
Contents
What causes muscle pain
Muscle pain is common, but the understanding of its causes is still patchy. Muscle aches and pains can involve more than one muscle. Muscle pain also can involve ligaments, tendons, and fascia. Fascia are the soft tissues that connect muscles, bones, and organs 1. Muscle pain can involve a small area or your whole body, ranging from mild to excruciating. Muscle pain is a major medical problem: in the majority (60% to 85%) of the population has had (nonspecific) back pain of muscular origin at some time or other (lifetime prevalence) 2. Pain evoked by myofascial trigger points has a point prevalence of approximately 30% 3. More than 7% of all women aged 70 to 80 years suffer from the fibromyalgia 4.
Although most muscle aches and pains go away on their own within a short time, sometimes muscle pain can linger for months. Muscle pain can develop almost anywhere in your body, including your neck, back, legs and even your hands.
Muscle pain differs in many ways from pain in the skin or internal organs. These differences concern not just the underlying mechanisms, but also a number of subjective features. The main subjective differences between muscle pain and cutaneous pain are listed in the Table 1 below. One example is that pain arising in muscle tends to be referred pain more often than does pain arising in the skin. Referred pain is pain that is felt not (only) at its site of origin, but at another site some distance away. A possible mechanism of referred pain is the spread, within the spinal cord, of excitation due to the muscle lesion 5. As soon as the excitation reaches sensory posterior horn neurons that innervate an area beyond the site of the original muscle lesion, the patient feels referred pain in that area, even though none of the nociceptors in it are activated 6.
Objective differences are found at all levels of the nervous system. Thus, one cannot simply assume that the mechanisms of cutaneous pain are shared by muscle pain. An example is shown in figure 1: a stimulus delivered to the myofascial trigger point (MTrP) in the soleus muscle causes only mild local pain, while the patient feels more severe (referred) pain in the sacroiliac joint. No conclusive answers are yet available to the questions of why muscle pain is more likely than cutaneous pain to be referred, why it is usually not referred to both proximal and distal sites, and why pain referral is often discontinuous. There is, however, a well-known discontinuity of spinal topography between the C4 and T2 dermatomes.
Figure 1. Pain referral from a myofascial trigger point (MTrP) in the soleus muscle to the sacroiliac (SI) joint
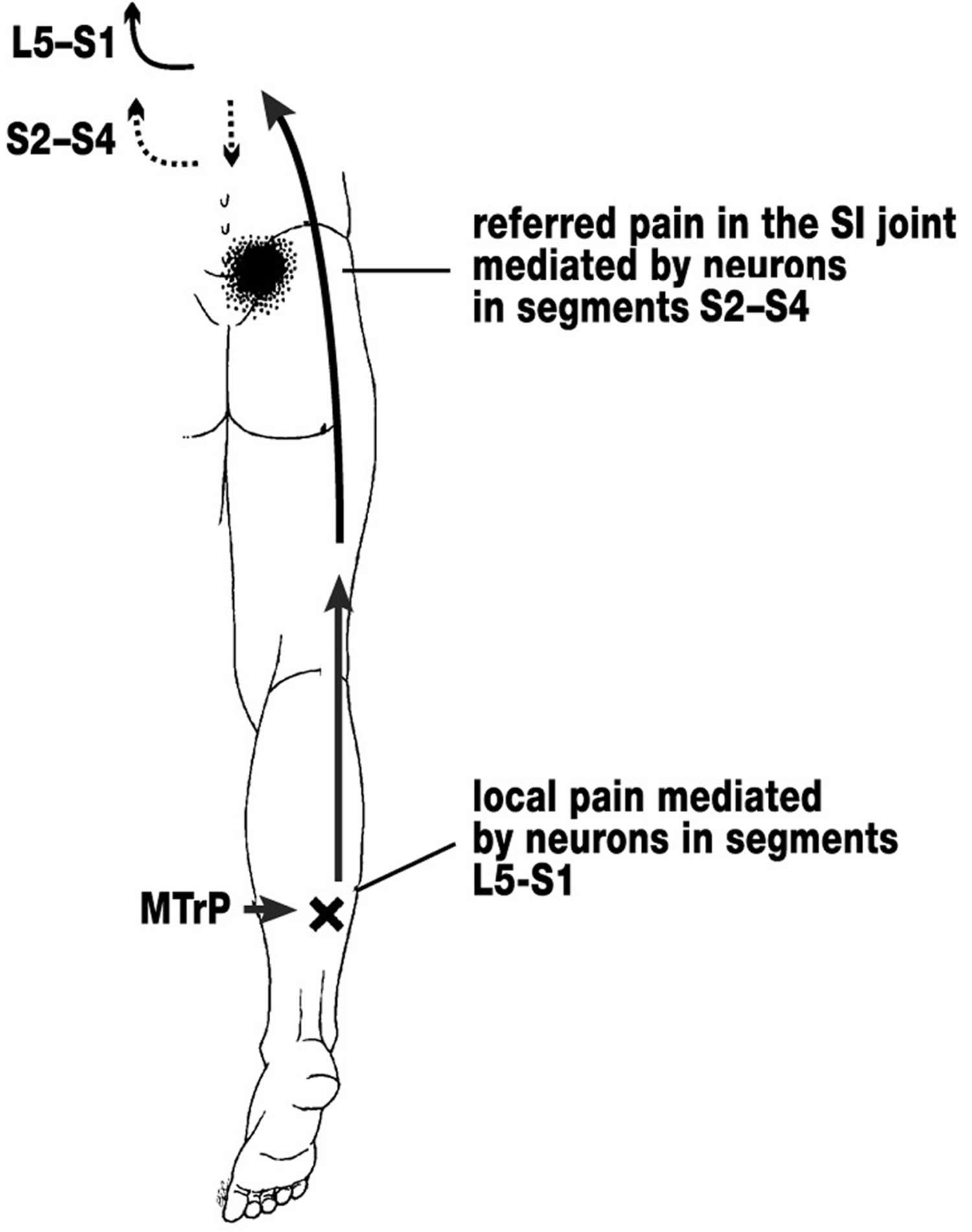
Note: Pain referral from a myofascial trigger point (MTrP) in the soleus muscle to the sacroiliac (SI) joint. As shown in figure 1, referral of pain to the sacroiliac (SI) joint can be explained as follows: first, nociceptors in the trigger point induce local pain. The nociceptive impulses arising from the trigger point are then carried over spinal cord neurons belonging to the segments L5–S1, which are the normal relay stations for impulses from the soleus muscle. As excitation spreads in the spinal cord (in this case, mainly in the caudal direction), the normally ineffective connections between the soleus muscle and the neurons of the S2–S4 segments become effective. Impulses from the trigger point nociceptors can now activate neurons in S2–S4 that otherwise provide sensory innervation to the sacroiliac (SI) joint. The individual therefore feels pain referred to the sacroiliac (SI) joint.
[Source 7]What are Myofascial trigger points
Myofascial trigger points (MTrP’s) are palpable, punctate areas of hardening in the muscle tissue that are painful on movement and palpation 8. Light-microscopic studies performed many years ago already revealed so-called contraction knots within MTrP’s 9: these are local thickenings of individual muscle fibers brought about by the contraction of a small number of sarcomeres.
In a widespread hypothesis on the origin of MTrP’s 10, it is supposed that a muscular lesion damages the neuromuscular endplate so that it secretes an excessive amount of acetylcholine. The ensuing depolarization of the muscle cell membrane produces a contraction knot that compresses the neighboring capillaries, causing local ischemia. Ischemia, in turn, leads to the release of substances into the tissue that sensitize nociceptors, accounting for the tenderness of MTrP’s to pressure. Substances of this type have been found to be present within the MTrP’s of these patients 11. This supposed mechanism leaves many questions unanswered but is currently the only comprehensive hypothesis on the origin of MTrP’s.
Patients with MTrP’s often have pain in three locations:
- at the site of the MTrP itself,
- at the origin or insertion of the affected muscle, because of pulling by the muscle fibers that have been stretched by the contraction knots,
- and referred pain outside the MTrP (see Figure 1).
Because the MTrP is cut off from its blood supply by compression of the local microcirculation, oral NSAID’s are not very effective against TrP pain. Therapeutic injections into the trigger point presumably work by diluting the sensitizing substances that are present here (among other mechanisms), as normal saline injections have been found to be just as effective as local anesthetic injections 6.
The referred symptoms associated with an MTrP often lead patients to localize their pain incorrectly. In such cases, the physician must deliberately search for the actual source of the pain by palpation of the muscle, and then treat it accordingly.
Table 1. Subjective differences between muscle pain and cutaneous pain
| Muscle pain | Cutaneous pain |
|---|---|
| Electrical nerve stimulation induces only one pain | Electrical nerve stimulation induces a first pain and a second pain |
| Poorly localizable | Well-localized |
| Tearing, cramping, pressing quality | Stabbing, burning, cutting quality |
| Marked tendency toward referral of pain | No tendency toward referral of pain |
| Affective aspect: difficult to tolerate | Affective aspect: easier to tolerate |
The most common causes of muscle pain are tension, stress, overuse and minor injuries. This type of pain is usually localized, affecting just a few muscles or a small part of your body.
Systemic muscle pain — pain throughout your whole body — is more often the result of an infection, an illness or a side effect of a medication.
The most common causes of muscle aches and pains are:
- Injury or trauma, including sprains and strains
- Overuse including using a muscle too much, too soon before warming up, or too often
- Tension or stress
Muscle pain may also be due to:
- Certain medications, including ACE inhibitors for lowering blood pressure, cocaine, and statins for lowering cholesterol
- Dermatomyositis
- Electrolyte imbalance, such as too little potassium or calcium
- Dystonia
- Fibromyalgia
- Infections, including the flu, Lyme disease, malaria, muscle abscess, polio, Rocky Mountain spotted fever, trichinosis (roundworm)
- Lupus
- Polymyalgia rheumatica
- Polymyositis
- Rhabdomyolysis
- Chronic exertional compartment syndrome
- Claudication due to peripheral artery disease and spinal stenosis
- Hypothyroidism (underactive thyroid)
- Influenza (flu)
- Lyme disease
- Muscle cramp
- Myofascial pain syndrome
- Repetitive strain injuries
- Rheumatoid arthritis
- Rocky Mountain spotted fever
- Sprains and strains
When to see a doctor
Muscle pain from minor injuries, stress or exercise is usually helped with simple home treatment. Muscle pain from severe injuries or systemic disease is often serious and requires medical care.
Get immediate medical care (call your local emergency number) if you have muscle pain with:
- Trouble breathing or dizziness
- Extreme muscle weakness
- A high fever and stiff neck
- Sudden weight gain, water retention, or you are urinating less than usual.
- You are short of breath or have difficulty swallowing.
- You have muscle weakness or cannot move any part of your body.
- You are vomiting, or have a very stiff neck or high fever.
Schedule an office visit if you have:
- A known tick bite or could have had a tick bite
- A rash, especially the “bulls-eye” rash of Lyme disease
- Muscle pain, especially in your calves, that occurs with exercise and resolves with rest
- You have any sign of infection, such as swelling or redness around the tender muscle.
- Muscle pain after you start taking or increase the dosage of a medication — (particularly statins — medications used to control cholesterol
- Muscle pain that doesn’t improve with self-care
- Your muscle pain lasts more than 3 days.
- You have severe, unexplained pain.
- You have poor circulation in the area where you have muscles aches (for example, in your legs).
Muscle pain that occurs during an activity usually signals a “pulled” or strained muscle.
These types of injuries usually respond well to R.I.C.E. therapy:
- Rest. Take a break from your normal activities.
- Ice. Place an ice pack or bag of frozen peas on the sore area for 20 minutes several times a day.
- Compression. Use a compression bandage to reduce swelling.
- Elevation. Elevate your foot to help reduce swelling.
For muscle pain from overuse or injury, rest the affected body part and take acetaminophen or ibuprofen. Apply ice for the first 24 to 72 hours after injury to reduce pain and inflammation. After that, heat often feels more soothing.
Muscle aches from overuse and fibromyalgia often respond well to massage. Gentle stretching exercises after a long rest period are also helpful.
Regular exercise can help restore proper muscle tone. Walking, cycling, and swimming are good aerobic activities to try. A physical therapist can teach you stretching, toning, and aerobic exercises to help you feel better and stay pain-free. Begin slowly and increase workouts gradually. Avoid high-impact aerobic activities and weight lifting when injured or while in pain.
Be sure to get plenty of sleep and try to reduce stress. Yoga and meditation are excellent ways to help you sleep and relax.
If home measures aren’t working, your health care provider may prescribe medicine or physical therapy. You may need to be seen at a specialized pain clinic.
If your muscle aches are due to a specific disease, do the things your provider has told you to treat the underlying condition.
These steps may help lower the risk for getting muscle aches:
- Stretch before and after exercising.
- Warm up before exercising and cool down afterward.
- Drink lots of fluids before, during, and after exercise.
- If you work in the same position most of the day (such as sitting at a computer), stretch at least every hour.
Peripheral mechanisms of muscle pain
Muscle pain is produced by the activation of specific receptors (so-called nociceptors): these receptors are specialized for the detection of stimuli that are objectively capable of damaging tissue and that are subjectively perceived as painful 7. They consist of free nerve endings and are connected to the central nervous system (CNS) by way of unmyelinated (group IV) or thinly myelinated (group III) fibers. They can be sensitized and activated by strong mechanical stimuli, such as trauma or mechanical overloading, as well as by endogenous inflammatory mediators including bradykinin (BK), serotonin, and prostaglandin E2 (PGE2).
Two activating chemical substances are particularly important for the generation of muscle pain: adenosine triphosphate (ATP) and protons (H+ ions) 7. These chemical irritants activate nerve endings by binding to receptor molecules located in the membrane of the nerve ending. ATP activates muscle nociceptors mainly by binding to the P2X3 receptor molecule, H+ mainly by binding to the receptor molecules TRPV1 (transient receptor potential vanilloid 1) and ASICs (acid-sensing ion channels) 12. These receptor molecules are channel proteins that span the membrane of the nerve ending and mainly permit Na+ ions to enter the neuron. These Na+ ions then induce neural excitation.
ATP is found in all cells of the body and is released whenever bodily tissues of any type are injured. Rat muscle nociceptors can be activated by the injection of ATP in a concentration corresponding to that found in muscle cells 13. Weakly acidic solutions (pH 6 to 5) are also effective activators of muscle nociceptors 14. A drop in pH is probably one of the main activators of peripheral nociceptors, as many painful disturbances of muscle are associated with low pH in muscle tissue. Nerve growth factor (NGF) also has a connection to muscle pain: nerve growth factor is synthesized in muscle and activates muscle nociceptors 15. Nerve growth factor (NGF) synthesis is increased when a muscle is inflamed 16.
Muscle nociceptors contain neuropeptides, including substance P (SP) and calcitonin-gene-related peptide (CGRP). These peptides are released when nerve endings are activated and induce local edema by dilating the local blood vessels and increasing their permeability. Thus, a nociceptor can alter the microcirculation in its immediate neighborhood by releasing neuropeptides. Endogenous substances such as bradykinin and prostaglandin E2 are released by muscle lesions of all kinds. Bradykinin is synthesized from plasma proteins by the action of the enzyme kallikrein, while prostaglandins are synthesized from arachidonic acid by the action of cyclooxygenase. These two activating substances increase the sensitivity of nociceptors to external stimuli (peripheral sensitization).
The sensitization of the muscle nociceptors by endogenous mediators such as bradykinin and prostaglandin E2 is one of the reasons why patients with muscle lesions suffer from tenderness to pressure on the muscle, and from pain on movement or exercise. It is also the reason why many types of muscle pain respond well to the administration of non-steroidal anti-inflammatory drugs (NSAIDs), which block prostaglandin synthesis. Sensitization manifests itself clinically in two closely related phenomena: stimuli that normally do not cause pain are perceived as painful (allodynia), while stimuli that are normally painful cause more severe pain than before (hyperalgesia). The principal mechanism for allodynia and hyperalgesia, however, is thought to be located in the central nervous system.
Changes of muscle tone as a cause of pain
Muscle spasm can be defined as persistent, involuntary muscle contraction (not including spasticity, a phenomenon of central nervous origin). The main reason why pain arises in muscle spasm is muscle ischemia, which leads to a drop in pH and the release of pain-producing substances such as bradykinin, ATP, and H+.
The vicious-circle concept of muscle spasm – muscle pain causes spasm, which causes more pain, etc. – should now be considered obsolete. Most studies have shown that muscle pain lowers the excitability of the α-motor neurons innervating the painful muscle 17 (a “pain adaptation” model) 18.
Muscle spasm can be precipitated by, among other things, pain in another muscle. Thus, a spasm-like increase electromyography (EMG) activity in the trapezius muscle has been described in response to painful stimulation of the biceps brachii muscle 18. Another source of muscle spasms is pathological changes in a neighboring joint. These sources of pain must be deliberately sought.
What is Delayed Onset Muscle Pain
Any type of activity that places unaccustomed loads on muscle may lead to delayed onset muscle soreness (DOMS) 19. This type of soreness is different from acute soreness, which is pain that develops during the actual activity. Delayed muscle soreness typically begins to develop 12-24 hours after the exercise has been performed and may produce the greatest pain between 24-72 hours after the exercise has been performed.
While origins of the soreness and accompanying symptoms are complex, it is well-established that many types of physical activity can cause delayed muscle soreness. Most believe muscle soreness develops as a result of microscopic damage to muscle fibers involved the exercise. This type of damage likely results from novel stresses that were experienced during the exercise.
One common misconception about delayed onset muscle soreness (DOMS) is that it is due to lactic acid accumulation, but lactic acid is not a component of this process. Delayed onset muscle soreness (DOMS) appears to be a side effect of the repair process that develops in response to microscopic muscle damage.
Examples of activities that are known to cause DOMS include:
- Strength training exercise
- Walking down hills
- Jogging
- Step aerobics
- Jumping
Activities which cause delayed onset muscle soreness (DOMS) all cause muscles to lengthen while force is applied. This is eccentric muscle action. Examples of eccentric muscle actions include the lowering phase of a bicep curl exercise or the lengthening of the thigh muscles while the limb brakes against your body’s momentum as it walks or jogs down a hill. Jogging or running on a flat surface can also elicit delayed onset muscle soreness (DOMS) symptoms for those who are unaccustomed to this type of activity.
The severity of muscle soreness depends on the types of forces placed on the muscle. Running down a hill will place greater force on the muscle than walking down the same hill. The soreness that develops will likely be greater after running down a hill. A high number of repetitions will cause more damage and soreness than a low number of repetitions. As a result, work your way gradually into a new exercise program.
All people are susceptible to delayed onset muscle soreness (DOMS), even those who have been exercising for years. However, the severity of soreness normally becomes less as your body becomes adapted to work it regularly performs. Just one bout of soreness-producing exercise actually develops a partial protective effect that reduces the chance of developing soreness in that same activity for weeks or months into the future.
Does delayed onset muscle soreness (DOMS) only cause muscle soreness ?
There are numerous characteristics of DOMS beyond local muscle pain. Some of the most common symptoms include:
- Swelling of the affected limbs;
- Stiffness of the joint accompanied by temporary reduction in a joint’s range of motion;
- Tenderness to the touch;
- Temporary reduction in strength of the affected muscles (lasting days);
- In rare and severe cases, muscle breakdown to the extent that the kidneys may be placed at risk; and
- Elevated creatine kinase (CK) enzyme in the blood, signaling muscle tissue damage.
When to see your doctor ?
DOMS symptoms do not typically necessitate the need for medical intervention. If the pain level becomes debilitating, if limbs experience heavy swelling or if urine becomes dark, then medical consultation is advisable.
DOMS Prevention
One of the best ways to reduce the severity of DOMS is to progress slowly in a new program. Allowing the muscle time to adapt to new stress should help to minimize the severity of symptoms, but it is unlikely that soreness can be avoided altogether. It is also important to allow the muscle time to recover from work that produces soreness, and participating in the same exercises on subsequent days should to be done judiciously.
Proper warmup is also important in preparing the muscle for the types of forces that may cause damage, but there is little evidence that warm-up will be effective in preventing DOMS symptoms.
Stretching is sometimes done before exercise, but it is better to stretch after the body is warmed up and after exercise. Stretching has not been shown to reduce or prevent symptoms of DOMS, but DOMS should last only a few days (usually 3-5 days) and the involved muscles will be better prepared for future bouts of the same type of exercise.
Discontinuing Exercise
Often, symptoms diminish during activity, but they will return after recovery. Performing exercise while experiencing severe symptoms may make matters worse. On the other hand, light activity should not impair your recovery. However, there is also not much evidence that this will hasten your recovery. If you find that your symptoms make it difficult or too painful to perform the activity, then it is advisable to refrain from the activity for a few days and return to the activity as symptoms subside.
Easing DOMS Symptoms
There is little evidence that such treatment strategies will hasten recovery and return to normal function. If the primary goal is to reduce symptoms, then treatments such as ice pack application, massage, tender-point acupressure, and oral pain relief agents may be useful in easing pain. It is important to be aware that pain reduction does not represent recovery. Rather, these treatments may only be effective in reducing symptoms of pain, but underlying muscle damage and reduced function may persist.
NO PAIN, NO GAIN ?
It is unlikely that you will avoid muscle soreness altogether when beginning a new exercise program. However, pain does not need to be present to achieve gains in fitness status, and pain may indicate a need to reduce or refrain from an activity. While eccentric loading of muscle to achieve gains in muscle size appears to be important, gains in strength will occur without overemphasizing the eccentric component of a weightlifting exercise. Pain that occurs during exercise (i.e., acute) signals a problem with the exercise (too intense, bad form, etc.) and should be halted before muscle or joint damage occurs.
What is Fibromyalgia (a chronic pain syndrome involving widespread muscle pain and fatigue)
Fibromyalgia is a common and complex chronic pain disorder that affects people physically, mentally and socially 20. In the past fibromyalgia has also been referred to as fibromyalgia syndrome, fibromyositis and fibrositis. It is characterized by chronic widespread pain, multiple tender points, abnormal pain processing, sleep disturbances, fatigue and often psychological distress. Symptoms can wax and wain, with severe symptoms being extremely debilitating and can interfere with an individuals basic daily activities.
Fibromyalgia is often considered a syndrome rather than a disease because it’s a collection of symptoms that seem to be related but, unlike a disease, there’s no cause that can be identified.
Fibromyalgia it affects millions of people in the United States. It’s far more common in females than males and can start when kids are in their teen years or even younger, although it’s most common in women between the ages of 20 and 50.
Chronic widespread body pain is the primary symptom of fibromyalgia. Most people with fibromyalgia also experience moderate to extreme fatigue, sleep disturbances, sensitivity to touch, light, and sound, and cognitive difficulties. Many individuals also experience a number of other symptoms and overlapping conditions, such as irritable bowel syndrome, lupus and arthritis.
An important symptom of the fibromyalgia is generalized pain that is mainly felt in the musculature 21. Two main models have been proposed to account for generalized muscle pain:
- An increased influx of nociceptive stimulation into muscle nociceptors leads to sensitization of neurons in the central nervous system, and thereby to generalized hypersensitivity to pain 22. In the muscles of fibromyalgia patients, however, only nonspecific changes have been found, which in all likelihood do not excite the muscle nociceptors. It remains an open question whether the changes in muscle histology that were seen in one study 23 have any relevance to the pain of fibromyalgia.
- The descending pain-modulating systems (i.e., pain-inhibiting and pain-promoting systems) are dysfunctional. The most important of these is the pain-inhibiting system that normally tonically dampens the activity of spinothalamic tract neurons 24, which constitute the main spinal nociceptive pathway. The neurons of origin of this pain-inhibiting system lie in the midbrain. The neural impulses of this system travel, by way of a relay station in the medulla, to the nociceptive cells of the spinal cord, where the actual inhibition takes place. The activity of the descending system is influenced by connections to the prefrontal cortex, the hypothalamus, and the limbic system. The descending system employs endogenous opioids as well as serotonin and noradrenaline as neurotransmitters 25. The descending pain-inhibiting system exerts a particularly strong effect on neurons that mediate muscle pain 26; thus, dysfunction of this system would be expected mainly to cause muscle pain.
The model of increased peripheral nociceptive activity leading to central sensitization can explain cases in which a local trauma, e.g., a whiplash injury of the cervical spine 27, develops into a generalized fibromyalgia.
Many authors favor a primary cause in the central nervous system in the form of a dysfunctional processing of nociceptive information. The dysfunction might consist, for example, of an insufficient degree of activity in the descending pain-inhibiting pathways, or of excessive activity in the descending pain-promoting pathways 25. Connections to the limbic system explain the fact that psychosocial influences play a major role in the pain of fibromyalgia. If the descending inhibition of pain is insufficient, i.e., if the neurons of the spinothalamic tract are disinhibited, then pain may arise even in the absence of a painful stimulus in the periphery.
Clinical examination reveals sites of excessive sensitivity to palpation (tender points, TeP), at which mild externally applied pressure causes pain. Many of these tender points are located at the myotendinous junction, rather than near the belly of the muscle, where MTrP’s are more likely to be found. These tender points are not associated with any local pathological changes (as far as is known) but are rather the expression of a generalized hypersensitivity to pain. Fibromyalgia patients have a low pain threshold in the skin and subcutaneous tissue as well as in muscle 28.
Dysfunction of the descending pain-inhibiting system is suggested by the fact that the pain of fibromyalgia usually does not respond to morphine, which exerts its analgesic effect mainly by activating the pain-inhibiting pathways.
Symptoms of fibromyalgia
Most people with fibromyalgia complain of widespread muscle pain, usually a dull or burning kind, but sometimes more of a shooting or throbbing pain. Widespread means the pain happens on both sides of the body, above and below the waist; it can range from mild to severe.
Usually, someone with fibromyalgia also has a number of tender spots (tender points, TeP) — places where he or she feels pain if the spot is pressed. Common tender spots include the back of the head, between the shoulder blades, shoulders, chest, neck, hips, knees, and elbows.
Fatigue (tiredness) is another common complaint of kids with fibromyalgia. Because of this, fibromyalgia can mimic the symptoms of a similar condition called chronic fatigue syndrome. Sometimes, a person can have both conditions, but they are separate syndromes.
Fibromyalgia also usually causes sleeping problems that make getting a good night’s sleep difficult. Some kids may have other sleep disorders like restless legs syndrome and sleep apnea. Poor sleep can also lead to waking up with body aches and stiffness that may improve during the day, then get worse at night.
Additional symptoms of fibromyalgia can include:
- gastrointestinal problems like irritable bowel syndrome
- problems with memory or concentration
- headaches
- irritability
- anxiety
- depression
People with fibromyalgia often notice a variety of external factors that can make their symptoms worse, from emotional stress to cold, damp weather.
Causes of fibromyalgia
- Recent research has suggested a strong genetic basis for fibromyalgia. The disorder is often seen in families, among siblings or mothers and their children.
- Fibromyalgia can occur following a physical trauma, such as an acute illness or injury, which may act as a “trigger” in the development of the disorder. Other “triggers” can include both physical and psychological forms of stress. While the stress may help trigger fibromyalgia, the stressor may not be involved in maintaining it once it starts
- Increasing attention is being devoted to the central nervous system as the underlying mechanism of fibromyalgia. Recent studies have suggested that fibromyalgia patients have generalized disturbance in pain processing and an amplified response to stimuli that would not ordinarily be painful in healthy individuals.
Diagnosis of fibromyalgia
If your child seems to be suffering from one or more of fibromyalgia’s major symptoms — such as chronic muscle pain, fatigue, or disrupted sleep — contact a doctor. While there’s no specific test to diagnose fibromyalgia, a doctor can run tests to rule out other possible causes, such as thyroid disorders, infectious diseases, or rheumatic diseases (like juvenile idiopathic arthritis).
Since fibromyalgia can’t be confirmed by any laboratory tests and has few, if any, visible signs, it can be difficult for doctors to diagnose the condition. This can be frustrating for someone who has it. Some estimates claim that it takes an average of 5 years for someone with fibromyalgia to get an accurate diagnosis, and some doctors are not as familiar with the condition as others.
Doctors diagnose fibromyalgia in someone based on medical history, the person’s description of symptoms, and a physical exam, including a check of 18 usual tender spots. Most kids with fibromyalgia will have pain when pressure is applied to at least five of the tender spots, and will have widespread musculoskeletal aches lasting for at least 3 months, with no other medical problem causing the pain.
Treatment for fibromyalgia
There is no cure for fibromyalgia, but treatment has been shown to improve the quality of life for those who have it. Treatment for fibromyalgia focuses on managing the pain and other symptoms and improving function. This often involves a combination of medicines and lifestyle changes, such as exercise, relaxation, and stress-management techniques.
- A variety of prescription medications are often used to reduce pain levels and improve sleep. On June 21, 2007, the U.S. Food and Drug Administration approved Lyrica (pregabalin) as the first drug to treat fibromyalgia. Cymbalta (duloxetine HCl) was approved in June 2008; and Savella (milnacipran HCl) was approved in January 2009. Additionally, healthcare providers may treat patients’ fibromyalgia symptoms with non-narcotic pain relievers (e.g. tramadol) or low doses of antidepressants (e.g. tricyclic antidepressants, serotonin reuptake inhibitors) or benzodiazepines. Patients must remember that antidepressants are “serotonin builders” and can be prescribed at low levels to help improve sleep and relieve pain. If the patient is experiencing depression, higher levels of these or other medications may need to be prescribed. Lidocaine injections into the patient’s tender points also work well on localized areas of pain. An important aspect of pain management is a regular program of gentle exercise and stretching, which helps maintain muscle tone and reduces pain and stiffness.
- Non-pharmacological therapies such as aerobic exercise, self-management, and cognitive-behavioral therapy have demonstrated benefits in fibromyalgia.
- Cognitive-behavioral therapy, a therapy used by mental health professionals, can help people learn to filter out negative thoughts, recognize what makes symptoms worse, and set limits to keep symptoms in check.
- Proper sleep. Getting enough sleep is one of the most effective ways to treat fibromyalgia, so children with fibromyalgia should be encouraged to avoid caffeine and sugary beverages and snacks right before bedtime. They also should go to bed and get up at the same time each day and limit napping during the daytime.
- Alternative therapies, such as massage, myofasical release, acupuncture, chiropractic, herbal supplements and yoga, may also be effective tools in managing fibromyalgia symptoms for some people.
- Increasing rest, pacing activities, reducing stress, practicing relaxation and improving nutrition can help minimize symptoms and improve quality of life.
- Healthy lifestyle choices. This includes eating a healthy diet and finding activities that help distract from the symptoms of fibromyalgia.
Low Back Pain
About 80 percent of adults experience low back pain at some point in their lifetimes. It is the most common cause of job-related disability and a leading contributor to missed work days. In a large survey, more than a quarter of adults reported experiencing low back pain during the past 3 months.
Men and women are equally affected by low back pain, which can range in intensity from a dull, constant ache to a sudden, sharp sensation that leaves the person incapacitated. Pain can begin abruptly as a result of an accident or by lifting something heavy, or it can develop over time due to age-related changes of the spine. Sedentary lifestyles also can set the stage for low back pain, especially when a weekday routine of getting too little exercise is punctuated by strenuous weekend workout.
Most low back pain is acute, or short term, and lasts a few days to a few weeks. It tends to resolve on its own with self-care and there is no residual loss of function. The majority of acute low back pain is mechanical in nature, meaning that there is a disruption in the way the components of the back (the spine, muscle, intervertebral discs, and nerves) fit together and move.
The lower back where most back pain occurs includes the five vertebrae (referred to as L1-L5) in the lumbar region, which supports much of the weight of the upper body. The spaces between the vertebrae are maintained by round, rubbery pads called intervertebral discs that act like shock absorbers throughout the spinal column to cushion the bones as the body moves. Bands of tissue known as ligaments hold the vertebrae in place, and tendons attach the muscles to the spinal column. Thirty-one pairs of nerves are rooted to the spinal cord and they control body movements and transmit signals from the body to the brain.
Subacute low back pain is defined as pain that lasts between 4 and 12 weeks.
Chronic back pain is defined as pain that persists for 12 weeks or longer, even after an initial injury or underlying cause of acute low back pain has been treated. About 20 percent of people affected by acute low back pain develop chronic low back pain with persistent symptoms at one year. In some cases, treatment successfully relieves chronic low back pain, but in other cases pain persists despite medical and surgical treatment.
The magnitude of the burden from low back pain has grown worse in recent years. In 1990, a study ranking the most burdensome conditions in the U.S. in terms of mortality or poor health as a result of disease put low back pain in sixth place; in 2010, low back pain jumped to third place, with only ischemic heart disease and chronic obstructive pulmonary disease ranking higher.
What causes lower back pain ?
The vast majority of low back pain is mechanical in nature. In many cases, low back pain is associated with spondylosis, a term that refers to the general degeneration of the spine associated with normal wear and tear that occurs in the joints, discs, and bones of the spine as people get older. Some examples of mechanical causes of low back pain include:
- Sprains and strains account for most acute back pain. Sprains are caused by overstretching or tearing ligaments, and strains are tears in tendon or muscle. Both can occur from twisting or lifting something improperly, lifting something too heavy, or overstretching. Such movements may also trigger spasms in back muscles, which can also be painful.
- Intervertebral disc degeneration is one of the most common mechanical causes of low back pain, and it occurs when the usually rubbery discs lose integrity as a normal process of aging. In a healthy back, intervertebral discs provide height and allow bending, flexion, and torsion of the lower back. As the discs deteriorate, they lose their cushioning ability.
- Herniated or ruptured discs can occur when the intervertebral discs become compressed and bulge outward (herniation) or rupture, causing low back pain.
- Radiculopathy is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
- Sciatica is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
- Spondylolisthesis is a condition in which a vertebra of the lower spine slips out of place, pinching the nerves exiting the spinal column.
- A traumatic injury, such as from playing sports, car accidents, or a fall can injure tendons, ligaments or muscle resulting in low back pain. Traumatic injury may also cause the spine to become overly compressed, which in turn can cause an intervertebral disc to rupture or herniate, exerting pressure on any of the nerves rooted to the spinal cord. When spinal nerves become compressed and irritated, back pain and sciatica may result.
- Spinal stenosis is a narrowing of the spinal column that puts pressure on the spinal cord and nerves that can cause pain or numbness with walking and over time leads to leg weakness and sensory loss.
- Skeletal irregularities include scoliosis, a curvature of the spine that does not usually cause pain until middle age; lordosis, an abnormally accentuated arch in the lower back; and other congenital anomalies of the spine.
Low back pain is rarely related to serious underlying conditions, but when these conditions do occur, they require immediate medical attention.
Serious underlying conditions include:
- Infections are not a common cause of back pain. However, infections can cause pain when they involve the vertebrae, a condition called osteomyelitis; the intervertebral discs, called discitis; or the sacroiliac joints connecting the lower spine to the pelvis, called sacroiliitis.
- Tumors are a relatively rare cause of back pain. Occasionally, tumors begin in the back, but more often they appear in the back as a result of cancer that has spread from elsewhere in the body.
- Cauda equina syndrome is a serious but rare complication of a ruptured disc. It occurs when disc material is pushed into the spinal canal and compresses the bundle of lumbar and sacral nerve roots, causing loss of bladder and bowel control. Permanent neurological damage may result if this syndrome is left untreated.
- Abdominal aortic aneurysms occur when the large blood vessel that supplies blood to the abdomen, pelvis, and legs becomes abnormally enlarged. Back pain can be a sign that the aneurysm is becoming larger and that the risk of rupture should be assessed.
- Kidney stones can cause sharp pain in the lower back, usually on one side.
Other underlying conditions that predispose people to low back pain include:
- Inflammatory diseases of the joints such as arthritis, including osteoarthritis and rheumatoid arthritis as well as spondylitis, an inflammation of the vertebrae, can also cause low back pain. Spondylitis is also called spondyloarthritis or spondyloarthropathy.
- Osteoporosis is a metabolic bone disease marked by a progressive decrease in bone density and strength, which can lead to painful fractures of the vertebrae.
- Endometriosis is the buildup of uterine tissue in places outside the uterus.
- Fibromyalgia, a chronic pain syndrome involving widespread muscle pain and fatigue.
What are the risk factors for developing low back pain ?
Beyond underlying diseases, certain other risk factors may elevate one’s risk for low back pain, including:
Age: The first attack of low back pain typically occurs between the ages of 30 and 50, and back pain becomes more common with advancing age. As people grow older, loss of bone strength from osteoporosis can lead to fractures, and at the same time, muscle elasticity and tone decrease. The intervertebral discs begin to lose fluid and flexibility with age, which decreases their ability to cushion the vertebrae. The risk of spinal stenosis also increases with age.
Fitness level: Back pain is more common among people who are not physically fit. Weak back and abdominal muscles may not properly support the spine. “Weekend warriors”—people who go out and exercise a lot after being inactive all week—are more likely to suffer painful back injuries than people who make moderate physical activity a daily habit. Studies show that low-impact aerobic exercise is beneficial for the maintaining the integrity of intervertebral discs.
Pregnancy is commonly accompanied by low back pain, which results from pelvic changes and alterations in weight loading. Back symptoms almost always resolve postpartum.
Weight gain: Being overweight, obese, or quickly gaining significant amounts of weight can put stress on the back and lead to low back pain.
Genetics: Some causes of back pain, such as ankylosing spondylitis, a form of arthritis that involves fusion of the spinal joints leading to some immobility of the spine, have a genetic component.
Occupational risk factors: Having a job that requires heavy lifting, pushing, or pulling, particularly when it involves twisting or vibrating the spine, can lead to injury and back pain. An inactive job or a desk job may also lead to or contribute to pain, especially if you have poor posture or sit all day in a chair with inadequate back support.
Mental health factors: Pre-existing mental health issues such as anxiety and depression can influence how closely one focuses on their pain as well as their perception of its severity. Pain that becomes chronic also can contribute to the development of such psychological factors. Stress can affect the body in numerous ways, including causing muscle tension.
Backpack overload in children: Low back pain unrelated to injury or other known cause is unusual in pre-teen children. However, a backpack overloaded with schoolbooks and supplies can strain the back and cause muscle fatigue. The American Academy of Orthopaedic Surgeons recommends that a child’s backpack should weigh no more than 15 to 20 percent of the child’s body weight.
How is low back pain diagnosed ?
A complete medical history and physical exam can usually identify any serious conditions that may be causing the pain. During the exam, a health care provider will ask about the onset, site, and severity of the pain; duration of symptoms and any limitations in movement; and history of previous episodes or any health conditions that might be related to the pain. Along with a thorough back examination, neurologic tests are conducted to determine the cause of pain and appropriate treatment. The cause of chronic lower back pain is often difficult to determine even after a thorough examination.
Imaging tests are not warranted in most cases. Under certain circumstances, however, imaging may be ordered to rule out specific causes of pain, including tumors and spinal stenosis. Imaging and other types of tests include:
X-ray is often the first imaging technique used to look for broken bones or an injured vertebra. X-rays show the bony structures and any vertebral misalignment or fractures. Soft tissues such as muscles, ligaments, or bulging discs are not visible on conventional x-rays.
Computerized tomography (CT) is used to see spinal structures that cannot be seen on conventional x-rays, such as disc rupture, spinal stenosis, or tumors. Using a computer, the CT scan creates a three-dimensional image from a series of two dimensional pictures.
Myelograms enhance the diagnostic imaging of x-rays and CT scans. In this procedure, a contrast dye is injected into the spinal canal, allowing spinal cord and nerve compression caused by herniated discs or fractures to be seen on an x-ray or CT scans.
Discography may be used when other diagnostic procedures fail to identify the cause of pain. This procedure involves the injection of a contrast dye into a spinal disc thought to be causing low back pain. The fluid’s pressure in the disc will reproduce the person’s symptoms if the disc is the cause. The dye helps to show the damaged areas on CT scans taken following the injection. Discography may provide useful information in cases where people are considering lumbar surgery or when their pain has not responded to conventional treatments.
Magnetic resonance imaging (MRI) uses a magnetic force instead of radiation to create a computer-generated image. Unlike x-ray, which shows only bony structures, MRI scans also produce images of soft tissues such as muscles, ligaments, tendons, and blood vessels. An MRI may be ordered if a problem such as infection, tumor, inflammation, disc herniation or rupture, or pressure on a nerve is suspected. MRI is a noninvasive way to identify a condition requiring prompt surgical treatment. However, in most instances, unless there are “red flags” in the history or physical exam, an MRI scan is not necessary during the early phases of low back pain.
Electrodiagnostics are procedures that, in the setting of low back pain, are primarily used to confirm whether a person has lumbar radiculopathy. The procedures include electromyography (EMG), nerve conduction studies (NCS), and evoked potential (EP) studies. EMG assesses the electrical activity in a muscle and can detect if muscle weakness results from a problem with the nerves that control the muscles. Very fine needles are inserted in muscles to measure electrical activity transmitted from the brain or spinal cord to a particular area of the body. NCSs are often performed along with EMG to exclude conditions that can mimic radiculopathy. In NCSs, two sets of electrodes are placed on the skin over the muscles. The first set provides a mild shock to stimulate the nerve that runs to a particular muscle. The second set records the nerve’s electrical signals, and from this information nerve damage that slows conduction of the nerve signal can be detected. EP tests also involve two sets of electrodes—one set to stimulate a sensory nerve, and the other placed on the scalp to record the speed of nerve signal transmissions to the brain.
Bone scans are used to detect and monitor infection, fracture, or disorders in the bone. A small amount of radioactive material is injected into the bloodstream and will collect in the bones, particularly in areas with some abnormality. Scanner-generated images can be used to identify specific areas of irregular bone metabolism or abnormal blood flow, as well as to measure levels of joint disease.
Ultrasound imaging, also called ultrasound scanning or sonography, uses high-frequency sound waves to obtain images inside the body. The sound wave echoes are recorded and displayed as a real-time visual image. Ultrasound imaging can show tears in ligaments, muscles, tendons, and other soft tissue masses in the back.
Blood tests are not routinely used to diagnose the cause of back pain; however in some cases they may be ordered to look for indications of inflammation, infection, and/or the presence of arthritis. Potential tests include complete blood count, erythrocyte sedimentation rate, and C-reactive protein. Blood tests may also detect HLA-B27, a genetic marker in the blood that is more common in people with ankylosing spondylitis or reactive arthritis (a form of arthritis that occurs following infection in another part of the body, usually the genitourinary tract).
How is back pain treated ?
Treatment for low back pain generally depends on whether the pain is acute or chronic. In general, surgery is recommended only if there is evidence of worsening nerve damage and when diagnostic tests indicate structural changes for which corrective surgical procedures have been developed.
Conventionally used treatments and their level of supportive evidence include:
Hot or cold packs have never been proven to quickly resolve low back injury; however, they may help ease pain and reduce inflammation for people with acute, subacute, or chronic pain, allowing for greater mobility among some individuals.
Activity: Bed rest should be limited. Individuals should begin stretching exercises and resume normal daily activities as soon as possible, while avoiding movements that aggravate pain. Strong evidence shows that persons who continue their activities without bed rest following onset of low back pain appeared to have better back flexibility than those who rested in bed for a week. Other studies suggest that bed rest alone may make back pain worse and can lead to secondary complications such as depression, decreased muscle tone, and blood clots in the legs.
Strengthening exercises, beyond general daily activities, are not advised for acute low back pain, but may be an effective way to speed recovery from chronic or subacute low back pain. Maintaining and building muscle strength is particularly important for persons with skeletal irregularities. Health care providers can provide a list of beneficial exercises that will help improve coordination and develop proper posture and muscle balance. Evidence supports short- and long-term benefits of yoga to ease chronic low back pain.
Physical therapy programs to strengthen core muscle groups that support the low back, improve mobility and flexibility, and promote proper positioning and posture are often used in combinations with other interventions.
Medications: A wide range of medications are used to treat acute and chronic low back pain. Some are available over the counter (OTC); others require a physician’s prescription. Certain drugs, even those available OTC, may be unsafe during pregnancy, may interact with other medications, cause side effects, or lead to serious adverse effects such as liver damage or gastrointestinal ulcers and bleeding. Consultation with a health care provider is advised before use. The following are the main types of medications used for low back pain:
- Analgesic medications are those specifically designed to relieve pain. They include OTC acetaminophen and aspirin, as well as prescription opioids such as codeine, oxycodone, hydrocodone, and morphine. Opioids should be used only for a short period of time and under a physician’s supervision. People can develop a tolerance to opioids and require increasingly higher dosages to achieve the same effect. Opioids can also be addictive. Their side effects can include drowsiness, constipation, decreased reaction time, and impaired judgment. Some specialists are concerned that chronic use of opioids is detrimental to people with back pain because they can aggravate depression, leading to a worsening of the pain.
- Nonsteroidal anti-inflammatory drugs (NSAIDS) relieve pain and inflammation and include OTC formulations (ibuprofen, ketoprofen, and naproxen sodium). Several others, including a type of NSAID called COX-2 inhibitors, are available only by prescription. Long-term use of NSAIDs has been associated with stomach irritation, ulcers, heartburn, diarrhea, fluid retention, and in rare cases, kidney dysfunction and cardiovascular disease. The longer a person uses NSAIDs the more likely they are to develop side effects. Many other drugs cannot be taken at the same time a person is treated with NSAIDs because they alter the way the body processes or eliminates other medications.
- Anticonvulsants—drugs primarily used to treat seizures—may be useful in treating people with radiculopathy and radicular pain.
Antidepressants such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit. - Counter-irritants such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Spinal manipulation and spinal mobilization are approaches in which professionally licensed specialists (doctors of chiropractic care) use their hands to mobilize, adjust, massage, or stimulate the spine and the surrounding tissues. Manipulation involves a rapid movement over which the individual has no control; mobilization involves slower adjustment movements. The techniques have been shown to provide small to moderate short-term benefits in people with chronic low back pain. Evidence supporting their use for acute or subacute low back pain is generally of low quality. Neither technique is appropriate when a person has an underlying medical cause for the back pain such as osteoporosis, spinal cord compression, or arthritis.
Traction involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released the back pain tends to return. There is no evidence that traction provides any longterm benefits for people with low back pain.
Acupuncture is moderately effective for chronic low back pain. It involves the insertion of thin needles into precise points throughout the body. Some practitioners believe this process helps clear away blockages in the body’s life force known as Qi (pronounced chee). Others who may not believe in the concept of Qi theorize that when the needles are inserted and then stimulated (by twisting or passing a low-voltage electrical current through them) naturally occurring painkilling chemicals such as endorphins, serotonin, and acetylcholine are released. Evidence of acupuncture’s benefit for acute low back pain is conflicting and clinical studies continue to investigate its benefits.
Biofeedback is used to treat many acute pain problems, most notably back pain and headache. The therapy involves the attachment of electrodes to the skin and the use of an electromyography machine that allows people to become aware of and self regulate their breathing, muscle tension, heart rate, and skin temperature. People regulate their response to pain by using relaxation techniques. Biofeedback is often used in combination with other treatment methods, generally without side effects. Evidence is lacking that biofeedback provides a clear benefit for low back pain.
Nerve block therapies aim to relieve chronic pain by blocking nerve conduction from specific areas of the body. Nerve block approaches range from injections of local anesthetics, botulinum toxin, or steroids into affected soft tissues or joints to more complex nerve root blocks and spinal cord stimulation. When extreme pain is involved, low doses of drugs may be administered by catheter directly into the spinal cord. The success of a nerve block approach depends on the ability of a practitioner to locate and inject precisely the correct nerve. Chronic use of steroid injections may lead to increased functional impairment.
Epidural steroid injections are a commonly used short-term option for treating low back pain and sciatica associated with inflammation. Pain relief associated with the injections, however, tends to be temporary and the injections are not advised for long-term use. A randomized controlled trial assessing the benefit of epidural steroid injections for the treatment of chronic low back pain associated with spinal stenosis showed that long-term outcomes were worse among those people who received the injections compared with those who did not.
Transcutaneous electrical nerve stimulation (TENS) involves wearing a battery-powered device consisting of electrodes placed on the skin over the painful area that generate electrical impulses designed to block incoming pain signals from the peripheral nerves. The theory is that stimulating the nervous system can modify the perception of pain. Early studies of TENS suggested that it elevated levels of endorphins, the body’s natural pain-numbing chemicals. More recent studies, however, have produced mixed results on its effectiveness for providing relief from low back pain.
Surgery
When other therapies fail, surgery may be considered an option to relieve pain caused by serious musculoskeletal injuries or nerve compression. It may be months following surgery before the patient is fully healed, and he or she may suffer permanent loss of flexibility.
Surgical procedures are not always successful, and there is little evidence to show which procedures work best for their particular indications. Patients considering surgical approaches should be fully informed of all related risks. Surgical options include:
- Vertebroplasty and kyphoplasty are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
- Spinal laminectomy (also known as spinal decompression) is performed when spinal stenosis causes a narrowing of the spinal canal that causes pain, numbness, or weakness. During the procedure, the lamina or bony walls of the vertebrae, along with any bone spurs, are removed. The aim of the procedure is to open up the spinal column to remove pressure on the nerves.
- Discectomy or microdiscectomy may be recommended to remove a disc, in cases where it has herniated and presses on a nerve root or the spinal cord, which may cause intense and enduring pain. Microdiscectomy is similar to a conventional discectomy; however, this procedure involves removing the herniated disc through a much smaller incision in the back and a more rapid recovery. Laminectomy and discectomy are frequently performed together and the combination is one of the more common ways to remove pressure on a nerve root from a herniated disc or bone spur.
- Foraminotomy is an operation that “cleans out” or enlarges the bony hole (foramen) where a nerve root exits the spinal canal. Bulging discs or joints thickened with age can cause narrowing of the space through which the spinal nerve exits and can press on the nerve, resulting in pain, numbness, and weakness in an arm or leg. Small pieces of bone over the nerve are removed through a small slit, allowing the surgeon to cut away the blockage and relieve pressure on the nerve.
- Intradiscal electrothermal therapy (IDET) is a treatment for discs that are cracked or bulging as a result of degenerative disc disease. The procedure involves inserting a catheter through a small incision at the site of the disc in the back. A special wire is passed through the catheter and an electrical current is applied to heat the disc, which helps strengthen the collagen fibers of the disc wall, reducing the bulging and the related irritation of the spinal nerve. IDET is of questionable benefit.
- Nucleoplasty, also called plasma disc decompression (PDD), is a type of laser surgery that uses radiofrequency energy to treat people with low back pain associated with mildly herniated discs. Under x-ray guidance, a needle is inserted into the disc. A plasma laser device is then inserted into the needle and the tip is heated to 40-70 degrees Celsius, creating a field that vaporizes the tissue in the disc, reducing its size and relieving pressure on the nerves. Several channels may be made depending on how tissue needs to be removed to decompress the disc and nerve root.
- Radiofrequency denervation is a procedure using electrical impulses to interrupt nerve conduction (including the conduction of pain signals). Using x-ray guidance, a needle is inserted into a target area of nerves and a local anesthetic is introduced as a way of confirming the involvement of the nerves in the person’s back pain. Next, the region is heated, resulting in localized destruction of the target nerves. Pain relief associated with the technique is temporary and the evidence supporting this technique is limited.
- Spinal fusion is used to strengthen the spine and prevent painful movements in people with degenerative disc disease or spondylolisthesis (following laminectomy). The spinal disc between two or more vertebrae is removed and the adjacent vertebrae are “fused” by bone grafts and/or metal devices secured by screws. The fusion can be performed through the abdomen, a procedure known as an anterior lumbar interbody fusion, or through the back, called posterior fusion. Spinal fusion may result in some loss of flexibility in the spine and requires a long recovery period to allow the bone grafts to grow and fuse the vertebrae together. Spinal fusion has been associated with an acceleration of disc degeneration at adjacent levels of the spine.
- Artificial disc replacement is considered an alternative to spinal fusion for the treatment of people with severely damaged discs. The procedure involves removal of the disc and its replacement by a synthetic disc that helps restore height and movement between the vertebrae.
Recommendations for keeping your lower back healthy
Following any period of prolonged inactivity, a regimen of low-impact exercises is advised. Speed walking, swimming, or stationary bike riding 30 minutes daily can increase muscle strength and flexibility. Yoga also can help stretch and strengthen muscles and improve posture. Consult a physician for a list of low-impact, age-appropriate exercises that are specifically targeted to strengthening lower back and abdominal muscles.
- Always stretch before exercise or other strenuous physical activity.
- Don’t slouch when standing or sitting. The lower back can support a person’s weight most easily when the curvature is reduced. When standing, keep your weight balanced on your feet.
- At home or work, make sure work surfaces are at a comfortable height.
- Sit in a chair with good lumbar support and proper position and height for the task. Keep shoulders back. Switch sitting positions often and periodically walk around the office or gently stretch muscles to relieve tension. A pillow or rolled-up towel placed behind the small of the back can provide some lumbar support. During prolonged periods of sitting, elevate feet on a low stool or a stack of books.
- Wear comfortable, low-heeled shoes.
- Sleeping on one’s side with the knees drawn up in a fetal position can help open up the joints in the spine and relieve pressure by reducing the curvature of the spine. Always sleep on a firm surface.
- Don’t try to lift objects that are too heavy. Lift from the knees, pull the stomach muscles in, and keep the head down and in line with a straight back. When lifting, keep objects close to the body. Do not twist when lifting.
- Maintain proper nutrition and diet to reduce and prevent excessive weight gain, especially weight around the waistline that taxes lower back muscles. A diet with sufficient daily intake of calcium, phosphorus, and vitamin D helps to promote new bone growth.
- Quit smoking. Smoking reduces blood flow to the lower spine, which can contribute to spinal disc degeneration. Smoking also increases the risk of osteoporosis and impedes healing. Coughing due to heavy smoking also may cause back pain.
- Muscle aches. https://medlineplus.gov/ency/article/003178.htm[↩]
- Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Krismer M, van Tulder M, Low Back Pain Group of the Bone and Joint Health Strategies for Europe Project. Best Pract Res Clin Rheumatol. 2007 Feb; 21(1):77-91.[↩]
- Prevalence of myofascial pain in general internal medicine practice. Skootsky SA, Jaeger B, Oye RK. West J Med. 1989 Aug; 151(2):157-60.[↩]
- The prevalence and characteristics of fibromyalgia in the general population. Wolfe F, Ross K, Anderson J, Russell IJ, Hebert L. Arthritis Rheum. 1995 Jan; 38(1):19-28.[↩]
- Muscle but not cutaneous C-afferent input produces prolonged increases in the excitability of the flexion reflex in the rat. Wall PD, Woolf CJ. J Physiol. 1984 Nov; 356():443-58.[↩]
- Mense S, Simons DG. Muscle Pain, Understanding its nature, diagnosis and treatment. London: Lippincott, Williams & Wilkins, Baltimore; 2001.[↩][↩]
- Mense S. Muscle Pain: Mechanisms and Clinical Significance. Deutsches Ärzteblatt International. 2008;105(12):214-219. doi:10.3238/artzebl.2008.0214. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696782/[↩][↩][↩][↩]
- Simons DG, Travell JG, Simons LS. Upper half of body. 2nd ed. Volume 1. London: Williams and Wilkins, Baltimore; 1999. Travell and Simons’ Myofascial pain and dysfunction. The trigger point manual.[↩]
- Microscopic features and transient contraction of palpable bands in canine muscle. Simons DG, Stolov WC. Am J Phys Med. 1976 Apr; 55(2):65-88.[↩]
- Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. Simons DG. J Electromyogr Kinesiol. 2004 Feb; 14(1):95-107.[↩]
- An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. Shah JP, Phillips TM, Danoff JV, Gerber LH. J Appl Physiol (1985). 2005 Nov; 99(5):1977-84.[↩]
- Ion channels of nociception. McCleskey EW, Gold MS. Annu Rev Physiol. 1999; 61():835-56.[↩]
- Adenosine triphosphate as a stimulant for nociceptive and non-nociceptive muscle group IV receptors in the rat. Reinöhl J, Hoheisel U, Unger T, Mense S. Neurosci Lett. 2003 Feb 20; 338(1):25-8.[↩]
- Acidic pH and capsaicin activate mechanosensitive group IV muscle receptors in the rat. Hoheisel U, Reinöhl J, Unger T, Mense S. Pain. 2004 Jul; 110(1-2):149-57.[↩]
- Excitatory and modulatory effects of inflammatory cytokines and neurotrophins on mechanosensitive group IV muscle afferents in the rat. Hoheisel U, Unger T, Mense S. Pain. 2005 Mar; 114(1-2):168-76.[↩]
- Inflammation-induced increase in the density of neuropeptide-immunoreactive nerve endings in rat skeletal muscle. Reinert A, Kaske A, Mense S. Exp Brain Res. 1998 Jul; 121(2):174-80.[↩]
- Inhibition of motor system excitability at cortical and spinal level by tonic muscle pain. Le Pera D, Graven-Nielsen T, Valeriani M, Oliviero A, Di Lazzaro V, Tonali PA, Arendt-Nielsen L. Clin Neurophysiol. 2001 Sep; 112(9):1633-41.[↩]
- The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity. Lund JP, Donga R, Widmer CG, Stohler CS. Can J Physiol Pharmacol. 1991 May; 69(5):683-94.[↩][↩]
- https://www.acsm.org/docs/brochures/delayed-onset-muscle-soreness-(doms).pdf[↩]
- About Fibromyalgia. http://www.fmaware.org/about-fibromyalgia/[↩]
- Mechanisms of disease: pain in fibromyalgia syndrome. Staud R, Rodriguez ME. Nat Clin Pract Rheumatol. 2006 Feb; 2(2):90-8.[↩]
- Vierck CJ. Mechanisms underlying development of spatially distributed chronic pain (fibromyalgia) Pain. 2006;124:242–263.[↩]
- Sprott H, Salemi S, Gay RE, et al. Increased DNA fragmentation and ultrastructural changes in fibromyalgic muscle fibres. Ann Rheum Dis. 2004;63:245–251.[↩]
- Fields HL, Basbaum AI. Central nervous system mechanisms of pain modulation. In: Wall PD, Melzack R, editors. Textbook of Pain. Edinburgh: Churchill Livingstone; 1999. pp. 309–329.[↩]
- Fields H. State-dependent control of pain. Nature Rev. 2004;5:565–575.[↩][↩]
- Yu X.-M, Mense S. Response properties and descending control of rat dorsal horn neurons with deep receptive fields. Neuroscience. 1990;39:823–831.[↩]
- Increased rates of fibromyalgia following cervical spine injury. A controlled study of 161 cases of traumatic injury. Buskila D, Neumann L, Vaisberg G, Alkalay D, Wolfe F. Arthritis Rheum. 1997 Mar; 40(3):446-52.[↩]
- Sensitivity disturbances in patients with irritable bowel syndrome and fibromyalgia. Caldarella MP, Giamberardino MA, Sacco F, Affaitati G, Milano A, Lerza R, Balatsinou C, Laterza F, Pierdomenico SD, Cuccurullo F, Neri M. Am J Gastroenterol. 2006 Dec; 101(12):2782-9.[↩]





{kind=link}