Contents
What is parotid tumor
Parotid tumors are the most common type of salivary gland tumors, accounting for 80 to 85 percent of all salivary gland tumors. While most parotid tumors are noncancerous (benign) around 80%, the parotid glands are where nearly 25 percent of cancerous (malignant) salivary gland tumors develop.
The parotid glands, located just in front of the ears on each side of the face, are the largest of the three sets of major salivary glands (Figure 1). They are responsible for producing saliva to aid in chewing and digesting food.
Parotid tumors may present a variety of characteristics. If you have a parotid tumor, you may notice a mass or swelling in your jaw area that may or may not be painful. If the tumor is malignant, it may also affect facial nerves, causing pain, numbness, a burning or prickling sensation, or loss of movement in the face.
Using ultrasound scanning and obtaining a small needle sample is a very useful way of indicating whether a parotid tumor may be benign or malignant.
Salivary gland cancers are not very common, making up less than 1% of cancers in the United States. They occur at a rate of about 1 case per 100,000 people per year in the United States.
These cancers can occur in people of almost any age, but they become more common as people get older. The average age at the time of diagnosis is 64. Because of its location, in many cases salivary gland cancer can be found early. Often patients, their dentists, or their doctors notice a lump within one of the salivary glands (usually on the sides of the face or in the mouth). Checking the salivary glands for tumors is often a routine part of general medical and dental check-ups.
Overall, about 72% of people diagnosed with salivary gland cancer are still alive at least 5 years after being diagnosed. (This includes people with all types and stages of salivary gland cancer, but the outlook for some people might be better or worse than this.)
The numbers below come from the National Cancer Database, and are based on people diagnosed with cancer of the major salivary glands between 1998 and 1999.
| Stage | 5-year Relative Survival Rate |
| I | 91% |
| II | 75% |
| III | 65% |
| IV | 39% |
The 5-year survival rate refers to the percentage of patients who live at least 5 years after their cancer is diagnosed. Of course, many people live much longer than 5 years (and many are cured). To get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. Improvements in treatment since then may result in a better outlook for people now being diagnosed with salivary gland cancer.
5-year relative survival rates (such as the numbers below) assume that some people will die of other causes and compare the observed survival with that expected for people without the cancer. This is a more accurate way to describe the prognosis for patients with a particular type and stage of cancer.
Again, these numbers include people who were diagnosed and treated many years ago, so the outlook for people now being diagnosed might be better.
Survival rates are based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any person’s case. The stage of the cancer is important, but many other factors can also affect a person’s outlook, such as their age, the type and grade of the cancer, and how well the cancer responds to treatment. Even when taking these factors into account, survival rates are at best rough estimates. Your doctor is familiar with the aspects of your particular situation and can tell you how the numbers above might apply to you.
The parotid glands
The parotid glands, the largest salivary glands, are just in front of the ears. The parotid glands make saliva – the lubricating fluid found in the mouth and throat. Chemically, saliva is 99.5% water and 0.5% solutes. Among the solutes are ions, including sodium, potassium, chloride, bicarbonate, and phosphate. Also present are some dissolved gases and various organic substances, including urea and uric acid, mucus, immunoglobulin A, the bacteriolytic enzyme lysozyme, and salivary amylase, a digestive enzyme that acts on starch.
The parotid glands secrete a watery (serous) liquid containing salivary amylase.
About 7 out of 10 salivary gland tumors start here. Most of these tumors are benign (not cancer), but the parotid glands still are where most malignant (cancerous) salivary gland tumors start.
Figure 1. Parotid gland
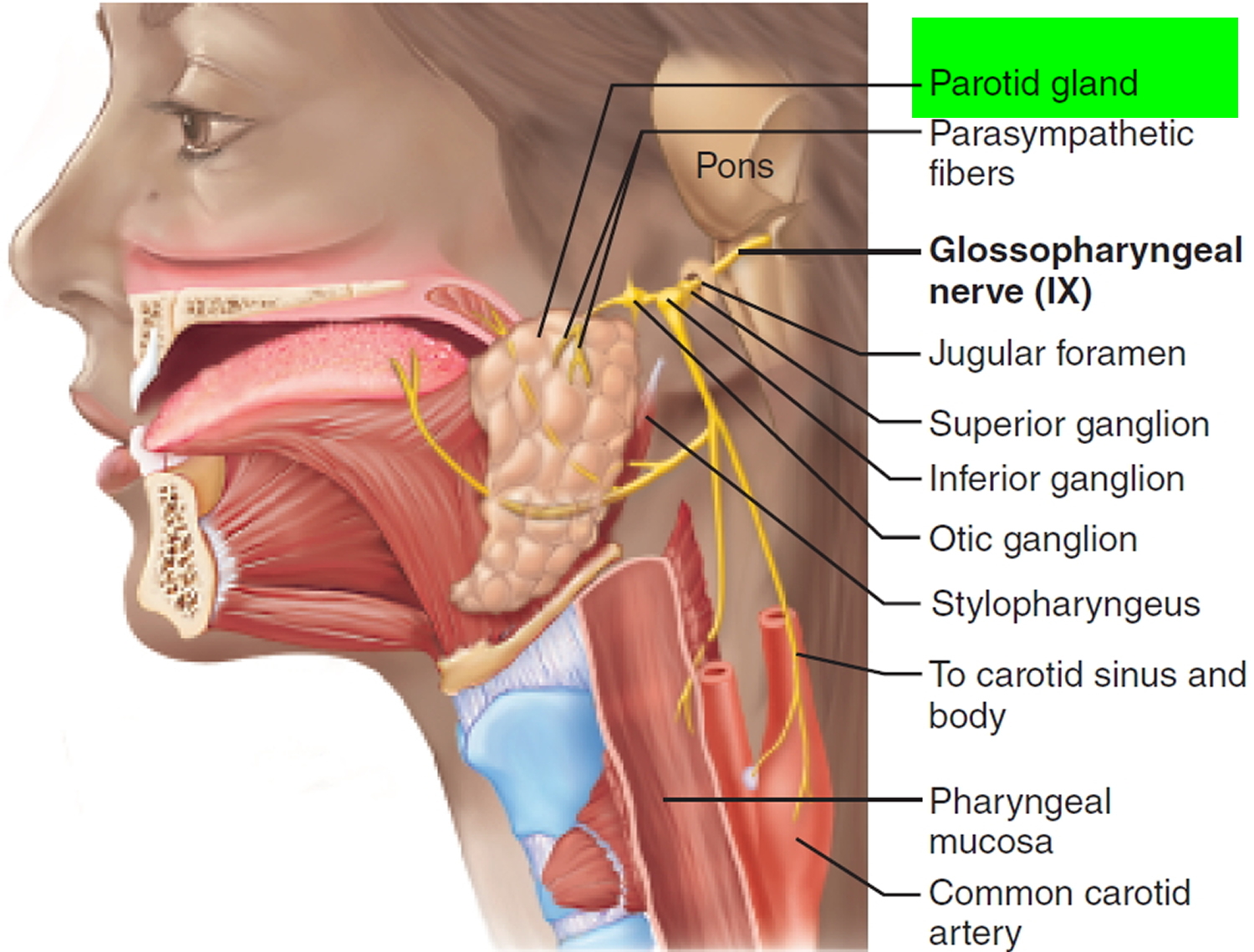
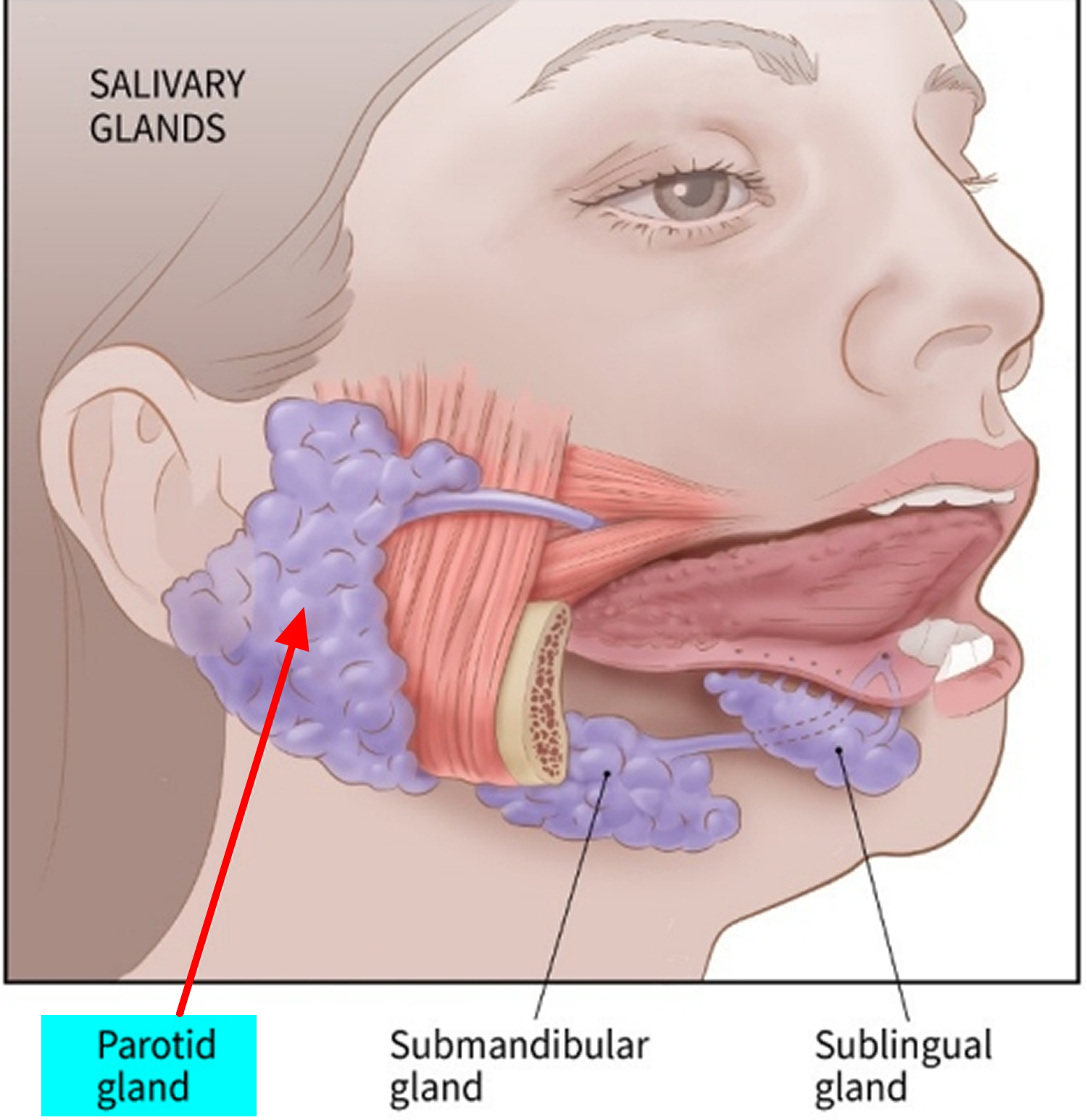
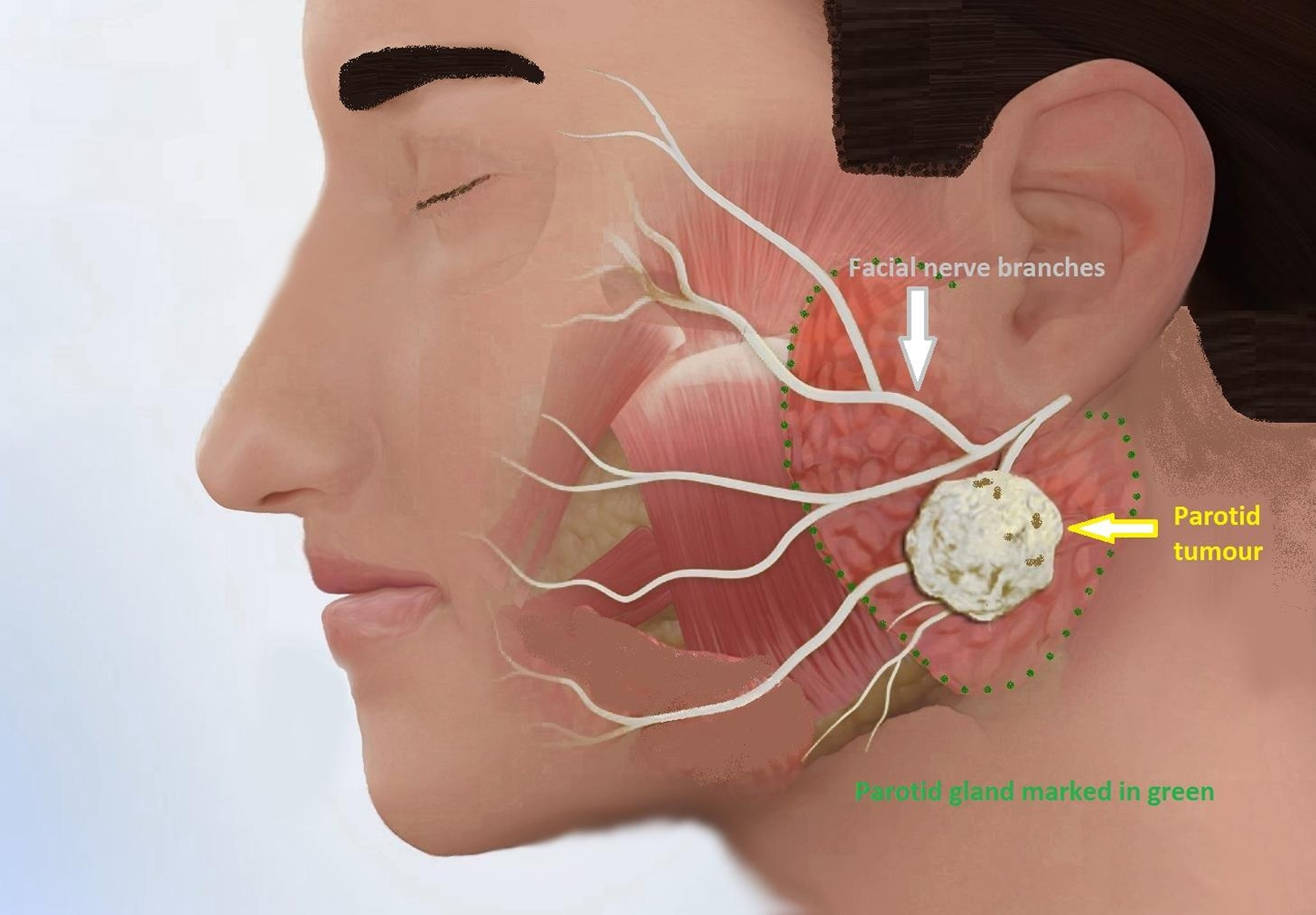
Figure 2. Parotid gland and facial nerve – Facial nerve is an important nerve that passes through the parotid gland and its function is to move facial muscles.
Benign parotid tumors
Most salivary gland tumors are benign – that is, they are not cancer and will not spread to other parts of the body. These tumors are almost never life threatening.
There are many types of benign salivary gland tumors, with names such as adenomas, oncocytomas, Warthin tumors, and benign mixed tumors (also known as pleomorphic adenomas).
Benign tumors are almost always cured by surgery. Very rarely, they may become cancer if left untreated for a long time or if they are not completely removed and grow back. It’s not clear exactly how benign tumors become cancers.
Parotid gland cancers (malignant salivary gland tumors)
There are many types of salivary gland cancers. Normal salivary glands are made up of many different kinds of cells, and tumors can start in any of these cell types. Salivary gland cancers are named according to which of these cell types they most look like when seen under a microscope. The main types of cancers are described below.
Doctors usually give salivary cancers a grade (from 1 to 3, or from low to high), based on how abnormal the cancers look under a microscope. The grade gives a rough idea of how quickly it is likely to grow and spread.
- Grade 1 cancers (also called low grade or well differentiated) look very much like normal salivary gland cells. They tend to grow slowly and have a good outcome (prognosis).
- Grade 2 cancers (also called intermediate grade or moderately differentiated) have an appearance and outlook that is between grade 1 and grade 3 cancers.
- Grade 3 cancers (also called high grade or poorly differentiated) look very different from normal cells and often grow and/or spread quickly. The outlook for these cancers is usually not as good as for lower grade cancers.
Mucoepidermoid carcinoma
Mucoepidermoid carcinomas are the most common type of salivary gland cancer. Most start in the parotid glands. They develop less often in the submandibular glands or in minor salivary glands inside the mouth. These cancers are usually low grade, but they can also be intermediate or high grade.
Adenoid cystic carcinoma
Adenoid cystic carcinoma is usually slow growing and often appears to be low-grade when looked at under the microscope. Still, it’s very hard to get rid of completely because it tends to spread along nerves. These tumors tend to come back after treatment (generally surgery and radiation), sometimes many years later. The outlook for patients is better for smaller tumors.
Adenocarcinomas
Adenocarcinoma is a term used to describe cancers that start in gland cells (cells that normally secrete a substance). There are many types of salivary gland adenocarcinomas.
- Acinic cell carcinoma: Most acinic cell carcinomas start in the parotid gland. They tend to be slow growing and tend to occur at a younger age than most other salivary gland cancers. They are usually low grade, but how far they have grown into nearby tissue is probably a better predictor of a patient’s outlook.
- Polymorphous low-grade adenocarcinoma: These tumors tend to start in the minor salivary glands. They usually (but not always) grow slowly and are mostly curable.
- Adenocarcinoma, not otherwise specified: When seen under a microscope, these cancers have enough features to tell that they are adenocarcinomas, but not enough detail to classify them further. They are most common in the parotid glands and the minor salivary glands. These tumors can be any grade.
- Rare adenocarcinomas: Several types of adenocarcinoma are quite rare.
Some of these tend to be low grade and usually have a very good outcome:
- Basal cell adenocarcinoma
- Clear cell carcinoma
- Cystadenocarcinoma
- Sebaceous adenocarcinoma
- Sebaceous lymphadenocarcinoma
- Mucinous adenocarcinoma
Other rare adenocarcinomas are more likely to be high grade and may have a less favorable outcome:
- Oncocytic carcinoma
- Salivary duct carcinoma
Malignant mixed tumors
There are 3 types of malignant mixed tumors:
- Carcinoma ex pleomorphic adenoma
- Carcinosarcoma
- Metastasizing mixed tumor
Nearly all of these cancers are carcinoma ex pleomorphic adenomas. The other 2 types are very, very rare.
Carcinoma ex pleomorphic adenoma develops from a benign mixed tumor (also known as a pleomorphic adenoma). This tumor occurs mainly in the major salivary glands. Both the grade of the cancer and how far it has spread (its stage) are important in predicting outcome.
Other rare salivary gland cancers
Several other types of cancer can develop in the salivary glands.
- Squamous cell carcinoma: This cancer occurs mainly in older men. It can develop after radiation therapy for other cancers in the area. This type of cancer tends to have a poorer outlook.
- Epithelial-myoepithelial carcinoma: This rare tumor tends to be low grade, but it can come back after treatment and/or spread to other parts of the body.
- Anaplastic small cell carcinoma: The cells in these tumors have nerve cell-like features. These tumors are most often found in minor salivary glands and tend to grow quickly.
- Undifferentiated carcinomas: This group of cancers includes small cell undifferentiated carcinoma, large cell undifferentiated carcinoma, and lymphoepithelial carcinoma. These are high-grade cancers that often spread. Overall, the survival outlook tends to be poor. Lymphoepithelial carcinoma, which is much more common in Eskimo and Inuit people, has a slightly better outcome.
Other cancers that can affect the salivary glands
These types of cancer are typically not thought of as true salivary gland cancers, either because they start more often in other parts of the body, or because they start elsewhere and then grow into or spread to the salivary glands.
- Non-Hodgkin lymphoma: Most non-Hodgkin lymphomas start in lymph nodes. Rarely, these cancers start in immune system cells within the salivary glands. They behave and are treated differently from other types of cancers in the salivary glands. Most lymphomas that start in the salivary glands affect people with Sjogren (Sjögren) syndrome (a disorder that causes the immune system to attack salivary gland cells). For more information, see Non-Hodgkin Lymphoma.
- Sarcomas: The salivary glands contain blood vessels, muscle cells, and cells that make connective tissue. Cancers that start in these types of cells are called sarcomas. These rarely occur in the salivary gland. For more information, see Sarcoma– Adult Soft Tissue Cancer.
- Secondary salivary gland cancers: Cancers that start elsewhere and spread to the salivary glands are called secondary salivary gland cancers. These cancers are treated based on where the cancer started.
Parotid tumor causes
Salivary gland tumors are rare, accounting for less than 10 percent of all head and neck tumors. It’s not clear what causes salivary gland tumors.
Doctors know salivary gland cancer occurs when some cells in a salivary gland develop mutations in their DNA. The mutations allow the cells to grow and divide rapidly. The mutated cells continue living when other cells would die. The accumulating cells form a tumor that can invade nearby tissue. Cancerous cells can break off and spread (metastasize) to distant areas of the body.
Risk factors for parotid tumor
Factors that may increase your risk of salivary gland tumors include:
- Older age. Though salivary gland tumors can occur at any age, they most commonly occur in older adults.
- Radiation exposure. Radiation, such as radiation used to treat head and neck cancers, increases the risk of salivary gland tumors.
- Workplace exposure to certain substances. People who work with certain substances may have an increased risk of salivary gland tumors. Some studies have suggested that people who work with certain metals (nickel alloy dust) or minerals (silica dust), and people who work in asbestos mining, plumbing, rubber products manufacturing, and some types of woodworking may be at increased risk for salivary gland cancer, but these links are not certain. The rarity of these cancers makes this hard to study.
- Tobacco and alcohol use. Tobacco and alcohol can increase the risk for several cancers of the head and neck area, but they have not been strongly linked to salivary gland cancers in most studies.
- Diet. Some studies have found that a diet low in vegetables and high in animal fat may increase the risk of salivary gland cancer, but more research is needed to confirm this possible link.
- Cell phone use. One study has suggested an increased risk of parotid gland tumors among heavy cell phone users. In this study, most of the tumors seen were benign (not cancer). Other studies looking at this issue have not found such a link. Research in this area is still in progress.
Salivary gland cancer prevention
Because scientists don’t know what causes most salivary gland cancers, they don’t yet know how to prevent many of them.
Avoiding some of the possible risk factors (such as tobacco, excess alcohol use, and unhealthy diets) might slightly lower the likelihood of developing salivary gland cancer, but no one knows for sure. However, scientists do know that avoiding these factors can help reduce your risk of other, more common cancers, as well as many other diseases.
For people who work in certain industries linked with an increased risk of salivary gland cancer, taking precautions to protect themselves might help lower their risk.
Parotid tumor symptoms
The major salivary glands are on each side of the face and below the tongue. Several important nerves and other structures run through or near salivary glands and can be affected by salivary tumors.
Having a lump or an area of swelling near your parotid gland is the most common sign of a parotid gland tumor, but it doesn’t mean you have cancer. Most salivary gland tumors are noncancerous (benign). Many other noncancerous conditions may lead to a swollen salivary gland, including an infection or a stone in a parotid gland duct.
Signs and symptoms of a salivary gland tumor may include:
- A lump or swelling on or near your jaw or in your neck or mouth
- Numbness in part of your face
- Muscle weakness on one side of your face
- Persistent pain in the area of a salivary gland
- Difficulty swallowing
- Trouble opening your mouth widely
Possible signs and symptoms of salivary gland cancer include:
- A lump or swelling in your mouth, cheek, jaw, or neck
- Pain in your mouth, cheek, jaw, ear, or neck that does not go away
- A difference between the size and/or shape of the left and right sides of your face or neck
- Numbness in part of your face
- Weakness of the muscles on one side of your face
- Trouble opening your mouth widely
- Fluid draining from an ear
- Trouble swallowing
Many of these signs and symptoms can also be caused by benign (non-cancerous) salivary gland tumors or by other conditions. Still, if you have any of these problems, it’s important to see your doctor right away so the cause can be found and treated, if needed.
Parotid tumor diagnosis
Tests and procedures used to diagnose a parotid tumor may include:
- A physical exam. Your doctor will feel your jaw, neck and throat for lumps or swelling.
- Collecting a sample of tissue for testing. Your doctor may recommend collecting a sample of tissue (biopsy) for laboratory testing to determine if the tumor is cancerous. During an aspiration biopsy, the doctor inserts a needle into the suspicious area and draws out fluid or cells. Salivary gland tumors are also analyzed in the laboratory after surgery to confirm the diagnosis.
- Imaging tests. If the parotid tumor is malignant, imaging tests, such as magnetic resonance imaging (MRI) and computerized tomography (CT), may help your doctor determine the size and location of the cancer.
If you’re diagnosed with having salivary gland cancer, your doctor will determine the extent (stage) of your cancer. Your cancer’s stage determines your treatment options and gives your doctor an idea of your prognosis.
Cancer stages are identified by Roman numerals, with stage I indicating a small, localized tumor and stage IV indicating an advanced cancer that has spread to the lymph nodes in the neck or to distant parts of the body.
Salivary Gland Cancer Stages
After someone is diagnosed with salivary gland cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and how best to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
The earliest stage salivary gland cancers are stage 0 (carcinoma in situ), and then stages range from I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
The staging system most often used for salivary gland cancers is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
- The extent of the tumor (T): How large is the cancer? Has it grown into nearby structures?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant organs such as the lungs?
The system described here is the most recent American Joint Committee on Cancer system, effective January 2018.
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The staging system in the table below is the pathologic stage (also called the surgical stage). It is determined by examining tissue removed during an operation. Sometimes, if surgery is not possible right away or at all, the cancer will be given a clinical stage instead. This is based on the results of a physical exam, biopsy, and imaging tests. The clinical stage will be used to help plan treatment. Sometimes, though, the cancer has spread further than the clinical stage estimates, and may not predict the patient’s outlook as accurately as a pathologic stage.
Salivary gland staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Salivary cancer staging
| AJCC stage | Stage grouping | Stage description* |
| 0 | Tis N0 M0 | The cancer is confined to the cells lining the salivary duct (Tis). It has not spread to nearby lymph nodes (N0) or distant sites (M0). This stage is also known as carcinoma in situ (Tis). |
| I | T1 N0 M0 | The cancer is 2 cm (about ¾ inch) or smaller. It’s not growing into nearby tissues (T1). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| II | T2 N0 M0 | The cancer is larger than 2 cm but no larger than 4 cm (about 1½ inch). It’s not growing into nearby tissues (T2). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| III
| T3 N0 M0 | The cancer is larger than 4 cm and/or is growing into nearby soft tissues (T3). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| OR | ||
| T0, T1, T2, T3 N1 M0 | The cancer is any size and might have grown into nearby soft tissues (T0-T3) AND has spread to 1 lymph node on the same side of the head or neck as the primary tumor. The cancer has not grown outside of the lymph node and the lymph node is no larger than 3 cm (about 1¼ inch) (N1). It has not spread to distant sites (M0). | |
| IVA | T4a N0 or N1 M0 | The cancer is any size and is growing into nearby structures such as the jaw bone, skin, ear canal, and/or facial nerve. This is known as moderately advanced disease T4a) AND:
It has not spread to distant sites (M0). |
| OR | ||
| T0, T1, T2, T3 or T4a N2 M0 | The cancer is any size and might have grown into nearby soft tissues or structures such as the jaw bone, skin, ear canal, and/or facial nerve (T0-T4a) AND any of the following:
It has not spread to distant organs (M0). | |
| IVB | Any T N3 M0 | The cancer is any size and might have grown into nearby soft tissues or structures (Any T) AND any of the following:
It has not spread to distant organs (M0). |
| OR | ||
| T4b Any N M0 | The cancer is any size and is growing into nearby structures such as the base of the skull or other bones nearby, or it surrounds the carotid artery. This is known as very advanced disease (T4b). It might or might not have spread to nearby lymph nodes (Any N). It has not spread to distant organs (M0). | |
| IVC | Any T Any N M1 | The cancer is any size and may have grown into nearby soft tissues or structures (Any T) AND it might or might not have spread to nearby lymph nodes (Any N). It has spread to distant sites such as the lungs (M1). |
* The following additional categories are not listed on the table above:
TX: Main tumor cannot be assessed due to lack of information.
T0: No evidence of a primary tumor. The N categories are described in the table above, except for:
NX: Regional lymph nodes cannot be assessed due to lack of information.
Parotid tumor removal
In most cases, parotid tumor surgery to remove all or a part of the parotid gland (parotidectomy) is the preferred treatment for parotid tumors.
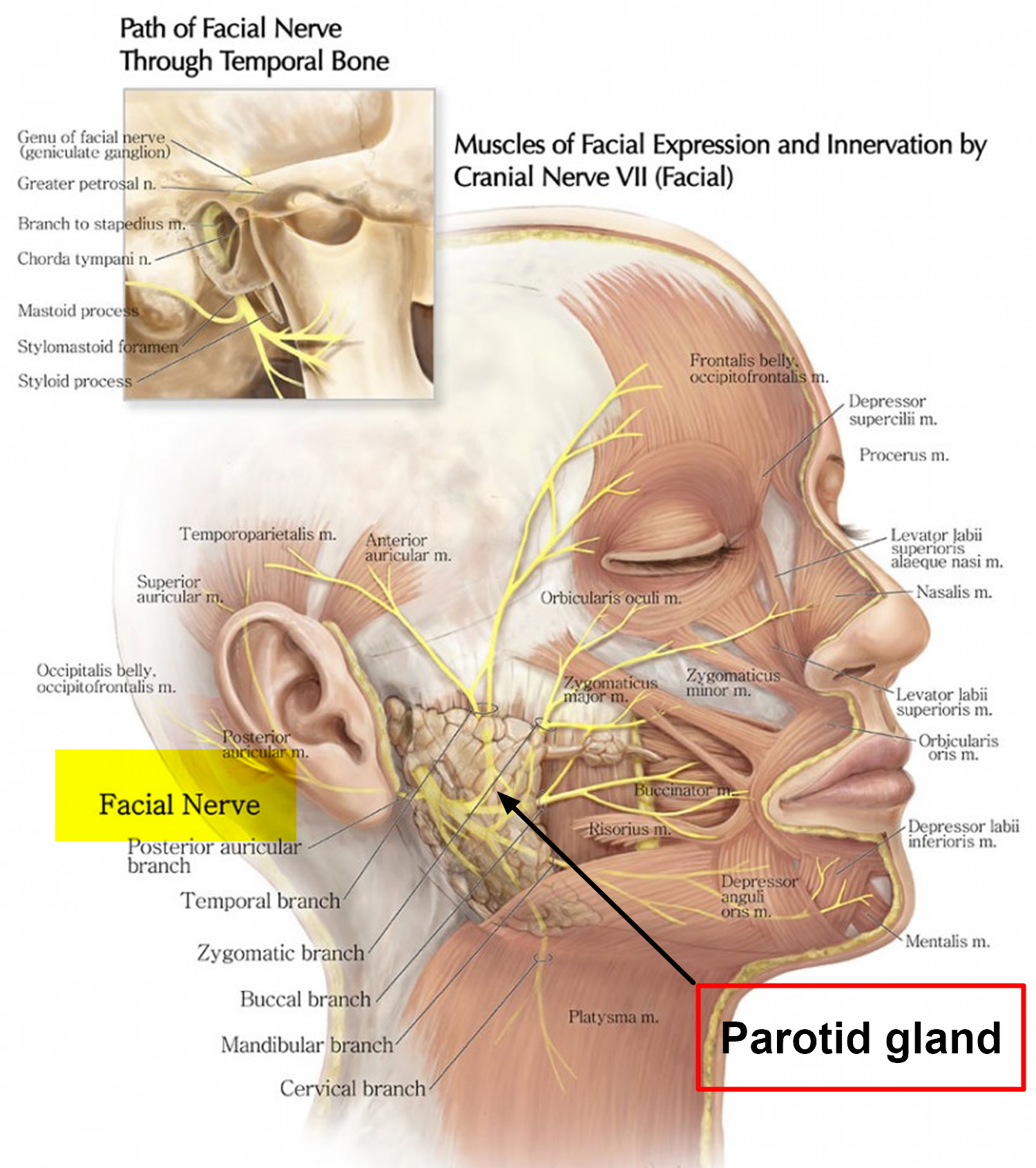
Salivary gland surgery can be difficult because several important nerves are located in and around the glands. For example, a nerve in the face that controls facial movement runs through the parotid gland.
Removing tumors that involve important nerves may require damaging the nerves, causing partial paralysis of your face (facial droop). Surgeons take care to preserve these nerves whenever possible. In some cases, severed nerves can be repaired with nerves taken from other areas of your body.
Special care must be taken to avoid damaging the facial nerve that runs through the parotid gland.
Surgery for salivary gland tumors may include:
- Removing a portion of the affected salivary gland. If your tumor is small and located in an easy-to-access spot, your surgeon may remove the tumor and a small portion of healthy tissue that surrounds it.
- Removing the entire salivary gland. If you have a larger tumor, your doctor may recommend removing the entire salivary gland. If your tumor extends into nearby structures — such as the facial nerves, the ducts that connect your salivary glands, facial bones and skin — these also may be removed.
- Removing lymph nodes in your neck. If there’s evidence that cancer has spread to the lymph nodes in your neck, your surgeon may remove most of the lymph nodes in your neck (neck dissection).
- Reconstructive surgery. After surgery to remove the tumor, your doctor may recommend reconstructive surgery to repair the area. If bone, skin or nerves are removed during your surgery, these may need to be repaired or replaced with reconstructive surgery. During reconstructive surgery, the surgeon works to make repairs that improve your ability to chew, swallow, speak or breathe. You may need grafts of skin, tissue or nerves from other parts of your body to rebuild areas in your mouth, throat or jaw.
How is parotid gland surgery performed?
Surgery to remove the parotid gland is performed under general anesthetic and usually takes about one to two hours to perform. A cut is made from in front of the ear and is usually extended down into the neck. At the end of the operation the cut is closed using stitches and usually heals very well.
Before removal of the gland, a very important nerve called the facial nerve needs to be identified. This nerve operates the muscles of the face and eyelid. So long as the nerve is not involved in the tumor and is fully functional, the aim will be to keep this nerve undamaged.
After removing the tumor, a plastic tube drain may be placed through the skin before closing the wound. This is to reduce chance of blood clot collection under the skin. It can usually be removed after 24-48 hours.
Possible complications of parotid tumor surgery
Facial weakness
The facial nerve, which operates the muscles of facial expression and eye closure, runs directly through the parotid gland. If it is damaged during the surgery this can lead to a weakness of the face (facial palsy). A temporary facial weakness (15-20%) may occur if the nerve is stretched or bruised, particularly when the tumor is very close to the nerve. This may last for a few weeks. It is rare (1% ) to get a permanent weakness of the face following this sort of surgery for benign tumors. For malignant tumors, there will be greater risk of temporary and permanent weakness
Numbness of the ear lobe and the face
The ear lobe may become permanently numb and extra care may be needed when shaving or inserting earring. The majority of patients become less aware of the numbness over time.
An expected consequence of the surgery is numbness on the side of the face for few weeks.
Hematoma
A blood clot (a hematoma) may collect beneath the skin after surgery. A drain is used to avoid this, but it can get blocked. Occasionally a return to the operating theater is required to remove the clot.
Salivary fistula
Occasionally the cut surface of the residual parotid gland may leak saliva and collect under the skin. The saliva may leak out along the skin incision. This will settle in time but may require medical intervention such as treatment of infection if present.
Frey’s syndrome
Some patients develop flushed and sweaty cheek on eating. The tiny nerves which usually cause the gland to produce saliva are interrupted during surgery. Their re-growth to supply the overlying skin is the cause of the Frey’s syndrome. Treatment with a roll-on antiperspirant and in severe cases with Botox injections may be required.
Cosmetic asymmetry
The bigger the parotid lump to begin with, the bigger the sunken appearance and asymmetry after surgery.
Salivary gland cancer treatment
If you’ve been diagnosed with salivary gland cancer, your cancer care team will discuss your treatment options with you. It’s important to weigh the benefits of each treatment option against the possible risks and side effects.
Which treatment option(s) might be best for you depends on many factors, including the type, grade, and stage of the cancer; your overall health; the chances of curing the disease; the impact of the treatment on functions like speech, chewing, and swallowing; and your own personal preferences.
Common treatment options for salivary gland cancer include:
- Surgery
- Radiation therapy
- Chemotherapy
Sometimes more than one type of treatment is used.
For malignant parotid tumors, your doctor may also recommend radiation therapy. To date, chemotherapy has proved to be ineffective for this type of cancer.
Radiation therapy
If you’re diagnosed with having salivary gland cancer, your doctor may recommend radiation therapy. Radiation therapy uses high-powered energy beams, such as X-rays and protons, to kill cancer cells. During radiation therapy, you lie on a table while a machine moves around you, directing high-powered beams at specific points on your body.
A newer type of radiation therapy that uses particles called neutrons may be more effective in treating certain salivary gland cancers. More study is needed to understand the benefits and risks of this treatment. Neutron radiation therapy isn’t widely available in the United States.
Radiation therapy can be used after surgery to kill any cancer cells that might remain. If surgery isn’t possible because a tumor is very large or is located in a place that makes removal too risky, your doctor may recommend radiation alone or in combination with chemotherapy.
Coping with dry mouth
People who undergo radiation therapy to the head and neck area often experience very dry mouth (xerostomia). Having a dry mouth can be uncomfortable. It can also lead to frequent infections in your mouth, cavities and problems with your teeth, and difficulty eating, swallowing and speaking.
You may find some relief from dry mouth and its complications if you:
- Brush your teeth several times each day. Use a soft-bristled toothbrush and gently brush your teeth several times each day. Tell your doctor if your mouth becomes too sensitive to tolerate gentle brushing.
- Rinse your mouth with warm salt water after meals. Make a mild solution of warm water and salt. Rinse your mouth with this solution after each meal.
- Keep your mouth moistened with water or sugarless candies. Drink water throughout the day to keep your mouth moistened. Also try sugarless gum or sugarless candies to stimulate your mouth to produce saliva.
- Choose moist foods. Avoid dry foods. Moisten dry food with sauce, gravy, broth, butter or milk.
- Avoid acidic or spicy foods and drinks. Choose foods and drinks that won’t irritate your mouth. Avoid caffeinated and alcoholic beverages.
Tell your doctor if you have dry mouth. Treatments may help you cope with more-severe signs and symptoms of dry mouth. Your doctor may also refer you to a dietitian who can help you find foods that are easier to eat if you’re experiencing dry mouth.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care. Palliative care can be used while undergoing other aggressive treatments, such as surgery, chemotherapy or radiation therapy.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.
Coping and support
Learning you have a salivary gland tumor can be frightening. Each person deals with this diagnosis in his or her own way. With time you’ll discover ways of coping that work for you. Until then, you might find some comfort if you:
- Learn enough to feel comfortable making treatment decisions. Ask your doctor for details about your tumor — the type, stage and treatment options. The more you know, the more comfortable you may feel when making treatment decisions. If you have salivary gland cancer, ask your doctor to recommend reliable sources of information where you can learn more. Good places to start include the National Cancer Institute and the American Cancer Society.
- Ask friends and family to be your support system. Your close friends and family can provide a support system that can help you cope during treatment. They can help you with the small tasks you may not have the energy for during treatment. And they can be there to listen when you need to talk.
- Connect with others. Other people who’ve had salivary gland tumors can offer unique support and insight because they understand what you’re experiencing. Connect with others through support groups in your community. If you have salivary gland cancer, ask your doctor about support groups or contact your local chapter of the American Cancer Society 1. Online support groups also are available.
- Take care of yourself during treatment. Get enough rest each night so that you wake feeling rested. Try to exercise when you feel up to it. Choose a healthy diet full of fruits and vegetables.
- American Cancer Society. https://www.cancer.org/[↩]





{kind=link}