
Contents
- What is Panic Disorder
- Panic disorder causes
- Panic disorder prevention
- Panic disorder signs and symptoms
- Panic disorder complications
- Panic disorder diagnosis
- Panic disorder treatment
- Panic disorder prognosis
What is Panic Disorder
Panic disorder is a type of anxiety disorder where you regularly experience unexpected panic attacks or sudden attacks of panic or fear 1. Panic disorder is used to describe the condition where panic attacks seem to happen unexpectedly rather than always in predictable situations. A main feature of panic disorder is that the panic attacks usually happen without warning and aren’t due to another mental health or physical condition. Many people experience feelings of anxiety and panic at certain times, it’s a natural response to stressful or dangerous situations. However, someone with panic disorder has more intense feelings of anxiety, stress and panic regularly and these intense sensations occur suddenly at any time, often for no apparent reason. A panic attack is a sudden (without warning) episode of intense fear or discomfort, accompanied by physical symptoms, which can feel like a heart attack, even though it is not dangerous. Panic attacks often feel like a rush of fear or impending doom. A panic attack can be very frightening and you may feel a strong desire to escape the situation or to seek emergency assistance. If frequent or severe, panic attacks can be a sign of panic disorder and should be addressed with professional help.
A person with panic disorder is always worried about the consequences of panic attack or has persistent fear about having more panic attacks. Many people with panic disorder change their behavior to try to prevent panic attacks in maladaptive ways such as avoidance of exercise, withdrawing from work, social activities or unfamiliar locations because of the fear of having another panic attack. Some people are affected so much that they try to avoid any place where it might be difficult to get help or to escape from. When this avoidance is severe it is called agoraphobia. If left
untreated, panic disorder may become accompanied by depression, other anxiety disorders, dependence on alcohol or drugs and may also lead to significant social and occupational impairment 2.
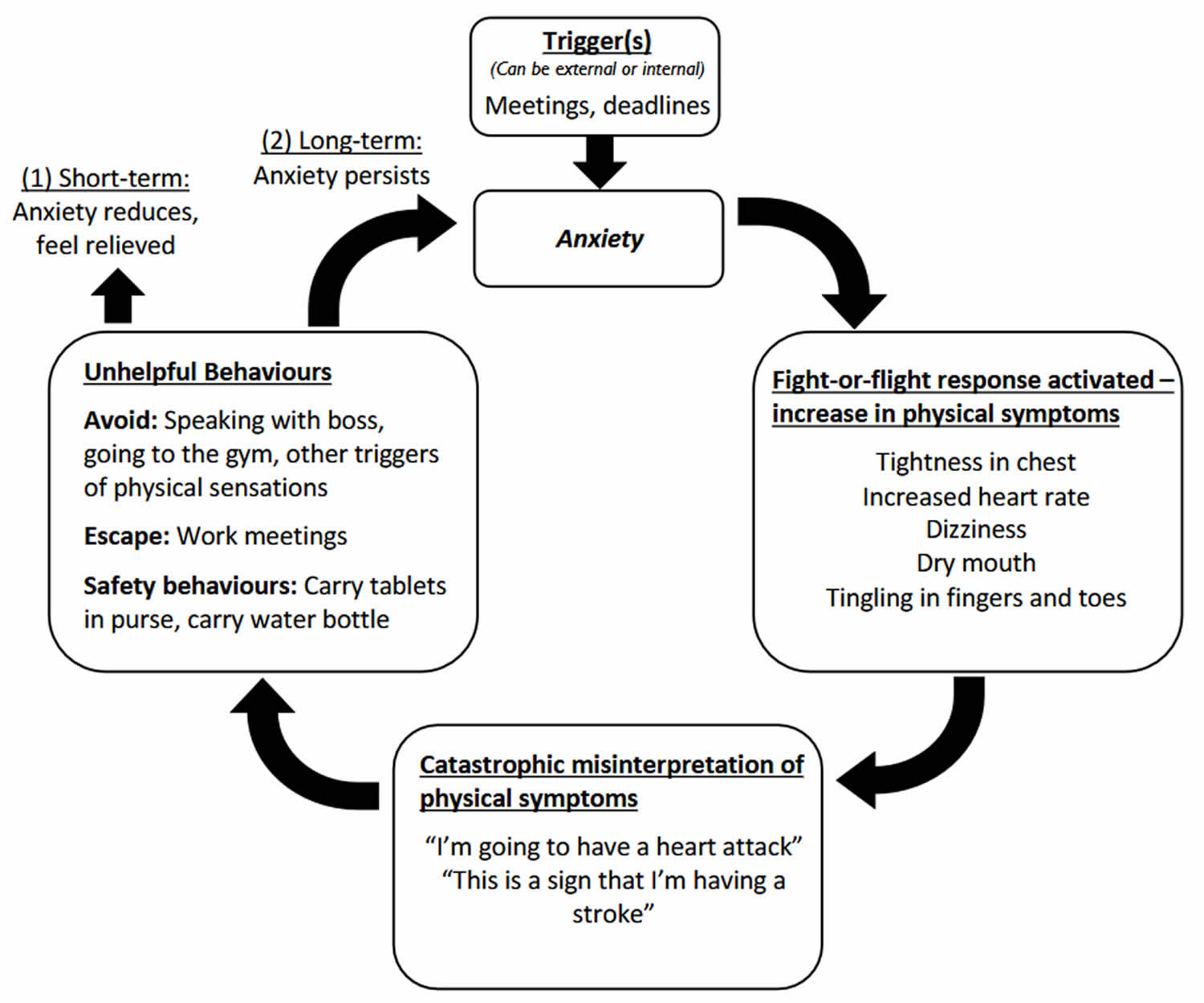
Figure 1. How panic disorder is maintained
Symptoms of panic disorder often start in the late teens or early adulthood and affect more women than men 4, 5, 6, 7, 8. Peak onset of panic disorder is between 15 and 19 years of age 9 and is experienced by around 1% of adolescents 10, 11, increasing to around 3% among older adolescents aged between 17 and 19 years 10, 12. The median age at onset for panic disorder in the United States is 20 to 24 years 13. A small number of cases begin in childhood, and onset after age 45 years is unusual but can occur 13. There are high levels of comorbidity, with around 90% of adolescents with panic disorder experiencing another anxiety or mood disorder 14. Among all anxiety disorders, panic disorder has the highest number of medical visits and serves as a very costly mental health condition.
Although panic disorder is very rare in childhood, first occurrence of “fearful spells” is often dated retrospectively back to childhood. As in adults, panic disorder in adolescents tends to have a chronic course and is frequently occurs with other anxiety, depressive, and bipolar disorders. To date, no differences in the clinical presentation between adolescents and adults have been found. However, adolescents may be less worried about additional panic attacks than are young adults. Lower prevalence of panic disorder in older adults appears to be attributable to age-related “dampening” of the autonomic nervous system (autonomic nervous system is a network of nerves that handle unconscious involuntary physiologic processes like heart rate, blood pressure, respiration, digestion, and sexual arousal) response. Many older individuals with “panicky feelings” are observed to have a “hybrid” of limited-symptom panic attacks and generalized anxiety. Also, older adults tend to attribute their panic attacks to certain stressful situations, such as a medical procedure or social setting. While the low rate of panic disorder in children could relate to difficulties in symptom reporting, this seems unlikely given that children are capable of reporting intense fear or panic in relation to separation and to phobic objects or phobic situations. Adolescents might be less willing than adults to openly discuss panic attacks. Therefore, clinicians should be aware that unexpected panic attacks do occur in adolescents, much as they do in adults, and be attuned to this possibility when encountering adolescents presenting with episodes of intense fear or distress.
Panic attacks typically include some of these signs or symptoms 2:
- Skipping, racing or pounding heart
- Sweating
- Trembling or shaking
- Shortness of breath or difficulty breathing or hyperventilation
- Choking sensations
- Chest pain, pressure or discomfort
- Nausea, stomach problems or sudden diarrhea
- Dizziness, lightheadedness, feeling faint
- Tingling or numbness in parts of your body or in your fingers or toes
- Hot flushes or chills
- Feeling things around you are strange, unreal (derealization), depersonalization (feeling detached from yourself), unfamiliar, or feeling detached from your body
- Thoughts of losing control or going crazy
- Fear of dying
Panic attacks are very unpleasant, distressing and can be frightening. During a panic attack you get a rush of intense mental and physical symptoms. Panic attack can come on very quickly without warning and for no apparent reason. Panic attacks can strike at any time when you’re driving a car, at the mall, sound asleep or in the middle of a business meeting. You may have occasional panic attacks, or they may occur frequently. As you can see from the list, many of the symptoms are similar to what you might experience if you were in a truly dangerous situation. A panic attack can be very frightening and you may feel a strong desire to escape the situation. Many of the symptoms may appear to indicate some medical condition and some people seek emergency assistance. However, panic attacks, while very frightening, are not life-threatening or dangerous or harmful to your health. Following a panic attack, you may feel fatigued and drained, even after the symptoms subside. Frequent panic attacks can lead to a decrease in your quality of life and other psychosocial issues. And not everyone who experiences a panic attack develops panic disorder.
If you’ve had symptoms of a panic attack, it’s important to see a doctor as soon as possible. Your doctor can give you an official diagnosis and ensure there’s no underlying physical cause. Panic attack symptoms can also resemble symptoms of other serious health problems, such as a heart attack, so it’s important to get evaluated by your doctor if you aren’t sure what’s causing your symptoms. Some symptoms that are common to panic attacks may also occur in some physical conditions. Some medications and drugs – such as tranquillizers (also known as anxiolytics or sedatives used to reduce anxiety, tension, and agitation), alcohol and caffeine – may also induce panic-like symptoms.
In order to diagnose your condition, your doctor will ask about your symptoms and medical history. Your doctor may run tests to rule out medical conditions that cause similar symptoms as panic attacks, such as heart disease, thyroid disease and respiratory (breathing) problems. If there’s no underlying physical cause, your doctor may make a diagnosis according to your symptoms and risk factors.
To help diagnose panic disorder, your doctor or a mental health professional may:
- Give you a psychological evaluation. This involves discussing your thoughts, feelings and behavior to help pinpoint a diagnosis and check for related complications. Anxiety disorders often occur along with other mental health problems — such as depression or substance misuse — which can make diagnosis more challenging.
- Compare your symptoms to the criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). See Panic Disorder DSM-5 Diagnostic Criteria below. Many doctors use the criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association, to diagnose panic disorder.
Your doctor may diagnose panic disorder when you have repeated, unexpected panic attacks as well as one month or more of:
- Persistently worrying about having more panic attacks or their consequences.
- Changing your behaviors to avoid situations that you think may trigger an attack.
In addition, the panic attacks can’t be due to the direct effects of a substance or general medical condition. And they can’t be better accounted for by another mental health condition, like a phobia or post-traumatic stress disorder (PTSD).
Panic attacks, while intensely uncomfortable, are not dangerous. But panic attacks are hard to manage on your own, and they may get worse without treatment.
Panic disorder and panic attacks treatment options may include talk therapy (psychotherapy), medications or a combination of both. A form of psychotherapy called cognitive behavioral therapy (CBT) can help you learn, through your own experience, that panic symptoms are not dangerous. Your therapist will help you gradually re-create the symptoms of a panic attack in a safe, repetitive manner. Once the physical sensations of panic no longer feel threatening, the attacks begin to resolve. Successful treatment can also help you overcome fears of situations that you’ve avoided because of panic attacks. How long you’ll need treatment depends on the severity of your condition and how well you respond to treatment.
The usual course, if panic disorder is untreated, is chronic but waxing and waning. Some individuals may have episodic outbreaks with years of remission in between, and others may have continuous severe symptoms. Only a minority of individuals have full remission without subsequent relapse within a few years. The course of panic disorder typically is complicated by a range of other disorders, in particular other anxiety disorders, depressive disorders, and substance use disorders.
What is Anxiety Disorder?
Anxiety disorders are a group of mental health conditions that cause fear, dread and other symptoms that are out of proportion to the situation. If you have an anxiety disorder, you may respond to certain things and situations with fear and dread. You may also experience physical signs of anxiety, such as a pounding heart and sweating. It’s normal to have some anxiety. You may feel anxious or nervous if you have to tackle a problem at work, go to an interview, take a test or make an important decision. Some anxiety can even be beneficial — it helps us notice dangerous situations and focuses our attention so we stay safe. But an anxiety disorder goes beyond the regular nervousness and slight fear you may feel from time to time.
An anxiety disorder happens when:
- Anxiety interferes with your ability to function.
- Your reactions are often out of proportion to situations (overreactions).
- You can’t control your responses to situations.
Children, adolescents and adults can experience anxiety disorders. Women are about twice as likely as men to have one.
According to the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5) 13, there are several types of anxiety disorders that include generalized anxiety disorder (GAD, specific phobias and social anxiety disorder.
Types of Anxiety Disorders 13:
- Generalized Anxiety Disorder (GAD): Excessive worry and anxiety about many things, often without a specific cause. Generalized anxiety disorder (GAD) causes fear, worry and a constant feeling of being overwhelmed. It’s characterized by excessive, frequent and unrealistic worry about everyday things, such as job responsibilities, health or chores.
- Panic Disorder: Sudden, intense episodes of fear or panic, often accompanied by physical symptoms. Panic disorder involves multiple unexpected panic attacks. A main feature of panic disorder is that the panic attacks usually happen without warning and aren’t due to another mental health or physical condition. Some people with panic disorder also have agoraphobia.
- Social Anxiety Disorder (social phobia): Intense fear or anxiety in social situations. Social anxiety disorder previously known as social phobia happens when you experience intense and ongoing fear of being judged negatively and/or watched by others.
- Specific phobias: Intense and irrational fear of specific objects or situations. A phobia is when something causes you to feel fear or anxiety that’s so severe it consistently and overwhelmingly disrupts your life. There are hundreds of different types of phobias, and there’s one diagnosis for almost all of them: specific phobia. Only one phobia, agoraphobia, is a distinct diagnosis.
- Agoraphobia: Fear of situations where escape might be difficult or help unavailable. Agoraphobia causes an intense fear of becoming overwhelmed or unable to escape or get help. People with agoraphobia often avoid new places and unfamiliar situations, like large, open areas or enclosed spaces, crowds and places outside of their homes.
- Separation anxiety disorder (SAD): Separation anxiety disorder happens when you feel intense fear or excessive anxiety when you’re separated from a loved one or a close attachment figure, like a primary caregiver. While separation anxiety in babies and toddlers is a normal stage of development, separation anxiety disorder can affect children and adults.
- Selective mutism: Selective mutism happens when you don’t talk in certain situations because of fear or anxiety. It usually affects young children, but it can also affect adolescents and adults.
Other mental health conditions share features with anxiety disorders. These include post-traumatic stress disorder (PTSD), acute stress disorder (a short-term mental health condition that can develop within a month after a traumatic event, characterized by symptoms like intrusive memories, avoidance behaviors, and increased arousal, similar to PTSD, but with a shorter duration) and obsessive-compulsive disorder (OCD). But the American Psychiatric Association classifies them as distinct conditions and not anxiety disorders 13.
Anxiety disorders can make it difficult to get through the day. Fortunately, there are several effective treatments for these conditions. Treatment is effective and usually includes medication and psychotherapy (talk therapy).
What is panic?
To understand panic, you need to understand fear. Fear is an unpleasant emotion that arises in response to perceived dangers or threats. Fear causes automatic physiological and psychological changes to perceived threats preparing your body to either confront the danger (“fight”) or escape (“flight”). Fear may produce behavioral reactions such as mounting an aggressive response (“fight”) or fleeing the threat (“flight”), commonly known as the “fight-or-flight response”. You can think of fear as an automatic alarm response that switches on the moment there is danger. Think about what would happen to you if a lion approached you. For most people it would be panic stations. You, and almost everyone, would go through a whole series of bodily changes, like your heart pumping faster, breathing faster, your muscle tensing and sweating (the fight-or-flight response) along with other changes, all in order to respond to the danger in front of you. This alarm response would probably lead you to either run for your life or become sufficiently ‘pumped up’ to physically defend yourself. This automatic alarm response is an important survival mechanism called the “fight-or-flight response”.
Sometimes, however, it is possible to have this intense fear response, the “fight-or-flight response”, when there is no danger – it is a false alarm that seems to happen when you least expect it. It is like someone ringing the fire alarm when there is no fire. Essentially, a panic attack is a false alarm. Many people experience some mild sensations when they feel anxious about something, but a panic attack is much more intense than usual. A panic attack is usually described as a sudden escalating surge of extreme fear. Some people portray the experience of panic as ‘sheer terror’.
What are panic attacks?
Panic attacks (the key feature of Panic Disorder) are abrupt surges of intense fear or intense discomfort that reach a peak within minutes, accompanied by physical and/or cognitive symptoms 13. A panic attack happens suddenly. Symptoms usually peak within 10 minutes after it starts and then disappear soon after. Panic attacks can be seen as a blend of biological, emotional and psychological reactions. The emotional response is purely fear. Limited-symptom panic attacks include fewer than four symptoms. Panic attacks may be expected, such as in response to a typically feared object or situation, or unexpected, meaning that the panic attack occurs for no apparent reason 13. Panic attacks function as a marker and prognostic factor for severity of diagnosis, course, and comorbidity across an array of disorders, including, but not limited to, the anxiety disorders (e.g., substance use, depressive and psychotic disorders) 13. Panic attack may therefore be used as a descriptive specifier for any anxiety disorder as well as other mental disorders 13.
Physical symptoms of a panic attack include 2:
- Skipping, racing or pounding heart
- Sweating
- Trembling or shaking
- Shortness of breath or difficulty breathing or hyperventilation
- Choking sensations
- Chest pain, pressure or discomfort
- Nausea, stomach problems or sudden diarrhea
- Dizziness, lightheadedness, feeling faint
- Tingling or numbness in parts of your body or in your fingers or toes
- Hot flushes or chills
- Feeling things around you are strange, unreal (derealization), depersonalization (feeling detached from yourself), unfamiliar, or feeling detached from your body
- Thoughts of losing control or going crazy
- Fear of dying
Panic attacks are very unpleasant and can be frightening. As you can see from the list, many of the symptoms are similar to what you might experience if you were in a truly dangerous situation. A panic attack can be very frightening and you may feel a strong desire to escape the situation. Many of the symptoms may appear to indicate some medical condition and some people seek emergency assistance. However, panic attacks, while very frightening, are not life-threatening or dangerous or harmful to your health. Following a panic attack, you may feel fatigued and drained, even after the symptoms subside. Frequent panic attacks can lead to a decrease in your quality of life and other psychosocial issues. And not everyone who experiences a panic attack develops panic disorder.
If you have panic attacks but not a diagnosed panic disorder, you can still benefit from treatment. If panic attacks aren’t treated, they can get worse and develop into panic disorder or phobias. Treatment can help reduce the intensity and frequency of your panic attacks and improve your function in daily life.
Characteristics of a Panic Attack
- It peaks quickly between 1 to 10 minutes
- The apex of the panic attack lasts for approximately 5 to 10 minutes (unless constantly rekindled)
- The initial attack is usually described as “coming out of the blue” and not consistently associated with a specific situation, although with time panics can become associated with specific situations
- The attack is not linked to marked physical exertion
- The attacks are recurrent over time
- During an attack the person experiences a strong urge to escape to safety
- Many people believe that they may faint whilst having a panic attack. This is highly unlikely because the physiological system producing a panic attack is the opposite of the one that produces fainting.
- Sometimes people have panic attacks that occur during the night when they are sleeping. They wake from sleep in a state of panic. These can be very frightening because they occur without an obvious trigger.
- Panic attacks in, and of themselves, are not a psychiatric condition. However, panic attacks constitute the key ingredient of Panic Disorder if the person experiences at least 4 symptoms of the Panic attack symptoms previously described, the attacks peak within about 10 minutes and the person has a persistent fear of having another attack.
- Panic attacks are the main feature of Panic Disorder. But they can happen alongside other conditions, such as:
- Anxiety disorders
- Mood disorders
- Phobias
- Psychotic disorders
- Substance use disorders
- Trauma- and stressor-related disorders
- Certain medical conditions.
What triggers panic attacks?
There’s often no specific trigger for panic attacks. But people who have a phobia can experience phobia-related triggers that lead to a panic attack. For example, someone with trypanophobia (intense fear of needles) may experience a panic attack if they have to get their blood drawn for a medical test. For some people, the fear of having a panic attack is often enough to trigger one. It’s important to note that one of the criteria for panic disorder is that the panic attacks don’t have a known trigger.
How common are panic attacks?
Panic attacks are common. Every year, up to 11% of people in the United States experience a panic attack. Approximately 2% to 3% of people in the U.S. have panic disorder. Women are two times more likely to have panic disorder than men. In the general population, the 12-month prevalence estimate for panic disorder across the United States and several European countries is about 2%-3% in adults and adolescents. In the United States, significantly lower rates of panic disorder are reported among Latinos, African Americans, Caribbean blacks, and Asian Americans, compared with non-Latino whites; American Indians, by contrast, have significantly higher rates 13.
Lower estimates have been reported for Asian, African, and Latin American countries, ranging from 0.1% to 0.8% 13. Females are more frequently affected than males, at a rate of approximately 2:1 13. The gender differentiation occurs in adolescence and is already observable before age 14 years. Although panic attacks occur in children, the overall prevalence of panic disorder is low before age 14 years (<0.4%) 13. The rates of panic disorder show a gradual increase during adolescence, particularly in females, and possibly following the onset of puberty, and peak during adulthood. The prevalence rates decline in older individuals (i.e., 0.7% in adults over the age of 64), possibly reflecting diminishing severity to subclinical levels 13.
What is the difference between a panic attack and an anxiety attack?
The main difference is that certain stressors often trigger anxiety attacks, and they may build up gradually. In contrast, panic attacks typically happen unexpectedly and suddenly.
Anxiety often causes physical symptoms, such as a racing heart or knots in your stomach. But these symptoms are generally less intense and last longer than a panic attack, which has very intense but brief symptoms.
How can I stop a panic attack?
While there’s no way to immediately stop a panic attack right after it starts, there are steps you can take to manage the symptoms until the attack resolves, including:
- Practicing deep breathing: Hyperventilating is a symptom of panic attacks that can increase fear. Deep breathing can reduce symptoms of panic during an attack. Breathe in as slowly, deeply and gently as you can through your nose and breathe out slowly through your mouth. Close your eyes and focus on your breathing.
- Acknowledging that you’re having a panic attack: Knowing that you’re having a panic attack — and not a dangerous health episode — can help manage the fear you’re experiencing. Remind yourself that the attack is temporary and will pass.
- Relaxing your muscles: Anxiety attacks can cause you to tense your muscles. Focus on relaxing one muscle group at a time to reduce tension and stay present.
- Practicing mindfulness: A panic attack can make you feel detached from reality or your body. Practice mindfulness and focus on the present to center your thoughts and ground yourself.
- Avoid ‘self-talk’ that focuses your attention on your symptoms – don’t tell yourself ‘Stop panicking!’ or ‘Relax!’
- Remind yourself that the symptoms of a panic attack are uncomfortable, but not life threatening. Reassure yourself that you’ve felt these feelings before and nothing bad happened to you.
- Focus your attention on something outside your own body and symptoms. For example, distract yourself by counting backwards in threes from 100, recall the words from a favorite song or concentrate on the sights and sounds around you.
- Fleeing from the situation will only reinforce the perception that your panic attacks are unbearable. If you sit and allow the symptoms to pass, you gain confidence in your ability to cope.
It’s important to seek medical treatment, like medication and psychotherapy, if you’re having frequent panic attacks.
What to do during a panic attack
The next time you feel a panic attack coming on:
- stay where you are, if possible
- breathe slowly and deeply
- remind yourself that the attack will pass
- focus on positive, peaceful and relaxing images
- remember it’s not life threatening
How can I help someone who’s having a panic attack?
If someone you know is having a panic attack, you can do the following to help them:
- Stay with them and remain calm.
- Ask them what they need.
- Speak to them in short, simple sentences.
- Help them focus on the present.
- Help them practice deep breathing by slowly counting to five for each inhale and exhale.
- Gently and confidently reassure them that they’re safe and that the attack is temporary.
Panic disorder causes
It’s not known what causes panic attacks or panic disorder, but scientists think panic attacks and panic disorder are caused by a combination of genetic, environmental, and psychological factors 1, 4, 15, 16, 17:
- Chemical imbalances: Several neurotransmitters and hormones play a role in anxiety, including norepinephrine (noradrenaline), serotonin, dopamine and gamma-aminobutyric acid (GABA). Neurotransmitters are chemical messengers that transmit signals between neurons (nerve cells) or from neurons to other cells like muscles or glands, enabling communication and function throughout the nervous system. Imbalances in these chemicals can contribute to an anxiety disorder.
- Brain changes: A part of your brain called the amygdala plays an important role in managing fear and anxiety and other emotions. Studies show that people with anxiety disorders show increased amygdala activity in response to anxiety cues.
- Genetics: Anxiety disorders tend to run in biological families. This suggests that genetics may play a role. You may be at an increased risk of developing one if you have a first-degree relative (biological parent or sibling) with an anxiety disorder.
- Environmental factors: Severe or long-lasting stress can change the balance of neurotransmitters that control your mood. Experiencing a lot of stress over a long period can contribute to an anxiety disorder. Experiencing a traumatic event can also trigger anxiety disorders.
- Stressful life events, trauma, and certain medical conditions can also contribute to the development of anxiety disorders.
Panic attacks may come on suddenly and without warning at first, but over time, they’re usually triggered by certain situations. Some research suggests that your body’s natural “fight-or-flight” response to danger is involved in panic attacks. For example, if a grizzly bear came after you, your body would react instinctively. Your heart rate and breathing would speed up as your body prepared for a life-threatening situation. Many of the same reactions occur in a panic attack. But it’s unknown why a panic attack occurs when there’s no obvious danger present.
The ‘flight-or-fight’ response
When your body is faced with immediate danger, your brain orders the autonomic nervous system to activate the “flight-or-fight” response. Your body is then flooded with a range of chemicals, including norepinephrine (noradrenaline) and serotonin that trigger physiological changes. For example, your heart rate and breathing are accelerated and blood is shifted to your muscles to prepare for physical combat or running away. A panic attack is said to occur when the ‘flight-or-fight’ response is triggered but there is no danger about to happen. A person may experience the symptoms of a panic attack in harmless and apparently stress-free situations, such as watching television or while asleep.
Some of the factors that can prime the body to inappropriately activate the ‘flight-or-fight’ response include:
- Chronic (ongoing) stress – this causes the body to produce higher than usual levels of stress chemicals such as adrenaline.
- Acute stress (such as experiencing a traumatic event) – can suddenly flood the body with large amounts of stress chemicals.
- Habitual hyperventilation – disturbs the balance of blood gases because there is not enough carbon dioxide in the blood.
- Intense physical exercise – for some people, this may cause extreme reactions.
- Excessive caffeine intake – the caffeine in coffee, tea and other beverages is a strong stimulant.
- Illness – may cause physical changes.
- A sudden change of environment – such as walking into an overcrowded, hot or stuffy environment.
Risk factors for panic disorder
Factors that may increase your risk of developing panic attacks or panic disorder include:
- Family history of panic attacks or panic disorder. Anxiety disorders, including panic disorder, often run in families. You have a 40% increased risk of developing panic disorder if one of your first-degree relatives (biological siblings, children or parents) has the condition.
- Mental health conditions. People who have anxiety disorders, depression or other mental health conditions are more prone to panic attacks. There is an increased risk for panic disorder among offspring of parents with anxiety, depressive, and bipolar disorders.
- Major life stress, such as the death or serious illness of a loved one. Most individuals report identifiable stressors in the months before their first panic attack (e.g., interpersonal stressors and stressors related to physical well-being, such as negative experiences with illicit or prescription drugs, disease, or death in the family).
- A traumatic event, such as sexual assault or a serious accident
- Major changes in your life, such as a divorce or the addition of a baby
- Smoking or excessive caffeine intake. Smoking or excessive caffeine intake is a risk factor for panic attacks and panic disorder.
- History of childhood physical or sexual abuse. Reports of childhood experiences of sexual and physical abuse are more common in panic disorder than in certain other anxiety disorders.
- Respiratory disturbance, such as asthma, is associated with panic disorder, in terms of past history, comorbidity, and family history.
Panic disorder prevention
There’s no sure way to prevent panic attacks or panic disorder. However, you can take these actions to lower your risk of having a panic attack:
- Get treatment for panic attacks as soon as possible to help stop them from getting worse or becoming more frequent.
- Stick with your treatment plan to help prevent relapses or worsening of panic attack symptoms.
- Exercise regularly, which may play a role in protecting against anxiety. Exercise also help you manage stress, relieve tension and boost your mood.
- Avoid caffeine, alcohol and smoking. These can make panic attacks worse.
- Eat a healthy diet.
- Manage stress in healthy ways.
- Talk to your doctor before taking herbal supplements or over-the-counter (OTC) medications. Certain substances can increase anxiety.
Panic disorder signs and symptoms
Panic disorder is a type of anxiety disorder where you regularly experience unexpected panic attacks or sudden attacks of panic or fear. A main feature of panic disorder is that the panic attacks usually happen without warning and aren’t due to another mental health or physical condition. Many people experience feelings of anxiety and panic at certain times, it’s a natural response to stressful or dangerous situations. However, someone with panic disorder has more intense feelings of anxiety, stress and panic regularly and these intense sensations occur suddenly at any time, often for no apparent reason. A panic attack is a sudden (without warning) episode of intense fear or discomfort, accompanied by physical symptoms, which can feel like a heart attack, even though it is not dangerous. Panic attacks often feel like a rush of fear or impending doom. A panic attack can be very frightening and you may feel a strong desire to escape the situation or to seek emergency assistance. If frequent or severe, panic attacks can be a sign of panic disorder and should be addressed with professional help.
People with panic disorder may have:
- Sudden and repeated panic attacks of overwhelming anxiety and fear
- A feeling of being out of control, or a fear of death or impending doom during a panic attack
- An intense worry about when the next panic attack will happen
- A fear or avoidance of places where panic attacks have occurred in the past
- Physical symptoms during a panic attack, such as:
- Pounding or racing heart
- Sweating
- Chills
- Trembling
- Difficulty breathing
- Weakness or dizziness
- Tingly or numb hands
- Chest pain
- Stomach pain or nausea
Anxiety
Anxiety is a common mental health condition characterized by excessive worry, fear, and apprehension that can significantly impact your daily life, often accompanied by physical symptoms like rapid heartbeat and sweating. Anxiety is a natural human emotion that can be a normal response to stress or perceived threats. However, when anxiety becomes persistent, intense, and difficult to control, it can indicate an anxiety disorder. Anxiety disorders are a group of mental disorders characterized by significant and uncontrollable feelings of anxiety and fear that impair a person’s social, occupational, and personal functions.
Anxiety can range from mild to severe, and can include feelings of worry and fear. Panic is the most severe form of anxiety.
You may start to avoid certain situations because you fear they’ll trigger another attack.
This can create a cycle of living “in fear of fear”. It can add to your sense of panic and may cause you to have more attacks.
Panic attacks
Panic attacks typically include some of these signs or symptoms 2:
- Skipping, racing or pounding heart
- Sweating
- Trembling or shaking
- Shortness of breath or difficulty breathing or hyperventilation
- Choking sensations
- Chest pain, pressure or discomfort
- Nausea, stomach problems or sudden diarrhea
- Dizziness, lightheadedness, feeling faint
- Tingling or numbness in parts of your body or in your fingers or toes
- Hot flushes or chills
- Feeling things around you are strange, unreal (derealization), depersonalization (feeling detached from yourself), unfamiliar, or feeling detached from your body
- Thoughts of losing control or going crazy
- Fear of dying
Panic attacks are very unpleasant, distressing and can be frightening. During a panic attack you get a rush of intense mental and physical symptoms. Panic attack can come on very quickly without warning and for no apparent reason. Panic attacks can strike at any time when you’re driving a car, at the mall, sound asleep or in the middle of a business meeting. You may have occasional panic attacks, or they may occur frequently. As you can see from the list, many of the symptoms are similar to what you might experience if you were in a truly dangerous situation. A panic attack can be very frightening and you may feel a strong desire to escape the situation. Many of the symptoms may appear to indicate some medical condition and some people seek emergency assistance. However, panic attacks, while very frightening, are not life-threatening or dangerous or harmful to your health. Following a panic attack, you may feel fatigued and drained, even after the symptoms subside. Frequent panic attacks can lead to a decrease in your quality of life and other psychosocial issues. And not everyone who experiences a panic attack develops panic disorder.
Panic disorder complications
Left untreated, panic attacks and panic disorder can affect almost every area of your life. You may be so afraid of having more panic attacks that you live in a constant state of fear, ruining your quality of life.
Complications that panic attacks may cause or be linked to include:
- Development of specific phobias, such as fear of driving or leaving your home
- Frequent medical care for health concerns and other medical conditions
- Avoidance of social situations
- Problems at work or school
- Depression, anxiety disorders and other psychiatric disorders
- Increased risk of suicide or suicidal thoughts
- Alcohol or other substance misuse
- Financial problems
For some people, panic disorder may include agoraphobia — avoiding places or situations that cause you anxiety because you fear being unable to escape or get help if you have a panic attack. Or you may become reliant on others to be with you in order to leave your home.
Panic disorder diagnosis
Panic disorder is diagnosed when a person experiences frequent and unexpected panic attacks, along with a persistent worry about future attacks. Your doctor will determine if you have panic attacks, panic disorder or another condition, such as heart or thyroid problems, with symptoms that resemble panic attacks.
To help your doctor pinpoint a diagnosis, you may have:
- A complete physical exam
- Blood tests to check your thyroid and other possible conditions and tests on your heart, such as an electrocardiogram (ECG or EKG)
- A psychological evaluation to talk about your symptoms, fears or concerns, stressful situations, relationship problems, situations you may be avoiding, and family history
You may fill out a psychological self-assessment or questionnaire. You also may be asked about alcohol or other substance use.
Panic Disorder DSM-5 Diagnostic Criteria
Not everyone who has panic attacks has panic disorder. For a diagnosis of panic disorder, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association list the following diagnostic criteria for panic disorder 13:
- Criterion A. Recurrent unexpected panic attacks. A panic attack is an abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, and during which time four
(or more) of the following symptoms occur; Note: The abrupt surge can occur from a calm state or an anxious state.- Palpitations, pounding heart, or accelerated heart rate.
- Sweating.
- Trembling or shaking.
- Sensations of shortness of breath or smothering.
- Feelings of choking.
- Chest pain or discomfort.
- Nausea or abdominal distress.
- Feeling dizzy, unsteady, light-headed, or faint.
- Chills or heat sensations.
- Paresthesias (numbness or tingling sensations).
- Derealization (feelings of unreality) or depersonalization (being detached from oneself).
- Fear of losing control or “going crazy.”
- Fear of dying.
- Note: Culture-specific symptoms (e.g., tinnitus, neck soreness, headache, uncontrollable screaming or crying) may be seen. Such symptoms should not count as one of the four required symptoms.
- Criterion B. At least one of the attacks has been followed by 1 month (or more) of one or both of the following:
- Persistent concern or worry about additional panic attacks or their consequences (e.g., losing control, having a heart attack, “going crazy”).
- A significant maladaptive change in behavior related to the attacks (e.g., behaviors designed to avoid having panic attacks, such as avoidance of exercise or unfamiliar situations).
- Criterion C. The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism, cardiopulmonary disorders).
- Criterion D. The disturbance is not better explained by another mental disorder (e.g., the panic attacks do not occur only in response to feared social situations, as in social anxiety disorder; in response to circumscribed phobic objects or situations, as in specific phobia; in response to obsessions, as in obsessive-compulsive disorder; in response to reminders of traumatic events, as in posttraumatic stress disorder; or in response to separation from attachment figures, as in separation anxiety disorder).
Panic disorder refers to recurrent unexpected panic attacks (Criterion A). A panic attack is an abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, and during which time four or more of a list of 13 physical and cognitive symptoms occur. The term recurrent literally means more than one unexpected panic attack. The term unexpected refers to a panic attack for which there is no obvious cue or trigger at the time of occurrence—that is, the attack appears to occur from out of the blue, such as when the individual is relaxing or emerging from sleep (nocturnal panic attack). In contrast, expected panic attacks are attacks for which there is an obvious cue or trigger, such as a situation in which panic attacks typically occur. The determination of whether panic attacks are expected or unexpected is made by the clinician, who makes this judgment based on a combination of careful questioning as to the sequence of events preceding or leading up to the attack and the individual’s own judgment of whether or not the attack seemed to occur for no apparent reason. Cultural interpretations may influence the assignment of panic attacks as expected or unexpected. In the United States and Europe, approximately one-half of individuals with panic disorder have expected panic attacks as well as unexpected panic attacks. Thus, the presence of expected panic attacks does not rule out the diagnosis of panic disorder. For more details regarding expected versus unexpected panic attacks, see the text accompanying panic attacks.
The frequency and severity of panic attacks vary widely. In terms of frequency, there may be moderately frequent attacks (e.g., one per week) for months at a time, or short bursts of more frequent attacks (e.g., daily) separated by weeks or months without any attacks or with less frequent attacks (e.g., two per month) over many years. Persons who have infrequent panic attacks resemble persons with more frequent panic attacks in terms of panic attack symptoms, demographic characteristics, comorbidity with other disorders, family history, and biological data. In terms of severity, individuals with panic disorder may have both full-symptom (four or more symptoms) and limited-symptom (fewer than four symptoms) attacks, and the number and type of panic attack symptoms frequently differ from one panic attack to the next. However, more than one unexpected full-symptom panic attack is required for the diagnosis of panic disorder.
The worries about panic attacks or their consequences usually pertain to physical concerns, such as worry that panic attacks reflect the presence of life-threatening illnesses (e.g., cardiac disease, seizure disorder); social concerns, such as embarrassment or fear of being judged negatively by others because of visible panic symptoms; and concerns about mental functioning, such as ”going crazy” or losing control (Criterion B). The maladaptive changes in behavior represent attempts to minimize or avoid panic attacks or their consequences. Examples include avoiding physical exertion, reorganizing daily life to ensure that help is available in the event of a panic attack, restricting usual daily activities, and avoiding agoraphobia-type situations, such as leaving home, using public transportation, or shopping. If agoraphobia is present, a separate diagnosis of agoraphobia is given.
Associated Features Supporting Diagnosis
One type of unexpected panic attack is a nocturnal panic attack (i.e., waking from sleep in a state of panic, which differs from panicking after fully waking from sleep). In the United States, this type of panic attack has been estimated to occur at least one time in roughly one-quarter to one-third of individuals with panic disorder, of whom the majority also have daytime panic attacks. In addition to worry about panic attacks and their consequences, many individuals with panic disorder report constant or intermittent feelings of anxiety that are more broadly related to health and mental health concerns. For example, individuals with panic disorder often anticipate a catastrophic outcome from a mild physical symptom or medication side effect (e.g., thinking that they may have heart disease or that a headache means presence of a brain tumor). Such individuals often are relatively intolerant of medication side effects. In addition, there may be pervasive concerns about abilities to complete daily tasks or withstand daily stressors, excessive use of drugs (e.g., alcohol, prescribed medications or illicit drugs) to control panic attacks, or extreme behaviors aimed at controlling panic attacks (e.g., severe restrictions on food intake or avoidance of specific foods or medications because of concerns about physical symptoms that provoke panic attacks).
Panic disorder treatment
Panic disorder main treatment options are talk therapy (psychotherapy), medication, or a combination of both. One or both types of treatment may be recommended, depending on your preference, your history, the severity of your panic disorder and whether you have access to therapists who have special training in treating panic disorders.
Psychotherapy (talk therapy)
Psychotherapy also called talk therapy is a term for a variety of treatment techniques that aim to help a person identify and change unhealthy emotions, thoughts and behaviors. Psychotherapy is considered an effective first choice treatment for panic attacks and panic disorder. Psychotherapy can help you understand panic attacks and panic disorder and learn how to cope with them. A form of psychotherapy called cognitive behavioral therapy (CBT) can help you learn, through your own experience, that panic symptoms are not dangerous. In cognitive behavioral therapy (CBT) you discuss your thoughts and emotions with a mental health professional, such as a licensed counselor or psychologist. This specialist helps identify panic attack triggers so you can change your thinking, behaviors and reactions. As you start to respond differently to triggers, the attacks may decrease and ultimately stop.
Another form of psychotherapy is exposure therapy. Exposure therapy is a type of therapy in which you’re gradually exposed to the things, situations and activities you fear. There are a few different approaches to this therapy. Exposure therapy involves exposing you gradually and repeatedly — in your imagination and/or in reality — to whatever triggers a panic attack. Your therapist will help you gradually re-create the symptoms of a panic attack in a safe, repetitive manner. Over time, you learn to become comfortable with the situation instead of it causing anxiety and panic. You’ll learn relaxation techniques, such as breathing exercises, to manage your anxiety throughout the process. Successful treatment can also help you overcome fears of situations that you’ve avoided because of panic attacks.
Seeing results from treatment can take time and effort. You may start to see panic attack symptoms reduce within several weeks, and often symptoms decrease significantly or go away within several months. You may schedule occasional maintenance visits to help ensure that your panic attacks remain under control or to treat recurrences.
Medications
Medications can help reduce your symptoms associated with panic attacks as well as depression if that’s an issue for you. Several types of medication have been shown to be effective in managing symptoms of panic attacks and panic disorder, including:
- Selective serotonin reuptake inhibitors (SSRIs). Generally safe with a low risk of serious side effects, SSRI antidepressants are typically recommended as the first choice of medications to treat panic attacks. SSRIs approved by the Food and Drug Administration (FDA) for the treatment of panic disorder include fluoxetine (Prozac), paroxetine (Paxil, Pexeva) and sertraline (Zoloft).
- Serotonin and norepinephrine reuptake inhibitors (SNRIs). These medications are another class of antidepressants. The serotonin and norepinephrine reuptake inhibitor (SNRI) venlafaxine (Effexor XR) is FDA approved for the treatment of panic disorder.
- Benzodiazepines. These sedatives are central nervous system (brain and spinal cord) depressants. Benzodiazepines approved by the FDA for the treatment of panic disorder include alprazolam (Xanax) and clonazepam (Klonopin). Benzodiazepines are generally used only on a short-term basis because they can be habit-forming or have addiction potential, causing mental or physical dependence, so it’s important to take them with caution. Benzodiazepines are not a good choice if you’ve had problems with alcohol or drug use. They can also interact with other drugs, causing dangerous side effects.
If one medication doesn’t work well for you, your doctor may recommend switching to another or combining certain medications to boost effectiveness. Keep in mind that it can take several weeks after first starting a medication to notice an improvement in symptoms.
All medications have a risk of side effects, and some may not be recommended in certain situations, such as pregnancy. Talk with your doctor about possible side effects and risks.
Lifestyle and home remedies
While panic attacks and panic disorder benefit from professional treatment, these self-care steps can help you manage symptoms:
- Stick to your treatment plan. Facing your fears can be difficult, but treatment can help you feel like you’re not a hostage in your own home.
- Join a support group. Joining a group for people with panic attacks or anxiety disorders can connect you with others facing the same problems.
- Avoid caffeine, alcohol, smoking and recreational drugs. All of these can trigger or worsen panic attacks.
- Practice stress management and relaxation techniques. For example, yoga, deep breathing and progressive muscle relaxation — tensing one muscle at a time, and then completely releasing the tension until every muscle in the body is relaxed — also may be helpful.
- Get physically active. Aerobic activity may have a calming effect on your mood.
- Get sufficient sleep. Get enough sleep so that you don’t feel drowsy during the day.
Alternative medicine
Some dietary supplements have been studied as a treatment for panic disorder, but more research is needed to understand the risks and benefits. Herbal products and dietary supplements aren’t monitored by the Food and Drug Administration (FDA) the same way medications are. You can’t always be certain of what you’re getting and whether it’s safe. Before trying herbal remedies or dietary supplements, talk to your doctor. Some of these products can interfere with prescription medications or cause dangerous interactions.
Panic disorder prognosis
With treatment, most people who experience panic attacks or have panic disorder get better. Without treatment, people with panic disorder have a higher risk of suicidal ideation. It may also decrease your quality of life due to impaired social functioning. If you do not get medical help, panic disorder can escalate and become very difficult to cope with. You’re also more at risk of developing other mental health conditions, such as agoraphobia or other phobias, or an alcohol or drug problem. Having panic disorder may affect your ability to drive.
Compliance with treatment is a major issue, and thus relapse of symptoms is common 1. Only about 60% of patients achieve remission within 6 months 1. Triggers for poor outcomes include a chronic illness, high interpersonal sensitivity, unmarried, low social class, and living alone. Besides premature adverse heart events, these patients are also at risk for suicide.
- Cackovic C, Nazir S, Marwaha R. Panic Disorder. [Updated 2023 Aug 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430973[↩][↩][↩][↩]
- What is Panic. https://www.cci.health.wa.gov.au/~/media/CCI/Mental-Health-Professionals/Panic/Panic—Information-Sheets/Panic-Information-Sheet—01—What-is-Panic.pdf[↩][↩][↩][↩]
- Module 2: What Keeps Panic Disorder Going. https://cci.health.wa.gov.au/~/media/CCI/Consumer-Modules/When-Panic-Attacks/When-Panic-Attacks—Module-2—What-Keeps-Panic-Disorder-Going.pdf[↩]
- Sivolap YP. Panicheskoe rasstroĭstvo: klinicheskie fenomeny i vozmozhnosti terapii [Panic disorder: clinical phenomena and treatment options]. Zh Nevrol Psikhiatr Im S S Korsakova. 2017;117(4):112-116. Russian. doi: 10.17116/jnevro20171174112-116[↩][↩]
- Baker HJ, Waite P. The identification and psychological treatment of panic disorder in adolescents: a survey of CAMHS clinicians. Child Adolesc Ment Health. 2020 Sep;25(3):135-142. doi: 10.1111/camh.12372[↩]
- Clark AE, Goodwin SR, Marks RM, Belcher AM, Heinlein E, Bennett ME, Roche DJO. A Narrative Literature Review of the Epidemiology, Etiology, and Treatment of Co-Occurring Panic Disorder and Opioid Use Disorder. J Dual Diagn. 2021 Oct-Dec;17(4):313-332. doi: 10.1080/15504263.2021.1965407[↩]
- Farris SG, Robinson JD, Zvolensky MJ, Hogan J, Rabius V, Cinciripini PM, Karam-Hage M, Blalock JA. Panic attacks and smoking cessation among cancer patients receiving smoking cessation treatment. Addict Behav. 2016 Oct;61:32-9. doi: 10.1016/j.addbeh.2016.05.011[↩]
- Foldes-Busque G, Fleet RP, Denis I, Poitras J, Chauny JM, Diodati JG, Marchand A. Nonfearful Panic Attacks in Patients With Noncardiac Chest Pain. Psychosomatics. 2015 Sep-Oct;56(5):513-20. doi: 10.1016/j.psym.2014.07.005[↩]
- Von Korff MR, Eaton WW, Keyl PM. The epidemiology of panic attacks and panic disorder. Results of three community surveys. Am J Epidemiol. 1985 Dec;122(6):970-81. doi: 10.1093/oxfordjournals.aje.a114201[↩]
- Vizard, T. , Pearce, N. , & Davis, J. (2018). Mental Health of Children and Young People in England, 2017. Leeds: Health and Social Care Information Centre.[↩][↩]
- Essau CA, Conradt J, Petermann F. Frequency, comorbidity, and psychosocial impairment of anxiety disorders in German adolescents. J Anxiety Disord. 2000 May-Jun;14(3):263-79. doi: 10.1016/s0887-6185(99)00039-0[↩]
- Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, Swendsen J. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010 Oct;49(10):980-9. doi: 10.1016/j.jaac.2010.05.017[↩]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Birmaher, B. , & Ollendick, T. H. (2004). Childhood‐onset panic disorder In Ollendick T. H., & March J. S. (Eds.), Phobic and anxiety disorders in children and adolescents (pp. 306–333). New York: Oxford University Press.[↩]
- Santos M, D’Amico D, Spadoni O, Amador-Arjona A, Stork O, Dierssen M. Hippocampal hyperexcitability underlies enhanced fear memories in TgNTRK3, a panic disorder mouse model. J Neurosci. 2013 Sep 18;33(38):15259-71. doi: 10.1523/JNEUROSCI.2161-13.2013[↩]
- Lai CH. Fear Network Model in Panic Disorder: The Past and the Future. Psychiatry Investig. 2019 Jan;16(1):16-26. doi: 10.30773/pi.2018.05.04.2[↩]
- Quagliato LA, Freire RC, Nardi AE. Risks and benefits of medications for panic disorder: a comparison of SSRIs and benzodiazepines. Expert Opin Drug Saf. 2018 Mar;17(3):315-324. doi: 10.1080/14740338.2018.1429403[↩]





{kind=link}