Contents
Vestibulocochlear nerve
Vestibulocochlear nerve or cranial nerve number 8 (CN VIII) carries sensory information (afferent nerves) for hearing and balance, and consists of two divisions:
- Vestibular nerve for balance and equilibrium.
- Cochlear nerve for hearing.
The vestibular nerve convey information concerning position, movement, and balance. The cochlear nerve conveys information concerning hearing. Lesions of cochlear nerve or cochlear receptors result in central or nerve deafness, whereas damage to vestibular division produces dizziness, rapid involuntary eye movements, loss of balance, nausea, and vomiting. Vestibulocochlear nerve (CN VIII) injuries can subsist as a result of pathological processes or traumas involving the pontocerebellar angle, the internal acoustic meatus, or the inner ear. In such cases, symptoms such as vertigo and nystagmus may occur due to the involvement of the vestibular part, and tinnitus and hypacusia due to the involvement of the cochlear part.
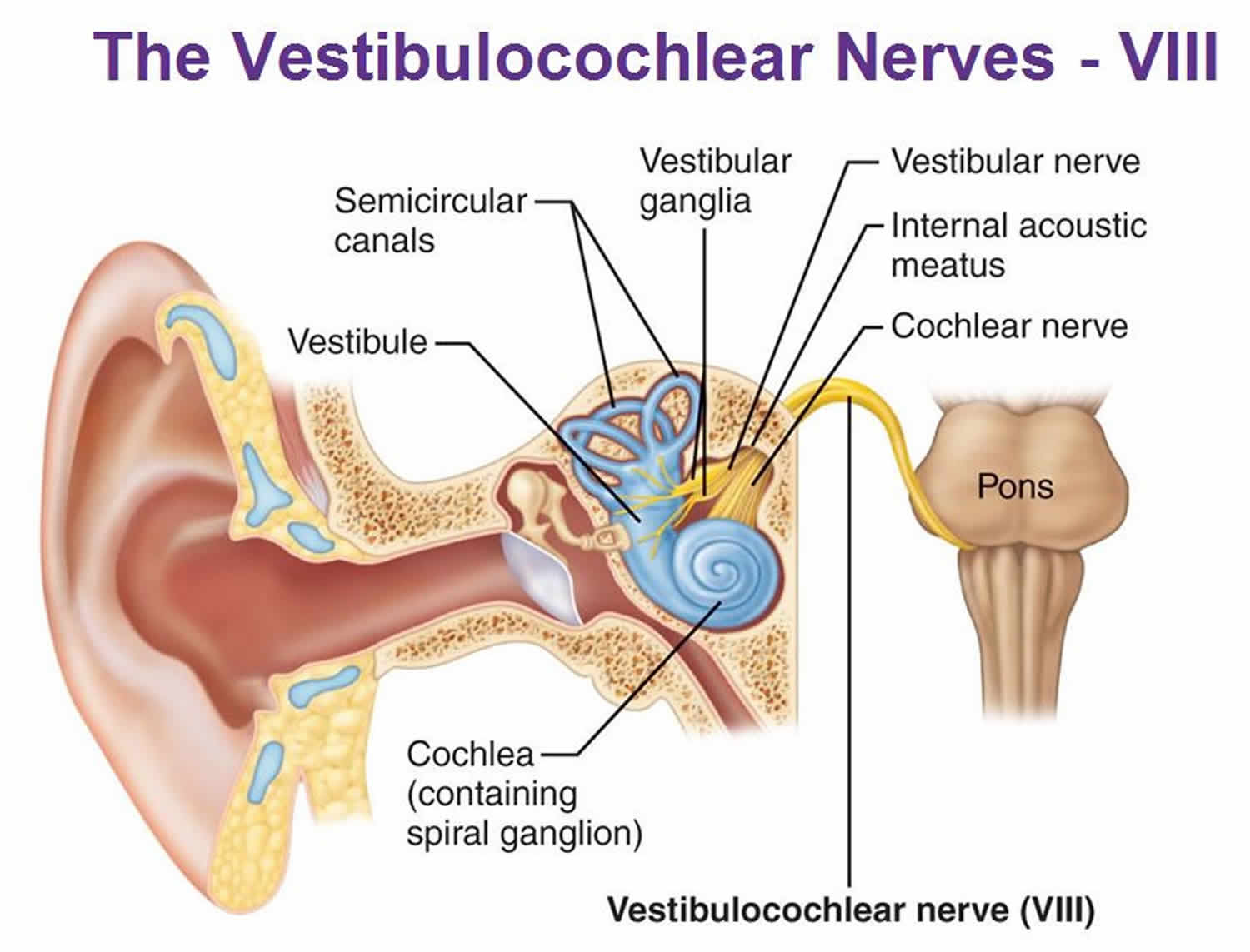
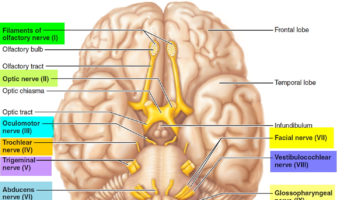
The vestibulocochlear nerve (CN VIII) originates at the sensory receptors in the inner ear from within the cochlea for hearing and for equilibrium and balance from within the semicircular canals and the vestibule (Figure 1). Sensory nerve cell bodies for vestibular branch located in vestibular ganglia (Figure 1); for the cochlear branch, in the spiral ganglia within the cochlea (Figure 1). From the inner ear cavity within the substance of the petrous part of the temporal bone, the vestibular nerve and the cochlear nerve fibers pass through the internal auditory canal, merge to form the vestibulocochlear nerve (CN VIII) (Figures 1 and 2) and enter the brain stem at the pons (Figure 4). The vestibular nerve is the larger of the two bundles.
Situated as it is in the groove between the pons and the medulla, the vestibulocochlear nerve makes up part of the acousticofacial bundle (Figure 3). The acousticofacial bundle is composed of the facial nerve (CN VII), the intermediary nerve of Wrisberg, the cochlear nerve and the vestibular nerve (Figure 3). Each nerve is surrounded by its own sheath of pia mater as it crosses the cistern of the cerebellopontine angle. The acousticofacial bundle is situated above the petro-occipital fissure, the inferior petrosal sinus and the posterior surface of the petrous part of the temporal bone. On its course from the pontomedullary junction to the internal acoustic meatus, the nerve runs laterally, slightly anterior and cephalad.
Vestibulocochlear nerve (CN VIII) is responsible for maintaining body balance and eye movements in addition to conveying neural impulses related to hearing 1. The vestibulocochlear nerve, is responsible for the auditory sense and the vestibular sense of orientation of the head. Vestibulocochlear nerve (CN VIII) conveys special sensory afferents from the inner ear to the cochlear nuclei and the vestibular nuclei in the caudal medulla oblongata 2. Hair cells within the cochlear duct, semicircular canals, utricle, and saccule are polarized sensory receptor cells with apical ciliary extensions that transduce an electrochemical signal upon mechanical deformation. Ganglionic neurons within the cochlea and the vestibular nerve receive this signal peripherally and transmit it centrally through the internal auditory meatus before entering the medulla. Damage to the vestibular component of this nerve causes dizziness, while damage to the cochlear part causes peripheral, or sensorineural, hearing loss. The internal auditory meatus is a narrow canal of the temporal bone through which these nerves course and a schwannoma of the vestibular or cochlear nerves in this meatus easily compresses and impinges these nerves. Early signs and symptoms are a progressive worsening hearing loss with tinnitus, imbalance, leading to a sense of pressure in the ear and facial weakness or paralysis 3. Vestibular schwannomas have an incidence rate of six to nine new cases per year per million people and are readily treatable with surgery or radiation 4. However, if the condition is left untreated, it can result in potentially large and life-threatening tumors.
The cochlear nerve has a peripheral sensory origin from the spiral organ of Corti, also known as the cochlear ganglion. The spiral organ of Corti is located in the cochlea of the inner ear 5. Neuronal projections from the cochlear ganglion form the cochlear nerve as they pass through the internal acoustic meatus. The cochlear nerve enter the brainstem laterally at the pontomedullary junction where they synapse on ventral and dorsal cochlear nuclei of the medulla oblongata (Figure 1). Cochlear nuclei are organized tonotopically, derived from the Greek word meaning “place of the sounds.” The afferents that arrive from the cochlear ganglion carrying impulses related to the base of the cochlea send signals of high-frequency tones, toward the dorsomedial quadrant of the nuclei. The afferents coming from the apex of the cochlea send signals for the low-frequency tones toward the ventrolateral quadrant of each nucleus. From the nuclei mentioned above, transverse fibers are born: dorsal acoustic striae; intermediate acoustic striae; ventral acoustic striae 6. The ventral cochlear nucleus plays a fundamental role in humans in the auditory pathways and from which the ventral striae are derived; these give rise to the trapezoid body once crossed the bridge in the ventral portion of the tegmen. The trapezoid body (in which you find the nucleus of the trapezoid body and the upper olivary complex) continues with an ascending path through the lateral lemniscus.
The peripheral vestibular apparatus is located within the temporal bone, and it consists of a bony and membranous labyrinth. The membranous labyrinth contains the sensory neuroepithelium and is located within the bony labyrinth, suspended in perilymph. The vestibular apparatus has five components: the utricle, saccule, and three semicircular ducts (contained within the semicircular canals). The two types of neuroepithelium are the macula and crista ampullaris, which both contain sensory hair cells or ciliated cells. The utricle and saccule contain macula, while the semicircular canals contain crista ampullaris 7.
The utricle and saccule sense the positioning of the head in space. Hair cells or ciliated cells within the utricle respond to horizontal acceleration, while the hair cells within the saccule respond to vertical acceleration. The hair cells within the three semicircular ducts (lateral, superior, and posterior) respond to angular acceleration or head rotation 7.
The stimulation of the hair cells results in depolarization and increased calcium (Ca) influx, leading to increased firing of afferent vestibular nerve fibers. Those fibers travel to the vestibular ganglion (Scarpa’s ganglion), located in the internal auditory canal. The vestibular ganglion (Scarpa’s ganglion) is composed of bipolar neurons that send peripheral processes to the vestibular apparatus and central processes that join together to form the vestibular nerve. The vestibular ganglion (Scarpa’s ganglion) is separated into upper and lower divisions. The upper division receives input from the utricle and superior and lateral semicircular ducts. The lower division receives input from the saccule and posterior semicircular duct 7.
The upper and lower post-ganglionic extensions join to form the vestibular nerve, which joins the cochlear nerve to become the vestibulocochlear nerve (CN VIII) within the internal auditory canal. Vestibulocochlear nerve (CN VIII) runs past the cerebellopontine angle and enters the brainstem at the pontomedullary junction. The vestibular nerve separates from the cochlear nerve before reaching the vestibular nuclear complex. The vestibular nuclear complex consists of four nuclei: medial, lateral, superior, and inferior. These nuclei range from the caudal pons to the rostral medulla in two columns and are closely related to the floor of the fourth ventricle 7. The vestibular nuclear complex receives input from the ipsilateral cerebellum, as well as the vestibular nerve, and projects to various ipsilateral and contralateral structures.
The medial nucleus receives input from the lateral semicircular ducts. It sends ascending fibers to the motor nuclei of the extraocular muscles ipsilaterally and contralateral via the medial longitudinal fasciculus (MLF), which helps facilitate the vestibulo-ocular reflex. The medial nucleus also helps mediate the vestibulospinal reflex by controlling head and neck movements 7.
The superior nucleus receives input from the superior and posterior semicircular ducts and mediates the vestibulo-ocular reflex 7. Furthermore, it projects to chiefly the ventral posterior intermediate nucleus of bilateral thalami in an ascending projection thought to play a fundamental role in conscious spatial awareness 8, mediating onward thalamocortical circuits 9.
The lateral nucleus receives input from all components of the vestibular apparatus and the vestibulocerebellum. Descending projections become the lateral vestibular tract within the ipsilateral spinal cord. This tract helps mediate the vestibulospinal reflex and maintain posture and balance 7.
The inferior nucleus receives input from the utricle and saccule and sends fibers to the other three vestibular nuclei and the cerebellum 7.
It has also been suggested that the auditory stimuli interact with the vestibular system to influence postural control 10. Additionally, the vestibular system helps control blood pressure by using sympathetic pathways and the baroreceptors on the carotid and the aortic arch 11.
Specifics regarding vestibular cortical connections are not well understood, but studies have suggested that the vestibular cortical area is adjacent to the parietal or insular cortex 7.
Figure 1. Vestibulocochlear nerve origin and destination
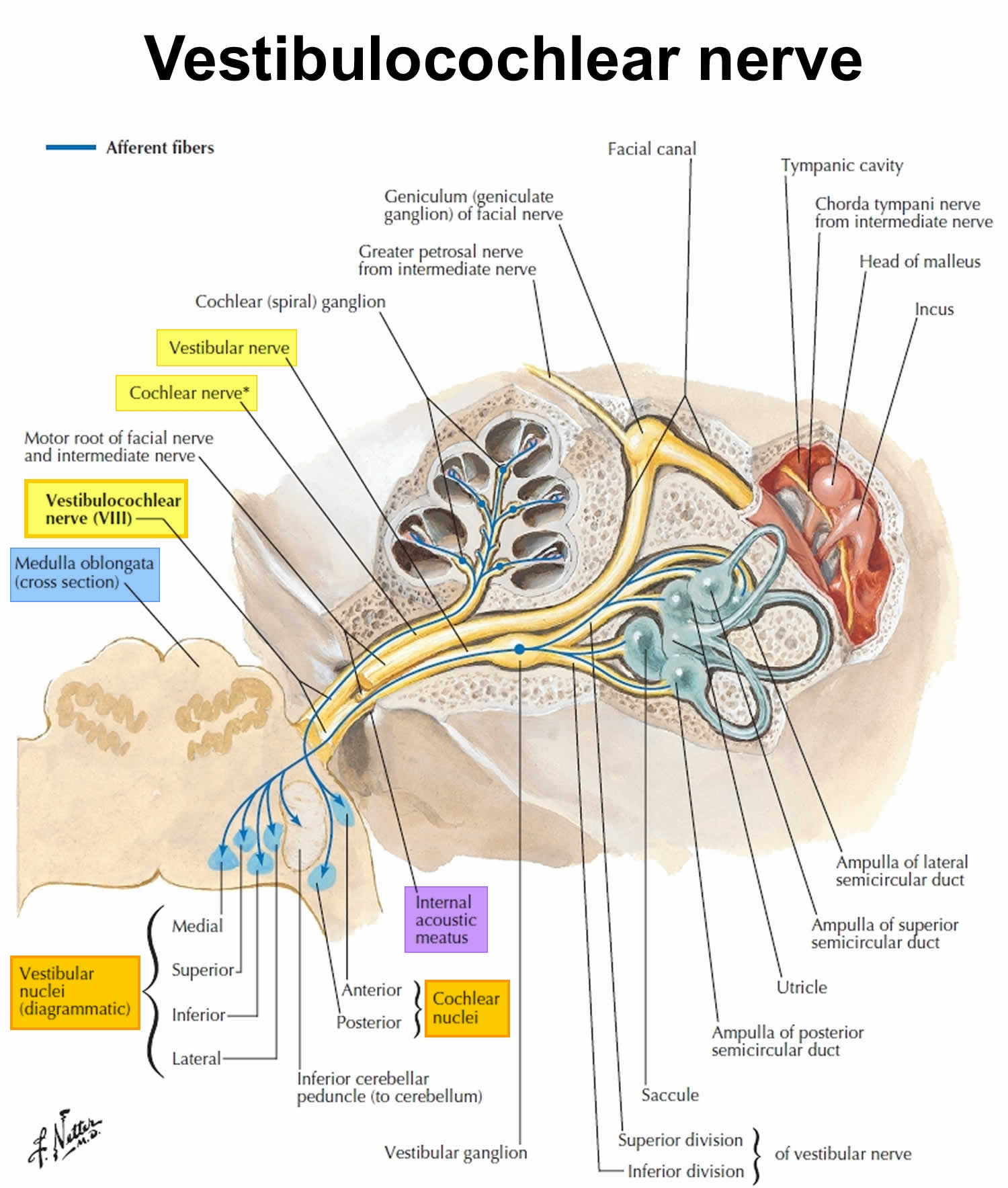
Figure 2. Vestibulocochlear nerve branches
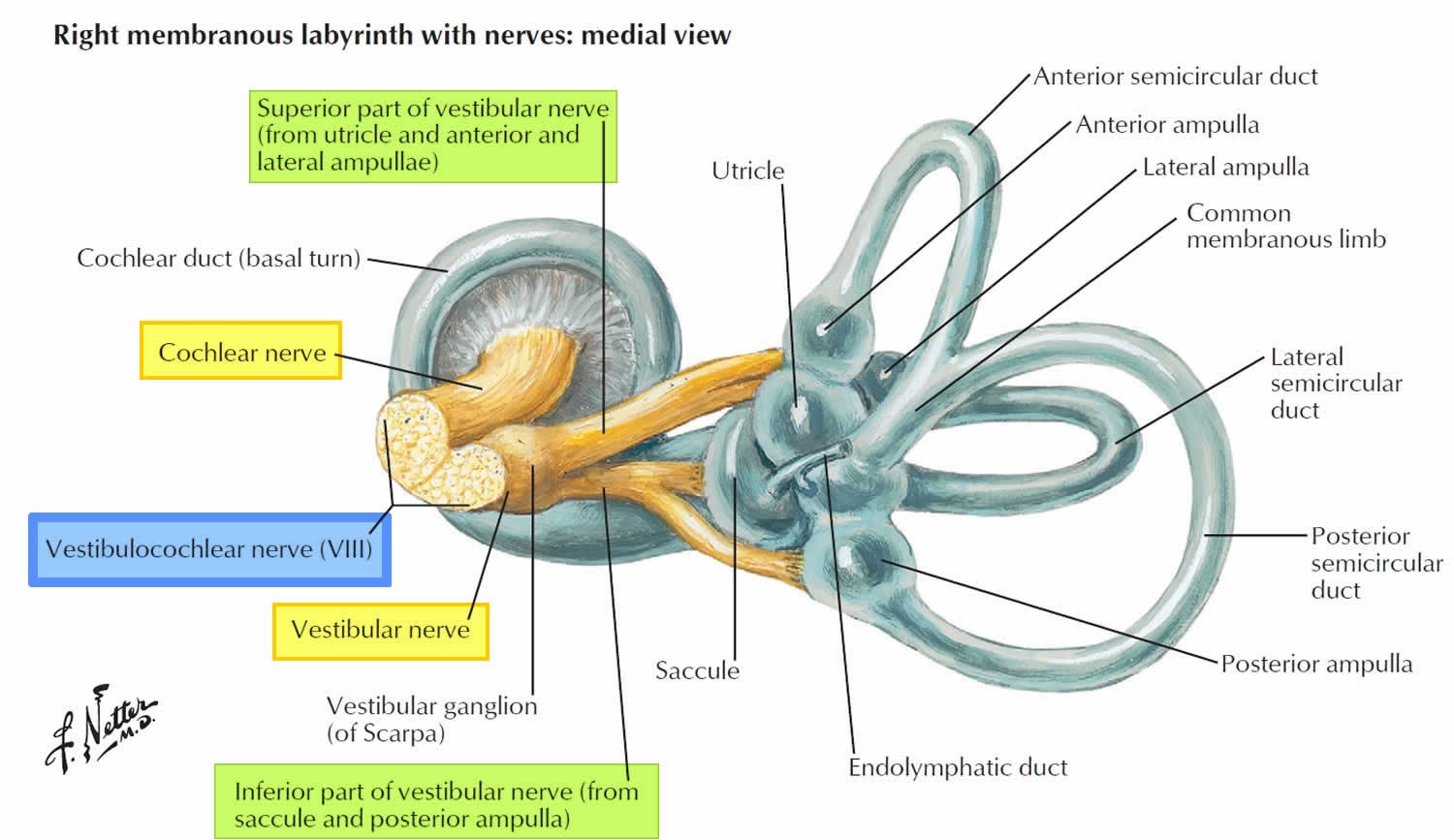
Figure 3. Vestibulocochlear nerve in the temporal bone
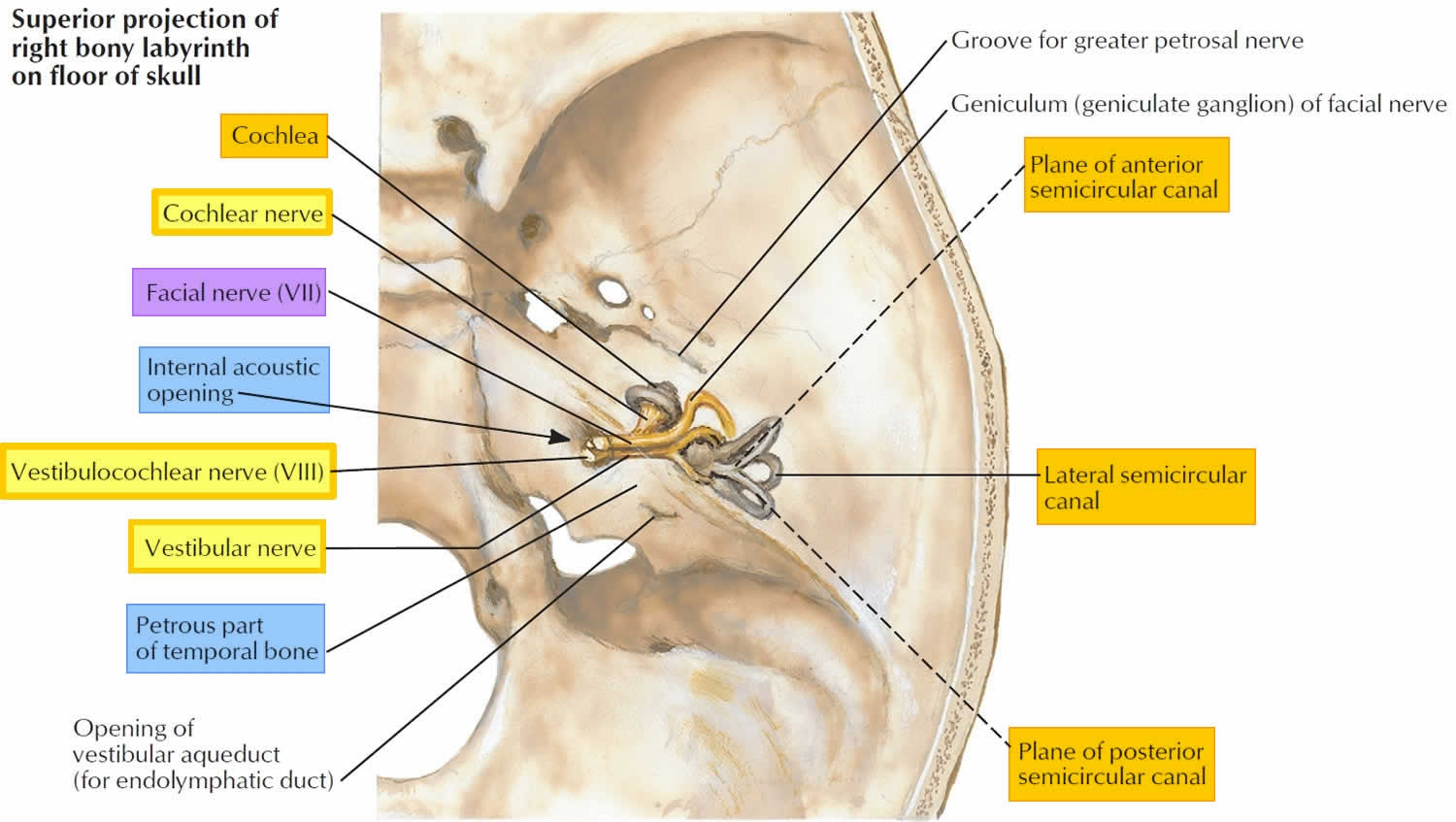
Figure 4. Vestibulocochlear nerve enters the brain stem at the pons
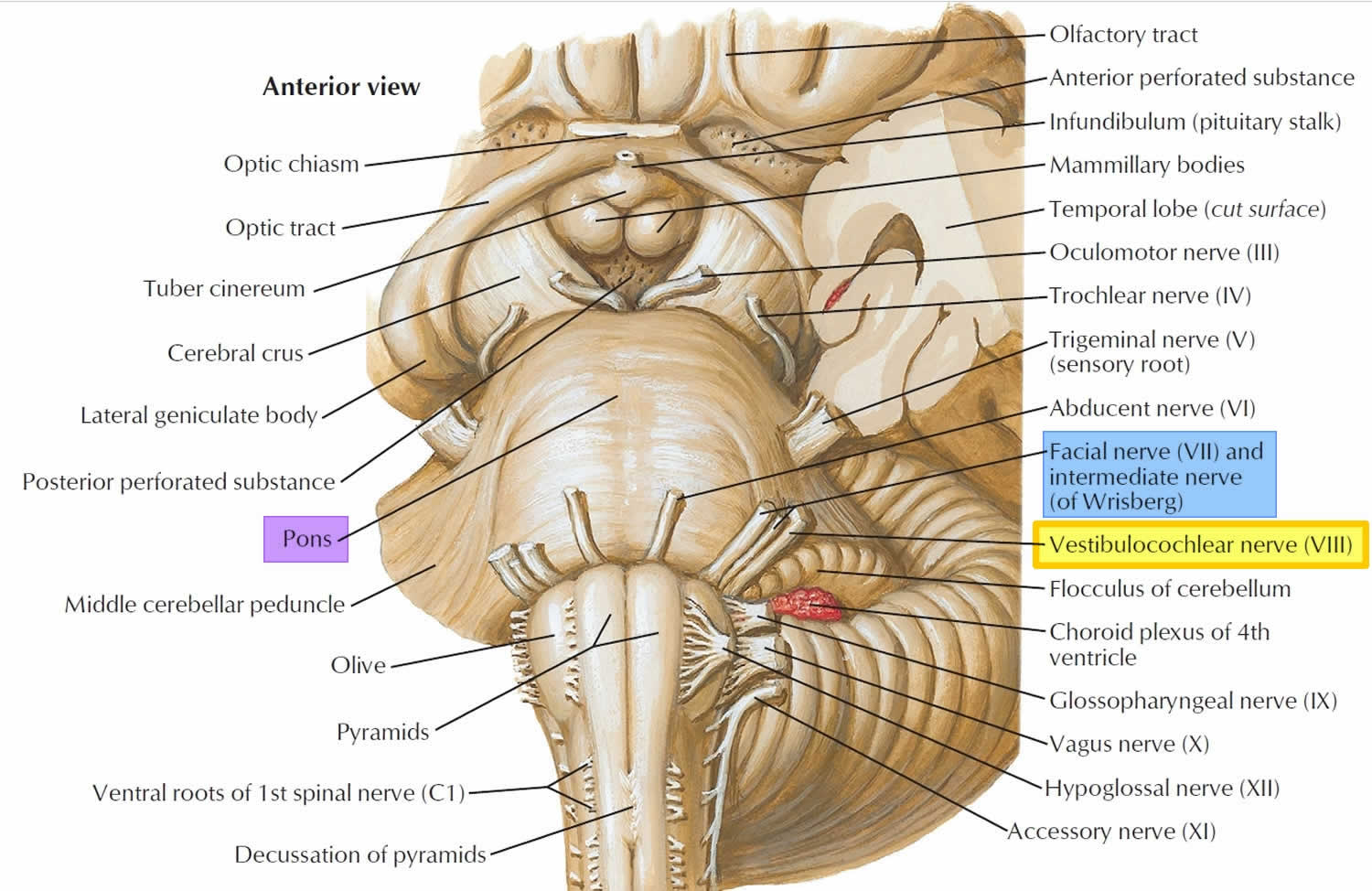
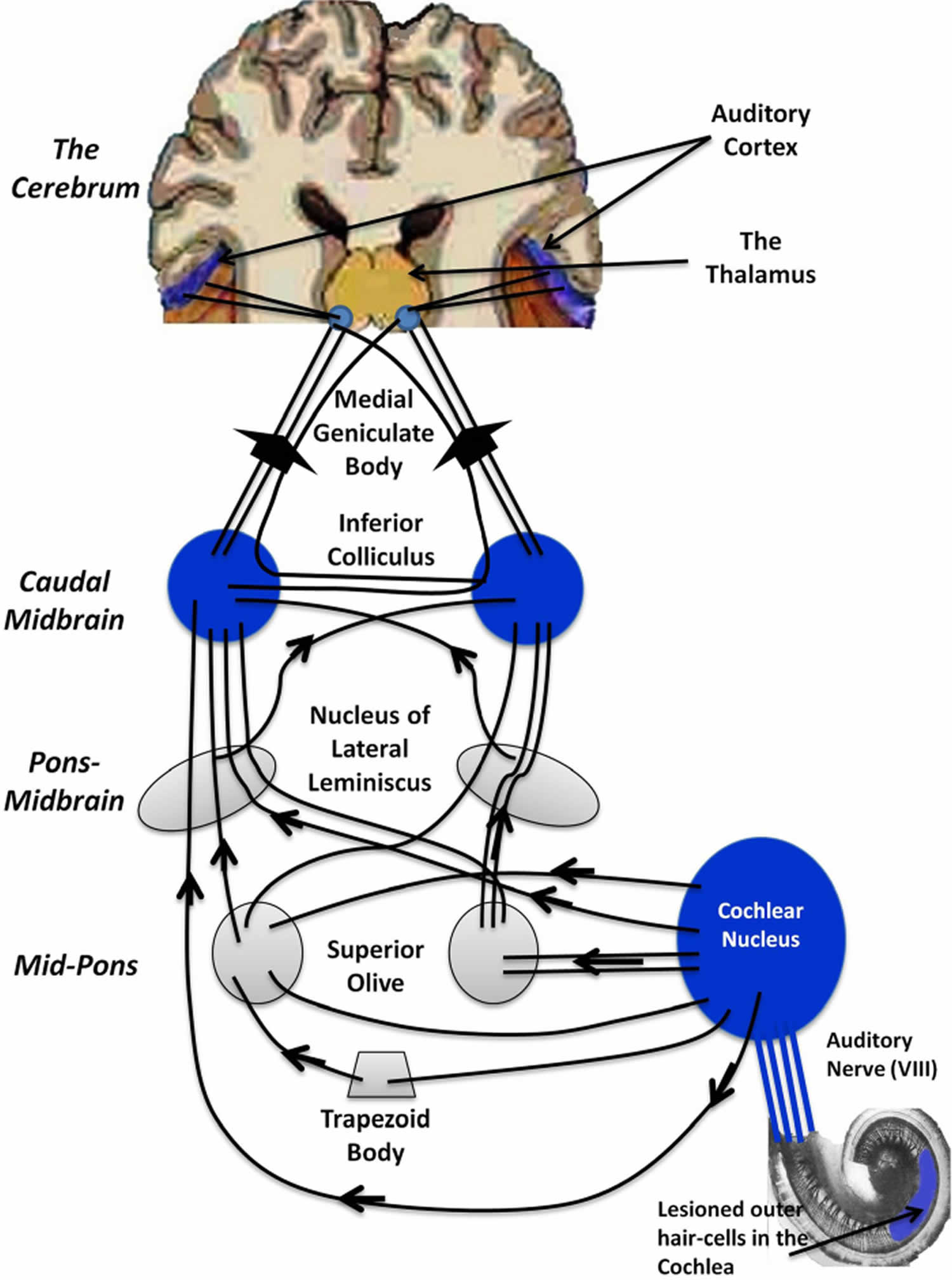
Figure 5. Peripheral and central auditory pathways
Vestibulocochlear nerve function
Two nerves – the vestibular nerve and the cochlear nerve – each with different functions form the vestibulocochlear nerve.
- Vestibular nerve for balance and equilibrium.
- Cochlear nerve for hearing.
Cochlear nerve and auditory system
The cochlear nerve is responsible for transmitting auditory signals from the inner ear to the cochlear nuclei within the brainstem and ultimately to the primary auditory cortex within the temporal lobe 13, 14.
The cochlea is a spiral, fluid-filled cavity in the bony auditory labyrinth that contains the organ of Corti along its basilar membrane (Figure 1). The bipolar neurons making up the spiral (cochlear) ganglion create the link between the central nervous system and the organ of Corti 15. The spiral ganglion is located at the spiral canal of the modiolus. Type 1 and Type 2 neurons populate the spiral (cochlear) ganglion, and both send peripheral processes to the ciliated hair cells of the organ of Corti and central processes that join together to form the cochlear nerve. Type 1 neurons are comparatively larger, myelinated, and account for 90% of cochlear nerve cells 5, 16, 17, 18. Type 2 neurons are smaller and nonmyelinated. Type 1 neurons project to the inner hair cells of the organ of Corti, while Type 2 neurons project to the outer hair cells 5, 16, 17, 18.
Central projections from the spiral (cochlear) ganglion form the cochlear nerve before entering the internal auditory canal. Within the internal auditory canal, the cochlear nerve joins the vestibular nerve to form vestibulocochlear nerve (CN VIII). The nerve fibers run past the cerebellopontine angle and enter the brainstem at the pontomedullary junction to innervate the cochlear nuclei within the rostral pole of the upper medulla. There are three divisions of the cochlear nuclei: anteroventral cochlear nucleus (AVCN), dorsal cochlear nucleus (DCN), and posteroventral cochlear nucleus (PVCN) 5, 16, 14.
Upon entering the brainstem, the cochlear nerve separates from the vestibular nerve and branches into anterior and posterior divisions. The anterior division innervates the anteroventral cochlear nucleus (AVCN), while the posterior division innervates the dorsal cochlear nucleus (DCN), and posteroventral cochlear nucleus (PVCN) 15. Cochlear nerve fibers are characterized tonotopically. Afferent nerve fibers from hair cells at the base of the cochlea transmit high frequencies. The afferents from the apex of the cochlea transmit low frequencies 15. This organization is preserved within the cochlear nuclei 14.
After the cochlear nuclei, the fibers cross and join the contralateral lateral lemniscus toward the midbrain inferior colliculus. Next, the fibers reach the thalamic medial geniculate nucleus before traveling to the primary auditory cortex, within the temporal lobe 13, 14.
Vestibular nerve and vestibular system
The vestibular nerve has complex functions. The vestibular nerve relays information related to motion, position and it is essential for posture and standing. The vestibular system involves coordinated communication between the vestibular apparatus (semicircular canals, saccule, utricle), ocular muscles, postural muscles, brainstem, and cerebral cortex 13, 7. The vestibular system is also essential for the auditory system, as it has been shown that the same sound affects the postural control 10. The vestibular system interacts for the control of blood pressure, using sympathetic communication and the baroreceptors of the carotid and the aortic arch 11.
The peripheral vestibular apparatus is located within the temporal bone, and it consists of a bony and membranous labyrinth. The membranous labyrinth contains the sensory neuroepithelium and is located within the bony labyrinth, suspended in perilymph. The vestibular apparatus has five components: the utricle, saccule, and three semicircular ducts (contained within the semicircular canals). The two types of neuroepithelium are the macula and crista ampullaris, which both contain sensory hair cells. The utricle and saccule contain macula, while the semicircular canals contain crista ampullaris 7.
The utricle and saccule sense the positioning of the head in space. Hair cells within the utricle respond to horizontal acceleration, while the hair cells within the saccule respond to vertical acceleration. The hair cells within the three semicircular ducts (lateral, superior, and posterior) respond to angular acceleration or head rotation 7.
The stimulation of the hair cells results in depolarization and increased calcium (Ca) influx, leading to increased firing of afferent vestibular nerve fibers. Those fibers travel to the vestibular ganglion (Scarpa’s ganglion), located in the internal auditory canal. The vestibular ganglion (Scarpa’s ganglion) is composed of bipolar neurons that send peripheral processes to the vestibular apparatus and central processes that join together to form the vestibular nerve. The vestibular ganglion (Scarpa’s ganglion) is separated into superior and inferior divisions. The superior division receives input from the utricle and superior and lateral semicircular ducts. The inferior division receives input from the saccule and posterior semicircular duct 7.
The superior and inferior post-ganglionic extensions join to form the vestibular nerve, which joins the cochlear nerve to become the vestibulocochlear nerve (CN VIII) within the internal auditory canal. Vestibulocochlear nerve (CN VIII) runs past the cerebellopontine angle and enters the brainstem at the pontomedullary junction. The vestibular nerve separates from the cochlear nerve before reaching the vestibular nuclear complex. The vestibular nuclear complex consists of four nuclei: medial, lateral, superior, and inferior. These nuclei range from the caudal pons to the rostral medulla in two columns and are closely related to the floor of the fourth ventricle 7. The vestibular nuclear complex receives input from the ipsilateral cerebellum, as well as the vestibular nerve, and projects to various ipsilateral and contralateral structures.
The medial nucleus receives input from the lateral semicircular ducts. It sends ascending fibers to the motor nuclei of the extraocular muscles ipsilaterally and contralateral via the medial longitudinal fasciculus (MLF), which helps facilitate the vestibulo-ocular reflex. The medial nucleus also helps mediate the vestibulospinal reflex by controlling head and neck movements 7.
The superior nucleus receives input from the superior and posterior semicircular ducts and mediates the vestibulo-ocular reflex 7. Furthermore, it projects to chiefly the ventral posterior intermediate nucleus of bilateral thalami in an ascending projection thought to play a fundamental role in conscious spatial awareness 8, mediating onward thalamocortical circuits 9.
The lateral nucleus receives input from all components of the vestibular apparatus and the vestibulocerebellum. Descending projections become the lateral vestibular tract within the ipsilateral spinal cord. This tract helps mediate the vestibulospinal reflex and maintain posture and balance 7.
The inferior nucleus receives input from the utricle and saccule and sends fibers to the other three vestibular nuclei and the cerebellum 7.
It has also been suggested that the auditory stimuli interact with the vestibular system to influence postural control 10. Additionally, the vestibular system helps control blood pressure by using sympathetic pathways and the baroreceptors on the carotid and the aortic arch 11.
Specifics regarding vestibular cortical connections are not well understood, but studies have suggested that the vestibular cortical area is adjacent to the parietal or insular cortex 7.
Vestibulocochlear nerve test
Testing of the vestibulocochlear nerve involves assessing both components of it via hearing assessment and the Weber and Rinne tuning fork tests before progressing onto more advanced formal testing 19, 20, 21.
Weber test is a useful, quick, and simple screening hearing tuning fork test used to establish a diagnosis in patients with unilateral (one-sided) conductive and unilateral (one-sided) sensorineural hearing loss 22. The outer and middle ear mediate conductive hearing. The inner ear mediates sensorineural hearing. The Weber test is often combined with the Rinne test to detect the location and nature of the hearing loss.
Weber test procedure 21:
- Place the vibrating tuning fork (512 Hz) on the vertex (other common sites used are the midline of the forehead, bridge of the nose, and chin), equidistant from both ears. These vibrations will be conducted through the skull and reach the cochlea. (The 512 Hz tuning fork should be struck against the elbow or knee of the patient to vibrate. While striking care must be taken that the strike is made at the junction of the upper 1/3 and lower 2/3 of the fork. This is the maximum vibratory area of the tuning fork. It should not be struck against metallic object because it can cause overtones. )
- Ask the patient whether it is heard loudest in either one side or the midline (e.g., “Is the sound louder in your right ear, left ear, or the middle?”)
Weber test interpretation 21:
- With symmetrical hearing or symmetrical hearing loss the sound should be central.
- With a unilateral (one-sided) sensorineural hearing loss the sound should be heard in the better ear.
- With a unilateral (one-sided) conductive hearing loss the sound should be heard in the poorer ear. This is because the conduction problem masks the ambient noise of the room, whilst the well-functioning inner ear picks the sound up via the bones of the skull causing it to be perceived as a louder sound than in the unaffected ear.
Points to note: Interpretation of the Weber test in isolation can be prone to error. Thiagarajan and Arjunan 23 suggest the Weber test can determine a difference of 5 decibels between each ear in terms of bone conduction thresholds at the frequency being tested. Weber test can be complicated by the presence of a unilateral or asymmetrical conductive hearing loss, where the tone can be heard on the conductive side or the side with the greater conductive loss.
Rinne test is a hearing tuning test used to evaluate the conductive hearing loss in one ear 24. Rinne test differentiates sound transmission via air conduction from sound transmission via bone conduction through the mastoid. Rinne test can serve as a quick screen for conductive hearing loss. Under normal circumstances, air conduction is better than bone conduction. Rinne test is performed in both the ears. A Rinne test should be done with a Weber test to detect a sensorineural hearing loss and thus confirm the nature of hearing loss 25.
Rinne test bone conduction technique 21:
- Place the vibrating tuning fork (512 Hz) on the mastoid process. (The 512 Hz tuning fork should be struck against the elbow or knee of the patient to vibrate. While striking care must be taken that the strike is made at the junction of the upper 1/3 and lower 2/3 of the fork. This is the maximum vibratory area of the tuning fork. It should not be struck against metallic object because it can cause overtones.)
- Place your other hand gently, but firmly to cover the opposite ear to ensure enough counter-pressure is applied.
- The patient should report when the sound can no longer be heard
- As soon as the patient signals that he is unable to hear the fork anymore the vibrating fork is transferred immediately just close to the ear canal to the ear without touching it and is held in such a way that the vibratory prongs vibrate parallel to the acoustic axis.
- The patient should indicate when air conduction of the sound can no longer be heard.
In patients with normal hearing he should be able to hear the fork as soon as it is transferred to the front of the ear. This result is known as Positive Rinne = Air conduction is better than bone conduction. Rinne positive test indicates either normal hearing or a sensorineural hearing loss 23, 21. In case of conductive deafness the patient will not be able to hear the fork as soon as it is transferred to the front of the ear. Bone conduction is better than air conduction is known as Negative Rinne 23. Negative Rinne (bone conduction is better than air conduction) occurs in conductive deafness. If the patient is suffering from severe sensorineural hearing loss predominantly on the test side then the sound will still be heard through the opposite ear this condition leads to a False Positive Rinne. False Positive Rinne occurs when the bone conduction transmits through the skull to the opposite ear and is detected through cross hearing by the better cochlea (in the non-test ear). It can be distinguished through considering if the Weber test result is contradictory and through asking the patient which ear the bone conduction part of the test was heard in.
Points to note: The Rinne test is able to distinguish a conductive hearing loss with an air-bone gap of 17.5 dB to 30 dB 26, 27. Rinne test has limited use detecting mild conductive hearing losses or mixed hearing losses where there is an air-bone gap of less than 17.5dB 21.
The specificity and sensitivity of both the Rinne and Weber tests have been evaluated 21. The sensitivity of both the Rinne and Weber tests is estimated at 76.86% and the specificity was projected to be 85.48% 28, 29. A subsequent study found that when using the Weber test in isolation as a screening tool for sudden sensorineural hearing loss it’s sensitivity was likely to be around 78% 30. The tester should therefore be aware of probable errors through administering tuning fork tests, particularly in isolation, rather than as part of a battery of tests 21.
To assess vestibular function, test for nystagmus and note the direction, duration, and trigger of the nystagmus. Further in-depth testing is used to distinguish central from peripheral sources, particularly if the patient is experiencing vertigo during the examination. Frenzel lenses or + 30 diopter glasses can be used to prevent visual fixation, which can suppress nystagmus. Testing involves the head thrust maneuver (for acute vestibular syndrome) or the Dix-Hallpike maneuver (for positional vertigo).
- The head thrust maneuver is performed by holding the head of the sitting patient while they focus on an object, such as the examiner’s nose, and quickly turning the patient’s head 20 degrees to the right or left. If the eyes remain focused on the examiner’s nose, this is a normal result. Temporary deviation away from the object with a corrective saccade that brings the eyes back to the object is indicative of a peripheral source of nystagmus, such as vestibular neuronitis.[29]
- For the Dix-Hallpike maneuver, the patient is quickly lowered to the supine position with the extended 45 degrees below the table and turned 45 degrees to one side. Note the direction and duration of nystagmus and assess for vertigo. Raise the patient back to the upright position and perform the maneuver with the head turned to the other side. Nystagmus with a 5 to 10-second latency period that is vertical when the eyes are turned away from the affected ear and rotary when the eyes face the involved ear is pathognomonic for benign paroxysmal positional vertigo. This response also diminishes with repeated testing. Positional nystagmus caused by central nervous system dysfunction will not have a latency period and will not diminish with further testing.
- Posturography. You stand in your bare feet on a platform and try to keep your balance under various conditions. This test tells your doctor which parts of the balance system you rely on the most and which parts may be giving you problems.
- The patient is made to walk with his/her eyes closed; if a change of direction occurs (or a positive Romberg test) it may be indicative of a unilateral vestibular lesion 31.
- Eye movement testing and eye-movement recordings. Your doctor may watch the path of your eyes when you track a moving object. And you may be given an eye motion test in which water or air is placed in your ear canal. Another way to see nystagmus is to spin a person around for about 30 seconds, stop and then have them try to stare at an object. If they have nystagmus, their eyes will first move slowly in one direction, then move rapidly in the opposite direction.
- Another test that can be performed is to observe the nystagmus according to how it behaves; this may be done by varying the position of the head and keeping it steady for 30 seconds (first sitting, then lying on the side, and keeping the head out of the bed slightly extended). If the nystagmus is persistent and changes direction with changes in the position of the head, it could mean an injury to the brainstem or posterior cranial fossa. If instead, the nystagmus disappears quickly and does not repeat itself in the other directions of the head, it should result in evidence of benign postural vertigo.
- Rotary chair testing. During this test you sit in a computer-controlled chair that moves very slowly in a full circle. At faster speeds, it moves back and forth in a very small arc.
- Also, the involvement of the facial nerve due to its proximity should not be excluded during the exam.
Several additional tests are often used to investigate vertigo, nystagmus, tinnitus, and sensorineural hearing loss:
- Tonal audiometry, which is a technique that studies bone (BC) and air (AC) conduction. In people with normal hearing, the BC is the same as the AC and sensory deafness, both curves are reduced
- Auditory evoked potentials (AEP), which measure electrical conduction in the auditory nerve running the cortex
- Electro-oculography: An electrical method of measuring eye movements using tiny electrodes
- Vestibular testing by recording the movements of the eyes
- MRI of the head visualizing the various auditory and vestibular anatomical structures
- Unenhanced CT scan of the head is useful to examine the bony structures of the labyrinth or if MRI of the head is contraindicated.
- In addition, you may be given blood tests to check for infection and other tests to check heart and blood vessel health.
Vestibulocochlear nerve damage
A variety of pathologies may affect the vestibulocochlear nerve (CN VIII) and result in vertigo, nystagmus, tinnitus, and sensorineural hearing loss for the patient. The pathologies that can affect the vestibulocochlear nerve (cranial nerve VIII) are multiple, from direct trauma to the nerve to problems associated with vascular compression, tumor formation, infection, vascular injury and congenital malformations.
Dysfunction of the cochlear nerve can occur anywhere in its path, central and peripheral, and be associated with a decrease in hearing, partial, total mono lateral or bilaterally. One can go from frank deafness to auditory hallucinations, from paracusia (the sound is felt for a few seconds even after its termination) to autophony (exaggerated resonance of one’s voice) 32. Another classic symptom is tinnitus, that is the perception of sounds in the absence of acoustic stimuli.
The most common mechanisms of auditory pathology are infarcts and demyelination (i.e., multiple sclerosis). Patients can present with unilateral or bilateral sensorineural loss, depending on the location of the injury. Additionally, traumatic injury to the temporal bone can present with unilateral sensorineural loss due to internal auditory canal or bony labyrinth fracture. There can also be a concussive injury to the labyrinth. Imaging studies for such injuries are typically negative unless an MRI shows an intralabyrinthine hemorrhage 14.
Notable congenital malformations of vestibulocochlear nerve (CN VIII) include aplasia or hypoplasia. These malformations are subdivided into three subtypes: 1, 2A, and 2B. Type 1 refers to an aplastic vestibulocochlear nerve (CN VIII) with a normal labyrinth. Type 2A refers to an aplastic/hypoplastic cochlear branch with an accompanying labyrinth malformation. Type 2B, the most common subtype, refers to an aplastic/hypoplastic cochlear branch but with a normal labyrinth 32.
The problems and pathologies affecting the vestibular nerve are highlighted with disturbances of balance, postural tonic deviations, vertigo, and nystagmus. Vestibular schwannomas (acoustic neuromas) are of Schwann cell origin, and they are the most common cerebellopontine angle tumors. All cranial nerves have a peripheral transition zone where glial myelination by oligodendrocytes gives way to peripheral myelination by Schwann cells 33. It was previously believed that all vestibular schwannomas arise from this transition zone, which for the vestibulocochlear nerve (CN VIII) lies between 9.28mm – 13.84 mm along its length after exiting the brainstem, in the medial third of the interior auditory canal 34. However, detailed anatomical study has revealed that schwannomas may occur at this point, as well as more laterally within the internal auditory canal and from the labyrinthine portion of the nerve 35.
Bilateral vestibular schwannomas are the hallmark sign of neurofibromatosis type 2 (NF-2), an autosomal dominant genetic syndrome. The usual presentation is progressive, unilateral sensorineural hearing loss, and commonly associated symptoms are tinnitus and vertigo. Notably, facial nerve (CN VII) palsy rarely occurs with vestibular schwannomas because the facial nerve is resistant to chronic pressure. MRI is the diagnostic imaging of choice 32, 36.
Acute vestibular syndrome is characterized by vertigo, nausea, vomiting, and gait disturbances with an acute onset (seconds to hours), which are associated with nystagmus and head-motion intolerance (days to weeks). The cause of acute vestibular syndrome can either be peripheral, most commonly vestibular neuritis, or central, such as brainstem or cerebellar stroke. Vestibular neuritis is usually viral in origin and self-limiting, while a central stroke can have permanent effects. Therefore, it is critical to distinguish between these two causes to ensure proper patient care. This can be done at the bedside using the “Head-Impulse—Nystagmus—Test-of-Skew” (HINTS) exam. The horizontal head-impulse test, which assesses the vestibulo-ocular reflex, would be normal with central etiologies and abnormal with peripheral etiologies. Nystagmus would be vertical and/or bidirectional with central etiologies and unidirectional with peripheral etiologies, regardless of gaze direction. Skew deviation would be present with central etiologies and absent with peripheral causes 37.
Also, the involvement of the facial nerve due to its proximity should not be excluded during evaluation.
Acoustic neuroma
Acoustic neuroma also known as a vestibular schwannoma, is a benign (non-cancerous) tumor of the vestibulocochlear nerve. Treatment modalities include microsurgical removal or radiotherapy. In some special cases, a waiting policy may be advisable. In its growth, the tumor can reach large dimensions and affect the nearby cranial nerves or the brain stem. Acoustic neuroma originates from the lining sheaths of the vestibulocochlear nerve.
The cause of acoustic neuroma is not well understood. For most acoustic neuromas, the cause at the level of the cellular machinery is the failure of a “governor” gene to exert its effect in suppressing the growth of Schwann cells—those cells responsible for coating nerve fibers with insulation. The result is “wart-like” growth of these cells to produce the neuroma.
The only environmental exposure that has been definitively associated with an increased incidence is high-dose, therapeutic radiation exposure to the head. While studying the association between cell phone use and the development of these tumors is difficult, the scientific community does not generally accept that any relationship has been proven.
For the most part it is not an inherited disease; however, 5% of cases are associated with a genetic disorder called neurofibromatosis type 2. These individuals demonstrate two-sided vestibular tumors often associated with other tumors around the brain and/or in the spine. The vast majority of acoustic neuromas are sporadic (nonhereditary).
The main and most important possible risks of vestibulocochlear nerve surgery are from tumors (meningiomas, lipomas, acoustic neurinoma or schwannomas).
Acoustic neuroma symptoms may include:
- Loss of hearing
- Tinnitus
- Disorders of taste and dryness of the mouth
- Vertigo and balance disorders
- Paralysis of the facial nerve
- Ocular complications
- Cerebral fluid loss after surgery
- Cerebral edema
Once the symptoms appear, a thorough ear examination and hearing and balance testing (audiogram, electronystagmography, auditory brainstem responses) are essential for proper diagnosis. The most effective instrumental examination in making an immediate diagnosis is magnetic resonance imaging (MRI). Magnetic resonance imaging (MRI) scans are critical in the early detection of a vestibular schwannoma and are helpful in determining the location and size of a tumor and in planning its microsurgical removal.
Early diagnosis of a vestibular schwannoma is key to preventing its serious consequences. There are three options for managing a vestibular schwannoma: (1) surgical removal, (2) radiation, and (3) observation. Sometimes, the tumor is surgically removed (excised). The exact type of operation done depends on the size of the tumor and the level of hearing in the affected ear. If the tumor is small, hearing may be saved and accompanying symptoms may improve by removing it to prevent its eventual effect on the hearing nerve. As the tumor grows larger, surgical removal is more complicated because the tumor may have damaged the nerves that control facial movement, hearing, and balance and may also have affected other nerves and structures of the brain.
The removal of tumors affecting the hearing, balance, or facial nerves can sometimes make the patient’s symptoms worse because these nerves may be injured during tumor removal.
As an alternative to conventional surgical techniques, radiosurgery (that is, radiation therapy—the “gamma knife” or LINAC) may be used to reduce the size or limit the growth of the tumor. Radiation therapy is sometimes the preferred option for elderly patients, patients in poor medical health, patients with bilateral vestibular schwannoma (tumor affecting both ears), or patients whose tumor is affecting their only hearing ear. When the tumor is small and not growing, it may be reasonable to “watch” the tumor for growth. MRI scans are used to carefully monitor the tumor for any growth.
- Bordoni B, Sugumar K, Daly DT. Neuroanatomy, Cranial Nerve 8 (Vestibulocochlear) [Updated 2019 Apr 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537359[↩]
- Sonne J, Lopez-Ojeda W. Neuroanatomy, Cranial Nerve. [Updated 2019 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470353[↩]
- Kentala E, Pyykkö I. Clinical picture of vestibular schwannoma. Auris Nasus Larynx. 2001 Jan;28(1):15-22.[↩]
- Acoustic neuroma. Consens Statement. 1991 Dec 11-13;9(4):1-24.[↩]
- Benoudiba F, Toulgoat F, Sarrazin JL. The vestibulocochlear nerve (VIII). Diagn Interv Imaging. 2013 Oct;94(10):1043-50. https://doi.org/10.1016/j.diii.2013.08.015[↩][↩][↩][↩]
- Pickles JO. Auditory pathways: anatomy and physiology. Handb Clin Neurol. 2015;129:3-25. doi: 10.1016/B978-0-444-62630-1.00001-9[↩]
- Khan S, Chang R. Anatomy of the vestibular system: a review. NeuroRehabilitation. 2013;32(3):437-43. doi: 10.3233/NRE-130866[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Lopez C, Blanke O. The thalamocortical vestibular system in animals and humans. Brain Res Rev. 2011 Jun 24;67(1-2):119-46. doi: 10.1016/j.brainresrev.2010.12.002[↩][↩]
- Wijesinghe R, Protti DA, Camp AJ. Vestibular Interactions in the Thalamus. Front Neural Circuits. 2015 Dec 2;9:79. doi: 10.3389/fncir.2015.00079[↩][↩]
- Ross JM, Balasubramaniam R. Auditory white noise reduces postural fluctuations even in the absence of vision. Exp Brain Res. 2015 Aug;233(8):2357-63. doi: 10.1007/s00221-015-4304-y[↩][↩][↩]
- Holstein GR, Friedrich VL Jr, Martinelli GP. Projection neurons of the vestibulo-sympathetic reflex pathway. J Comp Neurol. 2014 Jun 15;522(9):2053-74. doi: 10.1002/cne.23517[↩][↩][↩]
- Adjamian P, Hall DA, Palmer AR, Allan TW, Langers DR. Neuroanatomical abnormalities in chronic tinnitus in the human brain. Neurosci Biobehav Rev. 2014 Sep;45:119-33. doi: 10.1016/j.neubiorev.2014.05.013[↩]
- Sanders RD, Gillig PM. Cranial Nerve VIII: Hearing and Vestibular Functions. Psychiatry (Edgmont). 2010 Mar;7(3):17-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2861521[↩][↩][↩]
- Swartz JD. Pathology of the vestibulocochlear nerve. Neuroimaging Clin N Am. 2008 May;18(2):321-46, x-xi. doi: 10.1016/j.nic.2008.02.001[↩][↩][↩][↩][↩]
- Bordoni B, Mankowski NL, Daly DT. Neuroanatomy, Cranial Nerve 8 (Vestibulocochlear) [Updated 2022 May 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537359[↩][↩][↩]
- Pickles JO. Auditory pathways: anatomy and physiology. Handb Clin Neurol. 2015;129:3-25. https://doi.org/10.1016/B978-0-444-62630-1.00001-9[↩][↩][↩]
- Nayagam BA, Muniak MA, Ryugo DK. The spiral ganglion: connecting the peripheral and central auditory systems. Hear Res. 2011 Aug;278(1-2):2-20. doi: 10.1016/j.heares.2011.04.003[↩][↩]
- Yang T, Kersigo J, Jahan I, Pan N, Fritzsch B. The molecular basis of making spiral ganglion neurons and connecting them to hair cells of the organ of Corti. Hear Res. 2011 Aug;278(1-2):21-33. doi: 10.1016/j.heares.2011.03.002[↩][↩]
- Chapter 8 – Vestibulocochlear Nerve. Clinical Anatomy of the Cranial Nerves 2014, Pages 81-93. https://doi.org/10.1016/B978-0-12-800898-0.00008-7[↩]
- Ng M, Jackler RK. Early history of tuning-fork tests. Am J Otol. 1993;14:100–5. doi: 10.1016/0196-0709(93)90047-B[↩]
- https://www.thebsa.org.uk/wp-content/uploads/2022/02/OD104-51-BSA-Recommended-Procedure-Rinne-Weber-Tuning-Fork-Tests-February-2022.pdf[↩][↩][↩][↩][↩][↩][↩][↩]
- Wahid NWB, Hogan CJ, Attia M. Weber Test. [Updated 2023 Feb 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526135[↩]
- Thiagarajan B, Arjunan K. Tuning Fork Tests. WebmedCentral OTORHINOLARYNGOLOGY 2012;3(4):WMC003279 doi: 10.9754/journal.wmc.2012.003279[↩][↩][↩]
- Kong EL, Fowler JB. Rinne Test. [Updated 2019 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431071[↩]
- Wahid NWB, Attia M. Weber Test. [Updated 2019 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526135[↩]
- Jacob V, Alexander P, Nalinesha KM, Nayar RC. Can Rinne’s test quantify hearing loss? Ear Nose Throat J. 1993 Feb;72(2):152-3.[↩]
- Burkey JM, Lippy WH, Schuring AG, Rizer FM. Clinical utility of the 512-Hz Rinne tuning fork test. Am J Otol. 1998 Jan;19(1):59-62.[↩]
- Boatman DF, Miglioretti DL, Eberwein C, Alidoost M, Reich SG. How accurate are bedside hearing tests? Neurology. 2007 Apr 17;68(16):1311-4. doi: 10.1212/01.wnl.0000259524.08148.16[↩]
- Vikram KB, Naseeruddin K. Combined tuning fork tests in hearing loss: explorative clinical study of the patterns. J Otolaryngol. 2004 Aug;33(4):227-34. doi: 10.2310/7070.2004.00227[↩]
- Shuman AG, Li X, Halpin CF, Rauch SD, Telian SA. Tuning fork testing in sudden sensorineural hearing loss. JAMA Intern Med. 2013 Apr 22;173(8):706-7. doi: 10.1001/jamainternmed.2013.2813[↩]
- Butskiy O, Ng D, Hodgson M, Nunez DA. Rinne test: does the tuning fork position affect the sound amplitude at the ear? J Otolaryngol Head Neck Surg. 2016 Mar 24;45:21[↩]
- De Foer B, Kenis C, Van Melkebeke D, Vercruysse JP, Somers T, Pouillon M, Offeciers E, Casselman JW. Pathology of the vestibulocochlear nerve. Eur J Radiol. 2010 May;74(2):349-58. doi: 10.1016/j.ejrad.2009.06.033[↩][↩][↩]
- Haller S, Etienne L, Kövari E, Varoquaux AD, Urbach H, Becker M. Imaging of Neurovascular Compression Syndromes: Trigeminal Neuralgia, Hemifacial Spasm, Vestibular Paroxysmia, and Glossopharyngeal Neuralgia. AJNR Am J Neuroradiol. 2016 Aug;37(8):1384-92. doi: 10.3174/ajnr.A4683[↩]
- Guclu B, Sindou M, Meyronet D, Streichenberger N, Simon E, Mertens P. Anatomical study of the central myelin portion and transitional zone of the vestibulocochlear nerve. Acta Neurochir (Wien). 2012 Dec;154(12):2277-83; discussion 2283. doi: 10.1007/s00701-012-1479-x[↩]
- Roosli C, Linthicum FH Jr, Cureoglu S, Merchant SN. What is the site of origin of cochleovestibular schwannomas? Audiol Neurootol. 2012;17(2):121-5. doi: 10.1159/000331394[↩]
- Heman-Ackah SE, Golfinos JG, Roland JT Jr. Management of surgical complications and failures in acoustic neuroma surgery. Otolaryngol Clin North Am. 2012 Apr;45(2):455-70, x. doi: 10.1016/j.otc.2011.12.012[↩]
- Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009 Nov;40(11):3504-10. doi: 10.1161/STROKEAHA.109.551234[↩]

{kind=link}