-L-carnitine metabolism. Ann NY Acad Sci 2004;1033:30-41.[↩][↩]
- Systemic Primary Carnitine Deficiency. https://rarediseases.org/rare-diseases/systemic-primary-carnitine-deficiency[↩][↩][↩][↩][↩]
- Primary carnitine deficiency. https://medlineplus.gov/genetics/condition/primary-carnitine-deficiency[↩][↩][↩][↩][↩][↩]
- Rebouche CJ. Kinetics, pharmacokinetics, and regulation of L-carnitine and acetyl-L-carnitine metabolism. Ann N Y Acad Sci. 2004 Nov;1033:30-41. doi: 10.1196/annals.1320.003[↩][↩]
- Gross CJ, Henderson LM, Savaiano DA. Uptake of L-carnitine, D-carnitine and acetyl-L-carnitine by isolated guinea-pig enterocytes. Biochim Biophys Acta. 1986 May 29;886(3):425-33. doi: 10.1016/0167-4889(86)90178-3[↩]
- Hendler SS, Rorvik DR. Acetyl-L-carnitine. PDR for Nutritional Supplements. 2nd ed. Montvale: Thomson Reuters; 2008:13-16.[↩][↩][↩][↩]
- Olson AL, Nelson SE, Rebouche CJ. Low carnitine intake and altered lipid metabolism in infants. Am J Clin Nutr. 1989 Apr;49(4):624-8. doi: 10.1093/ajcn/49.4.624[↩]
- American Academy of Pediatrics, Committee on Nutrition. Soy protein-based formulas: recommendations for use in infant feeding. Pediatrics. 1998;101(1):148-152.[↩]
- Ferreira CR, Van Karnebeek CD. Inborn errors of metabolism. In: de Vries LS, Glass HC, eds. Handbook of Clinical Neurology, vol. 162: Neonatal Neurology. Elsevier; 2019:449-81.[↩][↩]
- Longo N, Frigeni M, Pasquali M. Carnitine transport and fatty acid oxidation. Biochim Biophys Acta. 2016 Oct;1863(10):2422-35. doi: 10.1016/j.bbamcr.2016.01.023[↩][↩][↩][↩]
- Eknoyan G, Latos DL, Lindberg J; National Kidney Foundation Carnitine Consensus Conference. Practice recommendations for the use of L-carnitine in dialysis-related carnitine disorder. National Kidney Foundation Carnitine Consensus Conference. Am J Kidney Dis. 2003 Apr;41(4):868-76. doi: 10.1016/s0272-6386(03)00110-0[↩][↩]
- Longo N. Primary Carnitine Deficiency and Newborn Screening for Disorders of the Carnitine Cycle. Ann Nutr Metab. 2016;68 Suppl 3:5-9. doi: 10.1159/000448321[↩]
- Dahash BA, Sankararaman S. Carnitine Deficiency. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559041[↩][↩]
- El-Hattab AW, Almannai M. Primary Carnitine Deficiency. 2012 Mar 15 [Updated 2024 Dec 5]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK84551[↩][↩][↩]
- Adeva-Andany MM, Calvo-Castro I, Fernández-Fernández C, Donapetry-García C, Pedre-Piñeiro AM. Significance of l-carnitine for human health. IUBMB Life. 2017 Aug;69(8):578-594. doi: 10.1002/iub.1646[↩]
- El-Hattab AW, Scaglia F. Disorders of carnitine biosynthesis and transport. Mol Genet Metab. 2015 Nov;116(3):107-12. doi: 10.1016/j.ymgme.2015.09.004[↩][↩][↩][↩]
- Breningstall GN. Carnitine deficiency syndromes. Pediatr Neurol. 1990 Mar-Apr;6(2):75-81. doi: 10.1016/0887-8994(90)90037-2[↩]
- Stanley CA. Carnitine deficiency disorders in children. Ann N Y Acad Sci. 2004 Nov;1033:42-51. doi: 10.1196/annals.1320.004[↩]
- Penn D, Ludwigs B, Schmidt-Sommerfeld E, Pascu F. Effect of nutrition on tissue carnitine concentrations in infants of different gestational ages. Biol Neonate. 1985;47(3):130-5. doi: 10.1159/000242103[↩]
- Cairns PA, Stalker DJ. Carnitine supplementation of parenterally fed neonates. Cochrane Database Syst Rev. 2000;2000(4):CD000950. doi: 10.1002/14651858.CD000950[↩]
- Calvani M, Benatti P, Mancinelli A, D’Iddio S, Giordano V, Koverech A, Amato A, Brass EP. Carnitine replacement in end-stage renal disease and hemodialysis. Ann N Y Acad Sci. 2004 Nov;1033:52-66. doi: 10.1196/annals.1320.005[↩][↩]
- Hurot JM, Cucherat M, Haugh M, Fouque D. Effects of L-carnitine supplementation in maintenance hemodialysis patients: a systematic review. J Am Soc Nephrol. 2002 Mar;13(3):708-714. doi: 10.1681/ASN.V133708[↩][↩]
- Pons R, De Vivo DC. Primary and secondary carnitine deficiency syndromes. J Child Neurol. 1995 Nov;10 Suppl 2:S8-24.[↩]
- Knottnerus SJG, Bleeker JC, Wüst RCI, Ferdinandusse S, IJlst L, Wijburg FA, Wanders RJA, Visser G, Houtkooper RH. Disorders of mitochondrial long-chain fatty acid oxidation and the carnitine shuttle. Rev Endocr Metab Disord. 2018 Mar;19(1):93-106. doi: 10.1007/s11154-018-9448-1[↩]
- El-Gharbawy A, Vockley J. Inborn Errors of Metabolism with Myopathy: Defects of Fatty Acid Oxidation and the Carnitine Shuttle System. Pediatr Clin North Am. 2018 Apr;65(2):317-335. doi: 10.1016/j.pcl.2017.11.006[↩]
- Karlic H, Lohninger A. Supplementation of L-carnitine in athletes: does it make sense? Nutrition. 2004;20:709–715. doi: 10.1016/j.nut.2004.04.003[↩]
- Fielding R, Riede L, Lugo JP, Bellamine A. L-carnitine supplementation in recovery after exercise. Nutrients. 2018 doi: 10.3390/nu10030349[↩]
- Ferreira-Vieira TH, Guimaraes IM, Silva FR, Ribeiro FM. Alzheimer’s disease: Targeting the Cholinergic System. Curr Neuropharmacol. 2016;14(1):101-15. doi: 10.2174/1570159×13666150716165726[↩][↩]
- Bianchetti A, Rozzini R, Trabucchi M. Effects of acetyl-L-carnitine in Alzheimer’s disease patients unresponsive to acetylcholinesterase inhibitors. Curr Med Res Opin. 2003;19(4):350-3. doi: 10.1185/030079903125001776[↩]
- Hudson S, Tabet N. Acetyl-L-carnitine for dementia. Cochrane Database Syst Rev. 2003;2003(2):CD003158. doi: 10.1002/14651858.CD003158[↩][↩][↩][↩][↩]
- Montgomery SA, Thal LJ, Amrein R. Meta-analysis of double blind randomized controlled clinical trials of acetyl-L-carnitine versus placebo in the treatment of mild cognitive impairment and mild Alzheimer’s disease. Int Clin Psychopharmacol. 2003 Mar;18(2):61-71. doi: 10.1097/00004850-200303000-00001[↩][↩]
- Pennisi M, Lanza G, Cantone M, D’Amico E, Fisicaro F, Puglisi V, Vinciguerra L, Bella R, Vicari E, Malaguarnera G. Acetyl-L-Carnitine in Dementia and Other Cognitive Disorders: A Critical Update. Nutrients. 2020 May 12;12(5):1389. doi: 10.3390/nu12051389[↩]
- Lodeiro M, Ibáñez C, Cifuentes A, Simó C, Cedazo-Mínguez Á. Decreased cerebrospinal fluid levels of L-carnitine in non-apolipoprotein E4 carriers at early stages of Alzheimer’s disease. J Alzheimers Dis. 2014;41(1):223-32. doi: 10.3233/JAD-132063[↩]
- DiNicolantonio JJ, Lavie CJ, Fares H, Menezes AR, O’Keefe JH. L-carnitine in the secondary prevention of cardiovascular disease: systematic review and meta-analysis. Mayo Clin Proc. 2013 Jun;88(6):544-51. doi: 10.1016/j.mayocp.2013.02.007[↩][↩][↩][↩]
- Oyanagi E, Yano H, Uchida M, Utsumi K, Sasaki J. Protective action of L-carnitine on cardiac mitochondrial function and structure against fatty acid stress. Biochem Biophys Res Commun. 2011 Aug 19;412(1):61-7. doi: 10.1016/j.bbrc.2011.07.039[↩]
- Haghighatdoost F, Jabbari M, Hariri M. The effect of L-carnitine on inflammatory mediators: a systematic review and meta-analysis of randomized clinical trials. Eur J Clin Pharmacol. 2019 Aug;75(8):1037-1046. doi: 10.1007/s00228-019-02666-5[↩]
- DiNicolantonio JJ, McCarty M, OKeefe J. Association of moderately elevated trimethylamine N-oxide with cardiovascular risk: is TMAO serving as a marker for hepatic insulin resistance. Open Heart. 2019 Feb 27;6(1):e000890. doi: 10.1136/openhrt-2018-000890[↩]
- Song X, Qu H, Yang Z, Rong J, Cai W, Zhou H. Efficacy and Safety of L-Carnitine Treatment for Chronic Heart Failure: A Meta-Analysis of Randomized Controlled Trials. Biomed Res Int. 2017;2017:6274854. doi: 10.1155/2017/6274854[↩][↩][↩]
- Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, Britt EB, Fu X, Wu Y, Li L, Smith JD, DiDonato JA, Chen J, Li H, Wu GD, Lewis JD, Warrier M, Brown JM, Krauss RM, Tang WH, Bushman FD, Lusis AJ, Hazen SL. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013 May;19(5):576-85. doi: 10.1038/nm.3145[↩][↩][↩][↩]
- Johri AM, Hétu MF, Heyland DK, Herr JE, Korol J, Froese S, Norman PA, Day AG, Matangi MF, Michos ED, LaHaye SA, Saunders FW, Spence JD. Progression of atherosclerosis with carnitine supplementation: a randomized controlled trial in the metabolic syndrome. Nutr Metab (Lond). 2022 Apr 2;19(1):26. doi: 10.1186/s12986-022-00661-9[↩][↩][↩][↩]
- Campia U, Gerhard-Herman M, Piazza G, Goldhaber SZ. Peripheral Artery Disease: Past, Present, and Future. Am J Med. 2019 Oct;132(10):1133-1141. doi: 10.1016/j.amjmed.2019.04.043[↩]
- Morley RL, Sharma A, Horsch AD, Hinchliffe RJ. Peripheral artery disease. BMJ. 2018 Feb 1;360:j5842. doi: 10.1136/bmj.j5842[↩]
- Tama B, Fabara SP, Zarrate D, Anas Sohail A. Effectiveness of Propionyl-L-Carnitine Supplementation on Exercise Performance in Intermittent Claudication: A Systematic Review. Cureus. 2021 Aug 31;13(8):e17592. doi: 10.7759/cureus.17592[↩][↩]
- Davini P, Bigalli A, Lamanna F, Boem A. Controlled study on L-carnitine therapeutic efficacy in post-infarction. Drugs Exp Clin Res. 1992;18(8):355-65.[↩]
- Xue YZ, Wang LX, Liu HZ, Qi XW, Wang XH, Ren HZ. L-carnitine as an adjunct therapy to percutaneous coronary intervention for non-ST elevation myocardial infarction. Cardiovasc Drugs Ther. 2007 Dec;21(6):445-8. doi: 10.1007/s10557-007-6056-9[↩]
- Iyer R, Gupta A, Khan A, Hiremath S, Lokhandwala Y. Does left ventricular function improve with L-carnitine after acute myocardial infarction? J Postgrad Med. 1999 Apr-Jun;45(2):38-41.[↩]
- Tarantini G, Scrutinio D, Bruzzi P, Boni L, Rizzon P, Iliceto S. Metabolic treatment with L-carnitine in acute anterior ST segment elevation myocardial infarction. A randomized controlled trial. Cardiology. 2006;106(4):215-23. doi: 10.1159/000093131[↩]
- Trupp RJ, Abraham WT. Congestive heart failure. In: Rakel RE, Bope ET, eds. Conn’s Current Therapy. 54th ed. New York: W.B. Sunders Company; 2002:306-313.[↩]
- Ruiz M, Labarthe F, Fortier A, Bouchard B, Thompson Legault J, Bolduc V, Rigal O, Chen J, Ducharme A, Crawford PA, Tardif JC, Des Rosiers C. Circulating acylcarnitine profile in human heart failure: a surrogate of fatty acid metabolic dysregulation in mitochondria and beyond. Am J Physiol Heart Circ Physiol. 2017 Oct 1;313(4):H768-H781. doi: 10.1152/ajpheart.00820.2016[↩]
- Ueland T, Svardal A, Øie E, Askevold ET, Nymoen SH, Bjørndal B, Dahl CP, Gullestad L, Berge RK, Aukrust P. Disturbed carnitine regulation in chronic heart failure–increased plasma levels of palmitoyl-carnitine are associated with poor prognosis. Int J Cardiol. 2013 Sep 1;167(5):1892-9. doi: 10.1016/j.ijcard.2012.04.150[↩]
- Yoshihisa A, Watanabe S, Yokokawa T, Misaka T, Sato T, Suzuki S, Oikawa M, Kobayashi A, Takeishi Y. Associations between acylcarnitine to free carnitine ratio and adverse prognosis in heart failure patients with reduced or preserved ejection fraction. ESC Heart Fail. 2017 Aug;4(3):360-364. doi: 10.1002/ehf2.12176[↩]
- What Is Angina? https://www.nhlbi.nih.gov/health/angina[↩]
- Strand E, Pedersen ER, Svingen GF, Olsen T, Bjørndal B, Karlsson T, Dierkes J, Njølstad PR, Mellgren G, Tell GS, Berge RK, Svardal A, Nygård O. Serum Acylcarnitines and Risk of Cardiovascular Death and Acute Myocardial Infarction in Patients With Stable Angina Pectoris. J Am Heart Assoc. 2017 Feb 3;6(2):e003620. doi: 10.1161/JAHA.116.003620[↩]
- Cacciatore L, Cerio R, Ciarimboli M, Cocozza M, Coto V, D’Alessandro A, D’Alessandro L, Grattarola G, Imparato L, Lingetti M, et al. The therapeutic effect of L-carnitine in patients with exercise-induced stable angina: a controlled study. Drugs Exp Clin Res. 1991;17(4):225-35.[↩]
- Cherchi A, Lai C, Angelino F, Trucco G, Caponnetto S, Mereto PE, Rosolen G, Manzoli U, Schiavoni G, Reale A, et al. Effects of L-carnitine on exercise tolerance in chronic stable angina: a multicenter, double-blind, randomized, placebo controlled crossover study. Int J Clin Pharmacol Ther Toxicol. 1985 Oct;23(10):569-72.[↩]
- Iyer RN, Khan AA, Gupta A, Vajifdar BU, Lokhandwala YY. L-carnitine moderately improves the exercise tolerance in chronic stable angina. J Assoc Physicians India. 2000 Nov;48(11):1050-2.[↩]
- Bartels GL, Remme WJ, Pillay M, Schönfeld DH, Kruijssen DA. Effects of L-propionylcarnitine on ischemia-induced myocardial dysfunction in men with angina pectoris. Am J Cardiol. 1994 Jul 15;74(2):125-30. doi: 10.1016/0002-9149(94)90084-1[↩][↩]
- Mingrone G. Carnitine in type 2 diabetes. Ann N Y Acad Sci. 2004 Nov;1033:99-107. doi: 10.1196/annals.1320.009[↩]
- Vidal-Casariego A, Burgos-Peláez R, Martínez-Faedo C, Calvo-Gracia F, Valero-Zanuy MÁ, Luengo-Pérez LM, Cuerda-Compés C. Metabolic effects of L-carnitine on type 2 diabetes mellitus: systematic review and meta-analysis. Exp Clin Endocrinol Diabetes. 2013 Apr;121(4):234-8. doi: 10.1055/s-0033-1333688[↩][↩]
- Sangwung P, Petersen KF, Shulman GI, Knowles JW. Mitochondrial Dysfunction, Insulin Resistance, and Potential Genetic Implications. Endocrinology. 2020 Apr 1;161(4):bqaa017. doi: 10.1210/endocr/bqaa017[↩]
- Yazıcı D, Sezer H. Insulin Resistance, Obesity and Lipotoxicity. Adv Exp Med Biol. 2017;960:277-304. doi: 10.1007/978-3-319-48382-5_12[↩]
- Zamani M, Pahlavani N, Nikbaf-Shandiz M, Rasaei N, Ghaffarian-Ensaf R, Asbaghi O, Shiraseb F, Rastgoo S. The effects of L-carnitine supplementation on glycemic markers in adults: A systematic review and dose-response meta-analysis. Front Nutr. 2023 Jan 10;9:1082097. doi: 10.3389/fnut.2022.1082097[↩][↩]
- Xu Y, Jiang W, Chen G, Zhu W, Ding W, Ge Z, Tan Y, Ma T, Cui G. L-carnitine treatment of insulin resistance: A systematic review and meta-analysis. Adv Clin Exp Med. 2017 Mar-Apr;26(2):333-338. doi: 10.17219/acem/61609[↩][↩][↩]
- Ringseis R, Keller J, Eder K. Mechanisms underlying the anti-wasting effect of L-carnitine supplementation under pathologic conditions: evidence from experimental and clinical studies. Eur J Nutr. 2013 Aug;52(5):1421-42. doi: 10.1007/s00394-013-0511-0[↩][↩]
- Asadi M, Rahimlou M, Shishehbor F, Mansoori A. The effect of l-carnitine supplementation on lipid profile and glycaemic control in adults with cardiovascular risk factors: A systematic review and meta-analysis of randomized controlled clinical trials. Clin Nutr. 2020 Jan;39(1):110-122. doi: 10.1016/j.clnu.2019.01.020[↩]
- Parvanova A, Trillini M, Podestà MA, Iliev IP, Aparicio C, Perna A, Peraro F, Rubis N, Gaspari F, Cannata A, Ferrari S, Bossi AC, Trevisan R, Parameswaran S, Chávez-Iñiguez JS, Masnic F, Seck SM, Jiamjariyaporn T, Cortinovis M, Perico L, Sharma K, Remuzzi G, Ruggenenti P, Warnock DG. Blood Pressure and Metabolic Effects of Acetyl-l-Carnitine in Type 2 Diabetes: DIABASI Randomized Controlled Trial. J Endocr Soc. 2018 Mar 22;2(5):420-436. doi: 10.1210/js.2017-00426[↩][↩]
- Skoracka K, Eder P, Łykowska-Szuber L, Dobrowolska A, Krela-Kaźmierczak I. Diet and Nutritional Factors in Male (In)fertility-Underestimated Factors. J Clin Med. 2020 May 9;9(5):1400. doi: 10.3390/jcm9051400[↩]
- Agarwal A, Sengupta P, Durairajanayagam D. Role of L-carnitine in female infertility. Reprod Biol Endocrinol. 2018 Jan 26;16(1):5. doi: 10.1186/s12958-018-0323-4[↩]
- Salas-Huetos A, Rosique-Esteban N, Becerra-Tomás N, Vizmanos B, Bulló M, Salas-Salvadó J. The Effect of Nutrients and Dietary Supplements on Sperm Quality Parameters: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Adv Nutr. 2018 Nov 1;9(6):833-848. doi: 10.1093/advances/nmy057[↩][↩]
- de Ligny W, Smits RM, Mackenzie-Proctor R, Jordan V, Fleischer K, de Bruin JP, Showell MG. Antioxidants for male subfertility. Cochrane Database Syst Rev. 2022 May 4;5(5):CD007411. doi: 10.1002/14651858.CD007411.pub5[↩][↩][↩]
- Ismail AM, Hamed AH, Saso S, Thabet HH. Adding L-carnitine to clomiphene resistant PCOS women improves the quality of ovulation and the pregnancy rate. A randomized clinical trial. Eur J Obstet Gynecol Reprod Biol. 2014 Sep;180:148-52. doi: 10.1016/j.ejogrb.2014.06.008. Epub 2014 Jun 23. Retraction in: Eur J Obstet Gynecol Reprod Biol. 2023 Dec;291:22. doi: 10.1016/j.ejogrb.2023.09.028[↩]
- El Sharkwy I, Sharaf El-Din M. l-Carnitine plus metformin in clomiphene-resistant obese PCOS women, reproductive and metabolic effects: a randomized clinical trial. Gynecol Endocrinol. 2019 Aug;35(8):701-705. doi: 10.1080/09513590.2019.1576622. Epub 2019 Feb 26. Retraction in: Gynecol Endocrinol. 2024 Dec;40(1):2419767. doi: 10.1080/09513590.2024.2419767[↩][↩]
- Showell MG, Mackenzie-Proctor R, Jordan V, Hart RJ. Antioxidants for female subfertility. Cochrane Database Syst Rev. 2017 Jul 28;7(7):CD007807. doi: 10.1002/14651858.CD007807.pub3. Update in: Cochrane Database Syst Rev. 2020 Aug 27;8:CD007807. doi: 10.1002/14651858.CD007807.pub4[↩][↩]
- Baghban F, Hosseinzadeh M, Mozaffari-Khosravi H, Dehghan A, Fallahzadeh H. The effect of L-Carnitine supplementation on clinical symptoms, C-reactive protein and malondialdehyde in obese women with knee osteoarthritis: a double blind randomized controlled trial. BMC Musculoskelet Disord. 2021 Feb 17;22(1):195. doi: 10.1186/s12891-021-04059-1[↩][↩][↩][↩]
- Tootsi K, Kals J, Zilmer M, Paapstel K, Ottas A, Märtson A. Medium- and long-chain acylcarnitines are associated with osteoarthritis severity and arterial stiffness in end-stage osteoarthritis patients: a case-control study. Int J Rheum Dis. 2018 Jun;21(6):1211-1218. doi: 10.1111/1756-185X.13251[↩]
- Liu X, Machado GC, Eyles JP, Ravi V, Hunter DJ. Dietary supplements for treating osteoarthritis: a systematic review and meta-analysis. Br J Sports Med. 2018 Feb;52(3):167-175. doi: 10.1136/bjsports-2016-097333[↩]
- Malek Mahdavi A, Mahdavi R, Kolahi S. Effects of l-Carnitine Supplementation on Serum Inflammatory Factors and Matrix Metalloproteinase Enzymes in Females with Knee Osteoarthritis: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. J Am Coll Nutr. 2016 Sep-Oct;35(7):597-603. doi: 10.1080/07315724.2015.1068139[↩][↩]
- Peeling P, Binnie MJ, Goods PSR, Sim M, Burke LM. Evidence-Based Supplements for the Enhancement of Athletic Performance. Int J Sport Nutr Exerc Metab. 2018 Mar 1;28(2):178-187. doi: 10.1123/ijsnem.2017-0343[↩]
- Wall BT, Stephens FB, Constantin-Teodosiu D, Marimuthu K, Macdonald IA, Greenhaff PL. Chronic oral ingestion of L-carnitine and carbohydrate increases muscle carnitine content and alters muscle fuel metabolism during exercise in humans. J Physiol. 2011 Feb 15;589(Pt 4):963-73. doi: 10.1113/jphysiol.2010.201343[↩][↩]
- Novakova K, Kummer O, Bouitbir J, Stoffel SD, Hoerler-Koerner U, Bodmer M, Roberts P, Urwyler A, Ehrsam R, Krähenbühl S. Effect of L-carnitine supplementation on the body carnitine pool, skeletal muscle energy metabolism and physical performance in male vegetarians. Eur J Nutr. 2016 Feb;55(1):207-17. doi: 10.1007/s00394-015-0838-9[↩][↩]
- Fielding R, Riede L, Lugo JP, Bellamine A. l-Carnitine Supplementation in Recovery after Exercise. Nutrients. 2018 Mar 13;10(3):349. doi: 10.3390/nu10030349. Erratum in: Nutrients. 2018 Apr 26;10(5):E541. doi: 10.3390/nu10050541[↩][↩][↩]
- Mielgo-Ayuso J, Pietrantonio L, Viribay A, Calleja-González J, González-Bernal J, Fernández-Lázaro D. Effect of Acute and Chronic Oral l-Carnitine Supplementation on Exercise Performance Based on the Exercise Intensity: A Systematic Review. Nutrients. 2021 Dec 3;13(12):4359. doi: 10.3390/nu13124359[↩][↩]
- Pooyandjoo M, Nouhi M, Shab-Bidar S, Djafarian K, Olyaeemanesh A. The effect of (L-)carnitine on weight loss in adults: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2016 Oct;17(10):970-6. doi: 10.1111/obr.12436[↩][↩][↩]
- Derosa G, Maffioli P, Ferrari I, D’Angelo A, Fogari E, Palumbo I, Randazzo S, Cicero AF. Orlistat and L-carnitine compared to orlistat alone on insulin resistance in obese diabetic patients. Endocr J. 2010;57(9):777-86. doi: 10.1507/endocrj.k10e-049[↩]
- Derosa G, Cicero AF, Gaddi A, Mugellini A, Ciccarelli L, Fogari R. The effect of L-carnitine on plasma lipoprotein(a) levels in hypercholesterolemic patients with type 2 diabetes mellitus. Clin Ther. 2003 May;25(5):1429-39. doi: 10.1016/s0149-2918(03)80130-3[↩]
- Campone M, Berton-Rigaud D, Joly-Lobbedez F, Baurain JF, Rolland F, Stenzl A, Fabbro M, van Dijk M, Pinkert J, Schmelter T, de Bont N, Pautier P. A double-blind, randomized phase II study to evaluate the safety and efficacy of acetyl-L-carnitine in the prevention of sagopilone-induced peripheral neuropathy. Oncologist. 2013;18(11):1190-1. doi: 10.1634/theoncologist.2013-0061[↩][↩]
- Hershman DL, Unger JM, Crew KD, Minasian LM, Awad D, Moinpour CM, Hansen L, Lew DL, Greenlee H, Fehrenbacher L, Wade JL 3rd, Wong SF, Hortobagyi GN, Meyskens FL, Albain KS. Randomized double-blind placebo-controlled trial of acetyl-L-carnitine for the prevention of taxane-induced neuropathy in women undergoing adjuvant breast cancer therapy. J Clin Oncol. 2013 Jul 10;31(20):2627-33. doi: 10.1200/JCO.2012.44.8738[↩]
- Hershman DL, Unger JM, Crew KD, Till C, Greenlee H, Minasian LM, Moinpour CM, Lew DL, Fehrenbacher L, Wade JL 3rd, Wong SF, Fisch MJ, Lynn Henry N, Albain KS. Two-Year Trends of Taxane-Induced Neuropathy in Women Enrolled in a Randomized Trial of Acetyl-L-Carnitine (SWOG S0715). J Natl Cancer Inst. 2018 Jun 1;110(6):669-676. doi: 10.1093/jnci/djx259[↩]
- Sun Y, Shu Y, Liu B, Liu P, Wu C, Zheng R, Zhang X, Zhuang Z, Deng Y, Zheng L, Xu Q, Jiang B, Ouyang X, Gao J, Xu N, Li X, Jiang S, Liang C, Yao Y. A prospective study to evaluate the efficacy and safety of oral acetyl-L-carnitine for the treatment of chemotherapy-induced peripheral neuropathy. Exp Ther Med. 2016 Dec;12(6):4017-4024. doi: 10.3892/etm.2016.3871[↩][↩]
- van Dam DG, Beijers AJ, Vreugdenhil G. Acetyl-L-carnitine undervalued in the treatment of chemotherapy-induced peripheral neuropathy? Acta Oncol. 2016 Dec;55(12):1495-1497. doi: 10.1080/0284186X.2016.1220678[↩]
- Tesfaye S, Selvarajah D. Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes Metab Res Rev. 2012 Feb;28 Suppl 1:8-14. doi: 10.1002/dmrr.2239[↩]
- Dy SM, Bennett WL, Sharma R, et al. Preventing Complications and Treating Symptoms of Diabetic Peripheral Neuropathy [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2017 Mar. (Comparative Effectiveness Reviews, No. 187.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK442335[↩]
- Rolim LC, da Silva EM, Flumignan RL, Abreu MM, Dib SA. Acetyl-L-carnitine for the treatment of diabetic peripheral neuropathy. Cochrane Database Syst Rev. 2019 Jun 15;6(6):CD011265. doi: 10.1002/14651858.CD011265.pub2[↩]
- Sima AA, Calvani M, Mehra M, Amato A; Acetyl-L-Carnitine Study Group. Acetyl-L-carnitine improves pain, nerve regeneration, and vibratory perception in patients with chronic diabetic neuropathy: an analysis of two randomized placebo-controlled trials. Diabetes Care. 2005 Jan;28(1):89-94. doi: 10.2337/diacare.28.1.89[↩]
- Li S, Chen X, Li Q, Du J, Liu Z, Peng Y, Xu M, Li Q, Lei M, Wang C, Zheng S, Zhang X, Yu H, Shi J, Tao S, Feng P, Tian H. Effects of acetyl-L-carnitine and methylcobalamin for diabetic peripheral neuropathy: A multicenter, randomized, double-blind, controlled trial. J Diabetes Investig. 2016 Sep;7(5):777-85. doi: 10.1111/jdi.12493[↩]
- Margolis AM, Heverling H, Pham PA, Stolbach A. A review of the toxicity of HIV medications. J Med Toxicol. 2014 Mar;10(1):26-39. doi: 10.1007/s13181-013-0325-8[↩]
- Moyle GJ, Sadler M. Peripheral neuropathy with nucleoside antiretrovirals: risk factors, incidence and management. Drug Saf. 1998 Dec;19(6):481-94. doi: 10.2165/00002018-199819060-00005[↩]
- Scarpini E, Sacilotto G, Baron P, Cusini M, Scarlato G. Effect of acetyl-L-carnitine in the treatment of painful peripheral neuropathies in HIV+ patients. J Peripher Nerv Syst. 1997;2(3):250-2.[↩]
- Hart AM, Wilson AD, Montovani C, Smith C, Johnson M, Terenghi G, Youle M. Acetyl-l-carnitine: a pathogenesis based treatment for HIV-associated antiretroviral toxic neuropathy. AIDS. 2004 Jul 23;18(11):1549-60. doi: 10.1097/01.aids.0000131354.14408.fb[↩]
- Herzmann C, Johnson MA, Youle M. Long-term effect of acetyl-L-carnitine for antiretroviral toxic neuropathy. HIV Clin Trials. 2005 Nov-Dec;6(6):344-50. doi: 10.1310/CH1N-YBNU-G3CU-JBXR[↩]
- Osio M, Muscia F, Zampini L, Nascimbene C, Mailland E, Cargnel A, Mariani C. Acetyl-l-carnitine in the treatment of painful antiretroviral toxic neuropathy in human immunodeficiency virus patients: an open label study. J Peripher Nerv Syst. 2006 Mar;11(1):72-6. doi: 10.1111/j.1085-9489.2006.00066.x[↩]
- Valcour V, Yeh TM, Bartt R, Clifford D, Gerschenson M, Evans SR, Cohen BA, Ebenezer GJ, Hauer P, Millar L, Gould M, Tran P, Shikuma C, Souza S, McArthur JC; AIDS Clinical Trials Group (ACTG) 5157 protocol team. Acetyl-l-carnitine and nucleoside reverse transcriptase inhibitor-associated neuropathy in HIV infection. HIV Med. 2009 Feb;10(2):103-10. doi: 10.1111/j.1468-1293.2008.00658.x[↩]
- Youle M, Osio M; ALCAR Study Group. A double-blind, parallel-group, placebo-controlled, multicentre study of acetyl L-carnitine in the symptomatic treatment of antiretroviral toxic neuropathy in patients with HIV-1 infection. HIV Med. 2007 May;8(4):241-50. doi: 10.1111/j.1468-1293.2007.00467.x[↩]
- Hatanaka Y, Higuchi T, Akiya Y, Horikami T, Tei R, Furukawa T, Takashima H, Tomita H, Abe M. Prevalence of Carnitine Deficiency and Decreased Carnitine Levels in Patients on Hemodialysis. Blood Purif. 2019;47 Suppl 2:38-44. doi: 10.1159/000496720[↩]
- Kalim S, Clish CB, Wenger J, Elmariah S, Yeh RW, Deferio JJ, Pierce K, Deik A, Gerszten RE, Thadhani R, Rhee EP. A plasma long-chain acylcarnitine predicts cardiovascular mortality in incident dialysis patients. J Am Heart Assoc. 2013 Dec 5;2(6):e000542. doi: 10.1161/JAHA.113.000542[↩]
- Chen Y, Abbate M, Tang L, Cai G, Gong Z, Wei R, Zhou J, Chen X. L-Carnitine supplementation for adults with end-stage kidney disease requiring maintenance hemodialysis: a systematic review and meta-analysis. Am J Clin Nutr. 2014 Feb;99(2):408-22. doi: 10.3945/ajcn.113.062802. Epub 2013 Dec 24. Erratum in: Am J Clin Nutr. 2014 May;99(5):1143.[↩][↩]
- Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis. 2000 Jun;35(6 Suppl 2):S17-S104. doi: 10.1053/ajkd.2000.v35.aajkd03517. Erratum in: Am J Kidney Dis 2001 Oct;38(4):917.[↩]
- KDOQI; National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Anemia in Chronic Kidney Disease. Am J Kidney Dis. 2006 May;47(5 Suppl 3):S11-145. doi: 10.1053/j.ajkd.2006.03.010. Erratum in: Am J Kidney Dis. 2006 Sep;48(3):518.[↩]
- Veronese N, Stubbs B, Solmi M, Ajnakina O, Carvalho AF, Maggi S. Acetyl-L-Carnitine Supplementation and the Treatment of Depressive Symptoms: A Systematic Review and Meta-Analysis. Psychosom Med. 2018 Feb/Mar;80(2):154-159. doi: 10.1097/PSY.0000000000000537[↩][↩]
- Meister R, von Wolff A, Mohr H, Härter M, Nestoriuc Y, Hölzel L, Kriston L. Comparative Safety of Pharmacologic Treatments for Persistent Depressive Disorder: A Systematic Review and Network Meta-Analysis. PLoS One. 2016 May 17;11(5):e0153380. doi: 10.1371/journal.pone.0153380[↩]
- Wijdicks EF. Hepatic Encephalopathy. N Engl J Med. 2016 Oct 27;375(17):1660-1670. doi: 10.1056/NEJMra1600561[↩][↩]
- Inglis JE, Lin PJ, Kerns SL, Kleckner IR, Kleckner AS, Castillo DA, Mustian KM, Peppone LJ. Nutritional Interventions for Treating Cancer-Related Fatigue: A Qualitative Review. Nutr Cancer. 2019;71(1):21-40. doi: 10.1080/01635581.2018.1513046[↩]
- Marx W, Teleni L, Opie RS, Kelly J, Marshall S, Itsiopoulos C, Isenring E. Efficacy and Effectiveness of Carnitine Supplementation for Cancer-Related Fatigue: A Systematic Literature Review and Meta-Analysis. Nutrients. 2017 Nov 7;9(11):1224. doi: 10.3390/nu9111224[↩][↩]
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004 Mar;59(3):255-63. doi: 10.1093/gerona/59.3.m255[↩]
- Vermeiren S, Vella-Azzopardi R, Beckwée D, Habbig AK, Scafoglieri A, Jansen B, Bautmans I; Gerontopole Brussels Study group. Frailty and the Prediction of Negative Health Outcomes: A Meta-Analysis. J Am Med Dir Assoc. 2016 Dec 1;17(12):1163.e1-1163.e17. doi: 10.1016/j.jamda.2016.09.010[↩]
- Crentsil V. Mechanistic contribution of carnitine deficiency to geriatric frailty. Ageing Res Rev. 2010 Jul;9(3):265-8. doi: 10.1016/j.arr.2010.02.005[↩]
- Badrasawi M, Shahar S, Zahara AM, Nor Fadilah R, Singh DK. Efficacy of L-carnitine supplementation on frailty status and its biomarkers, nutritional status, and physical and cognitive function among prefrail older adults: a double-blind, randomized, placebo-controlled clinical trial. Clin Interv Aging. 2016 Nov 17;11:1675-1686. doi: 10.2147/CIA.S113287[↩]
- Dhillon RJ, Hasni S. Pathogenesis and Management of Sarcopenia. Clin Geriatr Med. 2017 Feb;33(1):17-26. doi: 10.1016/j.cger.2016.08.002[↩]
- Ebadi M, Montano-Loza AJ. Clinical relevance of skeletal muscle abnormalities in patients with cirrhosis. Dig Liver Dis. 2019 Nov;51(11):1493-1499. doi: 10.1016/j.dld.2019.05.034[↩]
- Kim SH, Shin MJ, Shin YB, Kim KU. Sarcopenia Associated with Chronic Obstructive Pulmonary Disease. J Bone Metab. 2019 May;26(2):65-74. doi: 10.11005/jbm.2019.26.2.65[↩]
- Melenovsky V, Hlavata K, Sedivy P, Dezortova M, Borlaug BA, Petrak J, Kautzner J, Hajek M. Skeletal Muscle Abnormalities and Iron Deficiency in Chronic Heart FailureAn Exercise 31P Magnetic Resonance Spectroscopy Study of Calf Muscle. Circ Heart Fail. 2018 Sep;11(9):e004800. doi: 10.1161/CIRCHEARTFAILURE.117.004800[↩]
- Sawicka AK, Hartmane D, Lipinska P, Wojtowicz E, Lysiak-Szydlowska W, Olek RA. l-Carnitine Supplementation in Older Women. A Pilot Study on Aging Skeletal Muscle Mass and Function. Nutrients. 2018 Feb 23;10(2):255. doi: 10.3390/nu10020255[↩]
- Ohara M, Ogawa K, Suda G, Kimura M, Maehara O, Shimazaki T, Suzuki K, Nakamura A, Umemura M, Izumi T, Kawagishi N, Nakai M, Sho T, Natsuizaka M, Morikawa K, Ohnishi S, Sakamoto N. L-Carnitine Suppresses Loss of Skeletal Muscle Mass in Patients With Liver Cirrhosis. Hepatol Commun. 2018 Aug 6;2(8):906-918. doi: 10.1002/hep4.1207[↩][↩]
- Nakanishi H, Kurosaki M, Tsuchiya K, Nakakuki N, Takada H, Matsuda S, Gondo K, Asano Y, Hattori N, Tamaki N, Suzuki S, Yasui Y, Hosokawa T, Itakura J, Takahashi Y, Izumi N. L-carnitine Reduces Muscle Cramps in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2015 Aug;13(8):1540-3. doi: 10.1016/j.cgh.2014.12.005[↩]
- Hiraoka A, Kiguchi D, Ninomiya T, Hirooka M, Abe M, Matsuura B, Hiasa Y, Michitaka K. Can L-carnitine supplementation and exercise improve muscle complications in patients with liver cirrhosis who receive branched-chain amino acid supplementation? Eur J Gastroenterol Hepatol. 2019 Jul;31(7):878-884. doi: 10.1097/MEG.0000000000001368[↩]
- Imbe A, Tanimoto K, Inaba Y, Sakai S, Shishikura K, Imbe H, Tanimoto Y, Terasaki J, Imagawa A, Hanafusa T. Effects of L-carnitine supplementation on the quality of life in diabetic patients with muscle cramps. Endocr J. 2018 May 28;65(5):521-526. doi: 10.1507/endocrj.EJ17-0431[↩]
- Lynch KE, Feldman HI, Berlin JA, Flory J, Rowan CG, Brunelli SM. Effects of L-carnitine on dialysis-related hypotension and muscle cramps: a meta-analysis. Am J Kidney Dis. 2008 Nov;52(5):962-71. doi: 10.1053/j.ajkd.2008.05.031[↩]
- Sawicka, A.K., Renzi, G. & Olek, R.A. The bright and the dark sides of L-carnitine supplementation: a systematic review. J Int Soc Sports Nutr 17, 49 (2020). https://doi.org/10.1186/s12970-020-00377-2[↩]
- Rebouche C.J. Carnitine. In: Shils M.E., Olson J.A., Shike M., Ross A.C., editors. Modern Nutrition in Health and Disease. 9th ed. Lippincott Williams & Wilkins; New York, NY, USA: 1999. pp. 505–512.[↩]
- Alesci S., Manoli I., Costello R., Coates P., Gold P.W., Chrousos G.P., Blackman M.R. Carnitine: Lessons from one hundred years of research. Ann. N. Y. Acad. Sci. 2004;1033:ix–xi.[↩]
- Zeiler FA, Sader N, Gillman LM, West M. Levocarnitine induced seizures in patients on valproic acid: A negative systematic review. Seizure. 2016 Mar;36:36-39. doi: 10.1016/j.seizure.2016.01.020[↩]
- Buffa JA, Romano KA, Copeland MF, et al. The microbial gbu gene cluster links cardiovascular disease risk associated with red meat consumption to microbiota L-carnitine catabolism. Nat Microbiol. 2022 Jan;7(1):73-86. doi: 10.1038/s41564-021-01010-x[↩]
- Skagen K, Trøseid M, Ueland T, Holm S, Abbas A, Gregersen I, Kummen M, Bjerkeli V, Reier-Nilsen F, Russell D, Svardal A, Karlsen TH, Aukrust P, Berge RK, Hov JE, Halvorsen B, Skjelland M. The Carnitine-butyrobetaine-trimethylamine-N-oxide pathway and its association with cardiovascular mortality in patients with carotid atherosclerosis. Atherosclerosis. 2016 Apr;247:64-9. doi: 10.1016/j.atherosclerosis.2016.01.033[↩]
- Yang S, Li X, Yang F, Zhao R, Pan X, Liang J, Tian L, Li X, Liu L, Xing Y, Wu M. Gut Microbiota-Dependent Marker TMAO in Promoting Cardiovascular Disease: Inflammation Mechanism, Clinical Prognostic, and Potential as a Therapeutic Target. Front Pharmacol. 2019 Nov 19;10:1360. doi: 10.3389/fphar.2019.01360[↩]
- Brass EP. Pivalate-generating prodrugs and carnitine homeostasis in man. Pharmacol Rev. 2002 Dec;54(4):589-98. doi: 10.1124/pr.54.4.589[↩]
- Okumura A, Numoto S, Iwayama H, Azuma Y, Kurahashi H. Carnitine supplementation prevents carnitine deficiency caused by pivalate-conjugated antibiotics in patients with epilepsy prescribed valproate. Epilepsy Behav. 2021 Apr;117:107883. doi: 10.1016/j.yebeh.2021.107883[↩]
- Hug G, McGraw CA, Bates SR, Landrigan EA. Reduction of serum carnitine concentrations during anticonvulsant therapy with phenobarbital, valproic acid, phenytoin, and carbamazepine in children. J Pediatr. 1991 Nov;119(5):799-802. doi: 10.1016/s0022-3476(05)80306-3[↩]
- Castro-Gago M, Eirís-Puñal J, Novo-Rodríguez MI, Couceiro J, Camiña F, Rodríguez-Segade S. Serum carnitine levels in epileptic children before and during treatment with valproic acid, carbamazepine, and phenobarbital. J Child Neurol. 1998 Nov;13(11):546-9. doi: 10.1177/088307389801301104[↩]
- Verrotti A, Greco R, Morgese G, Chiarelli F. Carnitine deficiency and hyperammonemia in children receiving valproic acid with and without other anticonvulsant drugs. Int J Clin Lab Res. 1999;29(1):36-40. doi: 10.1007/s005990050060[↩][↩]
- Kobayashi H, Fukuda S, Yamada K, Hasegawa Y, Takahashi T, Purevsuren J, Yamaguchi S. Clinical Features of Carnitine Deficiency Secondary to Pivalate-Conjugated Antibiotic Therapy. J Pediatr. 2016 Jun;173:183-7. doi: 10.1016/j.jpeds.2016.02.080[↩]
- Lheureux PE, Hantson P. Carnitine in the treatment of valproic acid-induced toxicity. Clin Toxicol (Phila). 2009 Feb;47(2):101-11. doi: 10.1080/15563650902752376[↩]
- Perrott J, Murphy NG, Zed PJ. L-carnitine for acute valproic acid overdose: a systematic review of published cases. Ann Pharmacother. 2010 Jul-Aug;44(7-8):1287-93. doi: 10.1345/aph.1P135[↩]





{kind=link}