Red light therapy
Red light therapy also known as non-thermal LED light, low-intensity long-wavelength red light, low-level red light therapy, low-power laser therapy, low-level laser therapy (LLLT) or cold laser therapy is a treatment that uses low levels of red light (wavelength in the range 600 to to 1100 nm) to reportedly improve your skin’s appearance, like reducing wrinkles, photoaging (premature skin aging caused by repeated exposure to ultraviolet [UV] radiation from the sun or tanning beds), wound healing, scars, redness and acne. In skin applications, red light therapy has been shown to stimulate collagen production and increase fibroblast proliferation, increase mitochondrial cytochrome C oxidase, blood circulation and oxygenation, reduce inflammation and speed wound healing 1, 2, 3, 4, 5, 6. Red light has anti-inflammatory effects and has been shown to be beneficial for the treatment of inflammatory acne lesions 7, 8.
Red light therapy (wavelength in the range 635 to to 650 nm) is also touted to treat other medical conditions such as nearsightedness (myopia) 9, 10, 11, 12, 13, 14, 15. Short-sightedness or nearsightedness (myopia) means people struggle to see objects clearly that are far away, while objects that are near remain clear. Results from clinical trials in China suggest that red light therapy can prevent or slow down the progression of nearsightedness (myopia) in children, significantly reducing axial elongation and myopia progression 14, 16, 17, 18, 12, 13, 19. Some studies done in China 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 9. These studies included relatively small numbers of 192 Chinese children aged 6 to 16 years with at least −4.0 diopters of cycloplegic spherical equivalent refraction in 1 or both eyes who were treated using a portable desktop device (Eyerising Myopia Management Device, Suzhou Xuanjia Optoelectronics Technology, Suzhou, China) that incorporates a semiconductor laser diode capable of emitting low-level red light with a wavelength of 650 nm and a luminance of 1600 lux through the pupil to the retina 21. Children were excluded if they had history or presence of strabismus (crossed eyes or squint), eye trauma, other eye diseases, systemic diseases, or had received other myopia control treatment, such as atropine therapy, orthokeratology (a non-surgical treatment that uses specially designed, rigid contact lenses to gently reshape the cornea or the front surface of the eye while you sleep), or Defocus Incorporated Multiple Segments glasses 21. For the repeated low-level red light (RLRL) therapy, children are instructed to look into a red light-emitting instrument for 3 minutes per session, twice a day separated by minimum interval of 4 hours, 7 days per week until the 12-month follow-up 21. The participants attended follow-up appointments 1, 3, 6, 9, and 12 months after the baseline evaluation. Note that the portable desktop device (Eyerising Myopia Management Device) tested in these studies are not available in the U.S.
A recent study in the U.S. suggested that red light therapy with several available red light instruments (the Sky-n1201a and the Future Vision Class 1 laser products) could cause retinal damage 32. One published case study of a 12 year old girl who sustained retinal damage after 5-month application of repeated low-level red-light therapy 33. In this case, the child’s best corrected visual acuity decreased from 6/6 to 6/9 33. Fundus photos revealed bilaterally darkened foveae with a hypoautofluorescent plaque in autofluorescence images 33. Optical coherence tomography (OCT) imaging showed bilateral foveal ellipsoid zone disruption and interdigitation zone discontinuity 33. Multifocal electroretinography revealed moderately and mildly decreased responses in the macula and paramacula, respectively 33. Visual acuity improved to 6/7.5 three months after low-level red-light therapy was terminated 33. In this cohort study, among 52 children using repeated low-level red-light therapy for over 1 year compared with 47 nonusers, repeated low-level red-light therapy users showed lower cone density, particularly within 0.5 mm from the retinal fovea, with abnormal drusenlike lesions detected in some of these cases 34. These findings suggest that repeated low-level red-light therapy may be associated with cellular-level retinal changes in macular cone cells, highlighting the importance of further studies assessing its safety for young patients with nearsightedness (myopia), especially with long-term exposure 34. Low-level red-light therapy “may exceed tissue tolerance limits, causing unexpected ganglion cell layer damage”, the authors of the study wrote 34. Although low-level red-light therapy “might control the progression of myopia, further studies are needed to provide more definitive information regarding longer-term efficacy and safety” they added 34. These new study suggests low-level red-light therapy “may have subtle effects on cone density that are not readily visualized with standard clinical tests” wrote Jacque Duncan, MD, of the University of California San Francisco, in a commentary on the paper 35. These researchers warned doctors about using red light therapy to treat nearsightedness (myopia) with caution until safety standards can be confirmed 33, 32, 34, 36, 37. Lisa Ostrin and Alexander Schill, a University of Houston optometry researchers are warning against the use of low-level red light therapy as a method to control myopia, or nearsightedness, especially in children 32. The 3-minute protocol for low level red light therapy to treat nearsightedness (myopia) may put the retina at risk for photochemical and thermal damage 32. “Thermal ocular injury from a laser can occur with exposures at any wavelength when the temperature change of the retina is greater than 10° C, resulting in denaturation of proteins. With thermal damage, the lesion is typically less than the size of the beam diameter, and the resultant scotomas are permanent” 32. “In conclusion, based on measurements in our laboratory, it is recommended that clinicians strongly reconsider the use of LLRL therapy for myopia in children until safety standards can be confirmed” 32. Laura Enyedi, a pediatric ophthalmologist at the Duke Eye Center in North Carolina stated that “there simply is not enough information to assess the safety of red light therapy, and the devices available in the US are not regulated and could damage your child’s retina, leading to loss of vision. Right now, your best option is to make some simple changes for your child such as reducing screen time, increasing outdoor time for your child, and asking your child’s ophthalmologist about other potential solutions, such as low-dose atropine eye drops or special contact lenses which are approved by the FDA” 38.
To date, there’s a lot of ongoing research, publication of small studies and much discussion on the internet about the effectiveness of red light therapy for all types of health uses. Results of some studies do show some promise, but the full effectiveness of red light therapy has yet to be determined. What’s confusing — and controversial — is the effectiveness of the red light therapy for the purposes it’s being promoted.
Red light therapy is thought to work by acting on the “power plant” in your body’s cells called mitochondria 6. With more energy, other cells can do their work more efficiently, doing things like repairing skin, boosting new cell growth and enhancing skin rejuvenation. More specifically, certain cells absorb light wavelengths and are stimulated to work.
Most experts say that they don’t know yet if red light therapy is effective for all its claimed uses. Most say that the studies published so far show some potential for certain conditions, but that more studies need to be conducted. Red light therapy is still an emerging treatment that’s generating growing interest. But at this point in time, there’s not enough evidence to support most uses.
The gold standard of studies to determine if a product is effective is a randomized, placebo-controlled trial. This means that a certain number of people with the same range of characteristics (age, weight, race, sex, etc.) get either the study treatment or a placebo (fake or “sham” treatment) for treatment of the same condition.
Some studies also include a comparison to another commonly used treatment. Results can then be compared between the emerging treatment versus no treatment (the placebo group) or versus a “current standard” treatment.
Many of the published studies using red light therapy included only a small number of people, didn’t include a placebo group, weren’t conducted in humans (animal studies) or were limited to cell tissue itself. Most researchers say results so far look promising, but that more quality studies with larger numbers of people are needed.
Red light therapy may work in skin health to 39, 40, 41:
- Stimulate collagen production, which gives skin its structure, strength and elasticity.
- Increase fibroblast production, which makes collagen. Collagen is a component of connective tissue that builds skin.
- Increase blood circulation to the tissue.
- Reduce inflammation in cells.
Animal studies have shown that red light irradiation enhances mitochondrial catalase activity, which improves cell metabolism and leads to increased glycogen and protein biosynthesis. These changes promote cell growth and wound healing 42, 43, 6.
Red light therapy is promoted as a treatment for some common skin conditions to 44:
- Improve wound healing.
- Reduce stretch marks.
- Reduce wrinkles, fine lines and age spots.
- Improve facial texture.
- Improve psoriasis, rosacea and eczema (dermatitis).
- Improve scars.
- Improve sun-damaged skin.
- Improve hair growth in people with androgenic alopecia.
- Improve acne.
Other potential medical uses of red light therapy being investigated include 45, 46:
- To reduce cancer chemotherapy side effects, including oral mucositis.
- To relieve pain and inflammation associated with ankle tendonitis, rheumatoid arthritis, carpal tunnel syndrome and osteoarthritis of the knee.
- To prevent cold sores from herpes simplex virus from recurring.
Lots of other red light therapy uses are being touted on the internet. There’s no scientific evidence to support red light therapy use in weight loss, cancer, cellulite removal, warts, temporomandibular joint (TMJ) dysfunction or mental health conditions like depression, dementia and seasonal affective disorder (SAD) 47, 48, 49, 47, 50.
If you’re interested in red light therapy treatment, it’s best to first discuss this with your doctor or dermatologist (skin doctor). Your skin doctor will examine your skin first and then confirm a diagnosis. Then, you’ll work together to discuss treatment options that’ll achieve your desired result. Options may or may not include red light therapy.
Figure 1. Light (electromagnetic) spectrum
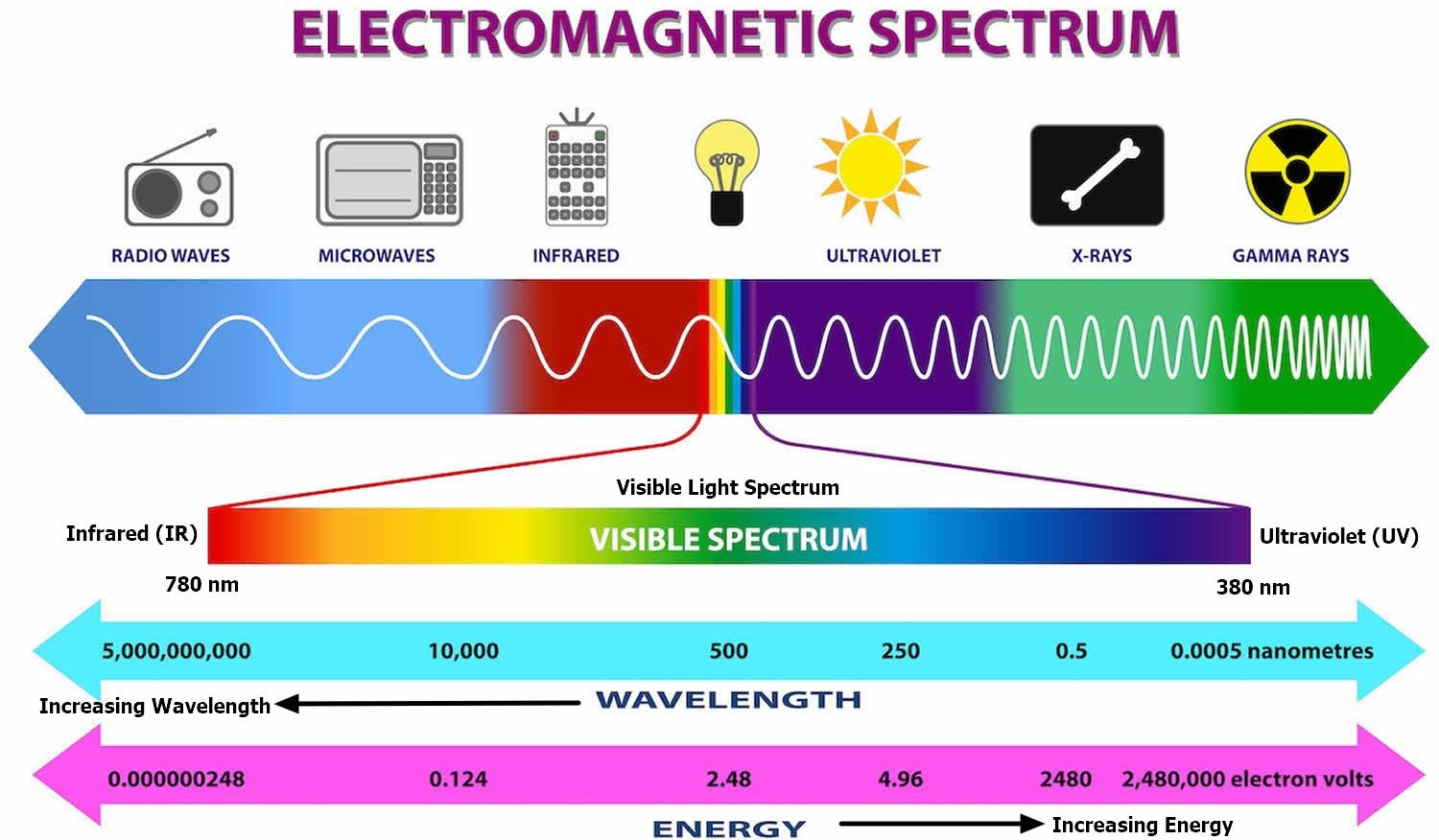
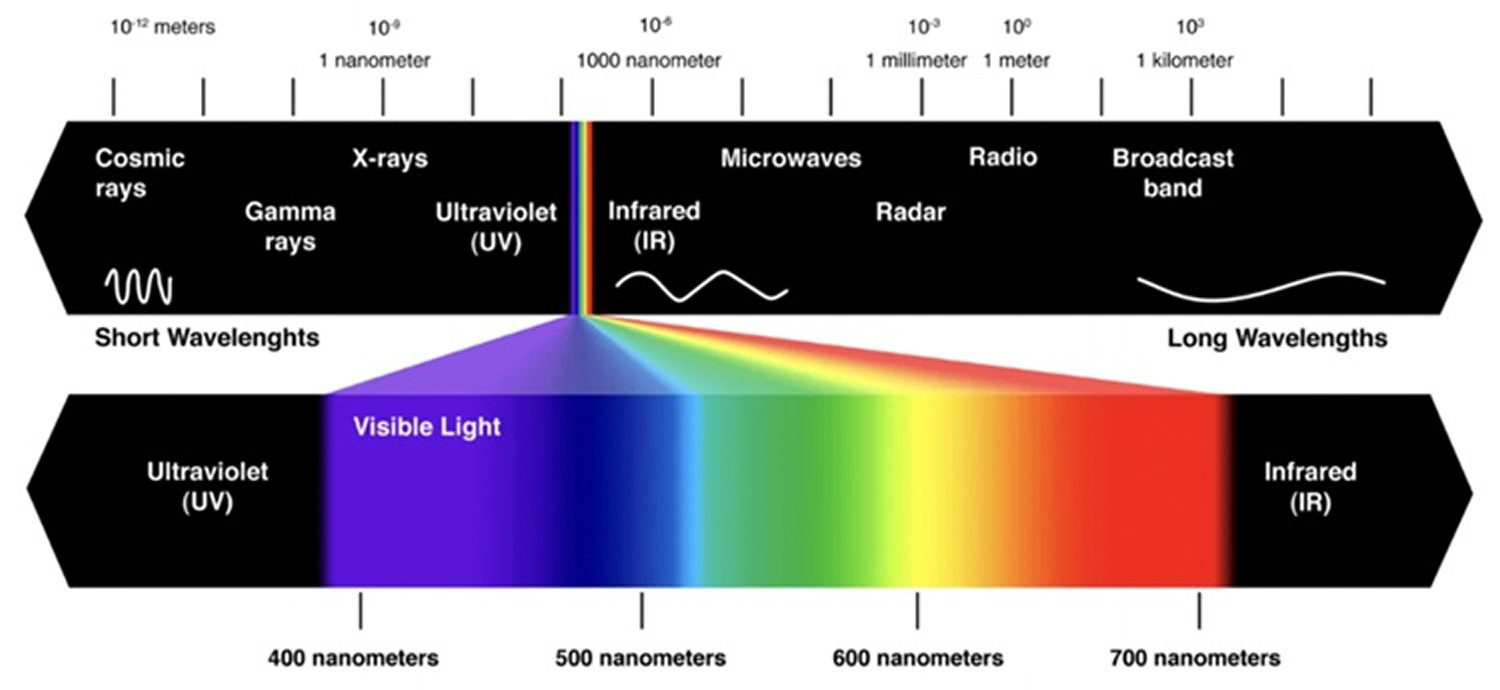
Figure 2. Visible light spectrum
Red light therapy benefits
Red light therapy is already widely medically accepted in its use in photodynamic therapy (PDT). In photodynamic therapy (PDT), low-power red laser light is used to activate a light-sensitive drug (photosensitizer) or photosensitizing agent. The interaction creates a chemical reaction that destroys cells. Photodynamic therapy (PDT) is used to treat some skin conditions, including superficial types of skin cancer and psoriasis, acne and warts, and other types of cancer 51, 52, 53, 54, 55, 56, 57. Topical aminolevulinic acid (ALA) and methyl aminolevulinate (MAL) are photosensitizing agents used in photodynamic therapy (PDT) for the treatment of actinic keratoses and superficial nonmelanoma skin cancers, particularly targeting superficial and in situ squamous cell carcinoma (Bowen disease) and superficial basal cell carcinomas 58. Indocyanine green and indole-3-acetic acid can also be used. Photodynamic therapy (PDT) may also be used for treatment of small, thin, low-risk nodular basal cell carcinomas (BCCs) outside of the head and neck area 59. The evidence that photodynamic therapy (PDT) is useful in the treatment of acne is positive but limited 60.
Photodynamic therapy (PDT) is also sometimes used off-label for facial rejuvenation and to treat a variety of skin infections including wound infections, onychomycosis (fungal infection that affects the nails particularly in toenails, and can cause discoloration, thickening, and separation of the nail from the nail bed), viral warts, and cutaneous leishmaniasis (a skin infection caused by leishmania parasites transmitted through the bite of infected sandflies) 61, 62, 63, 64, 65. Several other conditions have also been studied and may respond to photodynamic therapy (PDT) such as psoriasis, mycosis fungoides, and extramammary Paget disease.
Aminolevulinic acid (ALA) is approved by the FDA for the treatment of hypertrophic actinic keratoses on the face and scalp only with blue light 66. An aminolevulinic acid (ALA) patch and an aminolevulinic acid (ALA) gel formulation with nanoemulsion with red light are also approved in Europe 66. In the FDA-approved protocol, the aminolevulinic acid (ALA) photosensitizer is to be applied only to the lesions, but due to the phenomenon of field cancerization, many doctors are using broad facial applications. For broad area application, incubation period should be less than an hour in order to prevent a phototoxic reaction 66. Methyl aminolevulinate (MAL) is approved with an incubation period of 3 hours under occlusion with 37 J/cm² or 75 J/cm² of red light. A single therapy session is approved in Europe, with repeated sessions after three months for non-responsive/incompletely responsive lesions. Two therapy sessions using methyl aminolevulinate (MAL) instituted seven days apart are approved by the FDA.
- Basal Cell Carcinoma (BCC): Methyl aminolevulinate (MAL) photodynamic therapy is also approved for the treatment of basal cell carcinoma in Europe.
- Bowen disease also known as squamous cell carcinoma in situ, is an early form of skin cancer where abnormal cells are found in the top layer of the skin, the epidermis. It is considered a pre-cancerous condition and appears as a slow-growing, red, scaly patch on the skin, often resembling other skin conditions like eczema or psoriasis: Methyl aminolevulinate (MAL) photodynamic therapy is also approved for the treatment of Bowen disease in Europe.
Photodynamic therapy (PDT) Off-label Indications 67:
- Premalignant and malignant skin conditions: Nevoid BCC syndrome (Gorlin syndrome), actinic cheilitis, disseminated superficial actinic porokeratosis, keratoacanthoma, Kaposi sarcoma, cutaneous T-cell lymphoma, cutaneous metastasis.
- Inflammatory skin disorders: psoriasis, acne vulgaris, scleroderma, lichen sclerosis, alopecia areata.
- Skin infections: Prevention of MRSA infection, leishmaniasis, tinea pedis, HPV infections/ dermatosis (verruca vulgaris, condylomata, epidermodysplasia verruciformis), molluscum contagiosum.
- Aging and photorejuvenation: Photodynamic therapy (PDT) has been reported to stimulate the production of type 1 and type 3 procollagen and hence augment dermal remodeling.
- Tumor prevention.
To date, there’s a lot of ongoing research, publication of small studies and much discussion on the internet about the effectiveness of red light therapy for all types of health uses. Results of some studies do show some promise, but the full effectiveness of red light therapy has yet to be determined. What’s confusing — and controversial — is the effectiveness of the red light therapy for the purposes it’s being promoted.
Red light therapy is thought to work by acting on the “power plant” in your body’s cells called mitochondria. With more energy, other cells can do their work more efficiently, doing things like repairing skin, boosting new cell growth and enhancing skin rejuvenation. More specifically, certain cells absorb light wavelengths and are stimulated to work.
Most experts say that they don’t know yet if red light therapy is effective for all its claimed uses. Most say that the studies published so far show some potential for certain conditions, but that more studies need to be conducted. Red light therapy is still an emerging treatment that’s generating growing interest. But at this point in time, there’s not enough evidence to support most uses.
The gold standard of studies to determine if a product is effective is a randomized, placebo-controlled trial. This means that a certain number of people with the same range of characteristics (age, weight, race, sex, etc.) get either the study treatment or a placebo (fake or “sham” treatment) for treatment of the same condition.
Some studies also include a comparison to another commonly used treatment. Results can then be compared between the emerging treatment versus no treatment (the placebo group) or versus a “current standard” treatment.
Many of the published studies using red light therapy included only a small number of people, didn’t include a placebo group, weren’t conducted in humans (animal studies) or were limited to cell tissue itself. Most researchers say results so far look promising, but that more quality studies with larger numbers of people are needed.
Red light therapy may work in skin health to 39, 40, 41:
- Stimulate collagen production, which gives skin its structure, strength and elasticity.
- Increase fibroblast production, which makes collagen. Collagen is a component of connective tissue that builds skin.
- Increase blood circulation to the tissue.
- Reduce inflammation in cells.
Animal studies have shown that red light irradiation enhances mitochondrial catalase activity, which improves cell metabolism and leads to increased glycogen and protein biosynthesis. These changes promote cell growth and wound healing 42, 43.
Red light therapy is promoted as a treatment for some common skin conditions to 44:
- Improve wound healing.
- Reduce stretch marks.
- Reduce wrinkles, fine lines and age spots.
- Improve facial texture.
- Improve psoriasis, rosacea and eczema.
- Improve scars.
- Improve sun-damaged skin.
- Improve hair growth in people with androgenic alopecia.
- Improve acne.
Red light therapy to treat acne
Red light (wavelength in the range 600–650 nm) therapy reduces the activity of acne by accelerating wound healing and reducing the inflammatory response 5, 68, 2, 69, 70, 2, 71. Red light (600–650 nm) activates porphyrins with less intensity than blue light. Porphyrins are a group of naturally occurring cyclic organic compounds characterized by a specific ring structure composed of four modified pyrrole subunits connected by methine bridges that are essential for life, because of their key role in processes related to oxygen production, oxygen transport, oxygen use and various redox reactions 72. Porphyrins are crucial for various biological processes, particularly as components of hemoproteins like hemoglobin (the protein that carries oxygen in the blood). Red light (wavelength in the range 600–650 nm) have the deepest tissue penetration of the visible wavelengths and it penetrates the skin 1 to 2 mm deeper than blue light (wavelength in the range 400 to 545 nm) 73, 74. Blue light therapy has wavelengths 400 nm to 545 nm and penetrates approximately 0.3 mm into the skin and has a maximal penetration of up to 1 mm 39. Blue light therapy is best suited for the treatment of more superficial skin conditions, such as actinic keratosis (a precancerous skin condition characterized by rough, scaly patches on sun-exposed skin) or to target Propionibacterium acnes (a Gram-positive human skin commensal bacteria that prefers anaerobic growth conditions and is involved in the pathogenesis of acne) in acne 75, 76, 77. Although blue light has a somewhat limited depth of skin penetration, it is the most effective visible wavelength for treating Propionibacterium acnes bacteria because it produces the strongest photoactivation of endogenous porphyrins 75, 76. In addition to deeper penetration, red light also has anti-inflammatory effects and is beneficial for the treatment of inflammatory acne lesions 8, 7. Therefore, for acne treatment greater clinical improvement is associated with combined red and blue light therapy 78.
There are several reports that showed combination of blue and red light could obtain better result than monotherapy with red light 79, 80, 81. In comparison with blue light (415 nm), red light (660 nm) penetrates more deeply in tissue. In addition, it has been shown that red light can affect the sebum secretion of sebaceous glands (small gland in the skin which secretes a lubricating oily matter called sebum into the hair follicles to lubricate the skin and hair) and keratinocyte behaviors 82. Red light has less effectiveness on activation of Propionibacterium acnes (a Gram-positive human skin commensal bacteria that prefers anaerobic growth conditions and is involved in the pathogenesis of acne) porphyrin and it does not seem that the beneficial effect of red low-level laser therapy is related to photodynamic reactions 71. Low-level red light therapy using red light-emitting diode (LED) treatments also has anti-inflammatory properties through its influence on cytokine production by macrophages and by reducing inflammatory mediator expression from macrophages and causing a reduction in neutrophils, interleukins, and matrix metalloproteinase in acne animal models and has been shown to be beneficial for the treatment of inflammatory acne lesions 8, 82, 68. Red light may also inhibit keratinization (the process where epidermal cells, keratinocytes, change into tough, protective structures like hair, nails, and the outer layer of skin) and reduce skin barrier damage 83. Keratinization is crucial for maintaining a healthy skin barrier and protecting the body from external factors 84.
Light-emitting diode (LED) consist a semiconductor chip situated upon a reflective surface. Light is produced when electricity is run through the semiconductor. The wavelength of light produced is dependent on the composition of the semiconductor chip. Depth of tissue penetration, and therefore the light’s target, is primarily dependent upon the wavelength of the light.
Morton et al treated 30 patients with mild-to-moderate acne with 8-, 10-, or 20-minute blue light-emitting diode (LED) (415nm) treatments over a period of four weeks 85. Mean inflammatory lesion counts decreased at weeks 5, 8, and 12 by 25, 53, and 60 percent, respectively, with minimal effect on noninflammatory lesions 85. Tremblay et al 86 gave patients with mild-to-moderate inflammatory acne two 20-minute treatments of blue LED (415nm) per week for 4 to 8 weeks. Ninety percent of patients were satisfied with the result 86. Patients had a 50-percent reduction in lesion counts and nine patients were completely clear 86. Two similar clinical studies showed reductions in lesion size, number, and skin redness in patients as evaluated by physician and patients after treatment with blue LED 87, 88. Although blue light has been tried in combination with aminolevulinic acid in the treatment of acne of 20 patients, patients experienced greater side effects and the results were not clinically significant when compared with blue LED alone 89. Recently, blue LED has also shown promise in the treatment of thicker lesions such as psoriasis. A 2011 prospective, randomized study of 37 patients showed statistically significant improvement of irradiated psoriatic plaques after four weeks of treatment with an at-home LED-based on the Local Psoriasis Severity Index (LPSI) 90.
The results of this study 78 compare favorably with other studies, which used blue (415nm) with red (633nm) LEDs 91, 92, 93, blue (420nm) with red (660nm) LEDs 94, and blue (415nm) with red (660nm) LEDs 95. Two eight-week studies reported 34.28 and 77.93 percent improvements in noninflammatory and inflammatory acne lesions, respectively 92, and 48.8-percent improvements in noninflammatory acne lesions 91. Three 12-week studies reported 54 and 77-percent improvements in noninflammatory and inflammatory acne lesions, respectively 94, and overall improvements of 76 percent 95 and 81 percent 93. One other comparative study also reported that blue/red light therapy was superior to 5% topical benzoyl peroxide cream 95. It should be noted that most of these studies were small, enrolling only 17 to 35 subjects and these studies were required to expose treated subjects with blue and red light sequentially from different light sources.
Several devices that employ blue light-emitting diodes (LEDs) have been developed for the treatment of acne, which have a beneficial effect on acne lesions 96, 97, 88, 98, 99. In addition, studies have shown the use of combined red and blue light is also very effective 91, 100. The results of a randomized, double-blind, sham-controlled study indicate the addition of red light results in significant improvements in both inflammatory and noninflammatory acne lesions 94.
Home light therapy devices consist of wearable masks that use low-level light therapy as an light-emitting diode (LED) that emit both 445nm blue and 630nm red light, non-thermal, non-ablative treatment 83. Designed to be worn as a mask, it provides full-face treatment during each daily 15-minute light therapy session (illuMask® Acne Light Therapy Mask; La Lumiere, LLC, Cleveland, Ohio).
Currently approved devices on the market use both blue and red light and are approved for mild to moderate facial acne 83. Combination red and blue light therapy device uses low-level light therapy in both blue (415 nm) and red (650 nm) wavelengths 83. Multiple studies have shown it is well tolerated and effective through a reduction in inflammatory and non-inflammatory acne lesions and is superior to blue light alone 1, 101. The mechanism is thought to be synergistic in applying the antibacterial and anti-inflammatory actions of both blue (415 nm) and red (650 nm) wavelengths of light acting at different depths within the skin. Blue and red light is safe in pregnancy. Some patients may experience a deterioration of their acne with blue and red light therapy, and its side effects can include dryness, itch, a rash, and headaches.
Home light therapy devices are typically smaller than in-office LED devices and may require extended treatment sessions for a therapeutic effect 83. Home light therapy devices have been shown to reduce inflammatory and non-inflammatory acne lesion counts and reduce the size and sebum production of sebaceous glands 102. A recent clinical trial compared a blue and red light therapy mask with and without topical salicylic acid against topical benzoyl peroxide for mild to moderate acne 78. The trial found a 24.4% improvement in inflammatory lesions and 19.5% improvement in non-inflammatory lesions in patients using the light mask, concluding this to be a safe and effective therapy for mild to moderate acne 78.
Figure 3. Acne Light Therapy Mask


Footnotes: Red and blue light mask to treat acne.
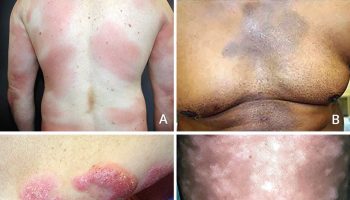
Figure 4. Acne treated by red low-level laser therapy

Footnotes: Acne treated by red low-level laser therapy in the red spectral range (630 nm) at baseline (a), after 6 weeks (b), and (c) after 10 weeks. There was not any significant reduction of active lesions count in patients treated with 890-nm low-level laser therapy. It seems that low-level laser therapy in red spectrum is a safe therapeutic modality in treating facial acne without any complication.
[Source 71 ]Risks and dangers of red light therapy
Red light therapy appears to be safe and isn’t associated with any side effects, if used short-term on your skin and as directed. Red light therapy isn’t toxic, not invasive and not as harsh as some topical skin treatments. Unlike the cancer-causing ultraviolet (UV) light from the sun or tanning booths, red light therapy doesn’t use this type of light therefore it does not usually cause permanent damage to your skin or your increase risk of skin cancers. However, there are side effects of red light therapy that you should be aware of. High levels of red light can cause redness, swelling, and blistering your skin. Red light can also damage to your eyes, so it is important to wear protective goggles when using red light therapy. If you have a history of skin or eye cancers, it is important to consult your oncologist (cancer specialist) or your family doctor before using red light therapy. The long-term safety of devices that use red light therapy isn’t yet known.
Your safest option is to see a dermatologist or qualified, trained, cosmetic therapist. A dermatologist can make sure your skin condition is what you think it is and can discuss the merits of red light therapy and other treatment options.
A recent study in the U.S. suggested that red light therapy with several available red light instruments (the Sky-n1201a and the Future Vision Class 1 laser products) could cause retinal damage 32. One published case study of a 12 year old girl who sustained retinal damage after 5-month application of repeated low-level red-light therapy 33. In this case, the child’s best corrected visual acuity decreased from 6/6 to 6/9 33. Fundus photos revealed bilaterally darkened foveae with a hypoautofluorescent plaque in autofluorescence images 33. Optical coherence tomography (OCT) imaging showed bilateral foveal ellipsoid zone disruption and interdigitation zone discontinuity 33. Multifocal electroretinography revealed moderately and mildly decreased responses in the macula and paramacula, respectively 33. Visual acuity improved to 6/7.5 three months after low-level red-light therapy was terminated 33. In this cohort study, among 52 children using repeated low-level red-light therapy for over 1 year compared with 47 nonusers, repeated low-level red-light therapy users showed lower cone density, particularly within 0.5 mm from the retinal fovea, with abnormal drusenlike lesions detected in some of these cases 34. These findings suggest that repeated low-level red-light therapy may be associated with cellular-level retinal changes in macular cone cells, highlighting the importance of further studies assessing its safety for young patients with nearsightedness (myopia), especially with long-term exposure 34. Low-level red-light therapy “may exceed tissue tolerance limits, causing unexpected ganglion cell layer damage”, the authors of the study wrote 34. Although low-level red-light therapy “might control the progression of myopia, further studies are needed to provide more definitive information regarding longer-term efficacy and safety” they added 34. These new study suggests low-level red-light therapy “may have subtle effects on cone density that are not readily visualized with standard clinical tests” wrote Jacque Duncan, MD, of the University of California San Francisco, in a commentary on the paper 35. These researchers warned doctors about using red light therapy to treat nearsightedness (myopia) with caution until safety standards can be confirmed 33, 32, 34, 36, 37. Lisa Ostrin and Alexander Schill, a University of Houston optometry researchers are warning against the use of low-level red light therapy as a method to control myopia, or nearsightedness, especially in children 32. The 3-minute protocol for low level red light therapy to treat nearsightedness (myopia) may put the retina at risk for photochemical and thermal damage 32. “Thermal ocular injury from a laser can occur with exposures at any wavelength when the temperature change of the retina is greater than 10° C, resulting in denaturation of proteins. With thermal damage, the lesion is typically less than the size of the beam diameter, and the resultant scotomas are permanent” 32. “In conclusion, based on measurements in our laboratory, it is recommended that clinicians strongly reconsider the use of LLRL therapy for myopia in children until safety standards can be confirmed” 32. Laura Enyedi, a pediatric ophthalmologist at the Duke Eye Center in North Carolina stated that “there simply is not enough information to assess the safety of red light therapy, and the devices available in the US are not regulated and could damage your child’s retina, leading to loss of vision. Right now, your best option is to make some simple changes for your child such as reducing screen time, increasing outdoor time for your child, and asking your child’s ophthalmologist about other potential solutions, such as low-dose atropine eye drops or special contact lenses which are approved by the FDA” 38.
- Guffey JS, Wilborn J. In vitro bactericidal effects of 405-nm and 470-nm blue light. Photomed Laser Surg. 2006 Dec;24(6):684-8. doi: 10.1089/pho.2006.24.684[↩][↩]
- Ross EV. Optical treatments for acne. Dermatol Ther. 2005 May-Jun;18(3):253-66. doi: 10.1111/j.1529-8019.2005.05024.x[↩][↩][↩]
- Tafur J, Mills PJ. Low-intensity light therapy: exploring the role of redox mechanisms. Photomed Laser Surg. 2008 Aug;26(4):323-8. doi: 10.1089/pho.2007.2184[↩]
- Chaves ME, Araújo AR, Piancastelli AC, Pinotti M. Effects of low-power light therapy on wound healing: LASER x LED. An Bras Dermatol. 2014 Jul-Aug;89(4):616-23. doi: 10.1590/abd1806-4841.20142519[↩]
- Cunliffe WJ, Goulden V. Phototherapy and acne vulgaris. Br J Dermatol. 2000 May;142(5):855-6. doi: 10.1046/j.1365-2133.2000.03528.x[↩][↩]
- Eells J.T., Wong-Riley M.T., VerHoeve J., Henry M., Buchman E.V., Kane M.P., Gould L.J., Das R., Jett M., Hodgson B.D., et al. Mitochondrial signal transduction in accelerated wound and retinal healing by near-infrared light therapy. Mitochondrion. 2004;4:559–567. doi: 10.1016/j.mito.2004.07.033[↩][↩][↩]
- Young S, Bolton P, Dyson M, et al. Macrophage responsiveness to light therapy. Lasers Surg Med. 1989;9:497–505. doi: 10.1002/lsm.1900090513[↩][↩]
- Aziz-Jalali MH, Tabaie SM, Djavid GE. Comparison of red and infrared low-level laser therapy in the treatment of acne vulgaris. Indian J Dermatol. 2012;57:128–130. doi: 10.4103/0019-5154.94283[↩][↩][↩]
- Tang J, Liao Y, Yan N, Dereje SB, Wang J, Luo Y, Wang Y, Zhou W, Wang X, Wang W. Efficacy of Repeated Low-Level Red-Light Therapy for Slowing the Progression of Childhood Myopia: A Systematic Review and Meta-analysis. Am J Ophthalmol. 2023 Aug;252:153-163. doi: 10.1016/j.ajo.2023.03.036[↩][↩]
- Xiong R, Zhu Z, Jiang Y, Kong X, Zhang J, Wang W, Kiburg K, Yuan Y, Chen Y, Zhang S, Xuan M, Zeng J, Morgan IG, He M. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clin Exp Ophthalmol. 2022 Dec;50(9):1013-1024. doi: 10.1111/ceo.14149[↩]
- AlGhamdi KM, Kumar A, Moussa NA. Low-level laser therapy: a useful technique for enhancing the proliferation of various cultured cells. Lasers Med Sci. 2012 Jan;27(1):237-49. doi: 10.1007/s10103-011-0885-2[↩]
- Xiong F, Mao T, Liao H, Hu X, Shang L, Yu L, Lin N, Huang L, Yi Y, Zhou R, Zhou X, Yi J. Orthokeratology and Low-Intensity Laser Therapy for Slowing the Progression of Myopia in Children. Biomed Res Int. 2021 Jan 27;2021:8915867. doi: 10.1155/2021/8915867[↩][↩]
- Zhou L, Xing C, Qiang W, Hua C, Tong L. Low-intensity, long-wavelength red light slows the progression of myopia in children: an Eastern China-based cohort. Ophthalmic Physiol Opt. 2022 Mar;42(2):335-344. doi: 10.1111/opo.12939[↩][↩]
- Jiang Y, Zhu Z, Tan X, Kong X, Zhong H, Zhang J, Xiong R, Yuan Y, Zeng J, Morgan IG, He M. Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children: A Multicenter Randomized Controlled Trial. Ophthalmology. 2022 May;129(5):509-519. https://www.aaojournal.org/article/S0161-6420(21)00916-7/fulltext[↩][↩]
- Amaral DC, Batista S, Dos Santos-Neto E, Manso JEF, Rodrigues MPM, Monteiro MLR, Alves MR, Louzada RN. Low-level red-light therapy for myopia control in children: A systematic review and meta-analysis. Clinics (Sao Paulo). 2024 May 8;79:100375. doi: 10.1016/j.clinsp.2024.100375[↩]
- Wang W, Jiang Y, Zhu Z, Zhang S, Xuan M, Tan X, Kong X, Zhong H, Bulloch G, Xiong R, Yuan Y, Chen Y, Zhang J, Zeng J, Morgan IG, He M. Axial Shortening in Myopic Children after Repeated Low-Level Red-Light Therapy: Post Hoc Analysis of a Randomized Trial. Ophthalmol Ther. 2023 Apr;12(2):1223-1237. doi: 10.1007/s40123-023-00671-7[↩]
- Zhou L, Tong L, Li Y, Williams BT, Qiu K. Photobiomodulation therapy retarded axial length growth in children with myopia: evidence from a 12-month randomized controlled trial evidence. Sci Rep. 2023 Feb 27;13(1):3321. doi: 10.1038/s41598-023-30500-7[↩]
- Chang DJ, P L S, Jeong J, Saw SM, Sevdalis N, Najjar RP. Light Therapy for Myopia Prevention and Control: A Systematic Review on Effectiveness, Safety, and Implementation. Transl Vis Sci Technol. 2024 Aug 1;13(8):31. doi: 10.1167/tvst.13.8.31[↩]
- Dong J, Zhu Z, Xu H, He M. Myopia Control Effect of Repeated Low-Level Red-Light Therapy in Chinese Children: A Randomized, Double-Blind, Controlled Clinical Trial. Ophthalmology. 2023 Feb;130(2):198-204. https://www.aaojournal.org/article/S0161-6420(22)00669-8/fulltext[↩]
- Jiang Y, Zhu Z, Tan X, Kong X, Zhong H, Zhang J, Xiong R, Yuan Y, Zeng J, Morgan IG, He M. Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children: A Multicenter Randomized Controlled Trial. Ophthalmology. 2022 May;129(5):509-519. https://www.aaojournal.org/article/S0161-6420(21)00916-7/fulltex[↩]
- Dong J, Zhu Z, Xu H, He M. Myopia Control Effect of Repeated Low-Level Red-Light Therapy in Chinese Children: A Randomized, Double-Blind, Controlled Clinical Trial. Ophthalmology. 2023 Feb;130(2):198-204. https://www.aaojournal.org/article/S0161-6420(24)00318-X/fulltext[↩][↩][↩][↩]
- Lin ZH, Tao ZY, Kang ZF, Deng HW. A Study on the Effectiveness of 650-nm Red-Light Feeding Instruments in the Control of Myopia. Ophthalmic Res. 2023;66(1):664-671. doi: 10.1159/000529819[↩]
- Xuan M, Zhu Z, Jiang Y, Wang W, Zhang J, Xiong R, Shi D, Bulloch G, Zeng J, He M. Longitudinal Changes in Choroidal Structure Following Repeated Low-Level Red-Light Therapy for Myopia Control: Secondary Analysis of a Randomized Controlled Trial. Asia Pac J Ophthalmol (Phila). 2023 Jul-Aug 01;12(4):377-383. doi: 10.1097/APO.0000000000000618[↩]
- He X, Wang J, Zhu Z, Xiang K, Zhang X, Zhang B, Chen J, Yang J, Du L, Niu C, Leng M, Huang J, Liu K, Zou H, He M, Xu X. Effect of Repeated Low-level Red Light on Myopia Prevention Among Children in China With Premyopia: A Randomized Clinical Trial. JAMA Netw Open. 2023 Apr 3;6(4):e239612. doi: 10.1001/jamanetworkopen.2023.9612. Erratum in: JAMA Netw Open. 2023 Sep 5;6(9):e2337652. doi: 10.1001/jamanetworkopen.2023.37652[↩]
- Yang W, Lin F, Li M, Wei R, Zhou J, Zhou X. Immediate Effect in the Retina and Choroid after 650 nm Low-Level Red Light Therapy in Children. Ophthalmic Res. 2023;66(1):312-318. doi: 10.1159/000527787[↩]
- Liu G, Li B, Rong H, Du B, Wang B, Hu J, Zhang B, Wei R. Axial Length Shortening and Choroid Thickening in Myopic Adults Treated with Repeated Low-Level Red Light. J Clin Med. 2022 Dec 17;11(24):7498. doi: 10.3390/jcm11247498[↩]
- Zhao C, Ni Y, Zeng J. Effect of red-light therapy on retinal and choroidal blood perfusion in myopic children. Ophthalmic Physiol Opt. 2023 Nov;43(6):1427-1437. doi: 10.1111/opo.13202[↩]
- Tian L, Cao K, Ma DL, Zhao SQ, Lu LX, Li A, Chen CX, Ma CR, Ma ZF, Jie Y. Investigation of the Efficacy and Safety of 650 nm Low-Level Red Light for Myopia Control in Children: A Randomized Controlled Trial. Ophthalmol Ther. 2022 Dec;11(6):2259-2270. doi: 10.1007/s40123-022-00585-w[↩]
- Chen Y, Xiong R, Chen X, Zhang J, Bulloch G, Lin X, Wu X, Li J. Efficacy Comparison of Repeated Low-Level Red Light and Low-Dose Atropine for Myopia Control: A Randomized Controlled Trial. Transl Vis Sci Technol. 2022 Oct 3;11(10):33. doi: 10.1167/tvst.11.10.33[↩]
- Zhu Q, Cao X, Zhang Y, Zhou Y, Zhang J, Zhang X, Zhu Y, Xue L. Repeated Low-Level Red-Light Therapy for Controlling Onset and Progression of Myopia-a Review. Int J Med Sci. 2023 Sep 4;20(10):1363-1376. doi: 10.7150/ijms.85746[↩]
- Wang F, Peng W, Jiang Z. Repeated Low-Level Red Light Therapy for the Control of Myopia in Children: A Meta-Analysis of Randomized Controlled Trials. Eye Contact Lens. 2023 Oct 1;49(10):438-446. doi: 10.1097/ICL.0000000000001020[↩]
- Ostrin LA, Schill AW. Red light instruments for myopia exceed safety limits. Ophthalmic Physiol Opt. 2024 Mar;44(2):241-248. doi: 10.1111/opo.13272[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Liu H, Yang Y, Guo J, Peng J, Zhao P. Retinal Damage After Repeated Low-level Red-Light Laser Exposure. JAMA Ophthalmol. 2023;141(7):693–695. doi:10.1001/jamaophthalmol.2023.1548[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Liao X, Yu J, Fan Y, et al. Cone Density Changes After Repeated Low-Level Red Light Treatment in Children With Myopia. JAMA Ophthalmol. 2025;143(6):480–488. doi:10.1001/jamaophthalmol.2025.0835[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Red-Light Therapy May Reduce Cone Density in Myopic Children. https://www.medscape.com/viewarticle/red-light-therapy-may-reduce-cone-density-myopic-children-2025a1000a5c[↩][↩]
- Lawrenson JG, Huntjens B, Virgili G, Ng S, Dhakal R, Downie LE, Verkicharla PK, Kernohan A, Li T, Walline JJ. Interventions for myopia control in children: a living systematic review and network meta‐analysis. Cochrane Database of Systematic Reviews 2025, Issue 2. Art. No.: CD014758. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD014758.pub3/epdf/full[↩][↩]
- Schaeffel F, Wildsoet CF. Red light therapy for myopia: Merits, risks and questions. Ophthalmic Physiol Opt. 2024 Jul;44(5):801-807. doi: 10.1111/opo.13306[↩][↩]
- Can Red Light Therapy Slow Nearsightedness in Children? https://www.aao.org/eye-health/news/red-light-therapy-nearsightedness-myopia-children[↩][↩]
- Barolet DB. Light-emitting diodes (LEDs) in dermatology. Semin Cutan Med Surg. 2008;27:227–238. doi: 10.1016/j.sder.2008.08.003[↩][↩][↩]
- Barolet D, Roberge C, Auger F, et al. Regulation of skin collagen metabolism in vitro using a pulsed 660 nm LED light source: clinical correlation with a single-blinded study. J Invest Dermatol. 2009;129:2751–2759. doi: 10.1038/jid.2009.186[↩][↩]
- Almeida Issa MC, Piñeiro-Maceira J, et al. Immunohistochemical expression of matrix metalloproteinases in photodamaged skin by photodynamic therapy. Br J Dermatol. 2009;161:647–653. doi: 10.1111/j.1365-2133.2009.09326.x[↩][↩]
- Holder MJ, Milward MR, Palin WM, Hadis MA, Cooper PR. Effects of red light-emitting diode irradiation on dental pulp cells. J Dent Res. 2012 Oct;91(10):961-6. doi: 10.1177/0022034512456040[↩][↩]
- Reddy GK, Stehno-Bittel L, Enwemeka CS. Laser photostimulation accelerates wound healing in diabetic rats. Wound Repair Regen. 2001 May-Jun;9(3):248-55. doi: 10.1046/j.1524-475x.2001.00248.x[↩][↩]
- Niu T, Tian Y, Ren Q, Wei L, Li X, Cai Q. Red light interferes in UVA-induced photoaging of human skin fibroblast cells. Photochem Photobiol. 2014 Nov-Dec;90(6):1349-58. doi: 10.1111/php.12316[↩][↩]
- Whelan HT, Connelly JF, Hodgson BD, et al. NASA light-emitting diodes for the prevention of oral mucositis in pediatric bone marrow transplant patients. J Clin Laser Med Surg. 2002;20:319–324. doi: 10.1089/104454702320901107[↩]
- Corti L, Chiaron-Sileni V, Aversa S, et al. Treatment of chemotherapy-induced oral mucositis with light-emitting diode. Photomed Laser Surg. 2006;24:207–213. doi: 10.1089/pho.2006.24.207[↩]
- Shi HJ, Song H, Zhao QY, Tao CX, Liu M, Zhu QQ. Efficacy and safety of combined high-dose interferon and red light therapy for the treatment of human papillomavirus and associated vaginitis and cervicitis: A prospective and randomized clinical study. Medicine (Baltimore). 2018 Sep;97(37):e12398. doi: 10.1097/MD.0000000000012398[↩][↩]
- Shi H, Zhang X, Ma C, Yu N, Wang J, Xia L, Ge X, Liu M, Duan A. Clinical analysis of five methods used to treat condylomata acuminata. Dermatology. 2013;227(4):338-45. doi: 10.1159/000355351[↩]
- Bais B, Kamperman AM, Bijma HH, Hoogendijk WJ, Souman JL, Knijff E, Lambregtse-van den Berg MP. Effects of bright light therapy for depression during pregnancy: a randomised, double-blind controlled trial. BMJ Open. 2020 Oct 28;10(10):e038030. doi: 10.1136/bmjopen-2020-038030[↩]
- Al-Quisi AF, Al-Anee AM, Al-Jumaily HA, Bahr EF, Finjan DA. Efficacy of the LED Red Light Therapy in the Treatment of Temporomandibular Disorders: Double Blind Randomized Controlled Trial. Pain Res Treat. 2019 May 6;2019:8578703. doi: 10.1155/2019/8578703[↩]
- Aebisher D, Rogóż K, Myśliwiec A, Dynarowicz K, Wiench R, Cieślar G, Kawczyk-Krupka A, Bartusik-Aebisher D. The use of photodynamic therapy in medical practice. Front Oncol. 2024 May 8;14:1373263. doi: 10.3389/fonc.2024.1373263[↩]
- Gunaydin G, Gedik ME, Ayan S. Photodynamic Therapy for the Treatment and Diagnosis of Cancer-A Review of the Current Clinical Status. Front Chem. 2021 Aug 2;9:686303. doi: 10.3389/fchem.2021.686303[↩]
- Domka W, Bartusik-Aebisher D, Mytych W, Myśliwiec A, Dynarowicz K, Cieślar G, Kawczyk-Krupka A, Aebisher D. Photodynamic Therapy for Eye, Ear, Laryngeal Area, and Nasal and Oral Cavity Diseases: A Review. Cancers (Basel). 2024 Feb 2;16(3):645. doi: 10.3390/cancers16030645[↩]
- Wang L, Chen Q, Liu D. Development of photodynamic therapy in treating oral diseases. Front Oral Health. 2025 Jan 15;5:1506407. doi: 10.3389/froh.2024.1506407[↩]
- Huis In ‘t Veld RV, Heuts J, Ma S, Cruz LJ, Ossendorp FA, Jager MJ. Current Challenges and Opportunities of Photodynamic Therapy against Cancer. Pharmaceutics. 2023 Jan 18;15(2):330. doi: 10.3390/pharmaceutics15020330[↩]
- Photodynamic Therapy to Treat Cancer. https://www.cancer.gov/about-cancer/treatment/types/photodynamic-therapy[↩]
- Photodynamic Therapy (PDT) for skin cancer. https://www.cancerresearchuk.org/about-cancer/skin-cancer/treatment/photodynamic-therapy[↩]
- Daniels P, Muse ME, Jaskolka M, et al. Treatment of Cutaneous Malignancies With Topical, Oral, and Injectable Medication. [Updated 2025 May 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK614161[↩]
- Photodynamic therapy. https://dermnetnz.org/topics/photodynamic-therapy[↩]
- Thiboutot DM, Dréno B, Abanmi A, Alexis AF, et al. Practical management of acne for clinicians: An international consensus from the Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2018 Feb;78(2 Suppl 1):S1-S23.e1. doi: 10.1016/j.jaad.2017.09.078[↩]
- Barolet D, Boucher A. LED photoprevention: reduced MED response following multiple LED exposures. Lasers Surg Med. 2008;40:106–112. doi: 10.1002/lsm.20615[↩]
- Wong TW, Sheu HM, Lee JY, Fletcher RJ. Photodynamic therapy for Bowen’s disease (squamous cell carcinoma in situ) of the digit. Dermatol Surg. 2001;27:452–456. doi: 10.1046/j.1524-4725.2001.00187.x[↩]
- Lopez N, Meyer-Gonzalez T, Herrera-Acosta E, et al. Photodynamic therapy in the treatment of extensive Bowen’s disease. J Dermatolog Treat. 2012;23:428–430. doi: 10.3109/09546634.2011.590789[↩]
- Calin MA, Diaconeasa A, Savastru D, Tautan M. Photosensitizers and light sources for photodynamic therapy of the Bowen’s disease. Arch Dermatol Res. 2011;303:145–151. doi: 10.1007/s00403-011-1122-3[↩]
- Baas P, Saarnak AE, Oppelaar H, et al. Photodynamic therapy with meta-tetrahydroxyphenylchlorin for basal cell carcinoma: a phase I/II study. Br J Dermatol. 2001;145:75–78. doi: 10.1046/j.1365-2133.2001.04284.x[↩]
- Raizada K, Naik M. Photodynamic Therapy for the Eye. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560686[↩][↩][↩]
- Nguyen K, Khachemoune A. An update on topical photodynamic therapy for clinical dermatologists. J Dermatolog Treat. 2019 Dec;30(8):732-744. doi: 10.1080/09546634.2019.1569752[↩]
- Young S, Bolton P, Dyson M, Harvey W, Diamantopoulos C. Macrophage responsiveness to light therapy. Lasers Surg Med. 1989;9(5):497-505. doi: 10.1002/lsm.1900090513[↩][↩]
- Opel DR, Hagstrom E, Pace AK, Sisto K, Hirano-Ali SA, Desai S, Swan J. Light-emitting Diodes: A Brief Review and Clinical Experience. J Clin Aesthet Dermatol. 2015 Jun;8(6):36-44. https://pmc.ncbi.nlm.nih.gov/articles/PMC4479368[↩]
- Barolet D. Light-emitting diodes (LEDs) in dermatology. Semin Cutan Med Surg. 2008 Dec;27(4):227-38. doi: 10.1016/j.sder.2008.08.003[↩]
- Aziz-Jalali MH, Tabaie SM, Djavid GE. Comparison of Red and Infrared Low-level Laser Therapy in the Treatment of Acne Vulgaris. Indian J Dermatol. 2012 Mar;57(2):128-30. doi: 10.4103/0019-5154.94283[↩][↩][↩]
- Porphyrin. https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/porphyrin[↩]
- Momen S, Al-Niaimi F. Acne vulgaris and light-based therapies. J Cosmet Laser Ther. 2015 Jun;17(3):122-8. doi: 10.3109/14764172.2014.988727[↩]
- Simpson CR, Kohl M, Essenpreis M, et al. Near infrared optical properties of ex-vivo human skin and subcutaneous tissues measured using the Monte Carlo inversion technique. Phys Med Biol. 1998;43:2465–2478. doi: 10.1088/0031-9155/43/9/003[↩]
- Ashkenazi H, Malik Z, Harth Y, et al. Eradication of Propionibacterium acnes by its endogenic porphyrins after illumination with high intensity blue light. FEMS Immunol Med Microbiol. 2003;35:17–24. doi: 10.1111/j.1574-695X.2003.tb00644.x[↩][↩]
- Melo TB. Uptake of protoporphyrin and violet light photodestruction of Propionibacterium acnes. Z Naturforsch C. 1987;42:123–128. doi: 10.1515/znc-1987-1-220[↩][↩]
- Fitz-Gibbon S, Tomida S, Chiu BH, et al. Propionibacterium acnes strain populations in the human skin microbiome associated with acne. J Invest Dermatol. 2013;133:2152–2160. doi: 10.1038/jid.2013.21[↩]
- Nestor MS, Swenson N, Macri A, Manway M, Paparone P. Efficacy and Tolerability of a Combined 445nm and 630nm Over-the-counter Light Therapy Mask with and without Topical Salicylic Acid versus Topical Benzoyl Peroxide for the Treatment of Mild-to-moderate Acne Vulgaris. J Clin Aesthet Dermatol. 2016 Mar;9(3):25-35. https://pmc.ncbi.nlm.nih.gov/articles/PMC4896818[↩][↩][↩][↩]
- Goldberg DJ, Russell BA. Combination blue (415 nm) and red (633 nm) LED phototherapy in the treatment of mild to severe acne vulgaris. J Cosmet Laser Ther. 2008;8:71–5. doi: 10.1080/14764170600735912[↩]
- Lee SY, You CE, Park MY. Blue and red light combination LED phototherapy for acne vulgaris in patients with skin phototype IV. Lasers Surg Med. 2007;39:180–8. doi: 10.1002/lsm.20412[↩]
- Papageorgiou P, Katsambas A, Chu A. Phototherapy with blue (415 nm) and red (660 nm) light in the treatment of acne vulgaris. Br J Dermatol. 2000;142:973–8. doi: 10.1046/j.1365-2133.2000.03481.x[↩]
- Sadick NS. Handheld LED array device in the treatment of acne vulgaris. J Drugs Dermatol. 2008 Apr;7(4):347-50.[↩][↩]
- Lasers, lights, and acne. https://dermnetnz.org/topics/lasers-lights-and-acne[↩][↩][↩][↩][↩]
- Shetty S; Gokul S. Keratinization and its disorders. Oman Med J. 2012 Sep;27(5):348-57. doi: 10.5001/omj.2012.90[↩]
- Morton CA, Scholefield RD, Whitehurst C, Birch J. An open study to determine the efficacy of blue light in the treatment of mild to moderate acne. J Dermatol Treat. 2005;16:219–223. doi: 10.1080/09546630500283664[↩][↩]
- Tremblay JF, Sire DJ, Lowe NJ, Moy RL. Light-emitting diode 415 nm in the treatment of inflammatory acne: an open-label, multicentric, pilot investigation. J Gosmet Laser Ther. 2006;8:31–33. doi: 10.1080/14764170600607624[↩][↩][↩]
- Gold MH, Sensing W, Biron JA. Clinical efficacy of home-use blue-light therapy for mild-to-moderate acne. J Gosmet Laser Ther. 2011;13:308–314. doi: 10.3109/14764172.2011.630081[↩]
- Wheeland RG, Dhawan S. Evaluation of self-treatment of mild-to-moderate facial acne with a blue light treatment system. J Drugs Dermatol. 2011 Jun;10(6):596-602.[↩][↩]
- Akaraphanth R, Kanjanawanitchkul W, Gritiyarangsan P. Efficacy of ALA-PDT vs blue light in the treatment of acne. PhotodermatolPhotoimmunolPhotomed. 2007;23:186–190. doi: 10.1111/j.1600-0781.2007.00303.x[↩]
- Weinstabl A, Hoff-Lesch S, Merk HF, von Felbert V. Prospective randomized study on the efficacy of blue light in the treatment of psoriasis vulgaris. Dermatology. 2011;223:251–259. doi: 10.1159/000333364[↩]
- Sadick N. A study to determine the effect of combination blue (415nm) and near-infrared (830nm) light-emitting diode (LED) therapy for moderate acne vulgaris. J Cosmet Laser Ther. 2009;11:125–128. doi: 10.1080/14764170902777349[↩][↩][↩]
- Lee SY, You CE, Park MY. Blue and red combination LED phototherapy for acne vulgaris in patients with skin phototype IV. Lasers Surg Med. 2006;39:180–188. doi: 10.1002/lsm.20412[↩][↩]
- Goldberg DJ, Hussain M, Fazeli A, et al. Treatment of skin laxity of the lower face and neck in older individuals with a broad-spectrum infrared light device. J Cosmet Laser Ther. 2007;9:35–40. doi: 10.1080/14764170601186107[↩][↩]
- Kwon HH, Lee JB, Yoon JY, et al. The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: a double-blind, randomized controlled trial. Br J Dermatol. 2013;168:1088–1094. doi: 10.1111/bjd.12186[↩][↩][↩]
- Papageorgiou P, Katsambas A, Chu A. Phototherapy with blue (415nm) and red (660nm) light in the treatment of acne vulgaris. Br J Dermatol. 2000;142:973–978. doi: 10.1046/j.1365-2133.2000.03481.x[↩][↩][↩]
- Gold MH, Sensing W, Biron JA. Clinical efficacy of home-use blue-light therapy for mild-to moderate acne. J Cosmet Laser Ther. 2011;13:308–14. doi: 10.3109/14764172.2011.630081[↩]
- Gold MH, Biron JA, Sensing W. Clinical and usability study to determine the safety and efficacy of the Silk’n Blue Device for the treatment of mild to moderate inflammatory acne vulgaris. J Cosmet Laser Ther. 2014;16:108–113. doi: 10.3109/14764172.2013.854638[↩]
- Ash C, Harrison A, Drew S, et al. A randomized controlled study for the treatment of acne vulgaris using high-intensity 414 nm solid state diode arrays. J Cosmet Laser Ther. 2015;20:1–7. doi: 10.3109/14764172.2015.1007064[↩]
- Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60:S1–S50. doi: 10.1016/j.jaad.2009.01.019[↩]
- Charakida A, Seaton ED, Charakida M, et al. Phototherapy in the treatment of acne vulgaris: What is its role? Am J Clin Dermatol. 2004;5:211–216. doi: 10.2165/00128071-200405040-00001[↩]
- Liu LH, Fan X, An YX, Zhang J, Wang CM, Yang RY. Randomized trial of three phototherapy methods for the treatment of acne vulgaris in Chinese patients. Photodermatol Photoimmunol Photomed. 2014 Oct;30(5):246-53. doi: 10.1111/phpp.12098[↩]
- Kwon HH, Lee JB, Yoon JY, Park SY, Ryu HH, Park BM, Kim YJ, Suh DH. The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: a double-blind, randomized controlled trial. Br J Dermatol. 2013 May;168(5):1088-94. doi: 10.1111/bjd.12186[↩]


{kind=link}