Contents
What is Moyamoya disease
Moyamoya disease is a rare, progressive disorder of blood vessels in the brain, specifically the internal carotid arteries and the arteries that branch from them. These vessels, which provide oxygen-rich blood to the brain, narrow over time. Narrowing of these blood arteries reduces blood flow in the brain, specifically in the base of the brain in an area called the basal ganglia. In an attempt to compensate, new networks of small, fragile blood vessels form. These networks, visualized by a particular test called an angiogram, resemble puffs of smoke, which is how the condition got its name: “moyamoya” is an expression meaning “something hazy like a puff of smoke” in Japanese (see Figures 1 to 6).
Collateral circulation forms from a number of sources:
- via the abnormal moyamoya vessels: lenticulostriate, thalamoperforating, leptomeningeal, and dural arteries
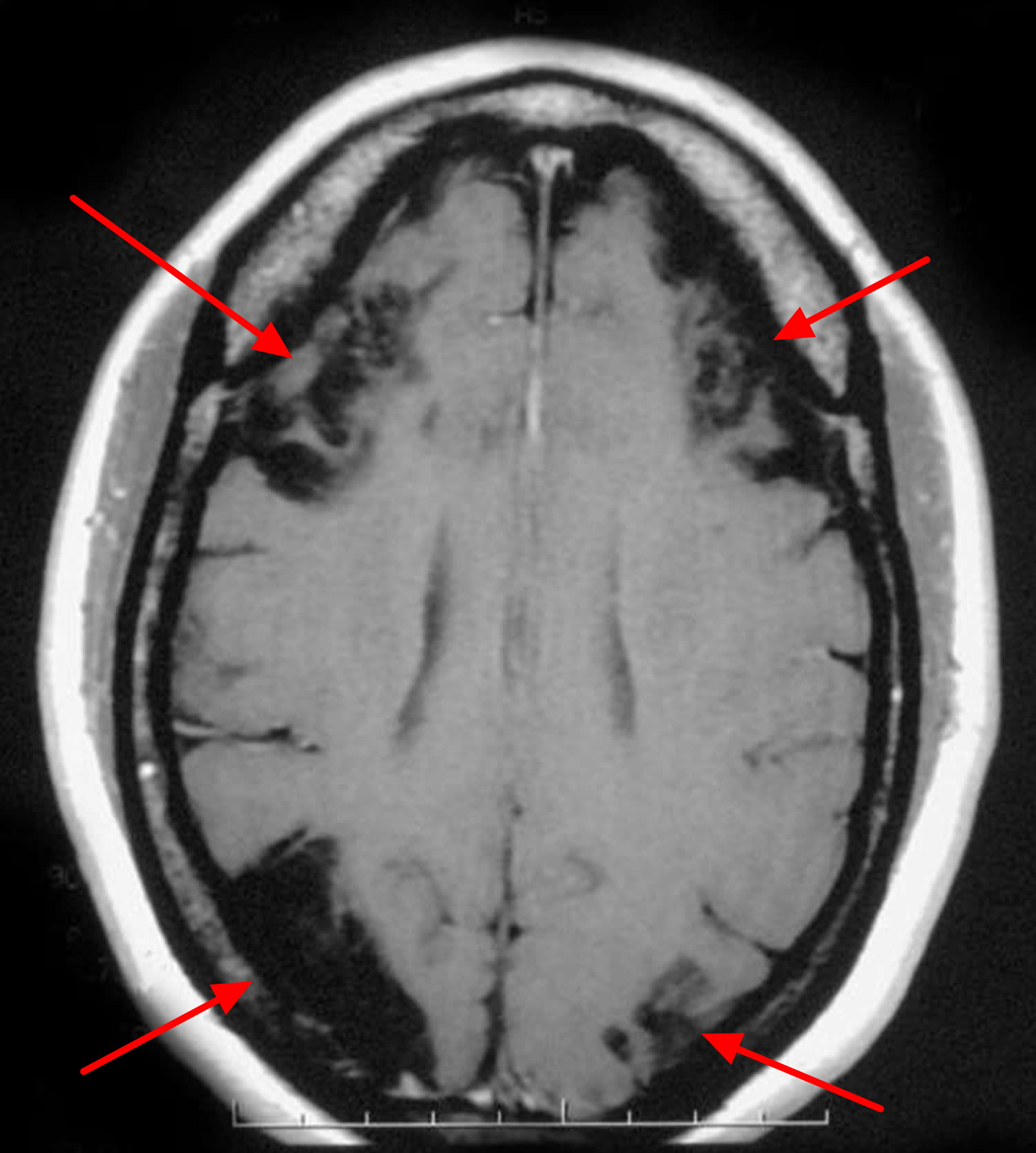
- pial collaterals from less affected vessels (especially posterior cerebral artery): forming the so called ivy sign (high serpentine sulcal FLAIR signal intensity due to slow flow and also high signal on T1 post contrast enhanced MRI) 1
- multiple foci of microbleeds and also prominent deep medullary veins “brush sign” on susceptibility sequences 2
- transdural branches of the middle meningeal and other dural branches
Although Moyamoya disease was classically described as affecting the internal carotid artery, over 50% of patients also have involvement of the posterior cerebral arteries. Generalized cerebral atrophy is a common finding.
Moyamoya disease primarily affects children around age 5, but it can also occur in adults in their thirties or forties, with a bi-modal age distribution 3:
- Early childhood: peak ~4 years of age (two-thirds). In children, the first symptom of Moyamoya disease is often stroke, or recurrent transient ischemic attacks (TIA, commonly referred to as “mini-strokes”), frequently accompanied by muscular weakness or paralysis affecting one side of the body, or seizures.
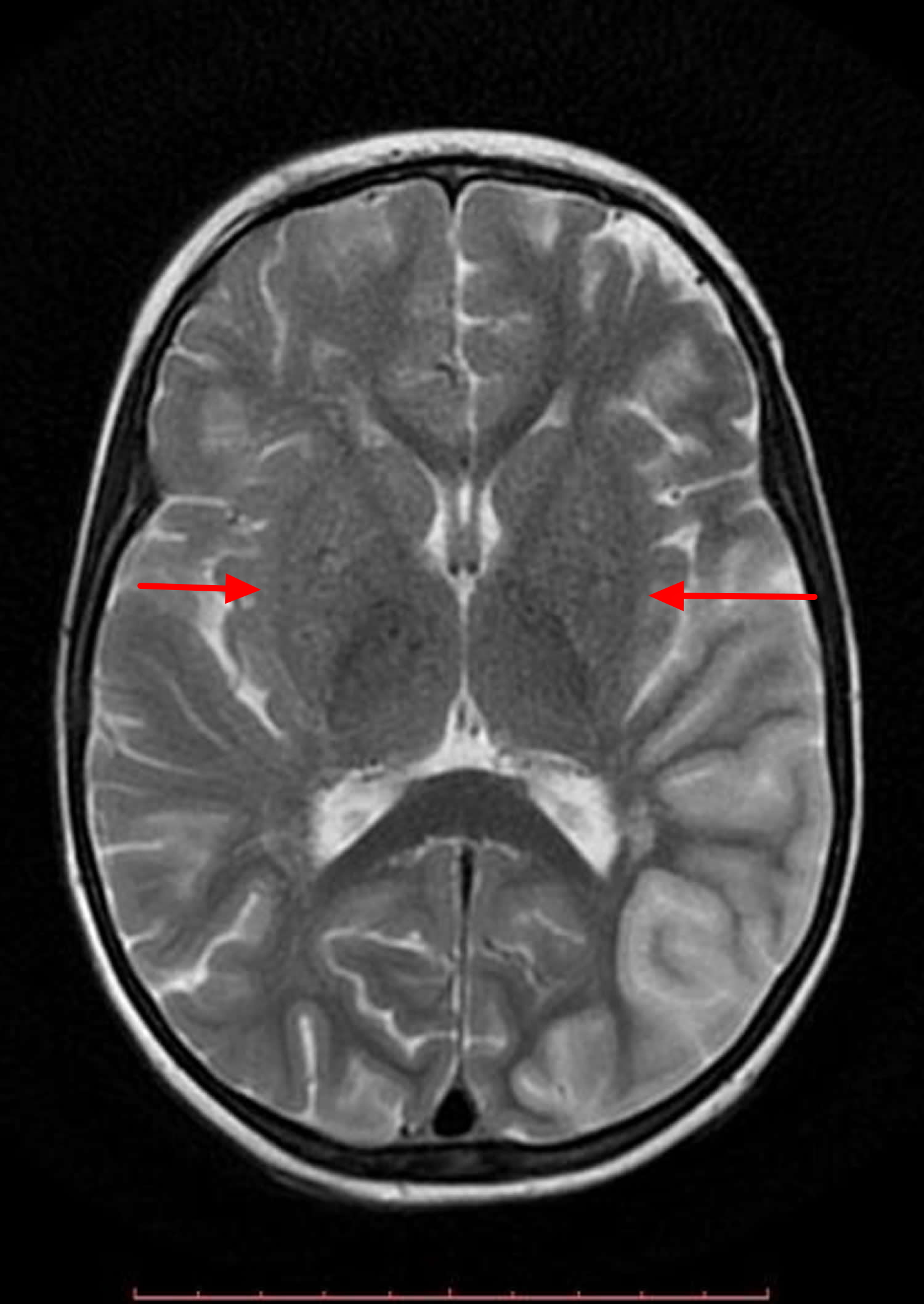
- Middle age adults: 30-40 years of age (one-third). Adults may also experience these symptoms that arise from blocked arteries, but more often experience a hemorrhagic stroke due to bleeding into the brain from the abnormal brain vessels. Individuals with this disorder may have disturbed consciousness, problems with speaking and understanding speech, sensory and cognitive impairments, involuntary movements, and vision problems. Watershed infarcts are also very commonly identified (see Figure 7 below).
The condition was initially described in Japanese patients, where it is still most common, affecting about 5 in 100,000 individuals, in which 7-10% of cases are familial. In Japan, moyamoya disease typically occurs in females under the age of 20. The condition is also relatively common in other Asian populations. In the United States, Asian Americans are four times more commonly affected than whites. For unknown reasons, moyamoya disease occurs twice as often in females as in males. Moyamoya disease has also been found in the US, Europe, Australia, North and South America and Africa. It is ten times less common in Europe.
The genetics of Moyamoya disease are not well understood. Research suggests that the condition can be passed through families, and changes in one gene, RNF213, have been associated with the condition. Other genes that have not been identified may be involved in Moyamoya disease. It is also likely that other factors (such as infection or inflammation) in combination with genetic factors play a role in the condition’s development.
The RNF213 gene provides instructions for making a protein whose function is unknown. However, research suggests that the RNF213 protein is involved in the proper development of blood vessels.
Researchers believe that Moyamoya disease is an inherited condition because it tends to run in families 4. About one in 10 (10%) individuals with Moyamoya disease has a close relative who is also affected; in these cases researchers think that Moyamoya disease is the result of inherited genetic abnormalities. Studies that look for the abnormal gene(s) may help reveal the biomechanisms that cause the disorder. Patients with this arterial disease that occurs either on a familial or idiopathic basis are said to have “moyamoya disease.” Patients in whom the artery changes occur in association with another process such as sickle cell disease or Down syndrome are said to have “moyamoya syndrome”, “moyamoya phenomenon”, “secondary phenomenon” or “moyamoya pattern.” Moyamoya syndrome is a related term that refers to cases of moyamoya disease that occur in association with other conditions or risk factors, such as neurofibromatosis, tuberculosis meningitis, sickle cell disease, leptospirosis, brain tumors, Sturge-Weber syndrome, and tuberous sclerosis 5.
A lack of blood supply to the brain leads to increased risk for blood clots resulting in several symptoms of the disorder, including transient ischemic attacks (TIAs), strokes, and seizures and muscular weakness, or paralysis on one side of the body. In addition, the fragile blood vessels that grow can develop bulges (aneurysms), or they can break open, leading to bleeding (hemorrhage) in the brain. Affected individuals may develop recurrent headaches, involuntary jerking movements (chorea), a decline in thinking ability (cognitive impairments), disturbed consciousness, speech deficits (usually aphasia), sensory and vision problems. The symptoms of moyamoya disease often worsen over time if the condition is not treated.
Clinical presentation
Presentation is to some degree age dependent 3.
- In children hemispheric ischemic strokes are most pronounced.
- In adults hemorrhage from the abnormal vessels is more common. Watershed infarcts are also very commonly identified.
Some people have the blood vessel changes characteristic of moyamoya disease in addition to features of another disorder, such as neurofibromatosis type 1, sickle cell disease, or Graves disease. These individuals are said to have “moyamoya syndrome” or “secondary moyamoya disease.”
Due to the progressive nature of moyamoya disease, surgical treatment for moyamoya disease should be considered for symptomatic patients. For pediatric patients, early diagnosis and active intervention before irreversible brain damage occurs are mandatory. Surgical revascularization is an effective treatment modality for preventing both ischemic and hemorrhagic stroke.
No medication can stop the narrowing of the brain’s blood vessels, or the development of the thin, fragile vessels that characterize the disease 6. However, medications are used to treat many of the symptoms of the disease, and are often an important part of the management. Medications may include aspirin (to prevent or reduce the development of small blood clots); calcium channel blockers (which may improve symptoms of headaches and reduce symptoms related to transient ischemic attacks); and anti-seizure medications (when needed for a seizure disorder). In a few cases, anticoagulants may be needed for people with unstable or frequent symptoms. However, they are not used long-term due to the risk of cerebral bleeding 7.
The main symptoms of stroke can be remembered with the word F.A.S.T.:
- Face – the face may have dropped on one side, the person may not be able to smile, or their mouth or eye may have dropped.
- Arms – the person with suspected stroke may not be able to lift both arms and keep them there because of weakness or numbness in one arm.
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake.
- Time – it’s time to dial your local emergency number immediately if you see any of these signs or symptoms.
If you have any of these symptoms or if you suspect someone else is having a stroke, you must get to a hospital quickly to begin treatment. Acute stroke therapies try to stop a stroke while it is happening by quickly dissolving the blood clot or by stopping the bleeding.
Post-stroke rehabilitation helps individuals overcome disabilities that result from stroke damage. Drug therapy with blood thinners is the most common treatment for stroke.
Figure 1. External and Internal carotid artery
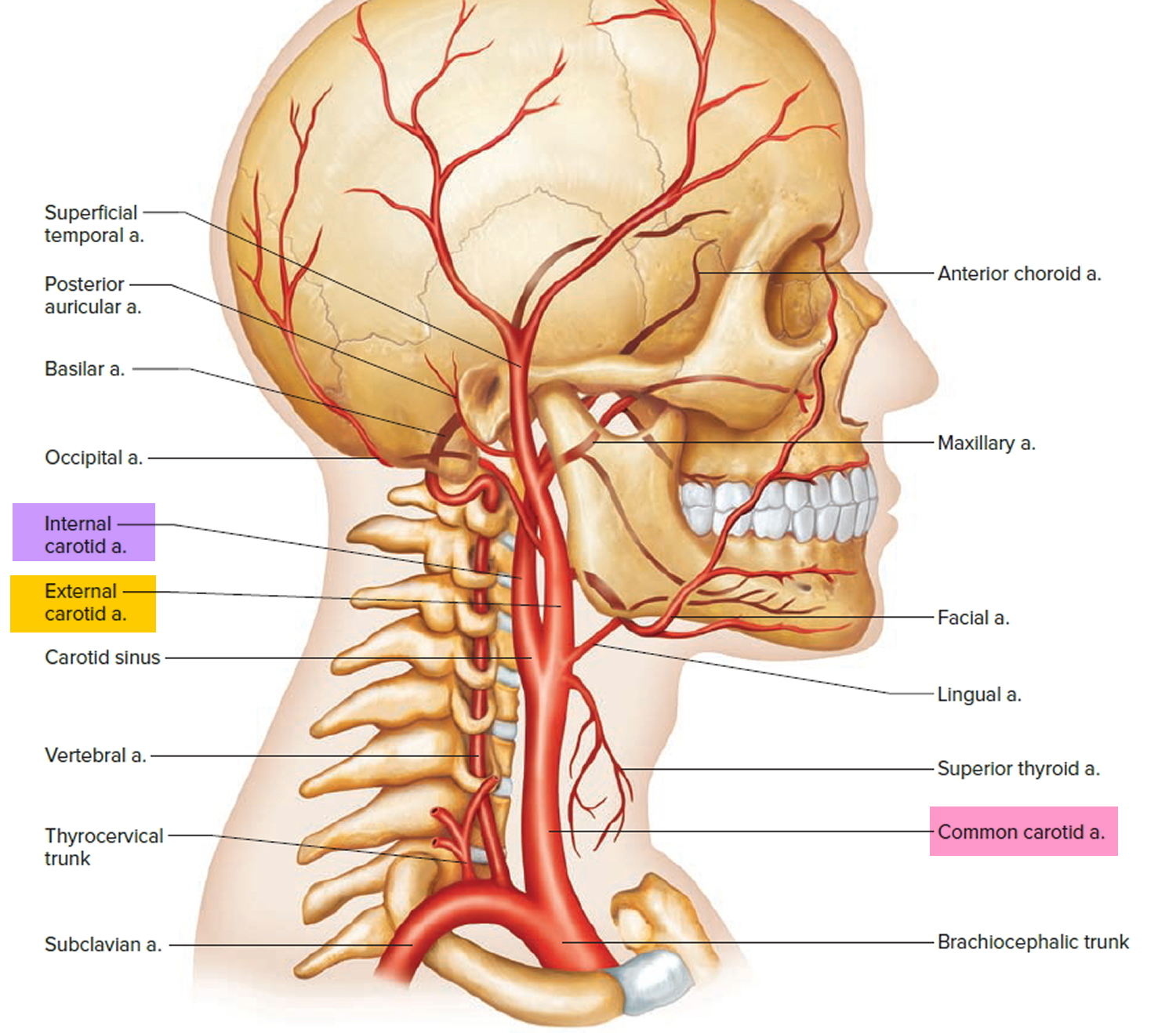
Figure 2. Branches of the Internal carotid artery supplying the brain (including frontal & parietal lobe) and the eye (& eye muscles)
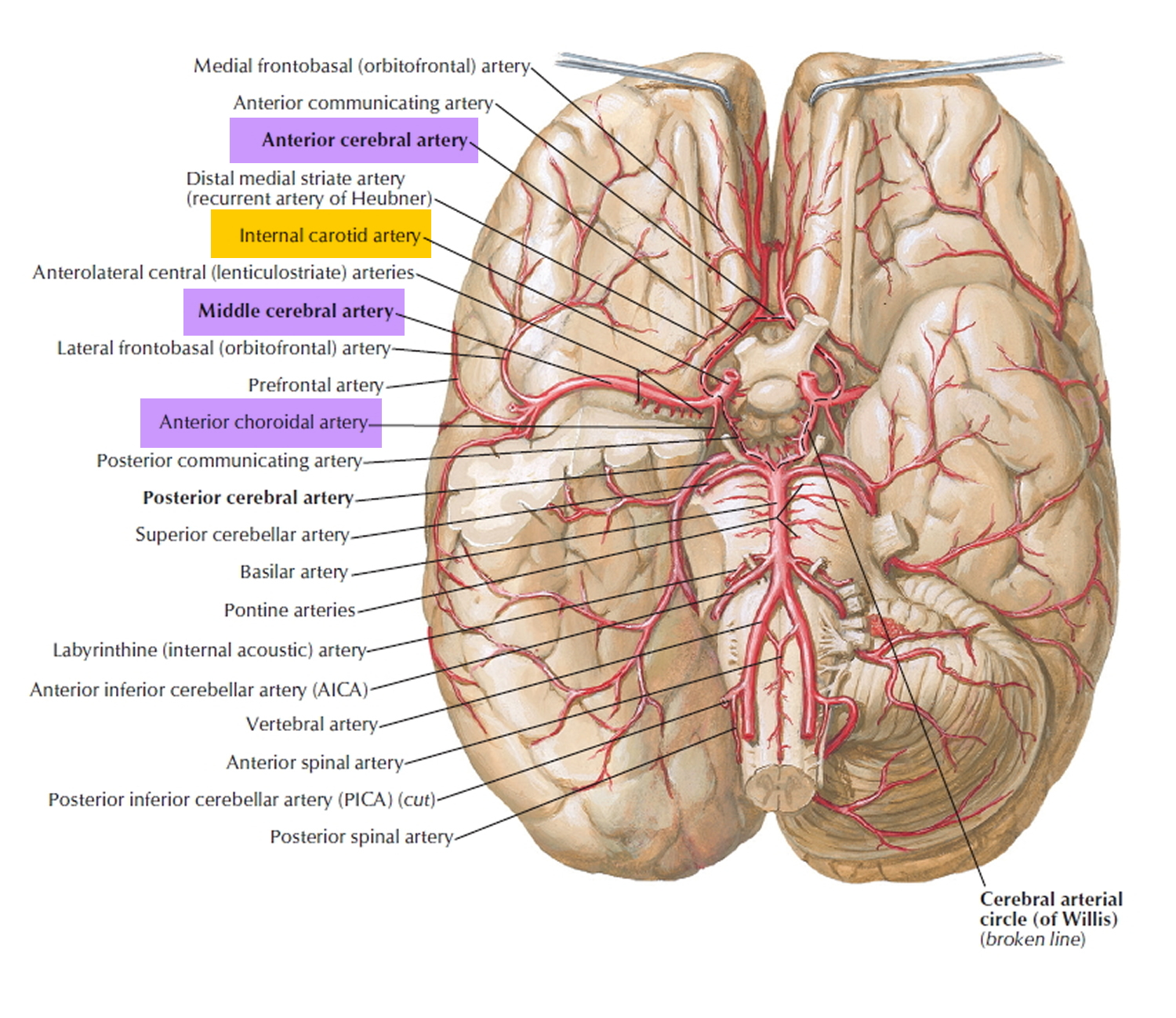
Figure 3. Medial aspect of the human brain
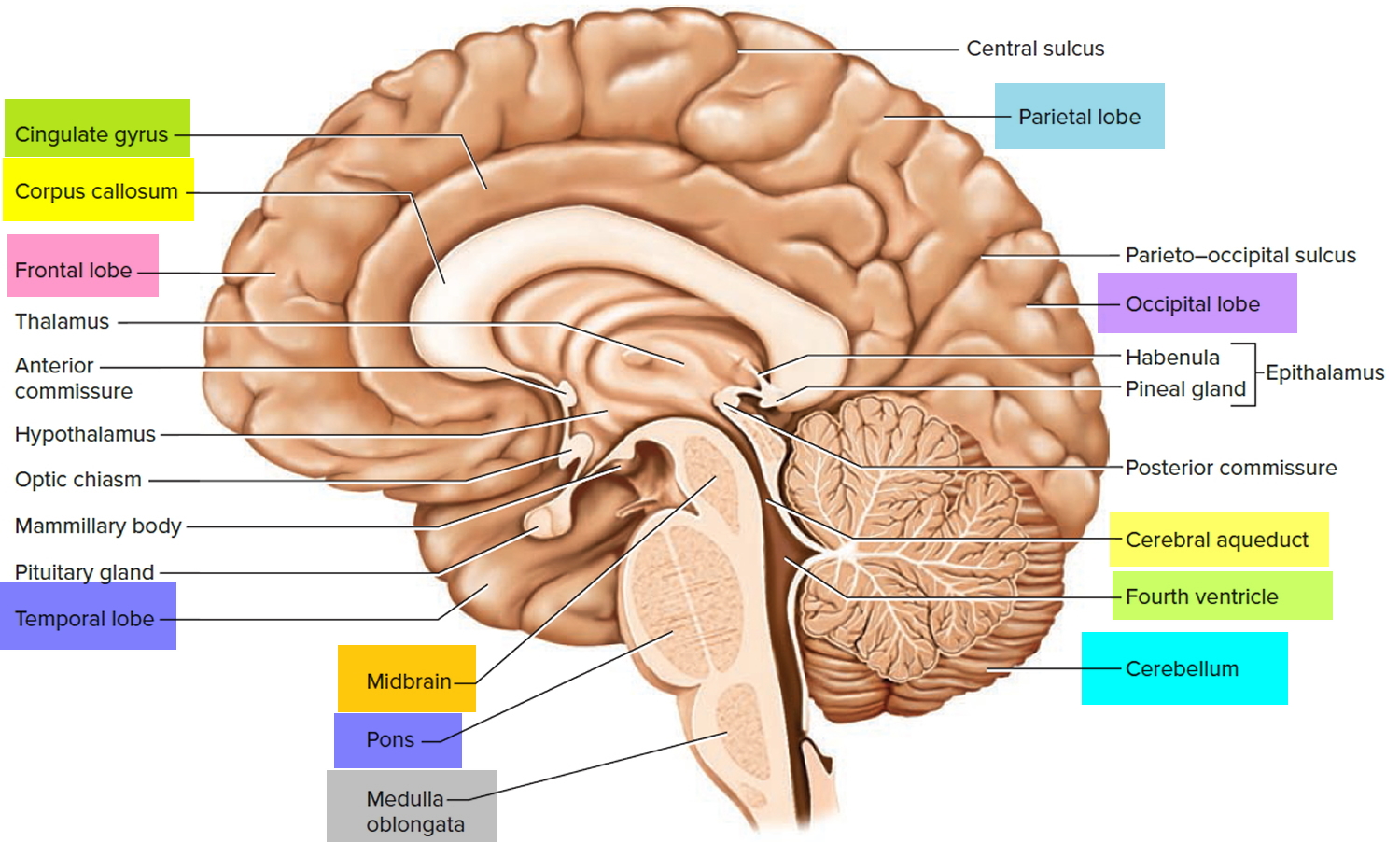
Figure 4. Basal ganglia of human brain
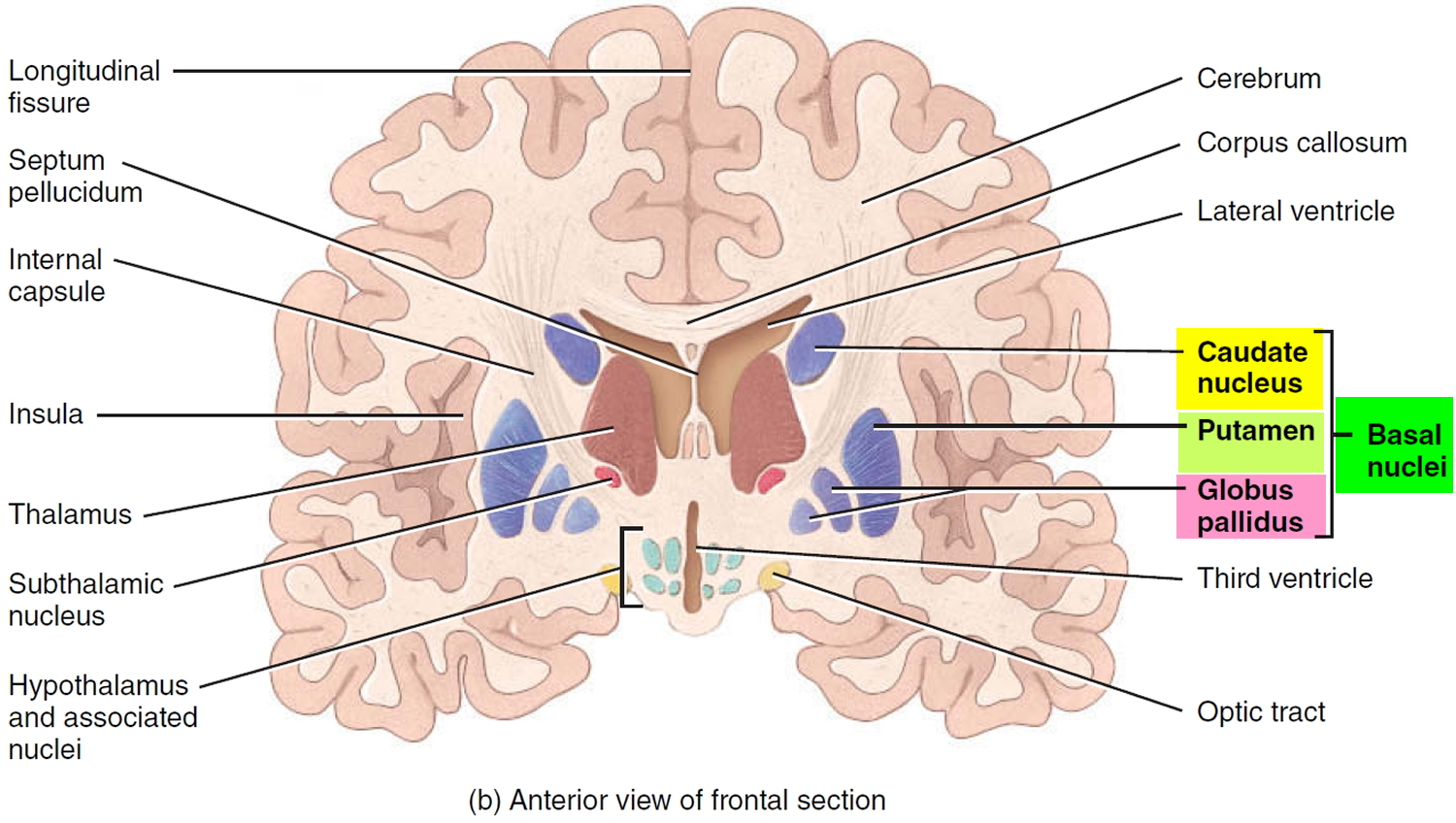
Figure 5. Moyamoya brain disease
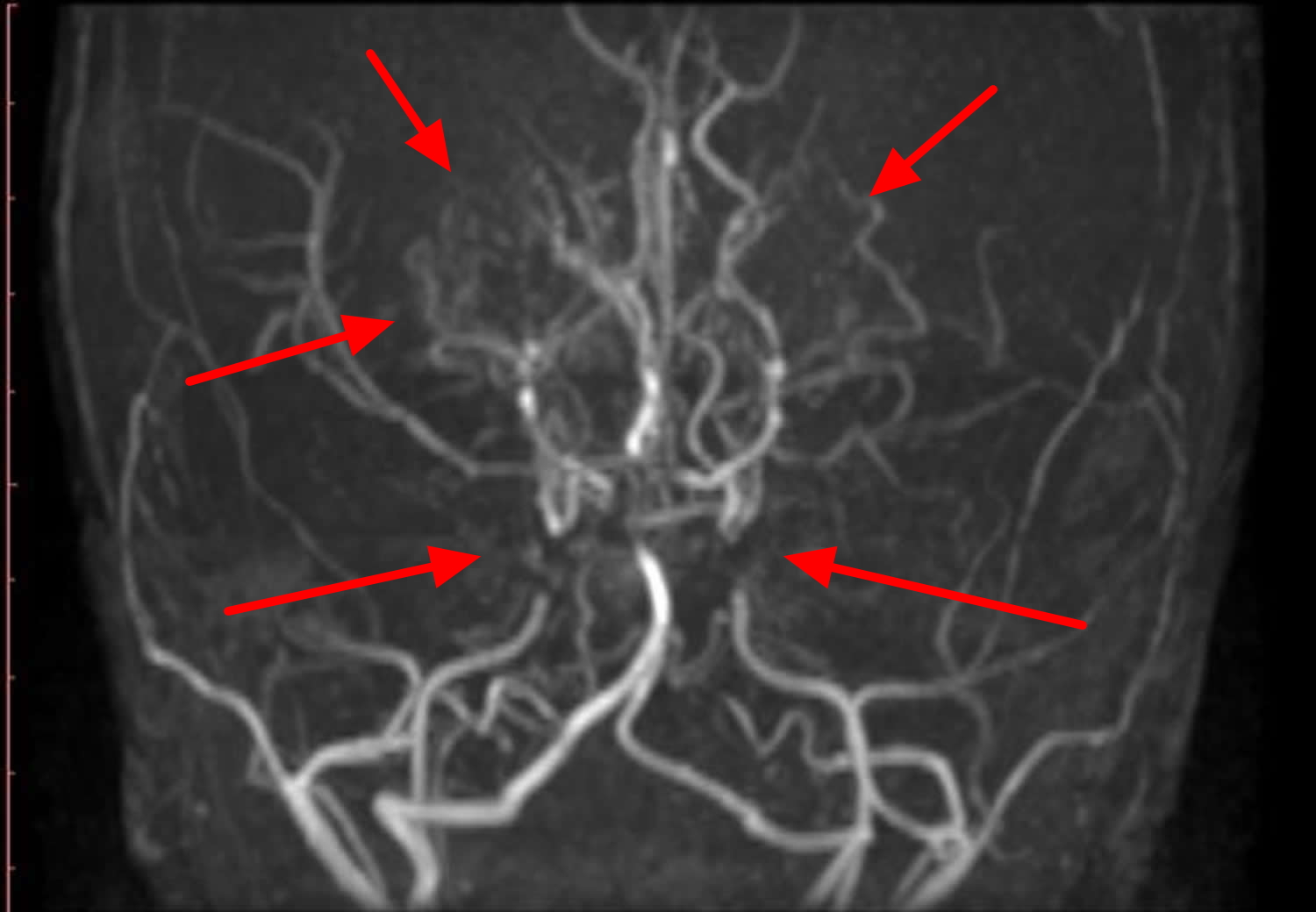
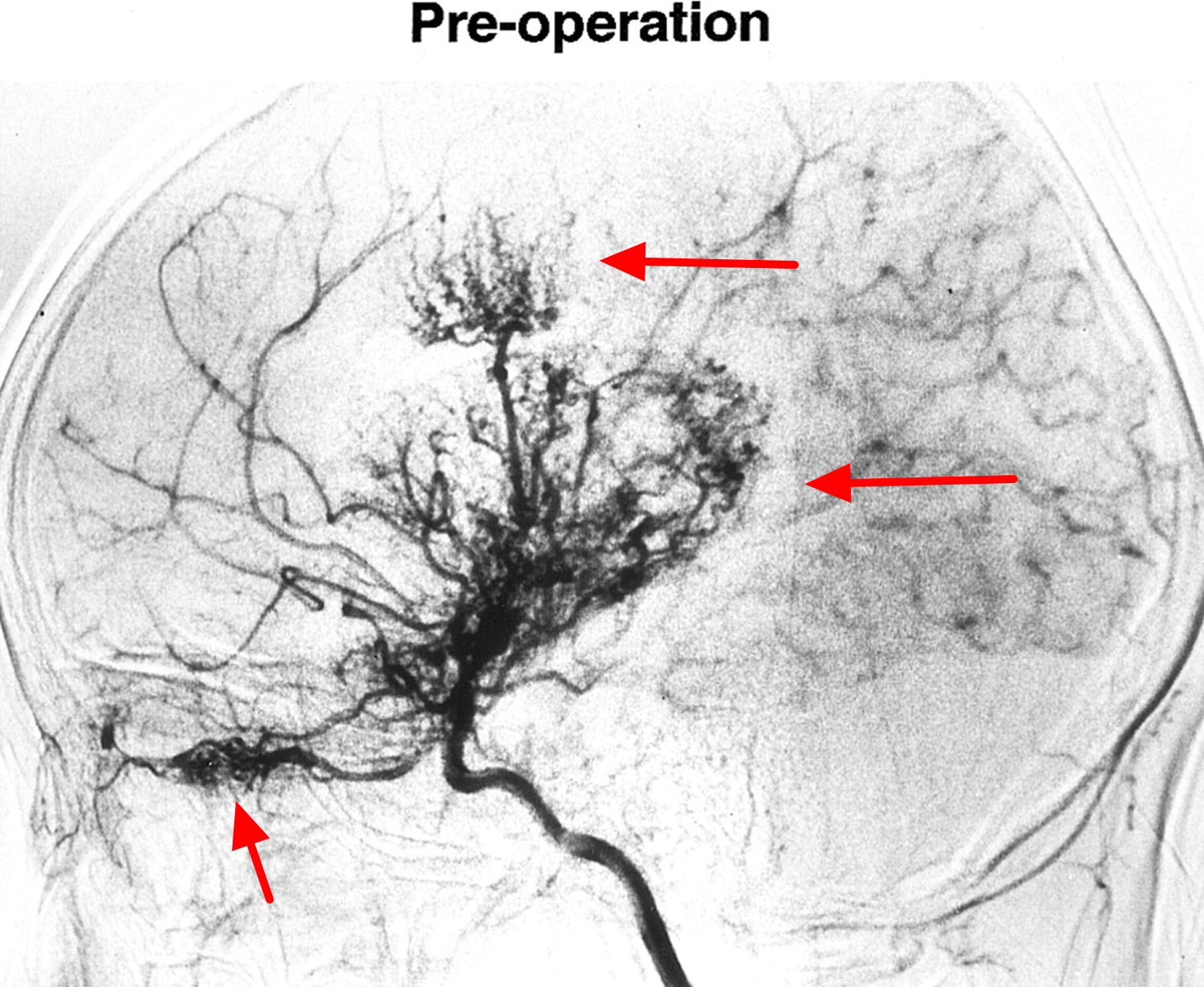
Note: Angiogram confirms extensive perforator colaterals giving the ‘puff of smoke’ characteristic of this disease, and involving both anterior and posterior circulation.
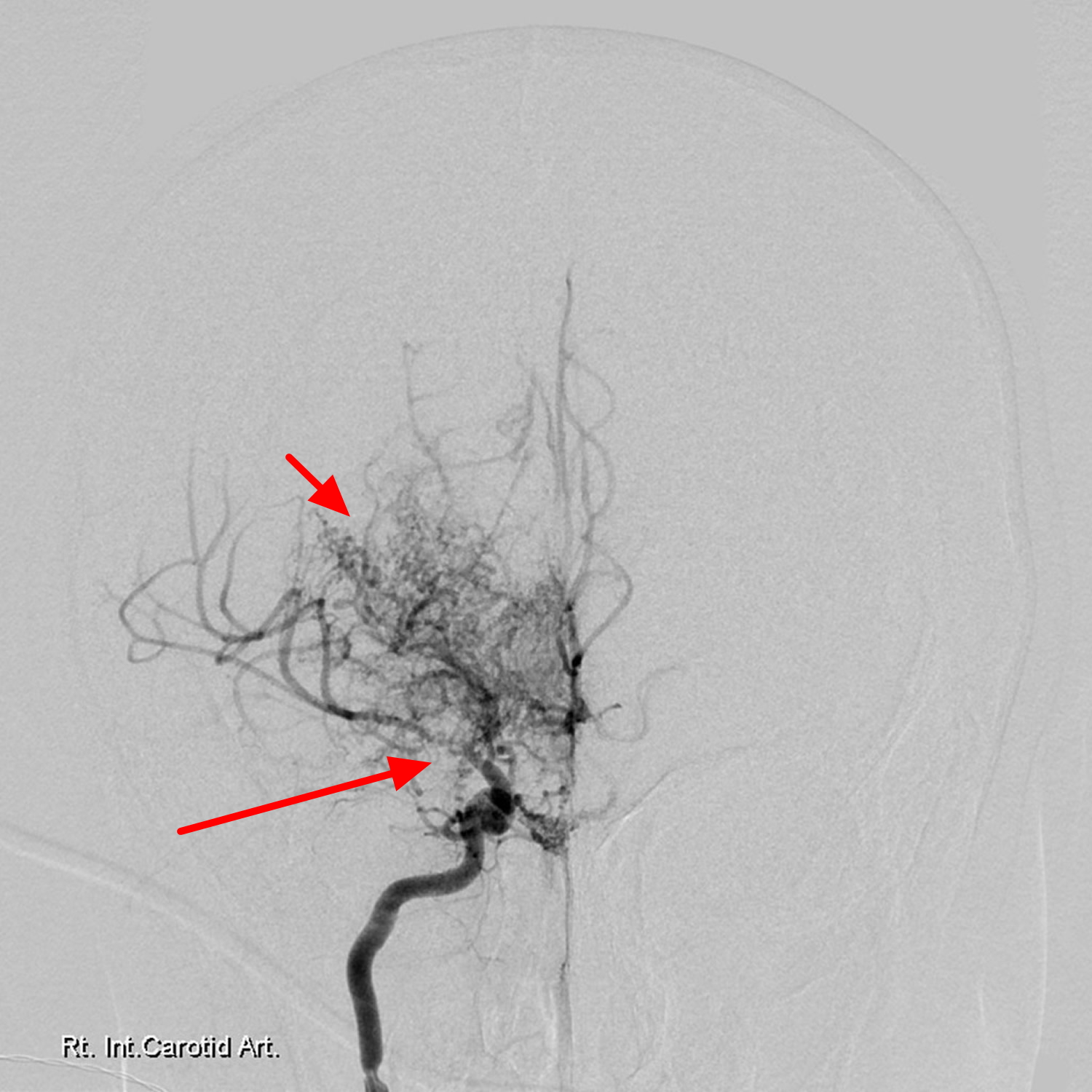
Figure 6. Moyamoya brain disease – note “puff of smoke” in the basal ganglia and thalamus
Note:
MR angiography of the brain, revealed:
- attenuated intracranial internal carotid artery on either side with occluded their cavernous and supraclinoid segments
- occluded left middle cerebral artery and attenuated right middle cerebral artery
- dilated and extensive lenticulo-striate and thalamo-striate collaterals are seen in the basal ganglia and thalamic regions (puff of smoke)
- no aneurysmal dilatation or AV (arterio-venous) malformation
- normal vertebro-basilar system
Figure 7. Moyamoya disease – bilateral watershed brain infarcts
Moyamoya disease staging system
The staging system for moyamoya disease first described by Suzuki and Takaku in their seminal 1969 article 8 is still in use today. Formally, the staging refers to findings on conventional angiography, although there are efforts to apply similar systems to MR angiography 9.
Suzuki stage appears to correlate with collateralization in children, but not in adults 10.
The vast majority of patients will progress through some or all of the Suzuki stages, although progression may occur at different rates5, and appears to occur more rapidly in children than in adolescents or adults 11.
The Suzuki stages of Moyamoya Disease are as follows:
- Stage I
- “narrowing of the carotid fork” *
- narrowed internal carotid artery bifurcation
- Stage II
- “initiation of the moyamoya”
- dilated anterior cerebral artery, middle cerebral artery and narrowed internal carotid artery bifurcation with moyamoya change
- Stage III
- “intensification of the moyamoya”
- further increase in moyamoya change of the internal carotid artery bifurcation and narrowed anterior cerebral artery and middle cerebral artery
- Stage IV
- “minimization of the moyamoya”
- moyamoya change reducing with occlusive changes in internal carotid artery and tenuous anterior cerebral artery and middle cerebral artery
- Stage V
- “reduction of the moyamoya”
- further decrease in moyamoya change with occlusion of internal carotid artery, anterior cerebral artery and middle cerebral artery
- Stage VI
- “disappearance of the moyamoya”
- internal carotid artery essentially disappeared with supply of brain from external carotid artery
* the description in inverted commas is that of Suzuki in the original paper.
Moyamoya disease prognosis
Without surgery, the majority of individuals with Moyamoya disease will experience mental decline and multiple strokes because of the progressive narrowing of arteries. Without treatment, Moyamoya disease can be fatal as the result of intracerebral hemorrhage (bleeding within the brain).
Long-term prognosis for patients with non-surgically treated Moyamoya disease is not fully understood. However, some reports have described its natural clinical course and the results of conservative treatment. Kuroda et al. 12 reported a disease progression rate of approximately 20% over 6 years. Being female was identified as an independent risk factor for disease progression by multivariate analysis. Other investigations on the progression rate of the unaffected side of surgically treated unilateral Moyamoya disease reported that six of the 41 cases (14.6%) exhibited contralateral progression during the mean follow-up of 34 months 13. Considering these reports, Moyamoya disease seems to have a progressive nature. Among many studies examining risk factors for Moyamoya disease progression, the presence of thyroid disease such as Graves’ disease has been a well-known medical condition linked to rapid progression of Moyamoya disease 14. Recently, the RNF213 variant was suggested as a possible causative genetic alteration leading to the development as well as progression of Moyamoya disease 15.
Moyamoya disease life expectancy
Moyamoya disease is progressive and without treatment can be fatal due to intracerebral hemorrhage 16. The outcome of Moyamoya disease depends on the severity and nature of the hemorrhage; the prognosis depends on recurrent attacks. Without surgery, the majority of affected people experience recurrent strokes and gradual deterioration of cognitive function. In studies with long-term follow-up of untreated patients, progressive neurologic deficits and poor outcome were reported in 50 to 66 percent 17. The overall mortality rate from Moyamoya disease is about 10% in adults, and 4.3% in children 18.
Patients with Moyamoya disease who present for treatment while symptoms are evolving have a better prognosis than do those who present with static symptoms (which probably indicate a completed stroke).
Moyamoya disease complications
Most complications from moyamoya disease are associated with the effects of stroke, such as:
- Vision problems. As a result of stroke, some people with moyamoya disease experience visual disturbances.
- Weakness (hemiparesis).
- Language disturbance (aphasia).
- Movement disorders. Though rare, some people with moyamoya disease experience involuntary movement of certain muscles.
- Learning or developmental issues. Following a stroke, a child may have problems with mental processing, which can affect schoolwork as well as cause emotional difficulties and low self-esteem. Adults may experience memory decline as well as challenges with other areas of cognitive function.
- Seizures.
Moyamoya disease causes
The causes of moyamoya disease are unknown. However, it is known that the disorder may appear as an isolated, primary disorder that may have genetic determinants or may occur in association with a number of different underlying disorders, as noted above. It is likely that the phenotypic arteriopathy of moyamoya actually represents a common end-pathway of a number of pathophysiologically distinct processes.
Primary moyamoya disease may be genetically transmitted as an autosomal recessive trait, and accounts for approximately 10% of all cases in Japan. Recently, two major mutations have been reported to be associated with specific subpopulations of moyamoya patients. The first, R179 mutations in the ACTA2 gene, correlate with a radiographically distinct subtype of moyamoya disease, identified in a very small cohort of patients related to a larger group of ACTA2 mutations that cause cardiac and aortic disorders 19. More significantly, mutations in RNF213 are strongly associated with the classic East Asian, bilateral, idiopathic familial disease presenting in adulthood and may be present in up to 70% of all East Asian familial cases of moyamoya 20.
Changes in the RNF213 gene involved in moyamoya disease replace single protein building blocks (amino acids) in the RNF213 protein. The effect of these changes on the function of the RNF213 protein is unknown, and researchers are unsure how the changes contribute to the narrowing of blood vessels or the characteristic blood vessel growth of moyamoya disease. For unknown reasons, people with moyamoya disease have elevated levels of proteins involved in cell and tissue growth, including the growth of blood vessels (angiogenesis). An excess of these proteins could account for the growth of new blood vessels characteristic of moyamoya disease. It is not clear if changes in the RNF213 gene are involved in the overproduction of these proteins.
Secondary moyamoya disease
Secondary moyamoya disease occurs in association with a number of different underlying disorders or conditions, including certain infections involving the central nervous system, neurofibromatosis type I, sickle cell disease, and Down syndrome, although there is now a long list of conditions now published in the medical literature with which moyamoya disease is associated. In susceptible patients, the disease may occur following radiation therapy to the brain to treat certain brain tumors such as optic glioma or craniopharyngioma. Unlike primary moyamoya disease, the disease can occasionally present with angiographic changes involving only on one side. This process can remain unilateral, or – in about 30% of patients – progress to involve the other side.
Moyamoya syndrome, also termed the moyamoya pattern or phenomenon, is due to numerous conditions that can cause arterial occlusion of the circle of Willis, with resultant collaterals, and appearances reminiscent of moyamoya disease. These conditions include 21:
Vessel wall abnormalities
- Atherosclerosis 22
- Radiation induced vasculopathy
- Fibromuscular dysplasia
- Marfan syndrome
- Ehlers-Danlos syndrome
Phakomatoses
- Neurofibromatosis type 1 (NF1)
- Tuberous sclerosis
Connective tissue disorders
- Systemic lupus erythematosus (SLE)
- Antiphospholipid syndrome
Blood dyscrasias
- Sickle cell disease
- Essential thrombocytopaenia 23
- Polycythaemia rubra vera 24
- Aplastic anaemia
- Fanconi anaemia
Infection
- Tuberculous meningitis
- Bacterial meningitis
- Post-varicella vasculitis
- Leptospirosis
Less common causes
- Graves disease 22
- Down syndrome
- Ulcerative colitis (UC)
- Apert syndrome
- Oral contraceptive use
Risk factors for Moyamoya disease
Though the cause of moyamoya disease is unknown, certain factors may increase your risk of having the condition, including:
- Being of Asian descent. Moyamoya disease is found all over the world, but it’s more common in East Asian countries, especially Korea, Japan and China. This may possibly be due to certain genetic factors in those populations. Higher rates of moyamoya disease have been documented among Asians living in western countries.
- Having a family history of moyamoya disease. If you have a family member with moyamoya disease, your risk of having the condition is 30 to 40 times higher than the general population — a factor that strongly suggests a genetic component to the disease and may justify screening of family members.
- Having a certain medical condition. Moyamoya disease sometimes occurs in association with another disorder, including neurofibromatosis type 1, sickle cell anemia and Down syndrome, among others.
- Being female. Females have a slightly higher incidence of moyamoya disease.
- Being young. Though adults can have moyamoya disease, children younger than 15 years old are most commonly affected.
Moyamoya disease symptoms
Moyamoya disease may occur at any age, though symptoms most commonly occur between 5 and 10 years of age in children and between 30 and 50 years of age in adults.
The first symptom of moyamoya disease is usually stroke or recurrent transient ischemic attacks (TIAs), especially in children. Adults may also experience these symptoms but more often experience bleeding in the brain (hemorrhagic stroke) from abnormal brain vessels.
Accompanying signs and symptoms of moyamoya disease related to reduced blood flow to the brain include:
- Headache
- Seizures
- Weakness, numbness or paralysis in your face, arm or leg, typically on one side of your body
- Visual disturbances
- Difficulties with speaking or understanding others (aphasia)
- Developmental delays
- Involuntary movements
- Cognitive decline
These symptoms can be triggered by exercise, crying, coughing, straining or fever.
Moyamoya disease diagnosis
To diagnose moyamoya disease, your doctor will review your symptoms and your family and medical history. Your doctor will perform a physical examination and may order several tests to diagnose moyamoya disease and any underlying conditions.
In most patients, the diagnosis of moyamoya can be made from a careful assessment of an magnetic resonance imaging (MRI) and magnetic resonance angiogram (MRA). Cerebral arteriography will confirm the diagnosis, establish the exact degree of blood vessel narrowing, demonstrate the existing blood flow patterns to various areas of the brain, and allow treatment decisions to be made; for these reasons, it is the standard diagnostic tool for this condition.
Tests may include:
- Magnetic resonance imaging (MRI). An MRI uses powerful magnets and radio waves to create detailed images of your brain. Your doctor may inject a dye into a blood vessel to view your arteries and veins and highlight blood circulation (magnetic resonance angiography). If available, your doctor may recommend a type of imaging that can measure the amount of blood passing through the vessels (perfusion MRI).
- Computerized tomography (CT) scan. A CT scan uses a series of X-rays to create a detailed image of your brain. Your doctor may inject a dye into a blood vessel to highlight blood flow in your arteries and veins (CT angiogram).
- Cerebral angiography. During a cerebral angiogram, your doctor inserts a long, thin tube (catheter) into a blood vessel in your groin and guides it to your brain using X-ray imaging. Your doctor then injects dye through the catheter into the blood vessels of your brain to make them visible under X-ray imaging.
- Transcranial Doppler ultrasound. In a transcranial Doppler ultrasound, sound waves are used to obtain images of your brain. Doctors may use this test to obtain information about the blood vessels in the brain.
- Positron emission tomography (PET) scan or single-photon emission computerized tomography (SPECT). In these tests, your doctor injects you with a small amount of a safe radioactive material and places emission detectors over your brain. PET provides visual images of brain activity. SPECT measures blood flow to various regions of your brain.
- Electroencephalography (EEG). An EEG monitors the electrical activity in your brain via a series of electrodes attached to your scalp. Children with moyamoya disease often exhibit abnormalities on EEG.
If necessary, your doctor may order other tests to rule out other conditions.
Moyamoya disease treatment
Doctors will evaluate your condition and determine the most appropriate treatment for your condition. The goal of treatment is to reduce your symptoms, improve your blood flow and lower your risk of serious complications such as an ischemic stroke caused by a lack of blood flow, bleeding in your brain (intracerebral hemorrhage) or death.
Your treatment may include:
Medication
Medical treatment of moyamoya disease has been utilized to treat many of the symptoms of moyamoya, and is often an important part of the patient’s management. Treatment measures include aspirin (to prevent or reduce the development of small blood clots developing within the narrowed vessels), calcium channel blockers (which may improve symptoms of headache and in some patients reduce symptoms related to transient ischemic attacks), and anti-seizure medications (when indicated because of a patient’s seizure disorder). In rare instances, anticoagulants such as lovenox or coumadin are administered in very unstable patients having frequent symptoms, but because of the obvious risk of cerebral bleeding in this condition, they are rarely indicated as long-term measures. There is no medication available which will stop the progression of the cerebral artery narrowing, however, and the disease will continue to progress in the vast majority of patients regardless of treatment.
Medications may be prescribed to reduce the risk of stroke or to aid in seizure control, including:
- Blood thinners. After you’re diagnosed with moyamoya disease, if you have mild or no symptoms at first, then your doctor may recommend you take aspirin or other blood thinner to prevent strokes.
- Calcium channel blockers. Also known as calcium antagonists, this type of medication may improve symptoms of headache and possibly reduce symptoms related to transient ischemic attacks.
- Anti-seizure medications. These may be prescribed if you or your child has an accompanying seizure disorder.
Because surgical revascularization has been recommended for symptomatic patients with impaired hemodynamics, some studies have described the outcomes of conservative treatment among asymptomatic or hemodynamically stable patients with Moyamoya disease. A multi-center, nationwide survey for conservative treatment results was conducted in 2007 in Japan 25. The authors reported the annual stroke rate as 3.2% from the observation of 34 asymptomatic patients conservatively followed over 44 months 25. Hemodynamic disturbance was revealed to be a risk factor for newly developed stroke 25. In a North American series, the rates of annual ischemic and hemorrhagic stroke rate were reported as 13.3% and 1.7%, respectively. Being female and smoking were risk factors for stroke development 26. Cho et al. 27 reported an annual stroke rate of 4.5% among 241 hemodynamically stable patients with Moyamoya disease over 83 months. The annual stroke rate was higher in the hemorrhagic presentation group (5.7%) than the ischemic presentation group (4.2%) or the asymptomatic group (3.4%). They found familial disease and thyroid disease to be risk factors affecting stroke occurrence. As for ischemic presenting Moyamoya disease, 5.6% of the annual ischemic stroke rate also reported that posterior circulation involvement was a strong risk factor for ischemic stroke 28.
Antiplatelet treatment for preventing stroke in patients with Moyamoya disease had been utilized by many physicians, especially in non-Asian areas. According to the reports of a worldwide survey, 31% of responders agreed to use long-term acetylsalicylic acid 29. However, the evidence for antiplatelet treatment is lacking. Recently, the efficacy of antiplatelet therapy for preventing stroke was investigated in a cohort study with a large sample size. According to the authors, antiplatelet therapy could not prevent recurrent cerebral infarction for ischemic presenting patients with Moyamoya disease. The nature of the ischemic insult in patients with Moyamoya disease is not an embolic infarction, but instead is mainly a hemodynamic infarction. The pathologic changes of the Moyamoya disease vessels near the internal carotid artery bifurcation are not a type of endothelial damage, which is prone to platelet adhesion. Therefore, theoretically, antiplatelet drugs will not be effective for preventing ischemic stroke in patients with Moyamoya disease. Although antiplatelet users are subject to hemorrhagic complications, the therapy was not associated with an increase in cerebral hemorrhage among patients with Moyamoya disease 30. Thus, prescribing antiplatelet agents for symptomatic patients with Moyamoya disease should not yet be considered as an alternative treatment.
Revascularization surgery
If your symptoms become worse or if tests show evidence of low blood flow, your doctor may recommend revascularization surgery. Surgical procedures are designed to reestablish blood supply to the brain by diverting scalp blood supply to the brain surface and thereby circumventing the progressive loss of brain hemisphere blood flow.
Bypassing the occlusive segments is the aim of most surgical therapy. There are several types of surgery that can restore blood flow (revascularization) to the brain by opening narrowed blood vessels or by bypassing blocked arteries. Children usually respond better to revascularization surgery than adults, but the majority of individuals have no further strokes or related problems after surgery.
There are many surgical procedures proposed to treat moyamoya, and they have been divided into so-called “indirect” and “direct” operations. Indirect procedures, usually carried out in children and younger patients, include pial synangiosis, encephalomyosynangiosis (EMS), encephaloduroarteriosynangiosis (EDAS), dural inversion, and other similar variants. These operations involve the placement of vascularized structures from the scalp and/or the membranes that surround the brain onto the brain surface, which in most moyamoya patients will induce the growth of new blood vessels into the brain. The most common direct procedure involves the direct suturing of a scalp blood vessel, the superficial temporal artery, to a middle cerebral artery branch on the brain surface. Long-term results following surgery of either type have been quite good, with long-term prevention of strokes seen in published series of both pediatric and adult patients.
In adults external carotid artery to middle cerebral artery (ECA-MCA) anastomoses can be performed as the vessels are larger. One of the surgical option is superficial temporal artery to middle cerebral artery (STA-MCA) bypass.
Encephaloduroarteriosynangiosis is the treatment of choice in pediatric patients as their vessels are too small to allow direct anastomosis.
Direct revascularization procedures
In direct revascularization surgery, surgeons stitch (suture) the scalp artery directly to a brain artery (superficial temporal artery to middle cerebral artery bypass surgery) to increase blood flow to your brain immediately.
Direct bypass surgery may be difficult to perform in children, due to the size of the blood vessels to be attached.
Direct revascularization surgery has a risk of complications, including stroke.
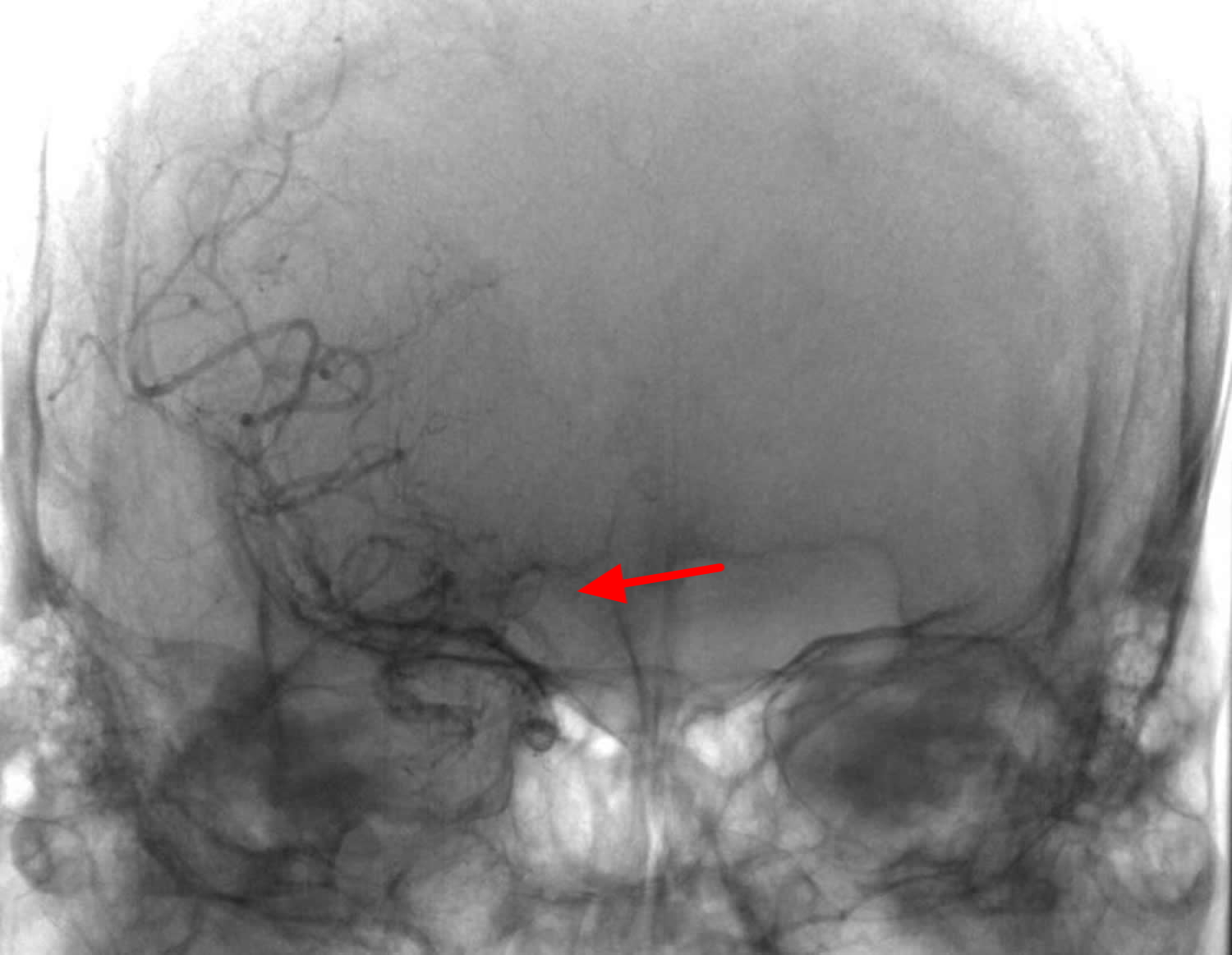
Figure 8. Moyamoya disease – direct revascularization surgery
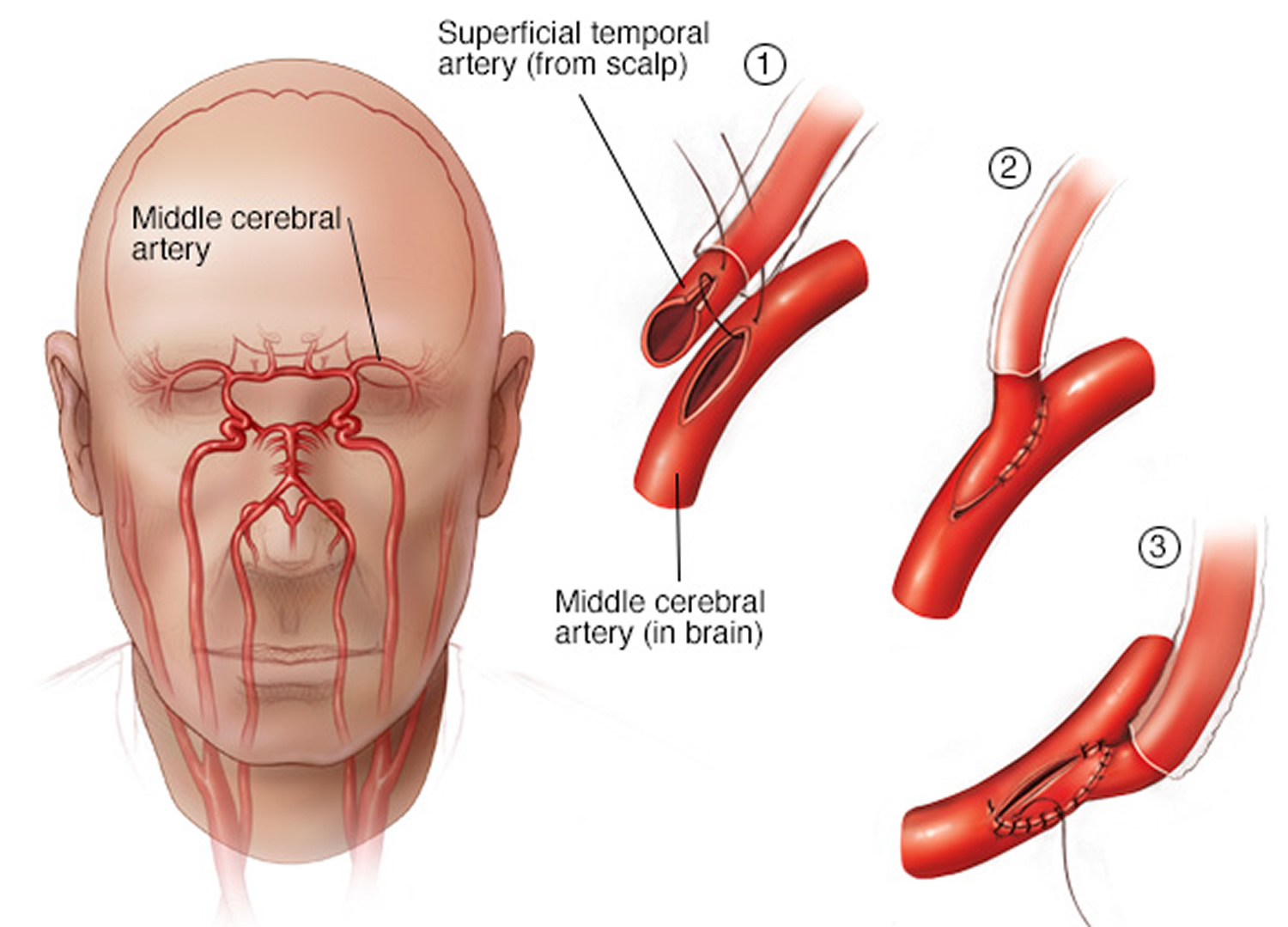 Figure 9. Post-operative angiography of the external carotid artery. Black arrowheads indicate the superficial temporal artery (donor artery). The tip of the black arrow is the anastomosis site to the angular artery (recipient artery). The middle cerebral artery is supplied from the superficial temporal artery with a reverse direction (white arrowheads).
Figure 9. Post-operative angiography of the external carotid artery. Black arrowheads indicate the superficial temporal artery (donor artery). The tip of the black arrow is the anastomosis site to the angular artery (recipient artery). The middle cerebral artery is supplied from the superficial temporal artery with a reverse direction (white arrowheads).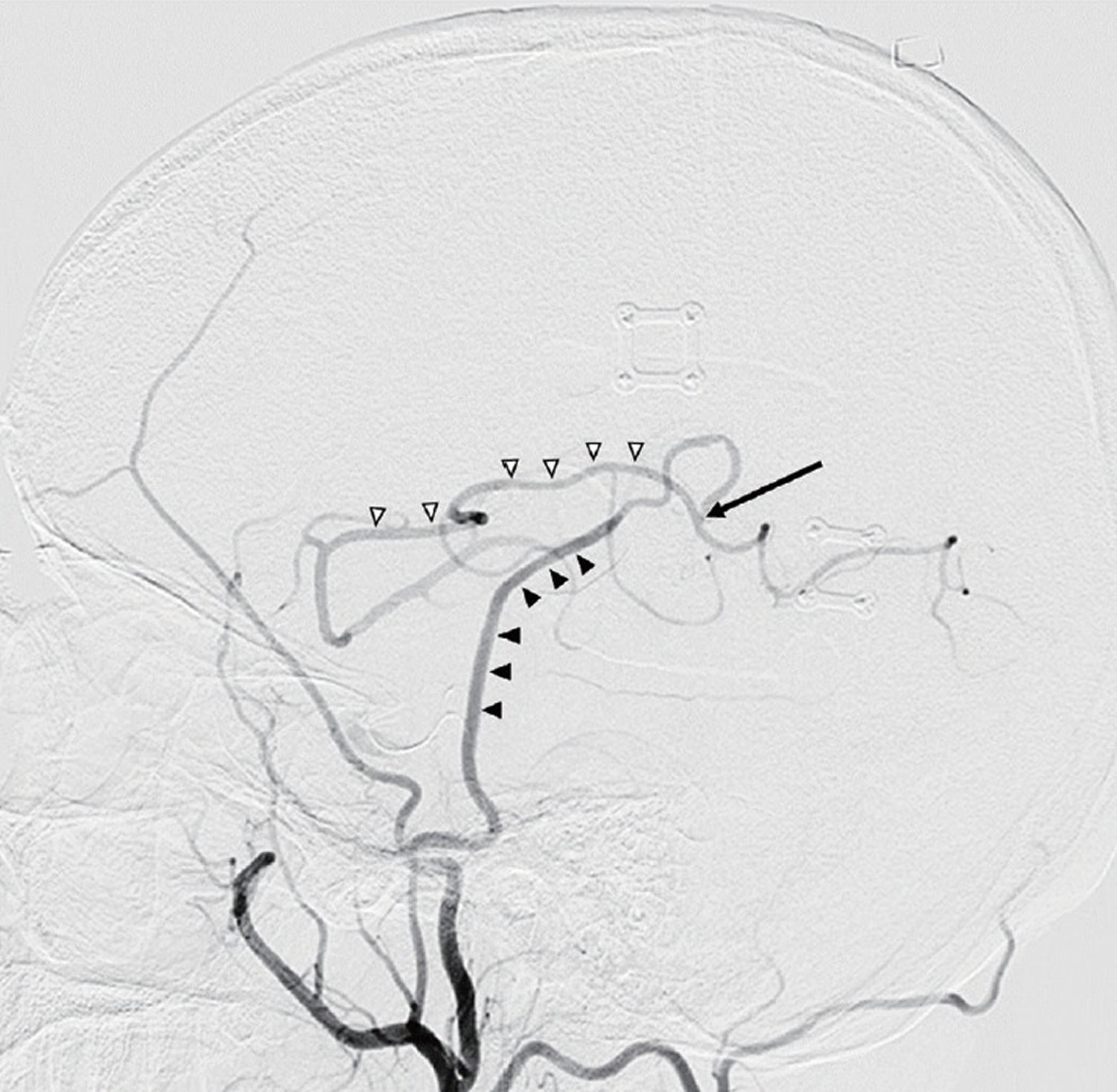
Indirect revascularization procedures
In indirect revascularization, the goal is to increase blood flow to your brain gradually over time.
Types of indirect revascularization procedures include encephaloduroarteriosynangiosis or encephalomyosynangiosis, or a combination of both.
In encephaloduroarteriosynangiosis, your surgeon separates (dissects) a scalp artery over several inches.
Your surgeon makes a small temporary opening in your skull directly beneath the artery and attaches (sutures) the intact scalp artery to the surface of your brain, which allows blood vessels from the artery to grow into your brain over time. The surgeon then replaces the bone and closes the opening in your skull.
In encephalomyosynangiosis, your surgeon separates (dissects) a muscle in the temple region of your forehead and places it onto the surface of your brain through an opening in your skull to help restore blood flow.
Your surgeon may perform encephalomyosynangiosis with encephaloduroarteriosynangiosis. In this procedure, your surgeon separates (dissects) a muscle in the temple region of your forehead and places it onto the surface of your brain, after attaching the scalp artery to the surface of your brain. The muscle helps to hold the artery in place as blood vessels grow into your brain over time.
Your surgeon may peel the outer layer of your skull bone (pericranium), which may serve as an additional source of new blood vessels to the brain. This may be important in areas that cannot be reached by a scalp artery.
Your surgeon may make multiple holes (burr holes) in your skull to allow new blood vessels to grow, either as a separate procedure or in combination with other procedures.
Other Surgery
Some people with moyamoya disease develop a bulge or ballooning of a blood vessel in the brain known as a brain aneurysm. If this occurs, surgery may be necessary to prevent or treat a ruptured brain aneurysm.
Physical therapy
To address the physical and psychological effects of stroke on you or your child, your doctor may recommend other therapies.
Physical and occupational therapy can help to attempt to regain any lost physical function caused by stroke. Speech therapy also may be recommended if needed.
Cognitive behavioral therapy can help address emotional issues related to having moyamoya disease, such as how to cope with fears and uncertainties about future stroke.
- Yoon HK, Shin HJ, Chang YW. “Ivy sign” in childhood moyamoya disease: depiction on FLAIR and contrast-enhanced T1-weighted MR images. Radiology. 2002;223 (2): 384-9. doi:10.1148/radiol.2232011094 https://www.ncbi.nlm.nih.gov/pubmed/11997541[↩]
- Horie N, Morikawa M, Nozaki A et-al. “Brush Sign” on susceptibility-weighted MR imaging indicates the severity of moyamoya disease. AJNR Am J Neuroradiol. 2011;32 (9): 1697-702. doi:10.3174/ajnr.A2568 http://www.ajnr.org/content/32/9/1697.long[↩]
- Kornienko VN, Pronin IN. Diagnostic Neuroradiology. Springer Verlag. (2008) ISBN:3540756523.[↩][↩]
- NINDS Moyamoya Disease Information Page. National Institute of Neurological Disorders and Stroke (NINDS). https://www.ninds.nih.gov/Disorders/All-Disorders/Moyamoya-Disease-Information-Page[↩]
- Smith ER & Scott RM. Moyamoya: epidemiology, presentation, and diagnosis. Neurosurg Clin N Am. July 2010. https://www.ncbi.nlm.nih.gov/pubmed/20561502[↩]
- Edward Smith. Moyamoya Disease. Boston Children’s Hospital. http://www.childrenshospital.org/conditions-and-treatments/conditions/m/moyamoya-disease[↩]
- Moyamoya syndrome. NORD. https://rarediseases.org/rare-diseases/moyamoya-disease/[↩]
- Jiro Suzuki, Akira Takaku. Cerebrovascular “Moyamoya” Disease: Disease Showing Abnormal Net-Like Vessels in Base of Brain. Arch Neurol. 1969;20(3):288-299.[↩]
- Houkin K, N Nakayama, S Kuroda, et al. Novel Magnetic Resonance Angiography Stage Grading for Moyamoya Disease. 2005;20 (5): 347–54. . doi:10.1159/000087935. https://www.karger.com/Article/Abstract/87935[↩]
- Suzuki J and N Kodama. Moyamoya disease–a review. 1983;14 (1): 104–9. . doi:10.1161/01.STR.14.1.104. http://stroke.ahajournals.org/content/14/1/104.full.pdf[↩]
- Houkin K, T Yoshimoto, S Kuroda, et al. Angiographic analysis of moyamoya disease–how does moyamoya disease progress? Neurol Med Chir (Tokyo). 1996;36 (11): 783–787; discussion 788.[↩]
- Kuroda S, Ishikawa T, Houkin K, Nanba R, Hokari M, Iwasaki Y. Incidence and clinical features of disease progression in adult moyamoya disease. Stroke. 2005;36:2148–2153. http://stroke.ahajournals.org/content/36/10/2148.long[↩]
- Lee SC, Jeon JS, Kim JE, Chung YS, Ahn JH, Cho WS, et al. Contralateral progression and its risk factor in surgically treated unilateral adult moyamoya disease with a review of pertinent literature. Acta Neurochir (Wien) 2014;156:103–111. https://www.ncbi.nlm.nih.gov/pubmed/24201757[↩]
- Kim SJ, Heo KG, Shin HY, Bang OY, Kim GM, Chung CS, et al. Association of thyroid autoantibodies with moyamoya-type cerebrovascular disease: a prospective study. Stroke. 2010;41:173–176. http://stroke.ahajournals.org/content/41/1/173.long[↩]
- Mineharu Y, Takagi Y, Takahashi JC, Hashikata H, Liu W, Hitomi T, et al. Rapid progression of unilateral moyamoya disease in a patient with a family history and an RNF213 risk variant. Cerebrovasc Dis. 2013;36:155–157. https://www.karger.com/Article/FullText/352065[↩]
- Moyamoya Disease Information Page. NINDS. https://www.ninds.nih.gov/Disorders/All-Disorders/Moyamoya-Disease-Information-Page[↩]
- Nijasri Charnnarong Suwanwela. Moyamoya disease: Treatment and prognosis. UpToDate. Waltham, MA:[↩]
- Roy Sucholeiki. Moyamoya Disease. Medscape Reference. http://emedicine.medscape.com/article/1180952-overview[↩]
- Munot P, Saunders DE, Milewicz DM, et al. A novel distinctive cerebrovascular phenotype is associated with heterozygous Arg179 ACTA2 mutations. Brain 2012 135(Pt 8): 2506–14.[↩]
- Kamada F, Aoki Y, Narisawa A, et al. A genome-wide association study identifies RNF213 as the first Moya-moya disease gene. J Hum Genet 2011; 56: 34–40.[↩]
- Hsu SW, Chaloupka JC, Fattal D. Rapidly progressive fatal bihemispheric infarction secondary to Moyamoya syndrome in association with Graves thyrotoxicosis. AJNR Am J Neuroradiol. 2006;27 (3): 643-7. AJNR Am J Neuroradiol. http://www.ajnr.org/content/27/3/643.full[↩]
- Jiang T, Perry A, Dacey RG et-al. Intracranial atherosclerotic disease associated with moyamoya collateral formation: histopathological findings. J. Neurosurg. 2013;118 (5): 1030-4. doi:10.3171/2013.1.JNS12565 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4598180/[↩][↩]
- Lazzaro MA, Cochran EJ, Lopes DK et-al. Moyamoya syndrome in an adult with essential thrombocythemia. Neurol Int. 2011;3 (1): e3. doi:10.4081/ni.2011.e3 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3141114/[↩]
- Hua le H, Dodd RL, Schwartz NE. Concurrent stenoocclusive disease of intracranial and extracranial arteries in a patient with polycythemia vera. Case Rep Med. 29;2012: 151767. doi:10.1155/2012/151767 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3368357/[↩]
- Kuroda S, Hashimoto N, Yoshimoto T, Iwasaki Y, Research Committee on Moyamoya Disease in Japan Radiological findings, clinical course, and outcome in asymptomatic moyamoya disease: results of multicenter survey in Japan. Stroke. 2007;38:1430–1435. http://stroke.ahajournals.org/content/38/5/1430.long[↩][↩][↩]
- Gross BA, Du R. The natural history of moyamoya in a North American adult cohort. J Clin Neurosci. 2013;20:44–48. https://www.ncbi.nlm.nih.gov/pubmed/23146211[↩]
- Cho WS, Chung YS, Kim JE, Jeon JP, Son YJ, Bang JS, et al. The natural clinical course of hemodynamically stable adult moyamoya disease. J Neurosurg. 2015;122:82–89. https://www.ncbi.nlm.nih.gov/pubmed/25361479[↩]
- Noh HJ, Kim SJ, Kim JS, Hong SC, Kim KH, Jun P, et al. Long term outcome and predictors of ischemic stroke recurrence in adult moyamoya disease. J Neurol Sci. 2015;359:381–388. https://www.ncbi.nlm.nih.gov/pubmed/26671146[↩]
- Kraemer M, Berlit P, Diesner F, Khan N. What is the expert’s option on antiplatelet therapy in moyamoya disease? Results of a worldwide Survey. Eur J Neurol. 2012;19:163–167 https://www.ncbi.nlm.nih.gov/pubmed/21771204[↩]
- Yamada S, Oki K, Itoh Y, Kuroda S, Houkin K, Tominaga T, et al. Effects of Surgery and Antiplatelet Therapy in Ten-Year Follow-Up from the Registry Study of Research Committee on Moyamoya Disease in Japan. J Stroke Cerebrovasc Dis. 2016;25:340–349. https://www.ncbi.nlm.nih.gov/pubmed/26654669[↩]
- Kim T, Oh CW, Bang JS, Kim JE, Cho W-S. Moyamoya Disease: Treatment and Outcomes. Journal of Stroke. 2016;18(1):21-30. doi:10.5853/jos.2015.01739. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4747064/[↩]





{kind=link}