Contents
What is perianal abscess
An abscess is a localized collection of pus. In perianal abscess, a localized collection of pus can either occur near the anus under the skin, or deeper, adjacent to the rectum. Perianal abscesses are the most common type of anorectal abscesses 1). Perianal abscesses are more common in patients with diabetes mellitus, Crohn’s disease, and patients who are immunocompromised for any reason. Perianal abscess affects men more than women. Perianal abscess may occur in infants and toddlers who are still in diapers and who have a history of anal fissures. Perianal abscess rarely goes away on its own. Antibiotics alone usually cannot treat an abscess.
The prevalence of perianal abscesses and anorectal abscesses, in general, are underestimated, since most patients do not seek medical attention, or are dismissed as symptomatic hemorrhoids. It is estimated that there are approximately 100,000 cases of the benign anorectal disease in general. The mean age at presentation is 40 years old, and adult males are twice as likely to develop with abscess than females 2).
On presentation, patients will most commonly complain of severe pain in the anal area. This is due to an infection of the anal glands which are not adequately draining through the anal crypts. The anal glands empty into ducts that traverse the internal sphincter and empty into the anal crypts at the level of the dentate line. Infection of these glands if not adequately draining will form an abscess which can spread along several planes along the perianal or perirectal spaces. The perianal space surrounds the anus and is continuous with the fat of the buttock.
Aerobic and anaerobic organisms have been found to be responsible for these abscesses including Bacteroides fragilis, Peptostreptococcus, Prevotella, Fusobacterium, Porphyromonas, Clostridium species, Staphylococcus aureus, Streptococcus, and Escherichia coli. Once the collection forms, it can spread along the path of least resistance, which is typically into the intersphincteric space and other potential spaces.
Perianal abscesses can cause quite a bit of discomfort for patients. Patients with perianal abscess typically present with pain around the anus, which may or may not be associated with bowel movements, but is usually constant. Purulent discharge may be reported if the abscess is spontaneously draining, and blood per rectum may be reported in a spontaneously draining abscess.
Perianal abscesses are located at the anal verge and if left untreated can extend into the ischioanal space or intersphincteric space since these areas are continuous with the perianal space. Perianal abscesses can also cause systemic infection if left untreated 3).
A perianal abscess fistula is an abnormal communication/track between two epithelial surfaces – in the case of fistula-in-ano, between the ano-rectal passage and the surface skin near the anus. It occurs as a complication of an ano-rectal abscess which has discharged to the skin, with the track from anorectal passage to the skin remaining patent. A perianal abscess fistula (fistula-in-ano) complicates 30-50% of perianal abscesses. They are more common in patients with inflammatory bowel disease, in particular Crohn’s disease and diabetes mellitus. Surgical correction is the treatment of choice for a fistula-in-ano because spontaneous healing of a fistula is rare. A fistulotomy is used to open the track and subsequently allow it to heal. Fistulas in Crohn’s disease may be more difficult to treat.
Horseshoe perianal abscesses are uncommon. They are abscesses which surround the entire anus. These abscesses are typically drained through an incision and drainage posterior to the anus. It is helpful to place counter incisions at the anterior extent of the abscess to ensure adequate drainage. Penrose drains may be placed through these incisions to aid in continued drainage. These drains are left in place for 2 to 3 weeks and then removed in the post-operative office visit.
Prompt follow-up with surgical services is advisable to monitor wound healing. Inadequate drainage may result in the reformation of an abscess, which may require repeat incision and drainage. If not promptly diagnosed and treated, perianal abscesses may lead to several other sequelae including fistula in ano, perianal sepsis, or necrotizing soft tissue infection of the anus and surrounding buttock. If fistula in ano is detected, patients will need operative drainage, fistulotomy or seton placement, which may have a risk of incontinence. A seton is a flexible piece of permanent material inserted through the fistula tract. Silastic vessel loops and silk sutures are common materials used as setons. Necrotizing soft tissue infection treatment goals are debridement of all non-viable tissue and may require colostomy for diversion of stool during healing. If not adequately treated, necrotizing soft tissue infection may have mortality as high as 50%.
Perianal abscess treatment
A perianal abscess should be treated in a timely fashion by incision and drainage 4).
Most perianal abscesses can be treated in the office setting. Some conditions, such as cellulitis without fluctuance, failed drainage in the office, abscesses with associated systemic signs of sepsis, or extensive abscesses, are more appropriately treated in the operating room, where a thorough examination under anesthesia can ensure optimal diagnostic evaluation and drainage.
Treatment involves surgery to open and drain the abscess:
- Surgery is usually done with local numbing medicine, along with medicine to make you sleepy. Sometimes, spinal or general anesthesia is used.
- Surgery is most often an outpatient procedure, which means that you go home on the same day. The surgeon cuts open the abscess and drains the pus.
- Sometimes a drain is put in to keep the incision open and draining, and sometimes the abscess cavity is packed with gauze.
- If the pus collection is deep, you may need to stay in the hospital longer for pain control and nursing care of the abscess drainage site.
- After surgery, you may need warm sitz baths (sitting in a tub of warm water). This helps relieve pain and reduce swelling.
Drained abscesses are usually left open and no stitches are needed.
The surgeon may prescribe painkillers and antibiotics.
You may need stool softeners. Practice good hygiene. Eat soft or liquid foods until the abscess has healed.
Avoiding constipation will help decrease pain. You may need stool softeners. Drinking fluids and eating foods with lots of fiber can also help.
Figure 1. Perianal abscess

Anus anatomy
Evaluation and treatment of perianal abscess-fistula disease require a thorough understanding of anal anatomy. Understanding the anatomy helps to determine the origin and the subsequent course of this disease process and also helps both to direct therapeutic interventions and to risk-stratify outcomes. The inner circular muscle of the rectal wall descends into the anal canal, where it becomes the internal sphincter. This is encircled by an outer funnel of muscular tissue that is composed of the levator, puborectalis, and external sphincter muscles. These two layers are separated by the intersphincteric plane, a fibrous extension of the outer longitudinal muscle layer of the rectum as it extends down into the anal canal. The lower edge of this plane, the intersphincteric groove, can be palpated at the lower border of the sphincter complex. Just distal to this is the anal verge, the true distal margin of the anal canal. The anal verge is the demarcation between the skin of the anal margin and the anoderm. The anoderm is specialized squamous epithelium, which, although devoid of secondary skin appendages such as hair follicles and sweat glands, has a rich vascular supply and is highly innervated. Midway up the anal canal lies the dentate line (pectinate line). This marks the true mucocutaneous junction between somatically innervated squamous epithelium distally and the viscerally innervated columnar epithelium proximally. Seminal work by Parks and Eisenhammer identified anal glands present at the level of the dentate line and showed that these glands are the etiology of most perirectal abscesses and fistulas 5).
When documenting anatomical findings and pathological processes in the perianal region, use of the “clock face” descriptive should be abandoned in favor of proper anatomical terminology such as “anterior,” “posterior,” “left,” and “right.” These terms are more accurate and less susceptible to misinterpretation, as the orientation of the clock face changes with the different positions of the patient and the examiner.
Figure 2. Anus anatomy
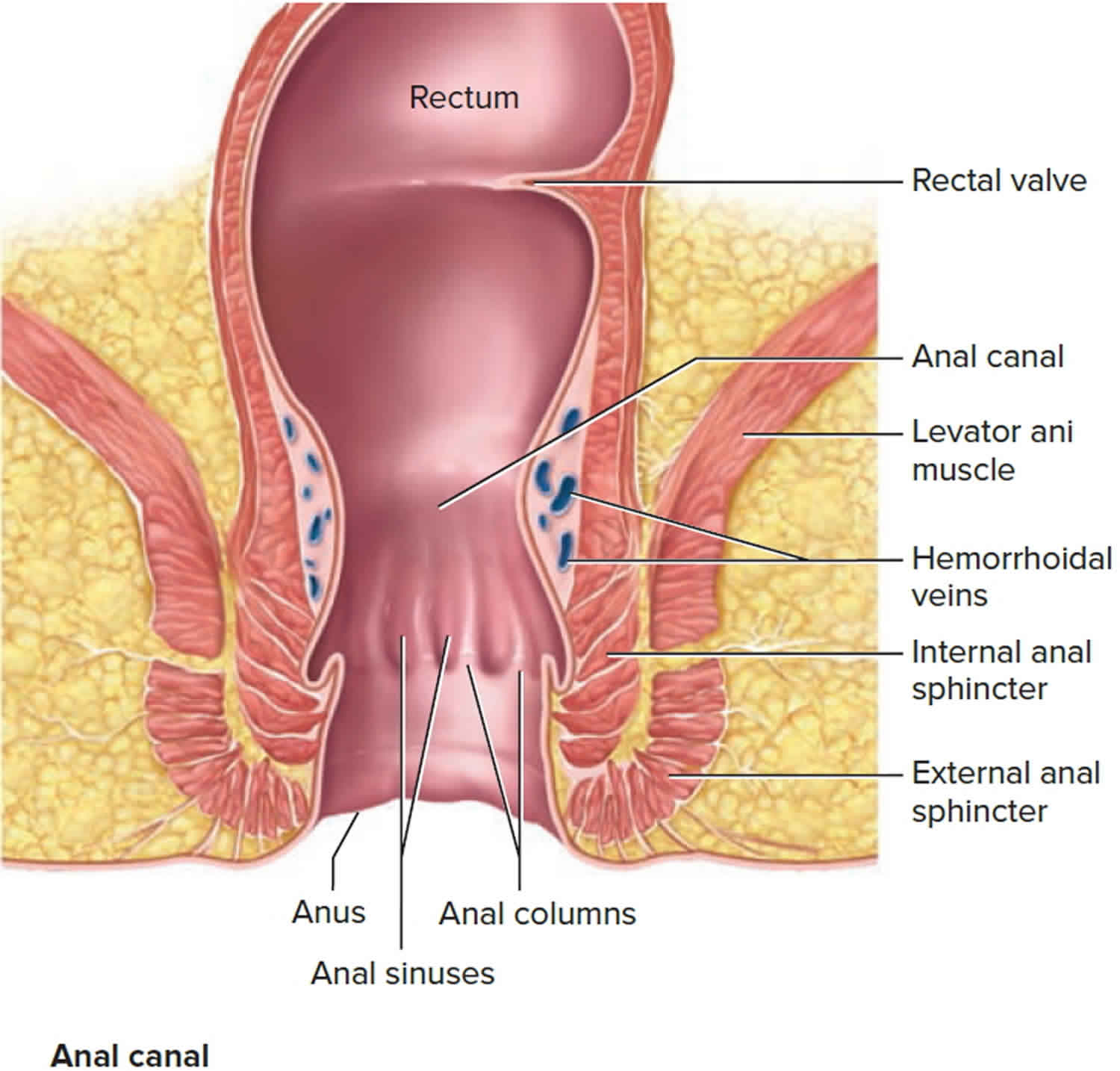
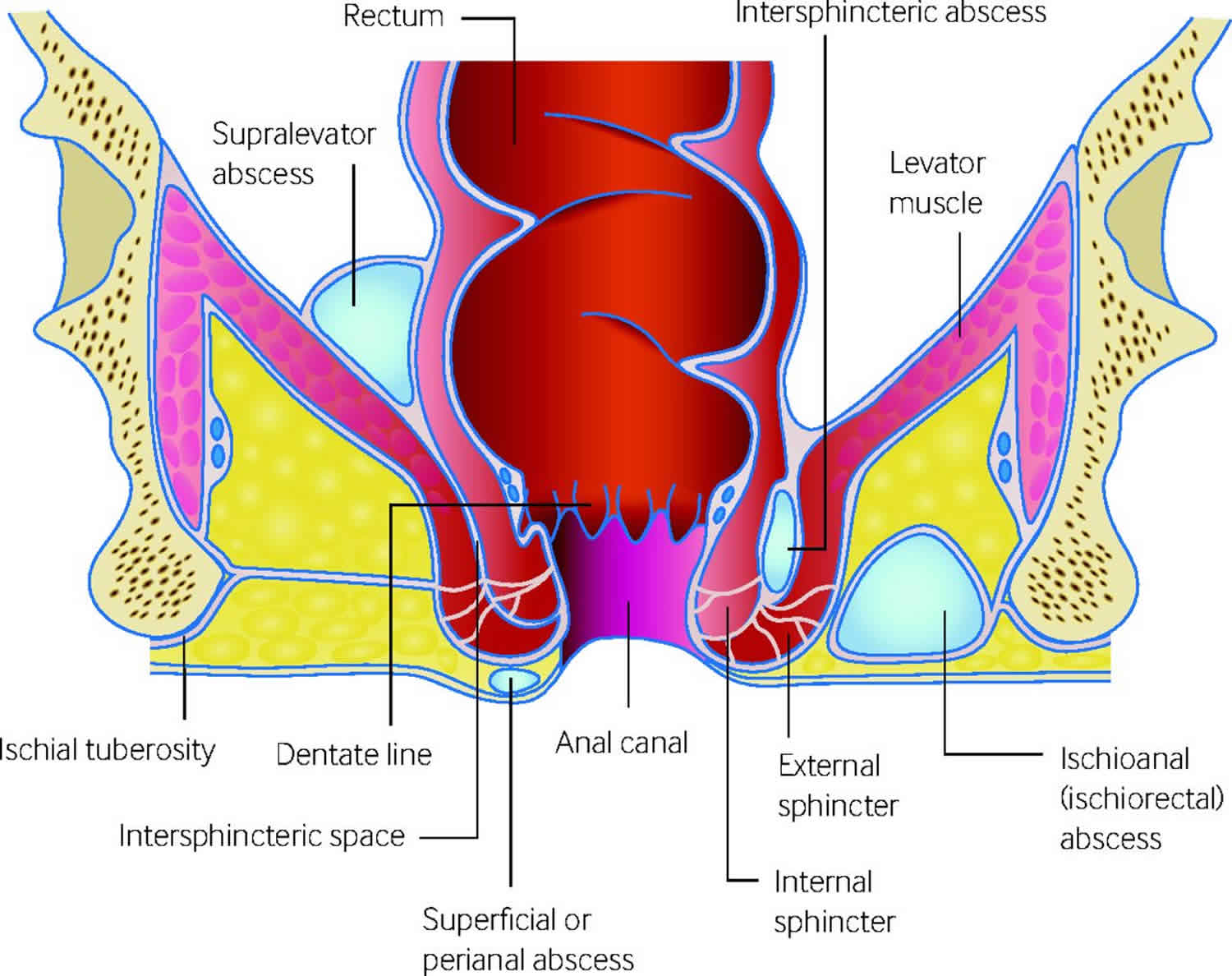
Figure 3. Perianal abscess anatomy
What is perianal abscess fistula
A fistula-in-ano represents the chronic phase of ongoing perianal sepsis. A previous history of perianal abscess, drained either spontaneously or surgically, can usually be elicited. Patients often report a cyclical pattern of pain, swelling, and drainage. Moisture can cause skin irritation, excoriation, and pruritus. Crohn’s disease should be excluded in a fistula patient reporting a history of chronic diarrhea or abdominal pain.
Physical examination usually identifies one or more external openings with or without granulation tissue. Occasionally, the external opening may be subtle and appreciated only after closer inspection of an indurated area. Palpation may elicit tenderness, expression of pus, and a fibrotic cord extending in toward the anus.
Fistula-in-ano classification
Parks et al. 6) categorized anal fistulas into four types based on their location relative to the anal sphincter complex: intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric. This system is clinically useful because it helps predict what risk a fistulotomy may pose to fecal continence based on the amount of overlying sphincter that would need to be divided.
Anal fistulas are also categorized as “complex” when they have any of the following risk factors: a high tract that traverses more than 30 to 50% of the external sphincter, an anterior location in a female, multiple tracts, and a patient with preexisting incontinence, recurrent fistula, local irradiation, chronic diarrhea, or Crohn’s disease 7). Treatment of complex fistulas carries higher risks of recurrence, derangements of fecal continence, and failure of or delayed healing. Most fistulas, however, are considered “simple” in that they do not have any of these risk factors, and treatment of simple fistulas results in a low incidence of fecal incontinence and poor wound healing.
Fistula-in-ano treatment
Simply stated, the goals in treatment of anal fistula are to eliminate the septic foci along with any associated epithelialized tracts and to do so with the least amount of functional derangement, the lowest recurrence rate, and the shortest healing time. No single technique is appropriate for treatment of all fistulas. Optimal treatment, therefore, must be directed by the surgeon’s experience and judgment. There is always a progressive trade-off between extent of operative sphincter division and the postoperative functional detriment 8) Postoperative functional outcomes can be adversely affected by preexisting incontinence, previous mechanical sphincter injury, the amount of sphincter at risk, anterior location in females, stool consistency, and the patient’s tolerance of potential imperfections in continence 9).
Treatment of a complex anal fistula
Anal fistulas are considered complex when they cross a significant amount of sphincter (high transsphincteric, extrasphincteric, suprasphincteric) or are associated with high-risk conditions (Crohn’s disease, preexisting fecal incontinence, multiple tracts, anterior location in women).
As with simple fistulas, the anatomy of most complex fistulas can be defined during careful examination under anesthesia. However, radiographic evaluation may be a beneficial adjunct to identify an occult internal opening, secondary tracts, or abscesses or to help delineate the fistula’s relationship to the sphincter complex 10). In these instances, computerized axial tomography scan and fistulography have been supplanted by magnetic resonance imaging and endorectal ultrasonography as the imaging modalities of choice.
Complex anal fistulas may be treated with fibrin glue injection or anal fistula plug. As mentioned previously, these two techniques are sphincter sparing, easily repeatable, and have low morbidity, making them particularly appealing in the setting where standard fistulotomy would place patients a high risk for alterations in continence.
Prior to the advent of fibrin glue and anal fistula plugs, the most popular sphincter-preserving technique for the repair of complex fistulas was that of an endorectal advancement flap 11). This technique obliterates the internal fistula opening, requires no sphincter division, and results in no external wound. Preparation for the procedure involves a full bowel preparation with intravenous antibiotics. An examination under anesthesia is performed to identify the fistula and its internal opening. Following curettage and débridement of the chronic tracts, a superiorly based endorectal advancement flap is mobilized in a submucosal plane with or without inclusion of a small portion of the internal sphincter. Mobilization continues proximally in a trapezoid shape, increasing its width with a more cephalad progression. The mobilization continues until completion of a tensionless repair of the rectal mucosa beyond the level of the trimmed internal opening.
The success rates for endorectal advancement flaps are between 55 and 98%. Repeated endorectal advancement flaps have been described; however, these can be more challenging in a scarred, reoperative field 12).
Complex anal fistulas may also be treated by use of setons or staged fistulotomy, or both. A seton is a flexible piece of permanent material inserted through the fistula tract. Silastic vessel loops and silk sutures are common materials used as setons. Setons are useful when fistulotomies are undesirable and likely to result in significant incontinence or poor healing. Setons are used in two fashions, draining (loose) and cutting. A draining seton, as the name implies, facilitates long-term drainage of the abscess cavity and fistula tract and thereby reduces the number of subsequent septic events, shrinks down the cavity, and promotes fibrosis of the tract. Draining setons are indicated for perianal Crohn’s disease or other fistulas with large abscess cavities or multiple tracts. Setons are placed in the operating room by threading the seton through the fistula and tying it loosely to itself. They are usually removed several months later but can be left in indefinitely. Draining setons alone rarely cure the fistula, and one of the other definitive techniques will need to be employed.
Setons may also be used in a cutting fashion. Once the seton is placed through the fistula and around the sphincter complex, the overlying skin and anoderm between the internal and external openings are cut and the seton is tightened down. The seton causes slow necrosis and gradual transection of the sphincter complex. Cutting setons require frequent tightening until the sphincter division is complete. Because cutting setons require frequent tightening and are uncomfortable, they are less well tolerated by patients and are a less appealing therapy than other options for complex fistulas. They are also associated with minor incontinence rates ranging from 34 to 63% 13).
Setons are also used during staged fistulotomies of high anal fistulas. The technique involves identification of the tract under anesthesia. A partial lay-open fistulotomy is performed by unroofing the lower portion of the fistula from the internal opening, through the distal internal sphincter and anoderm, and continuing out to the external opening. The external anal sphincter is then encircled with a draining seton, which is left in place. Over the subsequent 6 weeks the site of the internal sphincter division fibroses. The patient is then returned to the operating room for a subsequent fistulotomy of the encircled external anal sphincter. This should complete the obliteration of the fistula tract. Recurrence rates following staged fistulotomy are low (2 to 9%) but do not come without significant risk of minor (54 to 66%) and major (4 to 26%) incontinence 14).
Perianal abscess causes
Common causes of anorectal abscess include:
- Blocked glands in the anal area
- Infection of an anal fissure
- Sexually transmitted infection (STD)
- Trauma
Deep rectal abscesses may be caused by intestinal disorders such as Crohn disease or diverticulitis.
Perianal abscesses occur as a result of a blocked anal gland that subsequently becomes infected – and thus an abscess forms. These anal glands are at the base of the anal crypts and are located at the level of the dentate line. Most people have between six and eight such glands, which extend down into the internal sphincter and up to and including the intersphincteric groove. Obstruction of these glands leads to stasis, bacterial overgrowth, and ultimately abscesses that are located in the intersphincteric groove 15). These abscesses have several routes of egress, the most common of which are downward extension to the anoderm (perianal abscess) or across the external sphincter into the ischiorectal fossa (ischiorectal fossa abscess). Less common routes of spread are superiorly up the intersphincteric groove to the supralevator space or in the submucosal plane. When the abscess is drained, either surgically or spontaneously, persistence of the septic foci and epithelialization of the draining tract may occur and lead to a chronic fistula-in-ano.
Ninety percent of all anorectal abscesses are caused by non-specific obstruction and subsequent infection of the glandular crypts of the rectum or anus 16). A perianal abscess is a type of anorectal abscess that is confined to the perianal space.
Approximately 10% of perianal abscesses are thought not to be due to infected anal glands but to be a consequence of more specific causes such as Crohn’s disease, trauma, human immunodeficiency virus, sexually transmitted diseases, radiation therapy, foreign body or cancerous origin 17).
Patients with recurrent or complex abscesses should be evaluated for Crohn disease 18).
Fistula-in-ano frequently complicates the above conditions, but it can also be idiopathic (of unknown cause), or arise in patients with tuberculosis, trauma (especially obstetric – after traumatic delivery), carcinoma, pelvic inflammatory disease, radiation damage (post radiotherapy).
Perianal abscess risk factors
The following factors increase the risk for an anorectal abscess:
- Anal sex
- Chemotherapy medicines used to treat cancer
- Diabetes
- Inflammatory bowel disease (Crohn disease and ulcerative colitis)
- Use of corticosteroid medicines
- Weakened immune system (such as from HIV/AIDS)
Perianal abscess prevention
Prevention or prompt treatment of sexually transmitted infection (STDs) may prevent an anorectal abscess from forming. Use condoms during intercourse, including anal sex, to prevent such infections.
In infants and toddlers, frequent diaper changes and proper cleaning during diaper changes can help prevent both anal fissures and abscesses.
Perianal abscess symptoms
Superficial perianal abscesses are often associated with:
- Painful swelling which worsens overtime when left untreated
- Skin irritation around the anus, including swelling, redness, and tenderness
- Discharge of pus
Patients will complain of anal pain which may be dull, sharp, aching, or throbbing. Pain and swelling in the anal region with wetness and soiling, often on a background of Crohn’s disease. In the acute setting, the abscess causes pain and swelling which occurs when sitting and is aggravated by motion, coughing and straining. This may be accompanied by fever, chills, constipation or diarrhea, purulent discharge and bleeding may also occur. The pain is throbbing, continuous and worsened by bowel motions. The discharge on the skin causes erosion, excoriation and pruritis (itchiness).
- Superficial perianal abscesses (subcutaneous, submucosal, ischiorectal abscesses) show typical symptoms such as pain, swelling, tenderness, fever. Due to their anatomic location, they often cause discomfort on walking and sitting. Usually the vicinity to the anal canal causes painful defecation 19).
- Deep perianal abscesses (intermuscular, pelvirectal) often lack typical symptoms. Diffuse pelvic pain and raised body temperature are found occasionally 20).
Chronic fistula may present with discharge on the buttocks and pruritis, and the pain is usually less prominent.
Perianal abscess progression
Perianal abscess if left alone will discharge to the skin, but then the complication of fistula-in-ano will often (30-50%) occur, which will not heal spontaneously. Surgical treatment is, however, usually successful. Neglected perianal abscess fistulas can result in repeated abscesses, multiple openings and complications.
Patients with ano-rectal fistulas commonly have a history of a previously drained anal abscess.
Symptoms include:
- Anorectal pain
- Drainage from the perianal skin
- Irritation of the perianal skin
- Per rectal bleeding
Perianal abscess prognosis
The outcomes of perianal abscess treatment depend on the timing of the surgery. Patients with early diagnosis and treatment tend to have good outcomes, but those who have a delay in treatment usually have prolonged hospital course, need for repeated surgical treatments at higher risk of recurrence. The key to improving outcomes is to follow the patient and monitor for any perianal symptoms closely 21).
Perianal abscess possible complications
Complications of anorectal abscess may include:
- Anal fistula (abnormal connection between the anus and another structure)
- Infection that spreads to the blood (sepsis)
- Continuing pain
- Problem keeps coming back (recurrence)
Perianal abscess diagnosis
A detailed history and physical examination are pertinent to every patient and may be the only requirement for diagnosis.
A physical exam can typically rule out other causes of anal pain, such as hemorrhoids, and will yield an area of fluctuance or an area of erythema and induration in the skin around the perianal area. Cellulitis should be noted and marked if extending beyond the fluctuant area. For follow-up purposes, it should be noted whether the patient has diabetes, and their average blood sugar on routine fingerstick should also be noted.
The digital rectal exam should be performed and may yield a fluctuant mass.
Computed tomography or MRI may be used in the setting of clinical suspicion without signs discussed above, especially in the setting of unexplained significant anorectal pain, and in the immunocompromised patient who may not mount an immune response. MRI is the preferred method of imaging as CT scan may miss small abscesses in the immunocompromised patients. Anorectal ultrasound may be used however it is not tolerated well secondary to pain.
Laboratory testing will usually reveal an elevated white blood cell count. However, an absence of a leukocytosis should not deter the physician from appropriate treatment of an abscess.
Perianal abscess treatment
Perianal abscesses are an indication for timely incision and drainage. Antibiotic administration alone is inadequate and inappropriate, unless the patient is systemically unwell 22). Once incision and drainage are performed, there is no need for antibiotic administration unless certain medical issues necessitate the use 23). Such conditions include valvular heart disease, immunocompromised patients, diabetic patients, or in the setting of sepsis. Antibiotics are also considered in these patients or cases with signs of systemic infection or significant surrounding cellulitis 24).
Incision and drainage are typically performed in an office setting, or immediately in the emergency department. Local anesthesia with 1% lidocaine may be administered to the surrounding tissues. A cruciate incision is made as close to the anal verge as possible to shorten any potential fistula formation. Blunt palpation is used to ensure no other septation or abscess pocket is missed. The drainage should be performed as close to the anus as possible to shorten the length of any possible subsequent fistula tract. It is useful before completion of procedure to excise a skin flap of the cruciate incision or the tips of the four skin flaps to ensure adequate drainage and prevent premature healing of the skin over the abscess pocket. Packing may be placed initially for hemostasis. Continual packing may be further utilized for healing by secondary intention. Patients are encouraged to keep the incision and drainage site clean. Sitz baths may assist in pain relief.
After successful drainage of a perirectal abscess, pain relief is usually immediate. Patients should use warm tub soaks (Sitz bath), bulk-forming fiber laxatives, and analgesics. Bleeding and drainage usually subside within a few days. The wounds should heal over a matter of a few weeks. Surgical follow-up is encouraged because acute abscess recurrences occur in 10%, and development of chronic fistula-in-ano occurs in up to 50% of patients 25).
More extensive abscesses may require the operating room for the adequate exam under anesthesia to ensure adequate drainage, as well as inspect for other diseases such as fistula in ano 26).
Perianal abscess surgery
Perianal abscesses are incised and laid open on the shortest route. The location of the abscess determines the surgical approach. The operation should be performed under regional or general anesthesia.
In subcutaneous or submucosal abscesses located within the outer anal canal, a skin excision should be performed to create free drainage and to prevent early closure of the skin. In perianal abscesses synchronous fistulotomy seems not to impair functional outcome 27). In addition to adequate drainage, one should endeavor to prevent acute recurrence of an abscess by either excising the overlying skin, inserting a drainage catheter, or placing a loose seton 28).
Intermuscular abscesses can be drained transanally to the inside of the anal canal. The abscess cavity is opened by incision of the anoderm and the internal sphincter overlying the abscess. Ischiorectal abscesses are opened by a sufficiently large skin incision into the ischiorectal fossa 29), a synchronous fistulotomy does not seem to be necessary 30).
Drainage of pelvirectal abscesses can also be performed perineally, provided the levators are opened wide enough to assure adequate drainage.
In a pelvirectal abscess with a fistula towards the rectum, the drainage may also be performed transanally.
Perianal abscess antibiotics
Antibiotics are an unnecessary addition to routine incision and drainage of an uncomplicated abscess. They have not been shown to improve healing times or reduce recurrence rate 31). Antibiotics should be considered for patients with high-risk conditions such as immunosuppression, diabetes, extensive cellulitis, prosthetic devices, and high-risk cardiac, valvular, and anatomic conditions 32).
Perianal abscess in patients with Crohn disease
Perianal abscess in patients with Crohn’s disease causes significant morbidity. Even though there are several treatments for perianal abscess, very few are based on evidence 33). Some of the treatments include drainage of the abscess, assessment of the Crohn disease status, determining sinus tracts, medical treatment and surgery. With the availability of new biological therapies, the outcomes are even more conflicting. Once the abscess has been drained, attempts may be made to eradicate the fistula and control Crohn disease. Definitive treatment for perianal complications of Crohn disease is very challenging and rarely lead to complete healing. No matter what treatment is selected one must weight the risk of ana sphincter injury which can be devasting. Given these facts, expert opinion suggests that an interprofessional approach to management of perianal disease in these patients is crucial to improving outcomes 34). Because Crohn’s disease is a systemic disorder, the health care team should consist of the following:
- Colorectal surgeon
- Dietitian to determine the need for nutrition
- Gastroenterologist to monitor for Crohn disease
- Nurses to educate the patient on perianal complications
- Pharmacists to follow the prescribed drugs and ensure that the patient is not developing adverse drug reactions
References [ + ]





{kind=link}