
Contents
What is pseudobulbar affect
Pseudobulbar affect (PBA) is a neurologic condition characterized by episodes of sudden, uncontrollable and inappropriate episodes of crying or laughing. This phenomenon is variously referred to as pseudobulbar affect (PBA), pathological laughing and crying (or weeping), emotional lability, emotional incontinence, emotionalism, and involuntary crying.
Pseudobulbar affect (PBA) occurs when certain diseases or brain injuries damage areas of the brain that control normal expression of emotion. Various terms have been used to describe PBA such as emotional incontinence, pathological laughing and crying, emotional dyscontrol, emotionalism, involuntary emotional expressive disorder, forced or involuntary crying, pathological emotionality, emotional lability or affective lability 1.
Pseudobulbar affect (PBA) is characterized by involuntary displays of crying and/or laughing, typically without inner feelings of sadness, depression, happiness, or joy. While such feelings may sometimes be present, the crying and or/laughing are not clearly related to the underlying mood. Although they may start as a response to a situation—perhaps a sad or funny movie—the feelings are more intense and last longer than would be expected. The crying and/or laughing are difficult or impossible to stop. In short, the crying and laughing of PBA are not within voluntary control and are essentially disconnected from external circumstances and internal mood states. Episodes of anger and frustration may also occur. The emotional toll of such symptoms, both on people with multiple sclerosis (MS) and on their family members, friends, and colleagues, tends to be quite high. Patients and families are often worried and embarrassed by this behavior, and apprehensive about it happening again. When severe, PBA may interfere with daily functioning and relationships 2.
Pseudobulbar affect (PBA) episodes may 1:
- Occur several times a day and last from seconds to minutes
- Be exaggerated or incongruent to the patient’s inner emotional state
- Occur spontaneously, often with little to no clear trigger
Pseudobulbar affect can be embarrassing and disruptive to daily life. Patients report that their pseudobulbar affect disorder symptoms affect life situations such as: making or keeping friends, getting divorced or ending a significant relationship, becoming homebound, or moving to a supervised living facility. Patients with PBA symptoms also report greater feelings of frustration, such as being a burden to others and feelings of isolation.
Pseudobulbar affect (PBA) typically occurs in people with certain neurological conditions or injuries that affect the way the brain controls emotion. Pseudobulbar affect (PBA) is common in stroke survivors and people with conditions such as dementia, multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), Alzheimer’s disease, Parkinson’s disease and traumatic brain injury and and other causes of brain injury.
Figure 1. Pseudobulbar affect (PBA) brain lesions
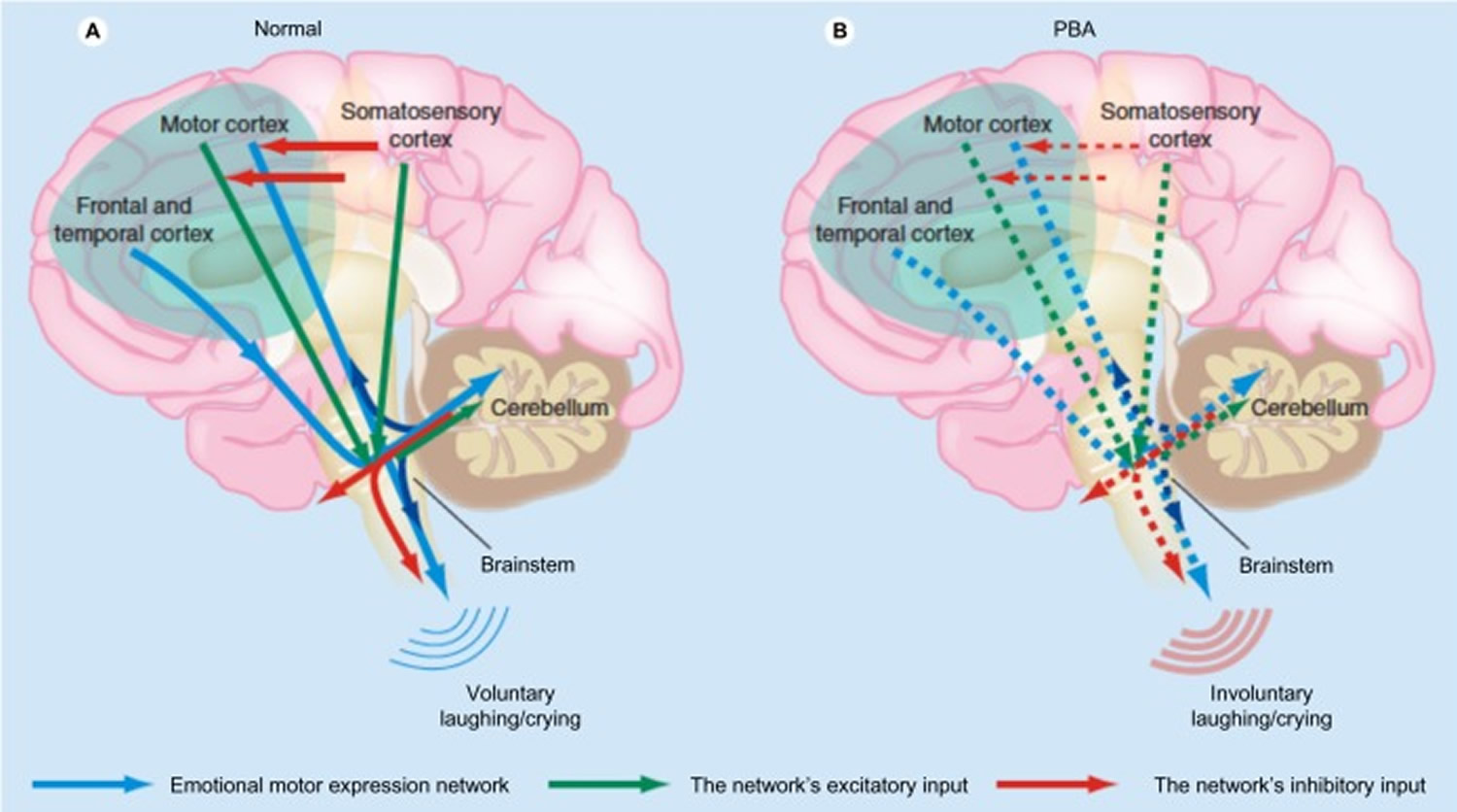
Note: Proposed pathophysiology of pseudobulbar affect. (A) Input from the motor, frontal, and temporal cortices to the brainstem is modulated by input from the cerebellum. Inhibitory input from the somatosensory cortex modulates the motor input. (B) Reduced inhibitory input (broken red arrows in the cortex) results in disinhibition, giving rise to pseudobulbar affect.
[Source 3]Pseudobulbar affect (PBA) is thought to affect nearly two million people in the United States and occurs secondary to a variety of underlying neurologic conditions, such as 4:
- Alzheimer’s disease or other dementias
- Amyotrophic Lateral Sclerosis (ALS)
- Multiple Sclerosis (MS)
- Parkinson’s disease
- Stroke
- Traumatic Brain Injury (TBI)
Prevalence estimates of pseudobulbar affect in multiple sclerosis (MS) have ranged from 7% to 95%, depending on terminology, diagnostic criteria, and populations being studied 5. Using criteria established by Poeck 6—sudden loss of emotional control (crying or laughing or both) on multiple occasions over one month, which occurs in response to nonspecific stimuli and lacks an associative, matching mood state—Feinstein and his colleagues obtained a point-in-time prevalence of 10% in a clinic sample that was representative of a large, community-based sample of multiple sclerosis (MS) patients. This 10% prevalence rate is similar to that proposed in two earlier studies 7, but significantly lower than that previously suggested by others (Cottrell & Wilson, 1926; Pratt, 1961; Sugar & Nadell, 1943), presumably because the strict diagnostic criteria used in the study helped to differentiate those with PBA from the larger number of patients exhibiting non-specific emotional lability.
The largest ever clinic-based study of pseudobulbar affect (PBA) symptom prevalence (PRISM) was conducted among 5,290 patients enrolled at 173 sites across the USA. The study revealed that 36.7% of all enrolled patients with neurologic conditions had pseudobulbar affect symptoms, as assessed by a Center for Neurologic Study-Lability Scale (CNS-LS) score ≥13.
The PRISM Study assessed the prevalence of pseudobulbar affect symptoms in a clinical practice setting. Patients with 6 different neurologic conditions were evaluated using the Center for Neurologic Study-Lability Scale. Pseudobulbar affect (PBA) symptoms were defined by a Center for Neurologic Study-Lability Scale ≥ 13. When evaluated by disease state, 29% of Alzheimer’s patients, 38% of Stroke patients, 46% of MS patients, and 52% of traumatic brain injury patients were found to have pseudobulbar affect symptoms. These findings suggest that routine screening for pseudobulbar affect is important.
Figure 2. Center for Neurologic Study–Lability Scale (Self Administered Questionnaire)
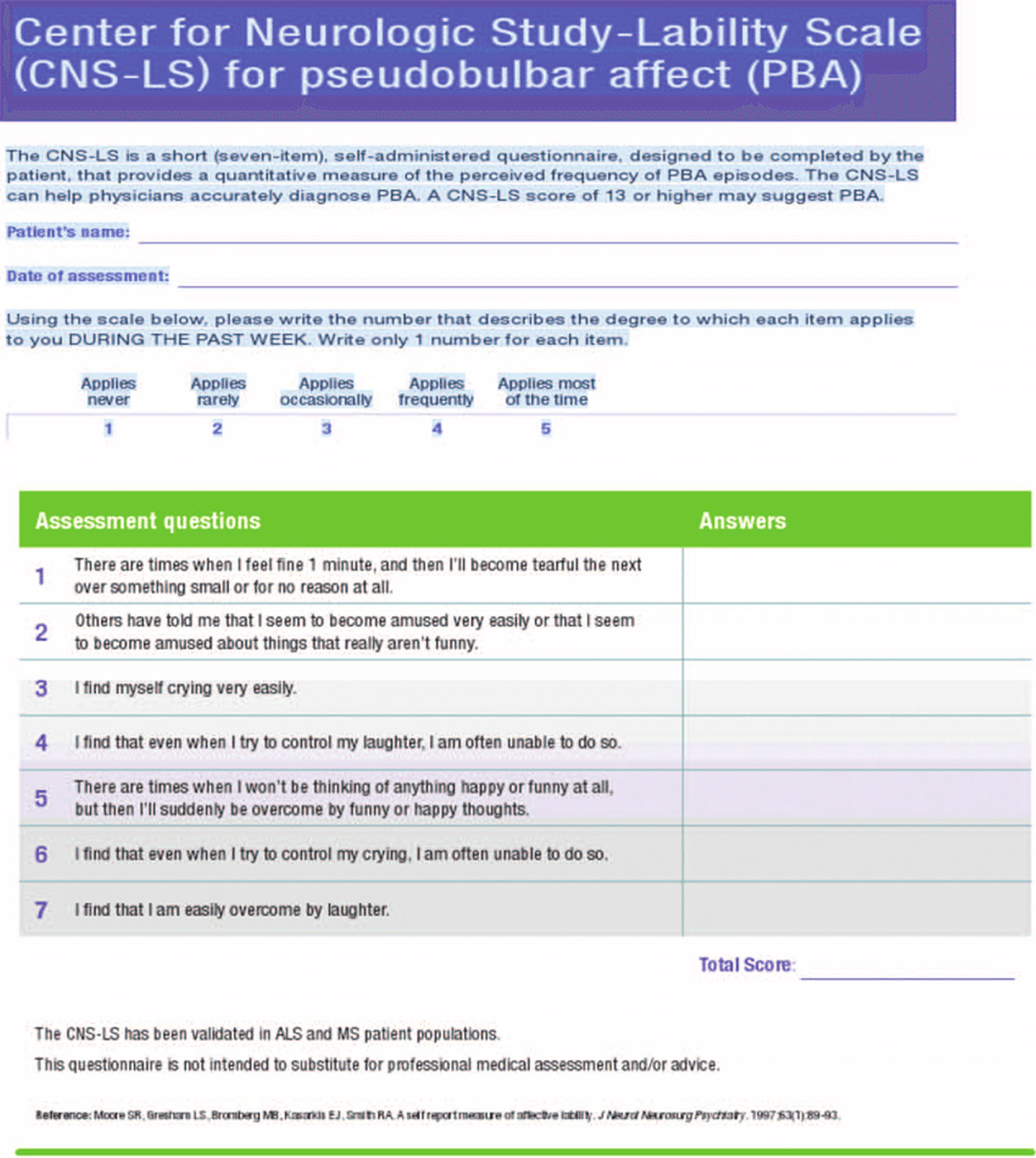
How to use the Center for Neurologic Study–Lability Scale
The Center for Neurologic Study–Lability Scale is a short 7-item, self-administered questionnaire, designed to be completed by the patient, that provides a quantitative measure of the perceived frequency of pseudobulbar affect episodes. The Center for Neurologic Study–Lability Scale can help accurately diagnose pseudobulbar affect 8.
How to Score
Add the values for each of the 7 items to get the total score. A Center for Neurologic Study–Lability Scale score of 13 or higher may suggest pseudobulbar affect (PBA).
Sensitivity & Specificity 8
- Sensitivity: 74%
- Specificity: 80%
Pseudobulbar affect is Distinct from Mood Disorders like Depression
There are five common ways to distinguish pseudobulbar affect disorder from depression 9:
- The emotional expression with pseudobulbar affect disorder may be crying or laughing or both. With depression, the emotional expression (if present) is mainly crying.
- With depression, episodes of depressed mood are long in duration and if crying episodes are present, the patient may be able to modulate the length and severity.
- An underlying neurologic disorder is always present with pseudobulbar affect disorder but only sometimes is present with depression.
- In pseudobulbar affect disorder, a provoking stimulus, or trigger, may be minimal or nonexistent and crying (affect) is exaggerated or incongruent to mood. With depression, crying may be provoked by mood-related situations.
- With depression, the patient may have feelings or thoughts of helplessness, hopelessness, guilt, worthlessness, and sometimes death. With pseudobulbar affect disorder, there is no specific relationship to such accompanying feelings or thoughts.
Depression and pseudobulbar affect disorder may often be comorbid and the presence of one does not exclude the other.
Pseudobulbar affect often goes undiagnosed or is mistaken for mood disorders. Once diagnosed, however, pseudobulbar affect can be managed with medication. The goal of treatment is to reduce the severity and frequency of emotional outbursts. Treatment may include the use of antidepressants and/or a combination of dextromethorphan and quinidine.
Pseudobulbar affect complications
Severe symptoms of pseudobulbar affect (PBA) can cause embarrassment, social isolation, anxiety and depression. The condition might interfere with your ability to work and do daily tasks, especially when you’re already coping with a neurological condition.
Pseudobulbar affect causes
Pseudobulbar affect (PBA) typically occurs in people with neurological conditions or injuries, including 10:
- Stroke
- Amyotrophic lateral sclerosis (ALS)
- Multiple sclerosis (MS)
- Traumatic brain injury
- Alzheimer’s disease
- Parkinson’s disease
- Brain tumors
- Extrapyramidal and cerebellar disorders
While further research is needed, the cause of PBA is believed to involve injury to the neurological pathways that regulate the external expression of emotion (affect). The underlying mechanism in pseudobulbar affect (PBA) appears to be a lack of voluntary control, also termed disinhibition, but the pathways are complex and are as yet incompletely understood 10.
The cerebellum appears to play a far larger role in PBA than was hypothesized a few years ago. There are pathways from the cortex to pons to cerebellum that appear to control not only motor, but also cognitive and affective function. In support of this, patients with cerebellar lesions may demonstrate abnormalities of affect and may show emotional lability,16 and patients with multiple system atrophy – cerebellar type have a high frequency of PBA 11. One hypothesis is that the cerebellum plays a key role in modulating emotional responses so as to keep them appropriate to the social situation and to the patient’s mood based on input from the cerebral cortex. Disruption of corticopontine–cerebellar circuits results in impairment of this cerebellar modulation, causing PBA 12. There appears to be both sensory and motor input. A theory has been proposed in which the motor control of emotions is modulated by the cerebellum, which acts as a “gate control.” There is direct input from the motor cortex and from the frontal and temporal cortices through the brainstem which is modulated by the cerebellum. The motor input is in turn modulated by inhibitory input from the somatosensory cortex. Reduction of the inhibitory input results in disinhibition of the cerebellum, resulting in socially inappropriate or situationally disproportionate emotional expression, which is manifested as PBA (see Figure 1 above) 3. The manner in which specific cerebellar circuitry is involved in this process is the subject of ongoing investigations.14,19,20 The primary neurotransmitters believed to be involved in PBA are serotonin and glutamate. The role of serotonin in corticolimbic or cerebellar pathways may account for its impact on PBA. Glutamate is an excitatory neurotransmitter whose receptors are widely distributed within the brain. Thus, modulation of glutamatergic transmission can have widespread effects 3.
Pseudobulbar affect symptoms
The primary sign of pseudobulbar affect (PBA) is frequent, involuntary and uncontrollable outbursts of crying or laughing that are exaggerated or not connected to your emotional state. Laughter often turns to tears. Your mood will appear normal between episodes, which can occur at any time. Crying appears to be a more common sign of PBA than laughing.
The degree of the emotional response caused by pseudobulbar affect is often striking, with crying or laughing lasting up to several minutes. For example, you might laugh uncontrollably in response to a mildly amusing comment. Or you might laugh or cry in situations that others don’t see as funny or sad. These emotional responses typically represent a change from how you would have previously responded.
Because pseudobulbar affect often involves crying, the condition is frequently mistaken for depression. However, pseudobulbar affect episodes tend to be short in duration, while depression causes a persistent feeling of sadness. Also, people with PBA often lack certain features of depression, such as sleep disturbances or a loss of appetite. But depression is common among those who have pseudobulbar affect.
Pseudobulbar affect diagnosis
Pseudobulbar affect (PBA) is typically diagnosed during a neurological evaluation. Specialists who can diagnose pseudobulbar affect include internists, neuropsychologists, neurologists and psychiatrists.
Pseudobulbar affect (PBA) is often misdiagnosed as depression, bipolar disorder, generalized anxiety disorder, schizophrenia, a personality disorder and epilepsy. To help your doctor determine if you have pseudobulbar affect, share specific details about your emotional outbursts.
Diagnostic criteria for pseudobulbar affect
Poeck 13
- The emotional response is situationally inappropriate
- The patient’s feelings and the affective response are not closely related
- The duration and severity of the episodes cannot be controlled by the patient
- Expression of the emotion does not lead to a feeling of relief
Cummings: necessary elements of the episodes 14
- A change from previous emotional responses
- Inconsistent with or disproportionate to mood
- Not dependent on a stimulus, or are excessive relative to that stimulus
- Cause significant distress or social/occupational impairment
- Not accounted for by another psychiatric or neurologic disorder
- Not due to a drug
Prompt and accurate diagnosis is important in order to provide the appropriate medical treatment for the person with MS as well as education and support for the patient and family. A comprehensive clinical assessment consists of a thorough history, detailed characterization of the episodes of crying and/or laughing, and complete medical, neurologic, and mental status examinations 15. This approach will distinguish PBA from depression, but an electroencephalogram may be needed to rule out partial complex epilepsy that very rarely produces episodic laughing and/or crying 1.
Using the two validated screening instruments described below, Work and colleagues 2 also found a 10% prevalence among people with MS. Two instruments designed to facilitate the diagnosis of PBA have been validated in populations other than MS. The Pathological Laughing and Crying Scale (PLACS), a clinician-administered interview, quantifies several aspects of laughing and crying episodes, including their duration, relationship to external events, degree of voluntary control, inappropriateness in relation to concurrent emotions, and extent of distress following the episode 16. The PLACS has since been used in studies of MS patients 2. The Center for Neurologic Study–Lability Scale (CNS–LS) is a self-report measure of affective lability
developed by Moore and colleagues 17. The scale reliably quantifies patients’ perceptions of several aspects of PBA episodes, including frequency, intensity, lability, degree of voluntary control, and inappropriateness to context. The Center for Neurologic Study–Lability Scale (CNS–LS), which was initially developed for use in patients with amyotrophic lateral sclerosis (ALS), has since been used to study patients with MS 18.
Pseudobulbar affect treatment
The goal of treatment for pseudobulbar affect (PBA) is to reduce the severity and frequency of emotional outbursts. An occupational therapist also can help you develop ways to complete everyday tasks despite your pseudobulbar affect (PBA).
Pseudobulbar affect medication
Medication options include:
- Antidepressants. Antidepressants, such as tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs), can help reduce the frequency and severity of your PBA episodes. Antidepressants for the treatment of PBA are typically prescribed at doses lower than are those used to treat depression.
- Dextromethorphan hydrobromide and quinidine sulfate (Nuedexta). This is the only medication approved by the Food and Drug Administration that is designed to specifically treat PBA. This compound contains dextromethorphan 20 mg and quinidine 10 mg, thus taking advantage of the blockade exerted by quinidine on the first-pass hepatic metabolism of dextromethorphan. A study on people with MS and ALS showed that those taking the medication had only about half as many laughing and crying episodes as did those taking the placebo.
Table 1. Placebo-controlled trials of medications in pseudobulbar affect
| Drug class | Drug | Disease | Number of subjects | Main findings | Reference |
|---|---|---|---|---|---|
| TCA | Nortriptyline | Stroke | 28 | Reduced severity on validated scale (PLACS) | 19 |
| SSRI | Fluoxetine | Stroke | 20 | Reduced severity on unvalidated scale | 20 |
| SSRI | Sertraline | Stroke | 28 | Reduced lability on unvalidated scale | 21 |
| SSRI | Fluoxetine | Stroke | 106 | Reduced crying on unvalidated scale | 22 |
| Antiglutamatergic | Nuedexta | MS | 150 | Reduced severity on validated scale (CNS-LS) | 23 |
| Antiglutamatergic | Nuedexta | ALS or MS | 326 | Reduced severity on validated scale (CNS-LS) | 24 |
Abbreviations: ALS, amyotrophic lateral sclerosis; CNS-LS, Center for Neurologic Study – Lability Scale; Nuedexta, dextromethorphan/quinidine; MS, multiple sclerosis; PLACS, Pathological Laughter and Crying Scale; SSRI, selective serotonin reductase inhibitor; TCA, tricyclic antidepressant.
Your doctor will help you choose the best therapy for you, taking into account possible medication side effects and any other conditions you have and medications you use.
Until recently, the management of PBA relied primarily on antidepressant medications in both the tricyclic (e.g., amitryptiline, imipramine, desipramine, nortriptyline), and selective-serotonin reuptake inhibitor classes (fluoxetine, fluvoxamine, citalopram,paroxetine, sertraline). No single agent appears to be more effective than others. Confirming the disassociation between pseudobulbar affect and depression, improvement occurs at doses generally lower than those used to treat depression and much more quickly, often in less than one week 1. Success has been reported with other agents, but with the limited research evidence, they should be reserved for people who cannot take or do not respond to first-line treatments. The include levodopa, reboxetine, venlafaxine, mirtazapine, lamotrigine, methylphenidate, dexamfetamine, and amantadine 1.
Trials sponsored by Avanir Pharmaceuticals with patients with MS and ALS led to FDA approval in 2010 of Nuedexta, an orally-administered combination of dextromethorphan and quinidine 25. There is more limited clinical experience with Nuedexta (dextromethorphan/quinidine) because of the relatively recent FDA approval. However, the most common side effects are dizziness, diarrhea, falls, headache, nausea, fatigue, nasopharyngitis, constipation, and dysphagia. At the dose contained in the approved compound, quinidine did not demonstrate adverse cardiac effects 26. The American Academy of Neurology published guidelines in 2009 which recommended that dextromethorphan/quinidine “should be considered for treatment of PBA in patients with ALS, if approved by the FDA and if side effects are acceptable.”12 Updated guidelines have yet to be issued. The FDA-approved dosing is one capsule daily for 7 days, followed by an increase to one capsule every 12 hours. It may take longer to notice an effect 1 up to 4–5 weeks of treatment—compared to antidepressants 1. All medications have side effects, many interact with other drugs being taken, and some are contraindicated for certain individuals. It is important to discuss these issues thoroughly with a physician and periodically reassess the need for medication because some patients improve spontaneously. Good communication and a solid patient–doctor relationship are essential components of effective treatment.
Coping and support
Living with psedobulbar affect (PBA) can be embarrassing and stressful. It might help to explain to family, friends and co-workers how the condition affects you, so they aren’t surprised or confused by your behavior.
Talking to other people who have PBA also might help you feel understood and give you a chance to discuss tips for coping with the condition.
To cope with an episode:
- Distract yourself
- Take slow, deep breaths
- Relax your body
- Change your position
- Wortzel HS, Oster TJ, Anderson CA, Arciniegas DB. Pathological laughing and crying: Epidemiology, pathophysiology and treatment. CNS Drugs 2008; 22: 531–545.[↩][↩][↩][↩][↩][↩][↩]
- Work SS, Colamonico JA, Bradley WG, Kaye RE. Pseudobulbar affect: an under-treated neurological disorder. Adv Ther 2011; 28(7): 586–601.[↩][↩][↩]
- Miller A, Pratt H, Schiffer RB. Pseudobulbar affect: the spectrum of clinical presentations, etiologies and treatments. Expert Rev Neurother. 2011;11(7):1077–1088. https://www.ncbi.nlm.nih.gov/pubmed/21539437[↩][↩][↩]
- Brooks BR, Crumpacker D, Fellus J, et al., PRISM: A Novel Research Tool to Assess the Prevalence of Pseudobulbar Affect Symptoms across Neurological Conditions, PLOS ONE 2013;8:e72232[↩]
- Feinstein A, Feinstein K, Gray T, O’Connor P. Prevalence and neurobehavioral correlates of pathological laughing and crying in multiple sclerosis. Archives of Neurology 1997; 54: 1116–1121.[↩]
- Poeck K. Pathophysiology of emotional disorders associated with brain damage. In Vinken PJ, Bruyn GW (eds): Handbook of Clinical Neurology. Amsterdam: North Holland Publishing, 1969: 343–367.[↩]
- Surridge D. An investigation into some psychiatric aspects of multiple sclerosis. British Journal of Psychiatry 1969; 115: 749–764.[↩]
- Moore SR, Gresham LS, Bromberg MB, Kasarkis EJ, Smith RA. A self report measure of affective lability. J Neurol Neurosurg Psychiatry. 1997;63(1):89-93.[↩][↩]
- Cummings JL, Arciniegas DB, Brooks BR, et al. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr 2006;11(6):1-7.[↩]
- Ahmed A, Simmons Z. Pseudobulbar affect: prevalence and management. Therapeutics and Clinical Risk Management. 2013;9:483-489. doi:10.2147/TCRM.S53906. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3849173/[↩][↩][↩]
- Parvizi J, Joseph J, Press DZ, Schmahmann JD. Pathological laughter and crying in patients with multiple system atrophy-cerebellar type. Mov Disord. 2007;22(6):798–803. https://www.ncbi.nlm.nih.gov/pubmed/17290465[↩]
- Parvizi J, Coburn KL, Shillcutt SD, Coffey CE, Lauterbach EC, Mendez MF. Neuroanatomy of pathological laughing and crying: a report of the American Neuropsychiatric Association Committee on Research. J Neuropsychiatry Clin Neurosci. 2009;21(1):75–87. https://www.ncbi.nlm.nih.gov/pubmed/19359455[↩]
- Poeck K. Pathophysiology of emotional disorders associated with brain damage. In: Vinken PJ, Bruyn GW, editors. Handbook of Clinical Neurology. Vol. 3. Amsterdam: North Holland Publishing; 1969. pp. 343–367.[↩]
- Cummings JL, Arciniegas DB, Brooks BR, et al. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr. 2006;11(6):1–7. https://www.ncbi.nlm.nih.gov/pubmed/16816786[↩]
- Arciniegas DB, Lauterbach EC, Anderson KE, et al. The differential diagnosis of pseudobulbar affect (PBA): Distinguishing PBA among disorders of mood and affect. Proceedings of a roundtable meeting. CNS Spectrums 2005; 10: 1–14.[↩]
- Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: Validation of a measurement scale and double-blind treatment study. American Journal of Psychiatry 1993; 150: 286–293.[↩]
- Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. Journal of Neurology, Neurosurgery, and Psychiatry 1997; 63: 89–93.[↩]
- Smith R, Berg J, Pope L, et al. Validation of the CNS emotional lability scale for pseudobulbar affect (pathological laughing and crying) in multiple sclerosis patients. Multiple Sclerosis 2004; 10: 679–685.[↩]
- Robinson RG, Parikh RM, Lipsey JR, Starkstein SE, Price TR. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry. 1993;150(2):286–293. https://www.ncbi.nlm.nih.gov/pubmed/8422080[↩]
- Brown KW, Sloan RL, Pentland B. Fluoxetine as a treatment for post-stroke emotionalism. Acta Psychiatr Scand. 1998;98(6):455–458. https://www.ncbi.nlm.nih.gov/pubmed/9879787[↩]
- Burns A, Russell E, Stratton-Powell H, Tyrell P, O’Neill P, Baldwin R. Sertraline in stroke-associated lability of mood. Int J Geriatr Psychiatry. 1999;14(8):681–685. https://www.ncbi.nlm.nih.gov/pubmed/10489659[↩]
- Choi-Kwon S, Han SW, Kwon SU, Kang DW, Choi JM, Kim JS. Fluoxetine treatment in poststroke depression, emotional incontinence, and anger proneness: a double-blind, placebo-controlled study. Stroke. 2006;37(1):156–161. http://stroke.ahajournals.org/content/37/1/156.long[↩]
- Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol. 2006;59(5):780–787. https://www.ncbi.nlm.nih.gov/pubmed/16634036[↩]
- Pioro EP, Brooks BR, Cummings J, et al. Dextromethorphan plus ultra low-dose quinidine reduces pseudobulbar affect. Ann Neurol. 2010;68(5):693–702. https://www.ncbi.nlm.nih.gov/pubmed/20839238[↩]
- Garnock-Jones KP. Dextromethorphan/quinidine: In pseudobulbar affect. CNS Drugs 2011; 25: 435–445.[↩]
- Pioro EP. Current concepts in the pharmacotherapy of pseudobulbar affect. Drugs. 2011;71(9):1193–1207. https://www.ncbi.nlm.nih.gov/pubmed/21711063[↩]





 is to reduce the severity and frequency of emotional outbursts.){kind=link}