
Contents
Upper Back Pain
It’s not always possible to identify the cause of upper back pain but it’s rarely anything serious.
Most upper back pain is what’s known as “non-specific” (there’s no obvious cause) or “mechanical” (the pain originates from the joints, bones or soft tissues in and around the spine). In fact back pain is second only to the common cold when it comes to making people miserable. Approximately 80% of the world’s population develops this symptom at some point during their life.
In most cases of back pain, patients pain results from degenerative changes in the spine, involving the intervertebral discs, facet joints and soft tissues. Less common causes of pseudoradicular pain 1 include infections, non-infectious inflammation, tumors and metabolic disease (e.g. osteoporosis). The second most common cause of back pain is compression of a spinal nerve root (radicular pain). Radicular pain may also occur in association with degenerative changes, infections, rheumatic and metabolic diseases, tumors and injuries.
A degenerative disease of the spine is the major cause of back pain 2. The first symptoms are experienced in the third and fourth decades of life. The pain usually quickly subsides, but depending on the location and severity of degenerative changes it may become chronic. Such chronic pain may be reported by up to 60% of patients.
In a degenerative disease of the spine, an intervertebral disc is the first structure affected with a loss of height and decreased content of proteoglycans and water in the annulus fibrosus and the nucleus pulposus (see Figure 3). As a result, discogenic pain may develop 3. Discogenic pain felt in the paraspinal region is diffuse and exacerbated by movement, and may persist for a few days to a few weeks. Degenerative changes in the intervertebral disc(s) may produce pain in the facet joints. That pain is associated with the increased pathological range of motion in the spine and increased forces acting on the joints caused by the reduction in the size of the intervertebral disc. Also, degenerative intervertebral disc changes may cause a tear in the annulus fibrosus and bulging of the nucleus pulposus into the spinal canal. The resulting compression of the neural structures may produce neurological symptoms corresponding to its site. Spinal stenosis, congenital or acquired, may be associated with radicular pain or pain due to decreased flow in the microcirculation of the nerve roots and spinal nerves. Acquired stenosis results from the degenerative changes in the intervertebral discs and facet joints which narrow the space for the neural structures. Neurogenic claudication is characterized by sensory neurological symptoms (e.g. paraesthesia, superficial sensation deficits) and muscular weakness in the lower extremities exacerbated by walking. Spine disorders may also be associated with pain felt in e.g. sacroiliac or hip joints. In some cases the pain only mimics spine disorders. Frequently, pain originating in the sacroiliac joints is felt in the low back and is considered a symptom of spine disorders. Also, disorders of the spine such as pathological curvature of the spine may lead to an excessive strain on the joints of the lower extremities with the resulting changes and joint pain.
See your doctor if your back pain hasn’t improved after a week of home treatment or if your back pain:
- Is constant or intense, especially at night or when you lie down
- Spreads down one or both legs, especially if the pain extends below your knee
- Causes weakness, numbness or tingling in one or both legs
- Occurs with unintended weight loss
- Occurs with swelling or redness on your back
If you have any of the following symptoms in addition to your back pain, see your doctor straight away. You may need immediate medical help.
- Fever of 100º F (38º C) or above
- Unexplained weight loss
- Swelling of the back
- Constant back pain that does not ease after lying down
- Pain in your chest or high up in your back
- Pain down your legs and below the knees
- Pain caused by a recent trauma or injury to your back
- Loss of bladder control
- Inability to pass urine
- Loss of bowel control
- Numbness (loss of feeling, or a tingling sensation) around your genitals, buttocks or anal area
- Pain that is worse at night.
There are things you can do to help relieve it. But sometimes the pain can last a long time or keep coming back. Surgery is rarely needed for back pain and is generally considered only as a last resort.
Anatomy
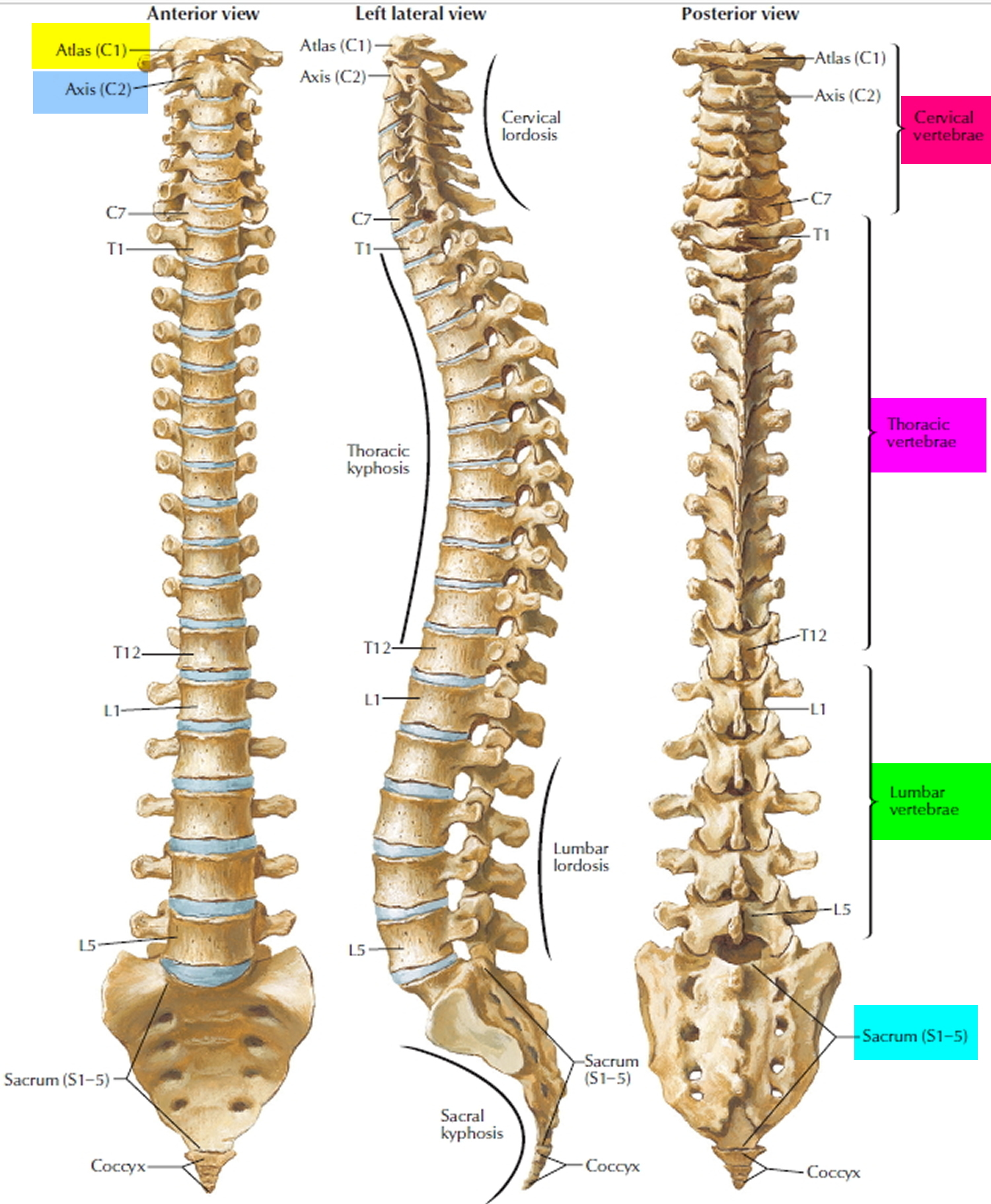
Your spine is made up of 24 bones, called vertebrae, that are stacked on top of one another. These bones connect to create a canal that protects the spinal cord.
The seven small vertebrae that begin at the base of the skull and form the neck comprise the cervical spine.
Figure 1. Vertebral spine
Other parts of your spine include:
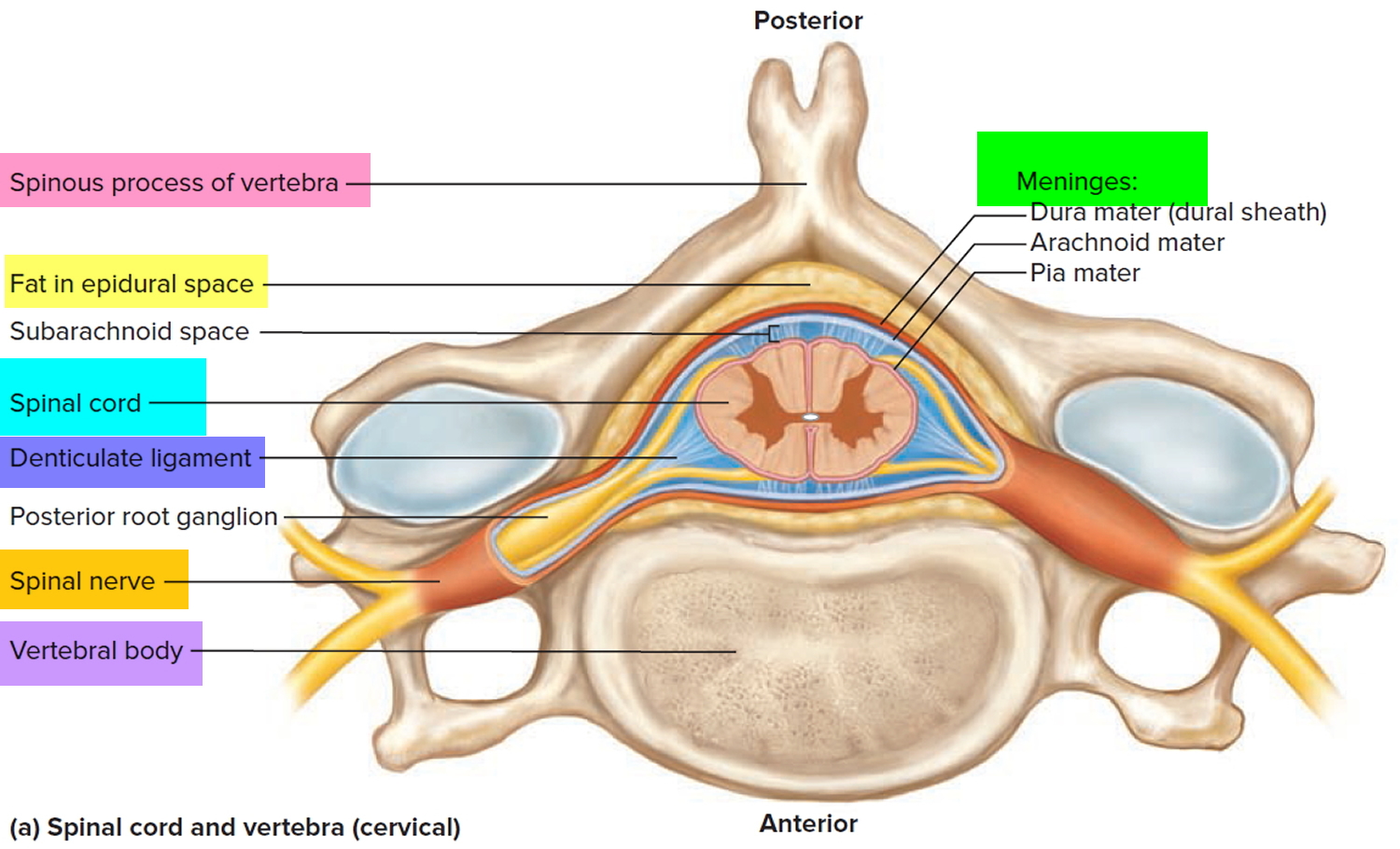
Spinal cord and nerves. These “electrical” cables travel through the spinal canal carrying messages between your brain and muscles. Nerve roots branch out from the spinal cord through openings in the vertebrae (foramen).
Figure 2. Spinal cord anatomy
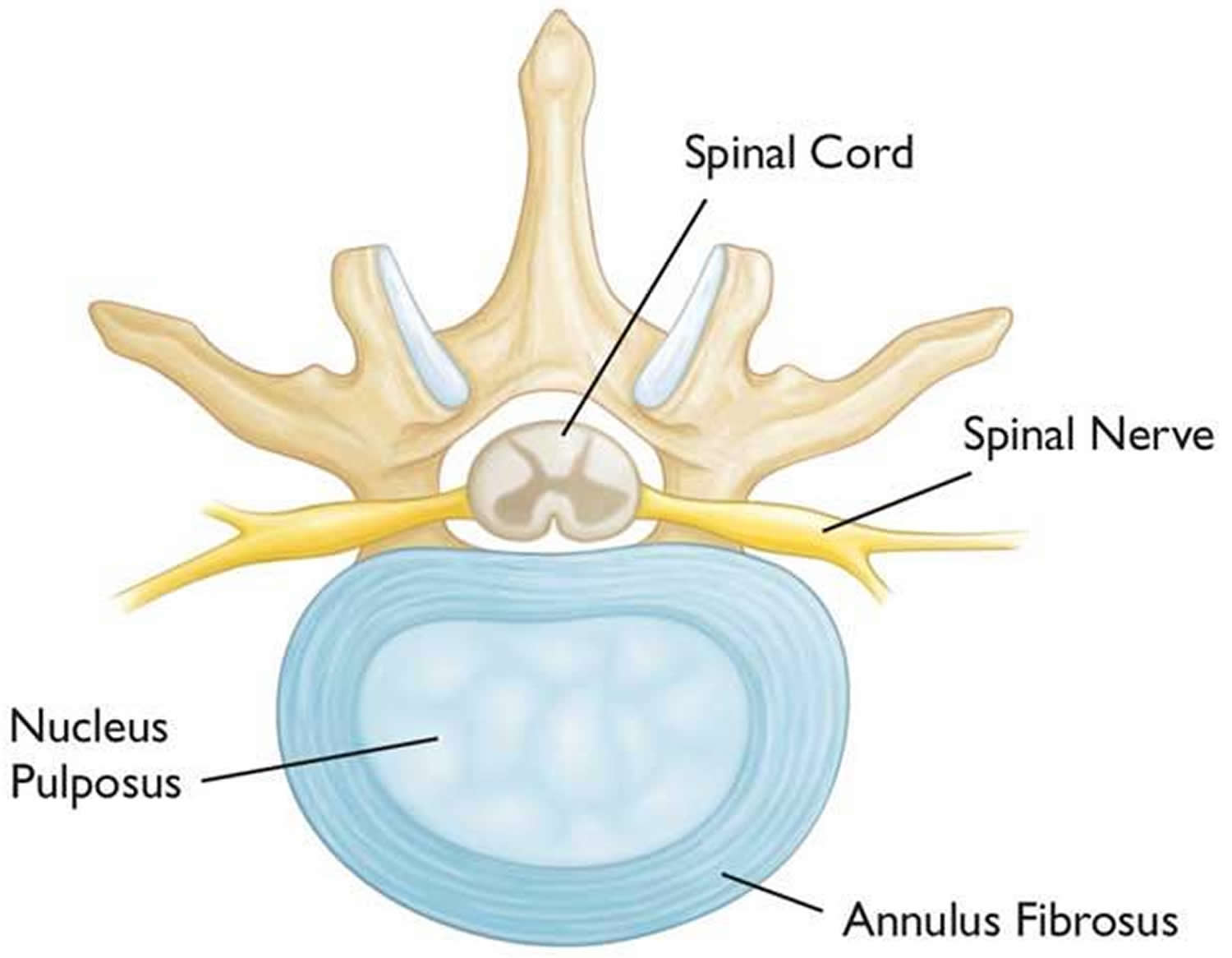
Intervertebral disks. In between your vertebrae are flexible intervertebral disks. They act as shock absorbers when you walk or run.
Intervertebral disks are flat and round and about a half inch thick. They are made up of two components:
- Annulus fibrosus. This is the tough, flexible outer ring of the disk.
- Nucleus pulposus. This is the soft, jelly-like center of the disk.
Figure 3. Intervertebral disk
Conditions that cause back pain
There are many causes of low back pain, but they can be grouped roughly as follows:
- Trauma;
- Spinal fractures
- Mechanical:
- Sprains and strains;
- Muscular pain;
- Vertebral dysfunction;
- Prolapsed or herniated disc (slipped disk);
- Narrowing of bony canals (spinal stenosis);
- Osteoarthritis;
- Fibromyalgia: Generalised aches and pains;
- Incorrect bone positions and articulation;
- Poor posture;
- Pregnancy;
- Obesity;
- Scoliosis;
- Meralgia paresthetica
- Inflammatory;
- Rheumatoid arthritis
- Infective lesions of the spine; Osteomyelitis
- Ankylosing spondylitis;
- Metabolic:
- Osteoporosis, fracture particularly in elderly, post-menopausal women;
- Paget’s disease of bone;
- Neoplastic (tumors/cancer):
- Metastases from tumors of other organs;
- Primary bone tumors;
- Multiple myeloma;
- Vascular: Disruption of the blood supply to the spinal cord (spinal claudication);
- Referred pain: Pain spreads to the back from somewhere else;
- Depression.
These conditions are treated differently to non-specific back pain.
Table 1. Red flags for serious spine disorders
| Red flags for serious spine disorders |
|---|
| First incident of back pain after the age of 50 years or before the age of 20 Back pain increasing in severity at night Back pain increasing in severity in the lying position and not related to physical activity Diagnosed cancer Immunosuppression Neurological deficit confirmed by physical examination
|
Back pain prevention
To avoid back pain, you must reduce excess stresses and strains on your back and ensure your back is strong and supple.
If you have recurring bouts of back pain, consider:
- losing any excess weight – you can use the body mass index BMI calculator to find out whether you are a healthy weight for your height
- wearing flat shoes with cushioned soles – these can reduce the stress on your back
- avoiding sudden movements or muscle strain
- trying to reduce any stress, anxiety and tension.
Posture
How you sit, stand and lie down can have an important effect on your back. The following tips should help you maintain a good posture.
Standing
Stand upright, with your head facing forward and your back straight. Balance your weight evenly on both feet and keep your legs straight.
Sitting
You should be able sit upright with support in the small of your back. Your knees and hips should be level and your feet should be flat on the floor (use a footstool if necessary). Some people find it useful to use a small cushion or rolled-up towel to support the small of the back.
If you use a keyboard, make sure that your forearms are horizontal and your elbows are at right angles.
Driving
Make sure that your lower back is properly supported. Correctly positioning your wing mirrors will prevent you from having to twist around. Foot controls should be squarely in front of your feet. If driving long distances, take regular breaks so that you can stretch your legs.
Sleeping
Your mattress should be firm enough to support your body while supporting the weight of your shoulders and buttocks, keeping your spine straight. If your mattress is too soft, place a firm board – ideally 2cm thick – on top of the base of your bed and under the mattress. Support your head with a pillow, but make sure that your neck is not forced up at a steep angle.
Exercise
Exercise is both an excellent way to prevent back pain and to reduce any back pain you might have. However, if you have chronic back pain (back pain that has lasted for more than 3 months), consult your doctor or physiotherapist before starting any exercise program.
Exercises such as walking or swimming strengthen the muscles that support your back without putting any strain on it or subjecting it to a sudden jolt.
Activities such as yoga or pilates can improve the flexibility and the strength of your back muscles. It is important that you carry out these activities under the guidance of a properly qualified instructor.
Many people injure their back when doing everyday chores at home or work, such as lifting, gardening or using a vacuum cleaner. ‘Warming up’ your back with some gentle stretching before you start these chores can help to prevent injury.
Lifting and handling
One of the biggest causes of back injury, especially at work, is lifting or handling objects incorrectly. Learning and following the correct method for lifting and handling objects can help to prevent back pain.
- Think before you lift – can you manage the lift? Are there any handling aids you can use? Where is the load going?
- Start in a good position – your feet should be apart, with one leg slightly forward to maintain balance. When lifting, let your legs take the strain – bend your back, knees and hips slightly, but do not stoop or squat. Tighten your stomach muscles to pull your pelvis in. Do not straighten your legs before lifting as you may strain your back on the way up.
- Keep the load close to your waist for as long as possible, with the heaviest end nearest to you.
- Avoid twisting your back or leaning sideways, especially when your back is bent. Your shoulders should be level and should face in the same direction as your hips. Turning by moving your feet is better than lifting and twisting at the same time.
- Keep your head up – once you have the load secure, look ahead, not down at the load.
- Know your limits – there is a big difference between what you can lift and what you can safely lift. If in doubt, get help.
- Push rather than pull – if you have to move a heavy object across the floor, it is better to push it rather than pull it.
- Distribute the weight evenly – if you are carrying shopping bags or luggage, try to distribute the weight evenly on both sides of your body.
Upper Back Pain Causes
Cervical intervertebral disc degeneration changes range from 5% to 10% in people between the ages of 20 and 30 years, to more than 50% by 45 years of age 4. Approximately, 90% of men over the age of 50 and 90% of women over the age of 60 have radiographic evidence of cervical spondylosis 5. Although there are many factors that can cause chronic neck, shoulder, and upper back pain 6, degeneration of the cervical spine is the most common condition contribution. Moreover, a degenerative cervical intervertebral disc in the cervicothoracic junction can also result in above syndromes 7.
Cervical spondylosis (Arthritis of the Neck)
Cervical spondylosis, commonly called arthritis of the neck, is a general term for age-related wear and tear affecting the spinal disks in your neck. As the discs dehydrate and shrink, signs of osteoarthritis develop, including bony projections along the edges of bones (bone spurs).
Cervical spondylosis is very common and worsens with age. More than 85 percent of people older than age 60 are affected by cervical spondylosis 8.
The condition most often causes pain and stiffness in the neck—although many people with cervical spondylosis experience no noticeable symptoms. In most cases, cervical spondylosis responds well to conservative treatment that includes medication and physical therapy. When symptoms do occur, nonsurgical treatments often are effective.
Figure 4. Cervical spondylosis
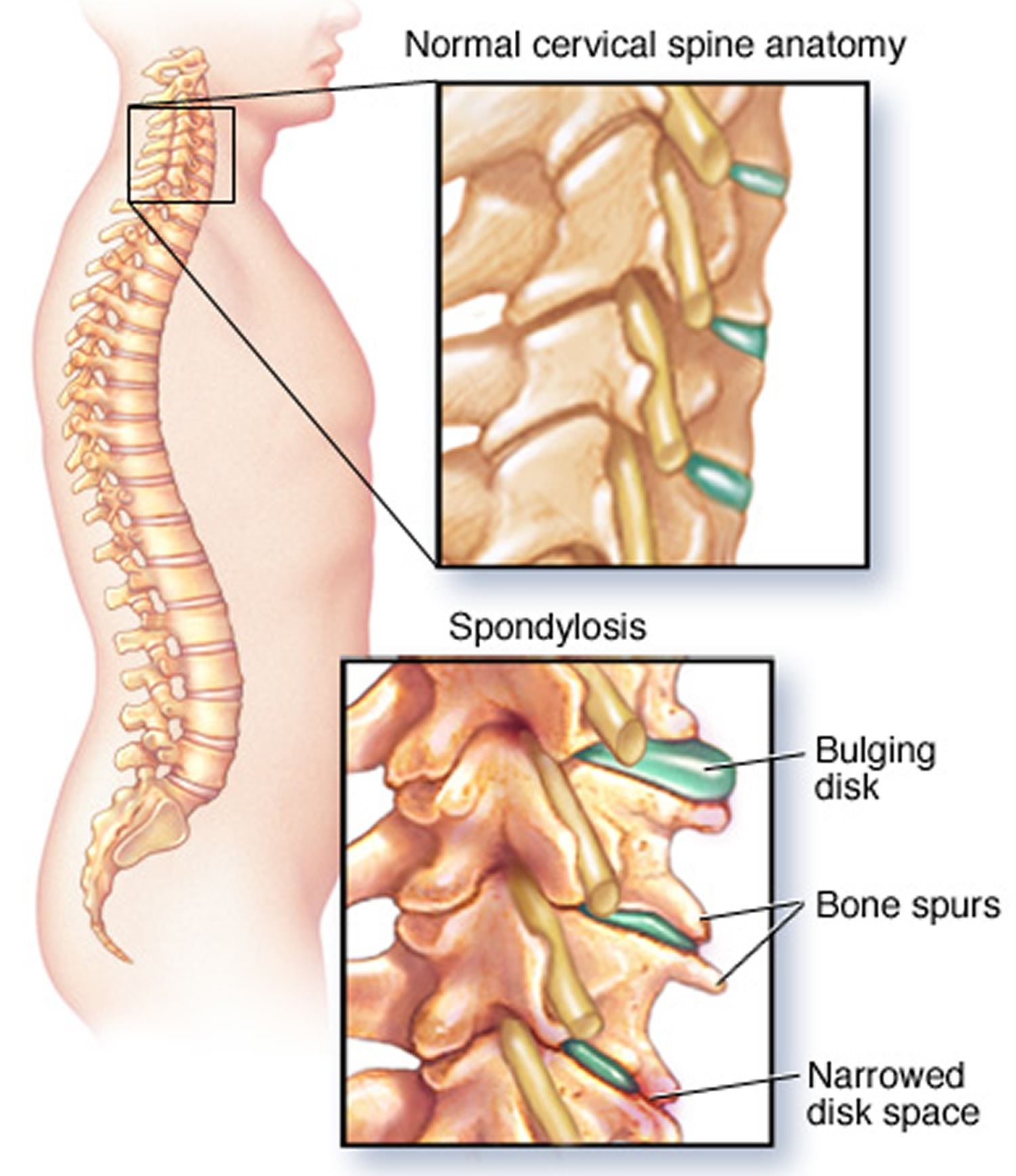
Note: Cervical spondylosis is degeneration of the bones and disks in the neck, which can lead to a variety of problems, including herniated disks and bone spurs.
Symptoms of cervical spondylosis
For most people cervical spondylosis causes no symptoms. When symptoms do occur, they typically include pain and stiffness in the neck. This pain can range from mild to severe. It is sometimes worsened by looking up or looking down for a long time, or by activities in which the neck is held in the same position for a prolonged period of time—such as driving or reading a book. The pain usually improves with rest or lying down.
Other symptoms may include:
- Headaches
- Grinding or popping noise or sensation when you turn your neck
- In some cases, cervical spondylosis results in a narrowing of the space needed for the spinal cord or nerve roots. If this occurs, your symptoms may include numbness and weakness in the arms, hands, and fingers
- Trouble walking, loss of balance, or weakness in the hands or legs
- Muscle spasms in the neck and shoulders
Sometimes, cervical spondylosis results in a narrowing of the space needed by the spinal cord and the nerve roots that pass through the spine to the rest of your body. If the spinal cord or nerve roots become pinched, you might experience:
- Tingling, numbness and weakness in your arms, hands, legs or feet
- Lack of coordination and difficulty walking
- Loss of bladder or bowel control
Seek medical attention if you notice a sudden onset of numbness or weakness, or loss of bladder or bowel control.
Causes of cervical spondylosis
As you age, the bones and cartilage that make up your backbone and neck gradually develop wear and tear. These changes can include:
- Dehydrated disks. Disks act like cushions between the vertebrae of your spine. By the age of 40, most people’s spinal disks begin drying out and shrinking, which allows more bone-on-bone contact between the vertebrae.
- Herniated disks. Age also affects the exterior of your spinal disks. Cracks often appear, leading to bulging (herniated) disks — which sometimes can press on the spinal cord and nerve roots.
- Bone spurs. Disk degeneration often results in the spine producing extra amounts of bone in a misguided effort to strengthen the spine. These bone spurs can sometimes pinch the spinal cord and nerve roots.
- Stiff ligaments. Ligaments are cords of tissue that connect bone to bone. Spinal ligaments can stiffen with age, making your neck less flexible.
Risk factors for cervical spondylosis
Risk factors for cervical spondylosis include:
- Age. Cervical spondylosis is a normal part of aging.
- Occupation. Jobs that involve repetitive neck motions, awkward positioning or a lot of overhead work put extra stress on your neck.
- Neck injuries. Previous neck injuries appear to increase the risk of cervical spondylosis.
- Genetic factors. Some individuals in certain families will experience more of these changes over time, while others will not.
- Smoking. Smoking has been linked to increased neck pain.
Complications of cervical spondylosis
If your spinal cord or nerve roots become severely compressed as a result of cervical spondylosis, the damage can be permanent.
Cervical spondylosis diagnosis
Your doctor will likely start with a physical exam that includes:
- Checking the range of motion in your neck
- Testing your reflexes and muscle strength to find out if there’s pressure on your spinal nerves or spinal cord
- Watching you walk to see if spinal compression is affecting your gait
Imaging tests
Imaging tests can provide detailed information to guide diagnosis and treatment. Your doctor might recommend:
- Neck X-ray. An X-ray can show abnormalities, such as bone spurs, that indicate cervical spondylosis. Neck X-ray can also rule out rare and more serious causes for neck pain and stiffness, such as tumors, infections or fractures.
- CT scan. CT scan can provide more detailed imaging, particularly of bones.
- MRI. MRI can help pinpoint areas where nerves might be pinched.
- Myelograpy. A tracer dye is injected into the spinal canal to provide more detailed X-ray or CT imaging.
Nerve function tests
Your doctor might recommend tests to determine if nerve signals are traveling properly to your muscles. Nerve function tests include:
- Electromyography (EMG). This test measures the electrical activity in your nerves as they transmit messages to your muscles when the muscles are contracting and when they’re at rest.
- Nerve conduction study. Electrodes are attached to your skin above the nerve to be studied. A small shock is passed through the nerve to measure the strength and speed of nerve signals.
Treatment for cervical spondylosis
Treatment for cervical spondylosis depends on the severity of your signs and symptoms. The goal of treatment is to relieve pain, help you maintain your usual activities as much as possible, and prevent permanent injury to the spinal cord and nerves.
Physical Therapy
Physical therapy is usually the first nonsurgical treatment that your doctor will recommend. Specific exercises can help relieve pain, as well as strengthen and stretch weakened or strained muscles.
A physical therapist can teach you exercises to help stretch and strengthen the muscles in your neck and shoulders. In some cases, physical therapy may include posture therapy or the use of traction to gently stretch the joints and muscles of your neck. Physical therapy programs vary in length, but generally last from 6 to 8 weeks. Typically, sessions are scheduled 2 to 3 times per week.
Some people with cervical spondylosis benefit from the use of traction, which can help provide more space within the spine if nerve roots are being pinched.
Medications
If over-the-counter pain relievers don’t help, your doctor might prescribe several medications to be used together to address both pain and inflammation:
- Acetaminophen. Mild pain is often relieved with acetaminophen.
- Nonsteroidal anti-inflammatory drugs (NSAIDs). Prescription-strength ibuprofen (Ibuprofen) or naproxen sodium (Anaprox, Anaprox DS) might be needed to relieve pain and inflammation.
- Corticosteroids. Oral medications, such as prednisone, might help ease pain. If your pain is severe, your doctor might suggest steroid injections.
- Steroid-based injections. Although less invasive than surgery, steroid-based injections are prescribed only after a complete evaluation by your doctor. Your doctor will talk with you about the risks and benefits of steroid-based injections for your specific condition. Many patients find short-term pain relief from steroid injections. The most common procedures for neck pain include:
- Cervical epidural block. In this procedure, steroid and anesthetic medicine is injected into the space next to the covering of the spinal cord (“epidural” space). This procedure is typically used for neck and/or arm pain that may be due to a cervical disk herniation, also known as radiculopathy or a “pinched nerve.”
- Cervical facet joint block. In this procedure, steroid and anesthetic medicine is injected into the capsule of the facet joint. The facet joints are located in the back of the neck and provide stability and movement. These joints can develop arthritic changes that may contribute to neck pain.
- Medial branch block and radiofrequency ablation. This procedure is used in some cases of chronic neck pain. It can be used to both diagnose and treat a painful joint. During the diagnosis portion of the procedure, the nerve that supplies the facet joint is blocked with a local anesthetic. If your pain is relieved, then your doctor may have pinpointed the source of your neck pain. The next step option may be to block the pain more permanently. This is done by damaging the nerves that supply the joint with a “burning” technique—a procedure called radiofrequency ablation.
- Muscle relaxants. Certain drugs, such as cyclobenzaprine (Amrix, Fexmid) and methocarbamol (Robaxin), can help relieve muscle spasms in the neck.
- Anti-seizure medications. Some types of epilepsy medications, such as gabapentin (Neurontin) and pregabalin (Lyrica), can dull the pain of damaged nerves.
- Antidepressants. Certain antidepressant medications have been found to help ease neck pain from cervical spondylosis.
- Prescription pain relievers. Your doctor might prescribe oxycodone (Percocet, Roxicet).
Acupuncture
Your doctor might recommend trying acupuncture to reduce your pain. Acupuncture is best provided by a licensed acupuncture practitioner.
Surgery
If conservative treatment fails or if your neurological signs and symptoms — such as weakness in your arms or legs — worsen, you might need surgery to create more room for your spinal cord and nerve roots.
The surgery might involve:
- Removing a herniated disk or bone spurs
- Removing part of a vertebra
- Fusing a segment of the neck using bone graft and hardware
Lifestyle and home remedies
Mild cervical spondylosis might respond to:
- Regular exercise. Maintaining activity will help speed recovery, even if you have to temporarily modify some of your exercises because of neck pain. People who walk daily are less likely to experience neck and low back pain.
- Over-the-counter pain relievers. Ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve) or acetaminophen (Tylenol, others) is often enough to control the pain associated with cervical spondylosis.
- Heat or ice. Applying heat or ice to your neck can ease sore neck muscles.
- Soft neck collar. This is a padded ring that wraps around the neck and is held in place with velcro. Your doctor may advise you to wear a soft cervical collar to limit neck motion and allow the muscles in your neck to rest. A soft collar should only be worn for a short period of time since long-term wear may decrease the strength of the muscles in your neck. Therefore it’s better to keep your neck moving and don’t wear a soft collar (unless a doctor tells you to).
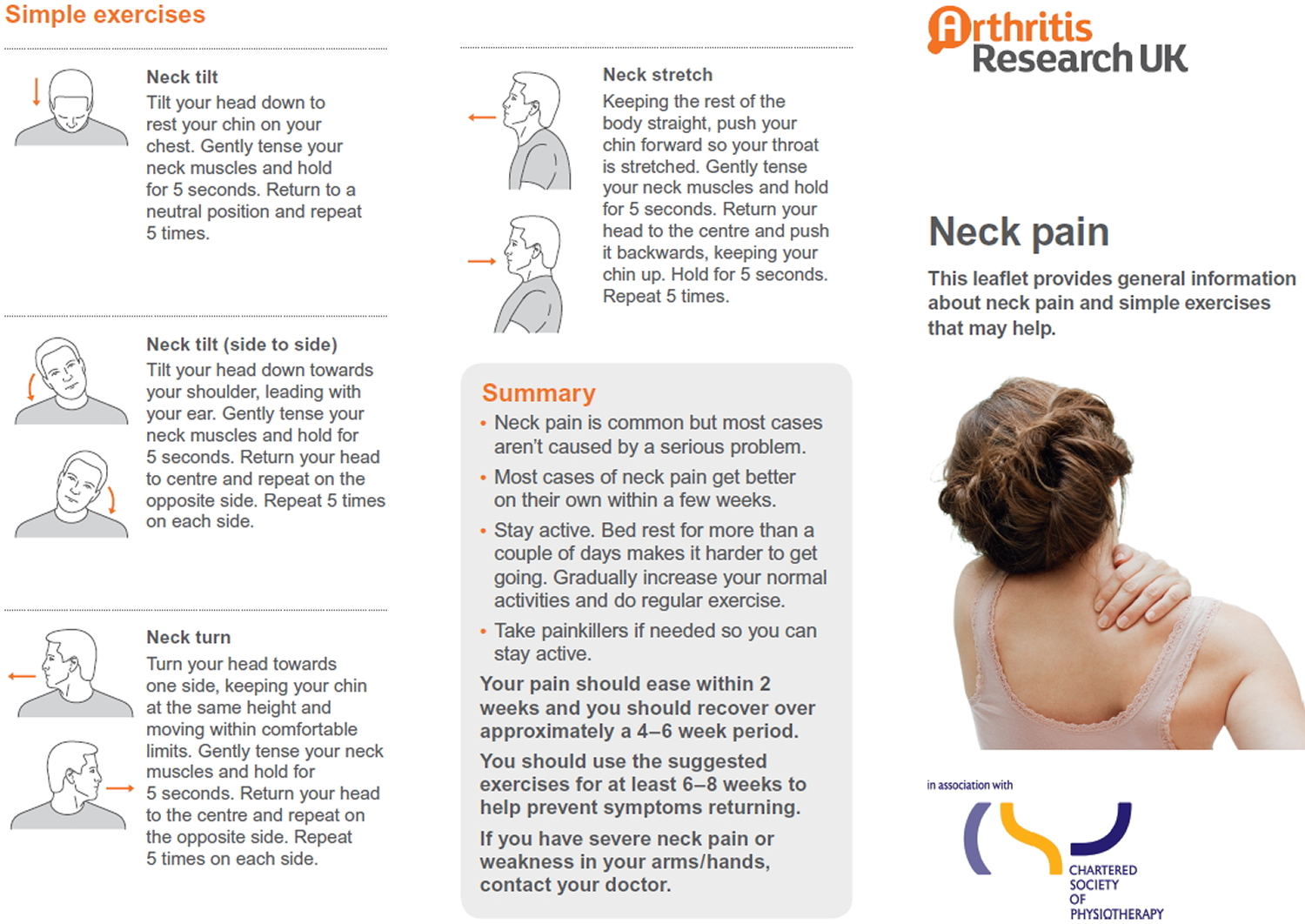
Figure 5. Neck exercises for neck pain
- Pseudoradicular and radicular low-back pain: How to diagnose clinically? Pain. 2008 Apr;135(3):311-2; author reply 313-5. doi: 10.1016/j.pain.2008.02.003. http://www.sciencedirect.com/science/article/pii/S0304395908000675[↩]
- Prevalence of degenerative changes of the spine on magnetic resonance images and radiographs in patients aged 16-45 years with chronic back pain of short duration in the Spondyloarthritis Caught Early (SPACE) cohort. de Bruin F, ter Horst S, Bloem HL, van den Berg R, de Hooge M, van Gaalen F, Fagerli KM, Landewé R, van Oosterhout M, van der Heijde D, Reijnierse M. Rheumatology (Oxford). 2016 Jan; 55(1):56-65. https://www.ncbi.nlm.nih.gov/pubmed/26275972/[↩]
- Prevalence and Characteristics of Discogenic Pain in Tertiary Practice: 223 Consecutive Cases Utilizing Lumbar Discography. Verrills P, Nowesenitz G, Barnard A. Pain Med. 2015 Aug; 16(8):1490-9. https://www.ncbi.nlm.nih.gov/pubmed/26217926/[↩]
- Xie R, Ruan linhui, chen L, et al. T2 relaxation time for intervertebral disc degeneration in patients with upper back pain: initial results on the clinical use of 3.0 Tesla MRI. BMC Medical Imaging. 2017;17:9. doi:10.1186/s12880-017-0182-z. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5282844/[↩]
- Grob D. Surgery in the degenerative cervical spine. Spine. 1998;23:2674–83. doi: 10.1097/00007632-199812150-00005. https://www.ncbi.nlm.nih.gov/pubmed/9879094[↩]
- Ehrmann Feldman D, Shrier I, Rossignol M, Abenhaim L. Risk factors for the development of neck and upper limb pain in adolescents. Spine (Phila Pa 1976) 2002;27:523–8. doi: 10.1097/00007632-200203010-00013. https://www.ncbi.nlm.nih.gov/pubmed/11880838[↩]
- Williams FM, Sambrook PN. Neck and back pain and intervertebral disc degeneration: role of occupational factors. Best Pract Res Clin Rheumatol. 2011;25:69–79. doi: 10.1016/j.berh.2011.01.007. https://www.ncbi.nlm.nih.gov/pubmed/21663851[↩]
- Cervical Spondylosis (Arthritis of the Neck). https://orthoinfo.aaos.org/en/diseases–conditions/cervical-spondylosis-arthritis-of-the-neck/[↩]





{kind=link}