Transposition of the great arteries
Transposition of the great arteries (TGA) also called transposition of the great vessels (TGV) or dextro-transposition of the great arteries (D-TGA), is a rare life-threatening heart birth defect (congenital heart defect) where the aorta and pulmonary artery are reversed or transposed, connecting to the wrong ventricles so that each one carries blood to the wrong location, creating separate, unmixed blood circuits 1. This leads to oxygen-poor blood being sent to the body and oxygen-rich blood to the lungs, causing symptoms like a blueish skin color (cyanosis) and requiring urgent surgical treatment. In a normal heart, one of two great arteries, known as the main pulmonary artery, brings oxygen-poor blood (blood that’s low in oxygen) from the right ventricle to the lungs, where it becomes oxygenated (oxygen-rich). Another great artery, the aorta, carries oxygen-rich blood from the left ventricle to the rest of the body. In an individual with transposition of the great arteries (TGA), the placement of the arteries, the aorta and pulmonary artery, is reversed, so that oxygen-poor blood, which should go through the main pulmonary artery from the right ventricle to the lungs to pick up oxygen, goes through the aorta instead, sending unoxygenated blood to the body. Similarly, oxygen-rich blood that is supposed to travel through the aorta instead enters the main pulmonary artery, sending oxygenated blood back to the lungs. This creates two separate circuits, the pulmonary and systemic circulations are separate and independent of each other, that is, they are in parallel, like two separate rings with no mixing of oxygenated and deoxygenated blood, which is incompatible with life.
To understand transposition of the great arteries, it may help to know how the heart usually pumps blood. The typical heart has four chambers (see Figures 1 to 4 below).
- The two upper chambers are called the atria.
- The two lower chambers are called the ventricles.
The artery that carries blood from the heart to the lungs is called the pulmonary artery. It connects to the heart’s lower right chamber, called the right ventricle. The right side of the heart moves blood to the lungs. In the lungs, blood picks up oxygen and then returns it to the heart’s left side. The left side of the heart then pumps the blood through the body’s main artery, called the aorta. The blood then goes out to the rest of the body.
There are several other heart abnormalities that may occur along with transposition of the great arteries. The most common associated problem is a ventricular septal defect (VSD). This is a defect or hole in the wall that separates the lower two chambers of the heart, the ventricles. There may be narrowing of the area of the heart where blood flows out to the pulmonary artery. This is called left ventricular outflow tract obstruction. Many babies with transposition of the great arteries also have an atrial septal defect (ASD) a hole in the wall that separates the top two chambers of the heart and/or a patent ductus arteriosus (PDA).
About 1,200 babies in the United States are born with transposition of the great arteries or transposition of the great vessels each year, accounting for about 3% of all congenital heart conditions and 20% of cyanotic heart diseases 2. Scientists don’t know the exact cause of transposition of the great arteries (TGA), but it’s thought to be multifactorial related to genetic factors and exposure to certain toxins during pregnancy, such as gestational diabetes.
Babies born with transposition of the great arteries are typically diagnosed before birth, during an ultrasound in mid-pregnancy to assess fetal heart anatomy. This diagnosis can also occur within the first hours or days of life if a baby’s skin appears bluish (cyanosis) and they have difficulty breathing and/or feeding, among other signs that they aren’t getting the oxygen that they need.
Babies with transposition of the great arteries or transposition of the great vessels require surgery called “Arterial Switch Operation“, which repositions the great arteries and coronary arteries, allowing oxygenated blood to reach the body within the first weeks of life so that oxygen-rich blood can be delivered to the body. In most cases of dextro-transposition of the great arteries (D-TGA), an arterial switch operation is performed. The arterial switch operation involves cutting off the aorta and pulmonary arteries just above the point where they leave the heart, and reconnecting them to the proper ventricle. The valve stays attached to the ventricle, so that what was once the pulmonary valve is now the aortic valve and vice versa. Since the coronary arteries must stay with the aorta, they must be taken off the area above the valve and reimplanted separately above the new aortic valve. This is often the most technically challenging part of the operation, particularly if there is any unusual branching of these arteries. Closure of ventricular septal defects (if present) and atrial septal defects are also performed as part of the operation. Without the surgery, most babies with transposition of the great arteries will not survive beyond their first year. Most babies who undergo the arterial switch operation as infants live into adulthood.
Occasionally, in more complex cases of transposition such as in those with narrowing below the pulmonary valve, the arterial switch operations is not recommended. These cases often involve complex decision making on a case-by-case basis to determine the best options and operative plan.
In very rare cases, Atrial Switch Operation commonly known as Mustard procedure or Senning procedure creates a tunnel (baffle) between the atria (atrial baffle). During Atrial Switch Operation, the aorta and pulmonary artery are left in place. However, a tunnel (baffle) is created between the top chambers (atria) of the heart. This redirects the oxygen-rich blood to the right ventricle and aorta and the oxygen-poor blood to the left ventricle and the pulmonary artery. Although this repair helps blood to go to the lungs and then out to the body, it also makes extra work for the right ventricle to pump blood to the entire body. Therefore, this repair can lead to difficulties later in life.
Infants who have surgical repairs for dextro-transposition of the great arteries (D-TGA) are not cured. They may have lifelong complications. A child or adult with dextro-transposition of the great arteries (D-TGA) will need regular follow-up visits with a cardiologist (a heart doctor) to monitor their progress and avoid complications or other health problems. Many patients do not require any specific medications. Possible discharge medications might include digoxin, furosemide (water pill or diuretic), or both.
All transposition of the great arteries patients require antibiotic prophylaxis prior to dental and indicated surgical procedures in order to reduce the risk of subacute bacterial endocarditis 3. Therefore, all patients require preoperative and postoperative antibiotic prophylaxis for dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa. Antibiotic prophylaxis is also recommended for invasive respiratory tract procedures that involve incision or biopsy of the respiratory mucosa (eg, tonsillectomy, adenoidectomy). Antibiotic prophylaxis is not recommended for bronchoscopy unless the procedure involves incision of the respiratory tract mucosa. For invasive respiratory tract procedures to treat an established infection (eg, drainage of abscess, empyema), administer an antibiotic active against Streptococcus viridans.
With proper treatment, most babies with dextro-transposition of the great arteries (D-TGA) grow up to lead healthy, productive lives. The survival of children with transposition of the great arteries has improved dramatically over recent decades. When there are no unusual risk factors identified, over 95% of infants successfully undergo surgery in the newborn period. Since the arterial switch operation (ASO) reconstructs the heart to a near normal configuration both anatomically and physiologically, long-term cardiac survival and function is typically excellent.
Evidence from the Boston Circulatory Arrest Trial suggests that neurodevelopmental outcomes for children with dextro-transposition of the great arteries (d-TGA) who undergo Arterial Switch Operation (ASO) and other complex neonatal operations may not be normal and may require further investigation and follow-up 4.
In a small percentage of children, narrowing (stenosis) may occur at the site that the pulmonary artery was reattached. The narrowing may occur months or years following surgery and may require intervention. Options for treating this narrowing include cardiac catheterization with balloon dilation of the narrowed area or reoperation, depending on the characteristics of the narrowing.
Even though patients are expected to do well after arterial switch operation, long-term follow-up with the cardiologist is important to detect problems early. This follow-up often consists of regular physical exams, periodic echocardiography, and perhaps an exercise stress test when a child is old enough to perform this test.
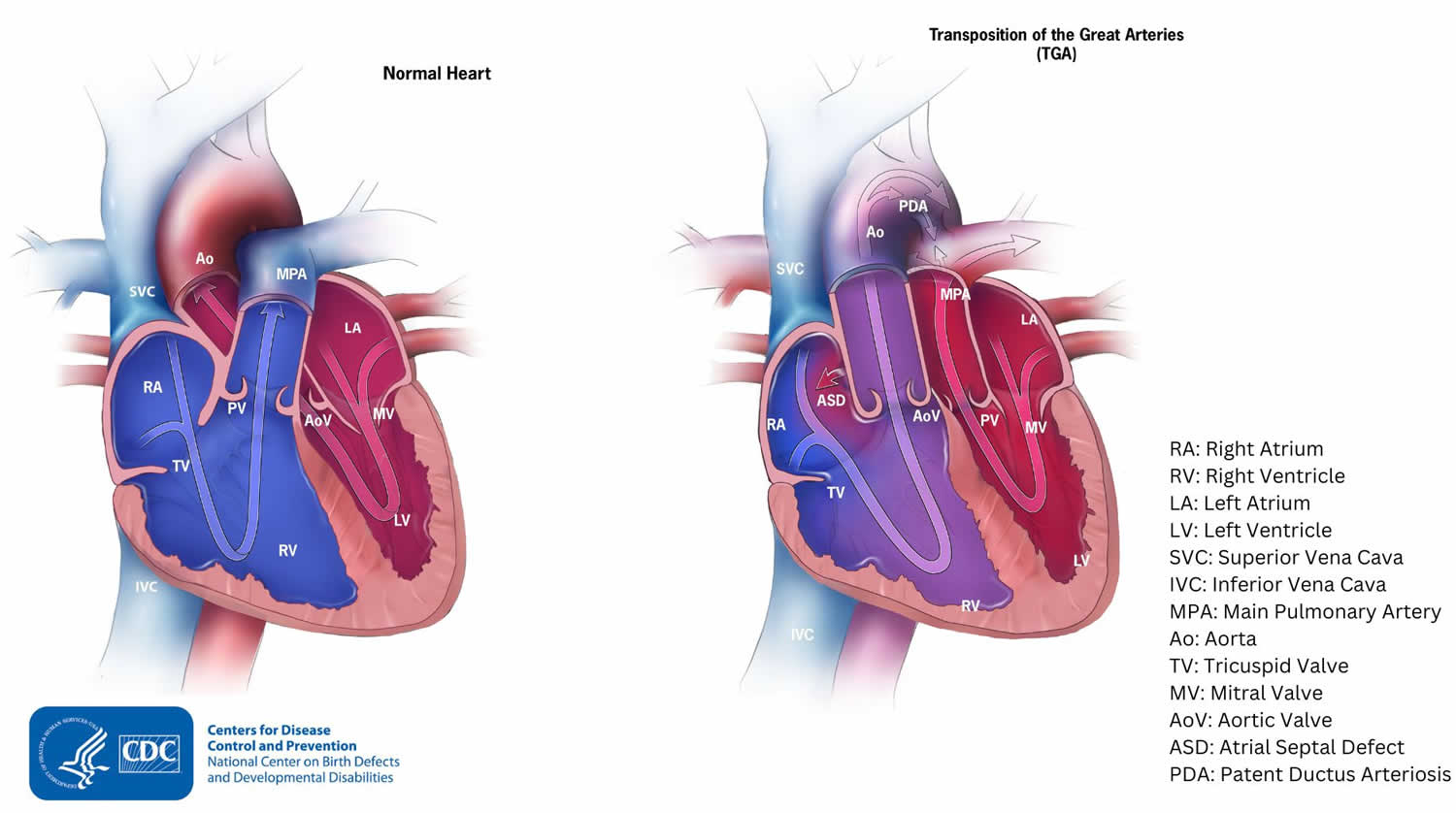
Figure 1. Normal heart blood flow

Abbreviations: PA = pulmonary artery; RA = right atrium; RV = right ventricle; AO = aorta; LA = left atrium; LV = left ventricle.
Footnotes: The normal heart has 4 chambers. The upper two chambers are the atria (left and right atrium), and the lower two are the ventricles (left and right ventricle). The heart chambers are separated by a wall of tissue called the septum. Blood is pumped through the chambers, aided by four heart valves. The valves open and close to let the blood flow in only one direction.
The four heart valves are:
- Tricuspid valve, located between the right atrium and the right ventricle. The tricuspid valve normally has three flaps.
- Pulmonary valve, between the right ventricle and the pulmonary artery. The pulmonary valve normally has three flaps.
- Mitral valve, between the left atrium and left ventricle. The mitral valve normally has two flaps.
- Aortic valve, between the left ventricle and the aorta. The aortic valve normally has three flaps.
Each heart valve has a set of “flaps” also called leaflets or cusps.
[Source 5 ]Figure 2. Normal heart blood flow patterns
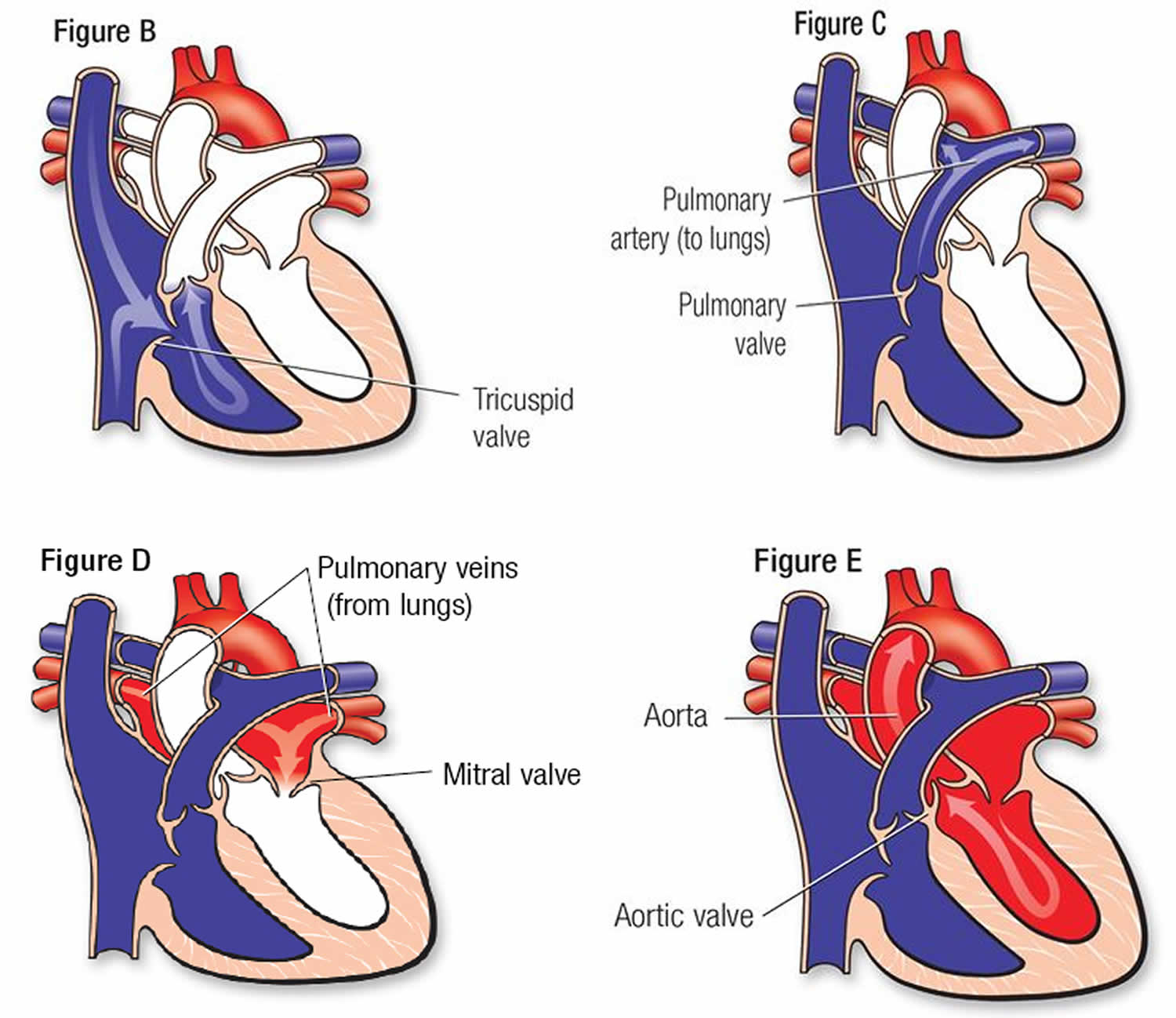
Footnotes: The normal heart blood flow blood flow is a cycle that flows like this: body –> heart –> lungs –> heart –>body.
- From the body to the heart. Figure B shows dark bluish blood, low in oxygen, flowing back to the heart after circulating through the body. It returns to the heart through veins and enters the right atrium. This chamber empties blood through the tricuspid valve into the right ventricle (RV).
- From the heart to the lungs. Figure C, the right ventricle (RV) pumps the blood under low pressure through the pulmonary valve into the pulmonary artery (PA). From there the blood goes to the lungs where it gets fresh oxygen.
- From the lungs to the heart. Figure D, after the blood is refreshed with oxygen in the lungs, it’s bright red. The red oxygen-rich blood returns to the left heart through the pulmonary veins to the left atrium. From there it passes through the mitral valve and enters the left ventricle (LV).
- From the heart to the body. Figure E, the left ventricle (LV) pumps the red oxygen-rich blood out through the aortic valve into the aorta. The aorta (AO) takes blood to the body’s general circulation. The blood pressure in the left ventricle (LV) is the same as the pressure measured in your arm.
Figure 3. Transposition of the great arteries
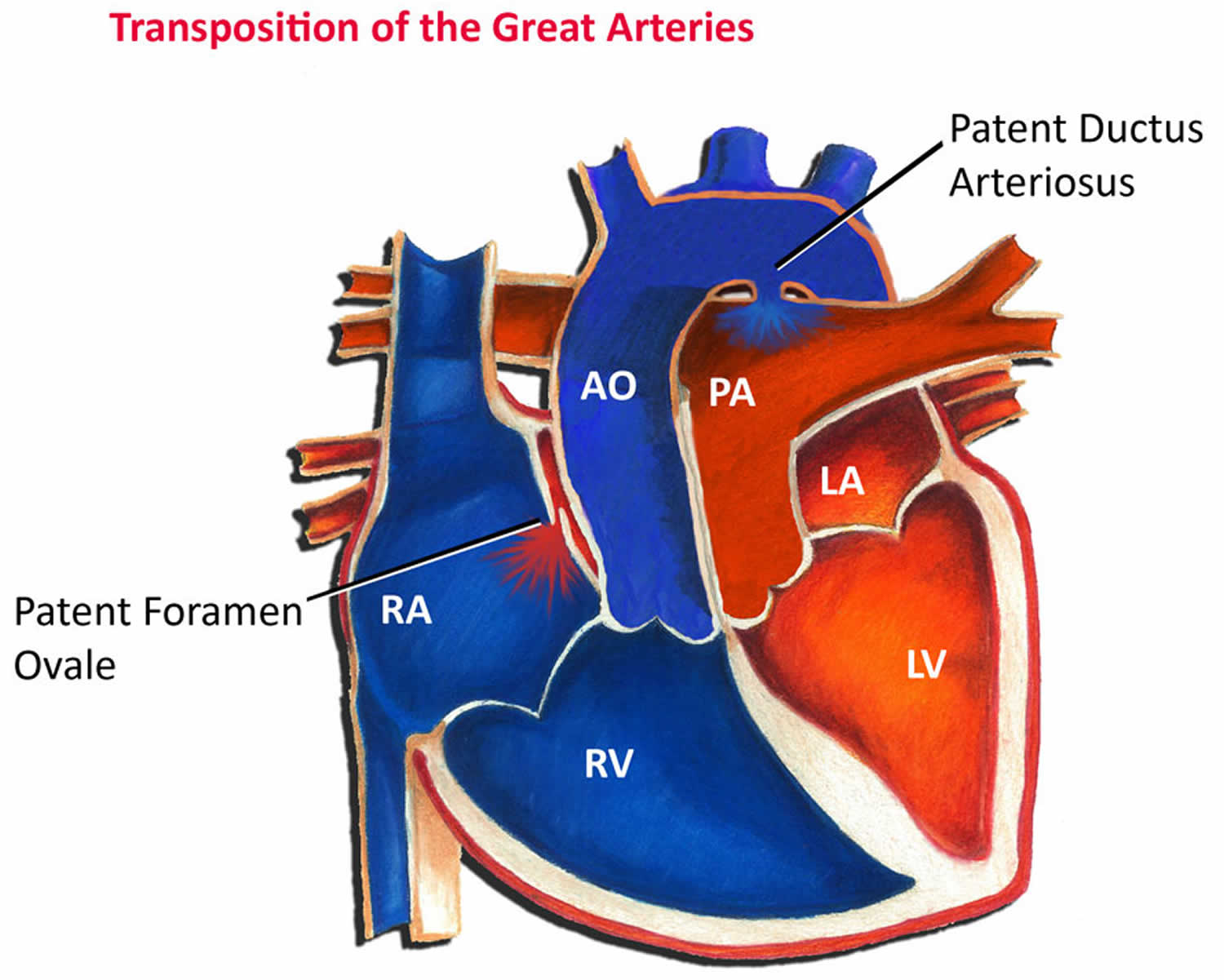
Footnotes: In transposition of the great arteries also called transposition of great vessels or dextro-transposition of the great arteries (d-TGA), the pulmonary artery and aorta switch places or “transposed”, so that the pulmonary artery (PA) arises from the left ventricle and the aorta (AO) from the right ventricle. The pulmonary artery connects to the left lower heart chamber, left ventricle. The aorta connects to the right lower heart chamber, right ventricle. Subsequently, oxygen-poor blue blood returning from the body to the right ventricle is pumped directly back out to the body through the aorta instead of passing through the pulmonary artery and to the lungs. Any oxygen-rich red blood returning from the lungs is pumped from the left ventricle out the pulmonary artery and returns to the lungs. In transposition of the great arteries, the pulmonary and systemic circulations are separate and independent of each other, that is, they are in parallel, like two separate rings. Unless there also is a hole in the heart, such as an atrial septal defect (ASD), that lets the blood mix, the body does not get oxygen-rich blood. This is life-threatening. If an infant with dextro-transposition of the great arteries (d-TGA) has an atrial septal defect (ASD), the atrial septal defect (ASD) forms a passageway for some oxygen-rich blood to reach the rest of the body. Therefore, this infant with both heart defects may not have as severe symptoms as infants whose hearts don’t have any mixing of blood.
When a transposition of the great arteries occurs, the blood pathway is impaired because the two arteries are connecting to the wrong chambers in the heart. This means that the blood flow cycle is stuck in either:
- body–>heart –>body (without being routed to the lungs for oxygen) or
- lungs–>heart–>lungs (without delivering oxygen to the body)
Without surgery, the only way to survive this condition temporarily is to have leakages that allow some oxygen-rich blood to cross into the oxygen-poor blood for delivery to the body. A hospital facility can also catheterize a patient until corrective surgery can be performed.
Abbreviations: PA = pulmonary artery; RA = right atrium; RV = right ventricle; AO = aorta; LA = left atrium; LV = left ventricle.
[Source 6 ]Figure 4. Dextro-transposition of the great arteries (d-TGA)
Footnotes: Often, babies with Dextro-transposition of the great arteries (d-TGA) have other heart defects, such as a ventricular septal defect (VSD) or an atrial septal defect (ASD). These heart defects allow blood to mix so that some oxygen-rich blood can be pumped to the rest of the body. The patent ductus arteriosus (PDA) also allows some oxygen-rich blood to be pumped to the rest of the body.
[Source 7 ]Figure 5. Congenitally corrected transposition of the great arteries (ccTGA) or Levo-transposition of the great arteries (l-TGA)
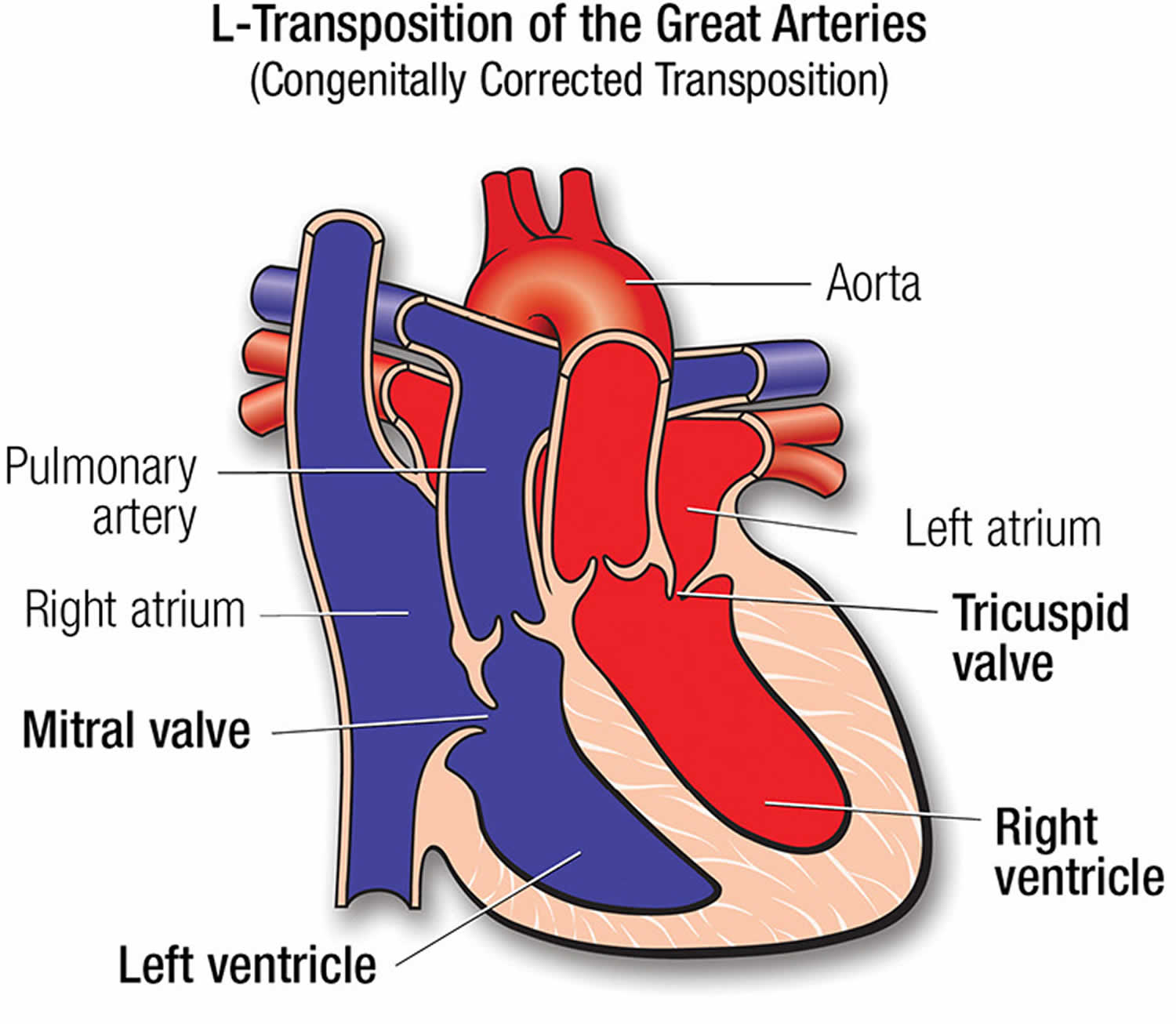
Footnotes: Levo-transposition of the great arteries (L-TGA) also called congenitally corrected transposition of the great arteries (ccTGA) occurs when the two lower heart chambers are reversed, resulting in both atrioventricular and ventriculoarterial discordance or “double discordance” where the ventricles are not properly aligned with their corresponding atria.
- The lower left heart chamber, called the left ventricle, is on the heart’s right side. It gets blood from the upper right heart chamber.
- The lower right heart chamber is on the heart’s left side. It gets blood from the left upper heart chamber.
- The blood usually still flows the right way through the heart and body. But the heart can have long-term trouble pumping blood.
Congenitally corrected transposition of the great arteries (ccTGA) is a less common type. Congenitally corrected transposition of the great arteries (ccTGA) occurs in about 0.05% of all congenital heart disease cases, with an estimated incidence of approximately 1 in every 33,000 live births 8. An international study examining the largest cohort of congenitally corrected transposition of the great arteries (ccTGA) cases identified nonsporadic occurrences, including familial clusters. The study also found associations between congenitally corrected transposition of the great arteries (ccTGA), dextro-transposition of the great arteries (D-TGA), laterality defects, and, in some instances, primary ciliary dyskinesia. These findings suggest a potential common pathogenetic pathway involving laterality genes in the development of congenitally corrected transposition of the great arteries (ccTGA) 9. Congenitally corrected transposition of the great arteries (ccTGA) is highly variable and can present with a range of anatomical features and clinical manifestations.
[Source 10 ]Figure 6. Transposition of the great arteries ultrasound
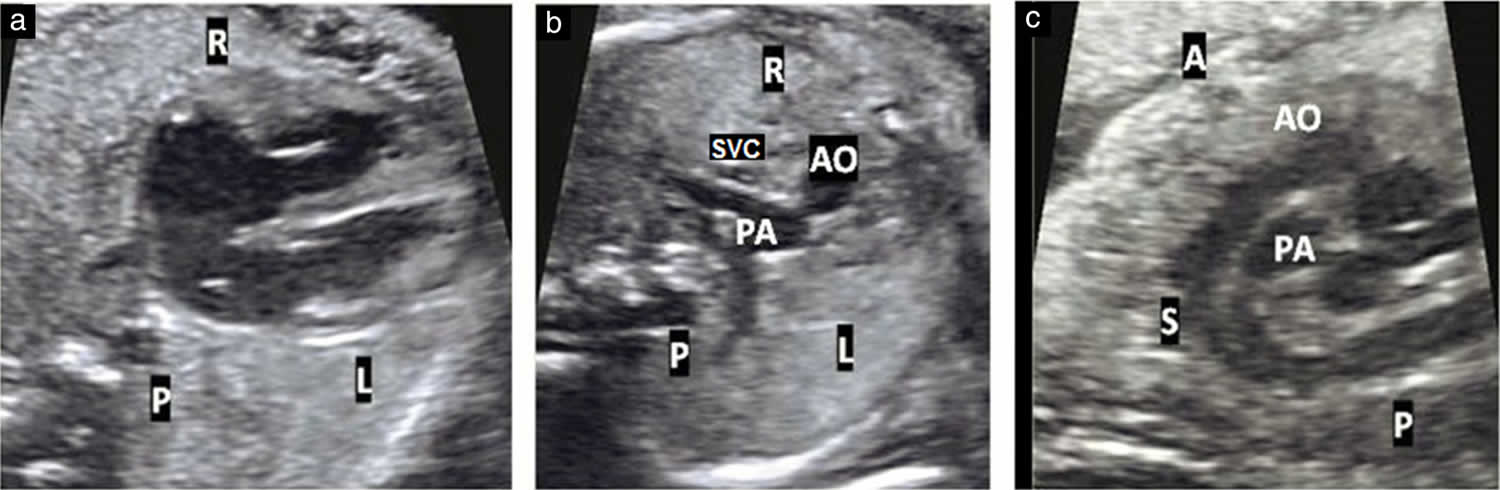
Footnotes: Ultrasound images of 22-week fetus showing: (a) normal four-chamber view including normal cardiac axis; (b) abnormal three-vessel view with triangular shape, with an anterior and rightward aorta (AO), posterior and leftward pulmonary artery (PA) and rightward and posterior superior vena cava (SVC); and (c) that both vessels do not cross but rather are seen coursing parallel to each other in their long axis.
Abbreviations: A = anterior; L= left; P = posterior; R = right; S = superior.
[Source 11 ]Figure 7. Transposition of the great arteries X-ray
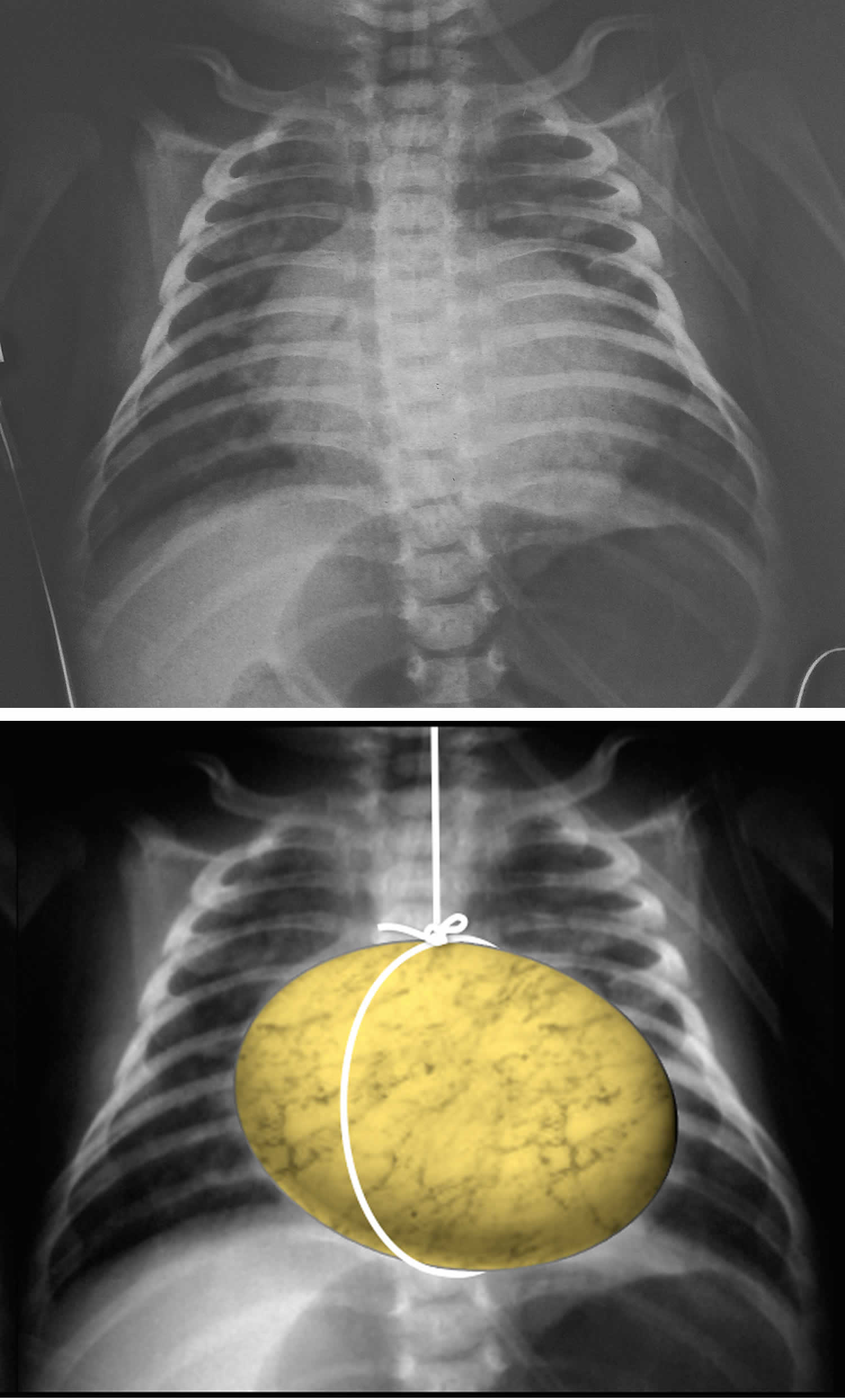
Footnotes: There is globular or ovoid appearance of the heart with apparent narrowing of the superior mediastinum (egg-on-a-string sign). Egg-on-a-string sign also referred to as egg on its side refers to the cardiomediastinal silhouette seen in transposition of the great arteries (TGA) 12. The heart appears globular due to an abnormal convexity of the right atrial border and left atrial enlargement and therefore appears like an egg. The superior mediastinum appears narrow due to stress-induced thymic atrophy and hyperinflated lungs which give the picture of an egg suspended by a string on a chest radiograph, hence the name egg-on-a-string.
[Source 13 ]Pregnancy and transposition of the great arteries
If you had transposition of the great arteries and want to become pregnant, talk with your heart specialist. It may be possible to have a healthy pregnancy. But special care may be needed.
Complications of transposition of the great arteries, such as changes in heart signaling, may make pregnancy risky. Pregnancy isn’t recommended for people who have severe complications of transposition of the great arteries, even if they had surgery to fix the heart condition.
A systematic review was performed on studies between 2000 and 2021 that identified 676 pregnancies in 444 women with transposition of the great arteries 14. A total of 556 pregnancies in women with atrial switch operation were tolerated by most cases with low mortality (0.6%). Most common maternal complications, however, were arrhythmias (9%) and heart failure (8%) associated with serious morbidity in some patients. Worsening functional capacity, right ventricular function, and tricuspid regurgitation occurred in ≈20% of the cases. Rate of fetal and neonatal mortality was 1.4% and 0.8%, respectively, and rate of prematurity was 32%. A total of 120 pregnancies in women with arterial switch operation were associated with no maternal mortality, numerically lower rates of arrhythmias and heart failure (6% and 5%, respectively), significantly lower rate of prematurity (11%; P<0.001), and only 1 fetal loss.
Pregnancy is tolerated by most women with transposition of the great arteries and atrial switch operation with low mortality but important morbidity. Most common maternal complications were arrhythmias, heart failure, worsening of right ventricular function, and tricuspid regurgitation. There was also a high incidence of prematurity and increased rate of fetal loss and neonatal mortality. Outcome of pregnancy in women after arterial switch operations is more favorable, with reduced incidence of maternal complications and fetal outcomes similar to women without underlying cardiac disease.
Transposition of the great arteries types
There are 2 types of transposition of the great arteries 1:
Transposition of the great arteries (TGA)
Transposition of the great arteries (TGA) also called dextro-transposition of the great arteries (D-TGA) or transposition of the great vessels (TGV) is a rare life-threatening heart birth defect (congenital heart defect) where the aorta and pulmonary artery are reversed or transposed, connecting to the wrong ventricles so that each one carries blood to the wrong location, creating separate, unmixed blood circuits. This leads to oxygen-poor blood being sent to the body and oxygen-rich blood to the lungs, causing symptoms like a blueish skin color (cyanosis) and requiring urgent surgical treatment. In a normal heart, one of two great arteries, known as the main pulmonary artery, brings oxygen-poor blood (blood that’s low in oxygen) from the right ventricle to the lungs, where it becomes oxygenated (oxygen-rich). Another great artery, the aorta, carries oxygen-rich blood from the left ventricle to the rest of the body. In an individual with transposition of the great arteries (TGA), the placement of the arteries, the aorta and pulmonary artery, is reversed, so that oxygen-poor blood, which should go through the main pulmonary artery from the right ventricle to the lungs to pick up oxygen, goes through the aorta instead, sending unoxygenated blood to the body. Similarly, oxygen-rich blood that is supposed to travel through the aorta instead enters the main pulmonary artery, sending oxygenated blood back to the lungs. This creates two separate circuits, the pulmonary and systemic circulations are separate and independent of each other, that is, they are in parallel, like two separate rings with no mixing of oxygenated and deoxygenated blood, which is incompatible with life. Transposition of the great arteries (TGA) is often diagnosed during pregnancy or soon after birth. Without treatment, serious complications or death can happen.
An isolated transposition of the great arteries (TGA) is incompatible with life at birth without one of the following additional anomalies, which are a common occurrence 15:
- Atrial septal defect (ASD): uncommon
- Ventricular septal defect (VSD): ~35%
- Patent ductus arteriosus (PDA): unstable due to closure following birth
- Patent foramen ovale (PFO): unstable
Unstable associations account for 60-65% of occurrences.
About 1,200 babies in the United States are born with transposition of the great arteries or transposition of the great vessels each year, accounting for about 3% of all congenital heart conditions and 20% of cyanotic heart diseases 2. Scientists don’t know the exact cause of transposition of the great arteries (TGA), but it’s thought to be multifactorial related to genetic factors and exposure to certain toxins during pregnancy, such as gestational diabetes.
Surgical repair for dextro-transposition of the great arteries (D-TGA) should be performed within the first week of life. The two most commonly used procedures are the standard atrial switch operation (ASO) and the Rastelli procedure, which is recommended for patients with dextro-transposition of the great arteries (D-TGA), a large ventricular septal defect (VSD), and pulmonary stenosis. Studies report a survival rate exceeding 95% at 15 to 25 years post-discharge 16, 17. Other corrective procedures, such as the Mustard, Senning, Nakaidoh, and REV, are available but less commonly performed.
Congenitally corrected transposition of the great arteries (ccTGA)
Congenitally corrected transposition of the great arteries (ccTGA) also called levo-transposition of the great arteries (L-TGA) the two lower heart chambers are reversed, resulting in both atrioventricular and ventriculoarterial discordance or “double discordance” where the ventricles are not properly aligned with their corresponding atria.
- The lower left heart chamber, called the left ventricle, is on the heart’s right side. It gets blood from the upper right heart chamber.
- The lower right heart chamber is on the heart’s left side. It gets blood from the left upper heart chamber.
- The blood usually still flows the right way through the heart and body. But the heart can have long-term trouble pumping blood.
Congenitally corrected transposition of the great arteries (ccTGA) is a less common type. Congenitally corrected transposition of the great arteries (ccTGA) occurs in about 0.05% of all congenital heart disease cases, with an estimated incidence of approximately 1 in every 33,000 live births 8. An international study examining the largest cohort of congenitally corrected transposition of the great arteries (ccTGA) cases identified nonsporadic occurrences, including familial clusters. The study also found associations between congenitally corrected transposition of the great arteries (ccTGA), dextro-transposition of the great arteries (D-TGA), laterality defects, and, in some instances, primary ciliary dyskinesia. These findings suggest a potential common pathogenetic pathway involving laterality genes in the development of congenitally corrected transposition of the great arteries (ccTGA) 9.
Congenitally corrected transposition of the great arteries (ccTGA) is highly variable and can present with a range of anatomical features and clinical manifestations.
The presence or absence of associated heart anomalies alters the natural history of congenitally corrected transposition of the great arteries (ccTGA). Patients may have one or more associated heart anomalies which include:
- Ventricular septal defect (VSD)
- Pulmonary stenosis
- Pulmonary atresia
- Systemic atrioventricular (tricuspid) valve abnormalities
- occurs in up to to 90% of patients 18
- inferior displacement of the valve closer to the cardiac apex
- Abnormal conduction system
- unusual position and course of the AV node and bundle of His
- dual AV nodes
- complete AV block and paroxysmal supraventricular tachycardia
- Mirror-image coronary artery distribution
- right coronary artery supplying the anterior descending branch and gives rise to a circumflex branch
- left coronary artery resembles a right coronary artery
- Situs inversus a rare genetic birth defect where internal organs in the chest and abdomen are arranged in a mirror image of their normal positions 20, 21, 22, 23. The most common form, situs inversus totalis, involves all major visceral organs, such as the heart, liver, stomach, and spleen, being reversed. This condition can go unnoticed or be discovered incidentally, and while many individuals live without complications, it poses unique challenges during medical procedures due to the altered anatomy.
Patients are usually asymptomatic when congenitally corrected transposition of the great arteries (ccTGA) is not associated with other heart anomalies or complications. Patients may present with congestive heart failure if there is an associated large ventricular septal defect (VSD) or with cyanosis if with associated VSD and pulmonary stenosis 24. If congenitally corrected transposition of the great arteries (ccTGA) is complicated by right ventricular or tricuspid valve dysfunction, patients can present with exertional dyspnea and easy fatigability. Those without such complications may not be identified until adulthood 24.
Patients with congenitally corrected transposition of the great arteries (ccTGA) may have problems with heart muscle, tricuspid valve leakage or heart rhythm as they enter adulthood, whether or not they had prior surgery. Like patients with atrial repair of dextro-transposition of the great arteries (D-TGA), the right ventricle may weaken, leading to congestive heart failure. Abnormally slow heart rhythms may cause fainting or fatigue. The most worrisome slow heart rhythm, complete heart block, is common in congenitally corrected transposition of the great arteries (ccTGA). Rapid heart rhythms are less common than in dextro-transposition of the great arteries (D-TGA).
Congenitally corrected transposition of the great arteries (ccTGA) treatment depends on the specific heart structure and if there are other heart conditions.
Most children without a ventricular septal defect (VSD) or pulmonary valve obstruction won’t need surgery. Children with these problems may require surgery to close the hole, relieve the blockage of blood flow to the lungs, and in some cases repair or replace the leaky tricuspid valve. In patients with ventricular septal defects (VSDs), it may be recommended to undergo a more complex surgical procedure known as a “double switch” which reroutes the oxygen rich blood to the left ventricle and aorta and oxygen poor blood to the right ventricle and pulmonary artery.
Medications to help the heart pump better, control fluid accumulation (diuretics) and control blood pressure may help with congestive heart failure symptoms. A pacemaker may be required in the event of abnormally slow heart rhythms. You should also consult a cardiologist with expertise in caring for adults with congenital heart disease if you are undergoing any type of non-heart surgery or invasive procedure.
Routine evaluation may include an EKG, echocardiogram, Holter monitor and stress testing. Your cardiologist may recommend other testing such as an MRI or heart catheterization.
Many patients don’t need to limit their activity, except to avoid activities like weight lifting that cause a rise in blood pressure. However, if your child’s heart doesn’t pump normally or if you have heart rhythm issues, you may need to limit your activity to your endurance. Your cardiologist will help determine if your child needs to limit your activity.
People who have levo-transposition of the great arteries (L-TGA) may require endocarditis prophylaxis if they have a prosthetic valve. In the majority of patients, there is no prosthetic valve and the cardiologist will be able to determine if the patient needs to keep taking routine antibiotics before certain dental work.
Transposition of the great arteries causes
The cause for transposition of the great arteries (TGA) is unknown and is presumed to be multifactorial 25. The embryology likely involves abnormal persistence of the subaortic conus with resorption or underdevelopment of the subpulmonary conus (infundibulum). This abnormality aligns the aorta anterior and superior with the right ventricle during development.
Some cases of transposition of the great arteries have been linked to rare mutations in specific genes, however, the genetic basis for most cases remains unclear. The pattern of familial recurrence, along with the sporadic nature of the majority of transposition of the great arteries cases, suggests polygenic inheritance 26.
Risk factors for developing transposition of the great arteries
Possible risk factors for congenital heart defects such as transposition of the great arteries include:
- Rubella also called German measles. Having rubella during pregnancy can cause changes in an unborn baby’s heart development. A blood test done before pregnancy can determine if you’re immune to rubella. A vaccine is available if you aren’t.
- Certain medicines. Taking certain medicines during pregnancy can cause congenital heart defects and other health conditions present at birth. Always tell your doctor about the medicines you take.
- Alcohol use. Drinking alcohol during pregnancy raises the risk of congenital heart defects in the baby.
- Smoking. If you smoke, quit. Smoking during pregnancy can be harmful to the unborn baby, also called a fetus.
- Diabetes. Careful control of blood sugar before and during pregnancy can reduce the risk of congenital heart defects in the baby. Diabetes that develops during pregnancy is called gestational diabetes.
Transposition of the great arteries prevention
Because the exact cause of most congenital heart defects is not known, it may not be possible to prevent these conditions. If you have a family history of heart conditions present at birth, talk with a genetic counselor and a healthcare professional trained in congenital heart defects before getting pregnant.
It’s important to take steps to have a healthy pregnancy. Get proper prenatal care. Before becoming pregnant, get recommended immunizations. Start taking a multivitamin with folic acid. Folic acid has been shown to prevent harmful changes in the unborn baby’s brain and spinal cord. It also may help reduce the risk of congenital heart defects.
Transposition of the great arteries signs and symptoms
Symptoms of transposition of the great arteries (TGA) or transposition of great vessels include:
- Blue or gray skin (cyanosis) due to low oxygen levels. Depending on skin color, these color changes may be harder or easier to see.
- Problems breathing.
- Pounding heartbeat.
- Weak pulse.
- Lack of appetite or poor feeding
- Poor weight gain.
Some people with the congenitally corrected transposition of the great arteries (ccTGA) may not have symptoms for many years. Individuals with congenitally corrected transposition of the great arteries (ccTGA) and major accompanying heart defects such as pulmonary stenosis or ventricular septal defect (VSD), are often diagnosed early in life, while those without such complications may not be identified until adulthood 24.
Also, skin color changes may not be seen right away if a baby with transposition of the great arteries also has other heart changes that let some oxygen-rich blood move through the body. But as the baby becomes more active, less oxygen-rich blood flows through the body. The changes in skin color become more noticeable as oxygen levels drop.
Transposition of the great arteries
The clinical features of dextro-transposition of the great arteries (D-TGA) depend solely on the degree of mixing between the parallel circuits. Most newborns present with signs and symptoms during the neonatal period or within the first 30 days of life. Typical clinical signs and symptoms include the below conditions.
- Cyanosis: The severity of cyanosis depends on the degree of intracardiac mixing between the two parallel circuits, which is influenced by the size and presence of an atrial septal defect (ASD) or ventricular septal defect (VSD). Cyanosis typically does not change with exertion or supplemental oxygen 27.
- Tachypnea: Patients often exhibit a respiratory rate exceeding 60 breaths per minute, but they do not show signs of retractions, grunting, or nasal flaring. Despite the elevated rate, they typically appear comfortable.
- Heart sounds: The first heart sound (S1) generally has normal intensity, as ventricular contraction remains unaffected. The second heart sound (S2) is often more pronounced and may be single, attributed to the anterior positioning of the aorta.
- Murmurs: Murmurs are usually absent unless a small ventricular septal defect (VSD) or pulmonary stenosis is present. When a ventricular septal defect (VSD) is involved, it produces a pansystolic murmur that is prominent at the lower left sternal border. In the case of pulmonary stenosis, a systolic ejection murmur is heard at the upper left sternal border 28.
Babies with dextro-transposition of the great arteries (D-TGA) who have a large, nonrestrictive ventricular septal defect (VSD) will be only mildly cyanotic during exertion and tend to present after a few weeks with symptoms of heart failure, such as:
- sweating
- irritability
- poor weight gain
- decreased activity levels
Physical examination may reveal a right ventricular heave, a thrill at the left lower sternal border, and if left ventricular outflow tract obstruction is present a systolic murmur at the upper sternal border may be appreciated. A pathognomonic feature, albeit rare, on the physical exam would be cyanosis manifest in the upper extremities with normal-appearing, acyanotic lower extremities. This is referred to as reverse differential cyanosis, and will only occur in dextro-transposition of the great arteries (D-TGA) which coexists with a patent ductus arteriosus as well as either an interrupted aortic arch or coarctation of the aorta.
Congenitally corrected transposition of the great arteries (ccTGA)
Newborns are usually asymptomatic when congenitally corrected transposition of the great arteries (ccTGA) is not associated with other heart anomalies or complications. The congenitally corrected transposition of the great arteries (ccTGA) may go undetected for a long time. It might not be diagnosed until well into adulthood when congestive heart failure, heart murmurs and abnormal heart rhythms can develop. Patients may present with congestive heart failure if there is an associated large ventricular septal defect (VSD) or with cyanosis if with associated VSD and pulmonary stenosis 24. If congenitally corrected transposition of the great arteries (ccTGA) is complicated by right ventricular or tricuspid valve dysfunction, patients can present with exertional dyspnea and easy fatigability. Those without such complications may not be identified until adulthood 24.
Transposition of the great arteries complications
Untreated transposition of the great arteries can result in congestive heart failure, life-threatening arrhythmias, and death. Not enough oxygen to body tissues. Unless there’s some mixing of oxygen-rich blood and oxygen-poor blood within the heart, this complication causes death.
Complications depend on the type of transposition of the great arteries. Possible complications of complete transposition of the great arteries may arise from surgical procedures for transposition of the great arteries include:
- Arrhythmias 29
- Complete heart block. Transposition of the great arteries can change the way electrical signals move through the heart and tell the heart to beat. A complete heart block occurs if all signals are blocked.
- Heart valve disease. In congenitally corrected transposition of the great arteries (ccTGA), the heart valve between the upper and lower heart chambers, called the tricuspid valve, may not close all the way. Blood might flow backward. This condition is called tricuspid valve regurgitation. It can make it harder for the heart to pump blood.
- Heart failure. The heart can’t pump enough blood to meet the body’s needs. Heart failure may happen over time in congenitally corrected transposition of the great arteries (ccTGA) because the right lower heart chamber is pumping under higher pressure than usual. The strain may make the muscle of the right lower chamber weak.
- Obstruction or leakage of the baffle (following a Rastelli procedure)
- Pulmonary artery stenosis
- Coronary artery stenosis
- Aortic root dilation
- Aortic valve regurgitation 30
- Rare cases of supravalvular aortic stenosis as a late complication of transposition of the great arteries have been reported 31.
Timely intervention and regular follow-up care can help minimize complications and improve outcomes for patients with transposition of the great arteries.
Transposition of the great arteries diagnosis
Transposition of the great arteries or transposition of great vessels is often diagnosed before birth during a routine pregnancy ultrasound 32, 33, 34, 35, 36. If not, it is diagnosed soon after birth. Dextro-transposition of the great arteries (d-TGA) can be diagnosed in utero using specialized views of the outflow tracts during fetal ultrasound 37. However, transposition of the great arteries is challenging to detect on fetal ultrasound due to the lack of size differences between the ventricles.
Immediately after birth, your baby’s doctor will listen to your baby’s heart and lungs. A whooshing heart sound, called a murmur, may be heard while listening to the baby’s heart. Some murmurs are caused by blood flow changes to and from the heart.
Babies with transposition of the great arteries (TGA) are usually born at term, with cyanosis apparent within hours of birth. The clinical course and manifestations depend on the extent of intercirculatory mixing and the presence of associated anatomic lesions. Note the following:
- Transposition of the great arteries with intact ventricular septum: Prominent and progressive cyanosis within the first 24 hours of life is the usual finding in infants if no significant mixing at the atrial level is evident.
- Transposition of the great arteries with large ventricular septal defect: Infants may not initially manifest symptoms of heart disease, although mild cyanosis (particularly when crying) is often noted. Signs of congestive heart failure (tachypnea, tachycardia, diaphoresis, and failure to gain weight) may become evident over the first 3-6 weeks as pulmonary blood flow increases.
- Transposition of the great arteries with ventricular septal defect and left ventricular outflow tract obstruction: Infants often present with extreme cyanosis at birth, proportional to the degree of left ventricular (pulmonary) outflow tract obstruction. The clinical history may be similar to that of an infant with tetralogy of Fallot.
- Transposition of the great arteries with ventricular septal defect and pulmonary vascular obstructive disease: Progressively advancing pulmonary vascular obstructive disease can prevent this rare subgroup of patients from developing symptoms of congestive heart failure, despite a large ventricular septal defect. Most often, patients present with progressive cyanosis, despite an early successful palliative procedure.
Tests to diagnose transposition of the great arteries include:
- Echocardiogram. Sound waves make images of the beating heart. An echocardiogram shows how blood moves through the heart and heart valves. It can tell if the two main arteries leaving the heart are in the correct position. If the test is done on an unborn baby before birth, it’s called a fetal echocardiogram.
- Transthoracic echocardiography is the primary imaging modality for transposition of the great arteries, providing essential information on the morphology, function, and hemodynamics of the ventricles and valves 38.
- Chest X-ray. This test shows the condition of the heart and lungs. The classic radiographic feature of transposition of the great arteries is the “egg on a string” or “egg on its side” appearance 39.
- Egg-on-a-string sign also referred to as egg on its side refers to the cardiomediastinal silhouette seen in transposition of the great arteries (TGA) 12. The heart appears globular due to an abnormal convexity of the right atrial border and left atrial enlargement and therefore appears like an egg. The superior mediastinum appears narrow due to stress-induced thymic atrophy and hyperinflated lungs which give the picture of an egg suspended by a string on a chest radiograph, hence the name egg-on-a-string.
- Electrocardiogram (ECG or EKG). This simple test shows how the heart is beating. Sticky patches with sensors on them go on the chest and sometimes the arms and legs. Wires connect the sensors to a computer, which prints or displays the test results. Electrocardiography usually appears normal but may demonstrate right-axis deviation and right ventricular hypertrophy (RVH). Several criteria, primarily based on the R and S wave amplitudes in leads I, V1, and V6, along with the R-wave peak time in V1, have been established for diagnosing right ventricular hypertrophy (RVH).
- Pulse oximetry. A sensor placed on the fingertip records the amount of oxygen in the blood. Too little oxygen may be a sign of a heart or lung condition.
- Cardiac catheterization is a procedure where a thin tube called a catheter is inserted into a blood vessel and guided to the heart to diagnose and treat heart conditions. During the procedure, a dye is injected to provide X-ray images of the coronary arteries, revealing blockages. Catheterization can also measure heart pressures, assess blood flow, and be used for interventional procedures like placing stents to open narrowed arteries or treat other heart defects.
- Catheterization is rarely used to diagnose transposition of the great arteries but remains the gold standard for determining the origins of the coronary arteries. Cardiac catheterization is routinely utilized in dextro-transposition of the great arteries (D-TGA) to perform balloon atrial septostomy in patients with severe cyanosis and may also assist in identifying coronary arteries 40.
- Chest computed tomography imaging: Computed tomography (CT) is often used in postsurgical patients who cannot undergo magnetic resonance imaging (MRI) due to contraindications or the presence of devices that may cause artifacts, such as pacemakers in individuals who have had an atrial switch operation (ASO) 41. CT imaging provides detailed information on the morphology of cardiovascular structures, including baffles, conduits, and coronary arteries 42. Although CT can provide quantification of ventricular function, it does not assess hemodynamics or blood flow 43.
- Cardiac magnetic resonance imaging: MRI offers detailed information on the anatomy and hemodynamics of cardiovascular structures, including baffles and conduits, and allows for the quantification of ventricular size, function, and valvular performance 44. Although invasive angiography was historically the primary method for assessing coronary arterial anatomy, CT and MRI can now effectively evaluate the coronary arteries. The MRI protocol is typically tailored to the patient’s specific clinical needs. Furthermore, with appropriate safety measures and image optimization, MRI can be safely performed in patients with various cardiac implantable devices 45.
Physical Examination
Newborns with transposition of the great arteries (TGA) are usually well developed, without dysmorphic features. Physical findings at presentation depend on the presence of associated lesions. Note the following:
- Transposition of the great arteries with intact ventricular septum: Infants typically present with progressive central (perioral and periorbital) cyanosis. Other than cyanosis and a loud, single second heart sound (S2), the physical examination is often unremarkable.
- Transposition of the great arteries with large ventricular septal defect: Cyanosis may be mild initially, although it is usually more apparent with stress or crying. Upon presentation, infants often have an increased right ventricular impulse; a loud, single second heart sound (S2); usually no systolic murmurs; possibly a mid-diastolic rumble; and gallop rhythm. Hepatomegaly may be present.
- Transposition of the great arteries with ventricular septal defect and left ventricular outflow tract obstruction: Cyanosis is prominent at birth, and the findings are similar to those of infants with tetralogy of Fallot. A single second heart sound (S2) and a systolic ejection murmur may be present. Hepatomegaly is rare.
- Transposition of the great arteries with ventricular septal defect and pulmonary vascular obstructive disease: Progressive pulmonary vascular obstructive disease is not always evident from physical examination findings. A loud, single second heart sound (S2) is present. Cyanosis is usually present and can progress despite palliative therapy in the newborn period.
Transposition of the great arteries treatment
Transposition of the great arteries treatment depends on the type of transposition of the great arteries. All babies with complete transposition of the great arteries or dextro-transposition of the great arteries (d-TGA) need surgery soon after birth (usually within the first week of life) to fix the heart in order to survive 46, 47..
Treatment for congenitally corrected transposition of the great arteries (ccTGA) or levo-transposition of the great arteries (L-TGA) depends on:
- When the condition is diagnosed.
- What other heart conditions exist.
The initial step in treatment is to allow oxygen-rich blood to mix with poorly oxygenated blood. The baby will immediately receive a medicine called prostaglandin through an IV (intravenous line). This medicine helps keep a blood vessel called the ductus arteriosus open, allowing some mixing of the two blood circulations. In some cases, an opening between the right and left atrium can be created with procedure using a balloon catheter. This allows blood to mix. This procedure is known as balloon atrial septostomy.
Many infants undergo a procedure in the balloon atrial septostomy (BAS) to “buy time” and delay the heart surgery until they can handle it better. The balloon atrial septostomy procedure enlarges a naturally occurring connection between the right and left upper chambers (the atria). This lets the blood mix so some oxygen-rich and oxygen-poor blood can be pumped to the correct side.
Permanent treatment involves major heart surgery during which the great arteries are cut and stitched back to their correct position. This is called an arterial switch operation (ASO). Prior to the development of this surgery, a surgery called an atrial switch or Mustard procedure or Senning procedure was used. Now, the Mustard procedure or Senning procedure is currently reserved for very rare cases.
Arterial Switch Operation (ASO): The aorta and pulmonary artery are switched back to their normal positions. The aorta is connected to the left ventricle, and the pulmonary artery is connected to the right ventricle. The coronary arteries, which carry the oxygen-rich blood that nourishes the heart muscle, also need to be reattached to the new aorta. The baby’s symptoms will improve after the heart surgery to correct the defect. Most infants who undergo arterial switch operation do not have symptoms after surgery and live normal lives. If corrective surgery is not performed, the life expectancy is only months.
Atrial Switch Operation commonly known as Mustard procedure or Senning procedure creates a tunnel (baffle) between the atria (atrial baffle). During Atrial Switch Operation, the aorta and pulmonary artery are left in place. However, a tunnel (baffle) is created between the top chambers (atria) of the heart. This redirects the oxygen-rich blood to the right ventricle and aorta and the oxygen-poor blood to the left ventricle and the pulmonary artery. Although this repair helps blood to go to the lungs and then out to the body, it also makes extra work for the right ventricle to pump blood to the entire body. Therefore, this repair can lead to difficulties later in life.
Other corrective procedures include the Nikaidoh, Réparation à l’Etage Ventriculaire (REV), and Yasui procedures, although these are less commonly performed 48.
After surgery, medications may be needed to:
- Help the heart pump better
- Control blood pressure
- Help get rid of extra fluid in the body
- Slow down the heart if it is beating too fast
If the heart is beating too slowly, a pacemaker can be used.
Transposition of the great arteries medication
Before heart repair surgery (particularly those with severe left ventricular outflow tract obstruction), the baby may get a medicine through an intravenous line (IV) called prostaglandin (Prostin Vr Pediatric). Continuous intravenous (IV) prostaglandin E1 (alprostadil) infusion promotes pulmonary blood flow, increase left atrial pressure, and promote left-to-right intercirculatory mixing of oxygen-poor and oxygen-rich blood at the atrial level. This is particularly important in patients with severe left ventricular outflow tract stenosis or atresia. Administration of prostaglandin E1 (PgE1) within the first 48 hours after birth is crucial to reduce early mortality in newborns with transposition of the great arteries, especially in the dextro-transposition of the great arteries (d-TGA) 49, 50.
Cardiac catheterization and balloon atrial septostomy is indicated in severely hypoxemic newborns with an inadequate atrial level communication and insufficient mixing (preductal saturations significantly lower than postductal saturations). Balloon atrial septostomy is used to increase the atrial level shunt and to improve mixing.
For the ill neonate, metabolic acidosis should be corrected with fluid replacement and bicarbonate administration.
Mechanical ventilation may be necessary if pulmonary edema develops in concert with severe hypoxemia.
After surgery to fix transposition of the great arteries, medicines are given to help the heart work better. Medicines may be needed to:
- Control the heartbeat. Slow down the heart if it is beating too fast
- Manage blood pressure.
- Help the body remove fluid.
- Help the heart pump better
Patients with transposition of the great arteries and ventricular septal defect who have not undergone surgical repair, and some patients following complete repair, might potentially benefit from digoxin and diuretic therapy to improve systemic ventricular function and avoid fluid retention.
All transposition of the great arteries patients require antibiotic prophylaxis prior to dental and indicated surgical procedures in order to reduce the risk of subacute bacterial endocarditis 3. Therefore, all patients require preoperative and postoperative antibiotic prophylaxis for dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa. Antibiotic prophylaxis is also recommended for invasive respiratory tract procedures that involve incision or biopsy of the respiratory mucosa (eg, tonsillectomy, adenoidectomy). Antibiotic prophylaxis is not recommended for bronchoscopy unless the procedure involves incision of the respiratory tract mucosa. For invasive respiratory tract procedures to treat an established infection (eg, drainage of abscess, empyema), administer an antibiotic active against Streptococcus viridans.
If the heart is beating too slowly, a pacemaker can be used.
Mustard procedure or Senning procedure
The first atrial switch procedure was performed by Senning in 1958 and involves the creation of an atrial tunnel (atrial baffle) using the atrial septum rather than using pericardium or synthetic material to direct the venous return to the contralateral atrioventricular (AV) valve and ventricle 51. During atrial switch procedure, the aorta and pulmonary artery are left in place. However, a tunnel (baffle) is created between the top chambers (atria) of the heart. This redirects the oxygen-rich blood to the right ventricle and aorta and the oxygen-poor blood to the left ventricle and the pulmonary artery. The deoxygenated blood from the vena cavae is directed to the mitral valve and left ventricle (LV) and thence to the pulmonary artery, and pulmonary venous blood is directed into the morphological right ventricle (RV) and into the aorta. Although this repair helps blood to go to the lungs and then out to the body, it also makes extra work for the right ventricle to pump blood to the entire body. Therefore, this repair can lead to difficulties later in life.
An alternative operation was subsequently developed by Mustard, who excised the atrial septum and used synthetic material to create the baffle 52. Sometimes an atrial switch is preceded by either the Rashkind balloon atrial septostomy or surgical atrial septectomy (Blalock-Hanlon) 53. Both atrial switch procedures provide excellent midterm clinical results but in the long term are associated with important complications.
Significant concerns exist regarding the ability of the anatomical right ventricle to sustain systemic circulation in patients with transposition of the great arteries who have undergone the Mustard procedure. In Mustard procedure, the anatomical right ventricle becomes the systemic ventricle, responsible for pumping blood into the main artery and managing pressures 3 to 4 times higher than those in the pulmonary circuit, leading to a considerable pressure load. Over time, the anatomical right ventricle often struggles to maintain systemic circulation, leading to a gradual decline in the clinical condition of patients following Mustard repair 54. These late complications are associated with poor outcomes, emphasizing the importance of timely intervention.
Additionally, conduction and electrical stimulation disorders are common complications in adults who have undergone intraatrial surgery for dextro-transposition of the great arteries (D-TGA). These issues may arise from congenital anomalies of the sinus node and conductive fibers, damage to these structures during surgery, or injury to the coronary arteries supplying these areas. Over time, the inevitable degeneration of tissues also contributes to these complications. Notably, only 40% to 50% of patients who underwent the Senning procedure maintain sinus rhythm after 20 years of follow-up 55.
Figure 8. Mustard procedure
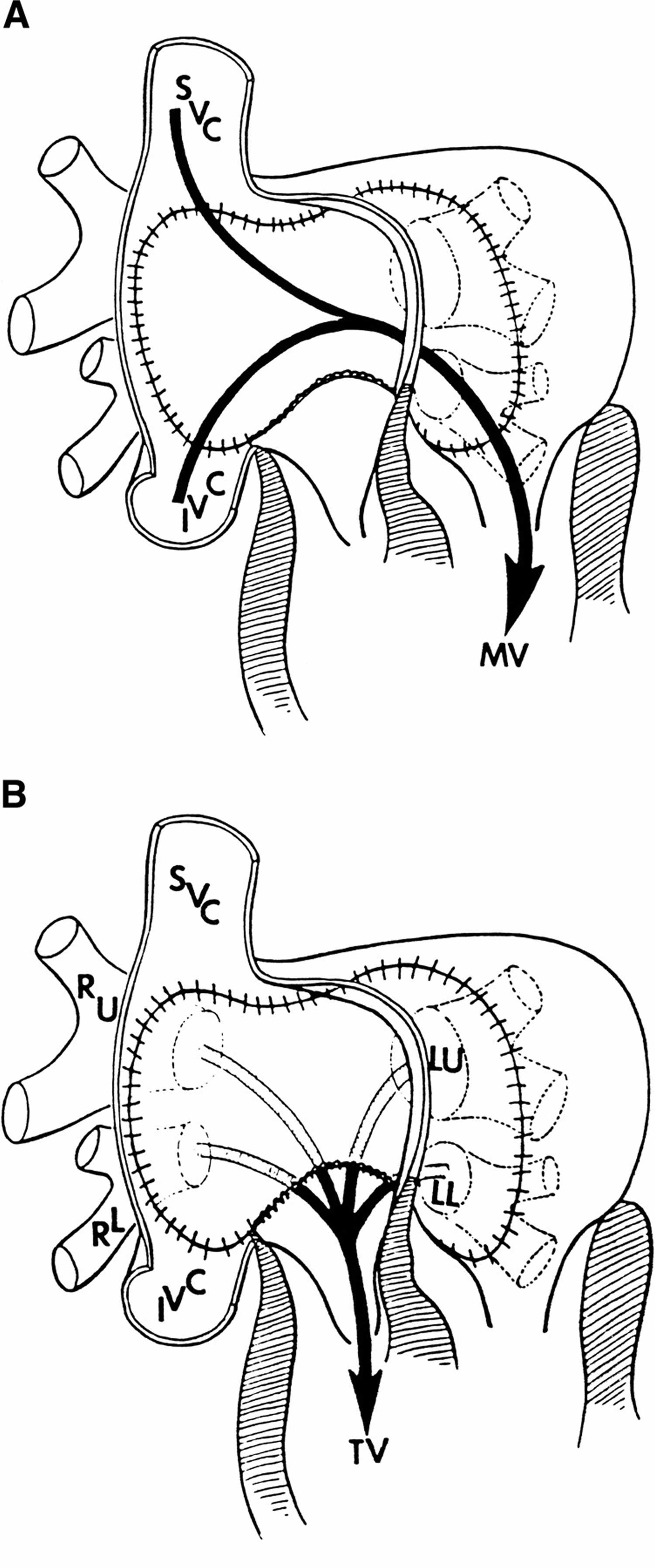
Footnotes: Mustard procedure. (A) An atrial baffle diverts blood from both the superior vena cava and the inferior vena cava across to the mitral valve (MV) and left ventricle (LV), which ejects blood to the pulmonary artery. (B) The pulmonary venous blood is returned to the tricuspid valve and right ventricle (RV), which ejects blood into the aorta.
Abbreviations: IVC = inferior vena cava; LL = left lower pulmonary vein; LU = left upper pulmonary vein; MV = mitral valve; RL = right lower pulmonary vein; RU = right upper pulmonary vein; SVC = superior vena cava; and TV = tricuspid valve.
[Source 56 ]Arterial switch operation
The arterial switch operation is now the standard procedure than either the Mustard or Senning repairs for patients with dextro-transposition of the great arteries (D-TGA) who do not have major pulmonic stenosis. The arterial switch procedure functionally provides an arterial rather than an atrial “switch” and anatomically corrects the abnormality. This is done partly to avoid the long-term complication of arrhythmia. During the arterial switch procedure, the surgeon transects the pulmonary trunk and aorta, repositioning these vessels to their correct anatomical locations. The coronary arteries are mobilized and reimplanted into the aortic trunk. Following this, a Lecompte maneuver is performed after implanting the coronary vessels into the proximal portion of the pulmonary trunk, which is now referred to as the neoaorta. This maneuver repositions the pulmonary trunk, originally located behind the aorta, to a new position in front of the ascending aorta. Additionally, any existing ventricular septal defect (VSD) is repaired during this procedure 57.
Following an arterial switch procedure, the outflow tracts must be meticulously identified during echocardiographic evaluation to assess for potential supravalvar narrowing and neovalvar regurgitation. This evaluation should utilize subxiphoid, apical, and parasternal views, with the apical and parasternal perspectives being particularly effective for evaluating regional wall motion abnormalities. When evaluating the translocated coronary arteries, the parasternal short-axis view should be utilized with a very low color scale to enhance color flow detection. Doppler interrogation of the branch pulmonary arteries should be performed, particularly from a high parasternal vantage point.
For long-term follow-up, the neoaortic root should be measured using the parasternal long-axis view, while neoaortic and neopulmonary valve regurgitation should be assessed from multiple angles. Echocardiographic imaging can be challenging in adult patients post-arterial switch procedure, making additional cross-sectional imaging modalities such as CT scans or MRI necessary for accurate visualization of the pulmonary artery branches and coronary arteries 58.
Figure 9. Arterial switch operation
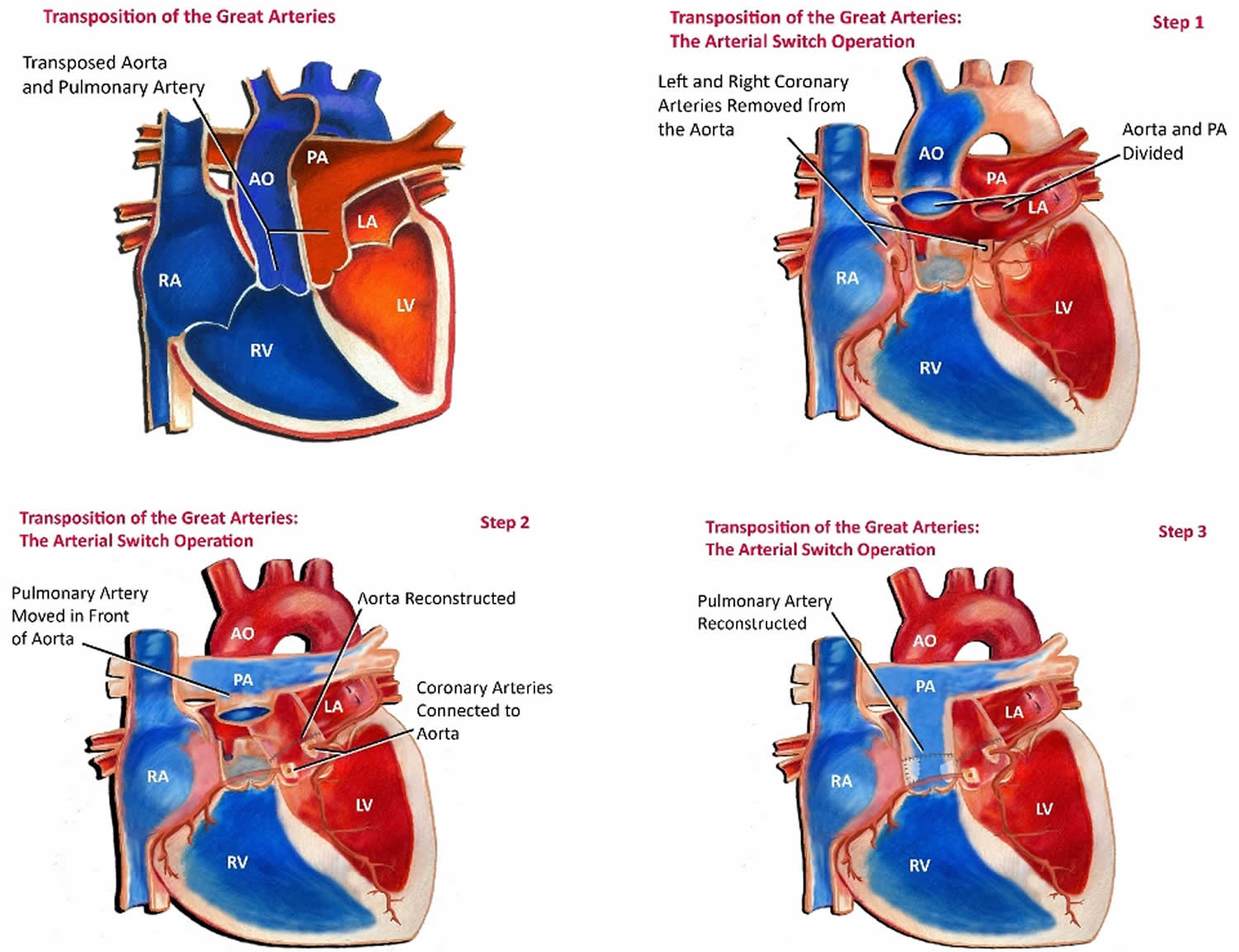
Footnotes: In most cases of dextro-transposition of the great arteries (D-TGA), an arterial switch operation is performed. The arterial switch operation involves cutting off the aorta and pulmonary arteries just above the point where they leave the heart, and reconnecting them to the proper ventricle. The valve stays attached to the ventricle, so that what was once the pulmonary valve is now the aortic valve and vice versa. Since the coronary arteries must stay with the aorta, they must be taken off the area above the valve and reimplanted separately above the new aortic valve. This is often the most technically challenging part of the operation, particularly if there is any unusual branching of these arteries. Closure of ventricular septal defects (if present) and atrial septal defects are also performed as part of the operation.
Abbreviations: PA = pulmonary artery; RA = right atrium; RV = right ventricle; AO = aorta; LA = left atrium; LV = left ventricle.
[Source 59 ]Rastelli procedure
In Rastelli procedure, an external right ventricle to the pulmonary artery (PA) conduit and an intraventricular left ventricle to the aorta via the ventricular septal defect (VSD) tunnel are created 60. The pulmonary valve may be atretic and is surgically closed at the time of the procedure 60. The Rastelli procedure is indicated for patients with dextro-transposition of the great arteries (D-TGA), a large ventricular septal defect (VSD), and pulmonary stenosis. In Rastelli procedure, the ventricular septal defect (VSD) is closed using a baffle, directing oxygenated blood from the left ventricle into the aorta. A conduit is then placed from the right ventricle to the pulmonary artery to shunt deoxygenated blood into the pulmonary artery 61.
Transposition of the great arteries surgery
Transposition of the great arteries surgical approach depends on the age of the patient at presentation, the presence of associated congenital heart lesions, and the experience of the cardiothoracic surgeon with a given surgical technique. Most full-term neonates with uncomplicated transposition of the great arteries can undergo an arterial switch procedure in one operation, with minimal mortality.
In patients with simple transposition of the great arteries, pulmonary blood flow gradually increases after birth, reaching nearly twice the normal level by 2 months of age. During the first few weeks of life, the left ventricular wall thickness decreases rapidly, a process known as left ventricular involution. Consequently, performing an arterial switch procedure on patients older than 2 weeks with transposition of the great arteries and an intact ventricular septum is considered risky, as numerous studies have shown 62.
In congenitally corrected transposition of the great arteries (ccTGA) or levo-transposition of the great arteries (L-TGA), the heart maintains a normal atrial position but has abnormal atrioventricular connections, resulting in reversed positions of the left and right ventricles. The anatomical left ventricle is located on the right side and connected to the pulmonary artery, while the anatomical right ventricle is on the left side and connected to the aorta. These structural abnormalities can disrupt the heart’s electrical system. Research indicates that approximately 30% of patients with congenitally corrected transposition of the great arteries (ccTGA) develop a complete atrioventricular block, potentially due to the anterior and superior displacement of the atrioventricular node or a conduction defect below the node 63.
For congenitally corrected transposition of the great arteries (ccTGA) or levo-transposition of the great arteries (L-TGA), a physiological repair strategy that preserves the right ventricle as the systemic ventricle is generally considered safe, but it often results in progressive congestive heart failure (CHF) over time. According to Graham et al 64, 67% of patients with congenitally corrected transposition of the great arteries (ccTGA) and associated abnormalities develop congestive heart failure by age 45. Hraska et al 65 report that the 10-year survival rate for individuals following physiological repair is only 68%. Anatomic repair is often considered unsuitable for older patients, especially those whose morphological left ventricles may not sustain systemic pressures or adequately respond to pulmonary artery band training 66. Additional factors predicting poor outcomes after anatomic repair include significant preexisting tricuspid regurgitation, right ventricular dysfunction, and the need for heart pacing 67.
Transposition of the great arteries with intact ventricular septum
The ideal operation is an arterial switch procedure. It represents an anatomic repair and establishes ventriculoarterial concordance. This procedure should be performed when the infant is younger than 4 weeks, as the left ventricle may not be able to handle systemic pressure postoperatively if left too long in the low-pressure, low-resistance pulmonary circuit. Rarely, however, depending on the particular coronary artery anatomy (eg, intramural coronary artery), coronary artery translocation may not be feasible, and an arterial switch is not recommended. In this subgroup, an atrial level switch (Senning or Mustard procedure) has lower surgical and short-term morbidity and mortality.
Transposition of the great arteries with ventricular septal defect
The preferred operation is an arterial switch procedure with ventricular septal defect closure (see the videos below). If the ventricular septal defect is large and nonrestrictive and coronary artery anatomy makes an arterial switch operation inadvisable, a Rastelli-type intracardiac repair may be feasible. In Rastelli procedure, an external right ventricle to the pulmonary artery (PA) conduit and an intraventricular left ventricle to the aorta via the ventricular septal defect (VSD) tunnel are created 60. The pulmonary valve may be atretic and is surgically closed at the time of the procedure 60. With the Rastelli-type procedure, waiting until the infant is older and larger may be preferred because of the need for a right ventricle–pulmonary artery conduit in the Rastelli operation. If the infant has excessive congestive heart failure (with growth failure), it may be advisable to either proceed with reparative surgery or, if not feasible, band the main pulmonary artery during the newborn period to restrict pulmonary blood flow.
Transposition of the great arteries with ventricular septal defect and left ventricular outflow tract obstruction
An arterial switch operation may not be feasible due to pulmonary valve (left ventricular outflow tract) stenosis or atresia. If the ventricular septal defect is nonrestrictive and remote from the aorta, a Rastelli intracardiac repair could be possible. Because the Rastelli procedure necessitates a conduit from the right ventricle to the pulmonary artery, delaying repair until the infant is older and larger may be preferable. In this case, placing an aortopulmonary shunt during the newborn period may be necessary to establish adequate pulmonary blood flow while waiting.
Transposition of the great arteries with ventricular septal defect and pulmonary vascular obstructive disease
These patients might not be appropriate surgical candidates because of the progressive increase in pulmonary vascular resistance. This is a small subgroup of patients whose conditions are not often diagnosed until after a palliative or reparative procedure is performed.
Transposition of the great arteries prognosis
Transposition of the great arteries prognosis depends on the specific anatomic substrate and type of surgical therapy used, arterial switch operation (ASO), atrial switch operation, or Rastelli procedure. The mortality (death) rate in untreated babies with transposition of great vessels is approximately 30% in the first week, 50% in the first month, and 90% by the end of the first year 68. Overall, perioperative survival following arterial switch operation (ASO) is greater than 90% 69. In one study, long-term and arrhythmia-free survival was excellent (approximately 97% at 25 years); late mortality was predominantly due to sudden death and heart attack 70. In another retrospective study, arrhythmias occurred in almost half of patients at a median age of 22 years, and 25% of patients received a pacemaker or implantable cardioverter‐defibrillator 71.
The overall mortality rate following an atrial level switch is low; however, long-term morbidity associated with systemic (right) ventricular dilatation and failure, systemic atrioventricular (tricuspid) valve regurgitation, and atrial bradyarrhythmias and tachyarrhythmias is significant. A subset of patients may experience profound right ventricular failure, but they may do well with left ventricular retraining and late arterial switch 72.
In congenitally corrected transposition of the great arteries (ccTGA) or levo-transposition of the great arteries (L-TGA), the improved long-term survival associated with anatomic repair must be carefully weighed against the short-term safety of a physiological repair strategy, which focuses solely on correcting associated abnormalities 73. However, surgical mortality in the physiological repair population is significant. For instance, a series from the Mayo Clinic reported a 3% surgical mortality rate for operations performed after 1986, with an overall mortality rate of 16% 74. Similarly, a Dutch series by Bogers et al documented a 6.7% mortality rate 75. An alternative approach for managing congenitally corrected transposition of the great arteries (ccTGA) is staged single-ventricle palliation with Fontan completion. While short-term outcomes regarding survival and symptoms are comparable, the long-term complications are significant, with many patients experiencing serious morbidities 76.
Reinterventions after anatomic correction for congenitally corrected transposition of the great arteries (ccTGA) are common 77. In particular, conduit replacements are especially frequent in the atrial switch-Rastelli cohort, with most patients likely requiring at least one exchange to a larger conduit suitable for transcatheter replacement. After the initial reoperation, procedures such as multiple transcatheter replacements are often performed, reducing the need for further surgeries. Complications related to baffles, such as residual leaks or stenosis, are well-documented after Mustard or Senning operations and are a common reason for reoperations following anatomic repair for levo-transposition of the great arteries (L-TGA). However, in the current era, most baffle-related issues can be effectively managed with transcatheter techniques, minimizing the need for additional surgeries. Residual Left Ventricular Outflow Tract Obstruction (LVOTO) is also a known complication following both types of anatomic repair 78.
After arterial switch operation (ASO), complications may include chronotropic incompetence and stenosis at the supravalve neoaortic, neopulmonary, branch pulmonary arteries, and coronary artery ostia. However, most patients maintain normal systolic function and exercise capacity 70.
Progressive neoaortic root dilation is common and is a risk factor for neoaortic valve regurgitation following arterial switch operation. Continued surveillance of this population is required 79.
Sickness and mortality
Long-term complications are secondary to prolonged cyanosis and include polycythemia and hyperviscosity syndrome 68. These patients may develop headache, decreased exercise tolerance, and stroke 68. Thrombocytopenia is common in patients with cyanotic congenital heart disease leading to bleeding complications 68. With improved diagnostic, medical, and surgical techniques, the overall short-term and midterm survival rate exceeds 90% 68.
Patients with a large ventricular septal defect, a patent ductus arteriosus, or both may have an early development of congestive heart failure, as pulmonary vascular resistance falls with increasing age 68. Heart failure may be mitigated in those patients with left ventricular outflow tract (pulmonary) stenosis.
Arterioplasty in patients with supravalvar pulmonary or pulmonary artery branch stenosis following arterial switch surgery may be an effective and durable management option in the immediate term 80. In a retrospective study (2004-2013) comprising 223 babies who underwent arterial switch for transposition of the great arteries, 38 babies (16%) developed supravalvar pulmonary stenosis within 12.5 months. The surgical morbidity (e.g., main pulmonary artery plasty) was 13%, without hospital or late mortality. At the 41.2 months postsurgical follow-up, all the patients had New York Heart Association (NYHA) functional grade 0 or 1 symptoms 80. Cardiac catheterization and endovascular stenting of the branch pulmonary arteries is an alternative in older patients versus cardiac surgery.
Transposition of the great arteries survival rate
Surgical repair for dextro-transposition of the great arteries (D-TGA) should be performed within the first week of life. The two most commonly used procedures are the standard atrial switch operation (ASO) and the Rastelli procedure, which is recommended for patients with dextro-transposition of the great arteries (D-TGA), a large ventricular septal defect (VSD), and pulmonary stenosis. Studies report a survival rate exceeding 95% at 15 to 25 years post-discharge 16, 17. Postoperative complications can result from the underlying pathophysiology, surgical intervention, or residual defects, leading to adverse effects such as right ventricular dysfunction, tricuspid valve regurgitation, supraventricular arrhythmias, interatrial and interventricular septal dysfunction, and, less commonly, pulmonary hypertension. Despite these potential complications, most treated patients reach adulthood, with a 20-year survival rate nearing 90%. The primary cause of death is sudden cardiac death, followed by anatomical right ventricular dysfunction.
A retrospective study (1995-2016) that evaluated midterm outcomes in 97 patients with congenitally corrected transposition of the great arteries (ccTGA) who underwent different management strategies reported heart transplant-free survivals at 10 years in those who underwent a systemic right ventricle (93%), anatomic repair (86%), and Fontan procedure (100%) (there was a 79% transplant-free survival for pulmonary artery band or shunt) 81. During the study, 10 (10%) patients died, and 3 (3%) patients underwent heart transplantation. At last follow-up, 11 (11%) patients were in New York Heart Association class 3/4, 5 (5%) had moderate or severe systemic ventricle dysfunction, and 16 (16%) had moderate or severe systemic atrioventricular valve regurgitation 81. On multivariate analysis, only systemic right ventricular dysfunction as a risk factor for death or heart transplantation 81.
A small percentage (approximately 5%) of patients with transposition of the great arteries and often a ventricular septal defect develop accelerated pulmonary vascular obstructive disease and progressive cyanosis despite surgical repair or palliation. Long-term survival in this subgroup is particularly poor.
- Szymanski MW, Sharma S, Kritzmire SM, et al. Transposition of the Great Arteries. [Updated 2025 Mar 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538434[↩][↩]
- Centers for Disease Control and Prevention (CDC). Improved national prevalence estimates for 18 selected major birth defects–United States, 1999-2001. MMWR Morb Mortal Wkly Rep. 2006 Jan 6;54(51):1301-5. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5451a2.htm[↩][↩]
- Wilson W, Taubert KA, Gewitz M, Lockhart PB, et al. American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; Council on Cardiovascular Surgery and Anesthesia; Quality of Care and Outcomes Research Interdisciplinary Working Group; American Dental Association. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2007 Jun;138(6):739-45, 747-60. doi: 10.14219/jada.archive.2007.0262[↩][↩]
- Wypij D, Newburger JW, Rappaport LA, duPlessis AJ, Jonas RA, Wernovsky G, Lin M, Bellinger DC. The effect of duration of deep hypothermic circulatory arrest in infant heart surgery on late neurodevelopment: the Boston Circulatory Arrest Trial. J Thorac Cardiovasc Surg. 2003 Nov;126(5):1397-403. doi: 10.1016/s0022-5223(03)00940-1[↩]
- How the Healthy Heart Works. https://www.heart.org/en/health-topics/congenital-heart-defects/about-congenital-heart-defects/how-the-healthy-heart-works[↩][↩]
- Transposition of the Great Arteries. https://www.kidsheartshouston.com/answers/21850-transposition-of-the-great-arteries[↩]
- About dextro-Transposition of the Great Arteries (d-TGA). https://www.cdc.gov/heart-defects/about/d-tga.html[↩]
- van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011 Nov 15;58(21):2241-7. doi: 10.1016/j.jacc.2011.08.025[↩][↩]
- Tortigue M, Nield LE, Karakachoff M, McLeod CJ, et al. Familial Recurrence Patterns in Congenitally Corrected Transposition of the Great Arteries: An International Study. Circ Genom Precis Med. 2022 Jun;15(3):e003464. doi: 10.1161/CIRCGEN.121.003464[↩][↩]
- L-Transposition of the Great Arteries. https://www.heart.org/en/health-topics/congenital-heart-defects/about-congenital-heart-defects/l-transposition-of-the-great-arteries[↩]
- Ravi, P., Mills, L., Fruitman, D., Savard, W., Colen, T., Khoo, N., Serrano-Lomelin, J. and Hornberger, L.K. (2018), Population trends in prenatal detection of transposition of great arteries: impact of obstetric screening ultrasound guidelines. Ultrasound Obstet Gynecol, 51: 659-664. https://doi.org/10.1002/uog.17496[↩]
- Egg-on-a-string sign (heart). https://radiopaedia.org/articles/egg-on-a-string-sign-heart[↩][↩]
- Transposition of the great arteries. https://radiopaedia.org/cases/transposition-of-the-great-arteries-3?lang=us[↩]
- Pizula J, Devera J, Ng TMH, Yeung SL, Thangathurai J, Herrick N, Chatfield AJ, Mehra A, Elkayam U. Outcome of Pregnancy in Women With D-Transposition of the Great Arteries: A Systematic Review. J Am Heart Assoc. 2022 Dec 6;11(23):e026862. doi: 10.1161/JAHA.122.026862[↩]
- Transposition of the great arteries. https://radiopaedia.org/articles/transposition-of-the-great-arteries?lang=us[↩]
- Hutter PA, Kreb DL, Mantel SF, Hitchcock JF, Meijboom EJ, Bennink GB. Twenty-five years’ experience with the arterial switch operation. J Thorac Cardiovasc Surg. 2002 Oct;124(4):790-7. doi: 10.1067/mtc.2002.120714[↩][↩]
- Tobler D, Williams WG, Jegatheeswaran A, Van Arsdell GS, McCrindle BW, Greutmann M, Oechslin EN, Silversides CK. Cardiac outcomes in young adult survivors of the arterial switch operation for transposition of the great arteries. J Am Coll Cardiol. 2010 Jun 29;56(1):58-64. doi: 10.1016/j.jacc.2010.03.031[↩][↩]
- Warnes CA. Transposition of the great arteries. Circulation. 2006 Dec 12;114(24):2699-709. doi: 10.1161/CIRCULATIONAHA.105.592352[↩][↩][↩]
- Karl TR. The role of the Fontan operation in the treatment of congenitally corrected transposition of the great arteries. Ann Pediatr Cardiol. 2011 Jul;4(2):103-10. doi: 10.4103/0974-2069.84634[↩][↩]
- Shamsaeefar A, Masjedi F, Roozbeh J, Nazari SS, Zarei E, Jafari M, Farifteh S, Alikhani M, Eslamian M, Mardani M, Naseri R, Nikoupour H. Liver and pancreas transplantation in adult donor and recipients with situs inversus totalis: a case series and review of the literature. J Med Case Rep. 2024 Aug 29;18(1):398. doi: 10.1186/s13256-024-04720-y[↩]
- Mesfin T, Kedir I, Tilahun T, Seyoum K, Dadi S, Ejigu N, Desta F, Geta G, Tsegaye M, Salih H. Situs inversus with levocardia in a 15-year-old male adolescent: a case report. J Med Case Rep. 2023 Dec 3;17(1):499. doi: 10.1186/s13256-023-04254-9[↩]
- Aylsworth AS. Clinical aspects of defects in the determination of laterality. Am J Med Genet. 2001;101(4):345–355. doi: 10.1002/ajmg.1219[↩]
- Yokoyama T, Copeland NG, Jenkins NA, Montgomery CA, Elder FF, Overbeek PA. Reversal of left-right asymmetry: a situs inversus mutation. Science. 1993 Apr 30;260(5108):679-82. doi: 10.1126/science.8480178[↩]
- van Dissel AC, Opotowsky AR, Burchill LJ, et al. End-stage heart failure in congenitally corrected transposition of the great arteries: a multicentre study. Eur Heart J. 2023 Sep 7;44(34):3278-3291. doi: 10.1093/eurheartj/ehad511[↩][↩][↩][↩][↩]
- Transposition of the Great Arteries. https://emedicine.medscape.com/article/900574-overview#a7[↩]
- Škorić-Milosavljević D, Tadros R, Bosada FM, et al. Common Genetic Variants Contribute to Risk of Transposition of the Great Arteries. Circ Res. 2022 Jan 21;130(2):166-180. doi: 10.1161/CIRCRESAHA.120.317107[↩]
- Oster ME, Aucott SW, Glidewell J, Hackell J, Kochilas L, Martin GR, Phillippi J, Pinto NM, Saarinen A, Sontag M, Kemper AR. Lessons Learned From Newborn Screening for Critical Congenital Heart Defects. Pediatrics. 2016 May;137(5):e20154573. doi: 10.1542/peds.2015-4573[↩]
- Van Praagh R, Geva T, Kreutzer J. Ventricular septal defects: how shall we describe, name and classify them? J Am Coll Cardiol. 1989 Nov 1;14(5):1298-9. doi: 10.1016/0735-1097(89)90431-2[↩]
- Gatzoulis MA, Walters J, McLaughlin PR, Merchant N, Webb GD, Liu P. Late arrhythmia in adults with the mustard procedure for transposition of great arteries: a surrogate marker for right ventricular dysfunction? Heart. 2000 Oct;84(4):409-15. doi: 10.1136/heart.84.4.409[↩]
- Schwartz ML, Gauvreau K, del Nido P, Mayer JE, Colan SD. Long-term predictors of aortic root dilation and aortic regurgitation after arterial switch operation. Circulation. 2004 Sep 14;110(11 Suppl 1):II128-32. doi: 10.1161/01.CIR.0000138392.68841.d3[↩]
- Maeda T, Koide M, Kunii Y, Watanabe K, Kanzaki T, Ohashi Y. Supravalvular aortic stenosis after arterial switch operation. Asian Cardiovasc Thorac Ann. 2016 Jul;24(6):578-80. doi: 10.1177/0218492315586483[↩]
- Bonnet D, Coltri A, Butera G, Fermont L, Le Bidois J, Kachaner J, Sidi D. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation. 1999 Feb 23;99(7):916-8. doi: 10.1161/01.cir.99.7.916[↩]
- Kumar RK, Newburger JW, Gauvreau K, Kamenir SA, Hornberger LK. Comparison of outcome when hypoplastic left heart syndrome and transposition of the great arteries are diagnosed prenatally versus when diagnosis of these two conditions is made only postnatally. Am J Cardiol. 1999 Jun 15;83(12):1649-53. doi: 10.1016/s0002-9149(99)00172-1[↩]
- Blyth M, Howe D, Gnanapragasam J, Wellesley D. The hidden mortality of transposition of the great arteries and survival advantage provided by prenatal diagnosis. BJOG. 2008 Aug;115(9):1096-100. doi: 10.1111/j.1471-0528.2008.01793.x[↩]
- Soongswang J, Adatia I, Newman C, Smallhorn JF, Williams WG, Freedom RM. Mortality in potential arterial switch candidates with transposition of the great arteries. J Am Coll Cardiol. 1998 Sep;32(3):753-7. doi: 10.1016/s0735-1097(98)00310-6[↩]
- van Velzen CL, Haak MC, Reijnders G, Rijlaarsdam ME, Bax CJ, Pajkrt E, Hruda J, Galindo-Garre F, Bilardo CM, de Groot CJ, Blom NA, Clur SA. Prenatal detection of transposition of the great arteries reduces mortality and morbidity. Ultrasound Obstet Gynecol. 2015 Mar;45(3):320-5. doi: 10.1002/uog.14689[↩]
- Ravi P, Mills L, Fruitman D, Savard W, Colen T, Khoo N, Serrano-Lomelin J, Hornberger LK. Population trends in prenatal detection of transposition of great arteries: impact of obstetric screening ultrasound guidelines. Ultrasound Obstet Gynecol. 2018 May;51(5):659-664. doi: 10.1002/uog.17496[↩]
- Canan A, Ashwath R, Agarwal PP, François C, Rajiah P. Multimodality Imaging of Transposition of the Great Arteries. Radiographics. 2021 Mar-Apr;41(2):338-360. doi: 10.1148/rg.2021200069[↩]
- Ferguson EC, Krishnamurthy R, Oldham SA. Classic imaging signs of congenital cardiovascular abnormalities. Radiographics. 2007 Sep-Oct;27(5):1323-34. doi: 10.1148/rg.275065148[↩]
- Gopalakrishnan A, Krishnamoorthy KM, Sivasubramonian S. Balloon atrial septostomy at the bedside versus the catheterisation laboratory. Cardiol Young. 2019 Mar;29(3):454. doi: 10.1017/S1047951118002214[↩]
- Ranganath P, Singh S, Abbara S, Agarwal PP, Rajiah P. Computed Tomography in Adult Congenital Heart Disease. Radiol Clin North Am. 2019 Jan;57(1):85-111. doi: 10.1016/j.rcl.2018.08.013[↩]
- Tomasian A, Malik S, Shamsa K, Krishnam MS. Congenital heart diseases: post-operative appearance on multi-detector CT-a pictorial essay. Eur Radiol. 2009 Dec;19(12):2941-9. doi: 10.1007/s00330-009-1474-7[↩]
- Yamasaki Y, Nagao M, Yamamura K, Yonezawa M, Matsuo Y, Kawanami S, Kamitani T, Higuchi K, Sakamoto I, Shiokawa Y, Yabuuchi H, Honda H. Quantitative assessment of right ventricular function and pulmonary regurgitation in surgically repaired tetralogy of Fallot using 256-slice CT: comparison with 3-Tesla MRI. Eur Radiol. 2014 Dec;24(12):3289-99. doi: 10.1007/s00330-014-3344-1[↩]
- Tsai-Goodman B, Geva T, Odegard KC, Sena LM, Powell AJ. Clinical role, accuracy, and technical aspects of cardiovascular magnetic resonance imaging in infants. Am J Cardiol. 2004 Jul 1;94(1):69-74. doi: 10.1016/j.amjcard.2004.03.033[↩]
- Rajiah P, Kay F, Bolen M, Patel AR, Landeras L. Cardiac Magnetic Resonance in Patients With Cardiac Implantable Electronic Devices: Challenges and Solutions. J Thorac Imaging. 2020 Jan;35(1):W1-W17. doi: 10.1097/RTI.0000000000000462[↩]
- Freed MD, Heymann MA, Lewis AB, Roehl SL, Kensey RC. Prostaglandin E1 infants with ductus arteriosus-dependent congenital heart disease. Circulation. 1981 Nov;64(5):899-905. doi: 10.1161/01.cir.64.5.899[↩]
- Rashkind WJ, Miller WW. Creation of an Atrial Septal Defect Without Thoracotomy: A Palliative Approach to Complete Transposition of the Great Arteries. JAMA. 1966;196(11):991–992. doi:10.1001/jama.1966.03100240125026[↩]
- Hazekamp MG, Gomez AA, Koolbergen DR, Hraska V, Metras DR, Mattila IP, Daenen W, Berggren HE, Rubay JE, Stellin G; European Congenital Heart Surgeons Association. Surgery for transposition of the great arteries, ventricular septal defect and left ventricular outflow tract obstruction: European Congenital Heart Surgeons Association multicentre study. Eur J Cardiothorac Surg. 2010 Dec;38(6):699-706. doi: 10.1016/j.ejcts.2010.03.030[↩]
- Oboli VN, Pizzolla A, Pattnaik P. A Diagnostic Dilemma: Transposition of the Great Arteries. Cureus. 2023 May 12;15(5):e38931. doi: 10.7759/cureus.38931[↩]
- Domínguez-Manzano P, Herraiz I, Mendoza A, Aguilar JM, Escribano D, Toral B, Gómez-Montes E, Galindo A. Impact of prenatal diagnosis of transposition of the great arteries on postnatal outcome. J Matern Fetal Neonatal Med. 2017 Dec;30(23):2858-2863. doi: 10.1080/14767058.2016.1265934[↩]
- Senning A. Surgical correction of transposition of the great arteries. Surgery. 1959; 45: 966–980.[↩]
- Mustard WT. Successful two-stage correction of transposition of the great vessels. Surgery. 1964; 55: 469–472.[↩]
- Blalock A, Hanlon CR. Surgical treatment of complete transposition of aorta and pulmonary artery. Surg Gynecol Obstet. 1950; 90: 1–15.[↩]
- Andrade L, Carazo M, Wu F, Kim Y, Wilson W. Mechanisms for heart failure in systemic right ventricle. Heart Fail Rev. 2020 Jul;25(4):599-607. doi: 10.1007/s10741-019-09902-1[↩]
- Love BA, Mehta D, Fuster VF. Evaluation and management of the adult patient with transposition of the great arteries following atrial-level (Senning or Mustard) repair. Nat Clin Pract Cardiovasc Med. 2008 Aug;5(8):454-67. doi: 10.1038/ncpcardio1252[↩]
- Warnes CA. Transposition of the great arteries. Circulation. 2006 Dec 12;114(24):2699-709. https://doi.org/10.1161/CIRCULATIONAHA.105.592352[↩]
- Jatene AD, Fontes VF, Paulista PP, Souza LC, Neger F, Galantier M, Sousa JE. Anatomic correction of transposition of the great vessels. J Thorac Cardiovasc Surg. 1976 Sep;72(3):364-70.[↩]
- Cohen MS, Mertens LL. EDUCATIONAL SERIES IN CONGENITAL HEART DISEASE: Echocardiographic assessment of transposition of the great arteries and congenitally corrected transposition of the great arteries. Echo Res Pract. 2019 Dec 1;6(4):R107-R119. doi: 10.1530/ERP-19-0047[↩]
- Transposition Of The Great Arteries. https://www.kidsheartshouston.com/answers/21850-transposition-of-the-great-arteries[↩]
- Kreutzer C, De Vive J, Oppido G, et al. Twenty-five year experience with Rastelli repair for transposition of the great arteries. J Thorac Cardiovasc Surg. 2000;120:211–223. doi: 10.1067/mtc.2000.108163[↩][↩][↩][↩]
- Rastelli GC, Wallace RB, Ongley PA. Complete repair of transposition of the great arteries with pulmonary stenosis. A review and report of a case corrected by using a new surgical technique. Circulation. 1969 Jan;39(1):83-95. doi: 10.1161/01.cir.39.1.83[↩]
- Duncan BW, Poirier NC, Mee RB, Drummond-Webb JJ, Qureshi A, Mesia CI, Graney JA, Malek CL, Latson LA. Selective timing for the arterial switch operation. Ann Thorac Surg. 2004 May;77(5):1691-6; discussion 1697. doi: 10.1016/j.athoracsur.2003.10.042[↩]
- Baruteau AE, Abrams DJ, Ho SY, Thambo JB, McLeod CJ, Shah MJ. Cardiac Conduction System in Congenitally Corrected Transposition of the Great Arteries and Its Clinical Relevance. J Am Heart Assoc. 2017 Dec 21;6(12):e007759. doi: 10.1161/JAHA.117.007759[↩]
- Graham TP Jr, Bernard YD, Mellen BG, Celermajer D, Baumgartner H, Cetta F, Connolly HM, Davidson WR, Dellborg M, Foster E, Gersony WM, Gessner IH, Hurwitz RA, Kaemmerer H, Kugler JD, Murphy DJ, Noonan JA, Morris C, Perloff JK, Sanders SP, Sutherland JL. Long-term outcome in congenitally corrected transposition of the great arteries: a multi-institutional study. J Am Coll Cardiol. 2000 Jul;36(1):255-61. doi: 10.1016/s0735-1097(00)00682-3[↩]
- Hraska V, Duncan BW, Mayer JE Jr, Freed M, del Nido PJ, Jonas RA. Long-term outcome of surgically treated patients with corrected transposition of the great arteries. J Thorac Cardiovasc Surg. 2005 Jan;129(1):182-91. doi: 10.1016/j.jtcvs.2004.02.046[↩]
- Myers PO, del Nido PJ, Geva T, Bautista-Hernandez V, Chen P, Mayer JE Jr, Emani SM. Impact of age and duration of banding on left ventricular preparation before anatomic repair for congenitally corrected transposition of the great arteries. Ann Thorac Surg. 2013 Aug;96(2):603-10. doi: 10.1016/j.athoracsur.2013.03.096[↩]
- Bautista-Hernandez V, Myers PO, Cecchin F, Marx GR, Del Nido PJ. Late left ventricular dysfunction after anatomic repair of congenitally corrected transposition of the great arteries. J Thorac Cardiovasc Surg. 2014 Jul;148(1):254-8. doi: 10.1016/j.jtcvs.2013.08.047[↩]
- Transposition of the Great Arteries Prognosis. https://emedicine.medscape.com/article/900574-overview#a5[↩][↩][↩][↩][↩][↩]
- Ossa Galvis MM, Bhakta RT, Tarmahomed A, et al. Cyanotic Heart Disease. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK500001[↩]
- Khairy P, Clair M, Fernandes SM, Blume ED, Powell AJ, Newburger JW, Landzberg MJ, Mayer JE Jr. Cardiovascular outcomes after the arterial switch operation for D-transposition of the great arteries. Circulation. 2013 Jan 22;127(3):331-9. doi: 10.1161/CIRCULATIONAHA.112.135046[↩][↩]
- Nozica N, Asatryan B, Aur S, Clement JB, Schwerzmann M, Guan F, Pascale P, Gass M, Duru F, Reichlin T, Pruvot E, Wolber T, Roten L. Arrhythmias and Clinical Outcomes in a Swiss Multicenter Cohort of Patients With Dextro-Transposition of the Great Arteries and Atrial Switch. J Am Heart Assoc. 2023 Jul 4;12(13):e028956. doi: 10.1161/JAHA.122.028956[↩]
- Watanabe N, Mainwaring RD, Carrillo SA, Lui GK, Reddy VM, Hanley FL. Left Ventricular Retraining and Late Arterial Switch for D-Transposition of the Great Arteries. Ann Thorac Surg. 2015 May;99(5):1655-61; discussion 1661-3. doi: 10.1016/j.athoracsur.2014.12.084[↩]
- Hirose K, Nishina T, Kanemitsu N, Mizuno A, Yasumizu D, Yada M, Onga Y, Yamanaka K. The long-term outcomes of physiologic repair for ccTGA (congenitally corrected transposition of the great arteries). Gen Thorac Cardiovasc Surg. 2015 Sep;63(9):496-501. doi: 10.1007/s11748-015-0550-y[↩]
- Biliciler-Denktas G, Feldt RH, Connolly HM, Weaver AL, Puga FJ, Danielson GK. Early and late results of operations for defects associated with corrected transposition and other anomalies with atrioventricular discordance in a pediatric population. J Thorac Cardiovasc Surg. 2001 Aug;122(2):234-41. doi: 10.1067/mtc.2001.115241[↩]
- Bogers AJ, Head SJ, de Jong PL, Witsenburg M, Kappetein AP. Long term follow up after surgery in congenitally corrected transposition of the great arteries with a right ventricle in the systemic circulation. J Cardiothorac Surg. 2010 Sep 28;5:74. doi: 10.1186/1749-8090-5-74[↩]
- Sun J, Brizard C, Winlaw D, Alphonso N, d’Udekem Y, Eastaugh L, Marathe S, Bell D, Ayer J. Biventricular repair versus Fontan completion for patients with d- or l-transposition of the great arteries with ventricular septal defect and left ventricular outflow tract obstruction. J Thorac Cardiovasc Surg. 2019 Oct;158(4):1158-1167.e1. doi: 10.1016/j.jtcvs.2019.05.061[↩]
- Caughron H, Kim D, Kamioka N, Lerakis S, Yousef A, Maini A, Reginauld S, Sahu A, Shashidharan S, Jokhadar M, Rodriguez FH 3rd, Book WM, McConnell M, Block PC, Babaliaros V. Repeat Pulmonary Valve Replacement: Similar Intermediate-Term Outcomes With Surgical and Transcatheter Procedures. JACC Cardiovasc Interv. 2018 Dec 24;11(24):2495-2503. doi: 10.1016/j.jcin.2018.07.042[↩]
- Chatterjee A, Miller NJ, Cribbs MG, Law MA. Transcatheter Repair of Pulmonary Venous Baffle Stenosis. JACC Cardiovasc Interv. 2018 Aug 27;11(16):e129-e130. doi: 10.1016/j.jcin.2018.06.031[↩]
- Co-Vu JG, Ginde S, Bartz PJ, Frommelt PC, Tweddell JS, Earing MG. Long-term outcomes of the neoaorta after arterial switch operation for transposition of the great arteries. Ann Thorac Surg. 2013 May;95(5):1654-9. doi: 10.1016/j.athoracsur.2012.10.081[↩]
- Wiggins LM, Kumar SR, Starnes VA, Wells WJ. Arterioplasty for Right Ventricular Outflow Tract Obstruction After Arterial Switch Is a Durable Procedure. Ann Thorac Surg. 2015 Jul;100(1):122-7; discussion 127-8. doi: 10.1016/j.athoracsur.2015.02.086[↩][↩]
- De León LE, Mery CM, Verm RA, Trujillo-Díaz D, Patro A, Guzmán-Pruneda FA, Adachi I, Heinle JS, Kane LC, McKenzie ED, Fraser CD Jr. Mid-Term Outcomes in Patients with Congenitally Corrected Transposition of the Great Arteries: A Single Center Experience. J Am Coll Surg. 2017 Apr;224(4):707-715. doi: 10.1016/j.jamcollsurg.2016.12.029[↩][↩][↩]


{kind=link}