
Contents
What is a heart transplant ?
Heart transplant is surgery that removes a diseased heart and replaces it with a healthy heart from a deceased donor to improve your quality of life and increase your lifespan 1). Most heart transplants are done on patients who have end-stage heart failure, a condition in which your heart is severely damaged or weakened, and on people who have failed other treatment options. End-stage heart failure may be caused by conditions such as coronary heart disease, viral infections, or hereditary conditions 2). In rare instances, heart transplant may be performed at the same time as lung transplant in patients who have severe heart and lung disease.
The first human heart transplantation was performed on 3 December 1967 by a South African doctor, Dr Christiaan Barnard at Groote Schuur Hospital, Cape Town, South Africa. The annual number of transplants only began to grow substantially from the 1980s, declining again after 1996 due to the shortage of donor hearts. Heart transplants are now the the third most common organ transplant operation in the U.S. 3). Meanwhile, more than 73,000 heart transplants have been performed worldwide 4).
Heart transplant recipient survival rates vary based on a number of factors. A 2014 report by the Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients stated that the overall survival rate in the U.S. is about 88 percent after one year and about 75 percent after five years 5).
Most people who receive a heart transplant enjoy a high quality of life. Depending on your condition, you may be able to return to many of your daily life activities, such as returning to work, participating in hobbies and sports, and exercise. Discuss with your doctor what activities are appropriate for you.
Some women who have had a heart transplant can become pregnant. However, discuss with your doctor if you’re considering having children after your transplant 6). You’ll likely need medication adjustments before becoming pregnant, as some medications can cause pregnancy complications 7).
You may be eligible for heart transplant surgery if you have severe heart disease leading to heart failure that does not respond to other treatments.
In adults, heart failure can be caused by several conditions, including:
- A weakening of the heart muscle (cardiomyopathy)
- Coronary artery disease
- Heart valve disease
- A heart problem you’re born with (congenital heart defect)
- Dangerous recurring abnormal heart rhythms (ventricular arrhythmias) not controlled by other treatments
- Amyloidosis
- Failure of a previous heart transplant
In children, heart failure is most often caused by either a congenital heart defect or a cardiomyopathy.
Another organ transplant may be performed at the same time as a heart transplant (multiorgan transplant) in people with certain conditions at select medical centers. Multiorgan transplants include:
- Heart-kidney transplant. This procedure may be an option for some people with kidney failure in addition to heart failure.
- Heart-liver transplant. This procedure may be an option for people with certain liver and heart conditions.
- Heart-lung transplant. Rarely, doctors may suggest this procedure for some people with severe lung and heart diseases, if the conditions aren’t able to be treated by only a heart transplant or lung transplant.
If you are otherwise healthy enough for surgery, you will be placed on the National Organ Procurement and Transplantation Network’s (OPTN) waiting list 8). This national network handles the organ-sharing process for the United States 9). If a match is found, you will need to have your heart transplant surgery right away.
Heart transplant surgery will be done in a hospital. You will have general anesthesia and will not be awake during the surgery. You will receive medicine through an intravenous (IV) line in your arm. A breathing tube connected to a ventilator will help you breathe. A surgeon will open your chest, connect your heart’s arteries and veins to a heart-lung bypass machine, and remove your diseased heart. The body’s arteries and veins will be taken off the bypass machine and reconnected to the healthy donor heart. The heart transplant is complete after the surgeon closes your chest.
After the surgery, you will recover in the hospital’s intensive care unit (ICU) and stay in the hospital for up to three weeks. During your recovery, you may start a cardiac rehabilitation program. Before leaving the hospital, you will learn how to keep track of your overall health; monitor your weight, blood pressure, pulse, and temperature; and learn the signs of heart transplant rejection and infection. For the first three months after leaving the hospital, you will return often for tests to check for infection or rejection of your new heart, to test your heart function, and to make sure that you are recovering well.
Practicing good hygiene, obtaining routine vaccines, and making healthy lifestyle choices are very important after a heart transplant to reduce your risk of infection. Regular dental care is also important. Your doctor or dentist may prescribe antibiotics before any dental work to prevent infection. Following your doctor’s advice will help you recover and stay as healthy as possible.
Heart transplant has some serious risks.
Complications of surgery
Heart transplant surgery requires open heart surgery, which carries the risk of many complications 10), including:
- Bleeding
- Infection
- Blood clots
- Heart attack
- Stroke
- Death
Risks of having a heart transplant
Although receiving a donor heart can save your life, having a heart transplant has many risks. Risks include:
- Primary graft dysfunction happens when the donor heart fails and cannot function 11). This is the most frequent cause of death for the first month after transplant.
- Rejection of the donor heart. One of the most significant risks after a heart transplant is your body rejecting the donor heart. Your immune system also may reject your new heart. Rejection is most likely to occur within six months after the transplant 12).
Your immune system will see your donor heart as a foreign object that’s not supposed to be in your body. Your immune system will try to attack your donor heart. Although all people who receive a heart transplant receive immunosuppressants — medications that reduce the activity of the immune system — about 10 percent of heart transplant recipients still have some signs of rejection that need treatment during the first year after transplantation. This is often effectively treated with medication. You will need to take these medicines for the rest of your life to suppress your immune system and help prevent your body from rejecting your new heart 13).
Usually the rejection is without any symptoms and requires only an adjustment of medications. If you miss doses of medications, however, the rejection can be severe and very serious. It’s important that you follow the instructions as explained by your doctors.
To determine whether your body is rejecting the new heart, you’ll have frequent heart biopsies to test your heart tissue during the first year after your transplant. After the first year, the number of biopsies is significantly reduced.
- Problems with your coronary arteries. After your transplant, it’s possible the walls of the arteries in your heart (coronary arteries) could thicken and harden, leading to cardiac allograft vasculopathy (CAV). Cardiac allograft vasculopathy is a common and serious complication of heart transplant. Cardiac allograft vasculopathy is an aggressive form of atherosclerosis that over months or a few years can quickly block the heart’s arteries and cause the donor heart to fail 14). Over time, your new heart may fail due to the same reasons that caused your original heart to fail. Some patients who have a heart transplant that fails may be eligible for another transplant.
Your doctor may recommend annual tests after your transplant to monitor your coronary arteries for cardiac allograft vasculopathy.
- Medication side effects. The immunosuppressants you’ll need to take for the rest of your life may cause kidney damage and other problems. Other complications of these medications can include high blood pressure, high cholesterol, diabetes and osteoporosis a condition in which your bones become thin and weak.
- Cancer. Immunosuppressants can also increase your cancer risk. Taking these medications can put you at a greater risk of skin cancer, non-Hodgkin’s lymphoma and other solid tumors. Regular checkups are necessary to detect the development of cancer.
- Infection. Immunosuppressants decrease your ability to fight infection. Some heart transplant recipients may develop an infection that requires them to be admitted to the hospital during the first year after their transplant. The risk of infection decreases over time as the amount of immunosuppressant medication is decreased.
Despite these risks, heart transplant has a good success rate that has improved over many decades of research. Recent survival rates are about 85 percent at one year after surgery, with survival rates decreasing by about three to four percent each additional year after surgery because of serious complications 15). Mechanical circulatory support, possibly from left ventricular assist devices, may be an alternative to heart transplant. But more research is needed to determine long-term survival rates for these new devices.
What is Heart Failure and What Causes it ?
There are two main reasons for heart problems.
- One is caused by plaque building up in the arteries of the heart. This is called coronary artery disease.
- The other is caused by disease of the heart muscle. This condition is called idiopathic cardiomyopathy. Doctors do not know what causes it.
In both cases, as the heart grows weaker, it is less able to pump oxygen-rich blood through the body. As it tries harder to pump blood, it grows larger. Doctors call this an enlarged heart. After a while, the enlarged heart has to work so hard that it just wears out. Soon it cannot pump even the smallest amount of blood.
A weak, enlarged heart can cause you to feel short of breath and tired, even when you are quiet, such as when resting or at night in bed. Your feet, legs, and stomach may swell, and you may feel sick to your stomach and not feel like eating.
How is Heart Failure Treated ?
There are several options for treating heart failure. Your doctors will first try medical therapy. In some cases, medicines alone can success fully treat heart failure.
If needed, your doctor may use other methods of treatment. These are:
- Pacemakers. These devices are used to treat a heart that beats too slowly. Some of the newer pacemakers are even better at helping the heart pump as it should.
- Angioplasty. This is a procedure that opens clogged arteries.
- Repair the heart valve. This procedure can often make your heart function much better. If doctors cannot repair the valve, they may be able to replace it with an artificial (man-made) valve.
- Cardiac size reduction. During this procedure, your doctor removes a piece of the heart muscle from an enlarged heart. This makes your heart smaller, which allows it to pump more efficiently and vigorously.
Contraindications for heart transplant
Contraindications are 16):
- irreversible pulmonary hypertension/elevated pulmonary vascular resistance;
- active systemic infection;
- active malignancy or history of malignancy with probability of recurrence;
- inability to comply with complex medical regimen;
- severe peripheral or cerebrovascular disease and irreversible dysfunction of another organ, including diseases that may limit prognosis after heart transplantation.
Ultimately, your transplant team will determine if you are a candidate for a heart transplant.
Ventricular assist devices
For some people who can’t have a heart transplant, another option may be a ventricular assist device. A ventricular assist device is a mechanical pump implanted in your chest that helps pump blood from the lower chambers of your heart (ventricles) to the rest of your body.
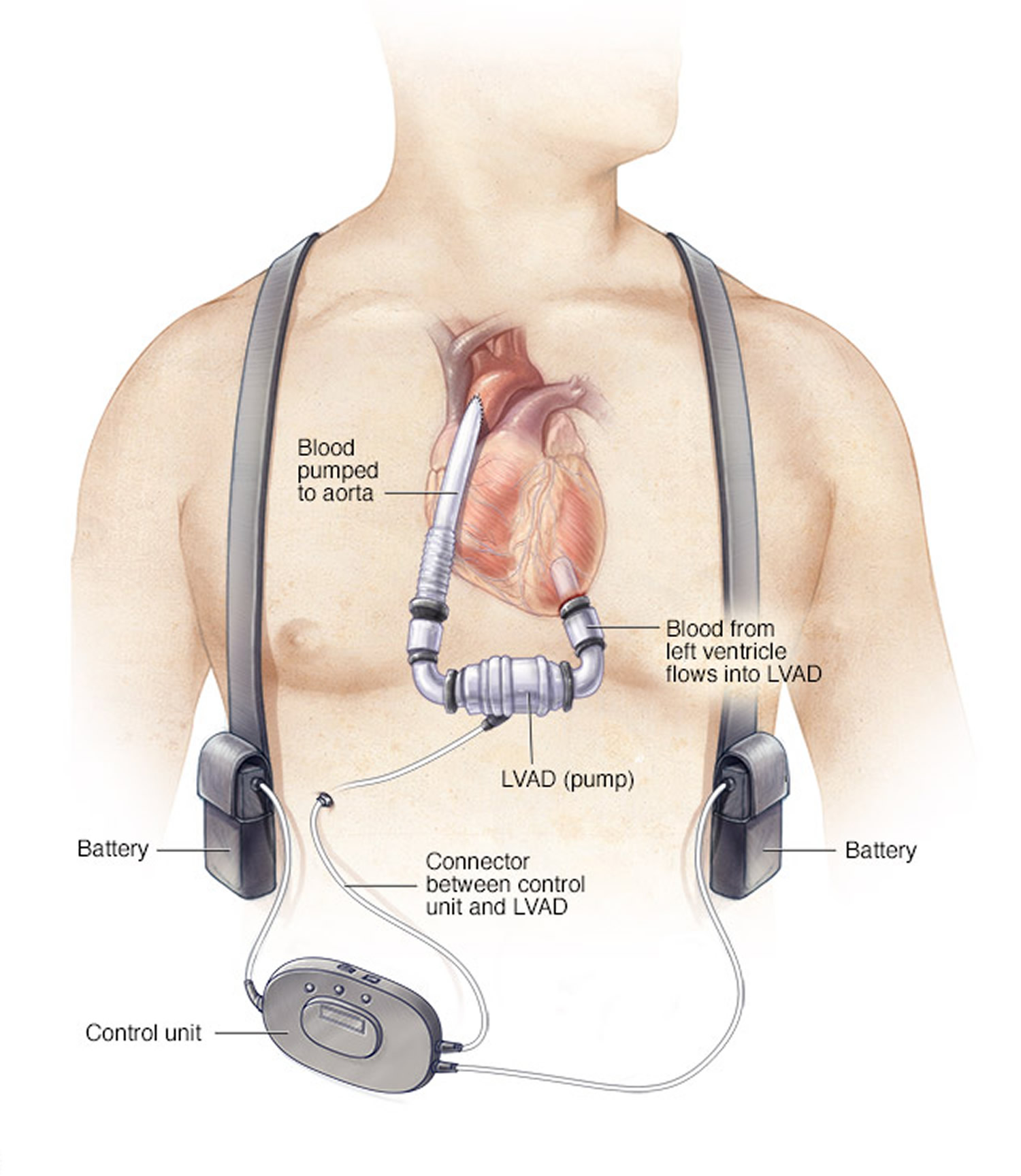
Ventricular assist devices are commonly used as a temporary treatment for people waiting for a heart transplant. These devices are increasingly being used as a long-term treatment for people who have heart failure but aren’t eligible for a heart transplant. A left ventricular assist device (LVAD) is implanted under your skin. It helps pump blood from the left ventricle of your heart and on to the rest of your body. A control unit and battery pack are worn outside your body and are connected to the LVAD through a port in your skin. If a ventricular assist device doesn’t help your heart, doctors may sometimes consider a total artificial heart — a device that replaces the ventricles of your heart — as an alternative short-term treatment while you’re waiting for a heart transplant.
Figure 1. Left ventricular assist device
Before a heart transplant
There are five steps to getting a heart transplant 17). Your transplant team will:
Decide if you need a new heart. Decide if you are healthy enough to receive a new heart. Prepare you for your operation. This can take a long time, and there is no guarantee that a heart will be found. Perform a heart transplant operation. Help you stay healthy after your operation.
Step 1. Your Transplant Team Decides If You Need a New Heart
Many heart diseases get worse very slowly. Sometimes one treatment will work where another did not. Because of this, the transplant center will first determine which therapy is best for your condition.
Sometimes a new drug or therapy can improve your heart condition. The transplant center will do its best to make sure you have every chance to get better and live longer with your own heart before they recommend a heart transplant.
Step 2. Your Transplant Team Decides If You Are Healthy Enough to Receive a New Heart
Before you have a heart transplant, a team of health care professionals will talk to you about what may happen if you get a new heart. What happens can depend on your physical health, your mental health, and how easy it will be for you to get the transplant medicines you will need.
There are four parts to this phase.
- First you will visit a transplant center. You, your doctor, a nurse, or a social worker can schedule this visit. Your doctor’s office will send your medical records to the transplant center before your appointment. Your records should show that you are taking your medicine properly and are on a restricted diet. Your records will also confirm that you have no medical conditions that can keep you from receiving a transplant.
- During this visit, your physical health will be evaluated. The transplant team will do a complete evaluation of your physical health. They may do more tests to evaluate your: heart kidneys and gallbladder stomach, esophagus, and intestines lungs bladder teeth and gums brain and nervous system prostate, if you are a man breasts and cervix, if you are a woman The transplant team may order other tests as well.
- Then, your mental health will be evaluated. You may need to see a social worker or psychologist to make sure you are not addicted to alcohol or drugs. It is also important to make sure you have no emotional problems that can interfere with your health.
- Finally, you will see an insurance specialist. An insurance specialist will review your insurance to make sure your policy covers the transplant operation and the medicines you will need after your transplant.
If the transplant team decides you are a good candidate for the operation, they will work with you to find a new heart.
Step 3. Your Transplant Team Prepares You for Your Operation
This step involves finding a new heart for you. Sometimes this can take a long time. How long it takes depends on your body size, your blood type, and how sick you are.
While waiting for your operation, you will have regular visits with your doctor and transplant team. They will monitor your health, and they will work with you to make sure you are eating and exercising properly. You need to let them know of any changes in your health.
Step 4. Your Transplant Team Performs a Heart Transplant Operation
Transporting donor organs for transplant
A heart transplant usually needs to occur within four hours of organ removal for the donor organ to remain usable. As a result, hearts are offered first to a transplant center close by, then to centers within certain distances of the donor hospital.
You’ll need to remain in close contact with the transplant team and let them know if you have any changes to your health. Make sure the transplant center has phone numbers to be able to contact you anytime. The transplant center needs to be able to reach you 24 hours a day.
When you’re notified that a potential organ is available, you and your transplant team have a limited amount of time to consider whether to accept the donation. You’ll be expected to travel to the transplant hospital immediately after being notified of the potential donation. You’ll usually need to be prepared to get to the hospital within three hours.
As much as possible, you should generally make travel plans ahead of time. Some heart transplant centers provide private air transportation or other travel arrangements. Have a suitcase packed with everything you’ll need for your hospital stay, as well as an extra 24-hour supply of your medications.
Once you arrive at the hospital, your doctors and transplant team will conduct a final evaluation to determine if the donor heart is suitable for you and if you’re ready to have surgery. If your doctors and transplant team decide that the donor heart isn’t appropriate for you or surgery isn’t appropriate for you, you may not be able to have the transplant.
The Procedure
When the right heart is found, the nurse coordinator will call you and you will go to the hospital. The transplant doctors will check the donor heart while you are being evaluated. You will be given medications before and during the operation to prevent your body from rejecting the new heart. If the donated heart is the right match for you, you will be taken to the operating room and put to sleep with an anesthetic.
A transplant surgeon will prepare your chest cavity so your heart can be removed. At the same time, the new heart will be removed from the donor and sent to your hospital. This heart will be placed in your chest through the opening in your chest cavity. This is called a sternotomy.
There are two very different surgical approaches to heart transplantation: the orthotopic and the heterotopic approach 18). Because the length of this surgery is different for every patient, families should talk with the surgeon about what to expect.
- Orthotopic Approach. The more common of the two procedures, the orthotopic approach, requires replacing the recipient heart with the donor heart. After the donor heart is removed, preserved and packed for transport, it must be transplanted into the recipient within four to five hours. The recipient receives general anesthesia and is placed on a bypass machine to oxygenate the blood while the heart transplant is being performed. After the recipient’s heart is removed, the donor heart is prepared to fit and implantation begins.
- Heterotopic Approach. Heterotopic transplantation, also called “piggyback” transplantation, is accomplished by leaving the recipient’s heart in place and connecting the donor heart to the right side of the chest. The procedure is rare compared to orthotopic transplantation and is advantageous because the new heart can act as an assist device if complications occur. Your physician can explain why this approach may better suit your needs.
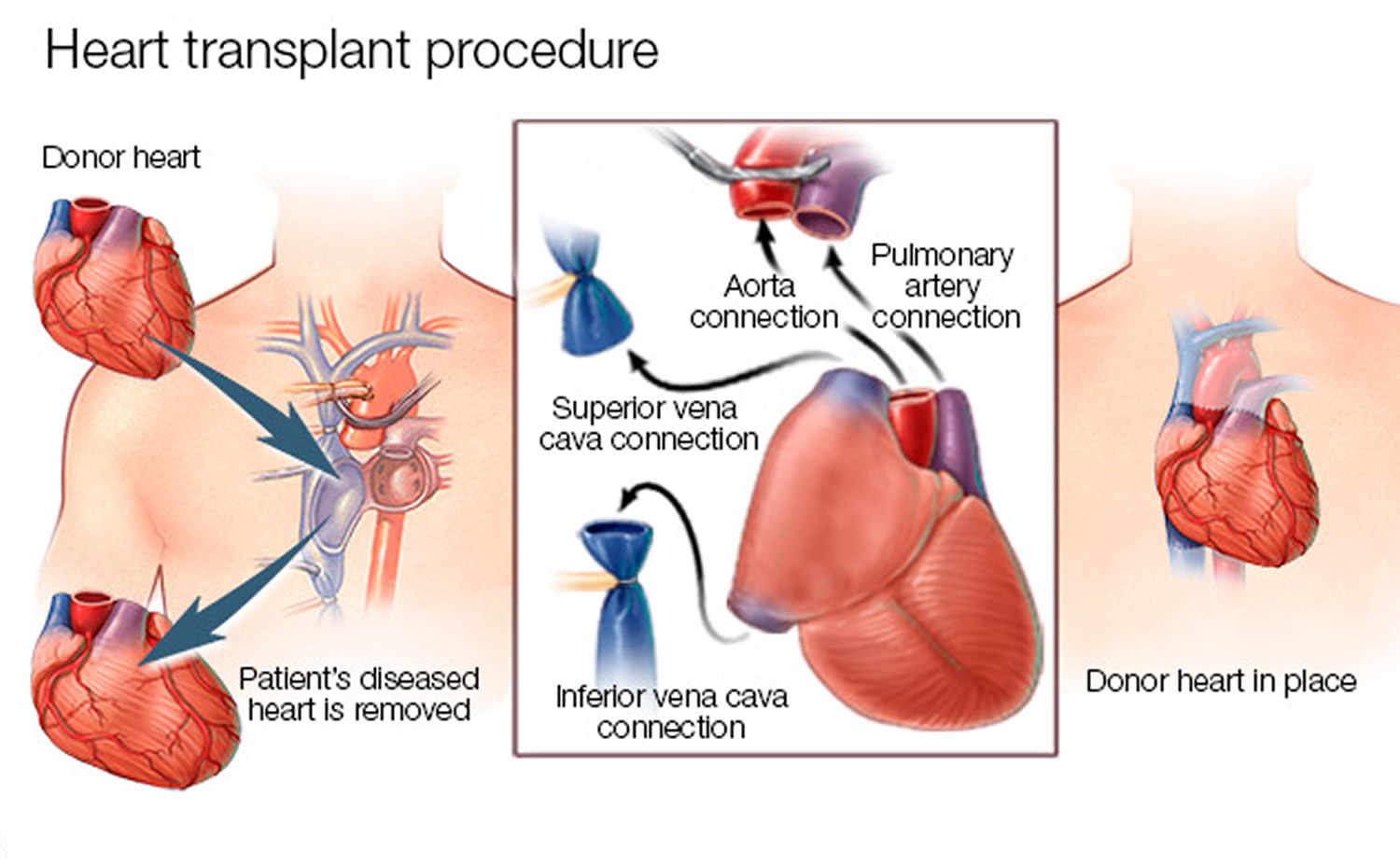
Most heart transplant surgeries are done with a method called orthotopic 19). Your heart is removed, and the donor heart is sewn in place. Once the new heart is in place, the donor’s main arteries – the aorta and pulmonary arteries – are sewn to yours 20).
Figure 2. Heart transplant procedure
After the operation, you will be taken to a special unit for recovery. You will stay in the hospital until your doctor feels you are ready to go home. How long you stay will depend on your health and how well your new heart is working. It will also depend on how quickly and easily you learn to take care of your new heart.
Transplant Medicines
After your operation, you will take strong medicines to keep your body from rejecting your new heart. Your immune system protects you from foreign invaders, and your body will think the new heart is a foreign invader. So your immune system will try to reject your new heart. This can damage it. Because of this, you will take immunosuppressants (im-u-no-su-pres-ants), also called anti-rejection medicines. These drugs suppress the immune system enough to keep your transplanted heart healthy.
That’s why these medicines are called immunosuppressants or anti-rejection drugs. Your body will remember that the heart once belonged to someone else, so you will need to take these drugs for as long as you have the transplant.
Step 5. Your Transplant Team Helps You Stay Healthy After Your Operation
It is very important that you keep yourself healthy after your transplant. Here are a few important reminders:
- After you leave the hospital, make sure you go to the transplant center often. Also be sure you go to all your doctor appointments. This very is important!
- You will only have to do this for a few months.
- Take your medicines properly. This is extremely important!
- Watch your weight and be sure to get some exercise on a regular basis.
- Be sure to tell the staff at the transplant center if you have problems keeping your appointments or taking your medicines.
Your Doctor Appointments
If your body begins to reject your new heart, you may not know it. Some patients may have signs, but most do not recognize them. If your body is rejecting the new heart, your doctors and nurses will know it. This is why it is so important to go to all your medical appointments. Your health care providers watch closely for signs of rejection and side effects from the medications. But, they must examine you and test your blood to know for sure.
Your doctor and transplant staff will watch for these signs:
- Rejection: The risk of rejection never goes away. You will always need anti-rejection drugs. Your doctor may lower the dosage, but you should never skip or stop taking the drugs. A biopsy of the heart is the best way to know if your body is rejecting your new heart. Your doctors will do this many times for the first year after your transplant. After that, they will biopsy your heart, but less often.
- Infection: Immunosuppressant drugs can increase the chance of getting infections. These infections can be treated. However, you need to tell your doctor if you have a fever, unusual pain, or any other new feelings. The risk of infection will go down when your doctor lowers the dosage.
- High blood pressure: High blood pressure is a common problem after transplant. It can damage your new heart and cause strokes and heart attacks.
- Diabetes Mellitus: Anti-rejection medications can cause diabetes. If you had diabetes before your transplant, you may find it harder to control your blood sugar level after your transplant.
- High cholesterol: Your anti-rejection medication can also cause high cholesterol. There are some medications called statins that control cholesterol and help prevent rejection because they also control inflammation.
- Heart disease: Some forms of heart disease can come back in the transplanted heart. Your doctor and transplant staff will monitor you for signs of this problem.
- Cancer: Anti-rejection drugs can raise the risk of getting cancer, especially blood cancer and skin cancer. Although blood cancer, called lymphoma, can be fatal, your doctor can lower the risk by lowering the dose of anti-rejection drugs. Your transplant team will suggest getting screened for cancer early and on a regular basis. They will recommend you regularly: get a colonoscopy, a mammogram, a pap smear, or prostate exam. And see a dermatologist.
- Osteoporosis: This is thinning of the bones. Being ill, eating a poor diet, being inactive, or taking prednisone and other anti-rejection drugs can cause osteoporosis. Your doctor will most likely order a bone density test and may put you on drugs that prevent osteoporosis.
- Cataracts: Prednisone (a steroid medication) and other drugs can cause cataracts, which are cloudy spots on the lens of your eye. You cannot prevent cataracts, but they can be surgically removed. Your doctor will ask you to see an eye doctor (ophthalmologist) at least once a year to get checked for cataracts and glaucoma. Glaucoma is pressure in the eye that can damage your vision.
- Kidney disease: The main medicines used to treat rejection, and many of the medicines used to treat infection, can hurt your kidneys. Your doctors will try to make sure you have enough medicine to prevent rejection of your new heart, but not so much that it hurts the kidneys. Sometimes this is hard to do. If you are older, or if your kidneys have already been injured by illness or medications, you may have permanent kidney damage. This can cause your feet to swell and your body to retain fluid. You may feel very tired and not feel well overall. Kidney disease is a serious problem. You will need to go for regular blood tests. These tests make sure the levels of your anti-rejection medications are not too high or too low.
Heart transplant list
Getting On The Heart Transplant List
For most transplant candidates, the first step in receiving a transplant is to get on national transplant waiting list:
- the OPTN (Organ Procurement & Transplantation Network) 21) or
- the UNOS (United Network for Organ Sharing) 22)
The Organ Procurement and Transplantation Network (OPTN) 23) secure transplant information database contains all national data on the candidate waiting list, organ donation and matching, and transplantation 24). This system is critical in helping organ transplant institutions match waiting candidates with donated organs. Institutions also rely on the database to manage time-sensitive, life-critical data of all candidates, before and after their transplants. The Organ Procurement and Transplantation Network (OPTN) is an official U.S. Government web site managed by the Health Resources and Services Administration, U.S. Department of Health & Human Services 25).
The National Waiting List
The waiting list is a computer database that contains medical information on every person who is waiting for any type of organ transplant in the U.S. and Puerto Rico. You will not have a number ranking for transplant based on all the other persons who are waiting for your organ. You also will not move up or down each time someone receives a transplant.
Here are the necessary steps to get on the national waiting list:
- Your physician must give you a referral.
- Contact a transplant hospital. Learn as much as possible about the 200+ transplant hospitals in the United States and choose one based on your needs, including insurance, location, finances and support group availability.
- Schedule an appointment for an evaluation and find out if you are a good candidate for transplant.
- During the evaluation, ask questions to learn as much as possible about that hospital and its transplant team.
- If the hospital’s transplant team determines that you are a good transplant candidate, they will add you to the national waiting list.
Your transplant hospital will notify you within 10 days to inform you about your date of listing. If you have questions about your status on the list, you should ask the team at your transplant hospital.
All transplant candidates who do not have the option of a living donor (and even some who do) usually wait for some length of time because there are not enough donor organs for all who need them.
Organ Type and Waiting Time
Most candidates, except those with living donors, wait for an organ due to the shortage of donor organs. Because each candidate’s situation is unique, waiting times can vary, depending on a number of factors, such as those described below. To better understand what influences waiting time, talk with your transplant team.
What determines who will be offered an organ?
Depending on the organ, there are many considerations. These include but are not limited to:
- age
- blood type
- medical urgency
- waiting time
- geographic distance between donor and recipient
- size of the donor organ in relation to the recipient
- type of organ needed
How does organ type affect waiting times ?
Heart Allocation
Physicians assign a status code to individuals waiting for a heart transplant. This code indicates how medically urgent it is that you receive a transplant. In addition, the system allocates hearts locally first, and then in a specific sequence by zone. Please see the OPTN/UNOS Allocation of Thoracic Organs Policy for details 26).
Lung Allocation
All candidates waiting for a lung will be grouped together, regardless of whether they are waiting for a single lung or a double lung. If one lung is allocated to a patient needing a single lung transplant, the other lung will be then allocated to another patient waiting for a single lung transplant. In addition, the system allocates thoracic organs locally first, and then in a specific sequence by zone. Please see the OPTN/UNOS Allocation of Thoracic Organs Policy for details 27).
Heart/Lung Allocation
If you are waiting for heart-lung transplant, you will be registered on the individual UNOS Patient Waiting lists for both the heart and the lung. When the patient is eligible to receive a heart, the lung will be allocated to the heart-lung candidate from the same donor. When the patient is eligible to receive a lung, the heart shall be allocated to the heart-lung candidate from the same donor isolated. In addition, thoracic organs are allocated locally first, and then in a specific sequence by zone. Please see the OPTN/UNOS Allocation of Thoracic Organs Policy for details 28).
Other Options to Consider
Multiple Listing
As addressed in the OPTN/UNOS Policy 29), patients may be listed at more than one transplant center. Being listed at more than one transplant center does not guarantee that an organ will become available faster than if you are listed at one transplant center. In addition, you probably would not benefit from listing at multiple centers in the same local allocation area. This is because waiting time priority is first calculated among candidates at all hospitals within the local donation area, not for each hospital individually.
It’s important to note that some transplant programs may not accept multiple-listed patients. Others may set their own requirements for multiple-listed candidates.
If you choose to multiple list, your primary care physician should contact your centers of choice so that you may be evaluated as a transplant candidate, as you did with your primary evaluation. Read a detailed brochure here now 30).
Transferal of Waiting Time
As addressed in the OPTN/UNOS Policy 31), patients may transfer their primary waiting time from one transplant center to another center. This transfer may be necessary for a number of reasons, such as a change in the transplant candidate’s health insurance or if the candidate has moved. Read a detailed brochure here now 32).
Living Donation
Living donor transplants are a viable alternative for patients in need of new organs. Learn more about living donation here 33).
Kidney paired donation is a type of living donation that is a transplant option for recipients who have a willing and able living donor but are an incompatible match due to blood or tissue type. Learn more paired donation here 34).
People You Should Know
Your Transplant Team
Many people at the transplant center work to make your transplant as successful as possible. It’s important that you know who each of these people are and what they will be doing to help you through your transplant. You will need to feel comfortable talking to them and asking them questions about your health and/or status concerning transplantation.
Your transplant team will include all or some of the following people:
- Transplant Coordinator. Usually a registered nurse, who will be your main contact and will work with you and other members of your transplant team to coordinate your care.
- Transplant Surgeon. The doctor who will evaluate your present condition, make recommendations, and ultimately perform your transplant surgery.
- Transplant Physician. This doctor, whether a nephrologist, hepatologist, cardiologist or other specialist, will assist the surgeon in evaluating your need for transplantation and help with your care.
- Transplant Financial Coordinator. The financial coordinator has detailed knowledge of financial matters and hospital billing methods. This person works with social workers to determine how you can best afford the cost of your transplant.
- Insurance Case Manager. Often your first point of contact, the insurance case manager helps navigate the specifics of insurance coverage.
- Social Worker. Most transplant programs are staffed with social workers who are ready to help you. Transplant social workers can assist transplant candidates and their families with a variety of helpful resources, including the development of a financial plan. They can also help address psycho-social issues and determine your needs and help you understand and cope with basic problems associated with your illness.
- Dietician. As an integral part of the transplant team, the registered dietitian develops nutrition therapy to patients before and after transplantation. Educating patients about maintaining a healthy weight and minimizing side effects of anti-rejection drug therapy ensures optimal nutrition status and improves transplant outcomes.
Questions to Ask Your Transplant Team
Patients usually have many questions about transplantation and their health as they go through the transplant process. In addition to financial questions, below is a list of issues and concerns you may want to discuss with your transplant team. Be sure to write your questions down and bring them to the appointment. You might also want to bring a trusted friend or family member with you and ask them to take notes.
Questions about Your Evaluation
- What should I bring with me?
- What should I do to prepare for the appointment?
- Does your center offer parking permits or overnight accommodations?
- What does the evaluation and testing process include? How does it affect whether I am put on the list?
Before the transplant
- Who will tell me and my family about the transplant process?
- Can I tour the transplant center?
- What other options do I have besides transplantation?
- What are the risks of transplantation?
- What are the benefits of transplantation?
- What are the transplant success rates at this hospital?
- How many transplants do you perform at this hospital each year?
- How long has this hospital been doing transplants?
- What is involved in the evaluation and testing process?
- How do my test results affect whether or not I am put on the list?
- How long is the local waiting list?
- How do you decide whether you will accept an organ offered to me?
- Who are the members of the transplant team and what are their jobs?
- How many attending surgeons are available to do my type of transplant?
- Do I need to stay close to the transplant hospital while I am put on the waiting list?
- How soon must I be at the transplant hospital after being called?
- Is there a special nursing unit for transplant patients?
- Will the transplant center team advise my local health care providers of my care requirements?
- Will I be asked to take part in research studies?
After the transplant
- What is the length of hospitalization after my transplant?
- Do I need to stay close to the hospital post-transplant? If so, for how long?
- What is the usual immunosuppressive treatment?
- What follow-up examinations and tests will I undergo? How frequently?
- Will I need to return to the transplant center if I have complications?
- What medications will I take after I leave the hospital and how much will they cost?
Financial Questions
- How much will the transplant cost? How much will I have to pay?
- What part of the transplant cost is covered by my insurance?
- What if my insurance does not pay for medications?
- What financial coverage is accepted by this hospital?
- What happens if my financial coverage runs out?
Questions about Living Donation
- Does the hospital do living donor transplants?
- What types of living donor transplants does the center do?
- Is a living donor transplant a choice in my case? If so, where can the living donor evaluation occur?
- What are the costs if I have a living donor?
Heart Transplant Cost
Financing a transplant raises many questions and concerns for patients and their families. The first step in developing a financial strategy is to figure out how much of your costs insurance will cover. Your financial coordinator or social worker can help. Then you can begin to explore other funding sources.
Most patients use a combination of sources. Some patients can finance the transplant procedure through their primary insurance coverage and use savings and other private funds to pay for other expenses. Many patients work with community fundraising groups to complete their transplant financial strategy.
Questions to Ask Your Transplant Financial Coordinator
- How much will the transplant cost ? How much will I have to pay ?
- What financial coverage does the hospital accept (such as Medicare, Medicaid, private insurance, etc) ?
- What happens if my financial coverage runs out ?
- Will the costs vary if I have a living donor ?
Questions to Ask Your Insurance Company
- Will my insurance cover me throughout the transplantation process?
- Am I covered for a transplant right now, or do I have to wait a certain period of time (pre-existing exclusion clause)? If yes, how long?
- Do I need authorization (approval) before I have a transplant?
- Do I need to notify you when I am admitted to the hospital? How soon after I am admitted?
- Do I need a second opinion? If so, who will pay for it?
- What do I do if I run out of insurance money?
- How are the costs of the transplant applied to my deductible?
- What happens if I change jobs or lose my job? Will it affect my insurance?
- How can I cut down on insurance expenses to make sure my coverage lasts as long as I need it?
- What pre- and post-transplant tests are covered? Do I need to go to a certain facility for these tests to be covered?
- Are expenses for food, housing and transportation covered while I wait for my transplant?
- How much coverage will I receive for post-transplant medications? What is the co-pay amount?
Questions to Ask When Choosing a Fundraising Organization
- Are you a 501(C)(3) (tax-exempt) organization? If so, can people who donate to my fund use the amount of money they donate as an income tax deduction?
- What type of account will be used?
- How can I find out how much money is in my account?
- Who has access to my funds?
- Are there any additional fees?
- What are my options if I don’t receive a transplant or don’t need all the money?
- Can I talk to other patients you have helped?
- Who should I call if I have questions or problems?
- What is the process of paying my bills with these funds?
- Will you check my bills for accuracy?
- What other services do you have available?
- Can you refer me to other sources for financial help?
Transplant Costs
The cost of a transplant, including preliminary testing, the surgery itself and post-operative recovery costs vary across the country and depend on the hospital and organ type. These costs start to add up, even before your transplant. Therefore, patients commonly rely on several sources to help pay for their medical and non-medical costs of pre- and post-transplantation.
Medical Costs
Medical costs include:
- insurance deductibles
- insurance co-pays
- pre-transplant evaluation and testing
- surgery
- fees for the recovery of the organ from the donor
- follow-up care and testing
- additional hospital stays for complications
- fees for surgeons, physicians, radiologist, anesthesiologist and recurrent lab testing
- anti-rejection and other drugs, which can easily exceed $2,500 per month
- rehabilitation
Non-Medical Costs
Non-medical costs include:
- food, lodging and long distance phone calls for you and your family
- transportation, to and from your transplant center, before and after your transplant
- plane travel to get to your transplant hospital quickly
- child care
- lost wages if your employer does not pay for the time you or a family member spends away from work
- If your transplant center is not close to your home, lodging close to the center before and after your surgery. Some centers offer free or low-cost hospitality houses for you and your family.
Table 1. Estimated U.S. Average 2011 Billed Charges Per Transplant
| Transplant | 30 Days Pre- transplant | Procurement | Hospital Transplant Admission | Physician During Transplant | 180 Days Post-transplant Admission | Immuno- suppressants | Total |
|---|---|---|---|---|---|---|---|
Heart Only | $47,200 | $80,400 | $634,300 | $67,700 | $137,800 | $30,300 | $997,700 |
Single Lung | $10,300 | $73,100 | $302,900 | $33,500 | $117,700 | $23,700 | $561,200 |
Double Lung | $21,400 | $90,300 | $458,500 | $56,300 | $142,600 | $28,200 | $797,300 |
Heart-Lung | $56,800 | $130,500 | $777,700 | $81,000 | $169,100 | $33,300 | $1,148,400 |
Liver | $25,400 | $71,000 | $316,900 | $46,600 | $93,900 | $23,300 | $577,100 |
Kidney | $17,000 | $67,200 | $91,200 | $18,500 | $50,800 | $18,200 | $262,900 |
Pancreas | $17,000 | $65,000 | $108,900 | $17,800 | $61,400 | $19,300 | $289,400 |
Intestine | $55,100 | $78,500 | $787,900 | $104,100 | $146,600 | $34,600 | $1,206,800 |
Funding Sources
Common funding sources to help with the costs of transplants include:
- Private Health Insurance
- COBRA Extended Employer Group Coverage
- Health Insurance Marketplace
- Medicare
- Medicare Prescription Drug Plans
- MediGap Plans
- State Health Insurance Assistance Programs
- Medicaid
- Charitable Organizations
- Advocacy Organizations
- Fundraising Campaigns
- TRICARE (Formerly Champus) and Veterans Administration (VA)
- State “High Risk” Insurance Pool
Note: This information is only a brief summary and is not intended to provide complete information. Ask your transplant financial team and your insurance provider or employee benefits officer for the latest information or help.
Private Health Insurance
You or your family may have health insurance coverage through an employer or a personal policy. Although many insurance companies offer optional coverage for transplant costs, the terms and benefits of insurance vary widely. Read your policy carefully and contact your insurance company if you have questions about how much of your costs they will pay, including your lab tests, medications and follow-up care after you leave the hospital.
Some insurance questions to consider:
- Is my transplant center in-network with my insurance company?
- If my transplant center is out-of network, do I have an out-of-network benefit for transplant?
- What deductibles will apply?
- What are my co-payments for doctor visits, hospitalizations and medications?
- Does my plan require prior authorization?
- Who needs to get prior authorization?
- Does my plan have a lifetime maximum or “cap” for transplant services?
- Do any pre-existing-condition requirements
Regardless of how much your insurance covers, you are responsible for any costs not paid by your insurance, unless you have made other arrangements. If you are responsible for paying any or all of your insurance premiums, be sure to pay them on time so that you do not lose your insurance.
Transplant center social workers and financial coordinators can also help you with the information you need. They can contact your insurance company to check on your benefits and explain your coverage in more detail.
Insurance “Caps”
Many insurance policies state a total amount of money that will pay out in your lifetime, also referred to as a “cap.” After the insurance company pays this amount, they are not required to pay additional benefits. Some policies also put a cap on how much they will pay for a particular procedure or treatment, such as a transplant or the total amount of drugs per year. Even after the actual transplant, the ongoing cost of care may exceed the cap. Because the amount of the cap varies greatly depending on the individual policy, it is important to be familiar with the terms of your insurance cap and keep track of how your insurance dollars are spent.
Experimental and Investigative Procedures
If your transplant center asks you to be involved in any experimental procedures or studies, be sure to ask your center or insurance company if your insurance policy will cover the payment. It is important to know that you do not have to agree to be involved in any experimental procedures or investigational studies. If you still have questions, contact your employer’s benefits office or your state insurance commissioner.
Tips
- Keep copies of all medical bills, insurance forms and payments (or canceled checks).
- Ask your insurance company about pre-certification or using a specific provider.
- Follow the rules set forth by your insurance company so that your benefits will not be decreased.
- Always keep a log (who you talked to, date and time and questions answered) of your conversations with anyone in the hospital’s billing office or your insurance company.
- Make sure to keep your transplant center informed about your insurance, especially if you have more than one insurance company.
COBRA Extended Employer Group Coverage
If you are insured by an employer group health plan and you must leave your job or reduce your work hours, you may qualify for extended coverage through COBRA (Consolidated Omnibus Budget Reconciliation Act of 1985). This federal law requires certain group health plans to extend coverage for 18 to 36 months after benefits end. This requirement is limited to companies employing 20 or more people. You pay the full cost of the premiums for the group health plan. Learn more by contacting your employer’s benefits office or visit the federal Department of Labor web site 36).
Health Insurance Marketplace
Also known as the health insurance “exchange,” the marketplace is a set of government-regulated and standardized health care plans in the United States. Learn more at Healthcare.gov 37).
Medicare
Medicare is a federal health insurance program available to people who are 65 or older, disabled or have end stage renal disease (ESRD).
Medicare, like most private insurance plans, does not always pay 100% of your medical expenses. In most cases, it pays hospitals and health providers according to a fixed fee schedule, which may be less than the actual cost. You must pay deductibles and other expenses. Medicare currently offers coverage for transplant of:
- kidneys
- kidney-pancreas
- pancreas, either after a kidney transplant or for certain indications
If you already have Medicare due to age or disability, Medicare also covers other transplants:
- heart, in certain circumstances
- lung
- heart-lung
- liver, including transplants necessitated by hepatocellular carcinoma (HCC)
- intestines
To receive full Medicare benefits for a transplant, you must go to a Medicare-approved transplant program. These programs meet Medicare criteria for the number of transplants they perform and the quality of patient outcomes.
If you have questions about Medicare eligibility, benefits, or transplant programs, contact your local Social Security office, or Medicare at or www.medicare.gov 38).
Medicare Prescription Drug Plans
Medicare Part D covers costs for prescription drugs. To get this coverage you must choose and join a Medicare drug plan. For more information visit www.medicare.gov 39).
MediGap Plans
Many people on Medicare also choose to buy a private “Medigap” policy to pay for costs not covered by Medicare. Check with a local insurance agent or go to www.medicare.gov 40).
State Health Insurance Assistance Program
The State Health Insurance Assistance Program (SHIP) is a national program that offers one-on-one counseling and assistance to people with Medicare and their families. Your transplant social worker or financial coordinator can provide information on your state’s SHIP program.
Medicaid
Medicaid is a federal and state government health insurance program for certain low-income individuals. Each state determines criteria for:
- eligibility
- benefits
- reimbursement rates
Most Medicaid programs only cover transplants performed in their state, unless there are no centers that can transplant that organ. For more information, contact your local human services department or the financial coordinator at your transplant center.
Charitable Organizations
Charitable organizations offer a range of support, from providing information about diseases, organs and transplants, to encouraging research into these diseases and treatments.
Also, although it is very unlikely that one organization can cover all of the costs for an individual patient, some organizations provide limited financial assistance through grants and direct funding. For example, an organization may only be able to help with direct transplant costs, food and lodging or medication costs.
Advocacy Organizations
Advocacy organizations advise transplant patients on financial matters. If you agree to a financial arrangement with an advocacy organization, it is important to make sure that the funds are available in a manner that suits your needs. You may even want legal assistance in reviewing a written agreement before signing. Your bank can also help you review the arrangement.
Every advocacy organization should be able to provide supporting information and background documentation to prove they are legally recognized to help those in need. Brochures and other background information should never serve as substitutes for these documents. Ask advocacy organizations to provide you with copies of the following documents:
- a current federal or state certification as a charitable, non-profit organization
- a current by-laws, constitution and/or articles of incorporation
- a financial statement for the preceding year, preferably one that
- an audit report from an independent organization
- references
Fundraising Campaigns
Public fundraising is often used to help cover transplant expenses not paid by medical insurance. Before you begin seeking donations, it may be necessary to check with your city/county governments, legal advisor or transplant team about the many legal and financial laws and guidelines.
If you decide to use public fundraising as a way to cover your expenses, you may want to contact local newspapers, radio or television stations to help support your cause. In addition, try to enlist the support of local merchants and other sponsors to promote or contribute to your events. Your friends, neighbors, religious groups, local chapters of volunteer or service groups and other community groups may also be able to help.
It is also very important to understand that the funds you raise only be used for your transplant-related expenses and donated money sometimes has to be counted as taxable income. In cases in which money must be counted as income, you may lose your Medicaid eligibility.
TRICARE and Veterans Administration
Government funding for families of active-duty, retired, or deceased military personnel may be available through TRICARE. TRICARE standard may share the cost of most organ transplants and combinations. TRICARE also covers living donor kidney, liver, and lung transplants. Patients must receive pre-authorization from the TRICARE medical director and meet TRICARE selection criteria. Pre-authorization is based on a narrative summary submitted by the attending transplant physician. For more information about TRICARE, contact the health benefits advisor at your nearest military health care facility, call the TRICARE Benefits Service Branch or learn more here 41).
State “High Risk” Insurance Pool
Many states offer a high-risk health insurance pool to provide access to coverage to individuals with serious pre-existing medical conditions. Typically the premiums are higher, and the coverage may be more limited. Ask your transplant center social worker or financial coordinator if your state has a high-risk insurance pool or learn more at www.Healthinsurance.org 42).
Financial Resources Directory
Because many patients cannot afford to pay for the full cost of organ transplant surgery, or even a small insurance deductible amount, using their personal funds, it is common for patients explore other options to help them fund their procedure.
The following organizations may provide financial assistance to transplant candidates or recipients and their families. This is a sample listing and should not be interpreted as a comprehensive list or an endorsement. Ask your transplant financial team for the latest information or help.
For a full financial resources directory listings 43) go here: https://transplantliving.org/before-the-transplant/financing-a-transplant/directory/
Selecting A Hospital
You do have choices when it comes to hospital care. The most important consideration in any choice is the individual’s specific situation. Each patient has different needs, preferences and desires that need to be taken into account when selecting an appropriate hospital.
When choosing a transplant center, patients should carefully consider these factors:
- The experience of the transplant team and support personnel. It is always important to know how much experience a hospital has with the type of care you need.
- The cost of the procedure and related items. The cost of a transplant, including preliminary testing, the surgery itself and post-operative recovery costs vary across the country by hospital and organ type.
- Insurance coverage. Although many insurance companies offer coverage for transplant costs, the terms and benefits of insurance policies vary widely. Some insurance companies establish network agreements with certain transplant centers; the insurer may pay a higher proportion of costs for centers within their network. In addition, many transplant centers have different policies about the types of insurance they accept for the type of transplant you need.
- Geographical proximity to the program. The travel time to the transplant center is important when you are waiting for an organ and is a key factor considered in organ distribution.
- The quality and availability of pre- and post-transplant services. Offering a comprehensive system of support services to meet the special needs of patients and their families is important. Education and emotional support can help you feel informed about your health care decisions.
- A commitment to keeping up with technologic advances. It may be important to identify if a transplant center has a commitment to technology and the latest procedures, both which offer assurance that a program is continually growing.
- Multicultural sensitivity. Does the transplant center have bilingual staff members and/or access to translators if needed? Regardless of treatment, patients should always feel understood and informed throughout the treatment process.
- Availability of friends and family for assistance. More and more, family members and friends are needed to help with the patient’s care as an outpatient.
Support Services
Common support services to help with recovering from a transplant include:
- vocational rehabilitation
- social security coverage for the disabled
- Americans with Disabilities Act (ADA)
Note: This information is only a brief summary and is not intended to provide complete information. Ask your transplant financial team and your insurance provider or employee benefits officer for the latest information or help.
Vocational Rehabilitation
Vocational rehabilitation provides assistance to individuals who cannot return to work after an injury or illness. It helps individuals achieve suitable employment or enhance their ability to function independently at home and in the community. Federal and state governments fund each state’s department of vocational rehabilitation, which, depending on the individual, may provide the following types of services:
- evaluation to determine job skills, abilities and attitudes, which includes medical, psychological and vocational testing
- development of an individualized rehabilitation plan, including long-range vocational goals, intermediate objectives to achieve vocational goals, the process for evaluating progress, rehabilitation equipment, client assistance (including financial services) and post-employment services
- vocational rehabilitation training and assistance, including training in the activities of daily living, physical and occupational therapy, use of physical aids or devices, such as artificial limbs or wheelchairs and skills training for the specific type of work (classroom instruction, individual tutoring and simulated work)
- job-seeking skills, such as preparing a résumé or handling job interviews
- placement with an employer and/or on-the-job training
- services to help your family adjust to your disability
- transportation to rehabilitation activities
Eligibility Requirements
You may be eligible if:
- You have a physical or mental condition that makes it difficult for you to work.
- You would be able to return to work after receiving rehabilitation.
- You need these services to be able to prepare for, start or maintain gainful employment.
Applying for Vocational Rehabilitation
You must complete an application and be evaluated for eligibility. You should start rehabilitation as soon as possible, after you are discharged from the hospital to protect your disability coverage. Your transplant social worker can help you apply or you can contact the agency yourself.
Social Security Coverage for the Disabled
The Social Security Administration’s two disability programs, Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI), are for individuals whose medical conditions prevent them from working. Both of these programs should be used as a move towards improving your economic condition.
Social Security Disability Insurance (SSDI)
- covers individuals who are working and paying Social Security taxes
- can be collected while you are involved in an approved rehabilitation program
Supplemental Security Income (SSI)
- makes monthly payments to disabled individuals with few assets and low incomes
- requires no waiting period
Eligibility Requirements
If you are eligible for SSDI or SSI, you may receive benefits until you are able to work again on a regular basis. Certain members of your family may also qualify for benefits.
Under this program:
- You must file a formal application.
- You must be unable to perform any work for which you are qualified.
- Your disability must be expected to last at least a year or result in death.
- You must have earned enough work credits when you were able to work (SSDI only).
- You may file an appeal if you are turned down the first time you apply, but believe that you qualify.
Applying for Disability
Even if another insurer or government agency has ruled that you are disabled, you must still meet Social Security requirements in order to receive Social Security benefits. Contact the Social Security Administration 44) or your transplant financial team to apply for these programs. It is also important to consider the following points when applying:
- Apply as soon as you become disabled.
- You may apply by telephone, mail or in person at any Social Security office.
- Ask your social worker for help in applying.
- You cannot collect benefits until your sixth full month of disability.
- You may be able to qualify retroactively (dating back to the disabling event).
- During the 60 to 90 day claims process, Social Security will be gathering your medical information and assessing your ability to work.
- If you meet the initial requirements for disability, the Social Security office will send your application to your state’s Disability Determination Service for a formal evaluation.
- Reviewers will gather information from your doctors about your medical condition, history and treatment, as well as your ability to perform normal work activities.
- You may need to take a physical examination for further assessment.
- If additional testing is required, Social Security will pay for these expenses.
- You will receive written notice about your claim.
Review Periods and Termination of Benefits
Your case will be reviewed periodically to see if you are still disabled. Your benefits will end if:
- you work on a regular basis and earn an average of $500 or more a month; or
- your medical condition improves and you are no longer considered disabled (unless you are in a vocational rehabilitation program).
Work Incentives
In effort to help you move from dependency on benefits to self-sufficiency, work incentives protect your entitlement to cash payments and/or Medicaid or Medicare protection, until you can support yourself. Also, because you can still receive Social Security benefits if you attempt to work, it is important to call your Social Security Administrator and ask about work incentives and how they affect your benefits. The following points will provide you with a basic overview of work incentives:
- You may work for up to nine “trial” months (when your earnings are more than $200 in one month) over a five-year period. After nine trial months, Social Security will evaluate your work.
- Generally, if your earnings average $500 a month or less, you will continue to receive benefits.
- If you earn more than $500 a month on average, you will receive benefits for three more months.
- If you are still defined as disabled, you may receive a monthly benefit for any month that your earnings fall below $500, for up to 36 months.
- You must make Social Security aware of any special expenses you must pay in order to work. These expenses will be subtracted from your earnings to calculate your monthly earnings. These expenses include things like medications, travel costs related to your job, and some medical costs.
Americans with Disabilities Act
The Americans with Disabilities Act (ADA) of 1990 prohibits discrimination against people with disabilities who wish to work. The Act applies to private companies, state and local governments and employment agencies and labor unions that employ 15 or more workers for more than 20 weeks, but does not cover all employers. The ADA specifically excludes drug and alcohol abuse among the disabilities it covers, but it does protect those who have stopped using illegal drugs and have enrolled in or completed a drug rehabilitation program.
Eligibility Requirements
To be protected under the ADA, you must:
- have a physical or mental impairment that restricts one or more major life activities; and
- be able to perform the essential functions of your current job or a job that your are seeking, either with or without “reasonable” accommodations from your employer.
Employer Responsibilities
Reasonable Accommodations
Employers are required to make reasonable accommodations for disabled workers, such as:
- changing work schedules as necessary
- providing restructured job duties and/or reassigning disabled workers to other positions
- improving access to work facilities for disabled persons
- constructing new devices (such as a wheelchair ramp) or modifying existing ones to assist disabled workers, and
- modifying job examinations, training materials or policies as appropriate
Exceptions
If you have not made your employer aware of your disability, they will be under obligation to accommodate you. Also, employers may not have to provide an accommodation if they can prove it would pose an undue hardship to the business.
Patient Rights
Although pre-employment drug testing is allowed, ADA regulations do not allow an employer to take a medical examination before you are considered for employment. However, the Act does allow a routine medical examination after a job offer has been made and before employment begins for all new employees.
In a job interview, you may only be asked about your disability if the company can prove that the questions relate directly to the necessities of the job and meet certain other considerations.
Filing a Claim
To report a potential ADA violation, contact your local Equal Employment Opportunity Commission office, listed under “United States Government” in the telephone book. By law, an employer cannot retaliate against anyone filing a claim or participating in an investigation.
References [ + ]
{kind=link}