Contents
- What is testicular cancer
What is testicular cancer
Cancer that starts in the testicles (testes) is called testicular cancer, which are located inside the scrotum, a loose bag of skin underneath the penis. The testicles produce male sex hormones and sperm for reproduction.
The testicles are made up of several types of cells, each of which can develop into one or more types of cancer. It is important to distinguish these types of cancers from one another because they differ in how they are treated and in their prognosis (outlook).
Compared with other types of cancer, testicular cancer is rare. But testicular cancer is the most common cancer in American males between the ages of 15 and 35.
Testicular cancer facts 1
- Males of any age can develop testicular cancer, including infants and elderly men.
- About half of all cases of testicular cancer are in men between the ages of 20 and 34.
- Testicular cancer is not common; a man’s lifetime chance of getting it is about 1 in 263. The risk of dying from this cancer is about 1 in 5,000.
- Testicular cancer can be treated and usually cured, especially when it’s found early – when it’s small and hasn’t spread.
The American Cancer Society’s estimates for testicular cancer in the United States for 2018 are 2:
- About 9,310 new cases of testicular cancer diagnosed
- About 400 deaths from testicular cancer
The incidence rate of testicular cancer has been increasing in the United States and many other countries for several decades. The increase is mostly in seminomas. Experts have not been able to find reasons for this increase. Lately, the rate of increase has slowed.
Testicular cancer is not common; about 1 of every 250 males will develop testicular cancer at some point during their lifetime.
The average age at the time of diagnosis of testicular cancer is about 33. This is largely a disease of young and middle-aged men, but about 6% of cases occur in children and teens, and about 8% occur in men over the age of 55.
Because testicular cancer usually can be treated successfully, a man’s lifetime risk of dying from this cancer is very low: about 1 in 5,000.
Testicular cancer is highly treatable, even when cancer has spread beyond the testicle. Depending on the type and stage of testicular cancer, you may receive one of several treatments, or a combination.
The Testes
The testes or testicles, are paired oval glands in the scrotum measuring about 5 cm (2 in.) long and 2.5 cm (1 in.) in diameter (Figures 1, 2 and 3). Each testis (singular) has a mass of 10–15 grams.
Testicles have 2 main functions:
- They make male hormones (androgens) such as testosterone.
- They make sperm, the male cells needed to fertilize a female egg cell to start a pregnancy.
The testes develop near the kidneys, in the posterior portion of the abdomen and they usually begin their descent into the scrotum through the inguinal canals (passageways in the lower anterior abdominal wall) during the latter half of the seventh month of fetal development.
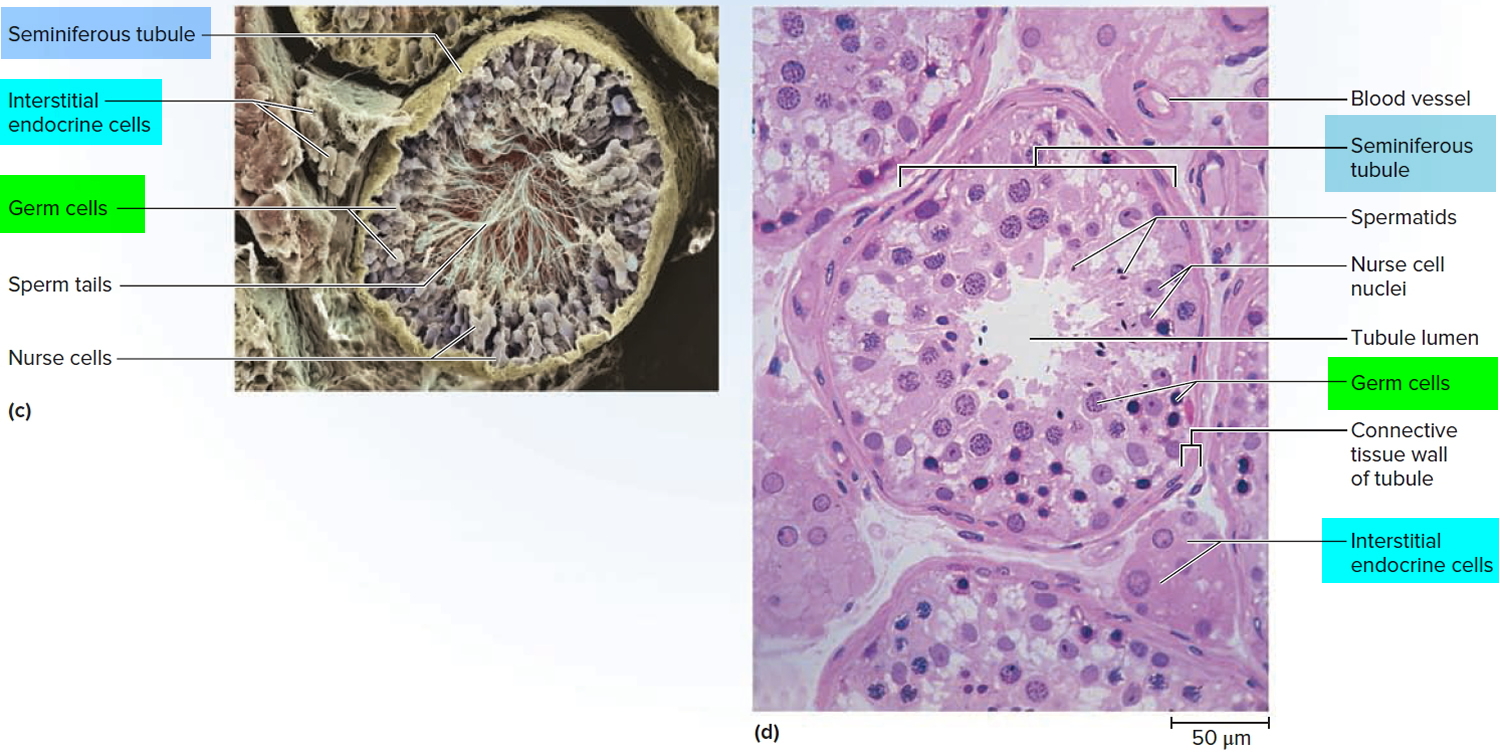
A serous membrane called the tunica vaginalis, which is derived from the peritoneum and forms during the descent of the testes, partially covers the testes. A collection of serous fluid in the tunica vaginalis is called a hydrocele. It may be caused by injury to the testes or inflammation of the epididymis. Usually, no treatment is required. Internal to the tunica vaginalis the testis is surrounded by a white fibrous capsule composed of dense irregular connective tissue, the tunica albuginea (see Figure 2); it extends inward, forming septa that divide the testis into a series of internal compartments called lobules. Each of the 200–300 lobules contains one to three tightly coiled tubules, the seminiferous tubules, where sperm are produced. The process by which the seminiferous tubules of the testes produce sperm is called spermatogenesis.
The seminiferous tubules contain two types of cells: spermatogenic cells, the sperm-forming cells, and sustentacular cells or Sertoli cells, which have several functions in supporting spermatogenesis. Stem cells called spermatogonia develop from primordial germ cells that arise from the yolk sac and enter the testes during the fifth week of development. In the embryonic testes, the primordial germ cells differentiate into spermatogonia, which remain dormant during childhood and actively begin producing sperm at puberty. Toward the lumen of the seminiferous tubule are layers of progressively more mature cells. In order of advancing maturity, these are primary spermatocytes, secondary spermatocytes, spermatids, and sperm cells. After a sperm cell, or spermatozoon, has formed, it is released into the lumen of the seminiferous tubule.
Embedded among the spermatogenic cells in the seminiferous tubules are large sustentacular cells or Sertoli cells, which extend from the basement membrane to the lumen of the tubule. Internal to the basement membrane and spermatogonia, tight junctions join neighboring sustentacular cells to one another. These junctions form an obstruction known as the blood–testis barrier because substances must first pass through the sustentacular cells before they can reach the developing sperm. By isolating the developing gametes from the blood, the blood–testis barrier prevents an immune response against the spermatogenic cell’s surface antigens, which are recognized as “foreign” by the immune system. The blood–testis barrier does not include spermatogonia.
Sustentacular cells (Sertoli cells) support and protect developing spermatogenic cells in several ways. They nourish spermatocytes, spermatids, and sperm; phagocytize excess spermatid cytoplasm as development proceeds; and control movements of spermatogenic cells and the release of sperm into the lumen of the seminiferous tubule. They also produce fluid for sperm transport, secrete the hormone inhibin, and regulate the effects of testosterone and FSH (follicle-stimulating hormone).
In the spaces between adjacent seminiferous tubules are clusters of cells called interstitial cells or Leydig cells. These cells secrete testosterone, the most prevalent androgen. An androgen is a hormone that promotes the development of masculine characteristics. Testosterone also promotes a man’s libido (sexual drive).
During ejaculation, sperm cells are carried from the epididymis through the vas deferens to seminal vesicles, where they mix with fluids made by the vesicles, prostate gland, and other glands to form semen. This fluid then enters the urethra, the tube in the center of the penis through which both urine and semen leave the body.
The scrotum (bag), the supporting structure for the testes, consists of loose skin and underlying subcutaneous layer that hangs from the root (attached portion) of the penis. Externally, the scrotum looks like a single pouch of skin separated into lateral portions by a median ridge called the raphe. Internally, the scrotal septum divides the scrotum into two compartments, each containing a single testis. The location of the scrotum and the contraction of its muscle fibers regulate the temperature of the testes. Normal sperm production requires a temperature about 2–3°C below core body temperature. This lowered temperature is maintained within the scrotum because it is outside the pelvic cavity. In response to cold temperatures, the cremaster and dartos muscles contract. Contraction of the cremaster muscles moves the testes closer to the body, where they can absorb body heat. Contraction of the dartos muscle causes the scrotum to become tight (wrinkled in appearance), which reduces heat loss. Exposure to warmth reverses these actions.
Figure 1. Testis
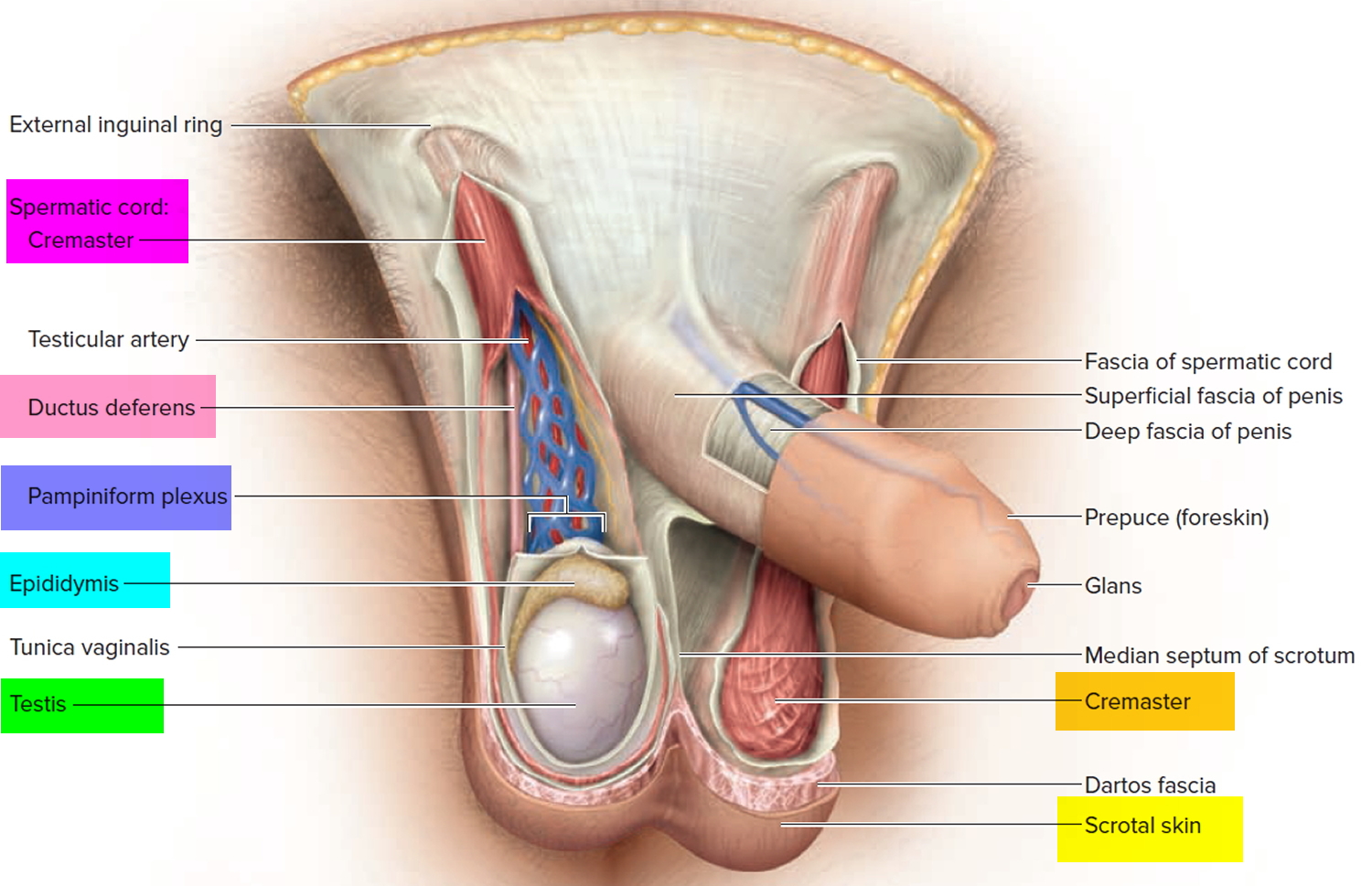 Figure 2. Testicle anatomy
Figure 2. Testicle anatomy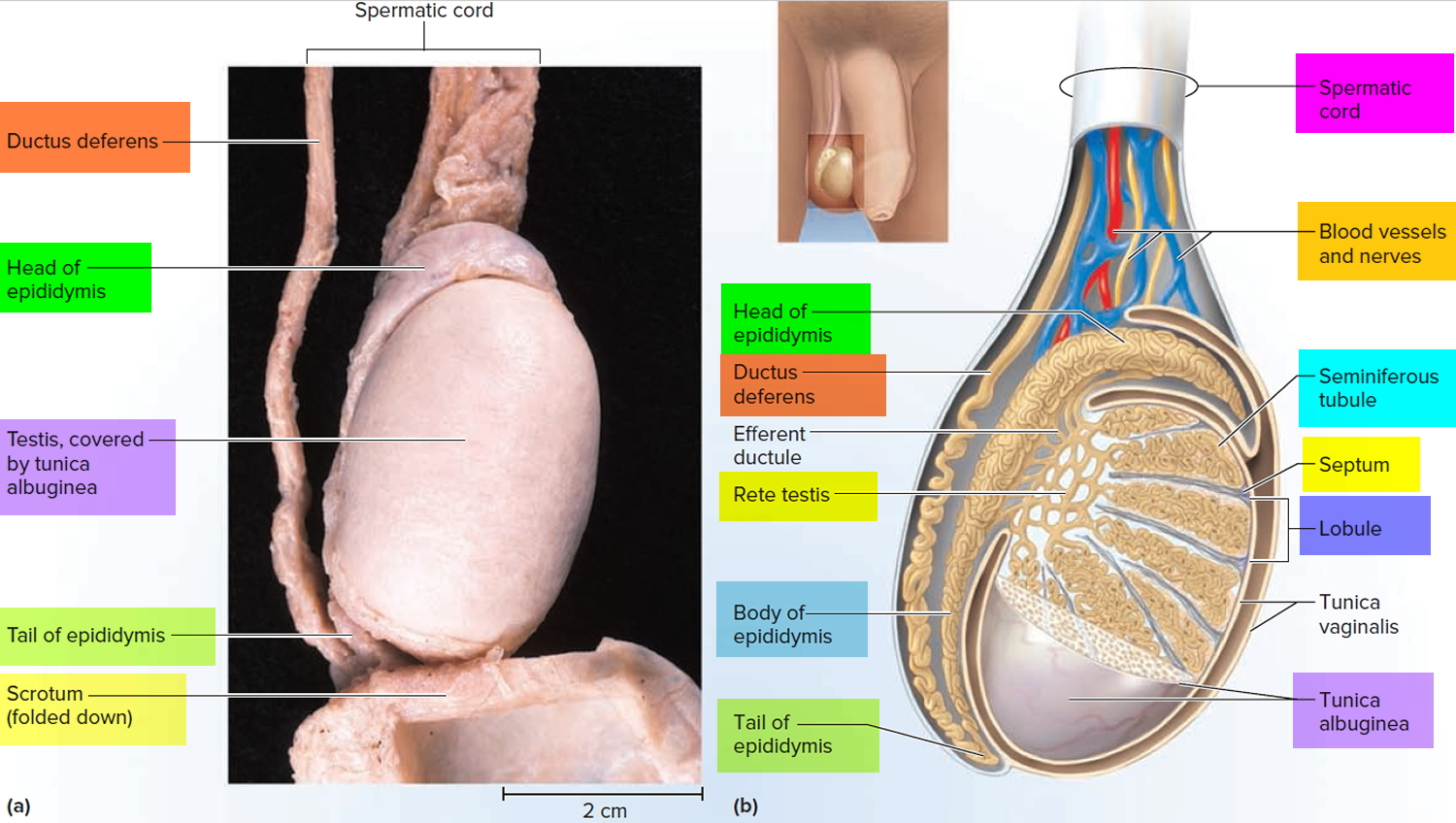
Figure 3. Testis and scrotum (cross section view)
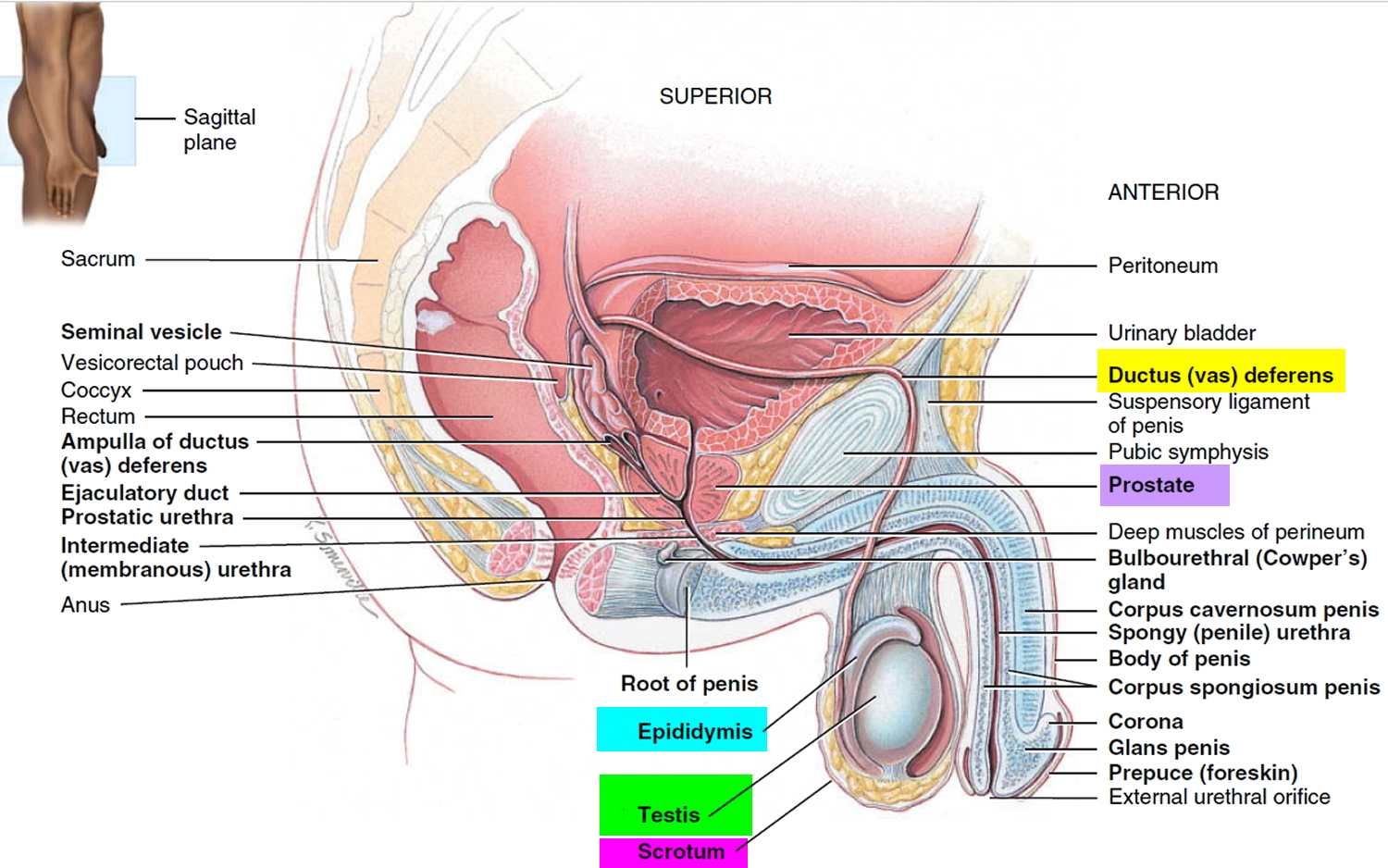
Figure 4. Scanning electron micrograph of the seminiferous tubules
 Types of testicular cancer
Types of testicular cancer
Germ cell tumors
More than 90% of cancers of the testicle develop in special cells known as germ cells. These are the cells that make sperm. The 2 main types of germ cell tumors in men are:
- Seminomas
- Non-seminomas, which are made up of embryonal carcinoma, yolk sac carcinoma, choriocarcinoma, and/or teratoma
Doctors can tell what type of testicular cancer you have by looking at the cells under a microscope.
These 2 types occur about equally. Many testicular cancers contain both seminoma and non-seminoma cells. These mixed germ cell tumors are treated as non-seminomas because they grow and spread like non-seminomas.
Seminomas
Seminomas tend to grow and spread more slowly than non-seminomas. The 2 main subtypes of these tumors are classical (or typical) seminomas and spermatocytic seminomas. Doctors can tell them apart by how they look under the microscope.
- Classical seminoma: More than 95% of seminomas are classical. These usually occur in men between 25 and 45.
- Spermatocytic seminoma: This rare type of seminoma tends to occur in older men. The average age of men diagnosed with spermatocytic seminoma is about 65. Spermatocytic tumors tend to grow more slowly and are less likely to spread to other parts of the body than classical seminomas.
Some seminomas can increase blood levels of a protein called human chorionic gonadotropin (HCG). Human chorionic gonadotropin (HCG) can be detected by a simple blood test and is considered a tumor marker for certain types of testicular cancer. It can be used for diagnosis and to check how the patient is responding to treatment.
Non-seminomas
These types of germ cell tumors usually occur in men between their late teens and early 30s. The 4 main types of non-seminoma tumors are:
- Embryonal carcinoma
- Yolk sac carcinoma
- Choriocarcinoma
- Teratoma
Most tumors are a mix of different types (sometimes with a seminoma component as well), but this doesn’t change the general approach to treatment of most non-seminoma cancers.
- 1) Embryonal carcinoma: This type of non-seminoma is present to some degree in about 40% of testicular tumors, but pure embryonal carcinomas occur only 3% to 4% of the time. When seen under a microscope, these tumors can look like tissues of very early embryos. This type of non-seminoma tends to grow rapidly and spread outside the testicle.
Embryonal carcinoma can increase blood levels of a tumor marker protein called alpha-fetoprotein (AFP), as well as human chorionic gonadotropin (HCG).
- 2) Yolk sac carcinoma: These tumors are so named because their cells look like the yolk sac of an early human embryo. Other names for this cancer include yolk sac tumor, endodermal sinus tumor, infantile embryonal carcinoma, or orchidoblastoma.
This is the most common form of testicular cancer in children (especially in infants), but pure yolk sac carcinomas (tumors that do not have other types of non-seminoma cells) are rare in adults. When they occur in children, these tumors usually are treated successfully. But they are of more concern when they occur in adults, especially if they are pure. Yolk sac carcinomas respond very well to chemotherapy, even if they have spread.
This type of tumor almost always increases blood levels of AFP (alpha-fetoprotein).
- 3) Choriocarcinoma: This is a very rare and aggressive type of testicular cancer in adults. Pure choriocarcinoma is likely to spread rapidly to distant organs of the body, including the lungs, bones, and brain. More often, choriocarcinoma cells are present with other types of non-seminoma cells in a mixed germ cell tumor. These mixed tumors tend to have a somewhat better outlook than pure choriocarcinomas, although the presence of choriocarcinoma is always a worrisome finding.
This type of tumor increases blood levels of HCG (human chorionic gonadotropin).
- 4) Teratoma: Teratomas are germ cell tumors with areas that, under a microscope, look like each of the 3 layers of a developing embryo: the endoderm (innermost layer), mesoderm (middle layer), and ectoderm (outer layer).
Pure teratomas of the testicles are rare and do not increase AFP (alpha-fetoprotein) or HCG (human chorionic gonadotropin) levels. More often, teratomas are seen as parts of mixed germ cell tumors.
There are 3 main types of teratomas:
- Mature teratomas are tumors formed by cells similar to cells of adult tissues. They rarely spread to nearby tissues and distant parts of the body. They can usually be cured with surgery, but some come back (recur) after treatment.
- Immature teratomas are less well-developed cancers with cells that look like those of an early embryo. This type is more likely than a mature teratoma to grow into (invade) surrounding tissues, to spread (metastasize) outside the testicle, and to come back (recur) years after treatment.
- Teratomas with somatic type malignancy are very rare cancers. These cancers have some areas that look like mature teratomas but have other areas where the cells have become a type of cancer that normally develops outside the testicle (such as a sarcoma, adenocarcinoma, or even leukemia).
Carcinoma in situ of the testicle
Testicular germ cell cancers can begin as a non-invasive form of the disease called carcinoma in situ (CIS) or intratubular germ cell neoplasia. In testicular carcinoma in situ, the cells look abnormal under the microscope, but they have not yet spread outside the walls of the seminiferous tubules (where sperm cells are formed). Carcinoma in situ doesn’t always progress to invasive cancer.
It is hard to find carcinoma in situ before it does become an invasive cancer because it generally does not cause symptoms and often does not form a lump that you or the doctor can feel. The only way to diagnose testicular carcinoma in situ is to have a biopsy (a procedure that removes a tissue sample and looks at it under a microscope). Some cases are found incidentally (by accident) when a testicular biopsy is done for another reason, such as infertility.
Experts don’t agree about the best treatment for carcinoma in situ. Since carcinoma in situ doesn’t always become an invasive cancer, many doctors in the United States consider observation (watchful waiting) to be the best treatment option.
When carcinoma in situ of the testicle becomes invasive, its cells are no longer just in the seminiferous tubules but have grown into other structures of the testicle. These cancer cells can then spread either to the lymph nodes (small, bean-shaped collections of white blood cells) through lymphatic channels (fluid-filled vessels that connect the lymph nodes), or through the blood to other parts of the body.
Stromal tumors
Tumors can also develop in the supportive and hormone-producing tissues, or stroma, of the testicles. These tumors are known as gonadal stromal tumors. They make up less than 5% of adult testicular tumors but up to 20% of childhood testicular tumors. The 2 main types are Leydig cell tumors and Sertoli cell tumors.
Leydig cell tumors
These tumors develop from the Leydig cells in the testicle that normally make male sex hormones (androgens like testosterone). Leydig cell tumors can develop in both adults and children. These tumors often make androgens (male hormones) but sometimes produce estrogens (female sex hormones).
Most Leydig cell tumors are benign. They usually do not spread beyond the testicle and are cured with surgery. But a small portion of Leydig cell tumors spread to other parts of the body and tend to have a poor outlook because they usually do not respond well to chemotherapy or radiation therapy.
Sertoli cell tumors
These tumors develop from normal Sertoli cells, which support and nourish the sperm-making germ cells. Like the Leydig cell tumors, these tumors are usually benign. But if they spread, they usually don’t respond well to chemotherapy and radiation therapy.
Secondary testicular cancers
Cancers that start in another organ and then spread to the testicle are called secondary testicular cancers. These are not true testicular cancers – they are named and treated based on where they started.
Lymphoma is the most common secondary testicular cancer. Testicular lymphoma occurs more often than primary testicular tumors in men older than 50. The outlook depends on the type and stage of lymphoma. The usual treatment is surgical removal, followed by radiation and/or chemotherapy.
In boys with acute leukemia, the leukemia cells can sometimes form a tumor in the testicle. Along with chemotherapy to treat the leukemia, this might require treatment with radiation or surgery to remove the testicle.
Cancers of the prostate, lung, skin (melanoma), kidney, and other organs also can spread to the testicles. The prognosis for these cancers tends to be poor because these cancers have usually spread widely to other organs as well. Treatment depends on the specific type of cancer.
Testicular cancer survival rate
The 5-year survival rate refers to the percentage of patients who live at least 5 years after their cancer is diagnosed. Of course, many people live much longer than 5 years (and many are cured).
Five-year relative survival rates assume that some people will die of other causes and compare the observed survival with that expected for people without the cancer. This is a better way to see the impact of the cancer on survival.
In order to get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. Improvements in treatment since then may result in a more favorable outlook for people now being diagnosed with testicular cancer.
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they cannot predict what will happen in any particular person’s case. Many other factors may affect a person’s outlook, such as your age and how well the cancer responds to treatment. Your doctor can tell you how the numbers below may apply to you, as he or she is familiar with your particular situation.
Testicular cancer survival rates, by stage
The survival statistics below come from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, and are based on patients who were diagnosed with testicular cancer (of any type) between 2003 and 2009.
The SEER database does not divide survival rates by the American Joint Committee on Cancer (AJCC) TNM stage. Instead, it divides cancers into summary stages: localized, regional, and distant:
- Localized means that the cancer is still only in the testicle. This includes most AJCC stage I tumors (stage 0 cancers are not included in these statistics).
- Regional means that the cancer has spread to nearby lymph nodes or tissues. This includes T4 tumors and cancers with lymph node spread (all stage II cancers and some stage IIIB and IIIC cancers).
- Distant means that the cancer has spread to organs or lymph nodes away from the tumor, such as all M1 cancers (which can be stage IIIA, IIIB, or IIIC).
| Stage | 5-Year Relative Survival Rate |
| Localized | 99% |
| Regional | 96% |
| Distant | 73% |
Other prognostic factors
As can be seen in the table above, how far the cancer has spread at the time it’s diagnosed can affect your chances of long-term survival. But in general, the outlook for testicular cancers is very good, and most of these cancers can be cured, even if they have spread.
Some other factors can also affect outlook, such as:
- The type of testicular cancer
- Levels of tumor markers after the testicular tumor has been removed
Ask your doctor how these or other prognostic factors might affect your outlook.
Testicular cancer causes
It’s not clear what causes testicular cancer in most cases.
Doctors know that testicular cancer occurs when healthy cells in a testicle become altered. Healthy cells grow and divide in an orderly way to keep your body functioning normally. But sometimes some cells develop abnormalities, causing this growth to get out of control — these cancer cells continue dividing even when new cells aren’t needed. The accumulating cells form a mass in the testicle.
Nearly all testicular cancers begin in the germ cells — the cells in the testicles that produce immature sperm. What causes germ cells to become abnormal and develop into cancer isn’t known.
Scientists have found that the disease is linked with a number of other conditions, which are described in the section the risk factors for testicular cancer. A great deal of research is being done to learn more about the causes.
Researchers are learning how certain changes in a cell’s DNA can cause the cell to become cancerous. DNA is the chemical in each of our cells that makes up our genes. Genes tell our cells how to function. They are packaged in chromosomes, which are long strands of DNA in each cell. Most cells in the body have 2 sets of 23 chromosomes (one set of chromosomes comes from each parent), but each sperm or egg cell has only 23 chromosomes. When the sperm and egg combine, the resulting embryo has a normal number of chromosomes in each cell, half of which are from each parent. We usually look like our parents because they are the source of our DNA. But DNA affects more than how we look.
Some genes control when our cells grow, divide into new cells, and die. Certain genes that help cells grow and divide are called oncogenes. Others that slow down cell division or make cells die at the right time are called tumor suppressor genes. Cancers can be caused by changes in chromosomes that turn on oncogenes or turn off tumor suppressor genes.
Most testicular cancer cells have extra copies of a part of chromosome 12 (called isochromosome 12p or i12p). Some testicular cancers have changes in other chromosomes as well, or even abnormal numbers of chromosomes (often too many). Scientists are studying these DNA and chromosome changes to learn more about which genes are affected and how this might lead to testicular cancer.
Risk factors for testicular cancer
Factors that may increase your risk of testicular cancer include:
- An undescended testicle (cryptorchidism). The testes form in the abdominal area during fetal development and usually descend into the scrotum before birth. Normally, the testicles develop inside the abdomen of the fetus and they go down (descend) into the scrotum before birth. In about 3% of boys, however, the testicles do not make it all the way down before the child is born. Sometimes the testicle remains in the abdomen. In other cases, the testicle starts to descend but remains stuck in the groin area. Men who have a testicle that never descended are at greater risk of testicular cancer than are men whose testicles descended normally. The risk remains elevated even if the testicle has been surgically relocated to the scrotum. Still, the majority of men who develop testicular cancer don’t have a history of undescended testicles. About 1 out of 4 cases of testicular cancer occur in the normally descended testicle. Because of this, some doctors conclude that cryptorchidism doesn’t actually cause testicular cancer but that there is something else that leads to both testicular cancer and abnormal positioning of one or both testicles.
- Abnormal testicle development. Conditions that cause testicles to develop abnormally, such as Klinefelter syndrome, may increase your risk of testicular cancer.
- Family history. If family members have had testicular cancer, you may have an increased risk. But only a small number of testicular cancers occur in families. Most men with testicular cancer do not have a family history of the disease.
- Age. Testicular cancer affects teens and younger men, particularly those between ages 15 and 35. However, it can occur at any age, including infants and elderly men.
- Race. Testicular cancer is more common in white men than in black men.
- HIV infection. Some evidence has shown that men infected with the human immunodeficiency virus (HIV), particularly those with AIDS, are at increased risk. No other infections have been shown to increase testicular cancer risk.
- Carcinoma in situ of the testicle. This condition often doesn’t cause a lump in the testicles or any other symptoms. It isn’t clear how often carcinoma in situ (CIS) in the testicles progresses to cancer. In some cases, CIS is found in men who have a testicular biopsy to evaluate infertility or have a testicle removed because of cryptorchidism. Doctors in Europe are more likely than the doctors in this country to look for CIS. This may be why the numbers for diagnosis and progression of CIS to cancer are lower in the United States than in parts of Europe. Since doctors don’t know how often CIS becomes true (invasive) cancer, it isn’t clear if treating CIS is a good idea. Some experts think that it may be better to wait and see if the disease gets worse or becomes a true cancer. This could allow many men with CIS to avoid the risks and side effects of treatment. When CIS is treated, radiation or surgery (to remove the testicle) is used.
- Having had testicular cancer before. A personal history of testicular cancer is another risk factor. About 3% or 4% of men who have been cured of cancer in one testicle will eventually develop cancer in the other testicle.
- Body size. Several studies have found that tall men have a somewhat higher risk of testicular cancer, but some other studies have not. Most studies have not found a link between testicular cancer and body weight.
Unproven or controversial risk factors
Prior injury or trauma to the testicles and recurrent actions such as horseback riding do not appear to be related to the development of testicular cancer.
Most studies have not found that strenuous physical activity increases testicular cancer risk. Being physically active has been linked with a lower risk of several other forms of cancer as well as a lower risk of many other health problems.
Testicular cancer signs and symptoms
If you have any of these signs or symptoms, see your doctor without delay. Many of these symptoms are more likely to be caused by something other than testicular cancer.
Symptoms of testicular cancer
You can’t be sure you have testicular cancer from just symptoms, so it’s important to see a health care provider about any testicular symptoms that concern you. Don’t wait.
- The most common symptom of testicular cancer is a painless lump on or in a testicle.
- Sometimes the testicle may become swollen or larger, without a lump. (It’s normal for one testicle to be slightly larger than the other, and for one to hang lower than the other.)
- Some testicular tumors might cause pain, but most of the time they don’t. Men with testicular cancer may also have a heavy or aching feeling in the lower belly or scrotum.
- Breast growth or soreness: Rarely, testicular cancers can cause men’s breasts to grow or become sore. This is because certain types of testicular cancer can make high levels of hormones that affect the breasts. Some men might also notice a loss of sexual desire.
- Signs of early puberty in boys: Some testicular cancers make male sex hormones. This may not cause any specific symptoms in men, but in boys it can cause signs of puberty, such as a deepening of the voice and the growth of facial and body hair, at an early age.
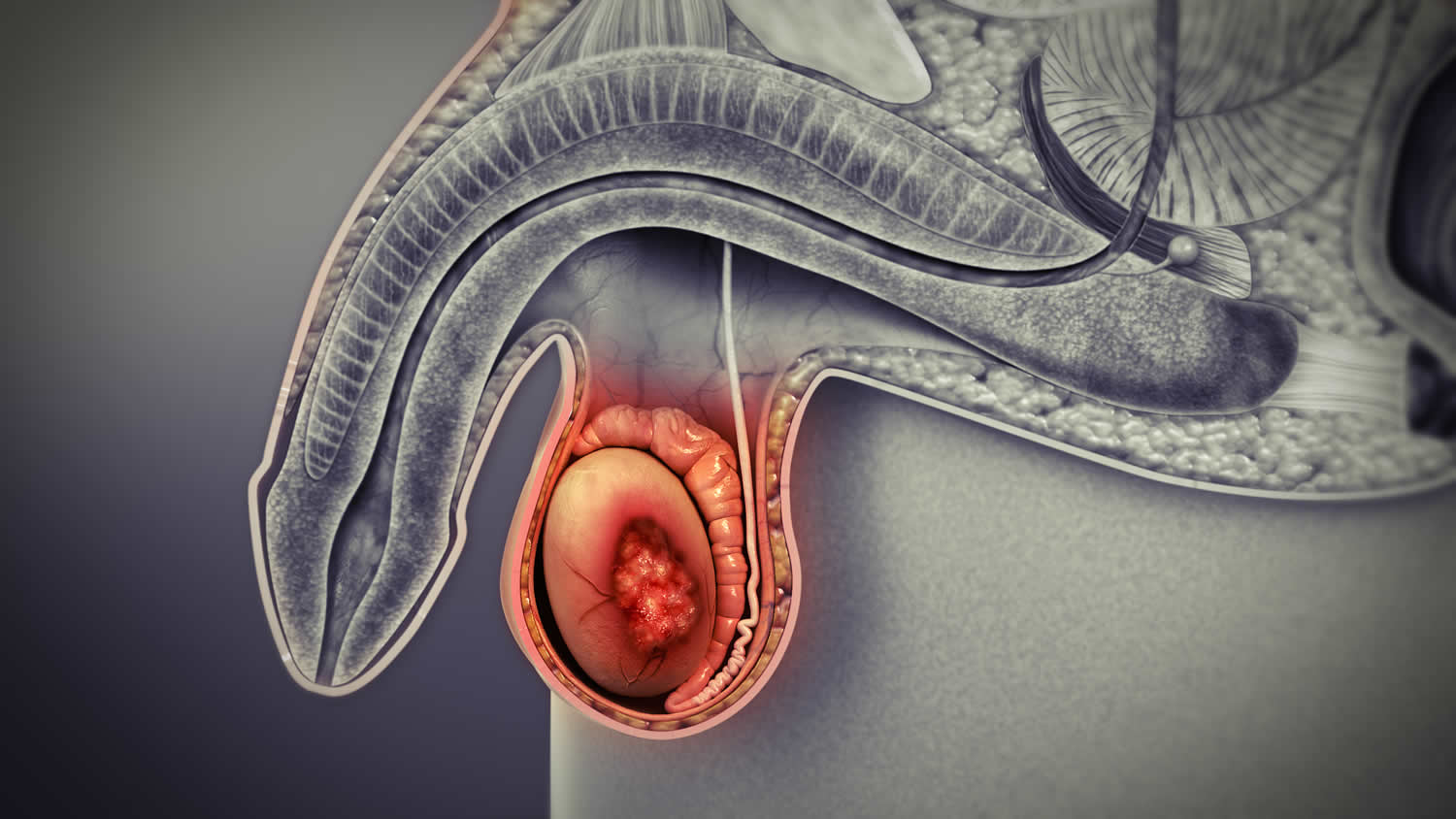
Lump or swelling in the testicle
Most often, the first symptom of testicular cancer is a lump on the testicle, or the testicle becomes swollen or larger. (It’s normal for one testicle to be slightly larger than the other, and for one to hang lower than the other.) Some testicular tumors might cause pain, but most of the time they do not. Men with testicular cancer can also have a feeling of heaviness or aching in the lower abdomen or scrotum.
Figure 5. Testicular cancer lump
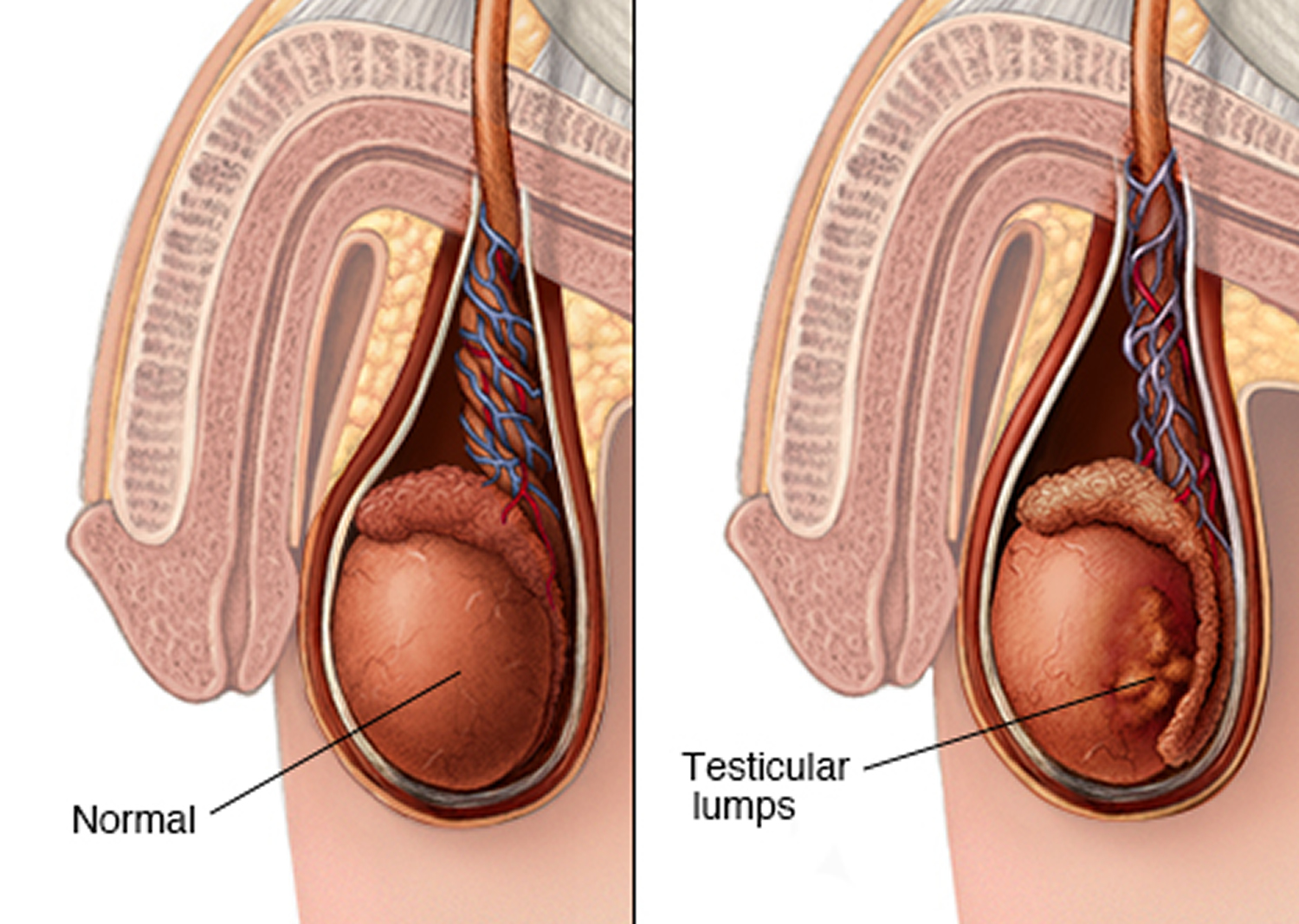
Note: Pain, swelling or lumps in your testicle or groin area may be a sign or symptom of testicular cancer or other medical conditions requiring treatment.
Breast growth or soreness
In rare cases, germ cell tumors can make breasts grow or become sore. This occurs because certain types of germ cell tumors secrete high levels of a hormone called human chorionic gonadotropin (HCG), which stimulates breast development.
Some Leydig cell tumors can make estrogens (female sex hormones), which can cause breast growth or loss of sexual desire.
Early puberty in boys
Some Leydig cell tumors can make androgens (male sex hormones). Androgen-producing tumors may not cause any specific symptoms in men, but in boys they can cause signs of puberty at an abnormally early age, such as a deepening voice and the growth of facial and body hair.
Symptoms of testicular cancer that has spread
If testicular cancer is not found early, it can spread to other parts of the body. Even when testicular cancer has spread, there may still be no symptoms. But some men might have some of the following:
- Low back pain from cancer that has spread to the lymph nodes in back of the belly. (Lymph nodes are bean-sized collections of immune cells.)
- Shortness of breath, chest pain, or a cough (even coughing up blood) from cancer spread in the lungs.
- Belly pain, either from enlarged lymph nodes, or because the cancer has spread to the liver.
- Headaches or confusion from cancer spread to the brain.
A number of non-cancerous conditions, such as testicle injury or inflammation, can cause symptoms similar to those of testicular cancer. Inflammation of the testicle (known as orchitis) and inflammation of the epididymis (epididymitis) can cause swelling and pain of the testicle. Both of these also can be caused by viral or bacterial infections.
Signs of testicular cancer
Some men with testicular cancer have no symptoms at all, and their cancer is found during medical testing for other conditions. Sometimes imaging tests done to find the cause of infertility can uncover a small testicular cancer.
Non-cancer causes of testicular or scrotal symptoms
Problems other than cancer can also cause symptoms. Because it’s hard to figure out the cause based on symptoms alone, it’s important to have any testicular or scrotal change checked by a health care provider.
Some of the conditions that can cause a testicle lump, swelling, and/or pain include:
- Torsion of the testicle
- Injury
- Infection
- Hydrocele
- Varicocele
- Epididymal cyst/spermatocele
- Inguinal hernia
- Kidney stones
Torsion of the testicle
In testicular torsion, one of the testicles gets twisted inside the scrotum. This cuts off the blood supply to the testicle, epididymis, and other structures, leading to sudden, severe pain in the scrotum along with swelling and redness. It can also cause belly pain or nausea and vomiting.
Testicular torsion occurs most often in teen boys, but may occur later in life. It’s often diagnosed using ultrasound of the testicle/scrotum. Torsion is a medical emergency that needs to be treated right away. Surgery is needed to untwist the testicle, which restores the blood supply. If the torsion isn’t treated within several hours, the testicle can die and will have to be removed.
Injury
Physical injury to the scrotum or testicle can cause pain right way, or it may cause slowly worsening pain and swelling later on as the scrotum fills with blood. This is known as a hematocele. Sometimes treatment may be needed to stop the bleeding, but the problem may get better on its own.
A testicular injury can be very painful, but it does not cause cancer.
Infection
Infections in the scrotal area are usually caused by bacteria or viruses.
Epididymitis is inflammation of the epididymis, the coiled tube next to each testicle that stores sperm. This can be caused by a sexually transmitted infection, but it can also be caused by other types of infection.
Epididymitis can cause:
- Pain and swelling on one side of the scrotum. The pain tends to come on slowly, and it may spread to the side or back.
- Pain when passing urine
- Fever
- Milky discharge from the penis
If the infection is caused by bacteria, antibiotics often will make the symptoms go away completely. But if these problems continue after you’ve taken antibiotics, you need to go back to the health care provider.
Orchitis happens when the testicle(s) becomes inflamed. It can cause painful swelling in one or both testicles. It also can impair fertility (make it harder to get a woman pregnant).
Orchitis can be caused by bacteria, including those that cause sexually transmitted infections and epididymitis. In fact, epididymitis and orchitis can happen at the same time. The mumps virus can also cause orchitis.
Hydrocele
Sometimes a testicle can feel enlarged because fluid has collected around it. This is called a hydrocele. It’s usually painless unless it grows too large. Sometimes the pain can spread to the lower belly or back. Hydroceles can have many causes. They’re usually harmless and rarely need to be treated. Hydroceles are often diagnosed with an ultrasound exam of the testicle and scrotum.
Varicocele
In varicocele, the veins within the scrotum get very large (dilate). This can cause swelling and lumpiness around the testicle. It has been described as the scrotum feeling like a “bag of worms.” It’s usually painless, but it may cause a feeling of heaviness in the scrotum. Varicoceles can be diagnosed by a physical exam or with an ultrasound exam of the testicle and scrotum. They do not usually need to be treated.
Epididymal cyst/spermatocele
An epididymal cyst may also be called a spermatocele. It’s a fluid-filled sac much like a hydrocele, but the fluid inside contains sperm cells. It’s usually a small, painless lump in the scrotum that’s not connected to the testicle. These cysts are very common, and rarely need to be treated. They are often diagnosed with an ultrasound exam of the testicle and scrotum.
Inguinal hernia
An inguinal hernia is in the groin. These hernias are caused by defects or weak spots in the muscles of the lower belly (the abdominal wall), which allow structures in the belly, such as fatty tissues and/or a loop of intestine, to go into the scrotum. There may be a slight lump or bulge in the groin or scrotum. The lump may be easier to see or feel when standing up. It’s sometimes painful, especially when bending over, lifting something heavy, coughing, or straining to pass urine or have a bowel movement.
Most of the time a hernia isn’t dangerous, but your doctor might recommend surgery to repair it, especially if it causes pain or is getting larger. Surgery can help prevent a problem called strangulation. This is when a part of the intestine gets trapped in the groin, cutting off its blood supply. This causes severe pain, nausea, and vomiting, and needs to be treated right away because it can be life threatening.
Kidney stones
Kidney stones are small crystals that form in the kidneys and can get stuck in the tubes leading to the bladder (the ureters). The stones can cause severe pain, most often in the back or belly. This pain can extend down to the scrotum. Many men also have nausea and vomiting. Blood is often found in the urine, but it might not be seen with the naked eye. Large stones may need to be removed using surgery or other procedures.
Testicular cancer prevention
There’s no way to prevent testicular cancer.
Some doctors recommend regular testicle self-examinations to identify testicular cancer at its earliest stage. But not all doctors agree. Discuss testicular self-examination with your doctor if you’re unsure about whether it’s right for you.
Testicular self-exam
Most health care providers agree that checking a man’s testicles should be part of a routine physical exam. And some doctors recommend that all men examine their testicles monthly after puberty.
How to do a testicular self-exam
The best time to do the self-exam is during or after a bath or shower, when the skin of the scrotum is relaxed.
- Hold your penis out of the way and check one testicle at a time.
- Hold the testicle between your thumbs and fingers of both hands and roll it gently between your fingers.
- Look and feel for any hard lumps or smooth rounded bumps or any change in the size, shape, or consistency of the testicles.
It’s normal for one testicle to be slightly larger than the other, and for one to hang lower than the other. You should also know that each normal testicle has a small, coiled tube (epididymis) that can feel like a small bump on the upper or middle outer side of the testicle. Normal testicles also have blood vessels, supporting tissues, and tubes that carry sperm. Some men may confuse these with abnormal lumps at first. If you have any concerns, ask your health care provider.
If you check your testicles regularly, in time you will learn what’s normal for you and will be able to tell when something is different.
What if you find something different?
If you find something unusual or something you’re not sure about, either during a self-exam or at any other time, see a health care provider right away.
The provider will ask if you’re having any symptoms (such as pain) and how long you’ve had them. During a physical exam, the provider will feel your testicles for swelling or tenderness and for the size and location of any lumps. The provider might also examine your abdomen (belly), groin area, and other parts of your body, looking for any possible signs of cancer spread.
If anything abnormal is found, an ultrasound may be done to look at the scrotum and testicles. This is an easy and painless way of finding out whether there’s a tumor or another problem. Other tests might be done as well.
Testicular cancer diagnosis
Testicular cancer is usually found as a result of symptoms that a person is having. It can also be found as a result of tests for another condition. Often the next step is an exam by a doctor.
The doctor will feel the testicles for swelling or tenderness and for the size and location of any lumps. The doctor will also examine your abdomen, lymph nodes, and other parts of your body carefully, looking for any possible signs of cancer spread. Often the results of the exam are normal aside from the testicles. If a lump or other sign of testicular cancer is found, testing is needed to look for the cause.
Ultrasound of the testicles
An ultrasound is often the first test done if the doctor thinks you might have testicular cancer.
This test uses sound waves to produce images of internal organs. A transducer (wand-like instrument) gives off sound waves and picks up the echoes as they bounce off the organs. A computer creates an image on a monitor from the pattern of the echoes.
The pattern of echoes can be used to distinguish certain benign conditions (like hydrocele or varicocele), from a solid tumor that could be a cancer. If the lump is solid, then it’s more likely to be a cancer, so the doctor will recommend further tests or even surgery to remove the testicle.
Ultrasound is an easy test to have and it uses no radiation. You are on your back on a table as the technician moves the transducer along the skin of the scrotum. Usually, the skin is first lubricated with gel.
Blood tests for tumor markers
Some blood tests can help diagnose testicular tumors. Many testicular cancers make high levels of certain proteins called tumor markers, such as alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG). When these tumor markers are in the blood, it suggests that there is a testicular tumor.
Rises in AFP or HCG can also help doctors tell which type of testicular cancer it might be. Non-seminomas often raise alpha-fetoprotein (AFP) and/or human chorionic gonadotropin (HCG) levels. Pure seminomas occasionally raise human chorionic gonadotropin (HCG) levels but never AFP levels, so any increase in AFP means that the tumor has a non-seminoma component. (Tumors can be mixed and have areas of seminoma and non-seminoma.) Sertoli and Leydig cell tumors do not make these substances. Some cancers are too small to elevate levels of these tumor markers.
A testicular tumor might also increase the levels of an enzyme called lactate dehydrogenase (LDH). LDH levels can also be increased in conditions other than cancer. A high LDH level often (but not always) indicates widespread disease.
Tumor marker tests sometimes are also used for other reasons, such as to help estimate how much cancer is present, to follow the patient’s response to treatment, or to look for signs the tumor might have returned.
Surgery to diagnose testicular cancer
Most types of cancer are diagnosed by removing a small piece of the tumor and looking at it under a microscope for cancer cells. This is known as a biopsy. But a biopsy is rarely done for a testicular tumor because it might risk spreading the cancer. The doctor can often get a good idea of whether it is testicular cancer based on the ultrasound and blood tumor marker tests, so instead of a biopsy the doctor will very likely recommend surgery to remove the tumor as soon as possible.
The operation to remove a testicular tumor or cancer is called a radical inguinal orchiectomy. In this procedure, the surgeon makes a cut (incision) just above the pubic area and then removes the entire tumor along with the testicle and spermatic cord. The spermatic cord contains part of the vas deferens, as well as blood and lymph vessels that could act as pathways for testicular cancer to spread to the rest of the body. To lessen the chance that cancer cells will spread, these vessels are tied off early in the operation.
The entire specimen is sent to the lab, where a pathologist (a doctor specializing in laboratory diagnosis of diseases) looks at pieces of the tumor under a microscope. If cancer cells are found, the pathologist sends back a report describing the type and extent of the cancer.
In rare cases, when a diagnosis of testicular cancer is uncertain, the doctor may biopsy the testicle before removing it. This is done in the operating room. The surgeon makes a cut above the pubic area, withdraws the testicle from the scrotum, and examines it without cutting the spermatic cord. If a suspicious area is seen, a portion of it is removed and looked at right away by the pathologist. If cancer is found, the testicle and spermatic cord are then removed. If the tissue is not cancerous, the testicle can often be returned to the scrotum, and treatment will be surgery to remove only the tumor or the use of appropriate medicines.
If testicular cancer is found, your doctor will order imaging tests of other parts of your body to check for spread outside the testicle. These tests may also be ordered before the diagnosis is confirmed by surgery.
Imaging tests
Imaging tests use x-rays, magnetic fields, sound waves, or radioactive substances to create pictures of the inside of your body. Ultrasound of the testicles, described above, is a type of imaging test. Other imaging tests may be done for a number of reasons after a testicular cancer diagnosis, including:
- To learn how far cancer might have spread
- To help determine if treatment has been effective
- To look for possible signs of cancer coming back after treatment
Computed tomography (CT) scan
CT scans can be used to help determine the stage (extent) of the cancer by showing if it has spread to the lymph nodes, lungs, liver, or other organs.
The CT scan uses x-rays to produce detailed cross-sectional images of your body. Instead of taking one picture, like a standard x-ray, a CT scanner takes many pictures of the part of your body being studied as it rotates around you. A computer then combines these pictures into an image of a slice of your body. Before the test, you might be asked to drink a contrast solution and/or get an intravenous (IV) injection of a contrast dye that helps better outline structures in the body. You may need an IV line to inject the contrast dye. The injection can cause some flushing (redness and a warm feeling that often lasts seconds). Some people are allergic to the dye and get hives. Rarely, more serious reactions like trouble breathing and low blood pressure can occur. Medicine can be given to prevent and treat allergic reactions. Be sure to tell the doctor if you have any allergies or if you have ever reacted to any contrast material used for x-rays.
A CT scanner has been described as a large donut, with a narrow table that slides in and out of the middle opening. You need to lie still on the table while the scan is being done. CT scans take longer that regular x-rays, and you might feel a bit confined by the ring you have to lie in while the pictures are being taken.
CT guided needle biopsy: CT scans are sometimes used to guide a biopsy needle precisely into a suspected area of cancer spread. For this procedure, you stay on the CT scanning table while a doctor advances a biopsy needle through the skin toward the mass. CT scans are repeated until the doctor can see that the needle is within the mass. A fine needle biopsy sample (tiny fragment of tissue) or a core needle biopsy sample (a thin cylinder of tissue) is then removed and examined under a microscope.
Magnetic resonance imaging (MRI) scan
MRI scans are particularly helpful in looking at the brain and spinal cord. They are only done in patients with testicular cancer if the doctor has reason to think the cancer might have spread to those areas.
Like CT scans, MRI scans provide detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays. The energy from the radio waves is absorbed and then released in a pattern formed by the type of body tissue and by certain diseases. A computer translates the pattern into a very detailed image of parts of the body. A contrast material might be injected just as with CT scans. MRI scans take longer than CT scans – often up to an hour – and are a little more uncomfortable. You lie on a table that slides inside a narrow tube, which is confining and can upset people with a fear of enclosed spaces. Special, more open MRI machines can help with this if needed, but the images may not be as sharp in some cases. The MRI machine makes buzzing and clicking noises, so some places will provide earplugs to help block this out.
Positron emission tomography (PET) scan
A PET scan can help spot small collections of cancer cells in the body. It is sometimes useful to see if lymph nodes that are still enlarged after chemotherapy contain cancer or are just scar tissue. PET scans are often more useful for seminomas than for non-seminomas, so they are less often used in patients with non-seminoma.
For this test, a form of radioactive sugar (known as fluorodeoxyglucose or FDG) is injected into a vein (IV). (The amount of radioactivity is very low and will pass out of the body over the next day or so.) Because of the way cancer cells in the body grow rapidly, they often take up and use more of the radioactive sugar. After about an hour, you will be moved onto a table in the PET scanner. You lie on the table for about 30 minutes while a special camera creates a picture of areas of radioactivity in the body. The picture is not finely detailed like a CT or MRI scan, but it can provide helpful information about your whole body.
Many centers have special machines that can do both a PET and CT scan at the same time (PET/CT scan). This lets the doctor compare areas of higher radioactivity on the PET with the more detailed appearance of that area on the CT.
Bone scan
A bone scan can help show if a cancer has spread to the bones. It might be done if there is reason to think the cancer might have spread to the bones (because of symptoms such as bone pain) and if other test results aren’t clear.
For this test, a small amount of low-level radioactive material is injected into a vein (IV). The substance settles in areas of bone changes throughout the entire skeleton over the course of a couple of hours. Then, you lie on a table for about 30 minutes while a special camera detects the radioactivity and creates a picture of your skeleton.
Areas of active bone changes attract the radioactivity and show up as “hot spots.” These areas may suggest metastatic cancer, but arthritis or other bone diseases can also cause the same pattern. To distinguish among these conditions, your cancer care team may use other imaging tests such as plain x-rays or MRI scans to get a better look at the areas that light up, or they may even take biopsy samples of the bone.
Testicular Cancer Stages
After someone is diagnosed with testicular cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and how best to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
The earliest stage of testicular cancer is stage 0 (also called germ cell neoplasia in situ, or GCNIS). The other main stages range from I (1) through III (3). There is no stage IV (4) testicular cancer. Some stages are split further, using capital letters (A, B, etc.).
As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage III, means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
How is the stage determined?
The staging system most often used for testicular cancer is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 4 key pieces of information:
- The size and extent of the main tumor (T): How large is the tumor? Has it grown into nearby structures or organs?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes? How large are they, and how many are affected?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant parts of the body? (The most common sites of spread are distant lymph nodes, the bones, the liver, and the lungs.)
- The serum (blood) levels of tumor markers (S): Are any tumor marker levels higher than normal? This includes lactate dehydrogenase (LDH), human chorionic gonadotropin (HCG), and alpha-fetoprotein (AFP).
Numbers or letters after T, N, M, and S provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, M, and S categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The system described below is the most recent AJCC system, effective as of January 2018. It is used for germ cell tumors (seminomas and non-seminomas) that occur after puberty, and for sex cord stromal tumors (Leydig cell tumors and Sertoli cell tumors).
Testicular cancer might be given a clinical T category (written as cT) based on the results of a physical exam, biopsy, and imaging tests (as described in How Is Testicular Cancer Diagnosed?). Once surgery is done, the pathologic T category (written as pT) is determined by examining tissue removed during the operation.
Testicular cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Stages of testicular cancer
| AJCC Stage | Stage grouping | Stage description* |
| 0 | pTis N0 M0 S0 | The cancer is only in the seminiferous tubules (small tubes inside each testicle). It has not grown into other parts of the testicle (pTis). It has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). All tumor marker levels are within normal limits (S0). |
| I | pT1-pT4 N0 M0 SX | The tumor has grown beyond the seminiferous tubules, and might have grown outside of the testicle and into nearby structures (pT1-pT4). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). Tumor marker test results aren’t available, or the tests haven’t been done (SX). |
| IA | pT1 N0 M0 S0 | The tumor has grown beyond the seminiferous tubules, but is still within the testicle, and it has not grown into nearby blood vessels or lymph nodes (pT1). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). All tumor marker levels are within normal limits (S0). |
| IB | pT2-pT4 N0 M0 S0 | The tumor has grown outside of the testicle and into nearby structures (pT2-pT4). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). All tumor marker levels are within normal limits (S0). |
| IS | Any pT (or TX) N0 M0 S1-S3 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). At least one tumor marker level is higher than normal (S1-S3). |
| II | Any pT (or TX) N1-N3 M0 SX | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to one or more nearby lymph nodes (N1-N3), but it has not spread to distant parts of the body (M0). Tumor marker test results aren’t available, or the tests haven’t been done (SX). |
| IIA | Any pT (or TX) N1 M0 S0 or S1 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to at least one nearby lymph node (but no more than 5, if checked by surgery), and none of the lymph nodes are larger than 2 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). All tumor marker levels are within normal limits (S0), or at least one tumor marker level is slightly higher than normal (S1). |
| IIB | Any pT (or TX) N2 M0 S0 or S1 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to at least one nearby lymph node that is larger than 2 cm but no larger than 5 cm across, OR it has grown outside of a lymph node, OR more than 5 nodes contain cancer (found during surgery) (N2). The cancer has not spread to distant parts of the body (M0). All tumor marker levels are within normal limits (S0), or at least one tumor marker level is slightly higher than normal (S1). |
| IIC | Any pT (or TX) N3 M0 S0 or S1 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to at least one nearby lymph node that is larger than 5 cm across (N3). The cancer has not spread to distant parts of the body (M0). All tumor marker levels are within normal limits (S0), or at least one tumor marker level is slightly higher than normal (S1). |
| III | Any pT (or TX) Any N M1 SX | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant parts of the body (M1). Tumor marker test results aren’t available, or the tests haven’t been done (SX). |
| IIIA | Any pT (or TX) Any N M1a S0 or S1 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes or to the lungs (M1a). All tumor marker levels are within normal limits (S0), or at least one tumor marker level is slightly higher than normal (S1). |
|
IIIB
| Any pT (or TX) N1-N3 M0 S2 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to one or more nearby lymph nodes (N1-N3), but it has not spread to distant parts of the body (M0). At least one tumor marker level is significantly higher than normal (S2). |
| OR | ||
| Any pT (or TX) Any N M1a S2 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes or to the lungs (M1a). At least one tumor marker level is significantly higher than normal (S2). | |
|
IIIC | Any pT (or TX) N1-N3 M0 S3 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to one or more nearby lymph nodes (N1-N3), but it has not spread to distant parts of the body (M0). At least one tumor marker level is very high (S3). |
| OR | ||
| Any pT (or TX) Any N M1a S3 | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes or to the lungs (M1a). At least one tumor marker level is very high (S3). | |
| OR | ||
| Any pT (or TX) Any N M1b Any S | The tumor might or might not have grown outside of the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant parts of the body other than the lymph nodes or to the lungs (M1b). Tumor marker levels might or might not be higher than normal (any S). | |
*The following additional category is not listed on the table above:
- NX: Nearby lymph nodes cannot be assessed due to lack of information.
Testicular cancer treatment
After the cancer is diagnosed and staged, your cancer care team will discuss treatment options with you.
Depending on the type and stage of the cancer and other factors, treatment options for testicular cancer can include:
- Surgery
- Radiation therapy
- Chemotherapy (chemo)
- High-dose chemotherapy and stem cell transplant
In some cases, more than one of type of treatment might be used.
You may have different types of doctors on your treatment team, depending on the stage of your cancer and your treatment options. These doctors may include:
- A urologist: a surgeon who specializes in treating diseases of the urinary system and male reproductive system
- A radiation oncologist: a doctor who treats cancer with radiation therapy
- A medical oncologist: a doctor who treats cancer with medicines such as chemotherapy
Many other specialists might be involved in your care as well, including physician assistants, nurse practitioners, nurses, physical therapists, social workers, and other health professionals.
Surgery
Operations used to treat testicular cancer include:
- Surgery to remove your testicle (radical inguinal orchiectomy) is the primary treatment for nearly all stages and types of testicular cancer. To remove your testicle, your surgeon makes an incision in your groin and extracts the entire testicle through the opening. A prosthetic, saline-filled testicle can be inserted if you choose. In cases of early-stage testicular cancer, surgical removal of the testicle may be the only treatment needed.
- Surgery to remove nearby lymph nodes (retroperitoneal lymph node dissection) is performed through an incision in your abdomen. Your surgeon takes care to avoid damaging nerves surrounding the lymph nodes, but in some cases harm to the nerves may be unavoidable. Damaged nerves can cause difficulty with ejaculation, but won’t prevent you from having an erection.
If surgery is your only treatment for testicular cancer, your doctor will recommend a schedule of follow-up appointments. At these appointments — typically every few months for the first few years and then less frequently after that — you’ll undergo blood tests, CT scans and other procedures to check for signs that your cancer has returned.
Radiation therapy
Radiation therapy uses high-powered energy beams, such as X-rays, to kill cancer cells. During radiation therapy, you’re positioned on a table and a large machine moves around you, aiming the energy beams at precise points on your body.
Radiation therapy is a treatment option that’s sometimes used in people who have the seminoma type of testicular cancer. Radiation therapy may be recommended after surgery to remove your testicle.
Side effects may include nausea and fatigue, as well as skin redness and irritation in your abdominal and groin areas. Radiation therapy is also likely to temporarily reduce sperm counts and may impact fertility in some men. Talk to your doctor about your options for preserving your sperm before beginning radiation therapy.
Chemotherapy
Chemotherapy treatment uses drugs to kill cancer cells. Chemotherapy drugs travel throughout your body to kill cancer cells that may have migrated from the original tumor.
Chemotherapy may be your only treatment, or it may be recommended before or after lymph node removal surgery.
Side effects of chemotherapy depend on the specific drugs being used. Ask your doctor what to expect. Common side effects include fatigue, nausea, hair loss and an increased risk of infection. There are medications and treatments available that reduce some of the side effects of chemotherapy.
Chemotherapy may also lead to infertility in some men, which can be permanent in some cases. Talk to your doctor about your options for preserving your sperm before beginning chemotherapy.
High-Dose Chemotherapy and Stem Cell Transplant for Testicular Cancer
In general, testicular cancers respond well to chemotherapy (chemo), but not all cancers are cured. Even though higher doses of chemo might be more effective, they are not given because they could severely damage the bone marrow, which is where new blood cells are formed. This could lead to life-threatening infections, bleeding, and other problems because of low blood cell counts.
A stem cell transplant allows doctors to use higher doses of chemo. Blood-forming stem cells are collected from the bloodstream in the weeks before treatment using a special machine. In the past the stem cells were taken from the bone marrow, but this is done less often now. The stem cells are frozen, and then the patient receives high-doses of chemo.
After the chemo the patient gets his stem cells back again. This is called a transplant, but it doesn’t involve surgery – the cells are infused into a vein much like a blood transfusion. The stem cells settle in the bone marrow and start making new blood cells over the next few weeks.
For testicular cancer, stem cell transplant is most often used to treat cancers that have come back after treatment with chemo. Current studies are exploring whether a stem cell transplant may be valuable in treating some patients with advanced germ cell cancers as part of their first treatment.
A stem cell transplant is a complex treatment that can cause life-threatening side effects because of the high doses of chemotherapy used. Be sure you understand the possible benefits and risks. If the doctors think you might benefit from a transplant, it should be done at a hospital where the staff has experience with the procedure and with managing the recovery phase.
Stem cell transplants often require a long hospital stay and can be very expensive. Even if the transplant is covered by your insurance, your co-pays or other costs could add up to a lot of money. It is important to find out what your insurer will cover before deciding on a transplant to get an idea of what you might have to pay.
Coping and support
Each man comes to terms with his testicular cancer and deals with the ensuing emotions in his own way. You may feel scared and unsure of your future after your diagnosis. While feelings of anxiety may never go away, you can create a plan to help manage your emotions. Try to:
- Learn enough about testicular cancer to feel comfortable making decisions about your care. Write down questions and ask them at your next doctor’s appointment. Ask your doctor or other members of your health care team to recommend reputable sources of further information. Good places to start include the National Cancer Institute 3 and the American Cancer Society 4.
- Take care of yourself. Make healthy choices in your everyday life to prepare for cancer treatment. Eat a healthy diet with a variety of fruits and vegetables.
- Get plenty of rest so that you wake each morning feeling refreshed. Eliminate unnecessary stress so that you can concentrate on getting well. Try to exercise most days of the week. If you smoke, stop. Talk to your doctor about medications and other strategies to help you stop smoking.
- Connect with other cancer survivors. Find other testicular cancer survivors in your community or online. Contact the American Cancer Society for support groups in your area.
- Stay connected with loved ones. Your family and friends are just as concerned for your health as you are. They want to help, so don’t turn down their offers to assist with transportation to appointments or with errands. Close friends and family will listen when you need someone to talk to or provide a distraction when you’re feeling down.
- Do I Have Testicular Cancer? https://www.cancer.org/cancer/testicular-cancer/do-i-have-testicular-cancer.html[↩]
- Key Statistics for Testicular Cancer. https://www.cancer.org/cancer/testicular-cancer/about/key-statistics.html[↩]
- National Cancer Institute. https://www.cancer.gov/[↩]
- American Cancer Society. https://www.cancer.org[↩]





{kind=link}