Heart arrhythmia
A heart arrhythmia, also known as an irregular heartbeat, is a problem with the rate or rhythm of your heartbeat. An arrhythmia occurs when your heart beats too fast (also called tachycardia with more than 100 beats per minute), too slow (also called bradycardia with less than 60 beats per minute), or irregularly due to problems with the electrical signals that control your heartbeat. The term “arrhythmia” refers to any change from the normal sequence of electrical impulses causing abnormal heart rhythms 1. During an arrhythmia, your heart can beat too fast, too slow, or with an irregular rhythm 2. When your heart doesn’t beat properly, not enough blood and oxygen is pumped around your body. As a result, your muscles and organs don’t get enough oxygen and nutrients. This may cause fluid to build up in your body, legs and make you feel breathless or tired. When your heart doesn’t pump blood effectively, your lungs, brain and all other organs can’t work properly and may shut down or be damaged.
- A heartbeat that is too fast is called tachycardia (in adults, more than 100 beats per minute) 1.
- A heartbeat that is too slow is called bradycardia (less than 60 beats per minute) 1.
- Atrial fibrillation is the most common type of irregular heartbeat 3. The abnormal firing of electrical impulses causes the atria (the top chambers in the heart) to quiver (or fibrillate).
The normal heart is a strong, muscular pump a little larger than a fist. It pumps blood continuously through the circulatory system.
- Each day the average heart beats (expands and contracts) 100,000 times and pumps about 2,000 gallons (7570 liters) of blood through your body.
- In a 70-year lifetime, an average human heart beats more than 2.5 billion times.
Most arrhythmias are harmless, but some can be serious or even life threatening. During an arrhythmia, the heart may not be able to pump enough blood to the body. Lack of blood flow can damage the brain, heart, and other organs.
How your Heart Works
Your heart is a muscular organ that pumps blood to your body. Your heart is at the center of your circulatory system. This system consists of a network of blood vessels, such as arteries, veins, and capillaries. These blood vessels carry blood to and from all areas of your body.
An electrical system controls your heart and uses electrical signals to contract the heart’s walls. When the walls contract, blood is pumped into your circulatory system. Inlet and outlet valves in your heart chambers ensure that blood flows in the right direction.
Your heart is vital to your health and nearly everything that goes on in your body. Without the heart’s pumping action, blood can’t move throughout your body.
Your blood carries the oxygen and nutrients that your organs need to work well. Blood also carries carbon dioxide (a waste product) to your lungs so you can breathe it out.
A healthy heart supplies your body with the right amount of blood at the rate needed to work well. If disease or injury weakens your heart, your body’s organs won’t receive enough blood to work normally.
The heart has two sides, separated by an inner wall called the septum. The right side of the heart pumps blood to the lungs to pick up oxygen. The left side of the heart receives the oxygen-rich blood from the lungs and pumps it to the body.
Figure 1. The anatomy of human heart
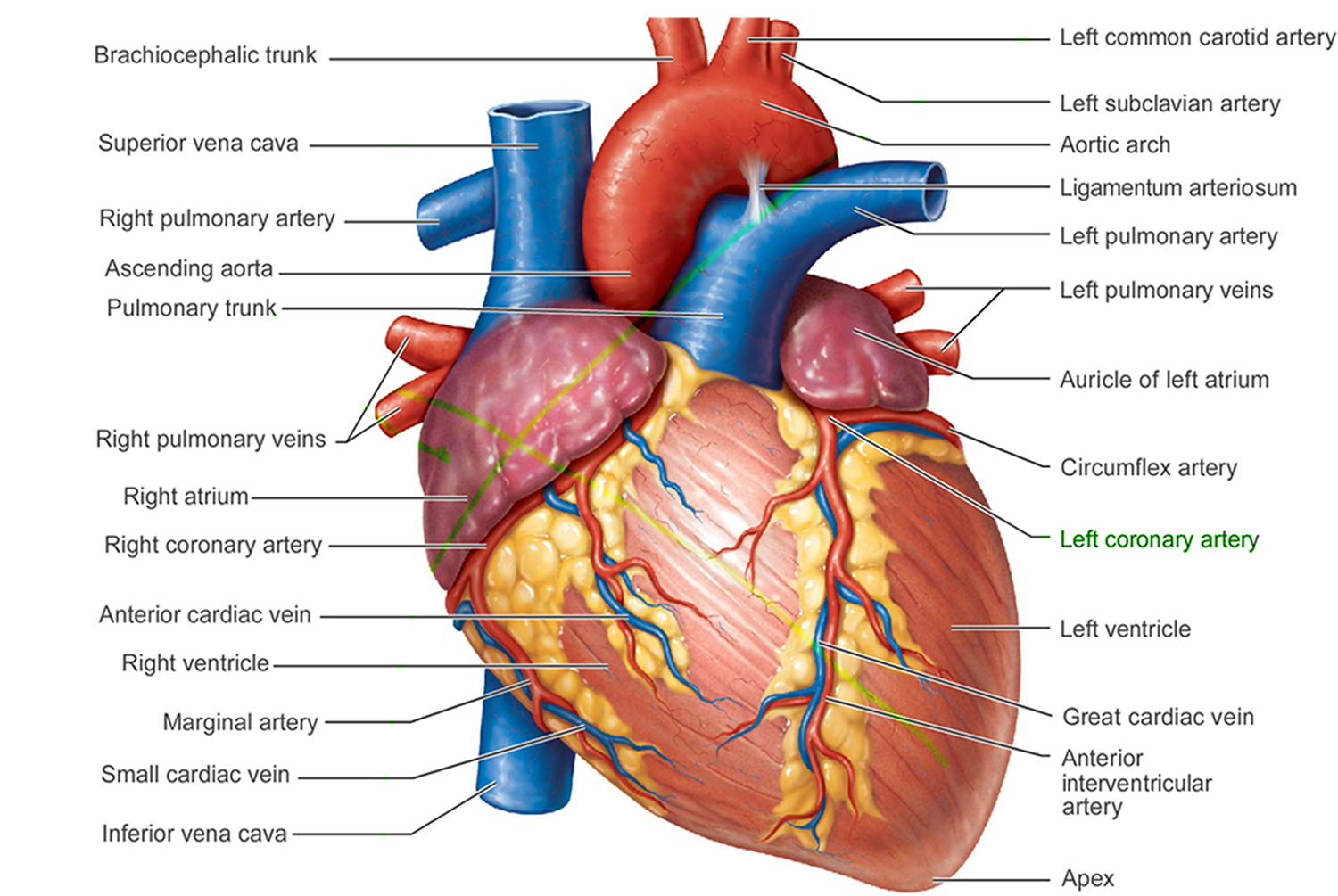
Figure 2. The anatomy of the heart chambers

Figure 3. Normal heart blood flow

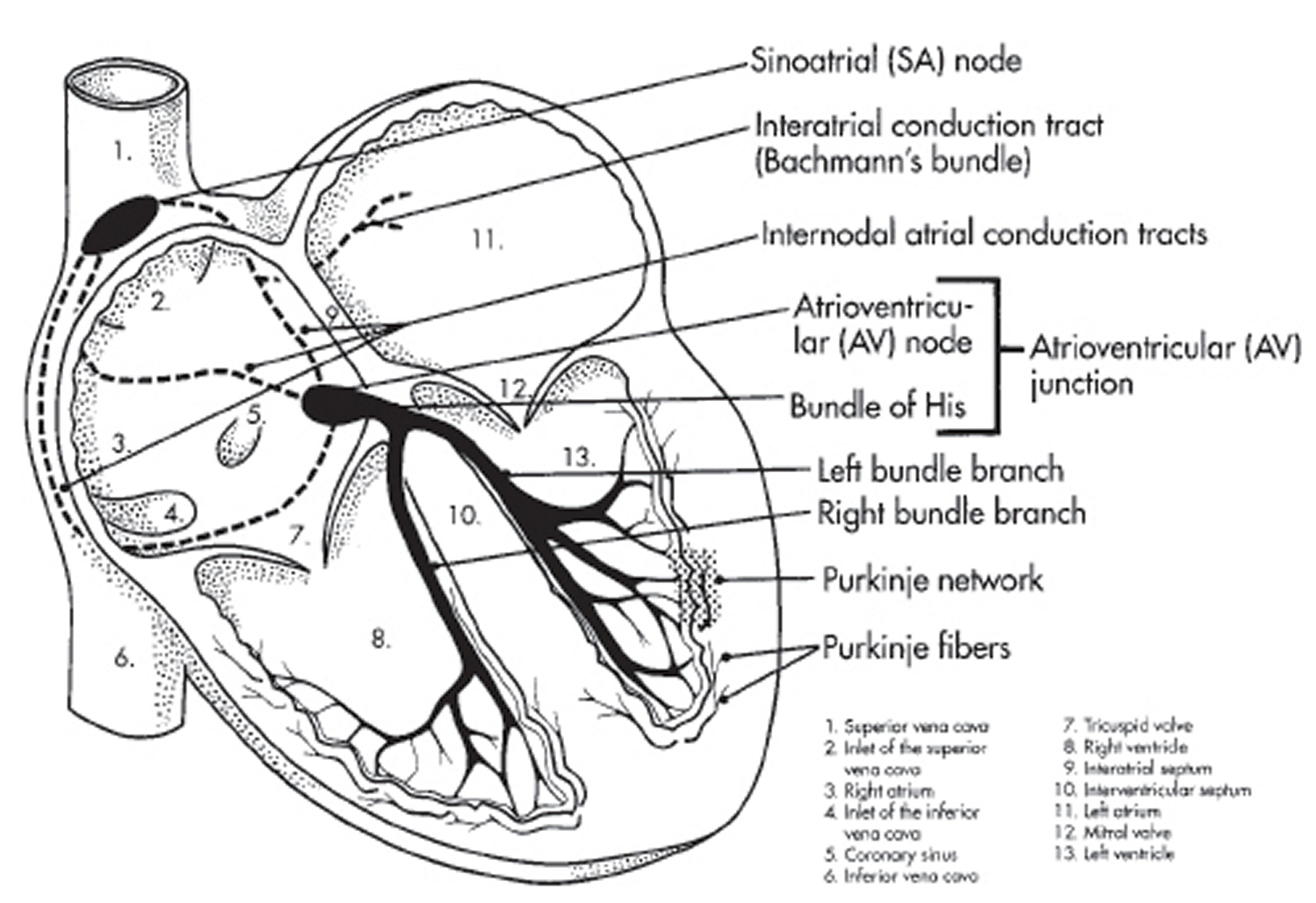
Figure 4. The heart’s electrical system

Heart Chambers
The heart has four chambers 1, two on the right and two on the left:
- 2 upper chambers are called atrium (two is called an atria). The atria collect blood as it flows into the heart.
- 2 lower chambers are called ventricles. The ventricles pump blood out of the heart to the lungs or other parts of the body.
The heart also has four valves that open and close to let blood flow from the atria to the ventricles and from the ventricles into the two large arteries connected to the heart in only one direction when the heart contracts (beats). The four heart valves are:
- Tricuspid valve, located between the right atrium and right ventricle
- Pulmonary or pulmonic valve, between the right ventricle and the pulmonary artery. This artery carries blood from the heart to the lungs.
- Mitral valve, between the left atrium and left ventricle
- Aortic valve, between the left ventricle and the aorta. This aorta carries blood from the heart to the body.
Each valve has a set of flaps (also called leaflets or cusps). The mitral valve has two flaps; the others have three. Valves are like doors that open and close. They open to allow blood to flow through to the next chamber or to one of the arteries. Then they shut to keep blood from flowing backward. Blood flow occurs only when there’s a difference in pressure across the valves, which causes them to open. Under normal conditions, the valves permit blood to flow in only one direction.
The heart four chambers and four valves and is connected to various blood vessels. Veins are blood vessels that carry blood from the body to the heart. Arteries are blood vessels that carry blood away from the heart to the body.
The heart pumps blood to the lungs and to all the body’s tissues by a sequence of highly organized contractions of the four chambers. For the heart to function properly, the four chambers must beat in an organized way.
When the heart’s valves open and close, they make a “lub-DUB” sound that a doctor can hear using a stethoscope 4.
- The first sound—the “lub”—is made by the mitral and tricuspid valves closing at the beginning of systole. Systole is when the ventricles contract, or squeeze, and pump blood out of the heart.
- The second sound—the “DUB”—is made by the aortic and pulmonary valves closing at the beginning of diastole. Diastole is when the ventricles relax and fill with blood pumped into them by the atria.
Arteries
The arteries are major blood vessels connected to your heart.
- Pulmonary artery carries blood from the right side of the heart to the lungs to pick up a fresh supply of oxygen.
- Aorta is the main artery that carries oxygen-rich blood from the left side of the heart to the body.
- Coronary arteries are the other important arteries attached to the heart. They carry oxygen-rich blood from the aorta to the heart muscle, which must have its own blood supply to function.
Veins
The veins also are major blood vessels connected to your heart.
- Pulmonary veins carry oxygen-rich blood from the lungs to the left side of the heart so it can be pumped to the body.
- Superior vena cava (SVC) and inferior vena cava (IVC) are large veins that carry oxygen-poor blood from the body back to the heart.
Blood Flow
The Right Side of Your Heart
In figure 3 above, the superior vena cava (SVC) and inferior vena cava (IVC) are shown in blue to the left of the heart muscle as you look at the picture. These veins are the largest veins in your body.
After your body’s organs and tissues have used the oxygen in your blood, the vena cavae carry the oxygen-poor blood back to the right atrium of your heart.
- The superior vena cava (SVC) carries oxygen-poor blood from the upper parts of your body, including your head, chest, arms, and neck.
- The inferior vena cava (IVC) carries oxygen-poor blood from the lower parts of your body.
The oxygen-poor blood from the vena cavae flows into your heart’s right atrium. From the right atrium, blood is pumped into the right ventricle. And then from the right ventricle, blood is pumped to your lungs through the pulmonary arteries (shown in blue in the center of figure 3).
Once in the lungs, the blood travels through many small, thin blood vessels called capillaries. There, the blood picks up more oxygen and transfers carbon dioxide to the lungs—a process called gas exchange.
The oxygen-rich blood passes from your lungs back to your heart through the pulmonary veins (shown in red to the left of the right atrium in figure 3).
The Left Side of Your Heart
Oxygen-rich blood from your lungs passes through the pulmonary veins (shown in red to the right of the left atrium in figure 3 above). The blood enters the left atrium and is pumped into the left ventricle.
From the left ventricle, the oxygen-rich blood is pumped to the rest of your body through the aorta. The aorta is the main artery that carries oxygen-rich blood to your body.
Like all of your organs, your heart needs oxygen-rich blood. As blood is pumped out of your heart’s left ventricle, some of it flows into the coronary arteries (shown in red in figure 3).
Your coronary arteries are located on your heart’s surface at the beginning of the aorta. They carry oxygen-rich blood to all parts of your heart.
For the heart to work well, your blood must flow in only one direction. Your heart’s valves make this possible. Both of your heart’s ventricles have an “in” (inlet) valve from the atria and an “out” (outlet) valve leading to your arteries.
Healthy valves open and close in exact coordination with the pumping action of your heart’s atria and ventricles. Each valve has a set of flaps called leaflets or cusps that seal or open the valve. This allows blood to pass through the chambers and into your arteries without backing up or flowing backward.
Heart’s Electrical System
To understand arrhythmias, it helps to understand the heart’s internal electrical system. The heart’s electrical system controls the rate and rhythm of the heartbeat.
With each heartbeat, an electrical signal spreads from the top of the heart to the bottom. As the signal travels, it causes the heart to contract and pump blood.
Your heart’s electrical system controls all the events that occur when your heart pumps blood 5. The electrical system also is called the cardiac conduction system. If you’ve ever seen the heart test called an EKG (electrocardiogram), you’ve seen a graphical picture of the heart’s electrical activity.
Your heart’s electrical system is made up of three main parts:
- Sinoatrial (SA) node, located in the right atrium of your heart
- Atrioventricular (AV) node, located on the interatrial septum close to the tricuspid valve
- His-Purkinje system, located along the walls of your heart’s ventricles
A heartbeat is a complex series of events. These events take place inside and around your heart. A heartbeat is a single cycle in which your heart’s chambers relax and contract to pump blood. This cycle includes the opening and closing of the inlet and outlet valves of the right and left ventricles of your heart.
Each heartbeat has two basic parts: diastole and systole. During diastole, the atria and ventricles of your heart relax and begin to fill with blood.
At the end of diastole, your heart’s atria contract (atrial systole) and pump blood into the ventricles. The atria then begin to relax. Your heart’s ventricles then contract (ventricular systole), pumping blood out of your heart.
Each electrical signal begins in a group of cells called the sinus node or sinoatrial (SA) node. The SA node is located in the heart’s upper right chamber, the right atrium. In a healthy adult heart at rest, the SA node fires off an electrical signal to begin a new heartbeat 60 to 100 times a minute. In a normal, healthy heart, each beat begins with a signal from the SA node. This is why the SA node sometimes is called your heart’s natural pacemaker. Your pulse, or heart rate, is the number of signals the SA node produces per minute.
The signal is generated as the vena cavae fill your heart’s right atrium with blood from other parts of your body. The signal spreads across the cells of your heart’s right and left atria.
From the SA node, the electrical signal travels through special pathways in the right and left atria. This causes the atria to contract and pump blood through the open valves from the atria into heart’s two lower chambers, the ventricles.
The electrical signal then moves down to a group of cells called the atrioventricular (AV) node, located between the atria and the ventricles. Here, the signal slows down just a little, allowing your heart’s right and left ventricles time to finish filling with blood.
The electrical signal then leaves the AV node and travels along a pathway called the bundle of His. This pathway divides into a right bundle branch and a left bundle branch. The signal goes down these branches to the ventricles, causing them to contract and pump blood to the lungs and the rest of the body.
From the bundle of His, the signal fibers divide into left and right bundle branches through the Purkinje fibers. These fibers connect directly to the cells in the walls of your heart’s left and right ventricles.
The signal spreads across the cells of your ventricle walls, and both ventricles contract. However, this doesn’t happen at exactly the same moment.
The left ventricle contracts an instant before the right ventricle. This pushes blood through the pulmonary valve (for the right ventricle) to your lungs, and through the aortic valve (for the left ventricle) to the rest of your body.
As the signal passes, the walls of the ventricles relax and await the next signal.
This process continues over and over as the atria refill with blood and more electrical signals come from the SA node.
A problem with any part of this process can cause an arrhythmia. For example, in atrial fibrillation, a common type of arrhythmia, electrical signals travel through the atria in a fast and disorganized way. This causes the atria to quiver instead of contract.
Heart arrhythmia symptoms
Arrhythmias may not cause any signs or symptoms 6. In fact, your doctor might find you have an arrhythmia before you do, during a routine examination. Noticeable signs and symptoms don’t necessarily mean you have a serious problem, however.
Noticeable arrhythmia symptoms may include:
- A fluttering in your chest
- A racing heartbeat (tachycardia)
- A slow heartbeat (bradycardia)
- Chest pain
- Shortness of breath
- Lightheadedness or dizziness
- Sweating
- Fainting (syncope) or near fainting
Arrhythmias may cause you to feel premature or extra heartbeats, or you may feel that your heart is racing or beating too slowly. Other signs and symptoms may be related to your heart not pumping effectively due to the fast or slow heartbeat. These include shortness of breath, weakness, dizziness, lightheadedness, fainting or near fainting, and chest pain or discomfort.
Seek urgent medical care if you suddenly or frequently experience any of these signs and symptoms at a time when you wouldn’t expect to feel them.
Ventricular fibrillation is one type of arrhythmia that can be deadly. It occurs when the heart beats with rapid, erratic electrical impulses. This causes pumping chambers in your heart (the ventricles) to quiver uselessly instead of pumping blood. Without an effective heartbeat, blood pressure plummets, cutting off blood supply to your vital organs.
A person with ventricular fibrillation will collapse within seconds and soon won’t be breathing or have a pulse. If this occurs, follow these steps:
- Call the emergency number in your area.
- If there’s no one nearby trained in cardiopulmonary resuscitation (CPR), provide hands-only CPR. That means uninterrupted chest compressions at a rate of 100 to 120 a minute until paramedics arrive. To do chest compressions, push hard and fast in the center of the chest. You don’t need to do rescue breathing.
- If you or someone nearby knows CPR, begin providing it if it’s needed. CPR can help maintain blood flow to the organs until an electrical shock (defibrillation) can be given.
Find out if an automated external defibrillator is available nearby. These portable defibrillators, which can deliver an electric shock that may restart heartbeats, are available in an increasing number of places, such as in airplanes, police cars and shopping malls. They can even be purchased for your home.
No training is required. The automated external defibrillator will tell you what to do. It’s programmed to allow a shock only when appropriate.
What causes heart arrhythmia
Normally, the heart’s most rapidly firing cells are in the sinus (or sinoatrial or SA) node, making that area a natural pacemaker 1. Under some conditions almost all heart tissue can start an impulse of the type that can generate a heartbeat 1. Cells in the heart’s conduction system can fire automatically and start electrical activity. This activity can interrupt the normal order of the heart’s pumping activity.
Secondary pacemakers elsewhere in the heart provide a “back-up” rhythm when the sinus node doesn’t work properly or when impulses are blocked somewhere in the conduction system 1.
An arrhythmia occurs when:
- The heart’s natural pacemaker develops an abnormal rate or rhythm.
- The normal conduction pathway is interrupted.
- Another part of the heart takes over as pacemaker.
Many things can lead to, or cause, an arrhythmia, including 6:
- A heart attack that’s occurring right now
- Scarring of heart tissue from a prior heart attack
- Changes to your heart’s structure, such as from cardiomyopathy
- Blocked arteries in your heart (coronary artery disease)
- High blood pressure
- Overactive thyroid gland (hyperthyroidism)
- Underactive thyroid gland (hypothyroidism)
- Smoking
- Drinking too much alcohol or caffeine
- Drug abuse
- Stress
- Certain medications and supplements, including over-the-counter cold and allergy drugs and nutritional supplements
- Diabetes
- Sleep apnea
- Genetics
Heart arrhythmia types
The four main types of arrhythmia are premature (extra) beats, supraventricular arrhythmias, ventricular arrhythmias, and bradyarrhythmias 7.
Premature (Extra) Beats
Premature beats are the most common type of arrhythmia. They’re harmless most of the time and often don’t cause any symptoms 7.
When symptoms do occur, they usually feel like fluttering in the chest or a feeling of a skipped heartbeat. If you’ve ever felt your heart “skip a beat,” it was probably from this early beat that disrupts the heart’s rhythm 8. In reality, the heart doesn’t skip a beat. Instead an extra beat comes sooner than normal. Then there’s usually a pause that causes the next beat to be more forceful. You felt this more-forceful beat.
Most of the time, premature beats need no treatment, especially in healthy people 7.
Types of premature contractions
- Premature beats that occur in the atria (the heart’s upper chambers) are called premature atrial contractions, or PACs.
- Premature beats that occur in the ventricles (the heart’s lower chambers) are called premature ventricular contractions, or PVCs.
Who is likely to have premature contractions
- Most people have them at some time 8.
- Premature beats are very common in normal children and teenagers 8.
Causes of premature contractions
- Usually no cause can be found.
- Occasionally premature beats may be caused by disease or injury to the heart. Your doctor may recommend more tests to make sure your heart is OK.
In most cases, premature beats happen naturally. However, some heart diseases can cause premature beats. They also can happen because of stress, too much exercise, or too much caffeine or nicotine 7.
Treatment of premature contractions
- Those without identifiable cause usually disappear on their own.
- If a cause is found, your healthcare professional will recommend a treatment plan.
Supraventricular Arrhythmias
Supraventricular arrhythmias are tachycardias (fast heart rates) that start in the atria or atrioventricular (AV) node. The AV node is a group of cells located between the atria and the ventricles.
Types of supraventricular arrhythmias include atrial fibrillation (AF), atrial flutter, paroxysmal supraventricular tachycardia (PSVT), and Wolff-Parkinson-White (WPW) syndrome.
Atrial Fibrillation
Atrial Fibrillation is the most common type of serious arrhythmia. It involves a very fast and irregular contraction of the atria 9.
In atrial fibrillation, the heart’s electrical signals don’t begin in the SA node. Instead, they begin in another part of the atria or in the nearby pulmonary veins 9.
The signals don’t travel normally. They may spread throughout the atria in a rapid, disorganized way. This causes the walls of the atria to quiver very fast (fibrillate) instead of beating normally. As a result, the atria aren’t able to pump blood into the ventricles the way they should.
In atrial fibrillation, electrical signals can travel through the atria at a rate of more than 300 per minute. However, the AV node can’t send the signals to the ventricles as fast as they arrive. So, even though the ventricles are beating faster than normal, they aren’t beating as fast as the atria.
Thus, the atria and ventricles no longer beat in a coordinated way. This creates a fast and irregular heart rhythm. In atrial fibrillation, the ventricles may beat 100 to 175 times a minute, in contrast to the normal rate of 60 to 100 beats a minute.
If this happens, blood isn’t pumped into the ventricles as well as it should be. Also, the amount of blood pumped out of the ventricles to the body is based on the random atrial beats.
Atrial Fibrillation may be brief, with symptoms that come and go and end on their own. Or, the condition may be ongoing and require treatment. Sometimes atrial fibrillation is permanent, and medicines or other treatments can’t restore a normal heart rhythm.
Atrial Fibrillation usually isn’t life threatening, but it can be dangerous if it causes the ventricles to beat very fast.
Atrial Fibrillation has two major complications:
- stroke and
- heart failure.
Stroke
During atrial fibrillation, the heart’s upper chambers, the atria, don’t pump all of their blood to the ventricles. Some blood pools in the atria. When this happens, a blood clot (also called a thrombus) can form.
If the clot breaks off and travels to the brain, it can cause a stroke. A clot that forms in one part of the body and travels in the bloodstream to another part of the body is called an embolus.
Blood-thinning medicines that reduce the risk of stroke are an important part of treatment for people who have atrial fibrillation. About 15–20 percent of people who have strokes have this heart arrhythmia. This clot risk is why patients with this condition are put on blood thinners 10.
Figure 5. Atrial Fibrillation and Stroke
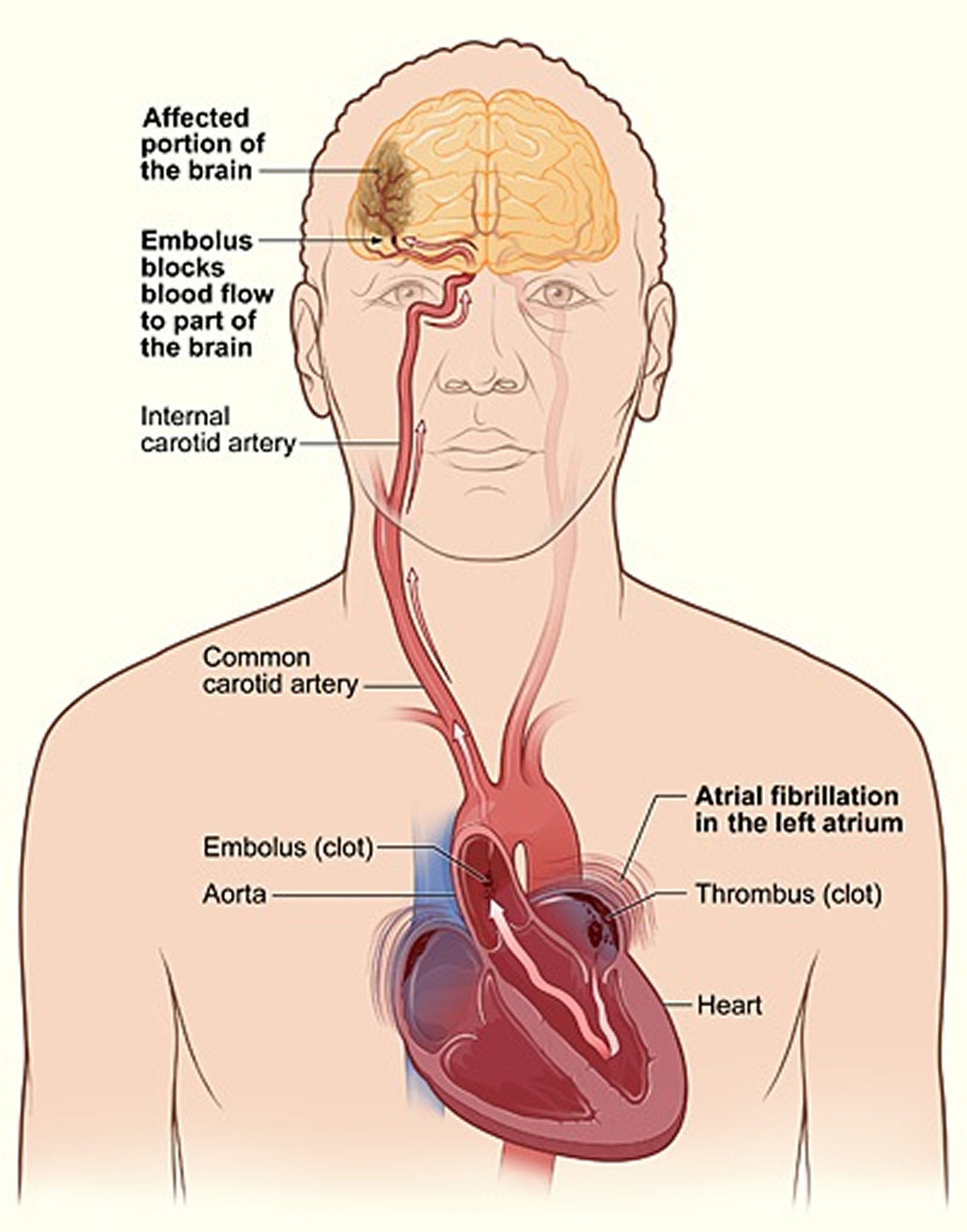
Note: The illustration shows how a stroke can occur during atrial fibrillation. A blood clot (thrombus) can form in the left atrium of the heart. If a piece of the clot breaks off and travels to an artery in the brain, it can block blood flow through the artery. The lack of blood flow to the portion of the brain fed by the artery causes a stroke.
Even though untreated atrial fibrillation doubles the risk of heart-related deaths and is associated with a 5-fold increased risk for stroke, many patients are unaware that atrial fibrillation is a serious condition 10.
Heart Failure
Heart failure occurs if the heart can’t pump enough blood to meet the body’s needs 11. Atrial fibrillation can lead to heart failure because the ventricles are beating very fast and can’t completely fill with blood. Thus, they may not be able to pump enough blood to the lungs and body.
Fatigue and shortness of breath are common symptoms of heart failure. A buildup of fluid in the lungs causes these symptoms. Fluid also can build up in the feet, ankles, and legs, causing weight gain.
Lifestyle changes, medicines, and procedures or surgery (rarely, a mechanical heart pump or heart transplant) are the main treatments for heart failure.
Damage to the heart’s electrical system causes atrial fibrillation. The damage most often is the result of other conditions that affect the health of the heart, such as high blood pressure, coronary heart disease, and rheumatic heart disease. Inflammation also is thought to play a role in the development of atrial fibrillation.
Other conditions also can lead to atrial fibrillation, including an overactive thyroid gland (too much thyroid hormone produced) and heavy alcohol use. The risk of atrial fibrillation increases with age.
Sometimes atrial fibrillation and other supraventricular arrhythmias can occur for no obvious reason.
Types of Atrial Fibrillation
- Paroxysmal Atrial Fibrillation
In paroxysmal atrial fibrillation, the faulty electrical signals and rapid heart rate begin suddenly and then stop on their own 12. Symptoms can be mild or severe. They stop within about a week, but usually in less than 24 hours. People who have this type of atrial fibrillation may have episodes only a few times a year or their symptoms may occur every day. These symptoms are very unpredictable and often can turn into a permanent form of atrial fibrillation 3.
- Persistent Atrial Fibrillation
Persistent atrial fibrillation is a condition in which the abnormal heart rhythm continues for more than a week 12. It may stop on its own, or it can be stopped with treatment.
- Permanent Atrial Fibrillation
Permanent atrial fibrillation is a condition in which a normal heart rhythm can’t be restored with treatment 12. Both paroxysmal and persistent atrial fibrillation may become more frequent and, over time, result in permanent atrial fibrillation.
Over a period of time, paroxysmal fibrillation may become more frequent and longer lasting, sometimes leading to permanent or chronic atrial fibrillation. All types of atrial fibrillation can increase your risk of stroke. Even if you have no symptoms at all, you are nearly 5 times more likely to have a stroke than someone who doesn’t have atrial fibrillation 3.
Causes Atrial Fibrillation
Atrial fibrillation occurs if the heart’s electrical signals don’t travel through the heart in a normal way. Instead, they become very rapid and disorganized.
Damage to the heart’s electrical system causes atrial fibrillation. The damage most often is the result of other conditions that affect the health of the heart, such as high blood pressure and coronary heart disease 13.
The risk of atrial fibrillation increases as you age. Inflammation also is thought to play a role in causing atrial fibrillation 13.
Sometimes, the cause of atrial fibrillation is unknown 13.
Who is at Risk for Atrial Fibrillation ?
Atrial fibrillation affects millions of people, and the number is rising. Men are more likely than women to have the condition 14. In the United States, atrial fibrillation is more common among Whites than African Americans or Hispanic Americans.
The risk of atrial fibrillation increases as you age. This is mostly because your risk for heart disease and other conditions that can cause AF also increases as you age. However, about half of the people who have atrial fibrillation are younger than 75.
Atrial fibrillation is uncommon in children.
Major Risk Factors
Atrial fibrillation is more common in people who have:
- High blood pressure
- Coronary heart disease (CHD)
- Heart failure
- Rheumatic heart disease
- Structural heart defects, such as mitral valve prolapse
- Pericarditis (a condition in which the membrane, or sac, around your heart is inflamed)
- Congenital heart defects
- Sick sinus syndrome (a condition in which the heart’s electrical signals don’t fire properly and the heart rate slows down; sometimes the heart will switch back and forth between a slow rate and a fast rate)
Atrial fibrillation also is more common in people who are having heart attacks or who have just had surgery.
Other Risk Factors
Other conditions that raise your risk for atrial fibrillation include hyperthyroidism (too much thyroid hormone), obesity, diabetes, and lung disease.
Certain factors also can raise your risk for atrial fibrillation. For example, drinking large amounts of alcohol, especially binge drinking, raises your risk. Even modest amounts of alcohol can trigger atrial fibrillation in some people. Caffeine or psychological stress also may trigger atrial fibrillation in some people.
Some data suggest that people who have sleep apnea are at greater risk for atrial fibrillation. Sleep apnea is a common disorder that causes one or more pauses in breathing or shallow breaths while you sleep.
Metabolic syndrome also raises your risk for atrial fibrillation. Metabolic syndrome is the name for a group of risk factors that raises your risk for coronary heart disease and other health problems, such as diabetes and stroke.
Research suggests that people who receive high-dose steroid therapy are at increased risk for atrial fibrillation. This therapy is used for asthma and some inflammatory conditions. It may act as a trigger in people who have other atrial fibrillation risk factors.
Genetic factors also may play a role in causing atrial fibrillation. However, their role isn’t fully known.
How can Atrial Fibrillation Be Prevented ?
Following a healthy lifestyle and taking steps to lower your risk for heart disease may help you prevent atrial fibrillation 15. These steps include:
- Following a heart healthy diet that’s low in saturated fat, trans fat, and cholesterol. A healthy diet includes a variety of whole grains, fruits, and vegetables daily.
- Not smoking.
- Being physically active.
- Maintaining a healthy weight.
If you already have heart disease or other atrial fibrillation risk factors, work with your doctor to manage your condition. In addition to adopting the healthy habits above, which can help control heart disease, your doctor may advise you to:
- Follow the DASH (Dietary Approaches to Stop Hypertension) eating plan to help lower your blood pressure.
- Keep your cholesterol and triglycerides at healthy levels with dietary changes and medicines (if prescribed).
- Limit or avoid alcohol.
- Control your blood sugar level if you have diabetes.
- Get ongoing medical care and take your medicines as prescribed.
For more information about following a healthy lifestyle, visit What is the DASH Diet ?, “Healthy Foods“, “Healthy Eating“, “Healthy Lifestyle” and “Healthy Exercise”
Symptoms and Signs of Atrial Fibrillation
Atrial fibrillation usually causes the heart’s lower chambers, the ventricles, to contract faster than normal.
When this happens, the ventricles can’t completely fill with blood. Thus, they may not be able to pump enough blood to the lungs and body.
Common symptoms of atrial fibrillation
Sometimes people with atrial fibrillation have no symptoms and their condition is only detectable upon physical examination. Still, others may experience one or more of the following symptoms 3:
- Palpitations (feelings that your heart is skipping a beat, fluttering, or beating too hard or fast)
- General fatigue
- Rapid and irregular heartbeat
- Fluttering or “thumping” in the chest
- Dizziness or fainting
- Shortness of breath and anxiety
- Weakness
- Faintness or confusion
- Fatigue when exercising
- Sweating
- *Chest pain or pressure
- *Chest pain or pressure is a medical emergency. You may be having a heart attack. Call your local emergency number immediately.
How is Atrial Fibrillation Diagnosed ?
Atrial fibrillation is diagnosed based on your medical and family histories, a physical exam, and the results from tests and procedures 16.
Sometimes atrial fibrillation doesn’t cause signs or symptoms. Thus, it may be found during a physical exam or EKG (electrocardiogram) test done for another purpose.
If you have atrial fibrillation, your doctor will want to find out what is causing it. This will help him or her plan the best way to treat the condition.
Specialists Involved
Primary care doctors often are involved in the diagnosis and treatment of atrial fibrillation. These doctors include family practitioners and internists.
Doctors who specialize in the diagnosis and treatment of heart disease also may be involved, such as:
- Cardiologists. These are doctors who diagnose and treat heart diseases and conditions.
- Electrophysiologists. These are cardiologists who specialize in arrhythmias.
Medical and Family Histories
Your doctor will likely ask questions about your:
- Signs and symptoms. What symptoms are you having? Have you had palpitations? Are you dizzy or short of breath? Are your feet or ankles swollen (a possible sign of heart failure)? Do you have any chest pain?
- Medical history. Do you have other health problems, such as a history of heart disease, high blood pressure, lung disease, diabetes, or thyroid problems?
- Family’s medical history. Does anyone in your family have a history of atrial fibrillation ? Has anyone in your family ever had heart disease or high blood pressure? Has anyone had thyroid problems? Does your family have a history of other illnesses or health problems?
- Health habits. Do you smoke or use alcohol or caffeine?
Physical Exam
Your doctor will do a complete cardiac exam. He or she will listen to the rate and rhythm of your heartbeat and take your pulse and blood pressure reading. Your doctor will likely check for any signs of heart muscle or heart valve problems. He or she will listen to your lungs to check for signs of heart failure.
Your doctor also will check for swelling in your legs or feet and look for an enlarged thyroid gland or other signs of hyperthyroidism (too much thyroid hormone).
Diagnostic Tests and Procedures
- EKG
An EKG is a simple, painless test that records the heart’s electrical activity. It’s the most useful test for diagnosing atrial fibrillation.
An EKG shows how fast your heart is beating and its rhythm (steady or irregular). It also records the strength and timing of electrical signals as they pass through your heart.
A standard EKG only records the heartbeat for a few seconds. It won’t detect AF that doesn’t happen during the test. To diagnose paroxysmal AF, your doctor may ask you to wear a portable EKG monitor that can record your heartbeat for longer periods.
The two most common types of portable EKGs are Holter and event monitors.
- Holter and Event Monitors
A Holter monitor records the heart’s electrical activity for a full 24- or 48-hour period. You wear small patches called electrodes on your chest. Wires connect these patches to a small, portable recorder. The recorder can be clipped to a belt, kept in a pocket, or hung around your neck.
You wear the Holter monitor while you do your normal daily activities. This allows the monitor to record your heart for a longer time than a standard EKG.
An event monitor is similar to a Holter monitor. You wear an event monitor while doing your normal activities. However, an event monitor only records your heart’s electrical activity at certain times while you’re wearing it.
For many event monitors, you push a button to start the monitor when you feel symptoms. Other event monitors start automatically when they sense abnormal heart rhythms.
You can wear an event monitor for weeks or until symptoms occur.
- Stress Test
Some heart problems are easier to diagnose when your heart is working hard and beating fast. During stress testing, you exercise to make your heart work hard and beat fast while heart tests are done. If you can’t exercise, you may be given medicine to make your heart work hard and beat fast.
- Echocardiography
Echocardiography (echo) uses sound waves to create a moving picture of your heart. The test shows the size and shape of your heart and how well your heart chambers and valves are working.
Echo also can identify areas of poor blood flow to the heart, areas of heart muscle that aren’t contracting normally, and previous injury to the heart muscle caused by poor blood flow.
This test sometimes is called transthoracic echocardiography. It’s painless and noninvasive (no instruments are inserted into the body). For the test, a device called a transducer is moved back and forth over your chest. The device sends special sound waves through your chest wall to your heart.
The sound waves bounce off the structures of your heart, and a computer converts them into pictures on a screen.
- Transesophageal Echocardiography
Transesophageal echo uses sound waves to take pictures of your heart through the esophagus. The esophagus is the passage leading from your mouth to your stomach.
Your heart’s upper chambers, the atria, are deep in your chest. They often can’t be seen very well using transthoracic echo. Your doctor can see the atria much better using transesophageal echo.
During this test, the transducer is attached to the end of a flexible tube. The tube is guided down your throat and into your esophagus. You’ll likely be given medicine to help you relax during the procedure.
Transesophageal echo is used to detect blood clots that may be forming in the atria because of atrial fibrillation.
- Chest X Ray
A chest x ray is a painless test that creates pictures of the structures in your chest, such as your heart and lungs. This test can show fluid buildup in the lungs and signs of other atrial fibrillation complications.
- Blood Tests
Blood tests check the level of thyroid hormone in your body and the balance of your body’s electrolytes. Electrolytes are minerals that help maintain fluid levels and acid-base balance in the body. They’re essential for normal health and functioning of your body’s cells and organs.
How is Atrial Fibrillation Treated ?
Treatment for atrial fibrillation depends on how often you have symptoms, how severe they are, and whether you already have heart disease. General treatment options include medicines, medical procedures, and lifestyle changes 17.
Goals of Treatment
The goals of treating atrial fibrillation include:
- Preventing blood clots from forming, thus lowering the risk of stroke.
- Controlling how many times a minute the ventricles contract. This is called rate control. Rate control is important because it allows the ventricles enough time to completely fill with blood. With this approach, the abnormal heart rhythm continues, but you feel better and have fewer symptoms.
- Restoring a normal heart rhythm. This is called rhythm control. Rhythm control allows the atria and ventricles to work together to efficiently pump blood to the body.
- Treating any underlying disorder that’s causing or raising the risk of atrial fibrillation—for example, hyperthyroidism (too much thyroid hormone).
Who Needs Treatment for Atrial Fibrillation ?
People who have atrial fibrillation but don’t have symptoms or related heart problems may not need treatment. Atrial fibrillation may even go back to a normal heart rhythm on its own. This also can occur in people who have atrial fibrillation with symptoms.
In some people who have atrial fibrillation for the first time, doctors may choose to use an electrical procedure or medicine to restore a normal heart rhythm.
Repeat episodes of atrial fibrillation tend to cause changes to the heart’s electrical system, leading to persistent or permanent atrial fibrillation. Most people who have persistent or permanent atrial fibrillation need treatment to control their heart rate and prevent complications.
Specific Types of Treatment
- Blood Clot Prevention
People who have atrial fibrillation are at increased risk for stroke. This is because blood can pool in the heart’s upper chambers (the atria), causing a blood clot to form. If the clot breaks off and travels to the brain, it can cause a stroke.
Preventing blood clots from forming is probably the most important part of treating atrial fibrillation. The benefits of this type of treatment have been proven in multiple studies.
Doctors prescribe blood-thinning medicines to prevent blood clots. These medicines include warfarin (Coumadin®), dabigatran, heparin, and aspirin.
People taking blood-thinning medicines need regular blood tests to check how well the medicines are working.
- Rate Control
Doctors can prescribe medicines to slow down the rate at which the ventricles are beating. These medicines help bring the heart rate to a normal level.
Rate control is the recommended treatment for most patients who have atrial fibrillation, even though an abnormal heart rhythm continues and the heart doesn’t work as well as it should. Most people feel better and can function well if their heart rates are well-controlled.
Medicines used to control the heart rate include beta blockers (for example, metoprolol and atenolol), calcium channel blockers (diltiazem and verapamil), and digitalis (digoxin). Several other medicines also are available.
- Rhythm Control
Restoring and maintaining a normal heart rhythm is a treatment approach recommended for people who aren’t doing well with rate control treatment. This treatment also may be used for people who have only recently started having atrial fibrillation. The long-term benefits of rhythm control have not been proven conclusively yet.
Doctors use medicines or procedures to control the heart’s rhythm. Patients often begin rhythm control treatment in a hospital so that their hearts can be closely watched.
The longer you have atrial fibrillation, the less likely it is that doctors can restore a normal heart rhythm. This is especially true for people who have had atrial fibrillation for 6 months or more.
Restoring a normal rhythm also becomes less likely if the atria are enlarged or if any underlying heart disease worsens. In these cases, the chance that atrial fibrillation will recur is high, even if you’re taking medicine to help convert atrial fibrillation to a normal rhythm.
Medicines
Medicines used to control the heart rhythm include amiodarone, sotalol, flecainide, propafenone, dofetilide, and ibutilide. Sometimes older medicines—such as quinidine, procainamide, and disopyramide—are used.
Your doctor will carefully tailor the dose and type of medicines he or she prescribes to treat your atrial fibrillation. This is because medicines used to treat atrial fibrillation can cause a different kind of arrhythmia.
These medicines also can harm people who have underlying diseases of the heart or other organs. This is especially true for patients who have an unusual heart rhythm problem called Wolff-Parkinson-White syndrome.
Your doctor may start you on a small dose of medicine and then gradually increase the dose until your symptoms are controlled. Medicines used for rhythm control can be given regularly by injection at a doctor’s office, clinic, or hospital. Or, you may routinely take pills to try to control AF or prevent repeat episodes.
If your doctor knows how you’ll react to a medicine, a specific dose may be prescribed for you to take on an as-needed basis if you have an episode of atrial fibrillation.
Procedures
Doctors use several procedures to restore a normal heart rhythm. For example, they may use electrical cardioversion to treat a fast or irregular heartbeat. For this procedure, low-energy shocks are given to your heart to trigger a normal rhythm. You’re temporarily put to sleep before you receive the shocks.
Electrical cardioversion isn’t the same as the emergency heart shocking procedure often seen on TV programs. It’s planned in advance and done under carefully controlled conditions.
Before doing electrical cardioversion, your doctor may recommend transesophageal echocardiography. This test can rule out the presence of blood clots in the atria. If clots are present, you may need to take blood-thinning medicines before the procedure. These medicines can help get rid of the clots.
Catheter ablation may be used to restore a normal heart rhythm if medicines or electrical cardioversion don’t work. For this procedure, a wire is inserted through a vein in the leg or arm and threaded to the heart.
Radio wave energy is sent through the wire to destroy abnormal tissue that may be disrupting the normal flow of electrical signals. An electrophysiologist usually does this procedure in a hospital. Your doctor may recommend a transesophageal echocardiography before catheter ablation to check for blood clots in the atria.
Sometimes doctors use catheter ablation to destroy the atrioventricular (AV) node. The AV node is where the heart’s electrical signals pass from the atria to the ventricles (the heart’s lower chambers). This procedure requires your doctor to surgically implant a device called a pacemaker, which helps maintain a normal heart rhythm.
Research on the benefits of catheter ablation as a treatment for atrial fibrillation is still ongoing.
Another procedure to restore a normal heart rhythm is called maze surgery. For this procedure, the surgeon makes small cuts or burns in the atria. These cuts or burns prevent the spread of disorganized electrical signals.
This procedure requires open-heart surgery, so it’s usually done when a person requires heart surgery for other reasons, such as for heart valve disease, which can increase the risk of atrial fibrillation.
Approaches To Treating Underlying Causes and Reducing Risk Factors
Your doctor may recommend treatments for an underlying cause of atrial fibrillation or to reduce atrial fibrillation risk factors. For example, he or she may prescribe medicines to treat an overactive thyroid, lower high blood pressure, or manage high blood cholesterol.
Your doctor also may recommend lifestyle changes, such as following a healthy diet, cutting back on salt intake (to help lower blood pressure), quitting smoking, and reducing stress.
Limiting or avoiding alcohol, caffeine, or other stimulants that may increase your heart rate also can help reduce your risk for atrial fibrillation.
Outlook for atrial fibrillation
People who have atrial fibrillation can live normal, active lives. For some people, treatment can restore normal heart rhythms.
For people who have permanent atrial fibrillation, treatment can help control symptoms and prevent complications. Treatment may include medicines, medical procedures, and lifestyle changes.
Living With Atrial Fibrillation
People who have atrial fibrillation—even permanent atrial fibrillation—can live normal, active lives 18. If you have atrial fibrillation, ongoing medical care is important.
Keep all your medical appointments. Bring a list of all the medicines you’re taking to every doctor and emergency room visit. This will help your doctor know exactly what medicines you’re taking.
Follow your doctor’s instructions for taking medicines. Be careful about taking over-the-counter medicines, nutritional supplements, and cold and allergy medicines. Some of these products contain stimulants that can trigger rapid heart rhythms. Also, some over-the-counter medicines can have harmful interactions with heart rhythm medicines.
Tell your doctor if your medicines are causing side effects, if your symptoms are getting worse, or if you have new symptoms.
If you’re taking blood-thinning medicines, you’ll need to be carefully monitored. For example, you may need routine blood tests to check how the medicines are working. Also, talk with your doctor about your diet. Some foods, such as leafy green vegetables, may interfere with warfarin, a blood-thinning medicine.
Ask your doctor about physical activity, weight control, and alcohol use. Find out what steps you can take to manage your condition.
Atrial Flutter
Atrial flutter is similar to atrial fibrillation. However, the heart’s electrical signals spread through the atria in a fast and regular—instead of irregular—rhythm 7. Atrial flutter is much less common than atrial fibrillation, but it has similar symptoms and complications.
Paroxysmal Supraventricular Tachycardia
Paroxysmal Supraventricular Tachycardia is a very fast heart rate that begins and ends suddenly 7. Paroxysmal Supraventricular Tachycardia occurs because of problems with the electrical connection between the atria and the ventricles.
In Paroxysmal Supraventricular Tachycardia, electrical signals that begin in the atria and travel to the ventricles can reenter the atria, causing extra heartbeats. This type of arrhythmia usually isn’t dangerous and tends to occur in young people 7. It can happen during vigorous physical activity 7.
A special type of Paroxysmal Supraventricular Tachycardia is called Wolff-Parkinson-White syndrome. Wolff-Parkinson-White syndrome is a condition in which the heart’s electrical signals travel along an extra pathway from the atria to the ventricles.
This extra pathway disrupts the timing of the heart’s electrical signals and can cause the ventricles to beat very fast. This type of arrhythmia can be life threatening 7.
Ventricular Arrhythmias
These arrhythmias start in the heart’s lower chambers, the ventricles. They can be very dangerous and usually require medical care right away 7.
Ventricular arrhythmias include ventricular tachycardia and ventricular fibrillation. Coronary heart disease, heart attack, a weakened heart muscle, and other problems can cause ventricular arrhythmias 7.
- Ventricular Tachycardia
Ventricular tachycardia is a fast, regular beating of the ventricles that may last for only a few seconds or for much longer.
A few beats of ventricular tachycardia often don’t cause problems. However, episodes that last for more than a few seconds can be dangerous. Ventricular tachycardia can turn into other, more serious arrhythmias, such as ventricular fibrillation.
- Ventricular Fibrillation
Ventricular fibrillation occurs if disorganized electrical signals make the ventricles quiver instead of pump normally. Without the ventricles pumping blood to the body, sudden cardiac arrest and death can occur within a few minutes.
To prevent death, the condition must be treated right away with an electric shock to the heart called defibrillation.
Ventricular fibrillation may occur during or after a heart attack or in someone whose heart is already weak because of another condition.
Torsades de pointes (torsades) is a type of ventricular fibrillation that causes a unique pattern on an EKG (electrocardiogram) test. Certain medicines or imbalanced amounts of potassium, calcium, or magnesium in the bloodstream can cause this condition.
People who have long QT syndrome are at increased risk for torsades. People who have this condition need to be careful about taking certain antibiotics, heart medicines, and over-the-counter products.
Bradyarrhythmias
Bradyarrhythmias occur if the heart rate is slower than normal. If the heart rate is too slow, not enough blood reaches the brain. This can cause you to pass out.
In adults, a heart rate slower than 60 beats per minute is considered a bradyarrhythmia. Some people normally have slow heart rates, especially people who are very physically fit. For them, a heartbeat slower than 60 beats per minute isn’t dangerous and doesn’t cause symptoms. But in other people, serious diseases or other conditions may cause bradyarrhythmias.
Bradyarrhythmias can be caused by:
- Heart attacks
- Conditions that harm or change the heart’s electrical activity, such as an underactive thyroid gland or aging
- An imbalance of chemicals or other substances in the blood, such as potassium
- Medicines such as beta blockers, calcium channel blockers, some antiarrhythmia medicines, and digoxin
Arrhythmias in Children
Children’s heart rates normally decrease as they get older. A newborn’s heart beats between 95 to 160 times a minute 7. A 1-year-old’s heart beats between 90 to 150 times a minute, and a 6- to 8-year-old’s heart beats between 60 to 110 times a minute 7.
A baby or child’s heart can beat fast or slow for many reasons. Like adults, when children are active, their hearts will beat faster. When they’re sleeping, their hearts will beat slower. Their heart rates can speed up and slow down as they breathe in and out. All of these changes are normal.
Some children are born with heart defects that cause arrhythmias. In other children, arrhythmias can develop later in childhood. Doctors use the same tests to diagnose arrhythmias in children and adults.
Treatments for children who have arrhythmias include medicines, defibrillation (electric shock), surgically implanted devices that control the heartbeat, and other procedures that fix abnormal electrical signals in the heart.
Long Q-T Syndrome
Long Q-T Syndrome is a disorder of the heart’s electrical system, like other arrhythmias. Since the hearts electrical activity is controlled by the flow of ions (that is electrically charged particles such as calcium, sodium, potassium and chloride), these ions move in and out of the cells of the heart. This flow is controlled by very small ion channels. When the heart contracts, it emits an electrical signal. This signal can be recorded on an electrocardiogram (EKG) and produces a characteristic waveform. The different parts of this waveform are designated by letters — P, Q, R, S and T. The Q-T interval represents the time for electrical activation and inactivation of the ventricles, the lower chambers of the heart. A doctor can measure the time it takes for the Q-T interval to occur (in fractions of a second) and can tell if it occurs in a normal amount of time. If it takes longer than normal, it’s called a prolonged Q-T interval 19.
What are the symptoms of Long Q-T Syndrome ?
People with Long Q-T Syndrome may not have any symptoms. People who do have symptoms often exhibit fainting (syncope) and abnormal rate and/or rhythm of the heartbeat (arrhythmia), a fluttering feeling in the chest. People with this syndrome may show prolongation of the Q-T interval during physical exercise, intense emotion (such as fright, anger or pain) or when startled by a noise. Some arrhythmias are potentially fatal, causing sudden death. In one type of inherited Long Q-T Syndrome, the person may also be deaf 19.
People with Long Q-T Syndrome don’t necessarily have a prolonged Q-T interval all the time. At the time that they have an electrocardiogram (such as during a routine physical examination), the Q-T interval may actually be normal. Alternatively, some healthy young people may not have a routine ECG, and Long Q-T Syndrome may be suspected because of their family history or because of unexplained fainting episodes. In any family where repeated episodes of fainting or a history of sudden death exists, an investigation of the cause, including Long Q-T Syndrome, should be undertaken.
How is Long Q-T Syndrome treated ?
There are treatments for Long Q-T Syndrome, including medications such as beta blockers. Sometimes a surgical procedure is performed, and some people may benefit from an implantable defibrillator. Avoid drugs and electrolyte imbalance known to prolong the Q-T interval.
Premature Atrial Contraction and Premature Ventricular Contraction
Premature beats or extra beats most often cause irregular heart rhythms. Those that start in the upper chambers (atria) are called premature atrial contractions or premature atrial contractions 19. Premature ventricular contractions start in the ventricles 19. If you’ve ever had the feeling that your heart “skipped a beat,” it was probably from this type of arrhythmia. The heart really doesn’t skip a beat. Instead, an extra beat comes sooner than normal. Then there’s usually a pause that causes the next beat to be more forceful. You felt this more-forceful beat.
Premature beats are very common in normal children and teenagers — most people have them at some time. Usually no cause can be found and no special treatment is needed 19. The premature beats may disappear later. Even if they continue, your child will stay well and won’t need any restrictions. Occasionally premature beats may be caused by disease or injury to the heart. Your child’s doctor may recommend more tests to make sure your child’s heart is okay.
Tachycardia
A fast heart rate is called tachycardia. The definition of “too fast” usually depends on the person’s age and physical activity. A newborn has tachycardia if the resting rate is more than 160 beats per minute 19. A teenager is considered to have tachycardia if the resting heart rate is more than 90 beats per minute. A teenager may have a normal heart rate of up to 200 beats per minute during exercise 19.
Sinus tachycardia
Sinus tachycardia is a normal increase in the heart rate. It occurs with fever, excitement and exercise. No treatment is needed. Rarely, disease, such as anemia (low blood counts) or increased thyroid activity can cause this fast heart rate. In these cases, when the disease is treated, the tachycardia goes away.
Supraventricular Tachycardia
The most common abnormal tachycardia in children is supraventricular tachycardia. It’s also called paroxysmal atrial tachycardia or paroxysmal supraventricular tachycardia. The fast heart rate involves both the heart’s upper and lower chambers. This isn’t a life-threatening problem for most children and adolescents. Treatment is only considered if episodes are prolonged or frequent. For many infants, supraventricular tachycardia is a time-limited problem. Symptoms often stop, with treatment, after six to 12 months 19.
Supraventricular tachycardia may occur in very young infants with otherwise-normal hearts. The heart rate is usually more than 220 beats a minute. Infants with an supraventricular tachycardia episode may breathe faster than normal and seem fussy or sleepier than usual. This situation must be diagnosed and treated to return the heart rate to normal. Once the rhythm is normal, medication usually can prevent future episodes.
Sometimes supraventricular tachycardia can be detected while a baby is still in the womb. Then the mother may take medications to slow her baby’s heart rate. If an older infant or child has supraventricular tachycardia, the child may be aware of the rapid heart rate. This may be associated with palpitations, dizziness, lightheadedness, chest discomfort, upset stomach or weakness. Some children can learn ways to slow down their heart rate. Straining — such as closing the nose and mouth and trying to breathe out — may be successful. This is called a Valsalva maneuver.
Older children are more likely to have more episodes of tachycardia. They’re more likely to need prolonged treatment. They also may need more diagnostic tests. It’s unusual for episodes of supraventricular tachycardia to keep a child from enjoying normal activities. Most children who have episodes of tachycardia stay well even though they may need to keep taking medicine. Your child will probably need periodic check-ups but will be able to enjoy unrestricted normal activities.
Treating supraventricular tachycardia usually has two parts. The first is stopping a current episode; the second is preventing recurrences. The approach to preventing recurrences depends on the child’s age. In some cases — especially those of infants — the child may need to enter the hospital for treatment and special studies.
Sometimes simple procedures can stop a fast heart rhythm. Your child’s doctor can explain this to you in more detail. At other times intravenous medications may be needed to control or stop the tachycardia. Another way to stop supraventricular tachycardia is to place a small catheter (a thin, flexible tube) through the nostril into the esophagus. A small amount of electricity is sent through this catheter to stop the supraventricular tachycardia. On rare occasions doctors stop supraventricular tachycardia by giving a small electrical shock to the chest wall. This is called electrical countershock or cardioversion. A sedative or anesthetic is given before this procedure.
Wolff-Parkinson-White Syndrome
Often medication can improve this condition. Sometimes, though, such treatment doesn’t work. Then your child will need more tests. Eliminating the abnormal pathway by passing energy through a catheter may be needed. Surgery is another option 19.
Ventricular tachycardia
Ventricular tachycardia is a fast heart rate that starts in the lower chambers (ventricles) 19. This uncommon but potentially serious condition can threaten a child’s life. Ventricular tachycardia may result from serious heart disease; it usually requires prompt treatment. Ventricular tachycardia occasionally occurs in children with otherwise normal hearts. Often specialized tests, including an intracardiac electrophysiologic procedure, may be needed to evaluate the tachycardia and the effect of drug treatment. Some forms of ventricular tachycardia may not need treatment 19.
If treatment is required, it includes medicines and addressing the cause, if possible. The type and length of treatment depends on what’s causing the problem. In some people radiofrequency ablation or surgery may be needed to control the tachycardia.
Bradycardia
A heart rate that’s too slow is called bradycardia. What’s “too slow” depends on a person’s age and activity. A newborn usually won’t have a heart rate of less than 80 beats a minute 19. An athletically trained teenager may have a normal resting heart rate of 50 beats a minute 19.
Sick Sinus Syndrome
Sometimes the sinus node doesn’t work properly. Some children who’ve had open-heart surgery have this problem. When the sinus node’s work is seriously disturbed, it’s called sick sinus syndrome 19. A child with this syndrome may not have any symptoms or may be tired, dizzy or faint. Children with sick sinus syndrome have episodes of tachycardia and bradycardia. Fortunately, sick sinus syndrome is unusual in children. If it does occur, an artificial pacemaker, medications or both may be needed.
Complete Heart Block
Heart block means that the heart’s electrical signal can’t pass normally from the upper to the lower chambers 19. The electrical signal within the heart is blocked, not the blood flow. When this occurs, another “natural” pacemaker in the lower chambers takes over, but at a slower rate.
Heart block may be present at — or even before — birth. This is congenital heart block 19. Disease or an injury to the electrical conduction system during heart surgery can also cause it 19. When the natural pacemaker in the lower chambers isn’t fast enough or reliable enough, an artificial pacemaker is put in.
- American Heart Association. About Arrhythmia. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/About-Arrhythmia_UCM_002010_Article.jsp[↩][↩][↩][↩][↩][↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Arrhythmia. https://www.nhlbi.nih.gov/health/health-topics/topics/arr[↩]
- American Heart Association. What are the Symptoms of Atrial Fibrillation (AFib or AF) ? http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/What-are-the-Symptoms-of-Atrial-Fibrillation-AFib-or-AF_UCM_423777_Article.jsp[↩][↩][↩][↩]
- Centers for Disease Control and Prevention. Division of Birth Defects and Developmental Disabilities. Congenital Heart Defects (CHDs). https://www.cdc.gov/ncbddd/heartdefects/index.html[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Your Heart’s Electrical System. https://www.nhlbi.nih.gov/health/health-topics/topics/hhw/electrical[↩]
- Mayo Foundation for Medical Education and Research. Heart arrhythmia symptoms and causes. http://www.mayoclinic.org/diseases-conditions/heart-arrhythmia/symptoms-causes/dxc-20188128[↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Types of Arrhythmia. https://www.nhlbi.nih.gov/health/health-topics/topics/arr/types[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- American Heart Association. Premature Contractions – PACs and PVCs. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/Premature-Contractions—PACs-and-PVCs_UCM_302043_Article.jsp[↩][↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Atrial Fibrillation. https://www.nhlbi.nih.gov/health/health-topics/topics/af[↩][↩]
- American Heart Association. What is Atrial Fibrillation (AFib or AF) ? http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/What-is-Atrial-Fibrillation-AFib-or-AF_UCM_423748_Article.jsp[↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. What Are the Signs and Symptoms of Atrial Fibrillation ? https://www.nhlbi.nih.gov/health/health-topics/topics/af/signs[↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Types of Atrial Fibrillation. https://www.nhlbi.nih.gov/health/health-topics/topics/af/types[↩][↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. What Causes Atrial Fibrillation ? https://www.nhlbi.nih.gov/health/health-topics/topics/af/causes[↩][↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Who Is at Risk for Atrial Fibrillation ? https://www.nhlbi.nih.gov/health/health-topics/topics/af/atrisk[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. How Can Atrial Fibrillation Be Prevented ? https://www.nhlbi.nih.gov/health/health-topics/topics/af/prevention[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is Atrial Fibrillation Diagnosed ? https://www.nhlbi.nih.gov/health/health-topics/topics/af/diagnosis[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is Atrial Fibrillation Treated ? https://www.nhlbi.nih.gov/health/health-topics/topics/af/treatment[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Living With Atrial Fibrillation. https://www.nhlbi.nih.gov/health/health-topics/topics/af/livingwith[↩]
- American Heart Association. Types of Arrhythmia in Children. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/Types-of-Arrhythmia-in-Children_UCM_302023_Article.jsp[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]





{kind=link}