
Contents
What are menstrual cramps
Many women will experience some form of pain during their period (painful menstruation or dysmenorrhea) – in fact most women experience menstrual cramps at some point in their lives 1 and one of the most common causes of pelvic pain 2. Dysmenorrhea is defined as a painful, cramping sensation in the lower abdomen (painful muscle cramps) or back associated with menstrual periods 3. The pain sometimes comes in intense spasms, while at other times it may be dull but more constant. Menstrual cramps may also vary with each monthly period. Some periods may cause little or no discomfort, while others may be more painful. Symptoms typically begin in adolescence and may lead to school and work absenteeism, as well as limitations on social, academic, and sports activities 4.
Sometimes you may experience pelvic pain even when you don’t have your period.
Painful menstruation is very common in young women, and the pain often tends to ease as you get older 5. Typical menstruation in adolescence includes pain (93%), cramping (71%), premenstrual symptoms (96%) and mood disturbance (73%) 6.
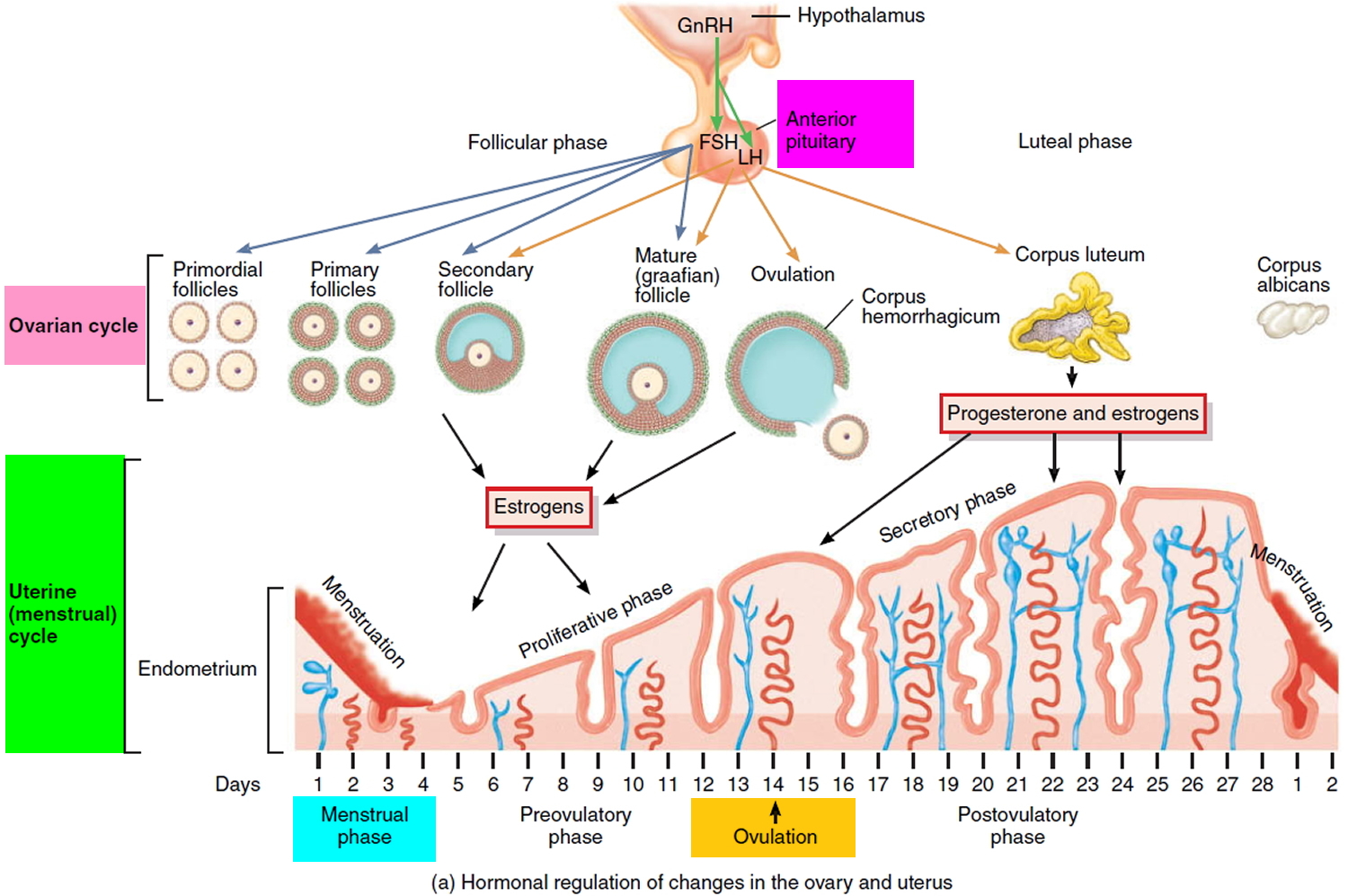
Figure 1. Menstrual cycle
Teenage girls with menstrual pain regularly present to their doctors. The experience of pain with menstruation is common for 70–91% of teenagers 7. Also, there are a number of physical, psychological and emotional symptoms that occur premenstrually and during menstruation, which are reported by 96% of teenagers 8. Menstrual pain and symptoms cause school absence in 14–51% of teenagers 9, and interference with life activities for 15–59% 10.
Severe menstrual pain has been reported to occur in 14–23% of teenagers 11.
In those reporting severe pain there is a higher rate for school absences, which may be as high as 50–54% 11.
Endometriosis has been reported in 47–73% of adolescent girls with severe menstrual or pelvic pain with no response to non-steroidal anti-inflammatory drugs (NSAIDs) or the oral contraceptive pill (OCP) 12. A number of teenage girls presenting to physicians with menstrual pain will be suffering from endometriosis and take a median of 12.1 years to obtain a diagnosis if aged ≤19 years, in comparison with women aged ≥30 years who will take 3.3 years to be diagnosed 13. In that time, the disease may prolong their studies, disrupt their career, affect their relationships, interfere with sexual function, cause infertility and lead to bowel, bladder or ureteric complications.
As a result of the overlap between dysmenorrheic, premenstrual and some endometriosis symptoms there is difficulty distinguishing normal pain and symptoms from those that result from pathological disease. Although there is a continuing misconception that teenagers rarely have endometriosis the disease is increasingly being diagnosed in teenagers 14. An accurate non-invasive diagnostic tool is not yet available.
‘Typical’ menstruation may be characterised by mild to moderate pain managed with analgesia, low interference with life activities, minimal school absence and manageable menstrual symptoms. Minimal treatment is required.
Moderate–severe menstrual cramps is defined as multiple menstrual symptoms; school absence; and high interference with life activities.
Treatment could involve optimizing first-line conservative measures, including the effective use of simple analgesics, such as NSAIDs with or without paracetamol (acetaminophen) in combination, and with or without hormonal medication. Lifestyle factors may be modified, such as diet and optimizing bowel function, exercise and sleep patterns. Recording the frequency and intensity of pain and symptoms with a menstrual and symptom chart may add further information, including symptom patterns and the effectiveness of some interventions.
Further investigation is required if symptoms are suggestive of endometriosis, that is, severe menstrual cramps that may include bowel or bladder, dyspareunia (painful sex), poor response to simple analgesia and/or hormonal medication, and significant interference with life activities. Adolescents with endometriosis may also present with acyclical menstrual pain 12.
The ultimate aim of treatment is for the restoration of full involvement in life activities. Protracted periods of unmanaged menstrual pain and interruption to life activities may cause depressive and anxiety symptoms, leading to further withdrawal from life activities. The repercussions of delayed diagnosis and under-management of symptoms on health-related quality of life are sufficiently documented 15.
Of note is that 15.5% of respondents reported menarche (first period) before the age of 12 years, and were likely to have been menstruating in primary school. This is similar to the UK study of 1166 girls aged 12–16 years, where 12% reported menarche before leaving primary school 16. Based on this knowledge, menstrual education including the management of menstrual pain and symptoms should be included in the senior primary school curriculum. Although uncommon, endometriosis has been found in young girls investigated for severe pelvic pain prior to menarche, but post thelarche (onset of female breast development) 17.
What does menstrual cramps feel like
Menstrual cramps are caused by menstruation, and most commonly cause a pain in the lower abdominal area. Sometimes this pain spreads towards the back and thigh areas.
The pain may feel like sharp twinges or a constant, dull pain. Everyone is different. Some women may not experience any menstrual cramps.
As well as the discomfort and aches, there are also a number of other symptoms that you may experience during your period, such as:
- headaches
- tiredness
- nausea
- dizziness
- diarrhea
- feeling faint.
All symptoms can vary each month and can usually be treated at home. If you find that any of these symptoms are very severe, you may want to contact your doctor.
How long does menstrual cramps last?
Menstrual cramps varies between women, although it’s most common to experience period pain at the beginning of your period, rather than during the middle or towards the end of it.
Some women don’t experience any period pain, while others may be in pain for the duration of their period and possibly before it starts and a few days after.
The pain normally lasts 48 to 72 hours, although it can last longer.
Since period pain is caused by the menstruation process, most women find that their pains are worst when their bleeding is at its heaviest.
Teenage girls often have period pain when they begin getting periods.
Menstrual cramps that doesn’t have an underlying cause tends to improve as a woman gets older. Many women also notice their period pains get better after they have given birth.
Home remedies for menstrual cramps
In most cases period pain is mild enough to treat at home.
Painkillers
You can take ibuprofen and aspirin to help manage your pain.
However, don’t take ibuprofen or aspirin if you have asthma or stomach, kidney or liver problems. Aspirin shouldn’t be given to anyone under 16 years of age.
You could also try paracetamol (acetaminophen), but studies have shown that it doesn’t reduce pain as effectively as ibuprofen or aspirin.
If ordinary painkillers are ineffective, your doctor may prescribe a stronger painkiller, such as naproxen or codeine.
You can help reduce menstrual cramps by trying the following:
- Stopping smoking – smoking is thought to increase the risk of period pain
- Gentle exercise, such as walking, swimming or cycling, is good to help ease the pain.
- Relaxation techniques, such as yoga or pilates, can help reduce your feelings of stress and tension. They can also increase your circulation and flexibility, help ease cramps, and improve sleep patterns.
- Apply a heat pad or hot water bottle to the painful area. Putting a heat pad or hot water bottle (wrapped in a tea towel) on your tummy may help reduce pain.
- Having a warm bath or shower. Taking a warm bath or shower can relieve pain and help you relax.
- Massage the painful area gently. Light, circular massage around your lower abdomen may also help reduce pain.
- Transcutaneous electronic nerve stimulation (TENS) – a small battery-operated device that delivers a mild electrical current to your tummy, which can help reduce pain.
When to see your doctor?
See your doctor if you have severe period pain or your normal pattern of periods changes – for example, if your periods become heavier than usual or irregular.
You should also see your doctor if you have symptoms of secondary dysmenorrhea (see description below for further detail), such as intense pain or heavy or painful periods.
Can period pain affect fertility?
Menstrual cramps that’s part of your normal menstrual cycle won’t affect your fertility. However, if the cause is an underlying condition, this may affect your fertility.
For example, endometriosis and pelvic inflammatory disease can cause scarring and a build-up of tissue in your fallopian tubes, making it harder for sperm to reach and fertilise an egg.
Uterine fibroids and adenomyosis can affect the womb and cause pain and heavy menstrual bleeding.
You should see your doctor if:
- you are 16 years or older and haven’t started to have periods
- your periods are getting heavier
- your periods get much closer together or further apart
- your periods have stopped and you’re not sure why
- you are bleeding in between periods or after sex
- you are bleeding after menopause
- you have severe period pain.
You can also talk to your doctor if, for any reason, your periods are affecting your wellbeing or enjoyment of life.
What is menstruation?
Menstruation is bleeding from the vagina that happens about once a month, as a normal part of the menstrual cycle. It is also known as having a period.
During this cycle, your hormones make the lining of the uterus become thicker, getting ready in case of pregnancy. Hormones also cause an egg to be released from an ovary, which is known as ovulation.
If you don’t become pregnant, then your periods starts about two weeks after ovulation. The lining of the uterus falls away and, along with some blood, flows out through the vagina. Periods can be light or heavy, and the blood can range from bright red to dark brown. You might also notice small clots.
Some women get symptoms leading up to and during menstruation, such as:
- cramps or pains low in the abdomen
- bloating or swelling in the abdomen
- constipation before your period
- diarrhea when your period starts
- acne
- tiredness.
When do periods typically start?
Girls have their first period during puberty. Most often, that is at age 12 or 13 years old, but girls can start menstruating as young as 9, or as late as 16.
What problems can women have with their periods?
Problems with periods can include:
- heavy bleeding
- period pain (also called dysmenorrhea)
- unpredictable or irregular periods
- premenstrual syndrome, or PMS, which makes some women feel irritable and sad.
When might periods stop?
Periods stop during pregnancy, and often while you are breastfeeding.
Some women find their periods stop for a time because of long-term illness, low body weight, stress, lots of strenuous exercise and hormone problems.
Some medications, such as contraceptives, might stop your period. This can be helpful for some women, especially if their periods are heavy or painful.
Sometimes after stopping the pill or other contraceptive, it can take a while for your periods to come back.
Periods stop altogether when women reach menopause – the average age is 51-52.
Types of menstrual cramps
There are two types of painful menstruation (also known as dysmenorrhea). These types are primary and secondary.
Primary dysmenorrhea
This is the common type of painful menstruation experienced by teenagers and young women where it is not due to other diseases and there is no underlying condition in the uterus (womb). Primary dysmenorrhea onset is typically six to 12 months after menarche (first period), with peak prevalence occurring in the late teens or early twenties.
It is not fully understood why primary dysmenorrhea happens, but it is thought that natural chemicals produced by the body (called prostaglandins) collect in the uterus (womb) lining.
These chemicals help the uterus to shed the lining during a period by making the walls of the uterus contract. Women who experience period pain may have higher levels of prostaglandins, making the contractions feel painful.
Cramps are the most common symptom; with some women experiencing them a day before their period starts. The cramps usually last between one to three days, but this can vary with each period.
Secondary dysmenorrhea
This type of painful menstruation is caused by an underlying condition affecting the uterus (womb). Conditions that can cause painful periods include endometriosis, uterine fibroids, pelvic inflammatory disease and adenomyosis.
You may not be aware of any problems, but if you have noticed a change to your period pain (such as it feels more painful, or lasts longer than normal), you may have secondary dysmenorrhea. It is unlikely that a woman under 30 years old will be affected by secondary dysmenorrhea.
Secondary dysmenorrhea should be suspected in older women with no history of dysmenorrhea until proven otherwise 18. Symptoms include menorrhagia (heavy period), bleeding between periods, dyspareunia (pain during sex), postcoital bleeding (bleeding after sex), irregular periods, pain (like period pain) between periods and infertility.
Endometriosis is the most common cause of secondary dysmenorrhea 19. The incidence is highest among women 25 to 29 years of age and lowest among women older than 44 years. Black women have a 40% lower incidence of endometriosis compared with white women 20. Table 1 lists risk factors for the development of dysmenorrhea; protective factors include regular exercise, oral contraceptive use, and early childbirth 18.
Table 1. Risk factors for menstrual cramps
| Risk factor |
| Heavy menstrual loss |
| Premenstrual symptoms |
| Irregular menstrual cycles |
| Age younger than 30 years |
| Clinically suspected pelvic inflammatory disease |
| Sexual abuse |
| Menarche before 12 years of age |
| Low body mass index |
| Sterilization |
What causes menstrual cramps
Menstrual cramps occurs when the muscular wall of the womb (uterus) tightens (contracts). Mild contractions continually pass through your womb (uterus), but they’re usually so mild that most women can’t feel them.
During your period, the wall of the womb starts to contract more vigorously to encourage the uterine lining to shed away as part of your monthly period.
When the muscular wall of the uterus contracts, it compresses the blood vessels lining your womb. This temporarily cuts off the blood supply – and hence oxygen supply – to your uterus. Without oxygen, the tissues in your uterus release chemicals that trigger pain.
While your body is releasing these pain-triggering chemicals, it’s also producing other chemicals called prostaglandins. These encourage the womb muscles to contract more, further increasing the level of pain.
It’s not known why some women experience more period pain than others. It may be that some women have a build-up of prostaglandins, which means they experience stronger contractions.
Period pain caused by a condition
Less commonly, menstrual cramps can be caused by an underlying medical condition. Doctors sometimes call this secondary dysmenorrhea.
Period pain linked to an underlying condition tends to affect older women. Women aged 30 to 45 are most commonly affected.
Conditions that can cause period pain include:
- Endometriosis – where cells that normally line the womb start to grow in other places, such as in the fallopian tubes and ovaries; these cells can cause intense pain when they shed and fall away
- Uterine Fibroids – non-cancerous tumors that can grow in the uterus and can make your periods heavy and painful
- Pelvic inflammatory disease – where your womb, fallopian tubes and ovaries become infected with bacteria, causing them to become severely inflamed
- Adenomyosis – where the tissue that normally lines the womb starts to grow within the muscular womb wall, making your periods particularly painful
- Cervical stenosis. In some women, the opening of the cervix may be so small that it impedes menstrual flow, causing a painful increase of pressure within the uterus.
An intrauterine device (IUD) is a type of contraception made from copper and plastic that fits inside the womb. It can also sometimes cause period pain, particularly during the first few months after it’s inserted.
You may notice a change in your normal pattern of pain if your period pain is linked to one of the above conditions. For example, the pain may be more severe or it may last much longer than normal.
If your period pain is caused by an underlying condition, you may also experience:
- irregular periods
- bleeding in between periods
- a thick or foul-smelling vaginal discharge
- pain during sex
See your doctor if you experience any of these symptoms.
Risk factors for menstrual cramps
You may be at greater risk of menstrual cramps if:
- You’re younger than age 30
- You started puberty early, at age 11 or younger
- You have heavy bleeding during periods (menorrhagia)
- You have irregular menstrual bleeding (metrorrhagia)
- You’ve never given birth
- You have a family history of dysmenorrhea
- You’re a smoker
Menstrual cramps diagnosis
Your doctor will review your medical history and perform a physical exam, including a pelvic exam. During the pelvic exam, your doctor will check for any abnormalities in your reproductive organs and look for signs of infection.
Characteristic symptoms of primary dysmenorrhea include lower abdominal or pelvic pain with or without radiation to the back or legs, with initial onset six to 12 months after menarche (Table 2). Pain typically lasts eight to 72 hours and usually occurs at the onset of menstrual flow. Other associated symptoms may include low back pain, headache, diarrhea, fatigue, nausea, or vomiting 1. A family history may be helpful in differentiating primary from secondary dysmenorrhea; patients with a family history of endometriosis in first-degree relatives are more likely to have secondary dysmenorrhea 1.
About 10% of young adults and adolescents with dysmenorrhea have secondary dysmenorrhea; the most common cause is endometriosis 21. Changes in timing and intensity of the pain or dyspareunia may suggest endometriosis, and menstrual flow abnormalities may be associated with adenomyosis or leiomyomata. A history of sexually transmitted infection or vaginal discharge associated with dyspareunia raises suspicion for pelvic inflammatory disease (PID). Asking about a history of sexual trauma is also recommended 22.
Figure 2. Evaluation and Treatment of Menstrual Cramps
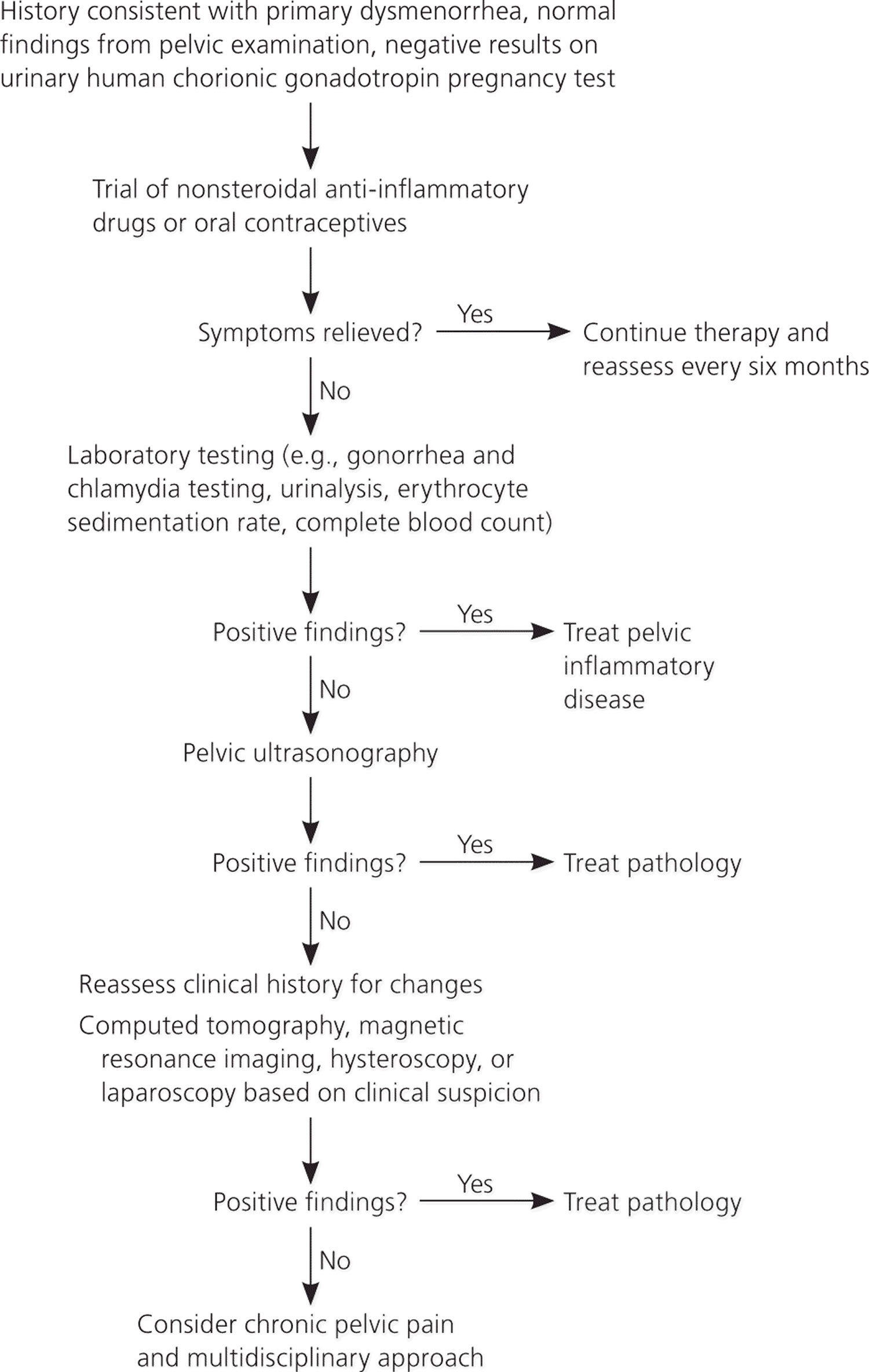
Table 2. Differential Diagnosis of Menstrual Cramps
| Suspected condition | Clinical presentation | Diagnostic evaluation |
|---|---|---|
Primary dysmenorrhea | Recurrent, crampy, suprapubic pain occurring just before or during menses and lasting two to three days; pain may radiate into the lower back and thighs, and may be associated with nausea, fatigue, bloating, and general malaise; normal pelvic examination findings1 | Diagnosis is clinical; urine tests should be ordered to rule out pregnancy or infection 24 |
Endometriosis | Cyclic (can be noncyclic) pelvic pain with menstruation; may be associated with deep dyspareunia, dysuria, dyschezia, and subfertility; rectovaginal examination findings include fixed or retroverted uterus or reduced uterine mobility, adnexal masses, and uterosacral nodularity 25 | Transvaginal and pelvic ultrasonography are highly accurate for detecting ovarian and bowel endometriomas; magnetic resonance imaging may be indicated for deeply infiltrating endometriosis 26; laparoscopy with biopsy and histology is the preferred diagnostic test 27 |
Pelvic inflammatory disease | History of lower abdominal pain in sexually active patients; abnormal pelvic examination findings consisting of cervical motion tenderness, uterine tenderness, and/or adnexal tenderness; other associated clinical features include oral temperature > 101°F (38.3°C) and abnormal cervical or vaginal mucopurulent discharge 28 | Saline microscopy of vaginal fluid may show organism; elevated erythrocyte sedimentation rate or C-reactive protein level suggests infection; laboratory documentation of cervical infection with Neisseria gonorrhoeae or Chlamydia trachomatis is confirmatory; transvaginal ultrasonography is not usually indicated but may show thickened tubes with fluid collection, free pelvic fluid, or tubo-ovarian complex 28 |
Adenomyosis | Usually associated with menorrhagia; may include intermenstrual bleeding; physical examination findings include enlarged, tender, boggy uterus | Transvaginal ultrasonography and, if necessary, magnetic resonance imaging will usually detect endometrial tissue within the myometrium 29 |
Leiomyomata | Cyclic pelvic pain with menorrhagia and occasionally dyspareunia, particularly with anterior and fundal fibroids | Transvaginal ultrasonography can identify uterine fibroids |
Ectopic pregnancy | History of amenorrhea, abnormal uterine bleeding, severe sharp lower abdominal pain, and/or cramping on the affected side of the pelvis; may present with complications (e.g., hypotension, shock) | Positive urinary human chorionic gonadotropin pregnancy test; pelvic or transvaginal ultrasonography demonstrating extrauterine gestational sac |
Interstitial cystitis | History of suprapubic pain (usually noncyclic) associated with urinary symptoms (e.g., frequency, nocturia); pain may radiate into the groin and rectum and is usually relieved by voiding; negative pelvic examination findings | Urinalysis; cystoscopy with hydrodistension and biopsy, which may show irritation of the bladder wall mucosa 22 |
Chronic pelvic pain | History of noncyclic pelvic pain for at least six months; pain may radiate anteriorly toward the vagina or posteriorly toward the rectum and is worsened by anxiety; may be associated with dyspareunia and difficulty with defecation; pelvic examination findings may be normal, but burning pain exacerbated by unilateral rectal palpation suggests pudendal nerve entrapment of the affected side 22 | Pelvic magnetic resonance imaging along the pudendal nerve to assess the nerve and surrounding structures; if findings on workup are negative, the diagnosis is based on clinical history 22 |
NOTE: Conditions are listed in approximate order of decreasing frequency.
Pelvic Examination
Your doctor may want to carry out a pelvic examination to help diagnose or rule out other conditions.
They’ll insert gloved, lubricated fingers into your vagina to feel for any abnormalities in your womb or ovaries.
Pelvic examinations are only carried out by qualified healthcare professionals, such as doctors or gynecologists.
The examination won’t be carried out without your permission (consent). You can also choose to have a friend or relative present, or a practice nurse to act as a chaperone.
A pelvic examination should be performed in adolescents who have had vaginal intercourse because of the high risk of pelvic inflammatory disease (PID) in this population. A pelvic examination is not essential for adolescents with symptoms of primary dysmenorrhea who have never had vaginal intercourse. However, if endometriosis is suspected, pelvic and rectovaginal examinations should be performed 25. Pelvic examination has a 76% sensitivity, 74% specificity, 67% positive predictive value, and 81% negative predictive value for endometriosis 30. Findings are usually normal in patients with primary dysmenorrhea. Findings in those with secondary dysmenorrhea include a fixed uterus or reduced uterine mobility, adnexal masses, and uterosacral nodularity in patients with endometriosis; mucopurulent cervical discharge in those with pelvic inflammatory disease (PID); and uterine enlargement or asymmetry in patients with adenomyosis 22.
One or more findings of uterine tenderness, adnexal tenderness, or cervical motion tenderness should raise the suspicion for pelvic inflammatory disease (PID) 28. Additional criteria include oral temperature greater than 101°F (38.3°C), abnormal cervical or vaginal mucopurulent discharge, abundant white blood cells on saline microscopy of vaginal fluid, elevated erythrocyte sedimentation rate, elevated C-reactive protein level, and laboratory documentation of cervical infection with Neisseria gonorrhoeae or Chlamydia trachomatis.
Adenomyosis
Adenomyosis is the presence of endometrial glands and stroma within the myometrium. Symptoms and signs include dysmenorrhea, menorrhagia, and a uniformly enlarged uterus. Diagnosis is usually confirmed through transvaginal ultrasonography and magnetic resonance imaging 29.
If your doctor suspects that your menstrual cramps are being caused by an underlying disorder, he or she may recommend other tests, such as:
The diagnosis of primary dysmenorrhea is based on the clinical history and physical examination 22. Laparoscopy is indicated if the etiology remains unknown after an appropriate noninvasive evaluation has been completed 31.
- Ultrasound. This test uses sound waves to create an image of your uterus, cervix, fallopian tubes and ovaries. Transvaginal ultrasonography should be performed if secondary dysmenorrhea is suspected 32. It has a 91% sensitivity and 98% specificity, a positive likelihood ratio of 30, and a negative likelihood ratio of 0.09 for detection of bowel endometriosis 27. It also has a high degree of accuracy for detection of ovarian endometriomas 30.
- Other imaging tests. A CT scan or magnetic resonance imaging (MRI) provides more detail than an ultrasound and can help your doctor diagnose underlying conditions. A CT scan combines X-ray images taken from many angles to produce cross-sectional images of bones, organs and other soft tissues inside your body. MRI uses radio waves and a powerful magnetic field to produce detailed images of internal structures. Both tests are noninvasive and painless. Magnetic resonance imaging may be considered as a second-line diagnostic option if adnexal torsion, deep pelvic endometriosis, or adenomyosis is still suspected after inconclusive or negative findings on transvaginal ultrasonography 33.
- Laparoscopy. Laparoscopy usually isn’t necessary for the diagnosis of menstrual cramps, but it can help detect an underlying condition, such as endometriosis, adhesions, fibroids, ovarian cysts and ectopic pregnancy. During this outpatient surgery and under general anesthetic, your doctor views your abdominal cavity and reproductive organs by making tiny incisions in your abdomen and inserting a fiber-optic telescope (laparoscope) with a small camera lens. Laparoscope can be used to look at your internal organs, as well as take samples of tissue (a biopsy)
- Hysteroscopy – allows the inside of the womb to be examined using a fibro-optic telescope; it’s carefully passed through your vagina and into the womb to check for abnormalities
Other useful tests include a urinary human chorionic gonadotropin (hCG) pregnancy test; vaginal and endocervical swabs, a complete blood count, erythrocyte sedimentation rate, and urinalysis. Cervical cytology should also be performed to rule out malignancy.
How to get rid of menstrual cramps
Menstrual cramps are treatable. Your doctor may recommend:
Medications
A Cochrane review 34 of 73 randomized controlled trials demonstrated strong evidence to support nonsteroidal anti-inflammatory drugs (NSAIDs) as the first-line treatment for primary dysmenorrhea (Table 3). The choice of NSAID should be based on effectiveness and tolerability for the individual patient, because no NSAID has been proven more effective than others. Medications should be taken one to two days before the anticipated onset of menses, and continued on a fixed schedule for two to three days 34.
If your symptoms or a laparoscopy point to endometriosis as the cause of your dysmenorrhea, birth control pills, the birth control implant, the injection, or the hormonal intrauterine device can be tried.
Gonadotropin-releasing hormone agonists are another type of medication that may relieve endometriosis pain. These drugs may cause side effects, including bone loss, hot flashes, and vaginal dryness. They usually are given for a limited amount of time. They are not recommended for teenagers except in severe cases when other treatments have not worked.
Table 3. Nonsteroidal Anti-Inflammatory Drugs Used in the Treatment of Primary Dysmenorrhea
| Drug | Dosage |
| Celecoxib (Celebrex)† | 400 mg initially, then 200 mg every 12 hours |
| Ibuprofen | 200 to 600 mg every six hours |
| Mefenamic acid | 500 mg initially, then 250 mg every six hours |
| Naproxen | 440 to 550 mg initially, then 220 to 275 mg every 12 hours |
†—For use in women older than 18 years.
What is the role of hormonal contraceptives?
Primary Dysmenorrhea
Oral, intravaginal, and intrauterine hormonal contraceptives have been recommended for management of primary dysmenorrhea (Table 4); however, the evidence supporting their effectiveness is limited 35. There is a lack of high-quality randomized controlled trials demonstrating pain improvement with the use of oral contraceptives27; however, smaller randomized controlled trials report response rates as high as 80% 36. Both 28-day and extended-cycle oral contraceptives are reasonable options in women with primary dysmenorrhea who also desire contraception 37.
Your doctor may try you on the combined oral contraceptive pill. This can ease period pain because it thins the womb lining and reduces the amount of prostaglandin your body releases.
A thinner womb lining means the muscles of the womb don’t have to contract as much when it sheds as part of your monthly menstrual cycle. Your period will also be lighter.
If the combined contraceptive pill isn’t suitable for you, contraceptive implants or injections are good alternatives. The Mirena intrauterine system (IUS) can also sometimes help with painful periods.
Table 4. Select Hormonal Contraceptives Approved for Treatment of Primary Dysmenorrhea
| Contraceptive |
| Combined oral contraceptives (monophasic or multiphasic) |
| Norgestimate/ethinyl estradiol 0.25 mg/0.035 mg (Ortho-Cyclen)† |
| Norethindrone/ethinyl estradiol 1 mg/0.035 mg (Ortho-Novum 1/35)† |
| Extended-cycle oral contraceptives |
| Levonorgestrel/ethinyl estradiol 0.15 mg/0.03 mg (Seasonique)† |
| Levonorgestrel/ethinyl estradiol 90 mcg/20 mcg (Amethyst)† |
| Other hormonal contraceptives |
| Etonogestrel implant (Nexplanon)† |
| Etonogestrel/ethinyl estradiol 0.12 mg/0.015 mg vaginal ring (Nuvaring) |
| Levonorgestrel-releasing intrauterine system (Mirena)‡ |
| Medroxyprogesterone 150 mg per mL injection (Depo-Provera)† |
†—First-line treatment for dysmenorrhea caused by endometriosis 25.
‡—Second-line treatment for dysmenorrhea caused by endometriosis 25.
Referral to a specialist
If your period pain hasn’t been controlled after three months of treatment with painkillers or the combined contraceptive pill, your family doctor may refer you to a specialist.
This is for further investigations to rule out an underlying medical condition.
Treating an underlying medical condition
If your period pain is caused by an underlying condition, your treatment will depend on which condition you have.
For example, pelvic inflammatory disease (PID) may require antibiotics to treat the infection, while uterine fibroids may need to be surgically removed.
Menstrual cramps caused by Endometriosis
Combined oral contraceptives are the first-line treatment for dysmenorrhea caused by endometriosis 33. A double-blind randomized controlled trial demonstrated the effectiveness of combined oral estrogen-progestin for the treatment of dysmenorrhea associated with endometriosis 38. Several trials have confirmed the effectiveness of oral and depot medroxyprogesterone (Provera), the etonogestrel implant (Nexplanon), and the levonorgestrel-releasing intrauterine system (Mirena) 36.
Menstrual cramps caused by Uterine Fibroids
If uterine fibroids are causing your dysmenorrhea, a treatment called uterine artery embolization (UAE) may help.
In this procedure, the blood vessels to the uterus are blocked with small particles, stopping the blood flow that allows fibroids to grow. Some women can have UAE as an outpatient procedure.
Complications of uterine artery embolization include infection, pain, and bleeding.
When is surgery done to treat dysmenorrhea?
If other treatments do not work in relieving dysmenorrhea, surgery may be needed. The type of surgery depends on the cause of your pain.
If fibroids are causing the pain, sometimes they can be removed with surgery. Endometriosis tissue can be removed during surgery. Endometriosis tissue may return after the surgery, but removing it can reduce the pain in the short term. Taking hormonal birth control or other medications after surgery may delay or prevent the return of pain.
Hysterectomy may be done if other treatments have not worked and if the disease causing the dysmenorrhea is severe. This procedure normally is the last resort.
What is the role of complementary therapies?
There is limited and inconsistent evidence on the effectiveness of nonpharmacologic therapies for primary dysmenorrhea 39. Expert consensus 21 and a small study 40 suggest that topical heat may be as effective as NSAIDs, but there is insufficient evidence for acupuncture, yoga, and massage. Exercise 41 and nutritional interventions (supplementation or increased intake of omega-3 fatty acids and vitamin B) 21, 35, 37 may provide some benefit, but the evidence is limited to small randomized controlled trials 37.
Lifestyle and home remedies
Things you may want to try at home include:
- Exercise. Studies have found that physical activity may ease the pain of menstrual cramps.
- Heat. Soaking in a hot bath or using a heating pad, hot water bottle or heat patch on your lower abdomen may ease menstrual cramps. Applying heat may be just as effective as over-the-counter pain medication for relieving menstrual cramps.
- Dietary supplements. A number of studies have indicated that vitamin E, omega-3 fatty acids, vitamin B-1 (thiamine), vitamin B-6 and magnesium supplements may effectively reduce menstrual cramps.
- Avoiding alcohol and tobacco. These substances can make menstrual cramps worse.
- Reducing stress. Psychological stress may increase your risk of menstrual cramps and their severity.
Alternative medicine
Most alternative therapies haven’t been well-studied for treating menstrual cramps and need further study before experts can clearly recommend one treatment or another. However, some alternative treatments may help with menstrual cramps, including:
- Acupuncture. Acupuncture involves inserting extremely thin needles through your skin at strategic points on your body. Some studies have found that acupuncture helps relieve menstrual cramps.
- Transcutaneous electrical nerve stimulation (TENS). A TENS device connects to the skin using adhesive patches with electrodes in them. The electrodes deliver a varying level of electric current to stimulate nerves. TENS may work by raising the threshold for pain signals and stimulating the release of endorphins, your body’s natural painkillers. In studies, TENS was more effective than a placebo in relieving menstrual cramp pain.
- Herbal medicine. Some herbal products, such as pycnogenol, fennel or combination products, may provide some relief from menstrual cramps.
- Acupressure. Like acupuncture, acupressure also involves stimulating certain points on the body. In acupressure, this is done with gentle pressure on the skin instead of needles. Although research on acupressure and menstrual cramps is limited, it appears that acupressure may be more effective than a placebo in easing menstrual cramps.
- Proctor M, Farquhar C. Diagnosis and management of dysmenorrhoea. BMJ. 2006;332(7550):1134–1138.[↩][↩][↩]
- Nasir L, Bope ET. Management of pelvic pain from dysmenorrhea or endometriosis. J Am Board Fam Pract. 2004;17(suppl):S43–S47.[↩]
- Harlow SD, Ephross SA. Epidemiology of menstruation and its relevance to women’s health. Epidemiol Rev 1995;17(2):265–86.[↩]
- Banikarim C, Chacko MR, Kelder SH. Prevalence and impact of dysmenorrhea on Hispanic female adolescents. Arch Pediatr Adolesc Med. 2000;154(12):1226–1229.[↩]
- Parker, M., Sneddon, A. and Arbon, P. (2010), The menstrual disorder of teenagers (MDOT) study: determining typical menstrual patterns and menstrual disturbance in a large population-based study of Australian teenagers. BJOG: An International Journal of Obstetrics & Gynaecology, 117: 185–192. doi:10.1111/j.1471-0528.2009.02407.x http://onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2009.02407.x/full[↩]
- Parker, M., Sneddon, A. and Arbon, P. (2010), The menstrual disorder of teenagers (MDOT) study: determining typical menstrual patterns and menstrual disturbance in a large population-based study of Australian teenagers. BJOG: An International Journal of Obstetrics & Gynaecology, 117: 185–192. doi:10.1111/j.1471-0528.2009.02407.x http://onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2009.02407.x/full[↩]
- Banikarum C, Chako MR, Kelder SH. Prevalence and impact of dysmenorrhoea on hispanic female adolescents. Arch Pediatr Adolesc 2000;154:1226–9. [↩]
- Wilson CA, Keye WR. A survey of adolescent dysmenorrhea and premenstrual symptom frequency: a model program for prevention, detection, and treatment. J Adolesc Health Care 1989;10:317–22. https://www.ncbi.nlm.nih.gov/pubmed/2786516[↩]
- Johnson J. Level of knowledge among adolescent girls regarding effective treatment for dysmenorrhea. J Adolesc Health Care 1988;9:398–412. https://www.ncbi.nlm.nih.gov/pubmed/3170307[↩]
- Banikarum C, Chako MR, Kelder SH. Prevalence and impact of dysmenorrhoea on hispanic female adolescents. Arch Pediatr Adolesc 2000;154:1226–9.[↩]
- Teperi J, Rimpelä M. Menstrual pain, health and behaviours in girls. Soc Sci Med 1989;29:163–9. https://www.ncbi.nlm.nih.gov/pubmed/2787534[↩][↩]
- Laufer MR, Goitein BA, Bush M. Prevalence of endometriosis in adolescent girls with chronic pelvic pain not responding to conventional therapy. J Pediatr Adolesc Gynecol 1997;10:199–202. https://www.ncbi.nlm.nih.gov/pubmed/9391902[↩][↩]
- Arruda MS, Petta CA, Abrão MS, Benetti-Pinto CL. Time elapsed from onset of symptoms to diagnosis of endometriosis in a cohort study of Brazilian women. Hum Reprod 2003;18:756–9. https://www.ncbi.nlm.nih.gov/pubmed/12660267[↩]
- American College of Obstetricians and Gynaecologists. ACOG committee opinion No. 310, April 2005. Endometriosis in adolescents. Obstet Gynecol 2005;105:921–7. https://www.ncbi.nlm.nih.gov/pubmed/15802438[↩]
- Gao X, Yeh YC, Outley J, Simon J, Botteman M, Spalding J. Health-related quality of life burden of women with endometriosis: a literature review. Curr Med Res Opin 2006;22:1787–97. https://www.ncbi.nlm.nih.gov/pubmed/16968582[↩]
- Whincup PH, Gilg JA, Odoki K, Taylor SJC, Cook DG. Age of menarche in contemporary British teenagers: survey of girls born between 1982 and 1986. BMJ 2001;322:1095–6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC31261/[↩]
- Batt RE, Mitwally MF. Endometriosis from thelarche to midteens: pathogenesis and prognosis, prevention and pedagogy. J Pediatr Adolesc Gynecol, 2003;16:337–47. https://www.ncbi.nlm.nih.gov/pubmed/14642954[↩]
- Latthe P, Mignini L, Gray R, Hills R, Khan K. Factors predisposing women to chronic pelvic pain: systematic review. BMJ. 2006;332(7544):749–755.[↩][↩]
- French L. Dysmenorrhea in adolescents: diagnosis and treatment. Paediatr Drugs. 2008;10(1):1–7.[↩]
- Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Marshall LM, Hunter DJ. Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am J Epidemiol. 2004;160(8):784–796.[↩]
- Harel Z. Dysmenorrhea in adolescents and young adults: etiology and management. J Pediatr Adolesc Gynecol. 2006;19(6):363–371.[↩][↩][↩]
- Fall M, Baranowski AP, Fowler CJ, et al.; European Association of Urology. EAU guidelines on chronic pelvic pain. Eur Urol. 2004;46(6):681–689.[↩][↩][↩][↩][↩][↩]
- Diagnosis and Initial Management of Dysmenorrhea. Am Fam Physician. 2014 Mar 1;89(5):341-346. https://www.aafp.org/afp/2014/0301/p341.html[↩][↩]
- Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol. 2006;108(2):428–441.[↩]
- Leyland N, Casper R, Laberge P, Singh SS; SOGC. Endometriosis: diagnosis and management. J Obstet Gynaecol Can. 2010;32(7 suppl 2):S1–S32.[↩][↩][↩][↩]
- Saccardi C, Cosmi E, Borghero A, Tregneghi A, Dessole S, Litta P. Comparison between transvaginal sonography, saline contrast sonovaginography and magnetic resonance imaging in the diagnosis of posterior deep infiltrating endometriosis. Ultrasound Obstet Gynecol. 2012;40(4):464–469.[↩]
- Hudelist G, English J, Thomas AE, Tinelli A, Singer CF, Keckstein J. Diagnostic accuracy of transvaginal ultrasound for non-invasive diagnosis of bowel endometriosis: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2011;37(3):257–263.[↩][↩]
- Workowski KA, Berman S; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010 [published correction appears in MMWR Recomm Rep. 2011;60(1):18]. MMWR Recomm Rep. 2010;59(RR-12):1–110.[↩][↩][↩]
- Benagiano G, Brosens I, Carrara S. Adenomyosis: new knowledge is generating new treatment strategies. Womens Health (Lond Engl). 2009;5(3):297–311.[↩][↩]
- Eskenazi B, Warner M, Bonsignore L, Olive D, Samuels S, Vercellini P. Validation study of nonsurgical diagnosis of endometriosis. Fertil Steril. 2001;76(5):929–935.[↩][↩]
- Hori Y; SAGES Guidelines Committee. Diagnostic laparoscopy guidelines. Surg Endosc. 2008;22(5):1353–1383.[↩]
- American Institute of Ultrasound in Medicine. AIUM practice guideline for the performance of pelvic ultrasound examinations. J Ultrasound Med. 2010;29(1):166–172.[↩]
- Wilkinson C, Sanderson A. Adnexal torsion—a multimodality imaging review. Clin Radiol. 2012;67(5):476–483.[↩][↩]
- Marjoribanks J, Proctor M, Farquhar C, Derks RS. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2010;(1):CD001751.[↩][↩]
- French L. Dysmenorrhea. Am Fam Physician. 2005;71(2):285–291.[↩][↩]
- American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 110: noncontraceptive uses of hormonal contraceptives. Obstet Gynecol. 2010;115(1):206–218.[↩][↩]
- Morrow C, Naumburg EH. Dysmenorrhea. Prim Care. 2009;36(1):19–32.[↩][↩][↩]
- Harada T, Momoeda M, Taketani Y, Hoshiai H, Terakawa N. Low-dose oral contraceptive pill for dysmenorrhea associated with endometriosis: a placebo-controlled, double-blind, randomized trial. Fertil Steril. 2008;90(5):1583–1588.[↩]
- Proctor ML, Murphy PA, Pattison HM, Suckling J, Farquhar CM. Behavioural interventions for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. 2007;(3):CD002248.[↩]
- Akin MD, Weingand KW, Hengehold DA, Goodale MB, Hinkle RT, Smith RP. Continuous low-level topical heat in the treatment of dysmenorrhea. Obstet Gynecol. 2001;97(3):343–349.[↩]
- Brown J, Brown S. Exercise for dysmenorrhoea. Cochrane Database Syst Rev. 2010;(2):CD004142.[↩]





{kind=link}