
Contents
- Premenstrual Dysphoric Disorder
- What is menstrual cycle?
- How long is a typical menstrual cycle?
- What is ovulation?
- How can I keep track of my menstrual cycle?
- Why should I keep track of my menstrual cycle?
- Who gets premenstrual dysphoric disorder?
- Is premenstrual dysphoric disorder considered a mental illness?
- Is premenstrual dysphoric disorder a form of bipolar disorder?
- Can I prevent premenstrual dysphoric disorder?
- Can you cure premenstrual dysphoric disorder naturally?
- PMDD vs PMS
- Premenstrual Dysphoric Disorder causes
- Premenstrual Dysphoric Disorder signs and symptoms
- Premenstrual Dysphoric Disorder Complications
- Premenstrual Dysphoric Disorder Diagnosis
- Premenstrual Dysphoric Disorder Differential Diagnosis
- Premenstrual Dysphoric Disorder treatment
- Premenstrual Dysphoric Disorder prognosis
Premenstrual Dysphoric Disorder
Premenstrual Dysphoric Disorder also called “PMDD” or PMS depression is a more severe form of premenstrual syndrome (PMS) characterized by extreme mood swings, anxiety, irritability, and depression, occurring in the week or two before your period starts (the luteal phase), most commonly in the days preceding menstruation 1, 2, 3, 4. And your symptoms usually go away two to three days after your period starts. Premenstrual Dysphoric Disorder (PMDD) is considered a mood disorder affecting young adult women that causes significant emotional, psychological, and physical symptoms, with significant distress or impairment in menstruating women during the the second half of a menstrual cycle occurring after ovulation and before the next period of your menstrual cycle. Premenstrual Dysphoric Disorder (PMDD) symptoms include mood swings, irritability, depression and fatigue are usually so severe that the young or adult woman misses school, work and/or avoids her regular social activities.
Symptoms of premenstrual dysphoric disorder (PMDD) include 5:
- Lasting irritability or anger that may affect other people
- Feelings of sadness or despair, or even thoughts of suicide
- Feelings of tension or anxiety
- Panic attacks
- Mood swings
- Sadness and crying often
- Lack of interest in daily activities and relationships
- Trouble thinking or focusing
- Tiredness or low energy
- Fatigue
- Food cravings or binge eating
- Trouble sleeping
- Feeling out of control
- Problems paying attention and concentrating
- Physical symptoms, such as cramps, bloating, breast tenderness, headaches, and joint or muscle pain
It is largely the emotional symptoms that are more severe when you have PMDD. You may have more severe depression symptoms, irritability, and tension 6. Premenstrual Dysphoric Disorder (PMDD) is diagnosed when women have 5 or more of the most common premenstrual syndrome (PMS) symptoms during the second half of her menstrual cycle for at least 2 menstrual cycles in a row, and symptoms are not due to a medical condition such as thyroid disease. According to the American Psychological Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5), Premenstrual Dysphoric Disorder (PMDD) is recognized as a mental health condition 5.
To help diagnose PMDD, your doctor may ask you to chart your symptoms (see sample chart in Figure 2 below).
Premenstrual Dysphoric Disorder (PMDD) affects up to 5% of women of childbearing age 7. If you suspect you have Premenstrual Dysphoric Disorder (PMDD), it’s important to talk to your doctor. A thorough medical evaluation may determine if your symptoms are due to premenstrual dysphoric disorder or some other condition. If you’re diagnosed with premenstrual dysphoric disorder (PMDD), your doctor can recommend specific treatments to help minimize your symptoms. Premenstrual Dysphoric Disorder (PMDD) treatment options may include dietary and lifestyle changes, medications such as antidepressants or birth control pills or other therapies.
Treatments for PMDD include:
- Diet and lifestyle changes. Regular exercise often reduces premenstrual symptoms. Cutting back on caffeine, avoiding alcohol and stopping smoking may ease symptoms, too. Getting enough sleep and using relaxation techniques, such as mindfulness, meditation and yoga, also may help. Avoid stressful and emotional triggers, such as arguments over financial issues or relationship problems, whenever possible.
- Nutritional supplements. Consuming 1,200 milligrams of calcium daily may possibly reduce symptoms of PMS and PMDD. Vitamin B6 (pyridoxine), magnesium and L-tryptophan also may help, but talk with your doctor for advice before taking any supplements.
- Herbal remedies. Some research suggests that chasteberry (Vitex agnus-castus) may possibly reduce irritability, mood swings, breast tenderness, swelling, cramps and food cravings associated with PMDD, but more research is needed. The U.S. Food and Drug Administration doesn’t regulate herbal supplements, so talk with your doctor before trying one.
- Antidepressants called selective serotonin reuptake inhibitors (SSRIs). SSRIs change serotonin levels in your brain. The Food and Drug Administration (FDA) approved three SSRIs to treat PMDD:
- Sertraline
- Fluoxetine
- Paroxetine
- Birth control pills. The FDA has approved a birth control pill containing drospirenone and ethinyl estradiol, to treat PMDD.
- Over-the-counter pain relievers may help relieve physical symptoms, such as cramps, joint pain, headaches, backaches, and breast tenderness. These include:
- Ibuprofen
- Naproxen
- Aspirin
- Stress management, such as relaxation techniques and spending time on activities you enjoy 8
Making healthy changes, such as eating a healthy combination of foods across the food groups, cutting back on salty and sugary foods, and getting more physical activity, may also help relieve some PMDD symptoms. But PMDD can be serious enough that some women should go to a doctor to discuss treatment options. According to a meta-analysis, women with PMDD have a fourfold higher risk of suicidal thoughts and a sevenfold higher risk of suicidal attempts 9. And, if you are thinking of hurting yourself or others, call your local emergency services number right away.
What is menstrual cycle?
Your menstrual cycle is the monthly hormonal cycle a female’s body goes through to prepare for pregnancy. Your menstrual cycle is counted from the first day of your period up to the first day of your next period. Your hormone levels (estrogen and progesterone) usually change throughout the menstrual cycle and can cause menstrual symptoms.
During your monthly menstrual cycle, your uterus lining builds up to prepare for pregnancy. If you do not get pregnant, estrogen and progesterone hormone levels begin falling. Very low levels of estrogen and progesterone tell your body to begin menstruation.
Periods usually start between age 11 and 14 (a girl’s first period is called menarche) and continue until menopause at about age 51 10. In the United States, most girls start menstruating shortly after 12 years of age 11. The average menstruation time in normally menstruating women is 3 to 5 days 12 but a normal menstrual period can lasts up to 8 days 13. Besides bleeding from the vagina, you may have:
- Abdominal or pelvic cramping pain
- Lower back pain
- Bloating and sore breasts
- Food cravings
- Mood swings and irritability
- Headache and fatigue.
Regular menstrual periods in the years between puberty and menopause are usually a sign that your body is working normally. Irregular or heavy, painful periods are not normal. Many women also get premenstrual syndrome (PMS) symptoms.
Figure 1. Ovarian activity during the Menstrual cycle
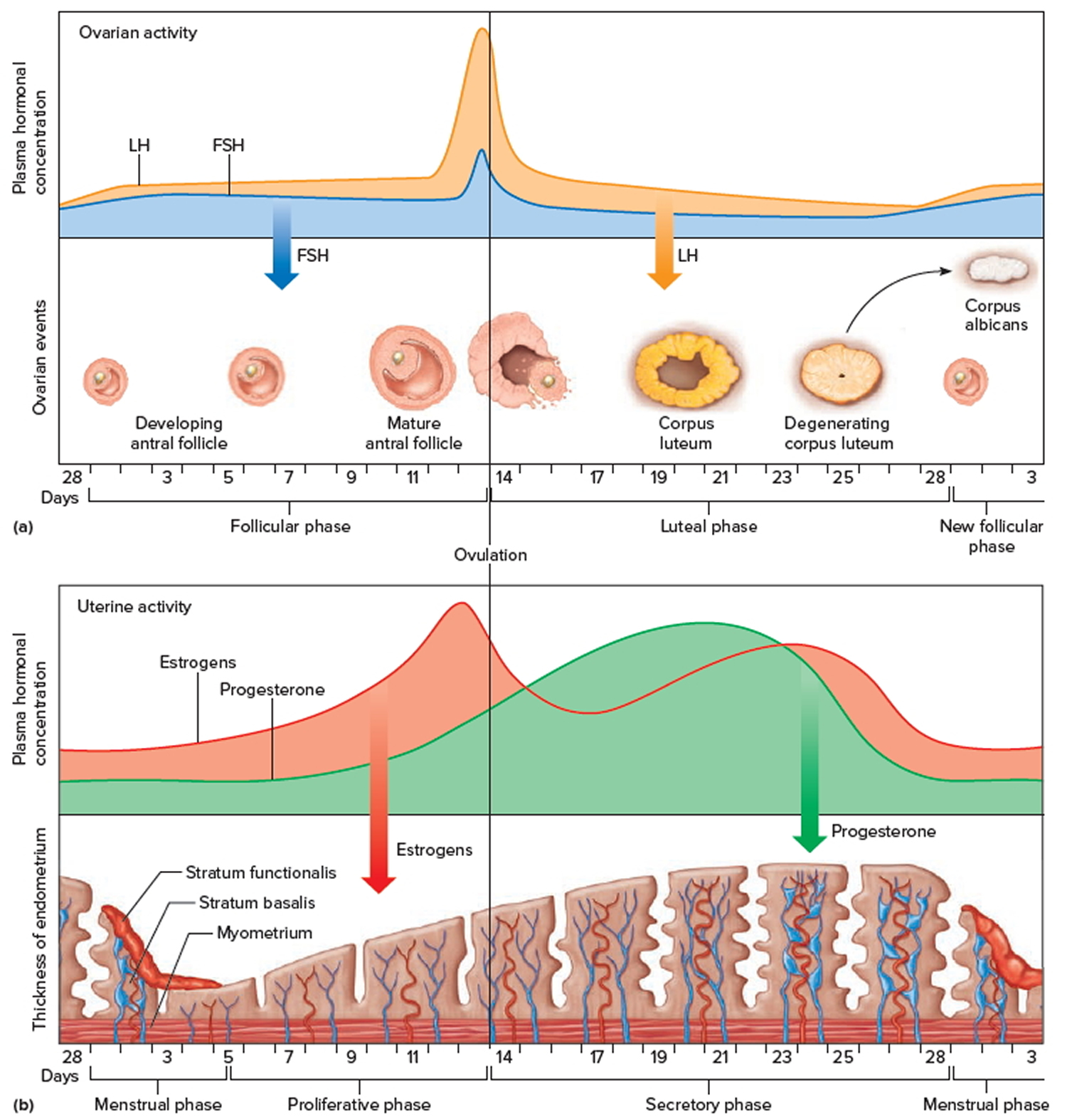
Footnotes: Major events in the female menstrual cycle. (a) Plasma hormonal concentrations of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) affect follicle maturation in the ovaries. (b) Plasma hormonal concentrations of estrogen and progesterone influence changes in the uterine lining.
How long is a typical menstrual cycle?
The typical menstrual cycle is 28 days long, but each woman is different 14. Also, a woman’s menstrual cycle length might be different from month-to-month. Your periods are still “regular” if they usually come every 24 to 38 days 15. This means that the time from the first day of your last period up to the start of your next period is at least 24 days but not more than 38 days.
Some women’s periods are so regular that they can predict the day and time that their periods will start. Other women are regular but can only predict the start of their period within a few days.
What is ovulation?
Ovulation is when the ovary releases an egg so it can be fertilized by a sperm in order to make a baby. A woman is most likely to get pregnant if she has sex without birth control in the three days before and up to the day of ovulation (since the sperm are already in place and ready to fertilize the egg as soon as it is released). A man’s sperm can live for 3 to 5 days in a woman’s reproductive organs, but a woman’s egg lives for just 12 to 24 hours after ovulation.
Each woman’s cycle length may be different, and the time between ovulation and when the next period starts can be anywhere from one week (7 days) to more than 2 weeks (19 days) 16.
At different times in a woman’s life, ovulation may or may not happen:
- Women who are pregnant do not ovulate.
- Women who are breastfeeding may or may not ovulate. Women who are breastfeeding should talk to their doctor about birth control methods if they do not want to get pregnant.
- During perimenopause, the transition to menopause, you may not ovulate every month.
- After menopause you do not ovulate.
How can I keep track of my menstrual cycle?
You can keep track of your menstrual cycle by marking the day you start your period on a calendar. After a few months, you can begin to see if your periods are regular or if your cycles are different each month.
You may want to track:
- Premenstrual syndrome (PMS) symptoms: Did you have cramping, headaches, moodiness, forgetfulness, bloating, or breast tenderness?
- When your bleeding begins: Was it earlier or later than expected?
- How heavy the bleeding was on your heaviest days: Was the bleeding heavier or lighter than usual? How many pads or tampons did you use?
- Period symptoms: Did you have pain or bleeding on any days that caused you to miss work or school?
- How many days your period lasted: Was your period shorter or longer than the month before?
You can also download apps (sometimes for free) for your phone to track your periods. Some include features to track your PMS symptoms, energy and activity levels, and more.
Why should I keep track of my menstrual cycle?
If your periods are regular, tracking them will help you know when you ovulate, when you are most likely to get pregnant, and when to expect your next period to start.
If your periods are not regular, tracking them can help you share any problems with your doctor.
If you have period pain or bleeding that causes you to miss school or work, tracking these period symptoms will help you and your doctor or nurse find treatments that work for you. Severe pain or bleeding that causes you to miss regular activities is not normal and can be treated.
Who gets premenstrual dysphoric disorder?
Premenstrual Dysphoric Disorder (PMDD) affects up to 5% of women of childbearing age 7. Many women with PMDD may also have anxiety or depression 17.
Is premenstrual dysphoric disorder considered a mental illness?
Premenstrual dysphoric disorder (PMDD) is a mental health condition listed in the DSM-5 as a “depressive disorder” 5. The DSM-5 stands for Diagnostic and Statistical Manual of Mental Disorders and is a criteria for diagnosing mental health conditions.
Is premenstrual dysphoric disorder a form of bipolar disorder?
No. Premenstrual dysphoric disorder (PMDD) and bipolar disorder aren’t the same condition. They do, however, have similar symptoms. During a depressive episode in bipolar disorder, you may feel irritable or like you’re losing control. You may also have suicidal thoughts. It’s important to get support and seek help if you have symptoms of either condition.
Can I prevent premenstrual dysphoric disorder?
Treating existing depression or anxiety may make it less likely that PMS could become premenstrual dysphoric disorder (PMDD). But PMDD could be related to the way your hormones work, and you might not be able to prevent it. In that case, treatment can bring relief.
Many women with premenstrual dysphoric disorder (PMDD) have:
- Anxiety
- Severe depression
- Seasonal affective disorder (SAD)
Other factors that may play a role include:
- Alcohol or substance abuse
- Cigarette smoking
- Thyroid disorders
- Being overweight
- Having a mother with a history of the disorder
- Lack of exercise
- Family history of PMS or PMDD
- Personal or family history of depression, postpartum depression, or other mood disorders
- Less access to education about the management and treatment of PMDD.
Can you cure premenstrual dysphoric disorder naturally?
There are some ways to manage symptoms of premenstrual dysphoric disorder (PMDD) that don’t involve medication. For example, you can practice yoga, try meditation or find other ways to improve your mood. Regular exercise often reduces premenstrual symptoms. Cutting back on caffeine, avoiding alcohol and stopping smoking may ease symptoms, too. Getting enough sleep and changing certain aspects of your diet may also bring relief. Avoid stressful and emotional triggers, such as arguments over financial issues or relationship problems, whenever possible. Additionally, support groups or resources may help you.
PMDD vs PMS
Premenstrual dysphoric disorder (PMDD) can be considered a severe form of premenstrual syndrome (PMS) 1, 18, 19. While both PMDD (Premenstrual Dysphoric Disorder) and PMS (Premenstrual Syndrome) involve physical and emotional symptoms that occur in the second half of a woman’s menstrual cycle, about 10-14 days before your period, PMS involves milder physical and emotional symptoms and PMDD is a more severe and disabling form of PMS, characterized by intense mood swings and emotional distress such as extreme depression, irritability, and anxiety that can be disabling significantly impacting your daily life. You may feel they are uncontrollable.
PMS (Premenstrual Syndrome)
PMS symptoms are different for every woman. You may get physical symptoms, such as bloating or gassiness, or emotional symptoms, such as sadness, or both. Your symptoms may also change throughout your life.
Physical symptoms of PMS can include 1:
- Swollen or tender breasts
- Constipation or diarrhea
- Bloating or a gassy feeling
- Cramping
- Headache or backache
- Clumsiness
- Lower tolerance for noise or light
Emotional or mental symptoms of PMS include 1:
- Irritability or hostile behavior
- Feeling tired
- Sleep problems (sleeping too much or too little)
- Appetite changes or food cravings
- Trouble with concentration or memory
- Tension or anxiety
- Depression, feelings of sadness, or crying spells
- Mood swings
- Less interest in sex
PMS can be diagnosed if a woman reports at least one of the following emotional or mental and physical symptoms during the 5 days before her periods in each of the previous 3 menstrual cycles 22:
- Emotional or mental symptoms:
- Angry outbursts
- Anxiety
- Confusion
- Depression
- Irritability
- Social withdrawal
- Physical symptoms:
- Abdominal bloating
- Breast tenderness or swelling
- Headache
- Joint or muscle pain
- Swelling of arms and legs
- Weight gain
- These symptoms must be relieved within 4 days of the onset of menses, without recurrence until at least day 13 of the cycle and must be present in the absence of any drug therapy, hormone ingestion, drug or alcohol use 22. The symptoms must occur reproducibly during 2 cycles of prospective recording. The woman must exhibit identifiable dysfunction in social, academic, or work performance 22.
In a study of 2,800 French women, about 12% met the diagnostic criteria for PMS, and 4% reported severe symptoms 7. The prevalence of PMS is not associated with age, educational achievement, or employment status 7. Symptom persistence and severity tend to fluctuate. One study found that only 36% of women who were diagnosed with PMS continued to meet the diagnostic criteria one year later 7. Women who gained weight or had a stressful event in the past year are more likely to be diagnosed with PMS 7.
PMDD (Premenstrual Dysphoric Disorder)
PMDD (Premenstrual Dysphoric Disorder) is characterized by more severe and debilitating symptoms than PMS, including intense mood swings, extreme irritability or anger, feelings of hopelessness or depression, and anxiety. PMDD symptoms are so severe that they can interfere with your daily functioning, work, relationships, and overall quality of life. PMDD requires more comprehensive treatment, which may include lifestyle changes, medication, or other therapies. Furthermore, PMDD only affects a smaller percentage of women, estimated to be between 1.3% and 8% of young adult women 23
Premenstrual Dysphoric Disorder causes
The exact cause of premenstrual dysphoric disorder (PMDD) is not known 3, 4. Changes in hormones related to your period may cause premenstrual dysphoric disorder. Several studies suggest that cyclical changes in estrogen and progesterone levels trigger the symptoms 24, 25, 26. However, premenstrual dysphoric disorder (PMDD) does not appear to be caused simply by an imbalance of female ovarian hormones. Research measuring estrogen and progesterone levels across the menstrual cycle found no difference between women with premenstrual dysphoric disorder (PMDD) and those without the disorder. On the other hand, hormones must play some role because premenstrual dysphoric disorder symptoms disappear if the ovaries are removed or not functioning (e.g. menopause). Recent evidence from research studies suggests that estrogen and progesterone hormone release patterns are normal in women with PMS or PMDD, but they have a heightened sensitivity to cyclical variations in levels of estrogen and progesterone hormones, which predisposes them to experience mood, behavioral, and somatic symptoms 26.
Postmenopausal women who had previously been diagnosed with PMS had recurrent psychiatric and physical symptoms when they received cyclical progestogen therapy 24. Furthermore, the suppression of estrogen with gonadotropin-releasing hormone (GnRH) analogues has been shown to significantly improve PMS symptoms 25.
Current theories suggest that normal ovarian function may trigger changes in brain chemistry in women predisposed to premenstrual dysphoric disorder (PMDD). One brain chemical that may be especially important is serotonin, a neurotransmitter. The serotonin system has a close relationship to the female hormones, and imbalances of the serotonin system may play an important role in causing premenstrual dysphoric disorder. Another tie-in is that medications most effective for treating premenstrual dysphoric disorder are those with specific effects on serotonin.
Changes in mood may be attributable to the effect estrogen and progesterone have on the serotonin, gamma-aminobutyric acid (GABA), and dopamine systems 26. These can also alter the renin-angiotensin-aldosterone system (RAAS), which could explain some of the bloating and swelling that occur during the luteal phase 26. Sex hormone levels alone cannot fully explain premenstrual disorders. Studies show that women diagnosed with a premenstrual disorder do not have higher levels of estrogen or progesterone than the general population, and accepted explanations as to why some women could be more sensitive to fluctuations in these sex hormones are lacking 7.
Premenstrual dysphoric disorder may also be inherited. Studies have shown that identical twins are more likely to share the disorder (93%) than non-identical twins (44%), and daughters of mothers with premenstrual dysphoric disorder are more likely to have it themselves. However, no specific genes have been identified to account for premenstrual dysphoric disorder 27. Therefore there may be a genetic predisposition to developing the disorder.
Psychological, social and cultural factors also may be involved in causing premenstrual dysphoric disorder or at least in the expression of premenstrual dysphoric disorder symptoms. Stressful life events and a family history of PMS or premenstrual dysphoric disorder may increase your chances of getting premenstrual dysphoric disorder. Major depression is common in women who have premenstrual dysphoric disorder. However, not all women who have premenstrual dysphoric disorder have major depression. Moreover, these factors alone are inadequate to explain the disorder, which almost certainly has a biological basis.
Risk factors for premenstrual dysphoric disorder
Proven Risk Factors
- Past traumatic events: Traumatic events and preexisting anxiety disorders are risk factors for the development of premenstrual dysphoric disorder (PMDD). The underlying mechanisms are unknown, making further investigation necessary 28.
- Cigarette smoking: There is a strong association of moderate-to-severe forms of PMS with current smoking status compared to non-smokers. The risk is elevated even for former smokers and the risk of incident PMS tends to increase with the quantity of cigarette smoking. Furthermore, the risk of premenstrual dysphoric disorder (PMDD) is significantly higher for women who began smoking during adolescence 29
- Obesity: There is a strong linear relationship between body mass index (BMI) at baseline and risk of incident PMS. For each 1 kg/m² increase, there was a significant associated increase (3%). The risk of PMS rose significantly in women with body mass index (BMI) at or higher than 27.5 kg/m² compared with women with a BMI of less than 20 kg/m². Relative risk in women with a BMI of 35.0 kg/m² was 1.66 30. Relative risk (RR) is a ratio of the probability of an event occurring in the exposed group versus the probability of the event occurring in the non-exposed group 31. In this example, in women with a BMI of 35.0 kg/m² a a relative risk of 1.66 means that the risk of an event occurring is 66% higher in the exposed group compared to the unexposed group.
Speculative Risk Factor
- Genetics: Twin studies have implicated heritable factors in the development of PMS (Premenstrual Syndrome) and premenstrual dysphoric disorder (PMDD). Recent studies have provided support for the involvement of the gene that codes for the serotonergic 5HT1A receptor 32 and genetic mutations of the estrogen receptor alpha gene (ESR1) in the development of PMS and PMDD 33.
Premenstrual Dysphoric Disorder signs and symptoms
Premenstrual Dysphoric Disorder (PMDD) symptoms can include:
- Emotional or Mood symptoms
- Severe irritability with frequent conflicts with family members or at work
- Anger
- Anxiety or the feeling of being on edge all the time
- Depression
- Feelings of sadness, hopeless, worthless or despair
- Mood swings, suddenly feeling sad or tearful
- Feeling overwhelmed or out of control
- Crying spells.
- Cognitive symptoms
- Difficulty concentrating
- Lack of interest in normal activities
- Feeling overwhelmed.
- Physical symptoms
- Fatigue
- Changes in appetite or sleep
- Breast swelling or tenderness
- Bloating or weight gain
- Headaches
- Joint pain
- Muscle aches
- Lack of energy
- Fatigability
- Behavioral symptoms
- Social withdrawal
- Changes in libido
- Changes in appetite, either overeating or craving a specific food
- Changes in sleep pattern, either hypersomnia or insomnia
These symptoms typically begin in the week or two before menstruation and usually subside a few days after menstruation begins. The length of time for which the women experience symptoms of Premenstrual Dysphoric Disorder (PMDD) varies from a few days to 2 weeks. For most symptomatic women, symptoms intensify 6 days before and are the most severe 2 days before the menses 34, 35. Of all the symptoms mentioned, anger and irritability are the most distressing and are experienced slightly before the other symptoms 34. Premenstrual Dysphoric Disorder (PMDD) symptoms can be so severe that they can disrupt daily life, impacting relationships, work, and overall well-being.
Premenstrual Dysphoric Disorder Complications
Premenstrual Dysphoric Disorder (PMDD) symptoms may be severe enough to interfere with a woman’s daily life. Women with depression may have worse symptoms during the second half of their cycle and may need changes in their medicine.
Some women with Premenstrual Dysphoric Disorder (PMDD) have suicidal thoughts. Suicide in women with depression is more likely to occur during the second half of their menstrual cycle. If you or someone you know is thinking about suicide call your local emergency services number right away. The Suicide and Crisis Lifeline provides free and confidential support 24/7, anytime day or night.
Premenstrual Dysphoric Disorder (PMDD) may be associated with eating disorders and smoking.
Premenstrual Dysphoric Disorder Diagnosis
Your doctor will talk to you about your health history and do a physical examination. You will need to keep a calendar or diary of your symptoms to help your doctor diagnose PMDD. Your doctor may also want to perform some laboratory tests to exclude the possibility of any illness responsible for causing your symptoms. Illnesses that may cause similar symptoms include anemia, migraines, endometriosis, menopause, and thyroid disease. These tests include a blood test that will be analyzed to see the total number of the different types of cells (full blood count), thyroid function tests, and the level of follicle stimulating hormone (FSH) in the blood.
Premenstrual Dysphoric Disorder DSM-5 Diagnostic Criteria
- Criterion A. In the majority of menstrual cycles, at least five symptoms must be present in the final week before the onset of menses, start to improve within a few days after the onset of
menses, and become minimal or absent in the week postmenses. - Criterion B. One (or more) of the following symptoms must be present:
- Marked affective lability (e.g., mood swings: feeling suddenly sad or tearful, or increased sensitivity to rejection).
- Marked irritability or anger or increased interpersonal conflicts.
- Marked depressed mood, feelings of hopelessness, or self-deprecating thoughts.
- Marked anxiety, tension, and/or feelings of being keyed up or on edge.
- Criterion C. One (or more) of the following symptoms must additionally be present, to reach a total of five symptoms when combined with symptoms from Criterion B above.
- Decreased interest in usual activities (e.g., work, school, friends, hobbies).
- Subjective difficulty in concentration.
- Lethargy, easy fatigability, or marked lack of energy.
- Marked change in appetite; overeating; or specific food cravings.
- Hypersomnia or insomnia.
- A sense of being ovenwhelmed or out of control.
- Physical symptoms such as breast tenderness or swelling, joint or muscle pain, a sensation of “bloating,” or weight gain.
- Note: The symptoms in Criteria A-C must have been met for most menstrual cycles that occurred in the preceding year.
- Criterion D. The symptoms are associated with clinically significant distress or interference with work, school, usual social activities, or relationships with others (e.g., avoidance of social
activities; decreased productivity and efficiency at work, school, or home). - Criterion E. The disturbance is not merely an exacerbation of the symptoms of another disorder, such as major depressive disorder, panic disorder, persistent depressive disorder (dysthymia), or a personality disorder (although it may co-occur with any of these disorders).
- Criterion F. Criterion A should be confirmed by prospective daily ratings during at least two symptomatic cycles. (Note: The diagnosis may be made provisionally prior to this confirmation.)
- Criterion G. The symptoms are not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication, other treatment) or another medical condition (e.g., hyperthyroidism).
Recording Procedures
If symptoms have not been confirmed by prospective daily ratings of at least two symptomatic cycles, “provisional” should be noted after the name of the diagnosis (i.e., “premenstrual dysphoric disorder, provisional”).
Diagnostic Features
The essential features of premenstrual dysphoric disorder (PMDD) are the expression of mood lability, irritability, dysphoria, and anxiety symptoms that occur repeatedly during the premenstrual
phase of the cycle and remit around the onset of menses or shortly thereafter. These symptoms may be accompanied by behavioral and physical symptoms. Symptoms must have occurred in most of the menstrual cycles during the past year and must have an adverse effect on work or social functioning. The intensity and/or expressivity of the accompanying symptoms may be closely related to social and cultural background characteristics of the affected female, family perspectives, and more specific factors such as religious beliefs, social tolerance, and female gender role issues.
Typically, symptoms peak around the time of the onset of menses. Although it is not uncommon for symptoms to linger into the first few days of menses, the individual must have a symptom-free period in the follicular phase after the menstrual period begins. While the core symptoms include mood and anxiety symptoms, behavioral and somatic symptoms commonly also occur. However, the presence of physical and/or behavioral symptoms in the absence of mood and/or anxious symptoms is not sufficient for a diagnosis. Symptoms are of comparable severity (but not duration) to those of another mental disorder, such as a major depressive episode or generalized anxiety disorder. In order to confirm a provisional diagnosis, daily prospective symptom ratings are required for at least two symptomatic cycles.
Associated Features Supporting Diagnosis
Delusions and hallucinations have been described in the late luteal phase of the menstrual cycle but are rare. The premenstrual phase has been considered by some to be a risk period for suicide.
[Source 5 ]Daily Record of Severity of Problems
To help diagnose premenstrual dysphoric disorder (PMDD), your family doctor may ask you to chart your symptoms (see sample chart below). The Daily Record of Severity of Problems for the diagnosis of premenstrual dysphoric disorder (PMDD) is a valid and reliable tool that can be used to diagnose PMS or PMDD 36. It is a daily log of symptoms that correlate with the diagnostic criteria for PMS and PMDD. Patients rate their symptoms through at least two menstrual cycles, which requires a significant investment of time and effort. Administering the Daily Record of Severity of Problems on the first day of menses may be an acceptable way to screen for premenstrual disorders. A cutoff value of 50 provides a positive predictive value of 63.4% and a negative predictive value of 90% 37.
Figure 2. Premenstrual dysphoric disorder (PMDD) Symptoms Chart
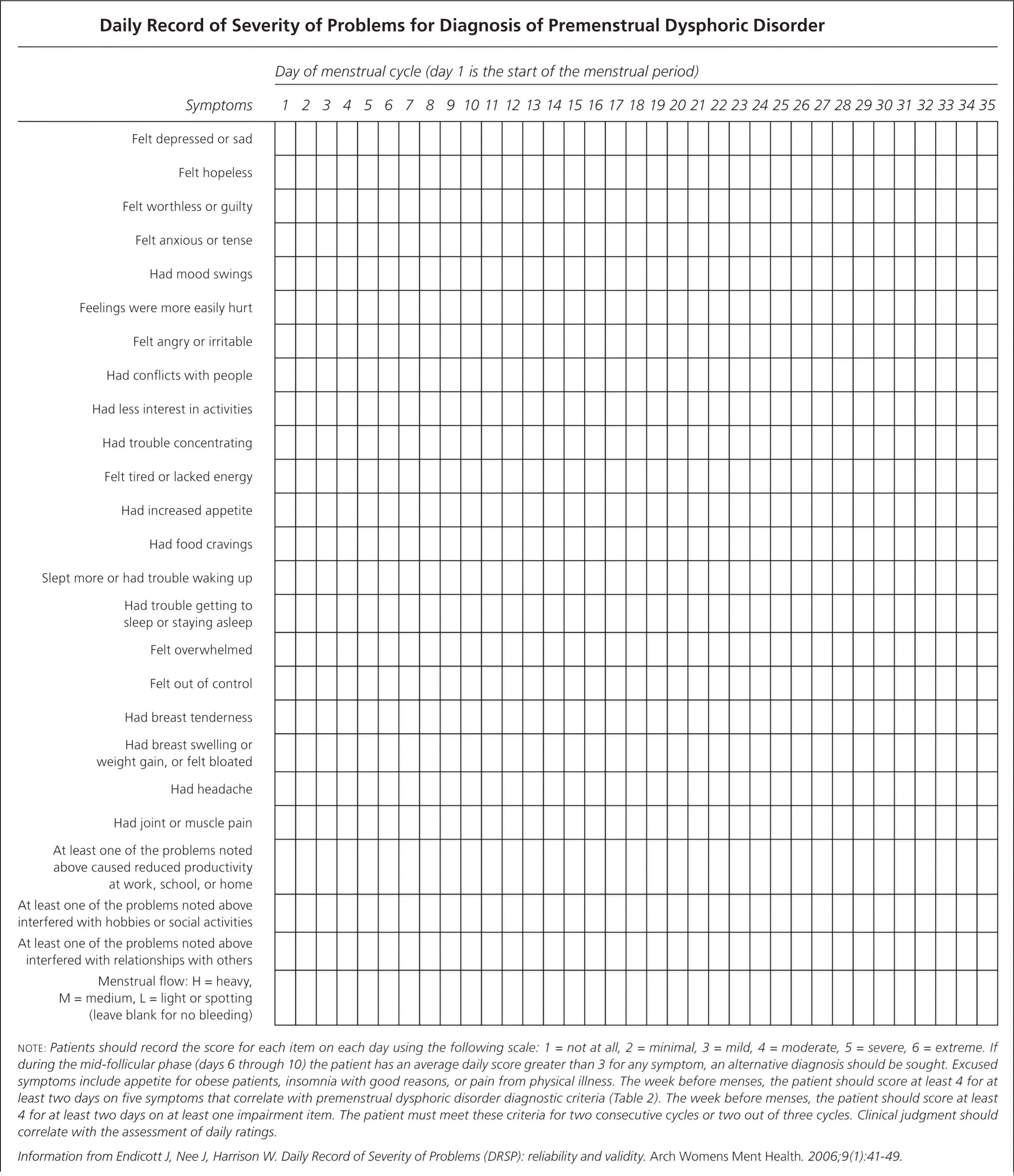
Footnotes: Patients should record the score for each item on each day using the following scale: 1 = not at all, 2 = minimal, 3 = mild, 4 = moderate, 5 = severe, 6 = extreme. If during the mid-follicular phase (days 6 through 10; day 1 is first day of your period) the patient has an average daily score greater than 3 for any symptom, an alternative diagnosis should be sought. Excused symptoms include appetite for obese patients, insomnia with good reasons, or pain from physical illness. The week before menses, the patient should score at least 4 for at least two days on five symptoms that correlate with premenstrual dysphoric disorder diagnostic criteria (DSM-5). The week before menses, the patient should score at least 4 for at least two days on at least one impairment item. The patient must meet these criteria for two consecutive cycles or two out of three cycles. Clinical judgment should correlate with the assessment of daily ratings.
[Source 38 ]Premenstrual Dysphoric Disorder Assessment Scales
- Premenstrual Symptom Screening Tool (PSST): A questionnaire used to diagnose Premenstrual Dysphoric Disorder (PMDD) with 19 items that allow the patient to rate the severity of their symptoms 39.
- Calendar of Premenstrual Experiences (COPE): Includes 22 symptoms grouped into 4 categories: mood reactivity, autonomic/ cognitive, appetitive, and related to fluid retention 40.
- Visual Analogue Scale (VAS): Steiner et al 39 used this scale in 1999 to rate each of the 4 core symptoms of PMDD: mood swings, irritability, tension, and depression. The scale consisted of a 100 mm vertical line labeled 0 or “no symptom” at the left end and 100 or “severe” at the right.
- Daily Record of Severity of Problems (DRSP): This scale consists of 24 items, out of which 21 items are grouped into 11 distinct symptoms and 3 functional impairment items. The items are rated from 1 (not at all) to 6 (extreme).
- Patient Reported Outcomes Measurement Information System (PROMIS): Junghaenel et al 41 used PROMIS computerized adaptive testing (PROMIS CAT) to detect premenstrual symptoms of depression, anxiety, and fatigue; the results of the study provided encouraging evidence for the utility of PROMIS instruments for the measurement of effective premenstrual symptoms.
Premenstrual Dysphoric Disorder Differential Diagnosis
The symptoms of premenstrual dysphoric disorder (PMDD) can overlap with other psychiatric disorders, most importantly major depression, and it is important to rule out another existing disorder before making the diagnosis of PMS or PMDD. The key factor in making the diagnosis of PMS and PMDD is the timing of your symptoms with your menstrual cycle 1. Symptoms must occur during the luteal phase and resolve shortly after the onset of menstruation. Other conditions, such as depression or anxiety, may worsen during the luteal phase, but these can be distinguished from PMS because they persist throughout the menstrual cycle. Migraines, anemia, endometriosis, and hypothyroidism may produce symptoms similar to PMS or PMDD and should also be considered.
Some common premenstrual dysphoric disorder (PMDD) differentials include:
- Major depressive disorder: Depression symptoms include low mood, low energy, anhedonia, appetite change, sleep disturbance, difficulty concentrating, and thoughts of suicide. Roughly half the cases of PMS/Premenstrual Dysphoric Disorder (PMDD) can have a coexisting diagnosis of depression.[50] A diagnosis of PMS or Premenstrual Dysphoric Disorder (PMDD) may predate a diagnosis of depression or depression and Premenstrual Dysphoric Disorder (PMDD) may coexist. Criteria for the diagnosis of these disorders are different but not exclusive.
- Thyroid disease (hyperthyroid or hypothyroid):
- Hypothyroid (underactive thyroid) symptoms and signs include weight gain, constipation, cold intolerance, depression, dry skin, and delayed deep tendon reflexes.
- Hyperthyroid (hyperactive thyroid) signs and symptoms include weight loss, poor sleep, heat intolerance, heart rhythm disturbance such as atrial fibrillation, and hyperreflexia.
- Generalized anxiety disorder (GAD): Generalized Anxiety Disorder (GAD) is a mental health condition characterized by persistent and excessive worry and anxiety about everyday events, often interfering with daily life and accompanied by physical symptoms like restlessness or fatigue. Triggers may be identified for anxiety attacks, and the patient shows avoidance of these triggers. Chronic or situational anxiety does not vary with the menstrual cycle. Generalized anxiety disorder and premenstrual dysphoric disorder (PMDD) may coexist. Criteria are different but not exclusive.
- Mastalgia (breast pain): Mastalgia is breast pain. The pain can range from minor discomfort to severely disabling pain in some cases. Many people with breast pain are afraid they may have breast cancer. But breast pain is rarely linked to breast cancer. It should not be considered a possible symptom of breast cancer. There are 2 main types of mastalgia (breast pain):
- Cyclical breast pain. The most common type of breast pain is linked to the menstrual cycle. It is nearly always hormonal. Some people begin to have pain around the time of ovulation. The pain continues until the start of their menstrual cycle. The pain may be barely noticeable. Or it may be so severe that you can’t wear tight-fitting clothing or handle close contact of any kind. The pain may be felt in only one breast. Or it may be felt as a radiating feeling in the underarm area.
- Noncyclic breast pain. The pain may come from the breast. Or it may come from somewhere else, such as nearby muscles or joints, and may be felt in the breast.
Premenstrual Dysphoric Disorder treatment
There are 3 broad approaches to treating premenstrual dysphoric disorder (PMDD). While most experts recommend a combination of all 3, there have been no scientific studies to determine if combination treatment is really the best approach. It is likely that the best approach or combination of approaches will vary from woman to woman based on things like symptom severity and which symptoms are most troublesome.
Here are the 3 approaches with some examples of each:
- Medications – including antidepressants, antianxiety drugs, analgesics, hormones and diuretics.
- Psychobehavioral – including exercise and psychotherapies (cognitive-behavioral therapy, coping skills training, relaxation).
- Nutritional – including diet modification, vitamins, minerals and herbal preparations.
Dietary and Lifestyle Changes
- Lifestyle changes. Regular exercise often reduces premenstrual symptoms. Getting enough sleep and using relaxation techniques, such as mindfulness, meditation and yoga, also may help. Avoid stressful and emotional triggers, such as arguments over financial issues or relationship problems, whenever possible.
- Dietary modifications: Increased intake of complex carbohydrates or proteins (“slow-burning fuels”) is believed to increase tryptophan availability, leading to increased serotonin levels. Cutting back caffeine, avoiding alcohol and stopping smoking may ease symptoms, too.
- Nutritional supplements. Consuming 1,200 milligrams of dietary and supplemental calcium daily may possibly reduce symptoms of PMS and premenstrual dysphoric disorder (PMDD) in some women, however the exact mechanism of action of calcium in PMS or PMDD is unknown 42. Randomized controlled trials have demonstrated the superiority of calcium in improving emotional and physical symptoms over placebo. A randomized controlled trial of 179 Tehran University students who met criteria for PMS without another psychiatric diagnosis found a 50% reduction in depression, appetite, and fatigue in women who received 500 mg of supplemental calcium carbonate twice daily for three months 43. This result was also demonstrated in a U.S. study of more than 400 women who supplemented with 1,200 mg of calcium carbonate daily 42. Vitamin B6 (pyridoxine), vitamin D, magnesium and L-tryptophan also may help. Vitamin D supplementation for treatment of PMS and PMDD symptoms was reviewed in a cross-sectional analysis of a large study 44. The cross-section analyzed was too small to make strong conclusions about the benefit of vitamin D 44. A separate study followed 401 women for 16 years and compared those who developed PMS with those who did not 45. The analysis concluded that low vitamin D levels were not associated with an increased risk of PMS 45. Further studies are needed to support the use of vitamin D as a treatment for symptoms of PMS and PMDD. Vitamin B6 (Pyridoxine) at a dosage of 80 mg per day has also been studied and recommended as treatment for primarily psychological symptoms of PMS, but these studies are small and more data is needed to recommend it as first-line treatment 46. Talk with your doctor for advice before taking any supplements.
- Herbal remedies. Some research suggests that Chaster-berry or Vitex agnus-castus (a herb also known as Chaste Tree and Monk’s Pepper) may possibly reduce irritability, mood swings, breast tenderness, swelling, cramps and food cravings associated with premenstrual dysphoric disorder (PMDD) by exerting some dopaminergic effect, but more research is needed 47, 3. The Food and Drug Administration doesn’t regulate herbal supplements, so talk with your doctor before trying one.
- Stress management: Relaxation/ meditation/ yoga/ breathing techniques.
- Cognitive Behavioral Therapy (CBT). A 2009 meta-analysis analyzed seven trials, three of which were randomized controlled trials, and showed improvement in functioning and depression scores for patients with PMS or PMDD 48. The frequency and duration of cogntive behavioral therapy (CBT) were not defined. However, the results suggest that mindfulness-based exercises and acceptance-based cognitive behavior therapy may be helpful for reducing symptoms. Further studies are needed to support the use of cognitive behavior therapy as first-line therapy.
Medications
Treatment of premenstrual dysphoric disorder is directed at preventing or minimizing symptoms and may include:
- Antidepressants.
- In the United States, selective serotonin reuptake inhibitors (SSRIs) are approved as first-line treatment for severe symptoms of PMS and PMDD. Although SSRIs are considered psychiatric medications, when used to treat premenstrual disorders they improve physical and psychiatric symptoms in most patients 49. Selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac), citalopram (Celexa), escitalopram (Lexapro), paroxetine (Paxil) and sertraline (Zoloft), may reduce symptoms such as emotional symptoms, fatigue, food cravings and sleep problems 49, 50, 51. You can reduce symptoms of premenstrual dysphoric disorder by taking SSRIs all month or only in the interval between ovulation and the start of your period. SSRI treatment probably increases your risk of adverse events, with the most common being nausea, weakness or lack of energy and drowsiness or excessive sleepiness 49.
- Antidepressants that predominantly affect noradrenergic transmission are not as effective for PMDD as SSRIs, which means that the effect of SSRIs in PMDD is not just an antidepressant effect 52, 53. This is supported by the fact that the beneficial effect of SSRIs begins rapidly in PMDD, whereas antidepressant effect takes several weeks. Therefore, clinicians can use SSRIs intermittently from mid-cycle to menses to treat symptoms of PMDD as opposed to continuous treatment 54. Side effects of SSRIs are usually mild. Nausea is the most common adverse effect, but it usually wears off in a couple of days after starting the therapy and doesn’t reappear even if the therapy is intermittent. Reduced libido and difficulty in achieving orgasm (anorgasmia) are other common side effects, but they are absent in drug-free intervals.
- Other antidepressants that are linked with the relief of symptoms include a tricyclic antidepressant (TCA) called Clomipramine 55, 56 and serotonin-norepinephrine reuptake inhibitors (SNRIs) like venlafaxine (Effexor).
- Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) such as venlafaxine (Effexor) have been used off-label to treat PMDD in women with predominantly psychological symptoms 57. The effect is achieved over a relatively short period, three to four weeks, and sustained throughout subsequent menstrual cycles 57.
- Benzodiazepines: Benzodiazepines like alprazolam have been found to be effective only in women with severe anxiety and premenstrual insomnia. However, since there is a risk of dependence, careful monitoring is required, especially in cases with reported prior substance abuse 58, 59.
- Hormonal therapies: For very severe symptoms, your doctor can use hormonal therapies to provide relief. The aim of hormonal therapy is to inhibit the hypothalamic-gonadal cycle; however, this causes medical menopause and leads to hot flashes and an increased risk of osteoporosis. Therefore, to prevent these adverse effects, women are also started back on estrogen and gestagen (a hormone with progesterone-like activity). Some patient reports suggesting recurrence of symptoms with the add-back gestagen (a hormone with progesterone-like activity) therapy. Hence, as an alternative, clinicians can combine gonadotropin hormone-releasing hormone (GnRH) agonist with tibolone (a synthetic steroid with weak estrogenic, progestogenic, and androgenic activity). Guidelines from the International Society of Premenstrual Disorders addressed gonadotropin-releasing hormone (GnRH) agonists as potential treatment of PMS and PMDD by eliminating luteal phase symptoms 60. Although these medications have been used since the 1980s and are effective, they are not practical for long-term use because of the increased heart and blood vessels disease and osteoporosis risks associated with extended use 60. Long-term users often need hormone add-back therapy to counteract many of their hypoestrogenic effects, which may cause a return of PMS symptoms 61.
- Birth control pills or oral contraceptive pills (OCPs). Taking birth control pills with no pill-free interval or with a shortened pill-free interval may reduce PMS and premenstrual dysphoric disorder (PMDD) symptoms for some women. Although oral birth control pills are widely used in clinical practice, their efficacy in treating PMDD has not been strongly supported by evidence. Studies have suggested that oral contraceptives provide benefit when treating physical and psychiatric symptoms of PMS or PMDD. Researchers analyzed four moderate-quality trials of continuous oral contraceptive use (90 mcg levonorgestrel/20 mcg ethinyl estradiol) in women who tracked their symptoms on the Daily Record of Severity of Problems 62. Although results were somewhat inconsistent, an improvement in depressive and physical symptoms (from 30% to 59%) was identified. A higher placebo response occurred in women with PMDD, which suggests that a greater improvement occurred in women with predominantly psychiatric symptoms at baseline 62, 63. A separate PMDD trial found that continuous treatment for 112 days resulted in the most improvement in Daily Record of Severity of Problems scores 63. Women on oral birth control pills experience more hormone-related symptoms on hormone-free days, and hence oral birth control pills treatment with fewer hormone-free days might be beneficial to these women.
- Drospirenone (a man-made progesterone) was particularly found to be effective in treating PMDD symptoms because of its anti-aldosterone and anti-androgenic effects. A 2023 Cochrane review of oral contraceptives containing drospirenone evaluated five trials with 858 women 64. Combined oral contraceptives with drospirenone and ethinylestradiol 20 μg may improve premenstrual symptoms in women with premenstrual dysphoric disorder (PMDD) 64. However, a powerful placebo effect was evident: in one trial, symptoms were reduced for 48% of the combined oral contraceptives containing drospirenone group versus 36% of the placebo group. The difference may not be clinically significant. Furthermore, combined oral contraceptives containing drospirenone may lead to more adverse effects compared to placebo. The effectiveness after three cycles is unknown. Little evidence exists for treating less severe symptoms, and determining whether combined oral contraceptives containing drospirenone work any better than other combined oral contraceptives that contain a different progestogen 64.
- Danazol: This is a synthetic partial androgen agonist/antagonist and gonadotropin inhibitor that has also been shown to be efficacious in treating PMDD by inhibiting ovulation. However, it is associated with hirsutism and teratogenicity and thus not preferred as an initial agent.
Premenstrual Dysphoric Disorder prognosis
When undergoing treatment for premenstrual dysphoric disorder, symptoms tend to improve rapidly and you’re able to enjoy your life more fully. After cessation of treatment, symptoms recur rapidly, and their reemergence is more predictable than that with other mood disorders such as major depressive disorder. Symptoms do not usually recur after removal of the ovaries. Most women don’t have symptoms after menopause.
- Hofmeister S, Bodden S. Premenstrual Syndrome and Premenstrual Dysphoric Disorder. Am Fam Physician. 2016 Aug 1;94(3):236-40. https://www.aafp.org/pubs/afp/issues/2016/0801/p236.html[↩][↩][↩][↩][↩]
- Liguori F, Saraiello E, Calella P. Premenstrual Syndrome and Premenstrual Dysphoric Disorder’s Impact on Quality of Life, and the Role of Physical Activity. Medicina (Kaunas). 2023 Nov 20;59(11):2044. doi: 10.3390/medicina59112044[↩]
- Mishra S, Elliott H, Marwaha R. Premenstrual Dysphoric Disorder. [Updated 2023 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532307[↩][↩][↩]
- Reid RL. Premenstrual Dysphoric Disorder (Formerly Premenstrual Syndrome) [Updated 2017 Jan 23]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279045[↩][↩]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596[↩][↩][↩][↩]
- Premenstrual Dysphoric Disorder. https://familydoctor.org/condition/premenstrual-dysphoric-disorder/[↩]
- Potter J, Bouyer J, Trussell J, Moreau C. Premenstrual syndrome prevalence and fluctuation over time: results from a French population-based survey. J Womens Health (Larchmt). 2009 Jan-Feb;18(1):31-9. doi: 10.1089/jwh.2008.0932[↩][↩][↩][↩][↩][↩][↩]
- Premenstrual Dysphoric Disorder Treatment & Management. https://emedicine.medscape.com/article/293257-treatment#d7[↩]
- Prasad D., Wollenhaupt-Aguiar B., Kidd K.N., de Azevedo Cardoso T., Frey B.N. Suicidal Risk in Women with Premenstrual Syndrome and Premenstrual Dysphoric Disorder: A Systematic Review and Meta-Analysis. J. Womens Health. 2021;30:1693–1707. doi: 10.1089/jwh.2021.0185[↩]
- Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American Family Physician, 85, 35–43.[↩]
- McDowell, M. A., Brody, D. J., & Hughes, J.P. (2007). Has age at menarche changed? Results from the National Health and Nutrition Examination Survey (NHANES) 1999-2004. Journal of Adolescent Health, 40, 227–231.[↩]
- Dasharathy, S. S., Mumford, S. L., Pollack, A. Z., Perkins, N. J., Mattison, D. R., Wactawski-Wende, J., & Schisterman, E. F. (2012). Menstrual bleeding patterns among regularly menstruating women. American Journal of Epidemiology, 175, 536–545.[↩]
- Abnormal Uterine Bleeding. https://www.acog.org/Patients/FAQs/Abnormal-Uterine-Bleeding[↩]
- Chiazze L, Brayer FT, Macisco JJ, Parker MP, Duffy BJ. The Length and Variability of the Human Menstrual Cycle. JAMA. 1968;203(6):377–380. doi:10.1001/jama.1968.03140060001001[↩]
- Fraser IS, Critchley HO, Broder M, Munro MG. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011 Sep;29(5):383-90. doi: 10.1055/s-0031-1287662[↩]
- Wilcox AJ, Dunson D, Baird DD. The timing of the “fertile window” in the menstrual cycle: day specific estimates from a prospective study. BMJ. 2000 Nov 18;321(7271):1259-62. doi: 10.1136/bmj.321.7271.1259[↩]
- Pearlstein T, Steiner M. Premenstrual dysphoric disorder: burden of illness and treatment update. J Psychiatry Neurosci. 2008 Jul;33(4):291-301. https://pmc.ncbi.nlm.nih.gov/articles/PMC2440788[↩]
- Takeda T. Premenstrual disorders: Premenstrual syndrome and premenstrual dysphoric disorder. J Obstet Gynaecol Res. 2023 Feb;49(2):510-518. https://doi.org/10.1111/jog.15484[↩]
- Haußmann J, Goeckenjan M, Haußmann R, Wimberger P. Prämenstruelles Syndrom und prämenstruelle dysphorische Störung – Übersicht zu Pathophysiologie, Diagnostik und Therapie [Premenstrual syndrome and premenstrual dysphoric disorder-Overview on pathophysiology, diagnostics and treatment]. Nervenarzt. 2024 Mar;95(3):268-274. German. doi: 10.1007/s00115-024-01625-5[↩]
- Winer SA, Rapkin AJ. Premenstrual disorders: prevalence, etiology and impact. J Reprod Med. 2006 Apr;51(4 Suppl):339-47.[↩]
- Dennerstein L, Lehert P, Heinemann K. Global study of women’s experiences of premenstrual symptoms and their effects on daily life. Menopause Int. 2011 Sep;17(3):88-95. doi: 10.1258/mi.2011.011027[↩]
- American College of Obstetricians and Gynecologists. Guidelines for Women’s Health Care: A Resource Manual. 4th ed. Washington, DC: American College of Obstetricians and Gynecologists; 2014:608.[↩][↩][↩]
- Wittchen H -U, Becker E, Lieb R, Krause P. Prevalence, incidence and stability of premenstrual dysphoric disorder in the community. Psychol Med. 2002 Jan;32(1):119-32. doi: 10.1017/s0033291701004925[↩]
- Hammarbäck S, Bäckström T, Holst J, von Schoultz B, Lyrenäs S. Cyclical mood changes as in the premenstrual tension syndrome during sequential estrogen-progestagen postmenopausal replacement therapy. Acta Obstet Gynecol Scand. 1985;64(5):393-7. doi: 10.3109/00016348509155154[↩][↩]
- Kumar P, Sharma A. Gonadotropin-releasing hormone analogs: Understanding advantages and limitations. J Hum Reprod Sci. 2014 Jul;7(3):170-4. doi: 10.4103/0974-1208.142476[↩][↩]
- Halbreich U. The etiology, biology, and evolving pathology of premenstrual syndromes. Psychoneuroendocrinology. 2003 Aug;28 Suppl 3:55-99. doi: 10.1016/s0306-4530(03)00097-0[↩][↩][↩][↩]
- Jahanfar S, Lye MS, Krishnarajah IS. The heritability of premenstrual syndrome. Twin Res Hum Genet. 2011 Oct;14(5):433-6. doi: 10.1375/twin.14.5.433[↩]
- Wittchen HU, Perkonigg A, Pfister H. Trauma and PTSD – an overlooked pathogenic pathway for premenstrual dysphoric disorder? Arch Womens Ment Health. 2003 Nov;6(4):293-7. doi: 10.1007/s00737-003-0028-2[↩]
- Bertone-Johnson ER, Hankinson SE, Johnson SR, Manson JE. Cigarette smoking and the development of premenstrual syndrome. Am J Epidemiol. 2008 Oct 15;168(8):938-45. doi: 10.1093/aje/kwn194[↩]
- Bertone-Johnson ER, Hankinson SE, Willett WC, Johnson SR, Manson JE. Adiposity and the development of premenstrual syndrome. J Womens Health (Larchmt). 2010 Nov;19(11):1955-62. doi: 10.1089/jwh.2010.2128[↩]
- Tenny S, Hoffman MR. Relative Risk. [Updated 2023 Mar 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430824[↩]
- Dhingra V, Magnay JL, O’Brien PM, Chapman G, Fryer AA, Ismail KM. Serotonin receptor 1A C(-1019)G polymorphism associated with premenstrual dysphoric disorder. Obstet Gynecol. 2007 Oct;110(4):788-92. doi: 10.1097/01.AOG.0000284448.73490.ac[↩]
- Huo L, Straub RE, Roca C, Schmidt PJ, Shi K, Vakkalanka R, Weinberger DR, Rubinow DR. Risk for premenstrual dysphoric disorder is associated with genetic variation in ESR1, the estrogen receptor alpha gene. Biol Psychiatry. 2007 Oct 15;62(8):925-33. doi: 10.1016/j.biopsych.2006.12.019[↩]
- Pearlstein T, Yonkers KA, Fayyad R, Gillespie JA. Pretreatment pattern of symptom expression in premenstrual dysphoric disorder. J Affect Disord. 2005 Apr;85(3):275-82. doi: 10.1016/j.jad.2004.10.004[↩][↩]
- Meaden PM, Hartlage SA, Cook-Karr J. Timing and severity of symptoms associated with the menstrual cycle in a community-based sample in the Midwestern United States. Psychiatry Res. 2005 Mar 30;134(1):27-36. doi: 10.1016/j.psychres.2005.01.003[↩]
- Endicott J, Nee J, Harrison W. Daily Record of Severity of Problems (DRSP): reliability and validity. Arch Womens Ment Health. 2006 Jan;9(1):41-9. doi: 10.1007/s00737-005-0103-y[↩]
- Borenstein JE, Dean BB, Yonkers KA, Endicott J. Using the daily record of severity of problems as a screening instrument for premenstrual syndrome. Obstet Gynecol. 2007 May;109(5):1068-75. doi: 10.1097/01.AOG.0000259920.73000.3b[↩]
- Premenstrual Syndrome and Premenstrual Dysphoric Disorder. Am Fam Physician. 2016 Aug 1;94(3):236-240. https://www.aafp.org/afp/2016/0801/p236.html[↩]
- Steiner M, Macdougall M, Brown E. The premenstrual symptoms screening tool (PSST) for clinicians. Arch Womens Ment Health. 2003 Aug;6(3):203-9. doi: 10.1007/s00737-003-0018-4[↩][↩]
- Feuerstein M, Shaw WS. Measurement properties of the calendar of premenstrual experience in patients with premenstrual syndrome. J Reprod Med. 2002 Apr;47(4):279-89.[↩]
- Junghaenel DU, Schneider S, Stone AA, Christodoulou C, Broderick JE. Ecological validity and clinical utility of Patient-Reported Outcomes Measurement Information System (PROMIS®) instruments for detecting premenstrual symptoms of depression, anger, and fatigue. J Psychosom Res. 2014 Apr;76(4):300-6. doi: 10.1016/j.jpsychores.2014.01.010[↩]
- Thys-Jacobs S, Starkey P, Bernstein D, Tian J. Calcium carbonate and the premenstrual syndrome: effects on premenstrual and menstrual symptoms. Premenstrual Syndrome Study Group. Am J Obstet Gynecol. 1998 Aug;179(2):444-52. doi: 10.1016/s0002-9378(98)70377-1[↩][↩]
- Ghanbari Z, Haghollahi F, Shariat M, Foroshani AR, Ashrafi M. Effects of calcium supplement therapy in women with premenstrual syndrome. Taiwan J Obstet Gynecol. 2009 Jun;48(2):124-9. doi: 10.1016/S1028-4559(09)60271-0[↩]
- Bertone-Johnson ER, Chocano-Bedoya PO, Zagarins SE, Micka AE, Ronnenberg AG. Dietary vitamin D intake, 25-hydroxyvitamin D3 levels and premenstrual syndrome in a college-aged population. J Steroid Biochem Mol Biol. 2010 Jul;121(1-2):434-7. doi: 10.1016/j.jsbmb.2010.03.076[↩][↩]
- Bertone-Johnson ER, Hankinson SE, Forger NG, Powers SI, Willett WC, Johnson SR, Manson JE. Plasma 25-hydroxyvitamin D and risk of premenstrual syndrome in a prospective cohort study. BMC Womens Health. 2014 Apr 12;14:56. doi: 10.1186/1472-6874-14-56[↩][↩]
- Kashanian M, Mazinani R, Jalalmanesh S, Babayanzad Ahari S. Pyridoxine (vitamin B6) therapy for premenstrual syndrome. Int J Gynaecol Obstet. 2007 Jan;96(1):43-4. doi: 10.1016/j.ijgo.2006.09.014. Epub 2006 Dec 21. Erratum in: Int J Gynaecol Obstet. 2020 Jul;150(1):135. doi: 10.1002/ijgo.13157[↩]
- Cerqueira RO, Frey BN, Leclerc E, Brietzke E. Vitex agnus castus for premenstrual syndrome and premenstrual dysphoric disorder: a systematic review. Arch Womens Ment Health. 2017 Dec;20(6):713-719. doi: 10.1007/s00737-017-0791-0[↩]
- Lustyk MK, Gerrish WG, Shaver S, Keys SL. Cognitive-behavioral therapy for premenstrual syndrome and premenstrual dysphoric disorder: a systematic review. Arch Womens Ment Health. 2009 Apr;12(2):85-96. doi: 10.1007/s00737-009-0052-y[↩]
- Jespersen C, Lauritsen MP, Frokjaer VG, Schroll JB. Selective serotonin reuptake inhibitors for premenstrual syndrome and premenstrual dysphoric disorder. Cochrane Database Syst Rev. 2024 Aug 14;8(8):CD001396. doi: 10.1002/14651858.CD001396.pub4[↩][↩][↩]
- Wikander I, Sundblad C, Andersch B, Dagnell I, Zylberstein D, Bengtsson F, Eriksson E. Citalopram in premenstrual dysphoria: is intermittent treatment during luteal phases more effective than continuous medication throughout the menstrual cycle? J Clin Psychopharmacol. 1998 Oct;18(5):390-8. doi: 10.1097/00004714-199810000-00007[↩]
- Ravindran LN, Woods SA, Steiner M, Ravindran AV. Symptom-onset dosing with citalopram in the treatment of premenstrual dysphoric disorder (PMDD): a case series. Arch Womens Ment Health. 2007;10(3):125-7. doi: 10.1007/s00737-007-0181-0[↩]
- Freeman EW, Rickels K, Sondheimer SJ, Polansky M. Differential response to antidepressants in women with premenstrual syndrome/premenstrual dysphoric disorder: a randomized controlled trial. Arch Gen Psychiatry. 1999 Oct;56(10):932-9. doi: 10.1001/archpsyc.56.10.932[↩]
- Pearlstein TB, Stone AB, Lund SA, Scheft H, Zlotnick C, Brown WA. Comparison of fluoxetine, bupropion, and placebo in the treatment of premenstrual dysphoric disorder. J Clin Psychopharmacol. 1997 Aug;17(4):261-6. doi: 10.1097/00004714-199708000-00004[↩]
- Sundblad C, Wikander I, Andersch B, Eriksson E. A naturalistic study of paroxetine in premenstrual syndrome: efficacy and side-effects during ten cycles of treatment. Eur Neuropsychopharmacol. 1997 Aug;7(3):201-6. doi: 10.1016/s0924-977x(97)00404-5[↩]
- Sundblad C, Hedberg MA, Eriksson E. Clomipramine administered during the luteal phase reduces the symptoms of premenstrual syndrome: a placebo-controlled trial. Neuropsychopharmacology. 1993 Sep;9(2):133-45. doi: 10.1038/npp.1993.52[↩]
- Sundblad C, Modigh K, Andersch B, Eriksson E. Clomipramine effectively reduces premenstrual irritability and dysphoria: a placebo-controlled trial. Acta Psychiatr Scand. 1992 Jan;85(1):39-47. doi: 10.1111/j.1600-0447.1992.tb01440.x[↩]
- Hsiao MC, Liu CY. Effective open-label treatment of premenstrual dysphoric disorder with venlafaxine. Psychiatry Clin Neurosci. 2003 Jun;57(3):317-21. doi: 10.1046/j.1440-1819.2003.01123.x[↩][↩]
- Smith S, Rinehart JS, Ruddock VE, Schiff I. Treatment of premenstrual syndrome with alprazolam: results of a double-blind, placebo-controlled, randomized crossover clinical trial. Obstet Gynecol. 1987 Jul;70(1):37-43.[↩]
- Harrison WM, Endicott J, Nee J. Treatment of premenstrual dysphoria with alprazolam. A controlled study. Arch Gen Psychiatry. 1990 Mar;47(3):270-5. doi: 10.1001/archpsyc.1990.01810150070011[↩]
- Nevatte T, O’Brien PM, Bäckström T, et al.; Consensus Group of the International Society for Premenstrual Disorders. ISPMD consensus on the management of premenstrual disorders. Arch Womens Ment Health. 2013 Aug;16(4):279-91. doi: 10.1007/s00737-013-0346-y[↩][↩]
- Imai A, Ichigo S, Matsunami K, Takagi H. Premenstrual syndrome: management and pathophysiology. Clin Exp Obstet Gynecol. 2015;42(2):123-8.[↩]
- Freeman EW, Halbreich U, Grubb GS, Rapkin AJ, Skouby SO, Smith L, Mirkin S, Constantine GD. An overview of four studies of a continuous oral contraceptive (levonorgestrel 90 mcg/ethinyl estradiol 20 mcg) on premenstrual dysphoric disorder and premenstrual syndrome. Contraception. 2012 May;85(5):437-45. doi: 10.1016/j.contraception.2011.09.010[↩][↩]
- Halbreich U, Freeman EW, Rapkin AJ, Cohen LS, Grubb GS, Bergeron R, Smith L, Mirkin S, Constantine GD. Continuous oral levonorgestrel/ethinyl estradiol for treating premenstrual dysphoric disorder. Contraception. 2012 Jan;85(1):19-27. doi: 10.1016/j.contraception.2011.05.008[↩][↩]
- Ma S, Song SJ. Oral contraceptives containing drospirenone for premenstrual syndrome. Cochrane Database Syst Rev. 2023 Jun 23;6(6):CD006586. doi: 10.1002/14651858.CD006586.pub5[↩][↩][↩]




{kind=link}