Contents
Perforated bowel
Perforated bowel is a hole in the wall of the small intestine (small bowel perforation) or large intestine (large bowel perforation), which is a life-threatening condition associated with mortality ranging from 30 to 50% 1, 2, 3, 4, 5. Perforation of the small intestine or large intestine causes the intestinal contents to leak into your abdomen. These contents can range from highly acidic gastric contents in more proximal bowel perforation, to fecal material from a more distal area of perforation. These contents can cause a severe infection called peritonitis, which is a life-threatening emergency that needs emergency surgery to repair the hole, stop the bleeding, remove the obstruction, infection, or ischemia. Symptoms of perforated bowel may include sudden and severe constant abdominal pain, nausea and vomiting, fever or chills, swelling and bloating of the abdomen, and inability to pass wind or stool and in severe cases sepsis (a life-threatening emergency that happens when your body’s response to an infection damages vital organs) and shock (a life-threatening condition that occurs when your body doesn’t get enough blood flow).
Your intestines can be damaged and perforated by a range of conditions, including 1, 2, 6, 7, 8, 9, 10, 11, 12, 13, 14:
- trauma, injury (e.g., blunt force trauma such as from a car accident or penetrating injuries such as from a knife or gunshot wound) or swallowing a foreign object
- bowel obstruction
- severe constipation or fecal impaction (e.g., stercoral perforation)
- medical procedures (e.g., after digestive surgery, colonoscopy or endoscopy). The overall incidence of perforation from colonoscopy has been reported, on average, around 2% with higher rates during colonoscopy requiring therapeutic interventions 15
- diverticulitis and inflammatory bowel disease such as Crohn’s disease or ulcerative colitis
- burst appendix or appendicitis
- a tumor that grows through the wall of your intestine (e.g., colorectal cancer or colon perforation from obstruction by distal colon cancer or extracolonic tumor)
- vascular disorders e.g., mesenteric ischemia, ischemic colitis or connective tissue disorders
- chemotherapy drugs
- radiation therapy to your pelvis or abdomen
- ingestion of caustic substances
- drug-induced ulcers (e.g., non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids are the most common)
- forceful vomiting
- bowel perforation in neonates is often due to necrotizing enterocolitis
In children, bowel perforation is most likely to follow abdominal trauma 1. The incidence of bowel perforation is 1% to 7% in pediatric trauma patients 1.
In adults, ulcerative disease represents the most common cause of bowel perforation, with duodenal ulcers causing 2- to 3-times the rate of perforation than gastric ulcers do 1. Perforation secondary to diverticular disease represents up to 15% of cases. In the elderly population, perforated appendicitis represents the most common cause of perforation 1.
It’s important to get treatment fast for perforated bowel. To diagnose a perforated bowel, a doctor talks with you about your medical history and gives you a physical exam. Your symptoms alone may be enough for your doctor to diagnose a perforated bowel.
If more tests are needed to confirm a diagnosis, your doctor may suggest:
- Abdominal and upright chest x-rays are quick and cheap and can identify even small amounts of pneumoperitoneum. X-rays of the chest or abdomen which may show air in your abdominal cavity. This is called free air. It is a sign of a perforation. If the esophagus is perforated free air can be seen in the mediastinum (the space between your lungs in the chest that contains the heart, trachea and esophagus) around your heart and in your chest. You also may have a test that uses sound waves to make images inside your body, called ultrasound.
- Colonic perforation tends to result in a greater amount of pneumoperitoneum than free fluid 16
- Upper gastrointestinal tract perforation tends to present with a relatively large volume of free fluid and less pneumoperitoneum 16
- The presence of pneumoperitoneum in the periportal region is also suggestive of upper gastrointestinal perforation 17
- CT scan of the abdomen and pelvis is the most sensitive and specific test to diagnose a perforation and ascertain the most likely cause 18. Disease processes such as diverticulitis, appendicitis, and bowel obstructions can be readily identified on CT scan. The use of intravenous contrast is recommended to aid in visualizing potential areas of ischemia. Complications from a perforation such as an abscess and secondary bowel obstruction can also be identified with CT scan and guide management accordingly.
- Blood tests. A sample of your blood may be taken to see if you have an increase in disease-fighting white blood cells. This is usually a sign of an infection or inflammation. You also might have a blood culture test to find out if bacteria are in your blood.
- Peritoneal fluid analysis. In this test, a thin needle is used to take a sample of the fluid in your peritoneum. You’re more likely to have this test if you get peritoneal dialysis or if you have fluid in your abdomen from liver disease. An increased white blood cell count in this fluid usually points to an infection or inflammation. A culture of the fluid may be used to spot bacteria.
- A procedure may help find the area of the perforation, such as an upper endoscopy (EGD) or a colonoscopy.
- In children, the preferred primary test is ultrasound given its ease and lack of radiation exposure. However, ultrasound is especially dependent on the experience level of the operator. If necessary, secondary testing such as x-ray, MRI, and CT are reasonable options 19.
Perforated bowel treatment most often involves emergency surgery to repair the hole 20. Sometimes, a small part of the intestine must be removed. One end of the intestine may be brought out through an opening called stoma made in your abdominal wall. This is called a colostomy or ileostomy. A drain from the abdomen or other organ may also be needed. In rare cases, people can be treated with antibiotics alone if the perforation has closed. Antibiotics clear out the infection and keep it from spreading. The type of antibiotic you’ll need and how long you’ll have to take it will vary. It depends on how serious your condition is and the kind of peritonitis you have. This can be confirmed by a physical exam, blood tests, CT scan, and x-rays.
A perforation from a colonoscopy may sometimes be closed during the procedure without surgery.
Contained or controlled bowel perforations can be managed conservatively with interventional radiology guided drainage of fluid collections 21. However, the failure of conservative management with persistence of symptoms and/or development of sepsis necessitate surgical intervention.
Historically, laparotomy has been the intervention of choice for acute abdomen; recently, however, laparoscopic exploration has emerged as a viable option to identify and treat the source of perforation 22. Resection or repair of the perforated site with or without drainage and diversion is usually undertaken. Duodenal perforations, on the other hand, are generally treated with omental patch repair without resection. Risks and benefits of surgery, particularly amongst elderly patient and those with medical conditions, should be thoroughly discussed before offering surgical intervention 23.
Surgery is successful most of the time. Your health status before the perforation occurs best predicts your outcome (prognosis). However, the outcome (prognosis) will depend on how severe the perforation is, and for how long it was present before treatment. The presence of other illnesses, septic shock and your age can also affect how well you will do after treatment.
Figure 1. Gastrointestinal tract anatomy
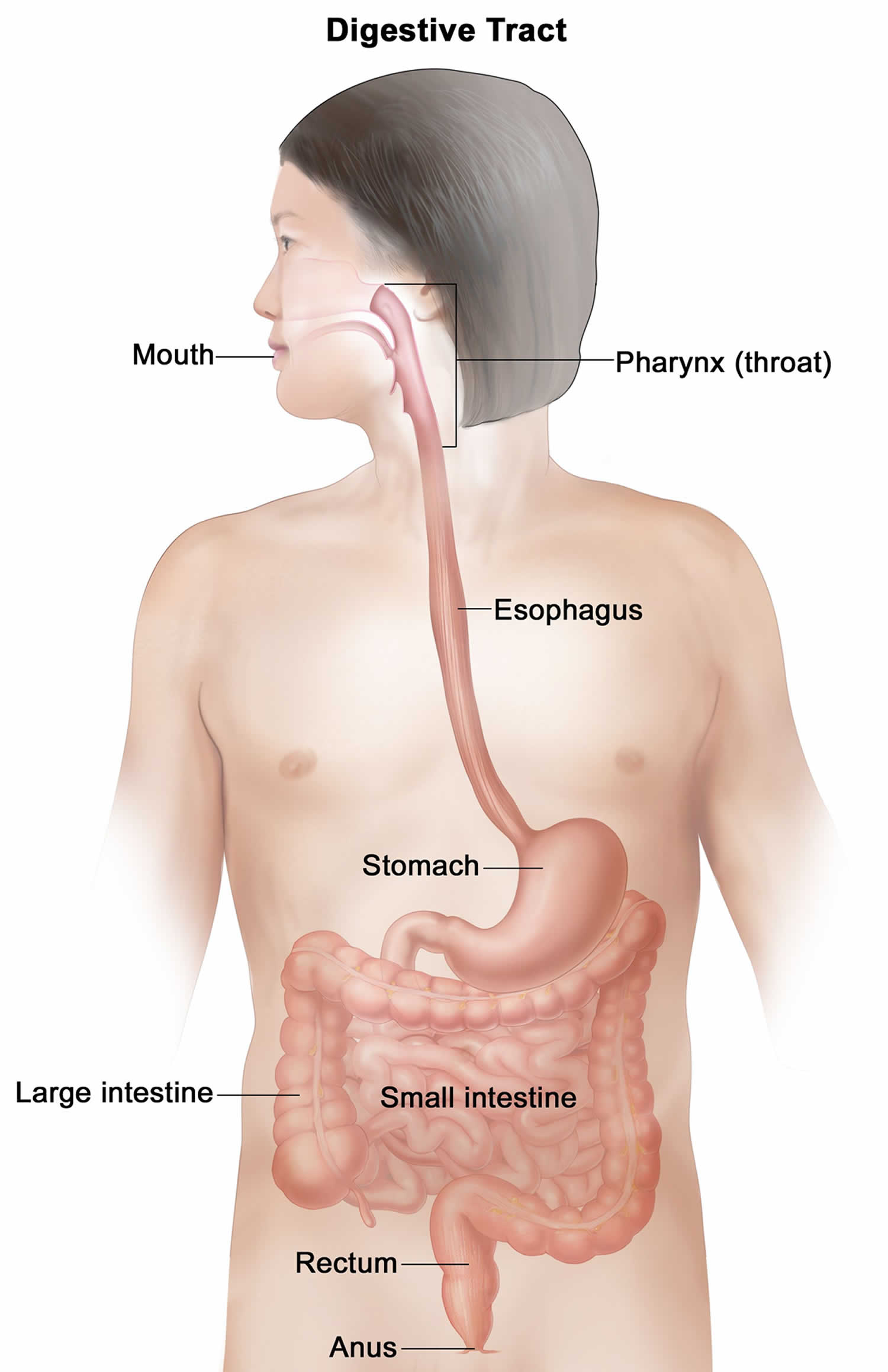
Figure 2. Bowel perforation with massive pneumoperitoneum

Footnotes: Bowel perforation with massive pneumoperitoneum evident by the excessive free gas in the abdominal cavity, including the bilateral subphrenic spaces and surrounding the edges of the liver (hepatic edge sign). Bowel double wall sign or Rigler sign is well-demonstrated. Some of the bowel loops are significantly dilated. Gas-fluid levels are seen in the dilated lower abdominal loops. No rectal gas is seen.
[Source 24 ]Figure 3. Small bowel perforation

Footnotes: Traumatic small bowel perforation in a construction worker where a metal bar fell on his abdomen 10 days prior. Initial CT was reported to be normal. Now peritonitic. 12 cm gas and fluid-filled walled-off collection in the midline of the abdomen largely occupying the small bowel mesentery. Suspicion of occasional bleb of intraperitoneal gas adjacent to the collection. Dilated fluid-filled small bowel distally in the pelvis. Small volume pelvic free fluid. Small bowel loops laterally in the left side of the abdomen indicating an element of malrotation. The solid organs are normal. Normal large bowel.
Comment: Enlarged intra-abdominal fluid collection, appears related to the mesentery and small bowel.
[Source 25 ]Figure 4. Large bowel obstruction and perforation

Footnotes: 75 year old male with short history of abdominal distension and no motion passed for 2 days. (Top image) Abdominal X-ray showing the large bowel is grossly dilated down to the level of a cut-off at the junction of the distal descending and sigmoid colon. The small bowel is moderately dilated. (Bottom image) Non contrast CT scan due to renal impairment showing 4.5cm stenosing tumor at the junction of the sigmoid and descending colon with resultant dilatation of the large bowel upto 9cm. Blebs of intramural gas throughout the colon. The distal small bowel is dilated due to a incompetent ileocecal valve. Multiple foci of pneumoperitoneum in the mid and upper abdomen. No overt infradiaphrgamatic nodes. At least two right lower lobe lung nodules, the largest 8mm.
[Source 26 ]Perforated bowel can be life-threatening if you don’t get medical treatment quickly. See a doctor right away if you have severe pain or tenderness of your abdomen, bloating or a feeling of fullness along with:
- Fever.
- Upset stomach and vomiting.
- Reduced urine.
- Thirst.
- Not able to pass stool or gas.
Perforated bowel also might happen after a burst appendix or a serious injury to your abdomen.
- Get medical help right away if you have severe abdominal pain. Your abdominal pain may feel so bad that you can’t sit still or find a comfortable position.
- Call your local emergency number or get emergency medical care if you have severe belly pain after an accident or injury.
Perforated bowel causes
Bowel perforation results from a destruction of the mucosal layers of the intestinal tract resulting in the spilling of air and digestive contents into the peritoneal cavity. Your intestines can be damaged and perforated by a range of conditions, including 27, 6, 7, 8, 9, 10, 11, 12, 13, 14:
- Bowel obstruction (both small and large intestine)
- Bowel ischemia e.g., mesenteric ischemia, ischemic colitis or connective tissue disorders
- Severe ulcer disease
- Trauma, injury (e.g., blunt force trauma such as from a car accident or penetrating injuries such as from a knife or gunshot wound) or swallowing a foreign object
- Severe constipation or fecal impaction
- Medical procedures (e.g., after digestive surgery, colonoscopy or endoscopy). The overall incidence of perforation from colonoscopy has been reported, on average, around 2% with higher rates during colonoscopy requiring therapeutic interventions 15
- Diverticulitis and inflammatory bowel disease such as Crohn’s disease or ulcerative colitis
- Burst appendix or appendicitis
- Gastrointestinal tumors that grow through the wall of your intestine (e.g., colorectal cancer or colon perforation from obstruction by distal colon cancer or extracolonic tumor)
- Chemotherapy drugs
- Radiation therapy to your pelvis or abdomen
- Ingestion of caustic substances
- Drug-induced ulcers (e.g., non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids are the most common)
- Forceful vomiting
- Bowel perforation in neonates is often due to necrotizing enterocolitis
Upper gastrointestinal perforation (stomach and duodenum) is most commonly caused by peptic ulcer disease with severe epigastric or back pain, with acute onset 1, 2. Sometimes there are chronic symptoms leading up to the perforation event, such as dyspepsia, bloating, nausea, and early satiety 11. Less commonly, cancer or traumatic perforation are possibilities. Imaging usually shows upper abdominal free air and possible leakage of contents into the peritoneal cavity. Usage of oral contrast can be seen extravasating soon after ingestion. Acute onset of periumbilical pain, nausea, vomiting, and decreased bowel function are symptoms of bowel obstruction 2. Imaging suggesting free intraperitoneal air with dilated small or large bowel can signify this as a source of perforation 2. Presence of an incarcerated hernia, history of abdominal surgery, or findings of intussusception on imaging sometimes is present in these cases 28.
Large intestine perforation should be considered with a history of left lower quadrant or history of diverticulitis also usually with decreased stool output 1, 2. Colon cancer is a consideration also, especially with lack of endoscopy screening history. Imaging typically shows free air located near the area of perforation with possible abscess formation present due to the leakage of stool into the peritoneal cavity 10. Rarely, free intraperitoneal air can be caused by benign pneumatosis intestinalis (a very rare condition where multiple gaseous cysts form in the wall of the small or large intestines) unrelated to ischemia and can be managed without surgical intervention 29.
In children, bowel perforation is most likely to follow abdominal trauma 1. The incidence of bowel perforation is 1% to 7% in pediatric trauma patients 1.
In adults, ulcerative disease represents the most common cause of bowel perforation, with duodenal ulcers causing 2- to 3-times the rate of perforation than gastric ulcers do 1. Perforation secondary to diverticular disease represents up to 15% of cases. In the elderly population, perforated appendicitis represents the most common cause of perforation 1.
Perforated bowel pathophysiology
There are 4 mechanisms that can lead to a intestinal tract perforation. A thorough understanding of these mechanisms is critical to guide the appropriate workup and management 2:
- Ischemia (bowel obstruction, necrosis)
- Numerous causes can lead to ischemia and perforation. In the case of bowel obstruction (small or large intestine), the physical distention of the bowel wall results in decreased perfusion 8. This ultimately leads to full thickness wall necrosis and subsequent perforation. Bowel obstruction due to adhesions is more common in patients with a prior history of surgery, but can also result from herniation and strangulation, inflammation, tumors, and foreign bodies. Decreased end-organ perfusion secondary to thrombotic or embolic disease can also result in full-thickness ischemia and perforation. This is more common in older patients, particularly those with a history of smoking, coronary artery disease, or clotting disorders 30.
- Infection (appendicitis, diverticulitis)
- The most common infectious causes of perforation are appendicitis and diverticulitis. Appendicitis can be considered at any age, whereas diverticulitis is more common beyond middle age 10. Both disease processes are usually presumed to be the result of entrapped fecal material in a blind ending structure, leading to increased intraluminal pressure, stasis, and infection leading to a localized abscess or frank perforation. Inflammatory diseases of the bowel, such as Crohn disease and ulcerative colitis can also lead to perforation, especially Crohn’s, which is characterized by full thickness inflammation of the bowel wall 31.
- Erosion (cancer, ulcerative disease)
- Erosive diseases, such as the local invasion of the wall of a viscus by a tumor or ulcerative disease, can also cause perforation. Stercoral perforation is a rare tear in the colon wall caused by hardened feces that is increasingly being recognized as a complication of severe constipation. In peptic ulcer disease, there is direct erosion through the layers of the bowel wall by the ulcer itself, usually due to Helicobacter pylori infection, acid overproduction, or lack of acid protective mechanisms 11. Tumors of the gastrointestinal (GI) tract are most commonly adenocarcinomas, which arise from the mucosa and, in advanced stages, can result in transmural invasion and perforation 32.
- Physical disruption (trauma, iatrogenic injury)
In addition to the mechanisms that can lead to a intestinal tract perforation, the variation in bacterial flora between the upper and lower intestinal tract must also be considered. For example, upper intestinal perforations proximal to the ligament of Trietz result in significantly less bacterial contamination than distal colonic perforations. In the treatment of distal perforations, antibiotics must include gram-negative and anaerobic coverage 34.
Perforated bowel prevention
People will often have a few days of pain before the intestinal perforation occurs. If you have pain in the abdomen, see your doctor right away. Treatment is much simpler and safer when it is started before the perforation occurs.
Perforated bowel signs and symptoms
Perforation of the intestine or other organs causes the intestinal contents to leak into your abdomen. This can lead to peritonitis and eventually sepsis if left untreated.
Perforated bowel symptoms may include:
- Severe abdominal pain
- Chills
- Fever
- Nausea
- Vomiting
- Shock
Perforated bowel signs and symptoms varies: esophageal perforations can present with non-specific symptoms such as acute chest pain, painful swallowing (odynophagia) and vomiting 5, gastroduodenal perforations typically present with acute abdominal pain 4, 35, whereas colonic perforations tend to follow a slower progression course, presenting with secondary bacterial peritonitis or localised abscess formation 4, 36. A subset of patients exhibits delayed symptoms, abscess formation that mimics an abdominal mass, or with sepsis 35.
Almost all patients with bowel perforation experience some element of abdominal pain, and this is usually accompanied by nausea, vomiting, decreased bowel function, or fever 2. Details about the symptoms including the length of time, prior episodes, recent procedures such as endoscopic retrograde cholangiopancreatography (ERCP) and colonoscopy and exacerbating and relieving factors can be crucial in determining the cause of the perforation 37, 38. A family history of cancer and a personal history of colonoscopy can be important to determine the likelihood of occult cancer or inflammatory bowel disease (IBD).
Perforated bowel complications
Complications caused by an intestinal perforation can be related to the disease process that caused it or the treatments given. Even after surgery for perforated bowel, infection is the most common complication. Infections can be either inside the abdomen such as abdominal abscess (a collection of pus and infected fluid in the abdomen) or peritonitis (inflammation of the lining of your belly or abdomen called the peritoneum), or throughout your whole body. Body-wide infection is called sepsis. Sepsis can be very serious and can lead to shock, organ failure and death.
Early complications
- Hemodynamic instability leading to hypoperfusion, shock, and multi-organ system failure, infection (whether local abscess formation, peritonitis, or systemic bacteremia)
Late complications
- Delayed wound healing, postoperative adhesions leading to bowel obstruction, fistula formation, and hernias 20.
Perforated bowel diagnosis
To diagnose a perforated bowel, a doctor talks with you about your medical history and gives you a physical exam. Your symptoms alone may be enough for your doctor to diagnose a perforated bowel.
If more tests are needed to confirm a diagnosis, your doctor may suggest:
- Abdominal and upright chest x-rays are quick and cheap and can identify even small amounts of pneumoperitoneum. X-rays of the chest or abdomen which may show air in your abdominal cavity. This is called free air. It is a sign of a perforation. If the esophagus is perforated free air can be seen in the mediastinum (the space between your lungs in the chest that contains the heart, trachea and esophagus) around your heart and in your chest. You also may have a test that uses sound waves to make images inside your body, called ultrasound.
- Upright chest radiography (50% to 70% sensitive) can help detect free intraperitoneal air below the diaphragm suggestive of bowel perforation 1. The likelihood of diagnosing free air is higher if the patient has been sitting upright for at least 15 minutes prior to the chest radiography 1. Lateral decubitus films can be used if the patient is unable to sit upright.
- Colonic perforation tends to result in a greater amount of pneumoperitoneum than free fluid 16.
- Upper gastrointestinal tract perforation tends to present with a relatively large volume of free fluid and less pneumoperitoneum 16.
- The presence of pneumoperitoneum in the periportal region is also suggestive of upper gastrointestinal perforation 17.
- Up to 40 percent of patients will demonstrate greater than 2 cm of free gas at 24 hours post laparoscopy, without any clinical evidence of bowel perforation 1. After laparotomy, free intra-abdominal gas often may be present for a longer duration postoperatively (up to one week), but the volume should be gradually decreased 1.
- CT scan of the abdomen and pelvis is the most sensitive and specific test to diagnose a perforation and ascertain the most likely cause 18. Disease processes such as diverticulitis, appendicitis, and bowel obstructions can be readily identified on CT scan. The use of intravenous contrast is recommended to aid in visualizing potential areas of ischemia. Complications from a perforation such as an abscess and secondary bowel obstruction can also be identified with CT scan and guide management accordingly.
- Blood tests. A sample of your blood may be taken to see if you have an increase in disease-fighting white blood cells. This is usually a sign of an infection or inflammation. You also might have a blood culture test to find out if bacteria are in your blood.
- Peritoneal fluid analysis. In this test, a thin needle is used to take a sample of the fluid in your peritoneum. You’re more likely to have this test if you get peritoneal dialysis or if you have fluid in your abdomen from liver disease. An increased white blood cell count in this fluid usually points to an infection or inflammation. A culture of the fluid may be used to spot bacteria.
- A procedure may help find the area of the perforation, such as an upper endoscopy (EGD) or a colonoscopy.
- In children, the preferred primary test is ultrasound given its ease and lack of radiation exposure. However, ultrasound is especially dependent on the experience level of the operator. If necessary, secondary testing such as x-ray, MRI, and CT are reasonable options 19.
Perforated bowel differential diagnosis
Perforated bowel differential diagnosis include the following 1:
- Acute cholecystitis and biliary colic
- Acute gastritis
- Acute pancreatitis
- Appendicitis
- Constipation
- Crohn’s disease
- Endometriosis
- Fallopian tube disorders
- Inflammatory bowel disease (IBD)
- Meckel diverticulum surgery
Perforated bowel treatment
Once the initial assessment is complete and bowel perforation is suspected, management can ensue. Many, but not all causes of perforated bowel, require surgery to repair the hole 20. However, all cases should be evaluated by a surgeon 6. Sometimes, a small part of the intestine must be removed. One end of the intestine may be brought out through an opening called stoma made in your abdominal wall. This is called a colostomy or ileostomy. A drain from the abdomen or other organ may also be needed. In rare cases, people can be treated with antibiotics alone if the perforation has closed. Antibiotics clear out the infection and keep it from spreading. The type of antibiotic you’ll need and how long you’ll have to take it will vary. It depends on how serious your condition is and the kind of peritonitis you have. This can be confirmed by a physical exam, blood tests, CT scan, and x-rays.
A perforation from a colonoscopy may sometimes be closed during the procedure without surgery.
Other treatments depend on your symptoms and may include:
- Pain medications.
- Intravenous fluids given through your vein.
- Oxygen.
- In some cases, a blood transfusion.
For both operative and nonoperative patients, initial treatment includes bowel rest, intravenous fluids, intravenous broad-spectrum antibiotics, and frequent abdominal examinations. Instances that are accompanied by sepsis and peritonitis are more likely to require surgery, whereas those that do not need surgery may be amenable to conservative management 39, 40.
Contained or controlled bowel perforations can be managed conservatively with interventional radiology guided drainage of fluid collections 21. However, the failure of conservative management with persistence of symptoms and/or development of sepsis necessitate surgical intervention.
Historically, laparotomy has been the intervention of choice for acute abdomen; recently, however, laparoscopic exploration has emerged as a viable option to identify and treat the source of perforation 22. Resection or repair of the perforated site with or without drainage and diversion is usually undertaken. Duodenal perforations, on the other hand, are generally treated with omental patch repair without resection. Risks and benefits of surgery, particularly amongst elderly patient and those with medical conditions, should be thoroughly discussed before offering surgical intervention 23.
Perforated bowel prognosis
Short- and long-term prognoses of a patient with bowel perforation depend on multiple factors. For instance, your age, medical conditions, benign or malignant cause, and tolerance to treatment are important considerations when discussing prognosis 2, 41. Since surgery is commonly necessary, patients who are unable to tolerate or choose not to undergo surgery when it is required may have a worse prognosis 41.
Risks of abdominal infection, bleeding, potential anastomotic leakage (a serious complication that occurs when the ends of a surgically connected intestines leak), hernia formation from surgical healing 2. Other risks include heart and lung (cardiopulmonary) complications, thromboembolic events (a condition in which a blood clot breaks off from its original site and travels through the bloodstream to obstruct a blood vessel, causing tissue ischemia and organ damage), cardiovascular events, and possible prolonged need for ventilator support must also be discussed as well as expected recovery and possible level of function.
Nationwide mortality (dying) from emergency general surgery cases is 5.0% for patients 65–69 years of age, but increases steadily to 20.4% for patients aged 90 and older 42. Serious morbidity (illness) for this patient group is also high, with a reported range from 17–83% 43, 44, 45, 46. These factors must be discussed candidly with patients and families before surgery, in the elderly especially, to determine their expectations and desires 47.
- Jones MW, Kashyap S, Zabbo CP. Bowel Perforation. [Updated 2023 Apr 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537224[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Hafner J, Tuma F, Hoilat GJ, et al. Intestinal Perforation. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538191[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Pouli, S., Kozana, A., Papakitsou, I. et al. Gastrointestinal perforation: clinical and MDCT clues for identification of aetiology. Insights Imaging 11, 31 (2020). https://doi.org/10.1186/s13244-019-0823-6[↩]
- Langell JT, Mulvihill SJ. Gastrointestinal perforation and the acute abdomen. Med Clin North Am. 2008 May;92(3):599-625, viii-ix. doi: 10.1016/j.mcna.2007.12.004[↩][↩][↩]
- Del Gaizo AJ, Lall C, Allen BC, Leyendecker JR. From esophagus to rectum: a comprehensive review of alimentary tract perforations at computed tomography. Abdom Imaging. 2014 Aug;39(4):802-23. doi: 10.1007/s00261-014-0110-4[↩][↩]
- Tanner TN, Hall BR, Oran J. Pneumoperitoneum. Surg Clin North Am. 2018 Oct;98(5):915-932. doi: 10.1016/j.suc.2018.06.004[↩][↩][↩]
- Grotelüschen R, Bergmann W, Welte MN, Reeh M, Izbicki JR, Bachmann K. What predicts the outcome in patients with intestinal ischemia? A single center experience. J Visc Surg. 2019 Oct;156(5):405-411. doi: 10.1016/j.jviscsurg.2019.01.007[↩][↩]
- Long B, Robertson J, Koyfman A. Emergency Medicine Evaluation and Management of Small Bowel Obstruction: Evidence-Based Recommendations. J Emerg Med. 2019 Feb;56(2):166-176. doi: 10.1016/j.jemermed.2018.10.024[↩][↩][↩]
- Low ZX, Bonney GK, So JBY, Loh DL, Ng JJ. Laparoscopic versus open appendectomy in pediatric patients with complicated appendicitis: a meta-analysis. Surg Endosc. 2019 Dec;33(12):4066-4077. doi: 10.1007/s00464-019-06709-x[↩][↩]
- Špičák J, Kučera M, Suchánková G. Divertikulární choroba: diagnostika a léčba [Diverticular disease: diagnosis and treatment]. Vnitr Lek. 2018 Summer;64(6):621-634. Czech.[↩][↩][↩][↩]
- Kavitt RT, Lipowska AM, Anyane-Yeboa A, Gralnek IM. Diagnosis and Treatment of Peptic Ulcer Disease. Am J Med. 2019 Apr;132(4):447-456. doi: 10.1016/j.amjmed.2018.12.009[↩][↩][↩][↩]
- Zhang L, Wang H. [Imaging characteristics of gastrointestinal neoplastic acute abdomen]. Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Nov 25;21(11):1223-1229. Chinese.[↩][↩]
- Biffl WL, Leppaniemi A. Management guidelines for penetrating abdominal trauma. World J Surg. 2015 Jun;39(6):1373-80. doi: 10.1007/s00268-014-2793-7[↩][↩][↩]
- Song WC, Lv WW, Gao XZ. Iatrogenic Gastrointestinal Perforation Following Therapeutic Endoscopic Procedures: Management and Outcome. J Coll Physicians Surg Pak. 2017 Sep;27(9):563-565.[↩][↩][↩]
- Garrido Serrano A, Fernández Álvarez P. A foreign body in the small bowel: a rare entity of acute abdomen. Rev Esp Enferm Dig. 2019 Jan;111(1):84. doi: 10.17235/reed.2018.5783/2018[↩][↩]
- Bowel perforation. https://radiopaedia.org/articles/bowel-perforation-1[↩][↩][↩][↩]
- Cho HS, Yoon SE, Park SH, Kim H, Lee YH, Yoon KH. Distinction between upper and lower gastrointestinal perforation: usefulness of the periportal free air sign on computed tomography. Eur J Radiol. 2009 Jan;69(1):108-13. doi: 10.1016/j.ejrad.2007.08.024[↩][↩]
- Paolantonio P, Rengo M, Ferrari R, Laghi A. Multidetector CT in emergency radiology: acute and generalized non-traumatic abdominal pain. Br J Radiol. 2016;89(1061):20150859. doi: 10.1259/bjr.20150859[↩][↩]
- Krüger PC, Mentzel HJ. Radiologische Abklärung des akuten Abdomens im Kindesalter [Radiological evaluation of acute abdomen in children]. Radiologe. 2019 Feb;59(2):146-153. German. doi: 10.1007/s00117-018-0464-7[↩][↩]
- Ruscelli P, Renzi C, Polistena A, Sanguinetti A, Avenia N, Popivanov G, Cirocchi R, Lancia M, Gioia S, Tabola R. Clinical signs of retroperitoneal abscess from colonic perforation: Two case reports and literature review. Medicine (Baltimore). 2018 Nov;97(45):e13176. doi: 10.1097/MD.0000000000013176[↩][↩][↩]
- Zhao N, Li Q, Cui J, Yang Z, Peng T. CT-guided special approaches of drainage for intraabdominal and pelvic abscesses: One single center’s experience and review of literature. Medicine (Baltimore). 2018 Oct;97(42):e12905. doi: 10.1097/MD.0000000000012905[↩][↩]
- Siragusa G, Gelarda E, Epifanio E, Geraci F, Geraci G. La videolaparoscopia nelle urgenze addominali [Video laparoscopy in abdominal emergencies]. Minerva Chir. 1999 Apr;54(4):199-204. Italian.[↩][↩]
- Tengberg LT. Perioperative treatment of patients undergoing acute high-risk abdominal surgery . Dan Med J. 2018 Feb;65(2):B5442. https://ugeskriftet.dk/dmj/perioperative-treatment-patients-undergoing-acute-high-risk-abdominal-surgery[↩][↩]
- Pneumoperitoneum. https://radiopaedia.org/cases/pneumoperitoneum-42[↩]
- Traumatic small bowel perforation. https://radiopaedia.org/cases/traumatic-small-bowel-perforation-1[↩]
- Tumoral large bowel obstruction and perforation. https://radiopaedia.org/cases/tumoral-large-bowel-obstruction-and-perforation[↩]
- Ugwu AU, Kerins N, Malik M. Traumatic small bowel perforation in a case of a perineal hernia. J Surg Case Rep. 2018 Dec 12;2018(12):rjy330. doi: 10.1093/jscr/rjy330[↩]
- Bower KL, Lollar DI, Williams SL, Adkins FC, Luyimbazi DT, Bower CE. Small Bowel Obstruction. Surg Clin North Am. 2018 Oct;98(5):945-971. doi: 10.1016/j.suc.2018.05.007[↩]
- Wada K, Takeuchi N, Emori M, Takada M, Nomura Y, Otsuka A. Two Cases of Pneumatosis Cystoides Intestinalis With Intraperitoneal Free Air. Gastroenterology Res. 2017 Jun;10(3):208-211. doi: 10.14740/gr834w[↩]
- Lim S, Halandras PM, Bechara C, Aulivola B, Crisostomo P. Contemporary Management of Acute Mesenteric Ischemia in the Endovascular Era. Vasc Endovascular Surg. 2019 Jan;53(1):42-50. doi: 10.1177/1538574418805228[↩]
- Pavlović-Calić N. Ulcerozni kolitis i Kronova bolest [Ulcerative colitis and Crohn’s disease]. Med Arh. 2003;57(1 Suppl 2):85-6. Bosnian.[↩]
- Ko BM. [Small Bowel Tumors and Polyposis: How to Approach and Manage?]. Korean J Gastroenterol. 2018 Dec 25;72(6):277-280. Korean. doi: 10.4166/kjg.2018.72.6.277[↩]
- Vanaclocha-Espi M, Ibáñez J, Molina-Barceló A, Valverde-Roig MJ, Pérez E, Nolasco A, de la Vega M, de la Lastra-Bosch ID, Oceja ME, Espinàs JA, Font R, Pérez-Riquelme F, Arana-Arri E, Portillo I, Salas D; CRIBEA Group. Risk factors for severe complications of colonoscopy in screening programs. Prev Med. 2019 Jan;118:304-308. doi: 10.1016/j.ypmed.2018.11.010[↩]
- Fan YC, Peery AF. Therapeutic management of acute uncomplicated diverticulitis. Minerva Gastroenterol Dietol. 2017 Jun;63(2):143-151. doi: 10.23736/S1121-421X.16.02361-8[↩]
- Picone D, Rusignuolo R, Midiri F, Lo Casto A, Vernuccio F, Pinto F, Lo Re G. Imaging Assessment of Gastroduodenal Perforations. Semin Ultrasound CT MR. 2016 Feb;37(1):16-22. doi: 10.1053/j.sult.2015.10.006[↩][↩]
- Saturnino PP, Pinto A, Liguori C, Ponticiello G, Romano L. Role of Multidetector Computed Tomography in the Diagnosis of Colorectal Perforations. Semin Ultrasound CT MR. 2016 Feb;37(1):49-53. doi: 10.1053/j.sult.2015.10.007[↩]
- Bill JG, Smith Z, Brancheck J, Elsner J, Hobbs P, Lang GD, Early DS, Das K, Hollander T, Doyle MBM, Fields RC, Hawkins WG, Strasberg SM, Hammill C, Chapman WC, Edmundowicz S, Mullady DK, Kushnir VM. The importance of early recognition in management of ERCP-related perforations. Surg Endosc. 2018 Dec;32(12):4841-4849. doi: 10.1007/s00464-018-6235-8[↩]
- Wang H, Li A, Shi X, Xu X, Wang H, Wang H, Yu E. [Diagnosis and treatment of iatrogenic colonoscopic perforation]. Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Jun 25;21(6):660-665. Chinese.[↩]
- Titos-García A, Aranda-Narváez JM, Romacho-López L, González-Sánchez AJ, Cabrera-Serna I, Santoyo-Santoyo J. Nonoperative management of perforated acute diverticulitis with extraluminal air: results and risk factors of failure. Int J Colorectal Dis. 2017 Oct;32(10):1503-1507. doi: 10.1007/s00384-017-2852-2[↩]
- Nimmagadda N, Matsushima K, Piccinini A, Park C, Strumwasser A, Lam L, Inaba K, Demetriades D. Complicated appendicitis: Immediate operation or trial of nonoperative management? Am J Surg. 2019 Apr;217(4):713-717. doi: 10.1016/j.amjsurg.2018.12.061[↩]
- Ho VP, Schiltz NK, Reimer AP, Madigan EA, Koroukian SM. High-Risk Comorbidity Combinations in Older Patients Undergoing Emergency General Surgery. J Am Geriatr Soc. 2019 Mar;67(3):503-510. doi: 10.1111/jgs.15682[↩][↩]
- Massarweh NN, Legner VJ, Symons RG, McCormick WC, Flum DR. Impact of advancing age on abdominal surgical outcomes. Arch Surg. 2009 Dec;144(12):1108-14. doi: 10.1001/archsurg.2009.204[↩]
- Shah AA, Haider AH, Zogg CK, Schwartz DA, Haut ER, Zafar SN, Schneider EB, Velopulos CG, Shafi S, Zafar H, Efron DT. National estimates of predictors of outcomes for emergency general surgery. J Trauma Acute Care Surg. 2015 Mar;78(3):482-90; discussion 490-1. doi: 10.1097/TA.0000000000000555[↩]
- Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK52651[↩]
- Southern DA, Quan H, Ghali WA. Comparison of the Elixhauser and Charlson/Deyo methods of comorbidity measurement in administrative data. Med Care. 2004 Apr;42(4):355-60. doi: 10.1097/01.mlr.0000118861.56848.ee[↩]
- Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998 Jan;36(1):8-27. doi: 10.1097/00005650-199801000-00004[↩]
- Cooper Z, Lilley EJ, Bollens-Lund E, Mitchell SL, Ritchie CS, Lipstiz SR, Kelley AS. High Burden of Palliative Care Needs of Older Adults During Emergency Major Abdominal Surgery. J Am Geriatr Soc. 2018 Nov;66(11):2072-2078. doi: 10.1111/jgs.15516[↩]





{kind=link}