Contents
- Allergic keratoconjunctivitis
- Allergic keratoconjunctivitis types
- Allergic keratoconjunctivitis causes
- Allergic keratoconjunctivitis pathophysiology
- Allergic keratoconjunctivitis signs and symptoms
- Allergic keratoconjunctivitis complications
- Allergic keratoconjunctivitis diagnosis
- Allergic keratoconjunctivitis differential diagnosis
- Allergic keratoconjunctivitis treatment
- Table 1. Allergic conjunctivitis treatment options
- Eye drops for allergic conjunctivitis
- Antihistamine eye drops
- Mast cell stabilizers
- Antihistamine and mast cell stabilizer eye drops
- Dual-Acting Antihistamine–Mast Cell Stabilizing Agents
- Leukotriene Receptor Antagonists
- Topical Vasoconstrictors (Decongestants)
- Combination eye drops including decongestant (Antihistamine-Vasoconstrictor Combinations)
- Topical nonsteroidal anti-inflammatory drugs (NSAIDS)
- Other eye drops, to prevent allergy symptoms
- Oral antihistamines (tablets and syrups)
- Corticosteroids
- Topical Calcineurin inhibitors
- Biologicals
- Immunotherapy
- Surgery
- Allergic conjunctivitis home remedies
- Allergic keratoconjunctivitis prognosis
Allergic keratoconjunctivitis
Allergic keratoconjunctivitis also called allergic conjunctivitis is caused by an allergic reaction, with the majority of cases (90–95%) attributed to seasonal (certain times of the year) allergic conjunctivitis or perennial (all year round) allergic conjunctivitis 1, 2, 3, 4, 5, 6. Allergic conjunctivitis is an inclusive term that encompasses seasonal allergic conjunctivitis (SAC), perennial allergic conjunctivitis (PAC), vernal keratoconjunctivitis (VKC), and atopic keratocongiuntivitis (AKC). However, atopic keratocongiuntivitis (AKC) and vernal keratoconjunctivitis (VKC) have clinical and pathophysiological features quite different from seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC), in spite of some common markers of allergy 7, 3. Also contact lenses or ocular prosthesis associated giant papillary conjunctivitis (GPC) are often included in the group of eye allergy, however they should not be considered as real allergic diseases, but as chronic ocular micro-trauma related disorders, which need to be managed by ophthalmologists in association with contact lenses experts 3, 8.
Allergic conjunctivitis is a common conjunctivitis that is caused by immunoglobulin E (IgE) immune responses or immediate type 1 hypersensitivity immune reactions affecting more than 40% of the general population and is estimated to occur in up to 30% of children, either alone or in association with allergic rhinitis 9, 10, 11, 12, 13. Allergic conjunctivitis is a reaction of the outer lining of the eyeball (conjunctiva) to things in the environment to which a person is allergic (allergens). Dust, pollen, animal dander (skin cells that are shed by animals with hair, fur or feathers), and sometimes even medications can all be allergens. When your eyes are in contact with these allergens, the eyes get red, inflamed, watery, itchy or swollen eyelid 14, 15. Although these symptoms can look like the signs of an infection, allergic conjunctivitis is not an infection and is not contagious. However, these signs and symptoms can be sufficiently bothersome that people with allergic conjunctivitis often experience decreased work productivity, increased work or school absenteeism, limitation of everyday activities, and reduced quality of life 14.
Unlike conjunctivitis that is caused by bacterial or viral infection, allergic keratoconjunctivitis is not contagious, so it cannot be transferred from one person to another.
Allergic keratoconjunctivitis usually affect both eyes and are often accompanied with other signs of hay fever. Allergic keratoconjunctivitis signs can include an itchy, runny nose and sneezing or a history of other allergic conditions. The eyes are itchy (the hallmark of allergic eye disease) and watery 16, 17.
Allergic keratoconjunctivitis other symptoms can include:
- redness behind the eyelid, spreading up the white of the eye
- swelling of the eye/s making them appear puffy
- foreign body sensation
- excessive tears
- serous or mucous discharge
- conjunctival hyperemia (increased amount of blood in the vessels)
- tarsal papillary reaction
- a dislike of bright lights (photophobia).
Allergic keratoconjunctivitis symptoms may be:
- Perennial (all year round) due to constant exposure to dust mites, animal dander, indoor and outdoor mold spores and, in some cases, foods or food additives.
- Seasonal (certain times of the year) due to airborne allergens such as mold spores and pollen from grasses, trees, and weeds. The amount of airborne pollen varies from day to day and is dependent on the weather. People with pollen allergies often find their symptoms improve in wet weather and become worse on hot windy days or after thunderstorms.
If allergic keratoconjunctivitis is suspected, allergy testing can help identify the allergen responsible, or “trigger”.
Avoiding or minimizing exposure to known allergens is an important first step in managing allergic keratoconjunctivitis.
Allergic keratoconjunctivitis may be helped by treatments used in conditions such as hay fever e.g. antihistamines. Cool compresses and lubricating eye drops may soothe the eyes.
Figure 1. Human eye
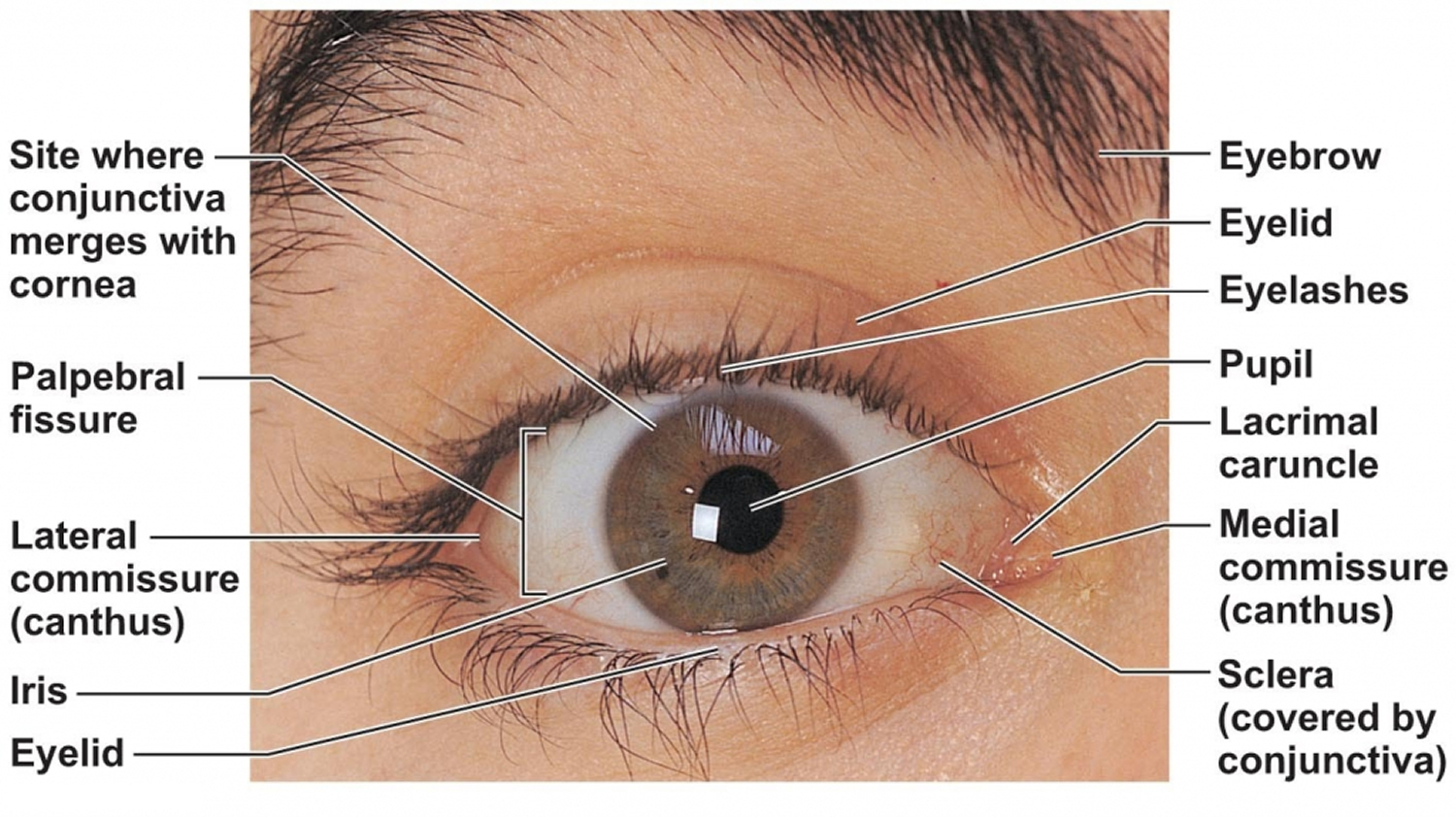
Figure 2. Eye anatomy
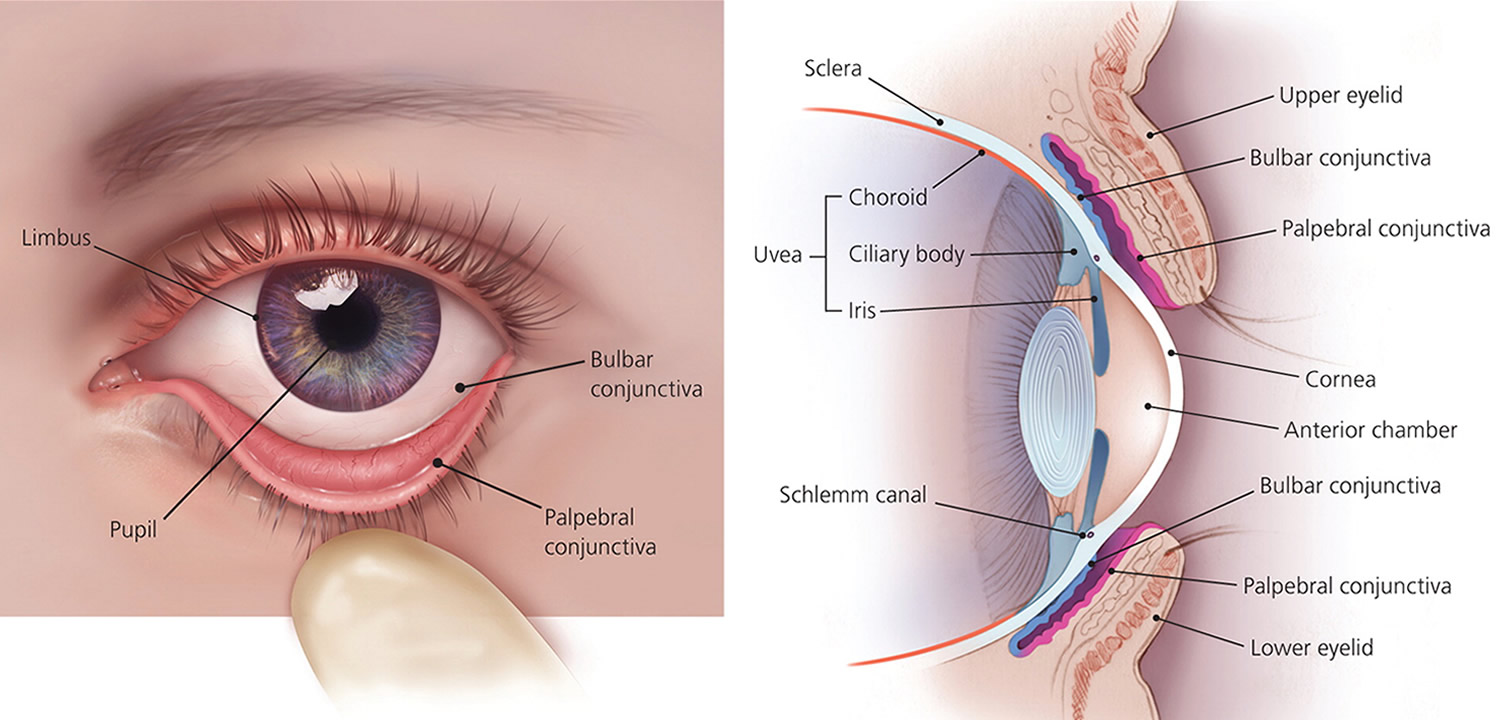
Figure 3. Allergic keratoconjunctivitis
Allergic keratoconjunctivitis types
The classification of allergic eye diseases includes different clinical forms and can be divided into 2 main categories: the most common seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC). The second category includes the less common severe persistent eye allergies namely vernal keratoconjunctivitis (VKC) and allergic keratoconjunctivitis (AKC) 19.
Seasonal allergic conjunctivitis (SAC)
Seasonal allergic conjunctivitis (SAC) also called “hay fever eyes” or “hay fever conjunctivitis” is the most common form of eye allergy and affects all age groups and occurs seasonally when pollen is released during spring and summer seasons in May and June 9, 1, 20, 21. The most common allergens responsible are tree and grass pollens, with the specific allergen varying depending on the geographic location 9, 22. Itching followed by watering and a burning sensation is seen in seasonal allergic conjunctivitis patients. Sometimes, seasonal allergic conjunctivitis may be associated with a running nose (allergic rhinitis or rhinoconjunctivitis). People with seasonal allergic conjunctivitis may complain of sinus pressure behind their eyes.
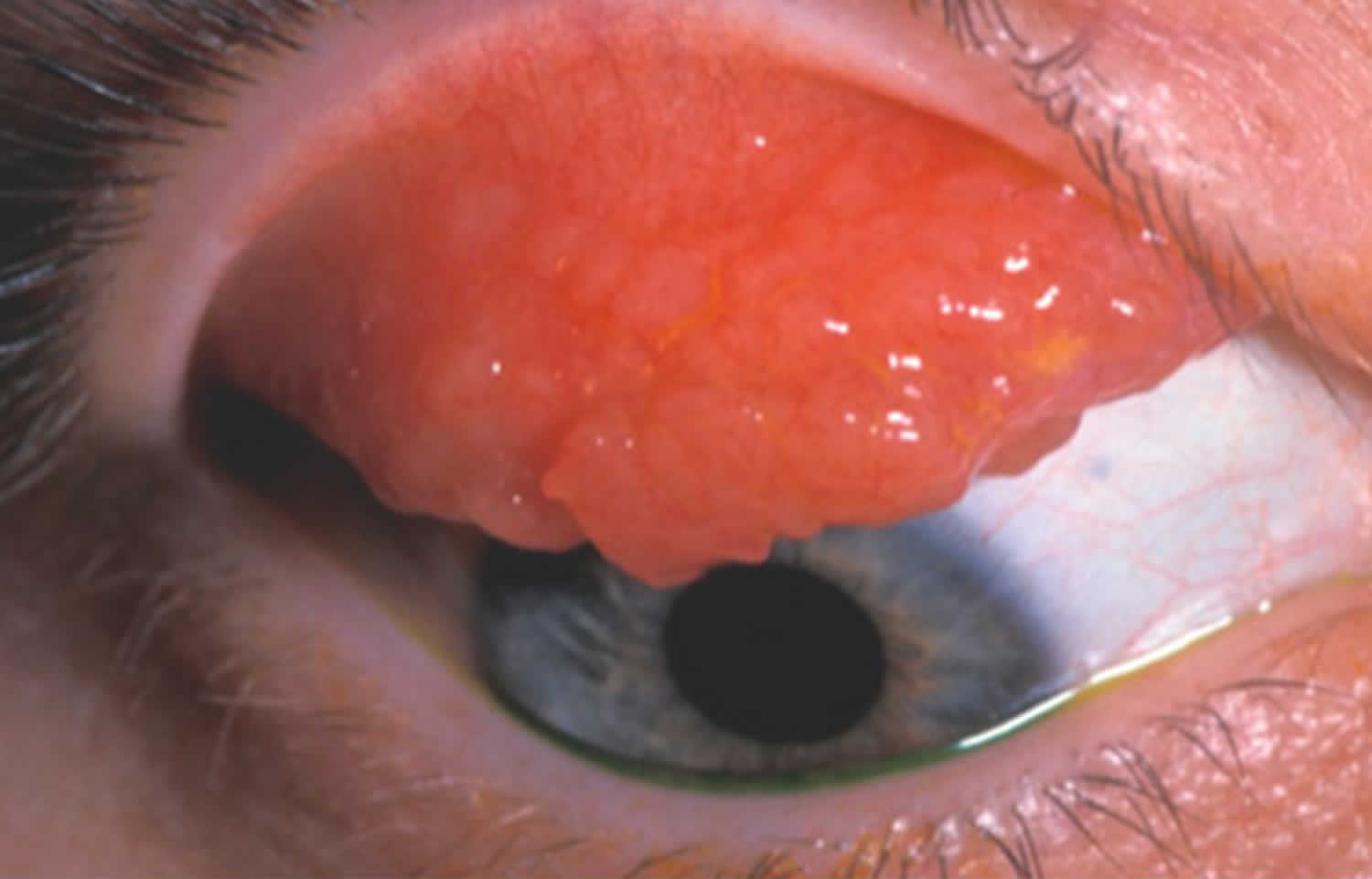
Figure 4. Seasonal and perennial allergic conjunctivitis
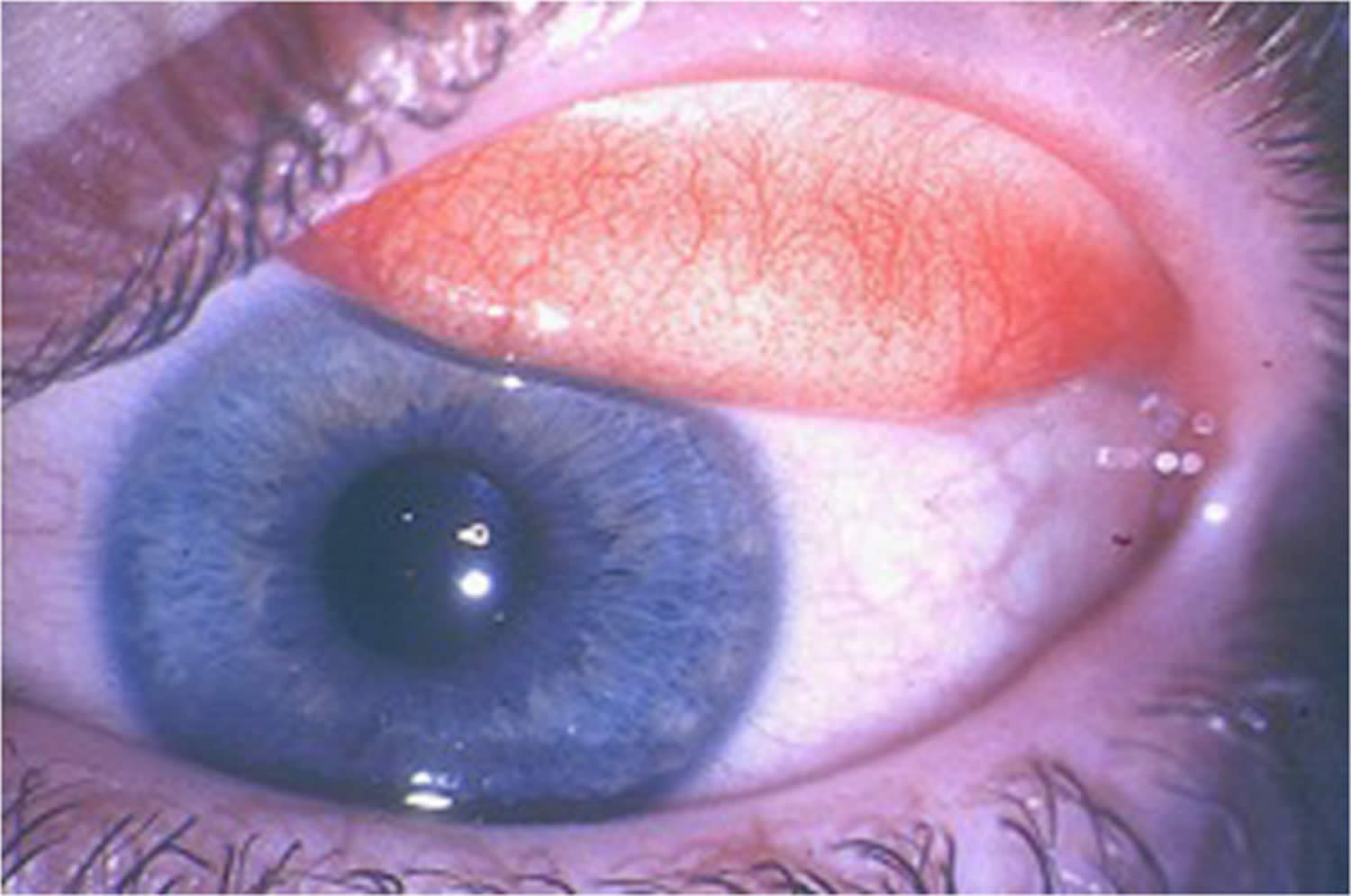
Footnote: Seasonal and perennial allergic conjunctivitis showing mild conjunctival injection and moderate chemosis. Itching is a fairly consistent symptom of seasonal and perennial allergic conjunctivitis. Corneal involvement is rare 23.
[Source 3 ]Perennial allergic conjunctivitis (PAC)
Perennial allergic conjunctivitis (PAC) has similar signs and symptoms to seasonal allergic conjunctivitis (SAC) but is chronic with remission and exacerbation periods and as the name suggests it occurs throughout the year (perennial) and is generally worse in autumn 21, 1. Perennial allergic conjunctivitis occurs due to indoor airborne allergens throughout the year such as allergy to animal dander (skin cells that are shed by animals with hair, fur or feathers), house mites, fungal spores and feathers 21, 1. Compared to the seasonal allergic conjunctivitis (SAC), perennial allergic conjunctivitis is less common and generally milder 24. Perennial allergic conjunctivitis frequency of occurrence increases as the age increases 25. People with perennial allergic conjunctivitis have itching, redness and swelling of conjunctiva. Corneal involvement in seasonal allergic conjunctivitis and perennial allergic conjunctivitis is rare 3.
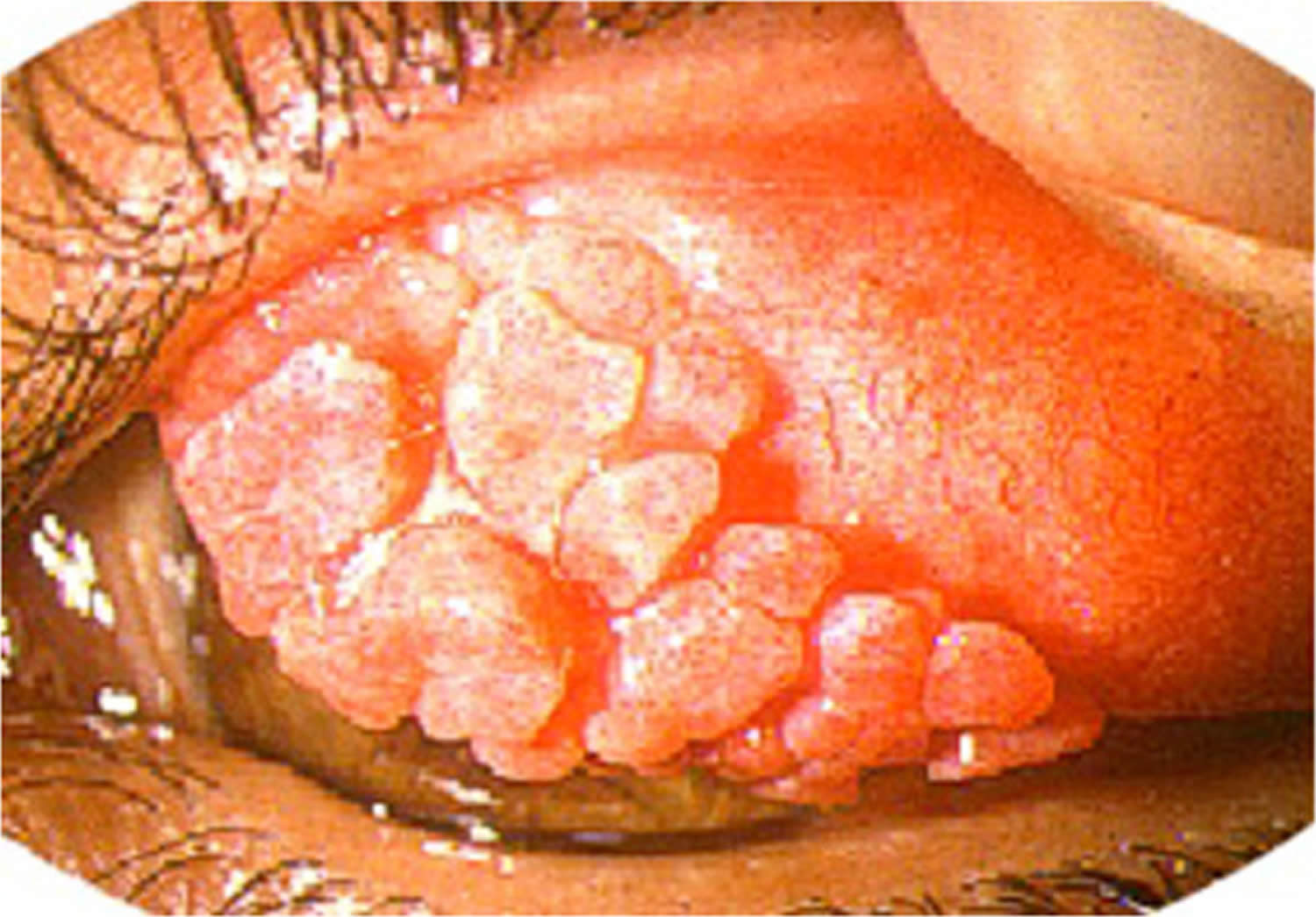
Vernal keratoconjunctivitis (VKC)
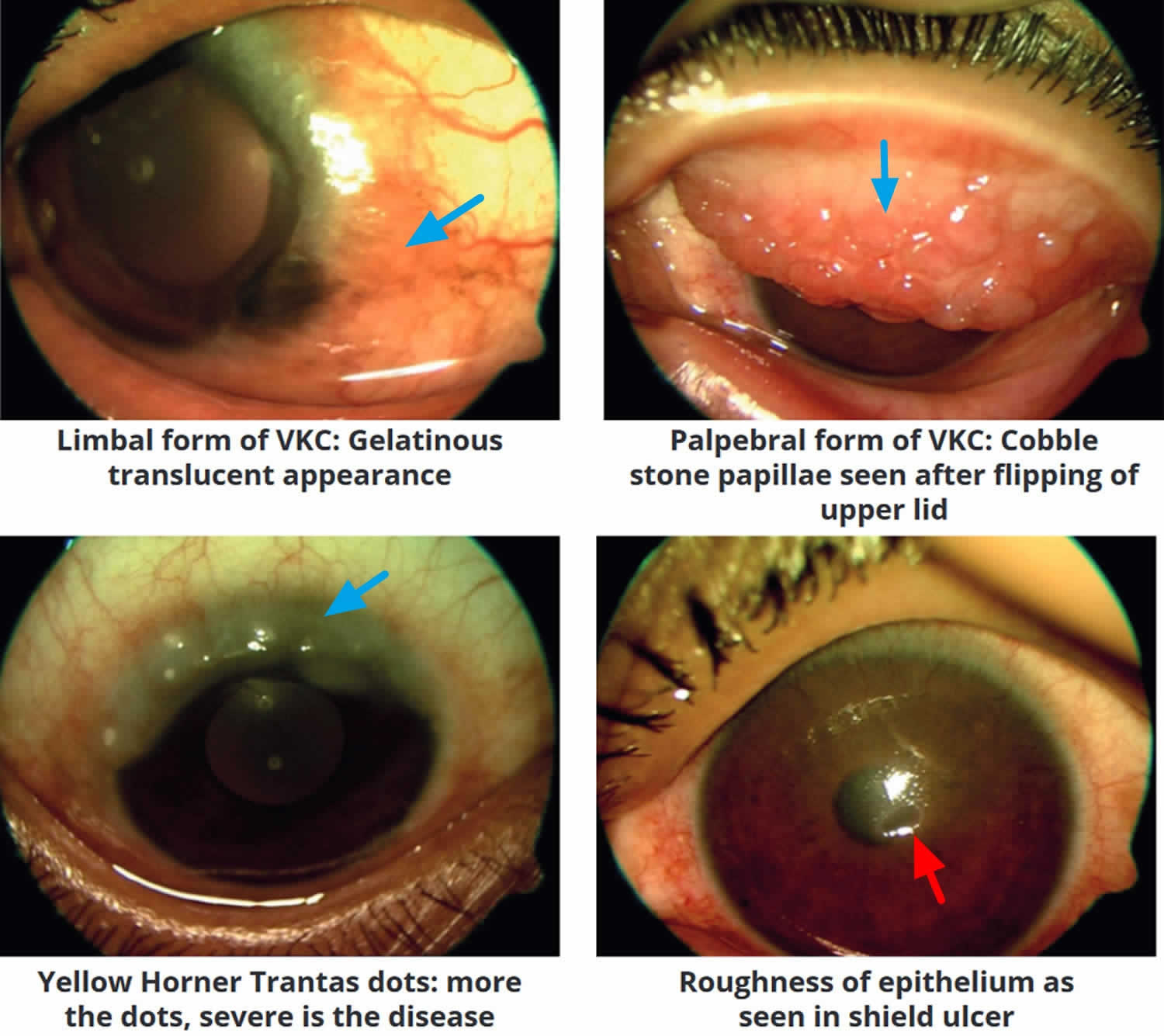
Vernal conjunctivitis also called vernal keratoconjunctivitis is a severe type of seasonal allergic conjunctivitis (SAC) that results in small, raised lumps on the inside of the upper eyelid called Horner Tranta dots and a stringy (ropey), mucus discharge (Figures 5 to 9) 26, 27, 28. Large bumps or papillae on the conjunctiva are a classic sign of vernal conjunctivitis. Histopathology shows eosinophils in the conjunctival secretions. Vernal conjunctivitis is frequently associated with allergic rhinitis, atopic dermatitis, or asthma. Vernal conjunctivitis may be associated with a single allergen but more usually with multiple sensitivities. Vernal conjunctivitis is often seen in areas of the world where the weather is hot and dry than in cold climates, most commonly in Asia, Central and West Africa and South America 29, 30, 31, 32, 33, 28. Vernal conjunctivitis is also seen commonly in the Middle East, Japan, India, the Mediterranean area, North America, and Australia 34, 35. At least one study showed prevalence ranges from 4.0 to 11.1% prevalence of vernal keratoconjunctivitis in African countries schoolchildren 31, 36. Vernal conjunctivitis is thought to be relatively unusual in North America and Western Europe 37, 34. One European study demonstrated the prevalence of vernal conjunctivitis was between 1.2 to 10.6 per 10,000 and 0.8/10,000 with corneal complications has been reported 32. The increased incidence in hot regions is speculated to be secondary to a higher level of pollution by pollens and various other allergens 28.
Vernal conjunctivitis is a T-helper-2 (Th2) lymphocyte-driven disease characterized by infiltration of the conjunctiva by a number of inflammatory cell types, including eosinophils, mast cells, and T lymphocytes 38, 39. This differs from atopic keratoconjunctivitis, which has been shown to involve both Th1 and Th2 inflammatory cascades 40. Increased levels of tumor necrosis factor (TNF) alpha, histamine, tryptase, IgE, and IgG antibodies are observed on pathologic examination of tears 41. It is believed that the exaggerated immunoglobulin E (IgE) response observed with vernal conjunctivitis in response to common allergens may be a secondary event 39. Mast cells and basophils cause the immediate reaction through the release of histamine and the recruitment of inflammatory cells lymphocytes and eosinophils 26. This results in the release of a number of pro-inflammatory cytokines, including but not limited to interleukin (IL)-4, IL-5, and IL-13, as well as other toxic cell mediators such as eosinophil cationic protein, eosinophil-derived neurotoxin/eosinophil protein X (EDN/EPX) that result in corneal damage 39, 42. Release of these factors mediates the remodeling, eye inflammation, and itch that are commonly associated with vernal conjunctivitis.
Vernal conjunctivitis is classified into 3 clinical subtypes based on the location of the papillae into palpebral (tarsal), limbal (bulbar), and mixed forms 38, 43, 26:
- Palpebral vernal conjunctivitis (tarsal vernal conjunctivitis). Palpebral vernal conjunctivitis is characterized by large, cobblestone-like papillae on the upper tarsal conjunctiva. These can differ in shape and size, but are usually defined as >1.0 mm in diameter 44, 38. There is a close association between the inflamed conjunctiva and the corneal epithelium, often leading to significant corneal disease.
- Limbal vernal conjunctivitis (bulbar vernal conjunctivitis). Limbal vernal conjunctivitis typically involves Horner–Trantas dots indicating lymphocytic and eosinophilic infiltration of the limbal conjunctiva 44, 38. Limbal vernal conjunctivitis typically affects the Black and Asian populations.
- Mixed vernal conjunctivitis. Mixed vernal conjunctivitis has features of both the palpebral (tarsal) and limbal (bulbar) subtypes in only one eye (as signs are often heterogeneous between eyes) 44.
According to the Management of Vernal Keratoconjunctivitis in Asia (MOVIA) Expert Working Group, the most common form of vernal conjunctivitis seen in clinics across Asia is the tarsal form; however, up to one-third of patients are assumed to have the mixed form 26. The limbal form of vernal conjunctivitis is considered less common in Asia (based on clinical experience) 26.
Diagnosis and treatment of vernal conjunctivitis is a challenge for many ophthalmologists, since no precise diagnostic criteria have been established, the pathogenesis of the disease is unclear, and anti-allergic treatments are often ineffective in patients with moderate or severe disease 26.
Vernal conjunctivitis usually affects both eyes and is severe, occurring seasonally and mainly in children and more common in young boys than girls, but this difference becomes smaller as age increases 45. Often, patients with vernal conjunctivitis also have asthma or eczema. The majority of vernal conjunctivitis occurs in patients between the ages of 5 to 25 years of age with an age of onset between 10 to 12 years old; however there are reports of patients as young as 5-months-old 35, 46. Symptoms typically occur throughout the year, but are worse in spring (vernal means springtime in Latin) and summer time. 23% of patients may have a perennial (all year round) form of them disease and many may have recurrences outside of the springtime 35, 45. Symptoms can be so bad that children need to be treated with topical (eye drops) or systemic (oral tablets) steroids in addition to allergy eye drops such as topical cromolyn or antihistamine preparations. However, vernal conjunctivitis is more difficult to treat than other types of allergic conjunctivitis, and may need special immune based medications such as cyclosporine drops to control the eye inflammation and prevent other eye problems. Sleeping in an air-conditioned room, ice packs and cold compresses can help with symptom relief. Furthermore, without adequate treatment, the seasonal vernal conjunctivitis can evolve into a chronic perennial vernal conjunctivitis after a mean of 3 years from disease onset 39.
Most vernal conjunctivitis patients eventually do grow out of vernal conjunctivitis usually lasts between five to ten years and usually resolves after puberty or adolescence and is rarely seen after the age of thirty. In contrast, children diagnosed with atopic keratoconjunctivitis will suffer from signs and symptoms throughout their life, and may develop more severe complications, as the atopic keratoconjunctivitis is progressive 47.
Figure 5. Vernal keratoconjunctivitis

Footnote: Large cobblestone papillae. Upper tarsal giant papillae are typical of vernal conjunctivitis. These have characteristically flattened tops which sometimes demonstrate stain with fluorescein. Giant papillae can sometimes be seen near the limbus and, while relatively uncommon, symblepharon formation (an eye condition that causes the conjunctiva of the eye to stick to itself or the cornea) and conjunctival fibrosis (scar) can occur.
[Source 28 ]Figure 6. Horner–Trantas dots

Footnote: Peri-limbal Horner–Trantas dots are focal white dots consisting of degenerated epithelial cells and eosinophils and are indicative of vernal keratoconjunctivitis.
[Source 26 ]Figure 7. Vernal keratoconjunctivitis types
Footnote: Clinical forms of vernal keratoconjunctivitis: Limbal or bulbar, palpebral and mixed vernal keratoconjunctivitis.
[Source 4 ]Figure 8. Palpebral vernal conjunctivitis
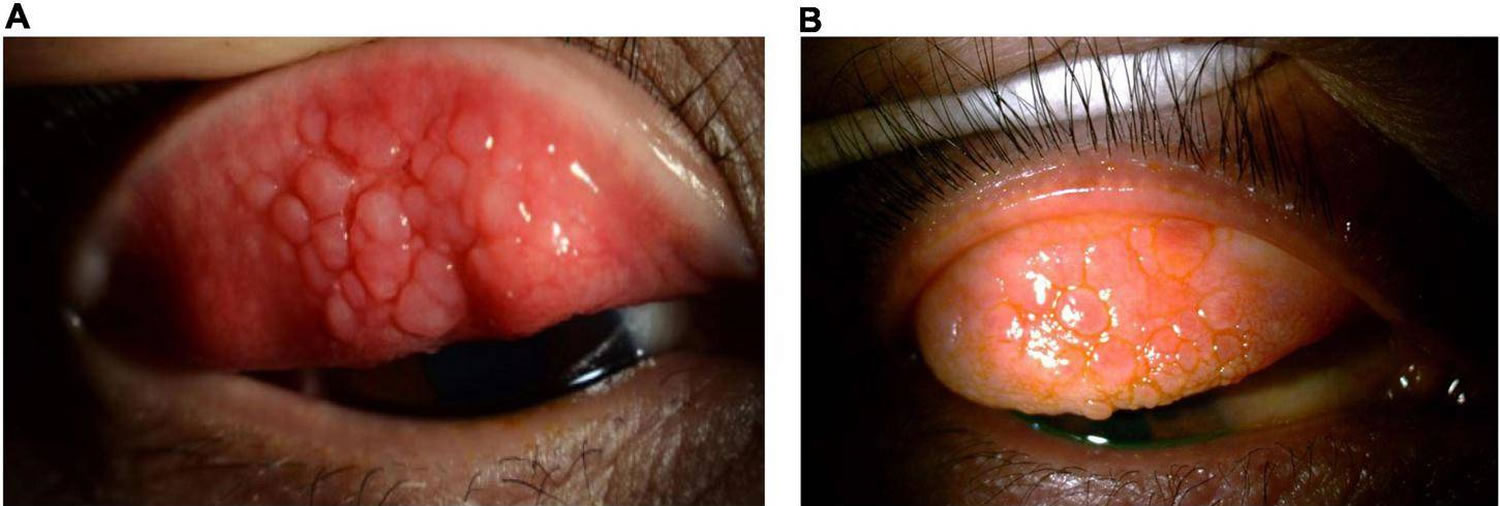
Footnote: Palpebral vernal conjunctivitis also called tarsal vernal conjunctivitis is characterized by large, cobblestone-like papillae on the upper tarsal conjunctiva.
[Source 26 ]Figure 9. Limbal vernal conjunctivitis
Footnote: Limbal vernal conjunctivitis typically involves Horner–Trantas dots, indicating lymphocytic and eosinophilic infiltration of the limbal (bulbar) conjunctiva. The mixed form is characterized by the presence of both tarsal and limbal subtypes in only one eye.
[Source 26 ]Atopic keratoconjunctivitis (AKC)
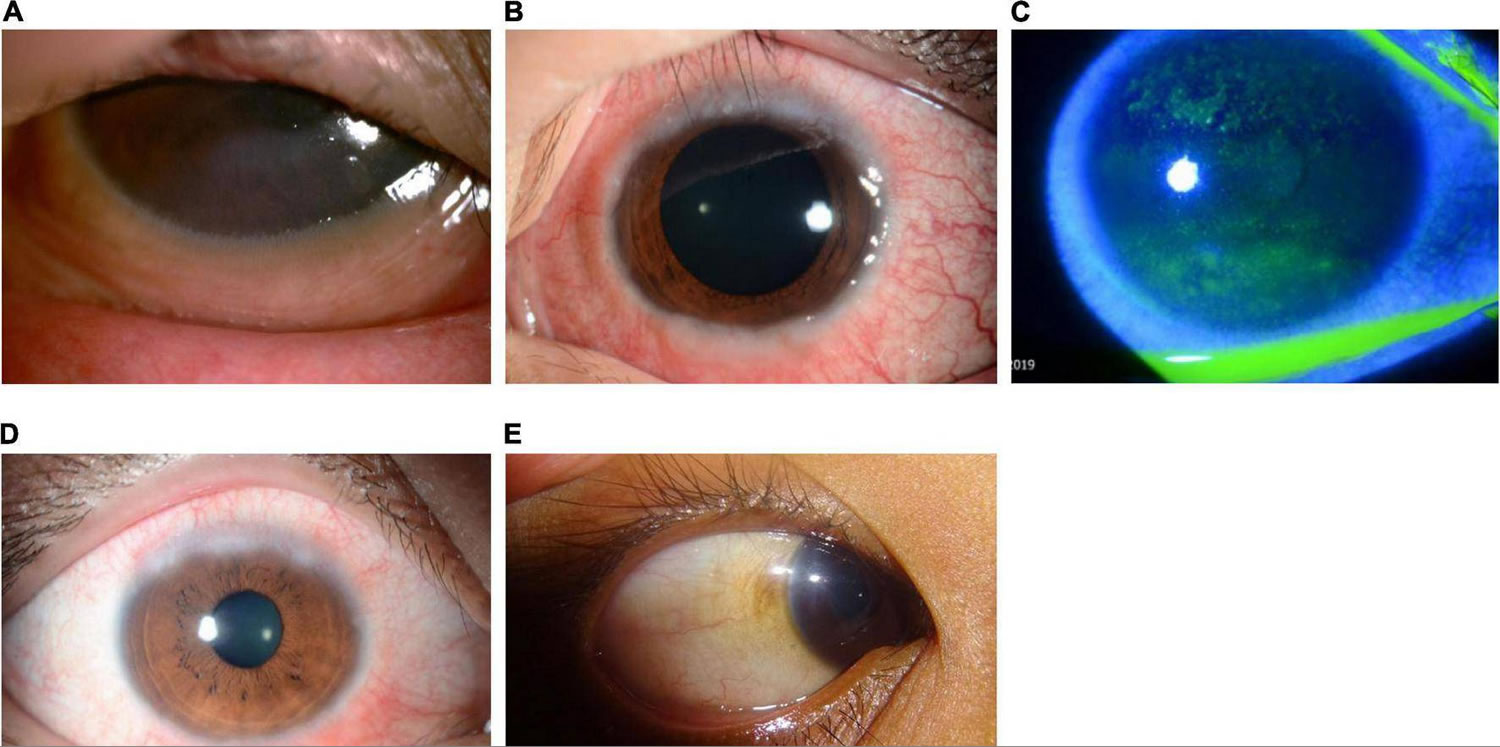
Atopic keratoconjunctivitis also called AKC is the most severe form of chronic allergic conjunctivitis or eye allergic reaction caused by immunoglobulin E (IgE) mediated mechanisms, which has been shown to involve both T-helper-1 (Th1) lymphocyte and T-helper-2 (Th2) lymphocyte inflammatory cascades, and that usually affects people with atopic disease, including atopic dermatitis, eczema, asthma, and food allergies and seasonal allergies, including a family history of allergies and hay fever 48, 49, 50, 51, 40, 52. Atopic keratoconjunctivitis is the chronic eye surface and eyelids (the conjunctiva and cornea) inflammation suffered by patients with atopic dermatitis (eczema). Atopic dermatitis also called atopic eczema, the most common inflammatory skin disease worldwide, presents as generalized skin dryness, itch, and rash 53. Atopic keratoconjunctivitis is the non-infectious inflammation of the conjunctiva (the transparent membrane that lines inside your eyelid and covers the white part of your eyeball) lining your eyelids (palpebral conjunctiva) which is red and swollen. The lower eyelid generally is affected more than the upper eyelid 51. This is a differentiating symptom from vernal keratoconjunctivitis (a severe type of seasonal allergic conjunctivitis) where the upper eyelid is most often affected. Atopy is a genetic condition where your immune system produces higher than normal antibodies in response to a given allergen. Allergic conjunctivitis is caused by contact with something to which a person may be sensitive or allergic to (allergens). However, 45% of the people with atopic keratoconjunctivitis do not display a hypersensitivity reaction to common allergens 54. Conjunctivitis is the inflammation or infection of the conjunctiva, which is the transparent membrane that lines inside your eyelid and covers the white part of your eyeball. The conjunctiva is a thin translucent mucous membrane that can be divided based on the location into palpebral conjunctiva (inside of the eyelids) and bulbar conjunctiva (begins at the edge of the cornea and covers the visible part of the sclera) (Figure 2). The conjunctiva contains nonkeratinizing, squamous epithelium and a thin, richly vascularized substantia propria containing lymphatic vessels and cells, such as lymphocytes, plasma cells, mast cells, and macrophages. The conjunctiva also has accessory lacrimal glands and goblet cells. When the small blood vessels in the conjunctiva become inflamed or infected, they’re more visible. This is what causes the whites of your eyes to appear reddish or pink. Atopic keratoconjunctivitis is a chronic eye surface inflammation with a relatively low expectation of resolution and can have low visual morbidity. If left untreated, atopic keratoconjunctivitis can progress to ulceration, scarring, cataract, keratoconus, and corneal vascularization (the process of growing blood vessels into a tissue).
Although atopic keratoconjunctivitis is a perennial (year round) disease, your symptoms may worsen in the winter. Unlike atopic dermatitis, which is generally seen early in childhood, atopic keratoconjunctivitis appears during late adolescence and early adulthood but may occur at all ages and there is a prevalence peak in patients between 20 and 50 years of age, with a personal or family history of atopic dermatitis or other allergic diseases such as eczema, asthma and/or urticaria 48, 55. The percentage of people with atopic dermatitis that develop atopic keratoconjunctivitis ranges from 25% to 42% 48. Men are more commonly affected than women with a ratio between 2 to 1 and 3 to 1 51. Approximately 5% of atopic keratoconjunctivitis patients have a history of childhood vernal keratoconjunctivitis (a severe type of seasonal allergic conjunctivitis) 1.
People with atopic keratoconjunctivitis usually show atopic dermatitis in the eyelids (see Figure 10A & 11). Eyelid dermatitis results in eyelid hyperpigmentation (panda eyes), swelling that causes horizontal eyelid creases (Dennie-Morgan lines), and absence of the lateral end of the eyebrows (Hertoghe’s sign) 48. More advanced chronic atopic keratoconjunctivitis may also cause keratinization of the eyelid margins, inflammation of the eyelid margins (blepharitis), the loss of eyelashes, and sometimes eyebrows (madarosis), thickening and fissuring of the skin (tylosis), eyelid deformities, and reactive droopy eyelids (ptosis) 48. People with atopic keratoconjunctivitis also show redness of the eyes, chemosis (a swelling of the conjunctiva), and tarsal papillae, typically in the inferior tarsal conjunctiva and sometimes even Horner-Trantas dots in the limbus (Figure 6), especially in more acute phases 48. Conjunctival scarring can lead to conjunctiva of the eyelid to stick to the conjunctiva of the eyeball (symblepharon) and shortening of the inferior conjunctival sac 48. The corneal involvement seems to be secondary to the conjunctival and palpebral involvement and may vary from superficial punctate keratitis to corneal ulcers, corneal scarring, and pannus 48.
People with atopic keratoconjunctivitis complain of severe itching most of the year that is usually more severe during the winter months and in colder climates. There is also discharge that tends to be more aqueous than in vernal keratoconjunctivitis (a severe type of seasonal allergic conjunctivitis), but it may also be mucous 48.
People with atopic keratoconjunctivitis may also complain of dry eyes that exacerbates itchiness and perpetuates conjunctival inflammation 48.
Chronic atopic keratoconjunctivitis leads to numerous complications: infections such as staphylococcal blepharoconjunctivitis and herpes simplex keratitis, cataracts (typically anterior subcapsular but also others), limbal stem-cell deficiency, keratoconus, glaucoma, retinal detachment, and corneoconjunctival tumors 48.
Atopic keratoconjunctivitis usually is diagnosed by clinical exam and a medical and family history, although a conjunctival biopsy may be helpful in distinguishing atopic keratoconjunctivitis from other conditions.
Atopic conjunctivitis treatment is complicated, often requiring input from multiple specialists such as cornea specialist, skin specialist (dermatologist) and doctor specializing in the diagnosis and treatment of allergies (allergist) to determine the most successful management.
The primary goal in managing allergic conjunctivitis, including vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis (AKC), is to avoid exposure to the allergen that triggers the allergic response 56.
If the allergen is known, steps can be taken to minimize exposure to it or, in some cases, get rid of it completely. For example, someone with an allergy to:
- House dust mites may find that minimisation measures such as removing carpet, using dust mite covers for pillows and mattresses, use of hypoallergenic bedding and washing bedding in hot water are enough to reduce symptoms.
- Animal dander may find the best option is to remove the animal or a pet from the house altogether, particularly if symptoms are severe.
- Use of air filtering devices, and dietary changes in cases of food sensitivity.
Mild to moderate symptoms of allergic conjunctivitis usually respond well to simple home treatments such as bathing eyes with cold water, ice packs and cold water compresses. Non-medicated eye drops can also help to lubricate the eye and gently flush allergens from the surface 52, 57, 58. More severe symptoms will usually require treatment with medication.
Figure 10. Atopic keratoconjunctivitis
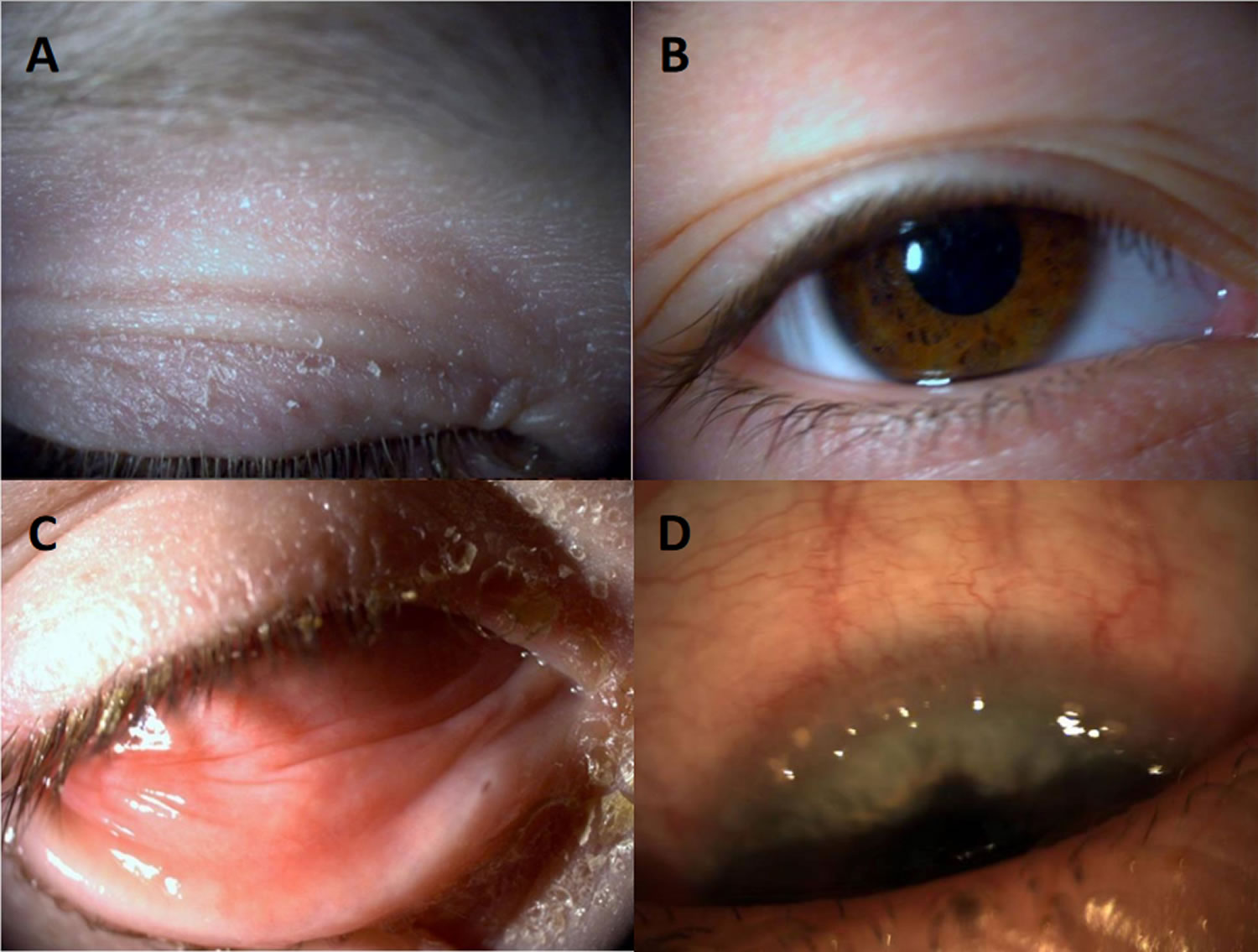
Footnotes: Atopic keratoconjunctivitis. (A) Eczema of the eyelid; (B) Pseudoptosis and Dennie–Morgan double fold of the upper and lower lid; (C) Infiltration of the inferior conjunctiva and blepharitis; (D) Limbal infiltration with Horner–Trantas dots.
[Source 59 ]Figure 11. Eyelid atopic dermatitis

Footnote: Atopic dermatitis of the eyelids in a child with characteristic lichenification (skin thickening, hyperpigmentation and exaggerated skin lines caused by sudden itching and excessive rubbing and scratching) and fine scaling 60.
[Source 53 ]Giant papillary conjunctivitis
Giant papillary conjunctivitis (GPC) is an inflammatory non-infectious disease characterized by papillary hypertrophy of the superior tarsal conjunctiva; the appearance is similar to vernal conjunctivitis (VKC) 61, 62, 63, but there is no significant corneal involvement (Figure 12). However, giant papillary conjunctivitis (GPC) is not truly categorized as an allergic disease but rather presents when the superior palpebral conjunctiva becomes in chronic contact with a foreign body 61, 62. Giant papillary conjunctivitis occurs secondary to direct mechanical irritation or injury, leading to an immune response involving type 1 and type 4 hypersensitivity immune reactions 64. In giant papillary conjunctivitis, the foreign object may become coated with different allergens on their surface or cause injury to ocular structures, enabling deeper allergen exposure, infiltration and triggering an immunological response 65, 66.
Giant papillary conjunctivitis (GPC) can be associated with various eye foreign bodies such as contact lenses, ocular prostheses, exposed suture, cyanoacrylate glue, glaucoma filtering blebs, exposed scleral buckles,and many others 67, 68, 69. Patients typically present with symptoms like an allergic presentation including mucous discharge, tearing, itching, and blurry vision. A key distinguishing factor, though, is complaints of diminished contact lens tolerance and increased lens awareness. Giant papillary conjunctivitis (GPC) is also commonly termed contact lens papillary conjunctivitis with papillae more than 1 mm in size 61.
The pathophysiology of giant papillary conjunctivitis (GPC) is multifactorial and is likely initiated with mechanical damage to the palpebral conjunctiva, leading to innate and adaptive immunity responses 9. It is hypothesized that the proteinaceous debris on the anterior surface of the contact lens acts as a presenting antigen to an IgE-bound mast cell on the conjunctival epithelium 9. Pathological testing indicates that these patients have high amounts of IgE and Ig-G and increased amounts of IL-3 and IL-4. Involved cell mediators include mast cells, basophils, Th2 lymphocytes, and the Th2-derived cytokines that perpetuate the inflammation process 61.
Figure 12. Giant papillary conjunctivitis
Contact blepharoconjunctivitis
Contact blepharoconjunctivitis is a type 4 delayed hypersensitivity immune reaction caused by contact with an allergen that impacts the eyelids and conjunctiva 68. Presenting symptoms typically include itch, red eye, papillary/follicular reaction of the inferior palpebral conjunctiva, punctate keratitis, and dermatitis of the surrounding periocular skin 70, 68. The reaction is a initiated by an exogenous allergen and mediated by Th1- and Th2-lymphocytes that secrete inflammatory cytokines 54, 68. The Th1-lymphocytes release cytokines and chemokines, activating and immigrating more inflammatory cells in the affected region 70, 68. Common allergens include mydriatic drugs, antibiotics, antiviral agents, glaucoma drops, anesthetics, preservatives, and cosmetics. In sensitized individuals, the immune response can take up to 48–72 hours to develop, in contrast to toxic or irritant allergens that can induce an innate immune response within 2–3 hours 68. Identification of the allergen is most important, because treatment starts with avoidance of the allergen and anti-inflammatory therapy 9.
Allergic keratoconjunctivitis causes
Allergic keratoconjunctivitis is caused by contact with something to which a person may be sensitive or allergic to (allergens), air pollution, atopy, pollen exposure, inflammation, and pet hair 1. Examples of common allergens to the conjunctival surface include tree/grass pollen, house dust mites, animal/pest dander, and mold spores 1, 71. Spring, summer and fall allergies tend to be caused by trees weed, grass, and flower pollen. Some people can have allergies all year round due to other household allergens, including dust, mold and animal dander/hair/fur. Some children may have an underlying medical problem making them more at risk for an allergic eye condition.
Allergic keratoconjunctivitis pathophysiology
The eye surface consists of the cornea and the conjunctival mucosal barrier, which protects the eye from foreign invasion and is a common site of allergic inflammation due to its easy access to airborne allergens 72. The ocular surface is blanketed by the tear film, which consists of a lipid, aqueous, and mucin layer formed by the meibomian glands, lacrimal glands, and goblet cells, respectively 73, 74. The tear film plays a vital role in visual acuity. It lubricates and protects the epithelium of the eye surface 75. The eye surface is an “immune-privileged” site as it maintains corneal transparency and integrity by suppressing unnecessary inflammatory responses while maintaining the capability to mount an effective immune response against pathogens 72, 76, 77. The cornea has no blood vessel and has no lymphatic drainage; therefore, no active blood-circulating leukocytes can enter or collect in the corneal tissue 76, 78. The healthy cornea also does not have any mature leukocytes, which decreases its ability to produce pro-inflammatory cytokines and are limited in their ability to produce lymphoid cells 79, 80:S49–S54. doi: 10.1097/ICO.0000000000001005)). The cornea is kept clear by producing anti-inflammatory cells such as regulatory T cells, IgA-producing plasma cells, and immunosuppressive cytokines 81, 82, 83.
Unlike the cornea, the conjunctiva harbors a diverse group of immune cells (primarily T cells) during its steady state. The conjunctival epithelial consists of goblet cells, CD8+T cells, and Langerhans cells, and the subepithelial layer of the conjunctiva consists of blood vessels, lymphatics, macrophages, dendritic cells, fibroblasts, and mast cells 81, 82, 83. This distribution of immune cells in the conjunctival mucosa is known as the conjunctival-associated lymphoid tissue (CALT) 82, 84. The conjunctival-associated lymphoid tissue (CALT) consists of conjunctival lymphoid follicles and diffuse lymphoid effector tissue. Conjunctival lymphoid follicles consist of B cells and T cells, whereas diffuse lymphoid effector tissue consists of mast cells, macrophages, IgA-secreting plasma cells, and effector T cells 85, 86:S180–S186. doi: 10.1016/S1542-0124(12)70251-3)), 87.
The major effector cell responsible for the majority of allergic inflammation responses is the mast cell 75, 81. In the acute phase, the cross-linking of IgE on the surface of mast cells releases preformed mediators of histamine, tryptases and leukotrienes, which play a major role in the clinical symptoms associated with allergy 88. The late phase is characterized by the release of various chemokines and inflammatory proteins and the infiltration of eosinophils, basophils, T cells, neutrophils, and macrophages that lead to further conjunctival inflammation 75, 89.
The conjunctival epithelial has tight junctions that prevent allergens from gaining access to the subepithelial layer 90, 91. In allergic conjunctivitis, this barrier function is compromised due to the activation of the protease-activating receptor 90, 92:17–21. doi: 10.1111/j.1365-2249.2008.03716.x)). This leads to the release of cytokines, chemokines, and adhesion molecules as part of the allergen-included immune response 86:S180–S186. doi: 10.1016/S1542-0124(12)70251-3)). These mediators are released by the conjunctival epithelial cells and encourage the influx of more immune cells to the site of inflammation 90, 92:17–21. doi: 10.1111/j.1365-2249.2008.03716.x)).
The immunopathogenic mechanisms of seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC) are usually type-1 hypersensitivity, IgE-mediated responses involving mast cells, whereas, in chronic allergic disorders like vernal keratoconjunctivitis (VKC) or atopic keratocongiuntivitis (AKC), the mechanisms are complex, including both IgE- and T-cell-mediated responses.
The immunological response to eye allergy can be broken down into three phases: sensitization, the early/acute phase, and the late/chronic phase 9.
Figure 13. Allergic keratoconjunctivitis pathophysiology
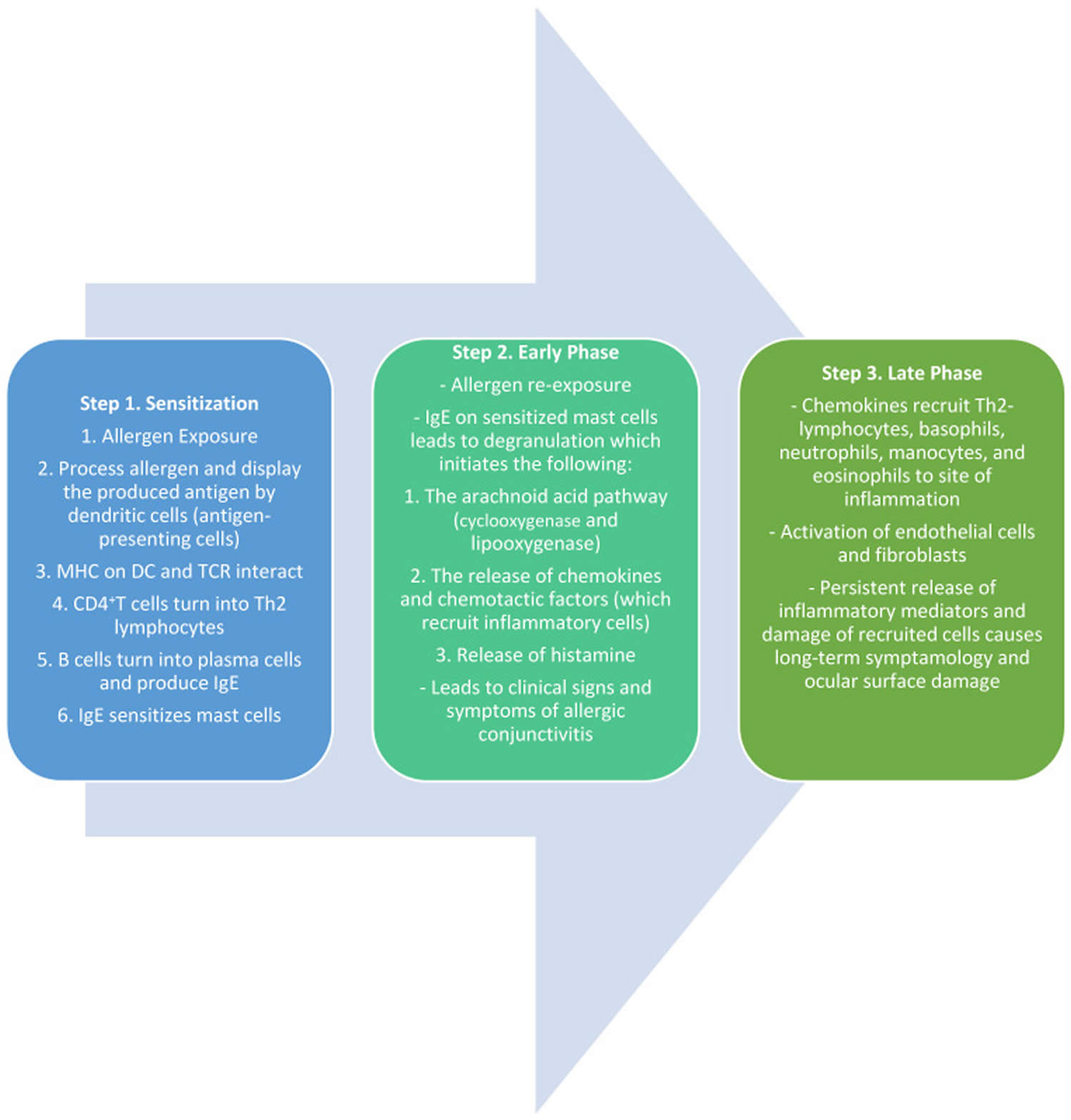
Abbreviations: APCs = antigen-presenting cells; MHC = major histocompatibility complex; DC = dendritic cell; TCR = T-cell receptor; Th2 = T Helper type 2
[Source 9 ]Sensitization
The first phase of the IgE-mediated immune response is sensitization 93. This phase defines the initial exposure of the allergen to the conjunctival mucosa. Once an allergen is deposited on the conjunctiva, it is processed and cleaved into peptide fragments by the Langerhans cells, dendritic cells, and other antigen-presenting cells (APCs) on the mucosal epithelium 93, 94. These peptide fragments are displayed on the surface of the APCs by major histocompatibility complex (MHC) class II molecules 94. The peptide/MHC II complex interacts with the T-cell receptor (TCR) on naïve CD4+T-lymphocytes. In conjunction with other co-stimulatory molecules, the MCH-TCR interaction activates the CD4+T-lymphocytes into T Helper type 2 (Th2) lymphocytes 93, 94. The Th2 lymphocytes then interact with B-lymphocytes, which trigger the release of Th2-lymphocyte-mediated cytokines (IL-3, IL-4, IL-5, IL-6, IL-10, and IL-13) 94. The release of IL-4 and other accessory molecules leads to the conversion of B-lymphocytes into antibody-producing plasma cells. These plasma cells undergo immunoglobulin class switching, which leads to the production of antigen-specific IgE. These IgE antibodies are now specific to the initial allergen and prime mast cells and basophils by binding to their surface receptors. These cells are now ready for subsequent exposure to allergens and mark the completion of the process of sensitization 93, 94.
Early Phase
Once an allergen is re-presented to sensitized mast cells, an allergic reaction is initiated. The natural environmental allergen binds to the IgE molecules on the mast cell receptors, leading to the cross-linking of molecules and subsequently signaling the degranulation of mast cells 93, 94, 95. The activation and degranulation of mast cells lead to a cascade of events, including the activation of the arachnoid acid pathway, the release of chemokines (such as eotaxin), and the release of preformed mediators such as histamine and tryptase. This marks the initiation of the early phase of allergic conjunctivitis. The increased levels of histamine cause the dilation of blood vessels, the stimulation of nerve endings, and the activation of mucous-producing cells, leading to the clinical manifestations of an ocular allergic reaction 94, 95. The presenting signs and symptoms include itching (a hallmark sign of ocular allergy), hyperemia, chemosis (a condition where the conjunctiva, or the outer surface of the eye, swells due to fluid build-up), tearing, mucus discharge, and eyelid swelling 93, 94, 95. The mast cell degranulation also leads to the activation of vascular endothelial cells and the release of adhesion molecules, chemokines, and cytokines 93, 94, 95. This also leads to the biosynthesis of lipid mediators such as prostaglandins and leukotrienes, resulting in the recruitment of inflammatory cells into the conjunctival mucosa and initiating the late phase of the allergic reaction 94.
Late Phase
The late phase of the allergic response typically occurs about 6–12 h after the initial exposure. The release of chemokine factors from the early phase is responsible for the recruitment and infiltration of eosinophils, basophils, neutrophils, Th2 lymphocytes, and monocytes into the conjunctiva 93, 94. This phase also includes the maturation of Th2 lymphocytes and the production and release of Th2-mediated cytokines such as IL-4, IL-5, and IL-13. IL-4 and IL-13 play an active role in the formation of giant papillae by stimulating conjunctival fibroblasts and overexpressing IgE 93, 94, 67, 96. IL-5 recruits and activates eosinophils which leads to continued inflammation, persistent symptoms, and an increased likelihood of long-term tissue damage, as seen in vernal keratoconjunctivitis (VKC) 94, 67.
Allergic keratoconjunctivitis signs and symptoms
Allergic keratoconjunctivitis symptoms may vary from person to person. Allergic keratoconjunctivitis symptoms can be very mild or very severe. Itching is the most common symptom and eye allergy is unlikely to be present if itching is not present. Other symptoms may include stinging, tearing, and burning. The conjunctiva is usually pink and/or bloodshot. The white area immediately around the colored part of the eyes can also swell, causing tiny bumps visible on the surface of the eye. Eyelid skin can also be affected, becoming thick, swollen, itchy, or red. Children may frequently rub or roll their eyes if they have allergies. They may even tightly squeeze or blink frequently to help with the itchiness. Symptoms are often worse in the spring and/or summer months, but may stick around throughout the year.
Typical signs and symptoms of allergic keratoconjunctivitis include:
- Redness in both eyes.
- Itching and burning of both the eye and surrounding tissues.
- Watery discharge, often accompanied by acute discomfort in bright light (photophobia).
- Swollen eyelids which may become ‘heavy’ or ‘droopy’. In some severe cases, the eyelids are so swollen that they cannot completely open.
- Swollen conjunctiva which may look light purple and affect vision. Blurred vision or any change in the appearance of the cornea (clear part of the eye that covers the pupil) requires urgent referral to an eye specialist. Speak to your doctor or optometrist for a referral.
Allergic keratoconjunctivitis complications
In most cases, allergic keratoconjunctivitis is not a severe health threat, but a common and often benign condition. Most often, allergic keratoconjunctivitis complications are because of poor compliance to treatment on the part of patient, or inadequate control of the disease when it presents in its severe form 24. Common complications include dry eye, infection and corneal scar 24. Chronicity of the untreated disease may lead to vision threatening problems like limbal stem cell deficiency (LSCD) and secondary keratoconus due to rubbing of the eyes 24.
As the treatment involves use of corticosteroids, steroid-induced raised intraocular pressure and cataract have been reported in these patients 97. Complications may lead to irreversible visual loss in some patients 97. Both keratoconus and limbal stem cell deficiency need timely surgical treatment to prevent visual malfunction 24.
Complications of allergic keratoconjunctivitis are rare, but when they do occur, they can be severe and may include 1:
- Scarring of the eye (severe cases).
- Progression to infective conjunctivitis, leading to the spread of infection to other areas of the body and potentially causing serious secondary infections.
- Conjunctival scarring
- Bacterial keratitis
- Corneal neovascularization
- Pannus
- Giant papillae
- Nonresolving epithelial defect
- Shield ulcer
- Steroid-induced glaucoma
- Dry eyes
- Keratoconus
- Herpetic keratitis
Allergic keratoconjunctivitis diagnosis
A diagnosis of allergic keratoconjunctivitis is made by history and examination. Although allergy testing may help pinpoint the specific allergens, it is usually not necessary since the types of allergens that usually cause conjunctivitis are very common, like grass, weed, and tree pollens. Eye drop treatments are the same no matter what allergen is causing the reaction.
If further investigation is needed, even if no identifiable allergens have been found, the second step is skin prick or patch tests 17. Patch tests are preferred in contact blepharoconjunctivitis, while skin prick tests are used in the other diseases 17. These tests are carried out with a standard battery of allergens and sometimes with others that are not normally tested but suspected as the cause of the allergy. If skin testing is indicated but not recommended (e.g., the patient is taking antihistaminic systemic medications), or if results are ambiguous (e.g., presence of dermatographism), or simply to complement the results of previous skin prick test, serum specific IgE measurements for the aeroallergens can be considered 98, 52.
In case of doubt after systemic allergy evaluation tests, a conjunctival allergen provocation test (CAPT) also known as conjunctival allergen challenge or ocular challenge test may be of use to identify the cause 52. In the conjunctival allergen provocation test (CAPT) an allergen is applied to the conjunctival mucosa to evaluate the patients’ immunoreactivity to the allergen. The conjunctival allergen provocation test (CAPT) is used to confirm which allergens the patient is sensitive to and has the same scientific background as other provocation tests used extensively in other mucosae such as nasal or digestive 52, 99. Non-specific or irritant challenges evaluate the hyperreactivity of the ocular mucosa, whilst direct mucosal challenges contain higher concentrations of the allergen encountered in environmental exposure and evaluate patients’ immunoreactivity to the allergen, following the guidelines for standard practice of the European Academy of Allergy and Clinical Immunology 52, 99, 57. A positive test will trigger the same signs and symptoms as those occurring when the allergen is encountered in real life, an IgE-mast cell-dependent immunoreactivity 100, 99. The conjunctival allergen provocation test (CAPT) is also useful to assess the relationship between symptoms and exposure in polysensitized patients and to assess response to therapy 98.
Allergic keratoconjunctivitis differential diagnosis
The differential diagnosis for allergic keratoconjunctivitis can be broad and may include the following conditions 1:
- Viral conjunctivitis
- Bacterial conjunctivitis
- Molluscum conjunctivitis
- Giant fornix syndrome
- Adult chlamydial conjunctivitis
- Trachoma
- Neonatal conjunctivitis
- Nonallergic eosinophilic conjunctivitis
- Contact allergic blepharoconjunctivitis
- Mucous membrane pemphigoid
- Stevens-Johnson syndrome/toxic epidermal necrolysis (Lyell syndrome)
- Superior limbic keratoconjunctivitis
- Ligneous conjunctivitis
- Parinaud oculoglandular syndrome
- Factitious conjunctivitis
Allergic keratoconjunctivitis treatment
Allergen avoidance is the first line of treatment for allergic keratoconjunctivitis 101, 102, 103. In the case of pollen allergies, symptoms are often made worse by outdoor activities. Wearing glasses or goggles outdoors can limit contact with allergens. Minimization measures for house dust mites may include removing carpet, using dust mite covers for pillows and mattresses, and washing bedding in hot water are enough to reduce symptoms. Frequent washing of pillowcases and mattress covers as well as vacuuming the carpeting in your room help remove allergens from your surroundings. Regular washing your hair and face can help remove these allergens from the surface of your eyes, hair, and skin. Animal dander can be reduced by keeping animals outside, avoiding touching them or rubbing your eyes after exposure, and washing your hands/clothes after coming in contact 101, 102. Using artificial tear drops to rinse the eye and remove allergens from the eye can help with symptoms and help calm down the eye inflammation. These drops can provide even more relief when used cold (refrigerated) instead of at room temperature. Other non-pharmacological interventions include using cool compresses to decrease eye swelling and redness in irritated eyes. It is also important to avoid rubbing the eyes, as this can make allergic conjunctivitis worse.
If you have allergic keratoconjunctivitis, both prescription and over-the-counter allergy eye drops can treat allergic keratoconjunctivitis 104. These may include medicines that help control allergic reactions, such as antihistamines and mast cell stabilizers. Or your doctor may recommend medicines to help control inflammation, such as decongestants, steroids and anti-inflammatory drops. Nonprescription versions of these medicines also may be effective. Most of the easily available allergy eye drops work best when used daily for at least a few weeks, and it may take up to a week to get full symptom relief. Some eye drops can be used only on an as needed basis. Allergy eye drops may work better for some than pill or liquid medications as eye drops do not cause any drowsiness or changes in appetite. However, pill or liquid medications may be more helpful if allergies cause a lot of eyelid swelling or affect more than just the eyes. Please speak with your ophthalmologist if you have questions about allergy medications.
Given the different types of over-the-counter eye drops, sometimes what works well for one person may not work as well for another person. You may need to try different types of eye drops before you find one that works for you. If there are still allergic conjunctivitis symptoms even after trying different kinds of allergy eye drops, adding a short-term liquid or pill allergy medication by mouth may help relieve symptoms. Pills and liquid medications by mouth may also a good treatment for people who don’t do well eye drops, or who have other allergy symptoms like a runny nose.
In some cases, steroid eye drops may be needed along with allergy eye drops if the allergic reaction is very severe. However, steroid use needs to be monitored closely by your ophthalmologist and used only as directed to prevent serious eye problems. Use of steroid drops for a long time or at a large amount can cause serious vision problems, including glaucoma, cataracts and eye infections (keratitis). Only ophthalmologists (eye specialists) who can monitor for side effects should prescribe steroids for allergic conjunctivitis. Talk with your ophthalmologist if you have questions about steroid drops.
Topical medications (eye drops) treat the symptoms of allergic keratoconjunctivitis directly. Small drops of medication are delivered straight to the surface of the eye and are available in many different types.
- Antihistamine eye drops – effective but should not be used for longer than 6 weeks without medical advice.
- Antihistamine eye drops containing a vasoconstrictor (substances that cause the walls of blood vessels to narrow, or constrict) – minimize itch and remove redness by narrowing the swollen blood vessels in the eye. They should not be used for longer than 14 days without medical advice.
- Mast cell stabilizer eye drops – best used to prevent symptoms from occurring as they can take three to seven days to work. These can be used as long as necessary.
- Mast cell stabilizer eye drops with antihistamines – fast acting, effective and generally well tolerated.
- Steroid eye drops – effective in relieving symptoms quickly, but are associated with cataract formation, glaucoma and bacterial and viral infections of the cornea and conjunctiva. They should only be used under medical supervision as a short-term treatment and should never be used in the presence of herpes infections.
Antihistamine tablets or syrups help some people when it is difficult to avoid the allergen. Some side effects may include dryness of the eyes, nose, and mouth, and blurred vision. Antihistamines are usually contraindicated for people with glaucoma, advice should be sought from an eye specialist.
Allergen immunotherapy for specific allergens may benefit people with persistent, severe allergic conjunctivitis. However, relief of allergic conjunctivitis symptoms will not happen straight away.
Table 1. Allergic conjunctivitis treatment options
| Drug Class | Mechanism of Action | Common Examples | Eye Side Effects |
|---|---|---|---|
| Vasoconstrictors (Decongestants) | a-adrenergic agonists (mainly stimulation of a-1 receptors) | Phenylephrine, Brimonidine, Ephedrine, Naphazoline, Tetrahydrozoline | Rebound redness, conjunctivitis medicamentosa |
| Antihistamines | Competitive blockage of histamine receptors (all block H1 with some blocking H2, H3 and/or H4) | Levocabastine, Emedastine | Dryness, irritation |
| Mast Cell Stabilizers | Inhibit degranulation of mast cell and consequent histamine release | Sodium cromoglycate, Nedocromil sodium, Pemirolast, Lodoxamide | Stinging, Burning |
| Dual-Acting Agents | Inverse agonists of histamine receptors and prevent mast cell degranulation | Olopatadine, Ketotifen, Azelastine Epinastine, Alcaftadine | Burning, headache, dry eye |
| NSAIDS | Inhibits cyclooxygenase enzymes (COX-1 and COX-2) resulting in inhibition of prostaglandins | Ketorolac, Diclofenac Flurbiprofen | Stinging, burning, corneal melt |
| Corticosteroids | Inhibits phospholipase A resulting in the inhibition of prostaglandins and leukotriene synthesis | Dexamethasone, Prednisolone, Loteprednol, Fluorometholone, Rimexalone | Increased intraocular pressure, cataract formation, delayed wound healing |
| Immunomodulators | Cyclosporin A, Tacrolimus | Inhibiting production of IL-2 resulting in inhibition of T-cell activation | Burning, irritation |
Eye drops for allergic conjunctivitis
When you have an allergic reaction your body releases histamine from mast cells, which leads to hay fever. Antihistamines block this reaction. Antihistamines act via histamine receptor antagonism to block the inflammatory effects of histamine and relieve any associated signs and symptoms. Most antihistamines used in the treatment of eye allergy are histamine-1 (H1) receptor antagonists, although some agents have affinity for other subtypes. Histamine-2 (H2) antagonists have been shown to modulate both cell growth and migration. Animal model studies have shown that antihistamines may even reduce infiltration of eosinophils and thus reduce the clinical aspects of the late-phase reaction 44.
First-generation antihistamines are well tolerated and associated with a favorable long-term safety record, but are associated with instillation pain, short duration of action, and limited potency 105. First-generation antihistamines remain available in over-the-counter products, particularly in combination with vasoconstrictors (substances that cause the walls of blood vessels to narrow, or constrict). While newer antihistamines are also H1 antagonists, they have a longer duration of action (4–6 hours) and are better tolerated than their predecessors 44.
Topical antihistamines are widely available without a prescription. Antihistamines competitively block histamine receptors (e.g., H1 or H4) on nerve endings and blood vessels of the mucosal surface, thereby reducing itchiness and conjunctival redness 106. First-generation antihistamines were associated with a range of systemic side effects (e.g., sedation, dizziness, cognitive impairment, blurred vision) caused by anticholinergic actions and nonspecific binding to histamine H2 receptors in addition to drying of the ocular surface. Newer oral, intranasal, and topical ocular antihistamines demonstrate improved H1 receptor selectivity, with fewer adverse effects; however, eye side effects, such as burning and dryness, remain a concern. Topical antihistamines (e.g., levocabastine, emedastine difumarate) are useful for providing rapid relief of allergic conjunctivitis symptoms, but their duration of action is limited; most topical antihistamines require dosing four times.
Antihistamine eye drops
Antihistamines are competitive antagonists of histamine receptors that are present in the conjunctiva and eyelids. Once stimulated, histamine receptors lead to capillary dilation and increased vascular permeability, which leads to common allergic symptoms of itching and edema. Therefore, antihistamines work by preventing the binding of histamine to histamine-1 (H1) receptors and preventing the cascade of inflammatory events. In the eye, only H1 receptors are available 107. Examples include azelastine (Eyezep Eye Drops), levocabastine (Livostin Eye Drops, Zyrtec Levocabastine Eye Drops) and emedastine.
Mast cell stabilizers
Mast cell stabilizers work by preventing the degranulation of sensitized mast cells, thus stopping the release of histamine and other inflammatory mediators 101, 108. Since mast cell stabilizers act before the mast cell is degranulated, they rarely have an impact on the inflammatory mediators once they are already released 109, 108. In other words, mast cell stabilizers are not effective once the patient is symptomatic, and clinical trials have had a difficult time showing their efficacy 109. Since there are other quicker and more effective treatment agents available on the market, mast cell stabilizers are rarely used as monotherapy. The most common mast cell stabilizers used for allergic conjunctivitis are sodium lodoxamide 0.1% (Alomide), cromoglycate 2%, and nedocromil 2% 101, 103. Mast cell stabilizers can be used as a prophylactic measure to prevent mast cell degranulation for repeated exposures to the allergen 67.
Antihistamine and mast cell stabilizer eye drops
When you have an allergic reaction your body releases histamine from mast cells, which leads to hay fever. Mast cell stabilizer medicines help reduce this histamine release after allergen exposure and reduce allergic reactions and hayfever 110. Topical mast cell stabilizers act to prevent mast cell degranulation and subsequent release of proinflammatory molecules triggered by IgE binding to sensitized conjunctival mast cells. Topical mast cell stabilizers (e.g., cromolyn sodium, lodoxamide tromethamine, nedocromil sodium, pemirolast potassium) effectively prevent activation of the early phase response by preventing release of histamine, cytokines, and other inflammatory and chemotactic mediators. Preventing the early phase response blocks downstream inflammation events, including production of prostaglandins and leukotrienes, eosinophil infiltration, chemokine and adhesion molecule expression, and chronic mast cell activation that perpetuate the late-phase response in allergic conjunctivitis. Most mast cell stabilizers require administration four to six times daily; nedocromil sodium can be given twice daily. Because of the required loading time for maximal efficacy of mast cell stabilizers, these medications are most effective when treatment is initiated before symptoms manifest; their effectiveness is limited when allergic conjunctivitis cascades have been activated and mast cell degranulation and histamine release have already occurred.
Dual-Acting Antihistamine–Mast Cell Stabilizing Agents
Agents with dual antihistamine and mast cell stabilizing actions are more suitable for extant allergic conjunctivitis than single-action medications because they block binding of free histamine to receptors and inhibit further release of proinflammatory mediators from mast cells. This dual action rapidly alleviates multiple signs and symptoms of allergic conjunctivitis in the short term and blocks the feed-forward cycle of persistent inflammation caused by continuous mast cell activation in the long term to promote regression of allergic conjunctivitis. Antihistamine–mast cell stabilizing agents (e.g., olopatadine, alcaftadine, epinastine, bepotastine besilate) are currently considered first-line therapeutics for allergic conjunctivitis because they offer acute symptomatic relief and control inflammation, and can be used chronically without long-term safety concerns. Most dual-acting agents require twice-daily dosing. Olopatadine 0.2% and alcaftadine are indicated for once-daily dosing and maintain effectiveness through 16 hours after administration in conjunctival allergen challenge studies 111, 112, 113.
Olopatadine 0.1% (Pataday Twice Daily Relief) was the first topical anti-allergy medication that was approved for twice-daily usage 101. These agents are all preserved with a surfactant called benzalkonium chloride that may cause ocular surface toxicity 114. These are now considered the first line of treatment for allergic eye disease and are the most common ophthalmic agents recommended by eye care practitioners and allergists 101. These agents can be used to prevent mast cell degranulation and acutely following the onset of symptoms 115.
Compared to placebo, olopatadine has been found to improve symptoms of eyelid swelling, eye redness, chemosis (a condition where the conjunctiva, or the outer surface of the eye, swells due to fluid build-up), itch, and overall quality of life. Multiple randomized control trials have compared ketotifen and olopatadine. One meta-analysis found improvement in symptoms of itching after 14 days in favor of olopatadine 0.1% when compared to ketotifen 0.025% 116. Before 2020, olopatadine was only available as a prescription medication, and ketotifen, in the form of Zaditor or Alaway, was clinically commonly prescribed as the first line of relief as an OTC medication. Within the last 4 years, olopatadine became available OTC and has gained popularity to become clinically superior to ketotifen in terms of efficacy.
Leukotriene Receptor Antagonists
Leukotriene receptor antagonists (e.g., montelukast), which are currently available for oral dosing, prevent leukotrienes from binding to their conjunctival receptors to decrease inflammatory signaling and improve multiple ocular symptoms of allergic conjunctivitis. Leukotriene receptor antagonists have a slower onset of action, are less effective than topical antihistamines, and are not used as first-line therapy or monotherapy for allergic conjunctivitis 106.
Topical Vasoconstrictors (Decongestants)
Topical vasoconstrictors (decongestants) were the first ocular medication approved for the treatment of allergic conjunctivitis. Over-the-counter (OTC) topical vasoconstrictors are effective at temporarily decreasing conjunctival hyperemia by stimulating alpha-adrenergic receptors 109. Alpha-adrenergic agonists cause vasoconstriction of conjunctival blood vessels, resulting in decongestion and whitening of the eye 117, 109. However, the use of these agonists can lead to side effects such as rebound hyperemia and tachyphylaxis and, chronically, can lead to conjunctivitis medicamentosa 67, 109. Commonly used topical vasoconstrictors are oxymetazoline, naphazoline, tetrahydrozoline, and phenylephrine. These are best utilized as short-term solutions and should be avoided in narrow-angle glaucoma and cardiovascular issues 117, 109. These should not be recommended as a standalone treatment and used in combination with antihistamines for the treatment of allergic conjunctivitis 117, 20.
Combination eye drops including decongestant (Antihistamine-Vasoconstrictor Combinations)
Some eye drops contain an antihistamine such as pheniramine or antazoline to stop itching, and a vasoconstrictor (substances that cause the walls of blood vessels to narrow, or constrict) such as naphazoline to take away redness through stimulation of vascular alpha-adrenergic receptors e.g. naphazoline + antazoline (Antistine-Privine, Albalon-A), pheniramine + naphazoline (Visine Allergy with Antihistamine, Naphcon-A). Vasoconstrictors are commonly available in nonprescription combination formulations that contain an antihistamine (e.g., naphazoline-antazoline, naphazoline-pheniramine). These formulations exhibit a rapid onset of action and relieve redness and itchiness associated with allergic conjunctivitis. However, they are not recommended for long-term use because of reduced effectiveness over time and a potential rebound effect that can produce persistent red eye on discontinuation 110. As with topical antihistamines, combination antihistamine–vasoconstrictor formulations have a relatively short duration of action and are administered four times daily 15, 104. Limit use of combination eye drops to no more than 5 to 7 days to avoid a ‘rebound’ redness from overuse.
Topical nonsteroidal anti-inflammatory drugs (NSAIDS)
Topical nonsteroidal anti-inflammatory drugs (NSAIDS) act by blocking the cyclooxygenase enzymes (COX-1 and COX-2) within the cyclooxygenase pathway, resulting in the inhibition of inflammatory mediators such as prostaglandins and leukotrienes 109, 108. These drugs have proven efficacy against conjunctival hyperemia, pruritus, pain, and irritation 109. Topical NSAID agents commonly associated with the relief of ocular allergy symptoms include ketorolac, diclofenac, indomethacin, and flurbiprofen 109, 108. Although ketorolac has been approved for treating allergic conjunctivitis, studies have indicated that it is less effective compared to topical antihistamine agents 109, 108, 118. Moreover, these agents can cause burning and stinging sensations upon instillation, so long-term compliance is an issue. Thus, NSAIDs may be used for temporary relief of itching and hyperemia compared to no treatment; however, they do not aid with symptoms of mucous discharge, chemosis (a condition where the conjunctiva, or the outer surface of the eye, swells due to fluid build-up), and corneal damage, so alternative methods should be considered 109, 108, 118, 119.
Other eye drops, to prevent allergy symptoms
These eye drops prevent allergic reactions in the eyes and need to be used 4 to 6 times per day, depending on the ingredient, for the entire time you are exposed to triggers, such as during spring e.g. cromoglycate (Cromolux Eye Drops, Opticrom), lodoxamide (Lomide Eye Drops 0.1%)
Oral antihistamines (tablets and syrups)
There are two types of oral antihistamines: newer, less sedating antihistamines, which do not typically cause drowsiness and older sedating antihistamines that cause drowsiness.
Oral antihistamines are good for treating hay fever symptoms, especially if you have a lot of different symptoms. You can also take oral antihistamines in advance if you know you are going to be exposed to allergens or triggers
Newer, less-sedating antihistamines
Newer antihistamines may rarely cause drowsiness; do not drive or operate machinery if you are affected e.g. cetirizine (Zilarex, Zyrtec), desloratadine (Aerius), fexofenadine (Fexotabs, Telfast), loratadine (Claratyne, Lorano).
Cetirizine and loratadine are available as syrups for children; check correct doses for different age groups. Cetirizine is more likely to cause drowsiness than other less sedating antihistamines
Older, sedating antihistamines
Older sedating antihistamines can cause drowsiness, sometimes the next day; it is important you do not drive or operate machinery e.g. chlorpheniramine + pseudoephedrine (Demazin 6 Hour Relief Tablets), dexchlorpheniramine (Polaramine), loratadine + pseudoephedrine (Claratyne-D with Decongestant Repetabs), promethazine (Phenergan, Sandoz Fenezal)
Older antihistamines are not available without a prescription for children under 2 years old. Do not drink alcohol with antihistamines that make you drowsy
If you have other medical conditions, such as glaucoma, epilepsy or prostate problems, or you take antidepressants, check with your doctor before taking these medicines
Corticosteroids
Corticosteroids prevent production of multiple classes of late-phase response mediators, including prostaglandins, leukotrienes, histamine, and some cytokines. The numerous points of intervention in the inflammatory cascade make glucocorticoids an effective pharmacologic therapy for allergic conjunctivitis, but long-term topical use can lead to serious adverse effects, including increased intraocular pressure and corneal abnormalities 110. Long-term systemic corticosteroid use increases the risk of posterior subcapsular cataract formation 120. For this reason, patients at risk (e.g., those with glaucoma or diabetic retinopathy) or patients who receive higher doses or longer treatment courses of corticosteroids should be monitored by an ophthalmologist.
Corticosteroids (e.g., loteprednol etabonate, given four times daily) are generally not used as primary therapy for allergic conjunctivitis unless there is persistent or moderate-to-severe inflammation that the eye doctor does not feel will respond sufficiently to antihistamine–mast cell stabilizer medications alone 15. When corticosteroids are prescribed, they typically are used for short durations in the early stages of allergic conjunctivitis or during flare-ups until allergic conjunctivitis can be controlled with safer medications such as antihistamines, mast cell stabilizers, or dual-acting, single-molecule antihistamine–mast cell stabilizer agents 121. Topical corticosteroids are important in severe cases of allergic eye disease to break the cycle of inflammation and can be discontinued once the condition is under control. Most cases of seasonal allergic conjunctivitis or perennial allergic conjunctivitis do not often require corticosteroid intervention. For patients who require long-term use of corticosteroids, close observation by an ophthalmologist is warranted.
Supratarsal steroids
Supratarsal steroids are required in patients with the severe palpebral form of the disease who are unresponsive to topical steroids or are non-compliant. The conjunctiva is everted, and injection is given in the supratarsal conjunctiva. An injection of 0.1 ml betamethasone 4 mg/mL, dexamethasone 4 mg/mL, or triamcinolone can be provided 122.
Topical Calcineurin inhibitors
The topical calcineurin inhibitors cyclosporine A and tacrolimus are very effective in the treatment of giant papillary conjunctivitis (GPC), atopic keratocongiuntivitis (AKC), and vernal keratoconjunctivitis (VKC) and may serve as steroid-sparing agents when these forms of chronic allergic conjunctivitis become steroid-dependent 48, 52.
Cyclosporine A (CsA) is also used worldwide for the treatment of dry eye. Suspensions of cyclosporine A may be prepared in pharmacies, although some countries also have commercialized forms 123. The concentrations of cyclosporine A in the different ophthalmic formulations range between 0.01% and 2% and therefore the administration varies between 1 and 6 times per day 57. Tacrolimus may also be prepared as suspension by pharmacies and exists as an ointment for dermatological purposes in most countries at a concentration of 0.03-0.1%. Recent research shows that tacrolimus may have similar if not superior effectivity than cyclosporine A for the treatment of vernal keratoconjunctivitis (VKC). Moreover, dermatologic ointment containing tacrolimus is effective for the treatment of lid eczema in atopic keratocongiuntivitis (AKC) 48, 52. Topical treatment with calcineurin inhibitors has side effects such as stinging/burning sensation and the possibility of molluscum contagiosum virus, papillomavirus, or herpesvirus infection, although there is evidence from studies on dry eye syndrome that treatment with cyclosporine A can be topically administered long term and without systemic absorption 52, 57, 49, 123. At present, tacrolimus is generally administered topically in cases that do not respond to cyclosporine A.1 Finally, in very severe cases, allergic conjunctivitis such as VKC and atopic keratocongiuntivitis (AKC) may require systemic immunosuppression that is usually achieved with cyclosporine A, tacrolimus, or mycophenolate mofetil 48, 52, 124.
Biologicals
In theory, biological treatments could have superior results because they block the underlying inflammation pathways by bonding with specific biological molecules to decrease conjunctival inflammation 125. A few trials have reported the systemic use of the biologicals omalizumab, indicated for severe asthma, and dupilumab, indicated for atopic dermatitis, in vernal keratoconjunctivitis (VKC) and atopic keratocongiuntivitis (AKC). Omalizumab shows generally good results, though it has not yet been approved for allergic conjunctivitis, while dupilumab may increase the risk of blepharoconjunctivitis, which is tacrolimus-responsive in patients with severe atopic disease or previous atopic keratocongiuntivitis (AKC) 48, 126, 127, 128. Benralizumab, mepolizumab, and reslizumab, which are anti IL-5 biologic agents have not been studied in the context of allergic conjunctivitis 98.
Insunakinra (EBI-005) is the first inmunophilin synthesized for topical ophthalmologic use. It is an antagonist of the IL-1 receptor and binds to it, blocking the rest of the pathway. It has been documented to diminish ocular surface symptoms such as itching, inflammation, and discomfort 129.
Another molecule called liftitegrast (Shire Pharmaceuticals) has both activity as an antagonist of the IL-1 receptor and as antagonist of the lymphocyte functional antigen-1 and has proven effective for treatment of ocular surface symptoms 130.
Immunotherapy
The goal of immunotherapy is to diminish the symptoms and signs of rhinitis and conjunctivitis triggered by known allergens and to prevent their recurrence. Allergen-specific immunotherapy may be considered in cases of failure of first line treatments, or as a modifier of the natural course of the disease 48, 131, 132. Changes involve downregulation of Th2 response and upregulation of regulatory T-cells 98. It is carried out by administering gradually increasing amounts of the allergen to induce an immunological tolerance. According to the European Academy of Allergy and Clinical Immunology guidelines, it is indicated in patients with a documented IgE-mediated hypersensitivity to airborne agents, with severe forms of rhinoconjunctivitis that affect their quality of life in spite of allergen avoidance and pharmacotherapy 133, 134, 135. Immunotherapy can also be applied in children, but because it requires a strict regimen of desensitization, it may be difficult to treat children below 6 years of age 56, 132. There are commercial forms of many recognized allergens and the allergist determines the allergen to be prescribed based on previous hypersensitivity tests. Desensitization consists of two phases, an induction phase that lasts 5-8 months and a maintenance phase that last 3-5 years 132, 135. The standard method of administering the antigen has been subcutaneous injection, but recently other less invasive methods have been developed, such as sublingual or epicutaneous administration, with good results 49, 132. Adherence to sublingual is deemed better because it does not involve injections but has not been studied as exhaustively as subcutaneous injection; more randomized controlled trials are needed. Other forms of immunotherapy such as intralymphatic administration or edible vaccines are still being studied 49, 135.
In isolated allergic conjunctivitis (IgE- and non-IgE-mediated), allergen immunotherapy may be considered on the same premise as in rhinoconjunctivitis. However, there is less evidence of its beneficial effects and a few studies have documented an improvement of the clinical symptoms in vernal keratoconjunctivitis (VKC) but not in atopic keratocongiuntivitis (AKC) 49, 136, 124, 135.
Surgery
In very recalcitrant cases of atopic keratocongiuntivitis (AKC) and vernal keratoconjunctivitis (VKC), eye surgery may be needed. Papillae resection, in some cases with grafting of autologous conjunctiva, amniotic membrane or mucous membrane are effective in the treatment of severe forms of vernal keratoconjunctivitis (VKC) with corneal ulcers 134, 137, 138. Plaque resection may be necessary for subepithelial deposits in vernal keratoconjunctivitis (VKC) 54, 139. In atopic keratocongiuntivitis (AKC), surgery may be needed for eyelid and conjunctival scarring.
Atopic disease and atopic keratocongiuntivitis (AKC) can be complicated by subcapsular cataracts and/or severe ocular surface disease that may require complex surgery such as superficial keratectomy, limbal transplantation, or keratoprosthesis implantation 140.
Allergic conjunctivitis home remedies
If your conjunctivitis is caused by allergies, stopping the source of the allergy is important. Allergic conjunctivitis will continue as long as you’re in contact with whatever is causing it. Allergic conjunctivitis is not contagious. You can still go to work or school with allergic conjunctivitis and no one else will catch it.
To reduce your symptoms of allergic conjunctivitis you can:
- Take allergy medicine or use allergy eye drops.
- Put a cool, damp washcloth over your eyes for a few minutes.
- Use over-the-counter lubricating eye drops (artificial tears).
Allergic keratoconjunctivitis prognosis
Most people with allergic keratoconjunctivitis the prognosis for allergic conjunctivitis is good 3, 1. However, visual impairment can occur related to certain types of severe eye allergies, too much eye rubbing, eye infections, corneal damage or steroid use. Additionally, the medications used to manage allergic conjunctivitis can be associated with the development of cataracts 1.
- Baab S, Le PH, Gurnani B, et al. Allergic Conjunctivitis. [Updated 2024 Jan 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448118[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Allergic conjunctivitis: Update on pathophysiology and prospects for future treatment. Ono, Santa Jeremy et al. Journal of Allergy and Clinical Immunology, Volume 115, Issue 1, 118 – 122. https://www.jacionline.org/article/S0091-6749(04)03032-5/fulltext[↩]
- La Rosa M, Lionetti E, Reibaldi M, Russo A, Longo A, Leonardi S, Tomarchio S, Avitabile T, Reibaldi A. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013 Mar 14;39:18. doi: 10.1186/1824-7288-39-18[↩][↩][↩][↩][↩][↩][↩]
- Rathi, V.M., & Murthy, S.I. (2017). Allergic conjunctivitis. Community Eye Health, 30, S7 – S10. https://pdfs.semanticscholar.org/d820/987003b832dc90f868f531c9616a4444ac4c.pdf[↩][↩]
- Butrus S, Portela R. Ocular allergy: diagnosis and treatment. Ophthalmol Clin North Am. 2005 Dec;18(4):485-92, v. doi: 10.1016/j.ohc.2005.07.007[↩]
- Gomes PJ. Trends in prevalence and treatment of ocular allergy. Curr Opin Allergy Clin Immunol. 2014 Oct;14(5):451-6. doi: 10.1097/ACI.0000000000000100[↩]
- Bielory L, Frohman L. Allergic and immunologic disorders of the eye. J Allergy Clin Immunol. 1992;86:1–20. doi: 10.1016/s0091-6749(05)80033-8[↩]
- Leonardi A, Motterle L, Bortolotti M. Allergy and the eye. Clin Exp Immunol. 2008;153:17–21. doi: 10.1111/j.1365-2249.2008.03716.x[↩]
- Tariq F. Allergic Conjunctivitis: Review of Current Types, Treatments, and Trends. Life (Basel). 2024 May 21;14(6):650. doi: 10.3390/life14060650[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Curr Opin Allergy Clin Immunol. 2015 Oct;15(5):482-8. doi: 10.1097/ACI.0000000000000204[↩]
- What is allergic conjunctivitis? https://aapos.org/glossary/allergic-conjunctivitis[↩]
- Carr W, Schaeffer J, Donnenfeld E. Treating Allergic Conjunctivitis: A Once-daily Medication that Provides 24-hour Symptom Relief. Allergy & Rhinology. 2016;7(2). doi:10.2500/ar.2016.7.0158[↩]
- Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergy in the United States, 1988-1994. J Allergy Clin Immunol. 2010 Oct;126(4):778-783.e6. doi: 10.1016/j.jaci.2010.06.050[↩]
- Chigbu D.I. The pathophysiology of ocular allergy: A review. Cont Lens Anterior Eye 32: 3–15; quiz 43–44, 2009.[↩][↩]
- Bielory L., Meltzer E.O., Nichols K.K.et al. An algorithm for the management of allergic conjunctivitis. Allergy Asthma Proc 34: 408–420, 2013.[↩][↩][↩]
- Palmares J, Delgado L, Cidade M, Quadrado MJ, Filipe HP; Season Study Group. Allergic conjunctivitis: a national cross-sectional study of clinical characteristics and quality of life. Eur J Ophthalmol. 2010;20:257–264. doi: 10.1177/112067211002000201[↩]
- Villegas BV, Benitez-Del-Castillo JM. Current Knowledge in Allergic Conjunctivitis. Turk J Ophthalmol. 2021 Feb 25;51(1):45-54. doi: 10.4274/tjo.galenos.2020.11456[↩][↩][↩]
- Allergic Conjunctivitis. https://www.mrverity.com/patient-information/images/dry-and-irritable-eyes/allergic-conjunctivitis/[↩]
- Rodrigues J, Kuruvilla ME, Vanijcharoenkarn K, Patel N, Hom MM, Wallace DV. The spectrum of allergic ocular diseases. Ann Allergy Asthma Immunol. 2021;126:240–254. doi: 10.1016/j.anai.2020.11.016[↩]
- Dupuis P., Prokopich C.L., Hynes A., Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin. Immunol. 2020;16:5. doi: 10.1186/s13223-020-0403-9[↩][↩]
- Villegas B.V., Benitez-Del-Castillo J.M. Current Knowledge in Allergic Conjunctivitis. Turk. J. Ophthalmol. 2021;51:45–54. doi: 10.4274/tjo.galenos.2020.11456[↩][↩][↩]
- Dupuis P, Prokopich CL, Hynes A, Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin Immunol. 2020 Jan 21;16:5. doi: 10.1186/s13223-020-0403-9[↩]
- Friedlander MH. Ocular Allergy. Curr Opin Allergy Clin Immunol. 2011;11(5):477–482. doi: 10.1097/ACI.0b013e32834a9652[↩]
- Rathi VM, Murthy SI. Allergic conjunctivitis. Community Eye Health. 2017;30(99):S7-S10. https://pmc.ncbi.nlm.nih.gov/articles/PMC5968423/[↩][↩][↩][↩][↩]
- Leonardi A, Piliego F, Castegnaro A, Lazzarini D, La Gloria Valerio A, Mattana P, Fregona I. Allergic conjunctivitis: a cross-sectional study. Clin Exp Allergy. 2015 Jun;45(6):1118-25. doi: 10.1111/cea.12536[↩]
- Mehta JS, Chen WL, Cheng ACK, Cung LX, Dualan IJ, Kekunnaya R, Khaliddin N, Kim TI, Lam DK, Leo SW, Manurung F, Tesavibul N, Bremond-Gignac D. Diagnosis, Management, and Treatment of Vernal Keratoconjunctivitis in Asia: Recommendations From the Management of Vernal Keratoconjunctivitis in Asia Expert Working Group. Front Med (Lausanne). 2022 Aug 1;9:882240. doi: 10.3389/fmed.2022.882240[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Kaur K, Gurnani B. Vernal Keratoconjunctivitis. [Updated 2023 Jun 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK576433[↩]
- Vernal Keratoconjunctivitis. https://eyewiki.org/Vernal_Keratoconjunctivitis[↩][↩][↩][↩]
- Katelaris CH. Ocular allergy in the Asia Pacific region. Asia Pac Allergy. (2011) 1:108–14. 10.5415/apallergy.2011.1.3.108[↩]
- Zicari AM, Capata G, Nebbioso M, De Castro G, Midulla F, Leonardi L, et al. Vernal keratoconjunctivitis: an update focused on clinical grading system. Ital J Pediatr. (2019) 45:64. 10.1186/s13052-019-0656-4[↩]
- Miyazaki D, Fukagawa K, Okamoto S, Fukushima A, Uchio E, Ebihara N, et al. Epidemiological aspects of allergic conjunctivitis. Allergol Int. (2020) 69:487–95. 10.1016/j.alit.2020.06.004[↩][↩]
- Bremond-Gignac D, Donadieu J, Leonardi A, Pouliquen P, Doan S, Chiambarretta F, et al. Prevalence of vernal keratoconjunctivitis: a rare disease? Br J Ophthalmol. (2008) 92:1097–102. 10.1136/bjo.2007.117812[↩][↩]
- Leonardi A. Management of vernal keratoconjunctivitis. Ophthalmol Ther. 2013 Dec;2(2):73-88. doi: 10.1007/s40123-013-0019-y[↩]
- De Smedt, S., G. Wildner, and P. Kestelyn, Vernal keratoconjunctivitis: an update. Br J Ophthalmol, 2013. 97(1): p. 9-14.[↩][↩]
- Kumar, S., Vernal keratoconjunctivitis: a major review. Acta Ophthalmologica, 2009. 87(2): p. 133-147.[↩][↩][↩]
- Smedt, S.D., et al., Vernal keratoconjunctivitis in school children in Rwanda and its association with socio-economic status: a population-based survey. Am J Trop Med Hyg, 2011. 85(4): p. 711-7.[↩]
- La Rosa, M., et al., Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr, 2013. 39: p. 18.[↩]
- Addis H, Jeng BH. Vernal keratoconjunctivitis. Clin Ophthalmol. (2018) 12:119–23. 10.2147/OPTH.S129552[↩][↩][↩][↩]
- Bonini S, Coassin M, Aronni S, Lambiase A. Vernal keratoconjunctivitis. Eye. (2004) 18:345–51. 10.1038/sj.eye.6700675[↩][↩][↩][↩]
- Baudouin C, Liang H, Bremond-Gignac D, Hamard P, Hreiche R, Creuzot-Garcher C, et al. CCR4 and CCR5 expression in conjunctival specimens as differential markers of T(H)1/T(H)2 in ocular surface disorders. J Allergy Clin Immunol. (2005) 116:614–9. 10.1016/j.jaci.2005.05.033[↩][↩]
- Mishra GP, Tamboli V, Jwala J, Mitra AK. Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat Inflamm Allergy Drug Discov. (2011) 5:26–36. 10.2174/187221311794474883[↩]
- Leonardi A. Vernal keratoconjunctivitis: pathogenesis and treatment. Prog Retin Eye Res. (2002) 21:319–39. 10.1016/S1350-9462(02)00006-X[↩]
- Barot RK, Shitole SC, Bhagat N, Patil D, Sawant P, Patil K. Therapeutic effect of 0.1% Tacrolimus Eye Ointment in Allergic Ocular Diseases. J Clin Diagn Res. 2016 Jun;10(6):NC05-9. doi: 10.7860/JCDR/2016/17847.7978[↩]
- Leonardi A. Management of vernal keratoconjunctivitis. Ophthalmol Ther. (2013) 2:73–88. 10.1007/s40123-013-0019-y[↩][↩][↩][↩][↩]
- Bonini, S., et al., Vernal keratoconjunctivitis revisited: a case series of 195 patients with long-term followup. Ophthalmology, 2000. 107(6): p. 1157-63.[↩][↩]
- Ukponmwan, C.U., Vernal keratoconjunctivitis in Nigerians: 109 consecutive cases. Trop Doct, 2003. 33(4): p. 242-5.[↩]
- Bremond-Gignac D. Atopic and vernal keratoconjunctivitis: differences and similarities. Acta Ophthalmologica. (2016) 94:S256. 10.1111/j.1755-3768.2016.0005[↩]
- Patel N, Venkateswaran N, Wang Z, Galor A. Ocular involvement in atopic disease: a review. Curr Opin Ophthalmol. 2018;29:576–581. doi: 10.1097/ICU.0000000000000532[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Bielory L, Schoenberg D. Emerging therapeutics for ocular surface disease. Curr Allergy Asthma Rep. 2019;28:19–16. doi: 10.1007/s11882-019-0844-8[↩][↩][↩][↩][↩]
- Atopic Keratoconjunctivitis. https://eyewiki.org/Atopic_Keratoconjunctivitis[↩]
- Atopic Keratoconjunctivitis (AKC). https://www.umkelloggeye.org/conditions-treatments/atopic-keratoconjunctivitis[↩][↩][↩]
- Fauquert JL, Jedrzejczak-Czechowicz M, Rondon C, Calder V, Silva D, Kvenshagen BK, Callebaut I, Allegri P, Santos N, Doan S, Perez Formigo D, Chiambaretta F, Delgado L, Leonardi A Interest Group on Ocular Allergy (IGOA) from the European Academy of Allergy and Clinical Immunology. Conjunctival allergen provocation test : guidelines for daily practice. Allergy. 2016;72:43–54. doi: 10.1111/all.12986[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Atopic dermatitis. https://dermnetnz.org/topics/atopic-dermatitis[↩][↩]
- La Rosa M, Lionetti E, Reibaldi M, Russo A, Longo A, Leonardi S, Tomarchio S, Avitabile T, Reibaldi A. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013;39:18. doi: 10.1186/1824-7288-39-18[↩][↩][↩]
- Leonardi A. Vernal keratoconjunctivitis: pathogenesis and treatment. Prog Retin Eye Res. 2002;21:319–339. doi: 10.1016/s1350-9462(02)00006-x[↩]
- Berger WE, Granet DB, Kabat AG. Diagnosis and management of allergic conjunctivitis in pediatric patients. Allergy Asthma Proc. 2017;38:16–27. doi: 10.2500/aap.2017.38.4003[↩][↩]
- Leonardi A, Bogacka E, Fauquert JL, Kowalski ML, Groblewska A, Jedrzejczak-Czechowicz M, Doan S, Marmouz F, Demoly P, Delgado L. Ocular allergy: recognizing and diagnosing hypersensitivity disorders of the ocular surface. Allergy. 2012;67:1327–1337. doi: 10.1111/all.12009[↩][↩][↩][↩]
- O’Brien TP. Allergic conjunctivitis: an update on diagnosis and management. Curr Opin Allergy Clin Immunol. 2013;13:543–549. doi: 10.1097/ACI.0b013e328364ec3a[↩]
- Brémond-Gignac D, Nischal KK, Mortemousque B, Gajdosova E, Granet DB, Chiambaretta F. Atopic Keratoconjunctivitis in Children: Clinical Features and Diagnosis. Ophthalmology. 2016 Feb;123(2):435-437. doi: 10.1016/j.ophtha.2015.07.012[↩]
- Aboobacker S, Harris BW, Limaiem F. Lichenification. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537332[↩]
- Kenny S.E., Tye C.B., Johnson D.A., Kheirkhah A. Giant papillary conjunctivitis: A review. Ocul. Surf. 2020;18:396–402. doi: 10.1016/j.jtos.2020.03.007[↩][↩][↩][↩]
- Azari A.A., Arabi A. Conjunctivitis: A Systematic Review. J. Ophthalmic Vis. Res. 2020;15:372–395. doi: 10.18502/jovr.v15i3.7456[↩][↩]
- Elhers WH, Donshik PC. Giant papillary conjunctivitis. Curr Opin Allergy Clin Immunol. 2008;8:445–449. doi: 10.1097/ACI.0b013e32830e6af0[↩]
- Sacchetti M, Plateroti R, Bruscolini A, Giustolisi R, Marenco M. Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms. Life (Basel). 2021 Sep 26;11(10):1012. doi: 10.3390/life11101012[↩]
- Jordakieva G, Jensen-Jarolim E. The impact of allergen exposure and specific immunotherapy on circulating blood cells in allergic rhinitis. World Allergy Organ J. 2018 Aug 15;11(1):19. doi: 10.1186/s40413-018-0197-0[↩]
- Li A, Li S, Ruan F, Jie Y. Atopic keratoconjunctivitis: A diagnostic dilemma-a case report. Medicine (Baltimore). 2018 Apr;97(16):e0372. doi: 10.1097/MD.0000000000010372[↩]
- La Rosa M., Lionetti E., Reibaldi M., Russo A., Longo A., Leonardi S., Tomarchio S., Avitabile T., Reibaldi A. Allergic conjunctivitis: A comprehensive review of the literature. Ital. J. Pediatr. 2013;39:18. doi: 10.1186/1824-7288-39-18[↩][↩][↩][↩][↩]
- Dordal M.T., Lluch-Bernal M., Sánchez M.C., Rondón C., Navarro A., Montoro J., Matheu V., Ibáñez M.D., Fernández-Parra B., Dávila I. Allergen-specific nasal provocation testing: Review by the rhinoconjunctivitis committee of the Spanish Society of Allergy and Clinical Immunology. J. Investig. Allergol. Clin. Immunol. 2011;21:1–12. quiz 12[↩][↩][↩][↩][↩][↩]
- Katelaris CH. Giant papillary conjunctivitis–a review. Acta Ophthalmol Scand Suppl. 1999;(228):17-20. doi: 10.1111/j.1600-0420.1999.tb01166.x[↩]
- Chigbu D.I. The pathophysiology of ocular allergy: A review. Contact Lens Anterior Eye. 2009;32:3–15. doi: 10.1016/j.clae.2008.07.003. quiz 43–44.[↩][↩]
- Wise S.K., Lin S.Y., Toskala E., Orlandi R.R., Akdis C.A., Alt J.A., Azar A., Baroody F.M., Bachert C., Canonica G.W., et al. International consensus statement on allergy and rhinology: Allergic rhinitis—2023. Int. Forum. Allergy Rhinol. 2023;13:293–859. doi: 10.1002/alr.23090[↩]
- Chen Y., Wang S., Alemi H., Dohlman T., Dana R. Immune regulation of the ocular surface. Exp. Eye Res. 2022;218:109007. doi: 10.1016/j.exer.2022.109007[↩][↩]
- Bron A.J., de Paiva C.S., Chauhan S.K., Bonini S., Gabison E.E., Jain S., Knop E., Markoulli M., Ogawa Y., Perez V., et al. TFOS DEWS II pathophysiology report. Ocul. Surf. 2017;15:438–510. doi: 10.1016/j.jtos.2017.05.011[↩]
- Dartt D.A., Willcox M.D. Complexity of the tear film: Importance in homeostasis and dysfunction during disease. Exp. Eye Res. 2013;117:1–3. doi: 10.1016/j.exer.2013.10.008[↩]
- Elieh Ali Komi D., Rambasek T., Bielory L. Clinical implications of mast cell involvement in allergic conjunctivitis. Allergy. 2018;73:528–539. doi: 10.1111/all.13334[↩][↩][↩]
- Cursiefen C. Immune privilege and angiogenic privilege of the cornea. Chem. Immunol. Allergy. 2007;92:50–57. doi: 10.1159/000099253[↩][↩]
- Zhou R., Caspi R.R. Ocular immune privilege. F1000 Biol. Rep. 2010;2:20948803. doi: 10.3410/B2-3[↩]
- Chauhan S.K., Dohlman T.H., Dana R. Corneal Lymphatics: Role in Ocular Inflammation as Inducer and Responder of Adaptive Immunity. J. Clin. Cell. Immunol. 2014;5:1000256. doi: 10.4172/2155-9899.1000256[↩]
- Barabino S., Chen Y., Chauhan S., Dana R. Ocular surface immunity: Homeostatic mechanisms and their disruption in dry eye disease. Prog. Retin. Eye Res. 2012;31:271–285. doi: 10.1016/j.preteyeres.2012.02.003[↩]
- Hattori T., Takahashi H., Dana R. Novel Insights Into the Immunoregulatory Function and Localization of Dendritic Cells. Cornea. 2016;35((Suppl. 1[↩]
- Chigbu D.I., Minhas B.K. Immunopathology of allergic conjunctivitis. Eur. Med. J. 2018;3:76–83. doi: 10.33590/emj/10312711[↩][↩][↩]
- Knop E., Knop N. Anatomy and immunology of the ocular surface. Chem. Immunol. Allergy. 2007;92:36–49. doi: 10.1159/000099252[↩][↩][↩]
- Galicia-Carreón J, Santacruz C, Hong E, Jiménez-Martínez MC. The ocular surface: from physiology to the ocular allergic diseases. Rev Alerg Mex. 2013 Oct-Dec;60(4):172-83.[↩][↩]
- Knop N., Knop E. Conjunctiva-associated lymphoid tissue in the human eye. Investig. Ophthalmol. Vis. Sci. 2000;41:1270–1279.[↩]
- Knop E., Knop N. The role of eye-associated lymphoid tissue in corneal immune protection. J. Anat. 2005;206:271–285. doi: 10.1111/j.1469-7580.2005.00394.x[↩]
- Knop E., Knop N. Influence of the eye-associated lymphoid tissue (EALT) on inflammatory ocular surface disease. Ocul. Surf. 2005;3((Suppl. 4[↩][↩]
- Chigbu D.I., Jain P., Khan Z.K. Immune Mechanisms, Pathology, and Management of Allergic Ocular Diseases. In: Jain P., Ndhlovu L.C., editors. Advanced Concepts in Human Immunology: Prospects for Disease Control. Springer Nature; Berlin/Heidelberg, Germany: 2020. pp. 229–277.[↩]
- Miyazaki D., Nakamura T., Ohbayashi M., Kuo C.H., Komatsu N., Yakura K., Tominaga T., Inoue Y., Higashi H., Murata M., et al. Ablation of type I hypersensitivity in experimental allergic conjunctivitis by eotaxin-1/CCR3 blockade. Int. Immunol. 2009;21:187–201. doi: 10.1093/intimm/dxn137[↩]
- Ackerman S., Smith L.M., Gomes P.J. Ocular itch associated with allergic conjunctivitis: Latest evidence and clinical management. Ther. Adv. Chronic. Dis. 2016;7:52–67. doi: 10.1177/2040622315612745[↩]
- Ono S.J., Lane K. Comparison of effects of alcaftadine and olopatadine on conjunctival epithelium and eosinophil recruitment in a murine model of allergic conjunctivitis. Drug Des. Dev. Ther. 2011;5:77–84. doi: 10.2147/DDDT.S15788[↩][↩][↩]
- Mantelli F., Mauris J., Argueso P. The ocular surface epithelial barrier and other mechanisms of mucosal protection: From allergy to infectious diseases. Curr. Opin. Allergy Clin. Immunol. 2013;13:563–568. doi: 10.1097/ACI.0b013e3283645899[↩]
- Leonardi A., Motterle L., Bortolotti M. Allergy and the eye. Clin. Exp. Immunol. 2008;153((Suppl. 1[↩][↩]
- Irkec M.T., Bozkurt B. Molecular immunology of allergic conjunctivitis. Curr. Opin. Allergy Clin. Immunol. 2012;12:534–539. doi: 10.1097/ACI.0b013e328357a21b[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Chigbu D.I. The pathophysiology of ocular allergy: A review. Contact Lens Anterior Eye. 2009;32:3–15. doi: 10.1016/j.clae.2008.07.003. quiz 43–44[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Labib B.A., Chigbu D.I. Therapeutic Targets in Allergic Conjunctivitis. Pharmaceuticals. 2022;15:547. doi: 10.3390/ph15050547[↩][↩][↩][↩]
- Chigbu D.I., Karbach N.J., Abu S.L., Hehar N.K. Cytokines in Allergic Conjunctivitis: Unraveling Their Pathophysiological Roles. Life. 2024;14:350. doi: 10.3390/life14030350[↩]
- Saboo US, Jain M, Reddy JC, Sangwan VS. Demographic and clinical profile of vernal keratoconjunctivitis at a tertiary eye care center in India. Indian J Ophthalmol. 2013 Sep;61(9):486-9. doi: 10.4103/0301-4738.119431[↩][↩]
- Dupuis P, Prokopich CL, Hynes A, Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin Immunol. 2020;16:5. doi: 10.1186/s13223-020-0403-9[↩][↩][↩][↩]
- Pepper AN, Ledford DK. Nasal and ocular challenges. J Allergy Clin Immunol. 2018;141:1570–1577. doi: 10.1016/j.jaci.2017.11.066[↩][↩][↩]
- Bilkhu PS, Wolffsohn JS, Naroo SA, Robertson L, Kennedy R. Effectiveness of nonpharmacologic treatments for acute seasonal allergic conjunctivitis. Ophthalmology. 2014;121:72–78. doi: 10.1016/j.ophtha.2013.08.007[↩]
- Bielory L. Ocular allergy overview. Immunol. Allergy Clin. N. Am. 2008;28:1–23. doi: 10.1016/j.iac.2007.12.011[↩][↩][↩][↩][↩][↩]
- Chan V.F., Yong A.C., Azuara-Blanco A., Gordon I., Safi S., Lingham G., Evans J., Keel S. A Systematic Review of Clinical Practice Guidelines for Infectious and Non-infectious Conjunctivitis. Ophthalmic Epidemiol. 2022;29:473–482. doi: 10.1080/09286586.2021.1971262[↩][↩]
- Palmares J., Delgado L., Cidade M., Quadrado M.J., Filipe H.P. Allergic conjunctivitis: A national cross-sectional study of clinical characteristics and quality of life. Eur. J. Ophthalmol. 2010;20:257–264. doi: 10.1177/112067211002000201[↩][↩]
- Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013 Oct 23;310(16):1721-9. doi: 10.1001/jama.2013.280318. Erratum in: JAMA. 2014 Jan 1;311(1):95. Dosage error in article text.[↩][↩]
- Yanni JM, Sharif NA, Gamache DA, Miller ST, Weimer LK, Spellman JM. A current appreciation of sites for pharmacological intervention in allergic conjunctivitis: effects of new topical ocular drugs. Acta Ophthalmol Scand Suppl. (1999) 228:33–7. 10.1111/j.1600-0420.1999.tb01171.x[↩]
- Gane J, Buckley R. Leukotriene receptor antagonists in allergic eye disease: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2013 Jan;1(1):65-74. doi: 10.1016/j.jaip.2012.07.001[↩][↩]
- Simons F.E., Simons K.J. Histamine and H1-antihistamines: Celebrating a century of progress. J. Allergy Clin. Immunol. 2011;128:1139–1150.e4. doi: 10.1016/j.jaci.2011.09.005[↩]
- Sanchez-Hernandez M.C., Campo P., Benitez del Castillo J.M., Merayo-Lloves J., Montero J., Valero A., Antón E., Rondon C., Matheu V., Fernández-Parra B., et al. Consensus document on allergic conjunctivitis (DECA) J. Investig. Allergol. Clin. Immunol. 2015;25:94–106.[↩][↩][↩][↩][↩][↩]
- Abelson M.B., Shetty S., Korchak M., Butrus S.I., Smith L.M. Advances in pharmacotherapy for allergic conjunctivitis. Expert. Opin. Pharmacother. 2015;16:1219–1231. doi: 10.1517/14656566.2015.1040760[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Bielory B.P., O’Brien T.P., and Bielory L. Management of seasonal allergic conjunctivitis: Guide to therapy. Acta Ophthalmol 90: 399–407, 2012.[↩][↩][↩]
- Abelson M.B., and Gomes P.J. Olopatadine 0.2% ophthalmic solution: The first ophthalmic antiallergy agent with once-daily dosing. Expert Opin Drug Metab Toxicol 4: 453–461, 2008.[↩]
- Greiner JV, Edwards-Swanson K, Ingerman A. Evaluation of alcaftadine 0.25% ophthalmic solution in acute allergic conjunctivitis at 15 minutes and 16 hours after instillation versus placebo and olopatadine 0.1%. Clin Ophthalmol. 2011 Jan 13;5:87-93. doi: 10.2147/OPTH.S15379[↩]
- Ackerman S, D’Ambrosio F Jr, Greiner JV, Villanueva L, Ciolino JB, Hollander DA. A multicenter evaluation of the efficacy and duration of action of alcaftadine 0.25% and olopatadine 0.2% in the conjunctival allergen challenge model. J Asthma Allergy. 2013 Apr 8;6:43-52. doi: 10.2147/JAA.S38671[↩]
- Kari O., Saari K.M. Updates in the treatment of ocular allergies. J. Asthma Allergy. 2010;3:149–158. doi: 10.2147/JAA.S13705[↩]
- Berger W., Gomes P.J., Beck M., Kimura S., Westbrook T., Storms W., Galant S. Effects of adjuvant therapy with 0.1% olopatadine hydrochloride ophthalmic solution on quality of life in patients with allergic rhinitis using systemic or nasal therapy. Ann. Allergy Asthma Immunol. 2005;95:361–371. doi: 10.1016/S1081-1206(10)61155-6[↩]
- Kam K.W., Chen L.J., Wat N., Young A.L. Topical Olopatadine in the Treatment of Allergic Conjunctivitis: A Systematic Review and Meta-analysis. Ocul. Immunol. Inflamm. 2017;25:663–677. doi: 10.3109/09273948.2016.1158282[↩]
- Dordal M.T., Lluch-Bernal M., Sánchez M.C., Rondón C., Navarro A., Montoro J., Matheu V., Ibáñez M.D., Fernández-Parra B., Dávila I. Allergen-specific nasal provocation testing: Review by the rhinoconjunctivitis committee of the Spanish Society of Allergy and Clinical Immunology. J. Investig. Allergol. Clin. Immunol. 2011;21:1–12. quiz 12.[↩][↩][↩]
- Mishra G.P., Tamboli V., Jwala J.K., Mitra A. Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat. Inflamm. Allergy Drug Discov. 2011;5:26–36. doi: 10.2174/187221311794474883[↩][↩]
- Swamy B.N., Chilov M., McClellan K., Petsoglou C. Topical non-steroidal anti-inflammatory drugs in allergic conjunctivitis: Meta-analysis of randomized trial data. Ophthalmic Epidemiol. 2007;14:311–319. doi: 10.1080/09286580701299411[↩]
- Carnahan MC, Goldstein DA. Ocular complications of topical, peri-ocular, and systemic corticosteroids. Curr Opin Ophthalmol. 2000 Dec;11(6):478-83. doi: 10.1097/00055735-200012000-00016[↩]
- O’Brien TP. Allergic conjunctivitis: an update on diagnosis and management. Curr Opin Allergy Clin Immunol. 2013 Oct;13(5):543-9. doi: 10.1097/ACI.0b013e328364ec3a[↩]
- Singh S, Pal V, Dhull CS. Supratarsal injection of corticosteroids in the treatment of refractory vernal keratoconjunctivitis. Indian J Ophthalmol. 2001 Dec;49(4):241-5.[↩]
- Hoy SM. Ciclosporin Ophthalmic Emulsion 0.1%: A Review in Severe Dry Eye Disease. Drugs. 2017;77:1909–1916. doi: 10.1007/s40265-017-0834-x[↩][↩]
- Bielory L, Schoenberg D. Ocular allergy: update on clinical trials. Curr Opin Allergy Clin Immunol. 2010;19:495–502. doi: 10.1097/ACI.0000000000000564[↩][↩]
- De Bosscher K, Haegeman G, Elewaut D. Targeting inflammation using selective glucocorticoid receptor modulators. Curr Opin Pharmacol. 2010;10:497–504. doi: 10.1016/j.coph.2010.04.007[↩]
- Bozkurt MK, Tülek B, Bozkurt B, Akyürek N, Öz M, Kiyici A. Comparison of the efficacy of prednisolone, montelukast, and omalizumab in an experimental allergic rhinitis model. Turk J Med Sci. 2014;44:439–447. doi: 10.3906/sag-1212-23[↩]
- van der Schaft J, Thijs JL, de Bruin-Weller MS, Balak DMW. Dupilumab after the 2017 approval for the treatment of atopic dermatitis: what’s new and what’s next? Curr Opin Allergy Clin Immunol. 2019;19:341–349. doi: 10.1097/ACI.0000000000000551[↩]
- Nahum Y, Mimouni M, Livny E, Bahar I, Hodak E, Leshem YA. Dupilumabinduced ocular surface disease (DIOSD) in patients with atopic dermatitis: clinical presentation, risk factors for development and outcomes of treatment with tacrolimus ointment. Br J Ophthalmol. 2020;104:776–779. doi: 10.1136/bjophthalmol-2019-315010[↩]
- Amparo F, Dastjerdi MH, Okanobo A, Ferrari G, Smaga L, Hamrah P, Jurkunas U, Schaumberg DA, Dana R. Topical interleukin 1 receptor antagonist for treatment of dry eye disease: a randomized clinical trial. JAMA Ophthalmol. 2013;131:715–723. doi: 10.1001/jamaophthalmol.2013.195[↩]
- Tauber J, Karpecki P, Latkany R, Luchs J, Martel J, Sall K, Raychaudhuri A, Smith V, Semba CP; OPUS-2 Investigators. Lifitegrast Ophthalmic Solution 5.0% versus Placebo for Treatment of Dry Eye Disease: Results of the Randomized Phase III OPUS-2 Study. Ophthalmology. 2015;122:2423–2431. doi: 10.1016/j.ophtha.2015.08.001[↩]
- Moote W, Kim H, Ellis AK. Allergen-specific immunotherapy. Allergy Asthma Clin Immunol. 2018;14(Suppl 2):53. doi: 10.1186/s13223-018-0282-5[↩]
- Calderon MA, Penagos M, Sheikh A, Canonica GW, Durham S. Sublingual immunotherapy for treating allergic conjunctivitis. Cochrane Database Syst Rev. 2011;7:CD007685. doi: 10.1002/14651858.CD007685.pub2[↩][↩][↩][↩]
- Roberts G, Pfaar O, Akdis CA, et al. EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis. Allergy. 2018;73:765–798. doi: 10.1111/all.13317[↩]
- Iyer G, Agarwal S, Srinivasan B. Outcomes and Rationale of Excision and Mucous Membrane Grafting in Palpebral Vernal Keratoconjunctivitis. Cornea. 2018;37:172–176. doi: 10.1097/ICO.0000000000001421[↩][↩]
- Bielory BP, Shah SP, O’Brien TP, Perez VL, Bielory L. Emerging therapeutics for ocular surface disease. Curr Opin Allergy Clin Immunol. 2016;16:477–486. doi: 10.1097/ACI.0000000000000309[↩][↩][↩][↩]
- Addis H, Jeng BH. Vernal Keratoconjunctivitis. Clinical Ophthalmol. 2018;12:119–123. doi: 10.2147/OPTH.S129552[↩]
- Nishiwaki-Dantas MC, Dantas PE, Pezzutti S, Finzi S. Surgical resection of giant papillae and autologous conjunctival graft in patients with severe vernal keratoconjunctivitis and giant papillae. Ophthalmic Plast Reconstr Surg. 2000;16:438–442. doi: 10.1097/00002341-200011000-00007[↩]
- Guo P, Kheirkhah A, Zhou WW, Qin L, Shen XL. Surgical resection and amniotic membrane transplantation for treatment of refractory giant papillae in vernal keratoconjunctivitis. Cornea. 2013;32:816–820. doi: 10.1097/ICO.0b013e31826a1e53[↩]
- Irkeç MT, Orhan M, Erdener U. Role of tear inflammatory mediators in contact lens-associated giant papillary conjunctivitis in soft contact lens wearers. Ocul Immunol Inflamm. 1999;7:35–38. doi: 10.1076/ocii.7.1.35.8107[↩]
- Jabbehdari S, Starnes TW, Kurji KH, Eslani M, Cortina MS, Holland EJ, Djalilian AR. Management of advanced ocular surface disease in patients with severe atopic keratoconjunctivitis. Ocul Surf. 2019;17:303–309. doi: 10.1016/j.jtos.2018.12.002[↩]





{kind=link}