Contents
What is Perthes disease
Legg Calve Perthes disease sometimes called Perthes disease or coxa plana, or avascular necrosis of the hip, is a bone disorder that affects the hips of children. Usually, only one hip is involved, but in about 10 percent of cases, both hips are affected. Legg Calve Perthes (named for the three individual doctors who first described the condition) disease begins in childhood, typically between ages 4 and 10, and affects boys more frequently than girls. Perthes disease is five times more common in boys than in girls, however, it is more likely to cause extensive damage to the bone in girls. In 10% to 15% of all cases, both hips are affected. Perthes disease is not contagious.
In Perthes disease the blood supply to the head of the thigh bone is disrupted temporarily which causes the femoral head to break down. As a result, the femoral head is no longer round and does not move easily in the hip socket, which leads to hip pain, limping, and restricted leg movement. The bone eventually begins to heal itself through a normal process called bone remodeling, by which old bone is removed and new bone is created to replace it. This cycle of breakdown and healing can recur multiple times. Affected individuals are often shorter than their peers due to the bone abnormalities. Many people with Legg Calve Perthes disease go on to develop a painful joint disorder called osteoarthritis in the hips at an early age. Most children recover from Perthes’ disease, but it can take two to five years for the bone to regrow and return to normal, or close to normal.
There are four stages in Perthes disease:
- Initial / necrosis. In this stage of the disease, the blood supply to the femoral head is disrupted and bone cells die. The area becomes intensely inflamed and irritated and your child may begin to show signs of the disease, such as a limp or different way of walking. This initial stage may last for several months.
- Fragmentation. Over a period of 1 to 2 years, the body removes the dead bone and quickly replaces it with an initial, softer bone (“woven bone”). It is during this phase that the bone is in a weaker state and the head of the femur is more likely to break apart and collapse.
- Reossification. New, stronger bone develops and begins to take shape in the head of the femur. The reossification stage is often the longest stage of the disease and can last a few years.
- Healed. In this stage, the bone regrowth is complete and the femoral head has reached its final shape. How close the shape is to round will depend on several factors, including the extent of damage that took place during the fragmentation phase, as well as the child’s age at the onset of disease, which affects the potential for bone regrowth.
To keep the ball part of the joint as round as possible, doctors may use a variety of treatments to keep it snug in the socket portion of the joint. The socket acts as a mold for the fractured femoral head as it heals.
The incidence of Legg Calve Perthes disease varies by population. The condition is most common in white populations, in which it affects an estimated 1 to 3 in 20,000 children under age 15. Perthes disease usually affects children aged from 3 to 11 in one hip. In some cases, it affects both hips, and it sometimes runs in families.
Despite general consensus that Legg-Calve-Perthes disease results from the uncoupling of bone metabolism with increased resorption and delayed formation, the exact cause remains elusive.
Legg Calve Perthes disease is usually not caused by genetic factors. The cause in these cases is unknown. In a small percentage of cases, mutations in the COL2A1 gene cause the bone abnormalities characteristic of Legg Calve Perthes disease. The COL2A1 gene provides instructions for making a protein that forms type II collagen. This type of collagen is found mostly in cartilage, a tough but flexible tissue that makes up much of the skeleton during early development. Most cartilage is later converted to bone, except for the cartilage that continues to cover and protect the ends of bones and is present in the nose and external ears. Type II collagen is essential for the normal development of bones and other connective tissues that form the body’s supportive framework.
COL2A1 gene mutations involved in Legg Calve Perthes disease lead to production of an altered protein; collagen that contains this protein may be less stable than normal. Researchers speculate that the breakdown of bone characteristic of Legg Calve Perthes disease is caused by impaired blood flow to the femoral head, which leads to death of the bone tissue (osteonecrosis); however it is unclear how abnormal type II collagen is involved in this process or why the hips are specifically affected.
When Perthes disease is associated with COL2A1 gene mutations, the condition is inherited in an autosomal dominant pattern, which means one copy of the altered COL2A1 gene in each cell is sufficient to cause the disorder.
Most COL2A1-associated Perthes disease cases result from new mutations in the gene and occur in people with no history of the disorder in their family. These cases are referred to as sporadic. In other cases, the condition is passed through families. In these cases, referred to as familial, an affected person inherits the mutation from one affected parent.
Figure 1. Hip joint
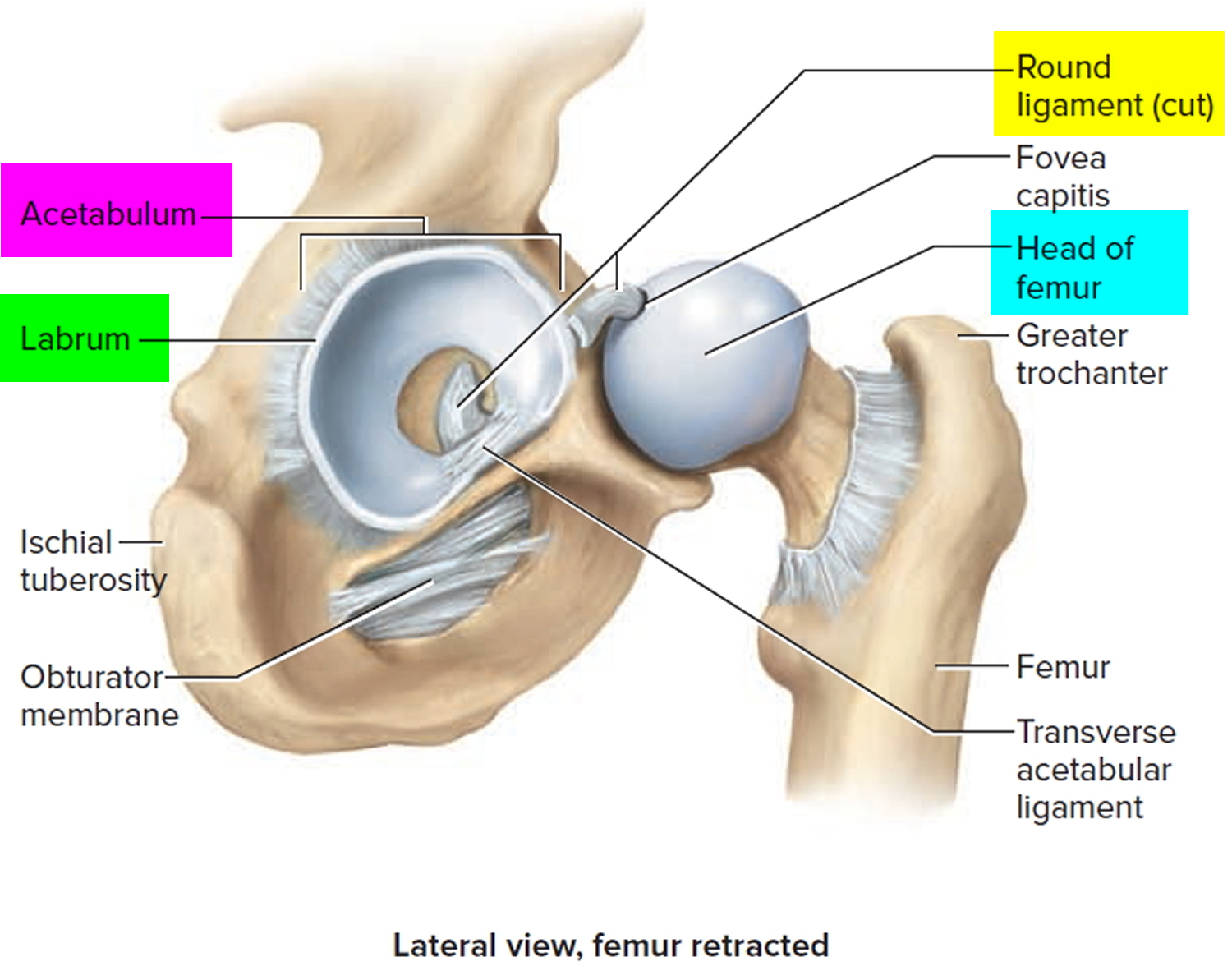
Figure 2. Hip joint frontal section
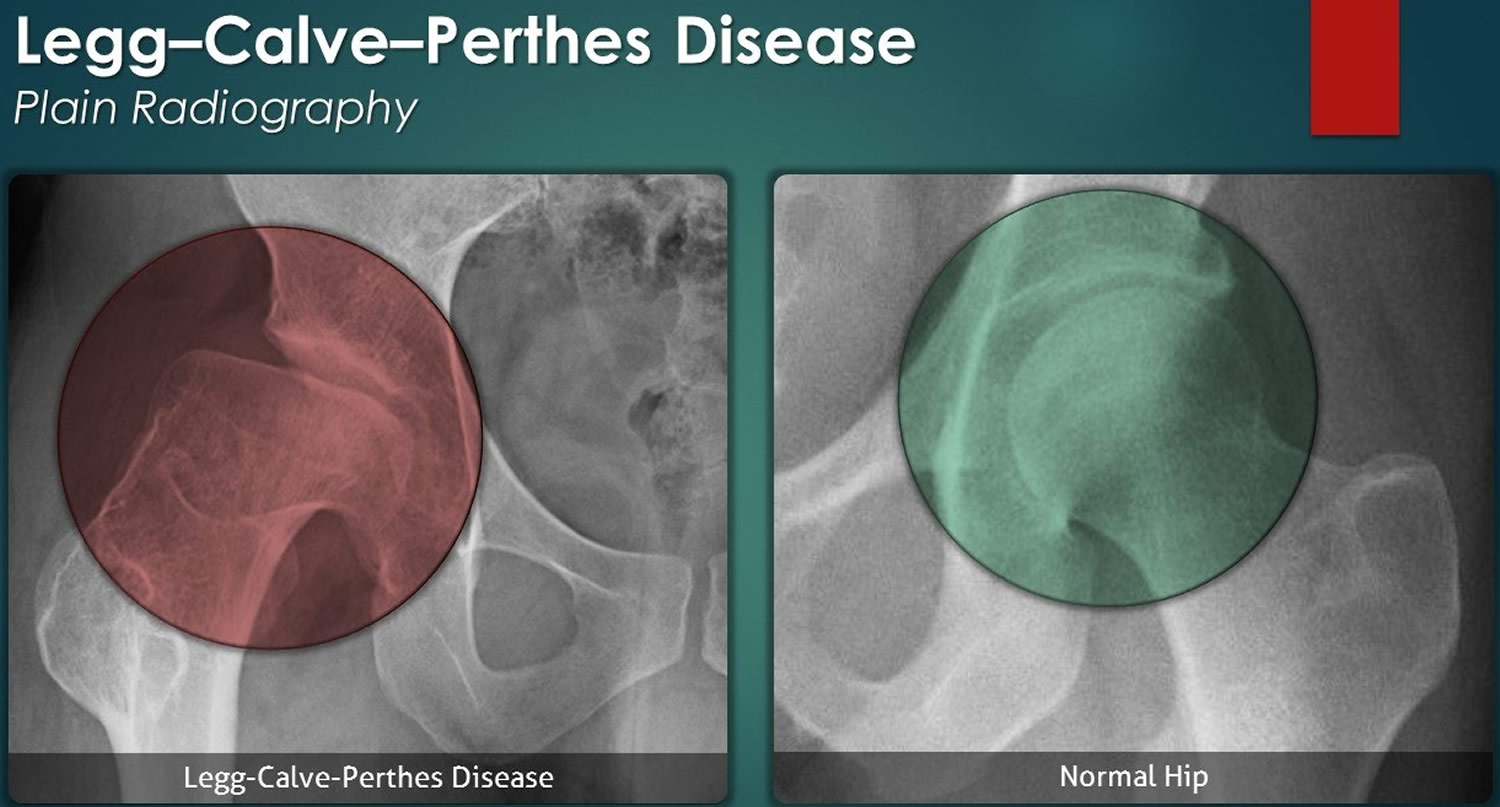
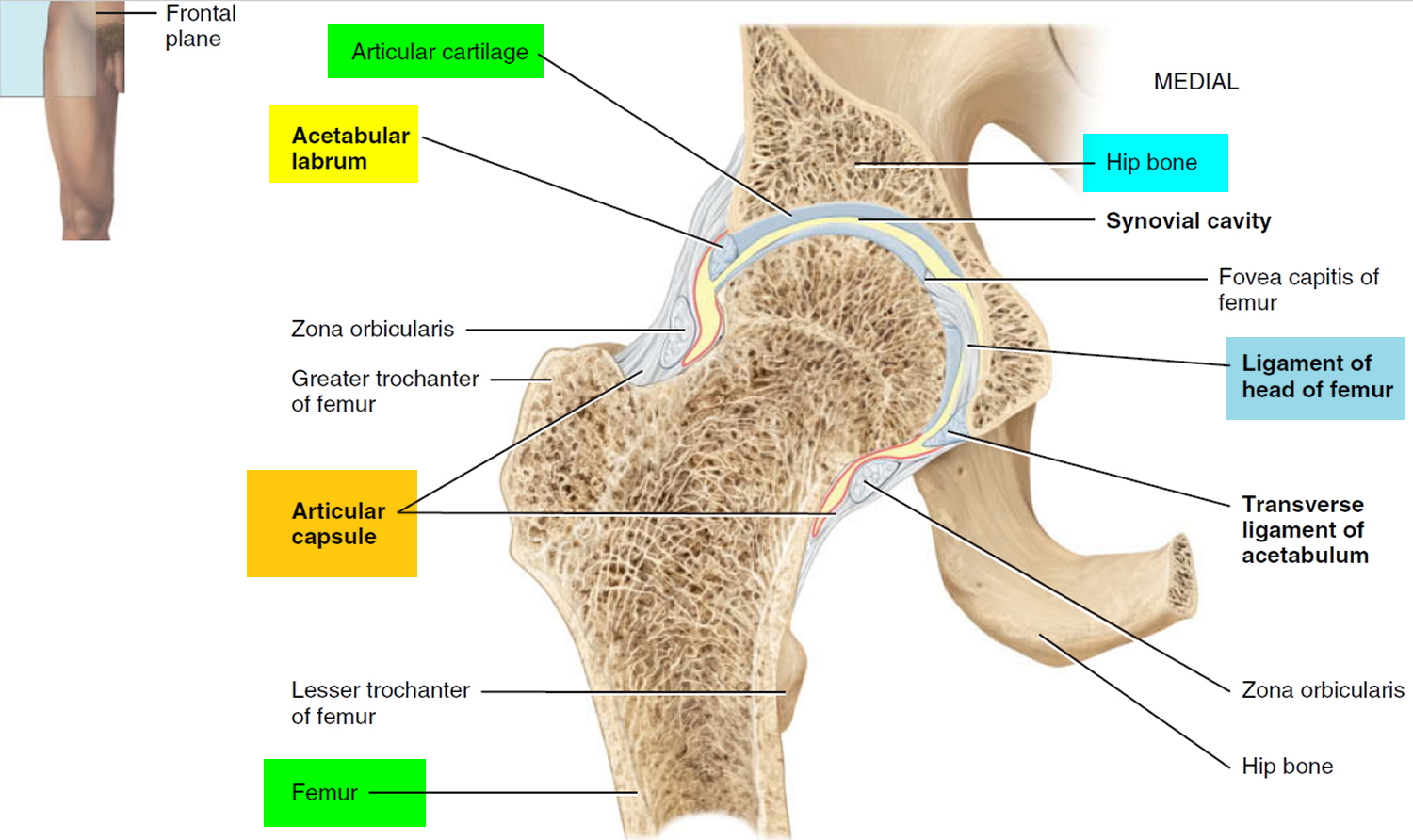 Figure 3. Legg-Calve-Perthes disease
Figure 3. Legg-Calve-Perthes disease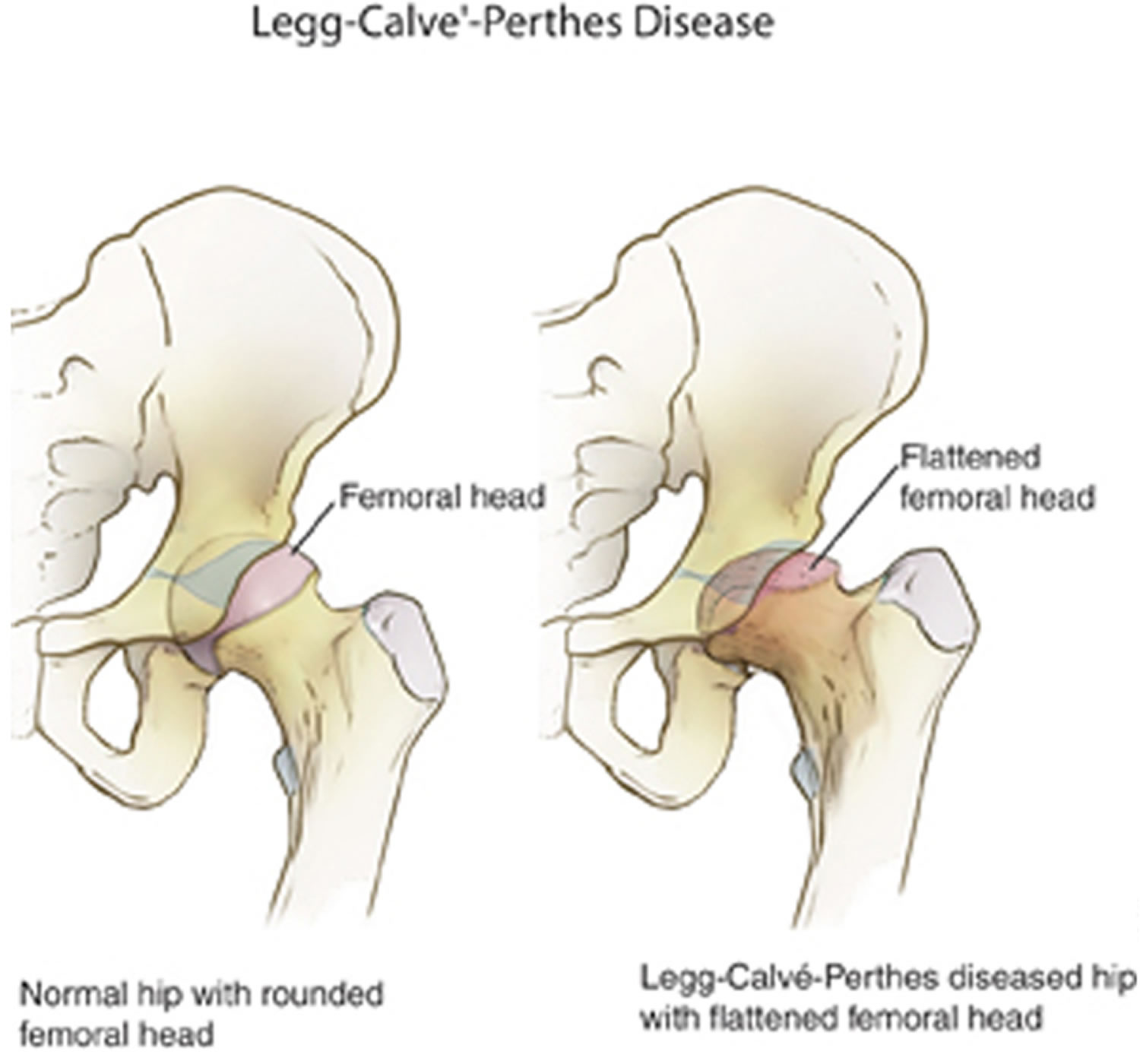
How long will Perthes Disease last?
Perthes disease runs a slow course. As you have probably already noted in your own child, the onset of symptoms – limp, pain in hip or thigh – develops slowly, indeed, there may be no pain at all.
Recovery also takes a long time – rarely less than 18 months, and sometimes longer than two years. This may seem an unbearably long time, but if considered as a part of a whole lifetime, it is worth some sacrifice of time and effort if it achieves a useful, instead of a permanently damaged, hip joint for your child. Your child will need to be in bed for only a small part of this.
What of my child’s future?
Perthes Disease is a self limiting disease. It will pass through the stages described above and finally heal. This may take a long time, but in the majority of cases, there will be a good recovery. This means that your child will have a painless hip with a good range of movement.
A few children will be left with some stiffness and pain in the hip. Because the precise cause is unknown, results cannot always be predicted. Nevertheless, it is known that the more closely the principles of treatment are adhered to the more likely is a good result.
Other problems
Various problems of a financial, social or domestic nature may arise during this long period of treatment. Both your doctor and the social workers at the hospital are available to discuss these with you so that all may work together towards ensuring the best possible outcome for your child with Perthes Disease.
Should either you or your family need any additional information please do not hesitate to contact your doctor or the orthopedic surgeon.
Perthes disease outlook (prognosis)
In most children, the blood supply to the hip joint returns and the femoral head regenerates by itself. This can take anywhere between two and five years. During this time provide understanding and support to help your child find other activities they can enjoy that don’t require weight bearing on the affected leg.
Generally speaking, the younger the child is when they develop Perthes’ disease, the better the outcome. The degree of damage to the femoral head also determines the long term outlook.
Some children may develop osteoarthritis in the affected joint later in life, and in rare cases, hip replacement surgery may be required. However most children respond well to treatment and are able to get back to their usual activities.
Legg-Calve-Perthes disease complications
Children who have had Legg-Calve-Perthes disease are at higher risk of developing hip arthritis in adulthood — particularly if the hip joint heals in an abnormal shape. If the hip bones don’t fit together well after healing, this can cause the joint to wear out early. Hip replacement surgery eventually may be required.
In general, children who are diagnosed with Legg-Calve-Perthes after age 6 are more likely to develop hip problems later in life. The younger the child is, the better the chances for the hip joint healing in a normal, round shape.
Perthes disease causes
The changes of Perthes disease occur because the head of the femur has its blood supply temporarily cut off. This results in the death of part or all of the bony center of the head but the smooth cartilage (‘gristle’) covering it survives, as it is fed by the joint fluid.
The cause of the interruption of blood supply is not known. The condition develops between the ages of about three and eleven years in one hip, when the stage of development of the head of the femur makes it more prone to interruption. In some cases, it affects both hips, and it sometimes runs in families. Perthes disease occurs much more commonly in boys than girls. Minor injuries may play a part. In most instances, infection (‘germs’) has nothing to do with the condition.
When the process develops, at first there is often pain (in hip or thigh) and some muscle spasm associated with limping. This stage of ‘irritability’ does not last more than a few weeks, and at no stage is there any upset to the child’s general health.
The dead portions of bone look whiter on x-rays. Over a period of time (measured in months), this dead bone is gradually and irregularly absorbed by the body, giving rise to the fragmented or broken-up appearance in the x-ray. Slowly, dead bone is replaced by new, living bone which looks of normal density in the x-ray.
While all this process is going on, the head of the femur, made up of both bone and cartilage, is relatively softened, and it may be ‘squashed’ out of its normal smoothly-rounded shape, especially if it has to try to support the whole weight of the body – as it normally does with each step taken. Once the head is squashed it does not return to its normal shape, but the new bone grows into a deformed shape which would then remain for the rest of the child’s life and may be a cause of disability in the hip.
The other hip may become affected in about one case in eight either at the same time or later and go through the same series of changes.
Risk factors for Legg-Calve-Perthes disease
Risk factors for Legg-Calve-Perthes disease include:
- Age. Although Legg-Calve-Perthes disease can affect children of nearly any age, it most commonly occurs between ages 4 and 8.
- Your child’s sex. Legg-Calve-Perthes is up to five times more common in boys than in girls.
- Race. White children are more likely to develop the disorder than are black children.
- Family history. In a small number of cases, Legg-Calve-Perthes appears to run in families.
Perthes disease symptoms
One of the earliest signs of Perthes is a change in the way your child walks and runs. This is often most apparent during sports activities. Your child may limp, have limited motion, or develop a peculiar running style.
Symptoms of Perthes disease include:
- pain in the hip, knee or groin when putting weight on the affected leg or moving the hip joint
- a slight limp in the earlier stages that becomes worse over time
- limited movement
- stiffness and reduced range of movement in the hip joint
- the affected leg may become shorter leading to uneven leg length
- thinner thigh muscles on the affected leg
- worsening pain and limping as time goes by.
Depending upon your child’s activity level, symptoms may come and go over a period of weeks or even months before a doctor visit is considered.
Perthes disease diagnosis
Your doctor will do a number of examinations and tests to work out what’s causing your child’s symptoms.
These will include:
- medical history – to get a better understanding of the situation your doctor will ask you when you first noticed the symptoms, what makes the symptoms worse, what makes them better, if there are any other health issues
- your doctor will also conduct a physical exam, which will involve moving your child’s legs through their range of movement. This will help identify any positions that cause pain or stiffness.
If your child has pain in the hip, your doctor may suggest an x-ray to diagnose Perthes disease. If the x-ray doesn’t provide an answer, other more sensitive tests can include:
- Magnetic resonance imaging (MRI). This technology uses radio waves and a strong magnetic field to produce very detailed images of bone and soft tissue inside the body. MRIs often can visualize bone damage caused by Legg-Calve-Perthes disease more clearly than X-rays can.
- X-rays. Initial X-rays may look normal because it can take one to two months after symptoms begin for the damage associated with Legg-Calve-Perthes disease to become evident on X-rays. Your doctor will likely recommend several X-rays over time, to track the progression of the disease.
- Bone scan. In this test, a small amount of radioactive material is injected into a vein. The material is attracted to areas where bone is rapidly breaking down and rebuilding itself, so these areas show up on the resulting scan images.
These will give your doctor a picture of what’s happening inside your child’s joints.
A child with Perthes can expect to have several x-rays taken over the course of treatment, which may be 2 years or longer. As the condition progresses, x-rays often look worse before gradual improvement is seen.
Perthes disease treatment
In most cases, the blood supply to the hip joint returns and the femoral head regenerates by itself. This can take anywhere between two and five years. During this critical period, the bone is soft and vulnerable to damage.
Because of uncertainty as to the exact cause of the disease, there are differences of opinion among doctors as to various details of treatment. However, with few exceptions, there is agreement as to the general principles of treatment.
Treatment of Perthes’ disease aims to make sure the femoral head remains as round as possible, and to reduce joint pain and stiffness.
Treatment depends on your child’s age and the severity of their condition, but may include:
- The hip joint should be rested from movement during the phase when it is painful and irritable.
- The more the head of the femur is ‘contained’ within its socket, the less the risk of deformity or of squashing as the socket tends to ‘mold’ the head.
In the first instance, your child may need to be admitted to hospital, to make sure the diagnosis and to rest the hip while it is painful. The range of movement of the hip is checked until full movement is possible. A period in springs and slings or traction may be necessary and analgesia is given for pain.
The bone will repair itself, as long as it is not too damaged. This takes time, usually between 1 and 5 years.
Your child may then be fitted with a brace (splint) or ‘broomstick plaster’ to contain the femur head in the hip socket. In either case, your child will be given crutches and encouraged to weight-bear. Some children do not require a brace.
The aim of treatment is to avoid making it worse. This might include:
- Avoiding activities with a high impact on the hip, such as running and jumping
- Rest and use of a wheelchair or crutches may be required when the pain is especially bad
- Your doctor may advise rest using crutches or a wheelchair for a period of time up to one year
- A splint, brace or a plaster may be used if your child’s range of movement in the hip is affected, or if x-rays show that the femoral head is losing its rounded shape
- Pain medication
- Special exercises – swimming and exercising in water
- Physiotherapy to help keep the hip joint moving and to help maintain muscle strength
- Regular monitoring by your doctor, including physical examinations and x-rays
- Some children require surgery to treat the deformed femoral head and fit it snugly within the hip socket
From time to time your child will be reviewed by a specialist, often with further x-rays being taken to assess progress.
In some cases progress may not be satisfactory, and occasionally it is necessary in a few children to need surgery to improve the ‘containment’ of the head, e.g. by turning the socket down over it.
Legg-Calve-Perthes disease treatment
If your child is younger than 6 or 7, your doctor may just recommend observation and symptomatic treatment with stretching, limited running and jumping, and medications as needed.
Observation. For very young children (those 2 to 6 years old) who show few changes in the femoral head on their initial x-rays, the recommended treatment is usually simple observation. Your doctor will regularly monitor your child using x-rays to make sure the regrowth of the femoral head is on track as the disease runs its course.
Anti-inflammatory medications. Painful symptoms are caused by inflammation of the hip joint. Anti-inflammatory medicines, such as ibuprofen, are used to reduce inflammation, and your doctor may recommend them for several months. As your child progresses through the disease stages, your doctor will adjust or discontinue dosages.
Physical therapy exercises. Hip stiffness is common in children with Perthes disease and physical therapy exercises are recommended to help restore hip joint range of motion. These exercises often focus on hip abduction and internal rotation. Parents or other caregivers are often needed to help the child complete the exercises.
- Hip abduction. The child lies on his or her back, keeping knees bent and feet flat. He or she will push the knees out and then squeeze the knees together. Parents should place their hands on the child’s knees to assist with reaching a greater range of motion.
- Hip rotation. With the child on his or her back and legs extended out straight, parents should roll the entire leg inward and outward.
Casting and bracing. If range of motion becomes limited or if x-rays or other image scans indicate that a deformity is developing, a cast or brace may be used to keep the head of the femur in its normal position within the acetabulum.
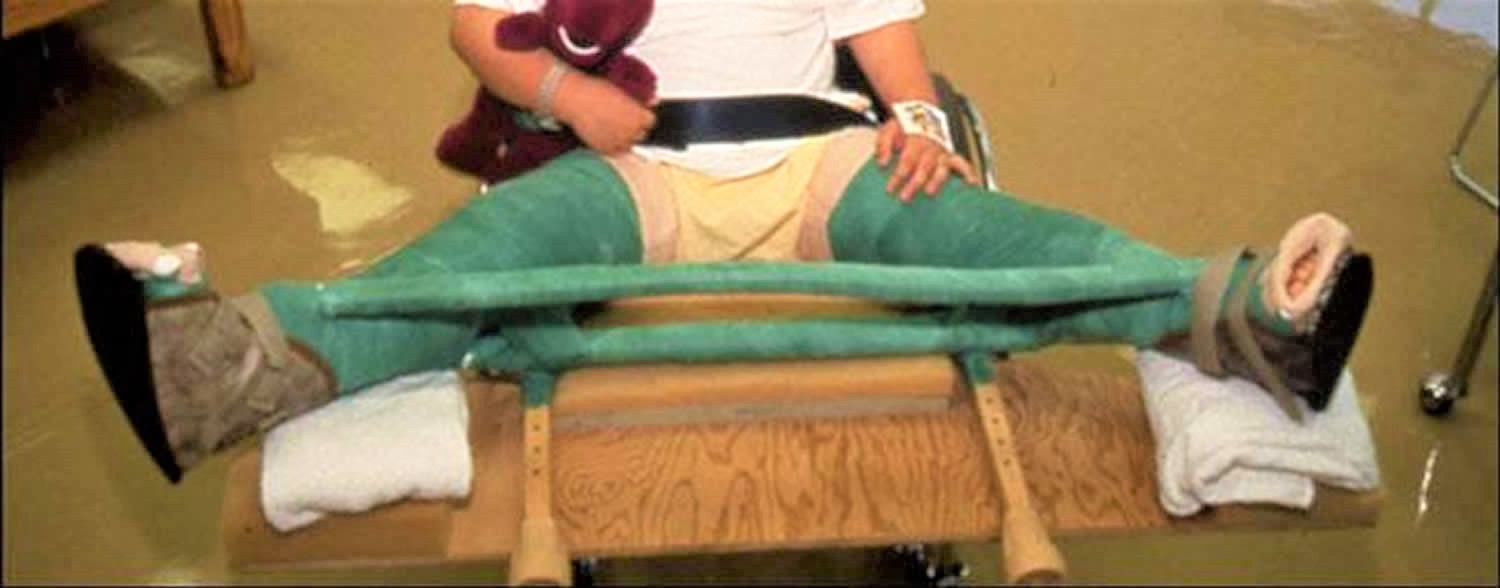
To keep the femoral head deep within its socket, your doctor may recommend a special type of leg cast that keeps both legs spread widely apart for four to six weeks. After this a night-time brace is sometimes used to maintain hip flexibility.
Petrie casts are two long-leg casts with a bar that hold the legs spread apart in a position similar to the letter “A.” Your doctor will most likely apply the initial Petrie cast in an operating room in order to have access to specific equipment.
- Arthrogram. During the procedure, your doctor will take a series of special x-ray images called arthrograms to see the degree of deformity of the femoral head and to make sure he or she positions the head accurately. In an arthrogram, a small amount of dye is injected into the hip joint to make the anatomy even easier to see.
- Tenotomy. In some cases, the adductor longus muscle in the groin is very tight and prevents the hip from rotating into the proper position. Your doctor will perform a minor procedure to release this tightness — called a tenotomy — before applying the Petrie casts. During this quick procedure, your doctor uses a thin instrument to make a small incision in the muscle.
Figure 4. Petrie cast – keep the legs spread far apart in an effort to maintain the hips in the best position for healing.
After the cast is removed, usually after 4 to 6 weeks, physical therapy exercises are resumed. Your doctor may recommend continued intermittent casting until the hip enters the final stage of the healing process.
Other nonsurgical treatments include:
- Crutches. In some cases, your child may need to avoid bearing weight on the affected hip. Using crutches can help protect the joint.
- Traction. If your child is in severe pain, a period of bed rest and traction may help. Traction involves a steady and gentle pulling force on your child’s leg.
How do you care for your child at home in a splint?
You will be shown how to fit the splint. It then becomes your responsibility to see that the splint is properly used at all times.
The splint may be removed for a daily bath or shower, but must be promptly re-applied. It is worn in bed at night. Please tell your doctor or physiotherapist if there is any discomfort or difficulty in managing the brace.
Can my child go to school?
Once your child is managing well in the splint he/she can and should, attend normal school. He/she may need special transport and may only be able to attend part time at first.
Legg-Calve-Perthes disease surgery
Most of the orthopedic treatments for Legg-Calve-Perthes disease are aimed at improving the shape of the hip joint to prevent arthritis later in life.
- Contracture release. Children who have Legg-Calve-Perthes often prefer to hold their leg across the body. This tends to shorten nearby muscles and tendons, which may cause the hip to pull inward (contracture). Surgery to lengthen these tissues may help restore the hip’s flexibility.
- Joint realignment. For children older than 6 to 8, realignment of the joint has been shown to restore a more normal shape to the hip joint. This involves making surgical cuts in the femur or pelvis to realign the joints. The bones are held in place with a plate while the bone heals.
- Removal of excess bone or loose bodies. In older children with painful, restricted motion, trimming extra bone around the femoral head or repairing damaged cartilage may ease motion and relieve pain. Loose bits of bone or torn flaps of cartilage can be removed.
- Joint replacement. Children who have had Legg-Calve-Perthes sometimes require hip replacement surgery later in life. These surgeries can be complicated because of a higher risk of bone fracture and nerve damage.
Figure 5. An osteotomy of the femur places the femoral head in a better position to heal.

Your doctor may recommend surgery to re-establish the proper alignment of the bones of the hip and to keep the head of the femur deep within the acetabulum until healing is complete. Surgery is most often recommended when:
- Your child is older than age 8 at the time of diagnosis. Because the potential for deformity during the reossification stage is greater in older children, preventing damage to femoral head is even more critical.
- More than 50% of the femoral head is damaged. Keeping the femoral head within the rounded acetabulum may help the bone grow into a functional shape.
- Nonsurgical treatment has not kept the hip in correct position for healing.
The most common surgical procedure for treating Perthes disease is an osteotomy. In this type of procedure, the bone is cut and repositioned to keep the femoral head snug within the acetabulum. This alignment is kept in place with screws and plates, which will be removed after the healed stage of the disease.
In many cases, the femur bone is cut to realign the joint. Sometimes, the socket must also be made deeper because the head of the femur has actually enlarged during the healing process and no longer fits snugly within it. After either procedure, the child is usually placed in a cast for 6 to 8 weeks to protect the alignment.
After the cast is removed, physical therapy will be needed to restore muscle strength and range of motion. Crutches or a walker will be necessary to reduce weight bearing on the affected hip. Your doctor will continue to monitor the hip with x-rays through the final stages of healing.
Post surgical outcomes
In most cases, the long-term prognosis for children with Perthes is good and they grow into adulthood without further hip problems.
If there is deformity in the shape of the femoral head, there is more potential for future problems; however, if the deformed head still fits into the acetabulum, problems may be avoided. In cases where the deformed head does not fit well into the acetabulum, hip pain or early onset of arthritis is likely in adulthood.





{kind=link}