



What is stinging nettle
Stinging nettle also known as Urtica dioica, is a herbaceous perennial flowering plant in the family Urticaceae, that is used in alternative medicine throughout North America and Europe to treat hay fever, asthma, diarrhea, osteoarthritis, circulation problems, diabetes, fluid retention, symptoms of enlarged prostate or benign prostatic hyperplasia (BPH), and other conditions 1). However, stinging nettle has not been proven with clinical research to be effective in treating these conditions. It is not certain whether nettle is effective in treating any medical condition. Medicinal use of this product has not been approved by the U.S. Food and Drug Administration (FDA). Stinging nettle should not be used in place of medication prescribed for you by your doctor. Stinging nettle seems to be generally well-tolerated in clinical trials and may produce mild gastrointestinal effects such as diarrhea, gastric pain, and nausea.
Stinging nettle has a long history as one among plants foraged from the wild and eaten as a vegetable 2). Stinging nettle is consumed primarily as a fresh vegetable whereby it is added to soups, cooked as a pot herb, or used as a vegetable complement in dishes. In Georgia, a meal of boiled stinging nettle seasoned with walnut is common 3). Romanians use sour soup made from fermented wheat bran vegetables and green nettle leaves harvested from young plants 4). In this sense, more work needs to be done on nutritive value of fresh stinging nettle, and the fate of minerals and bioactive compounds in processed products. A comprehensive proximate analysis showed the shoots harvested from stinging nettle (Shoot) showed close to 90% moisture and rests are proteins (3.7%), fat (0.6%), ash (2.1%), dietary fiber (6.4%), total carbohydrate (7.1%), and total calories (45.7 kcal/100 g) (wet basis). Besides, Stinging nettle (shoot) contains vitamin A, vitamin C, calcium, iron, sodium, and rich fatty acid profile 5).
Despite stinging nettle being recognized as an edible and highly nutritious vegetable, research attention has focused more on its value as a source of alternative medicine and fiber. Clinical trials have confirmed the effectiveness of stinging nettle root and saw palmetto (Serenoa repens (Bart.) Small) fruit extracts in the treatment of benign prostatic hyperplasia 6). Dried nettle leaf preparations are also known to alleviate symptoms associated with allergic rhinitis 7), and a technology for granulating lipophilic leaf extracts for medicine has been developed 8). A recent report from ongoing work in Italy confirms the potential of stinging nettle as a sustainable source of textile fiber 9).
Table 1. Stinging nettle nutrition facts
| Fall 2011 | Spring 2012 | |||||||
|---|---|---|---|---|---|---|---|---|
| Raw | Blanched | Cooked | Cooked + salt | Raw | Blanched | Cooked | Cooked + salt | |
| Proximate analysis | ||||||||
| Moisture (%) | 89.0 ± 1.4a | 87.2 ± 0.9a | 87.7 ± 0.7a | 88.6 ± 0.5a | 75.1 ± 1.5c | 84.6 ± 2.5b | 85.6 ± 0.8b | 91.7 ± 0.9a |
| Protein (%) | 3.7 ± 0.5a | 3.6 ± 0.4ab | 3.6 ± 0.3a | 2.7 ± 0.2b | 6.3 ± 0.3a | 4.1 ± 0.2b | 3.8 ± 0.3b | 2.2 ± 0.2c |
| Fat (%) | 0.6 ± 0.1a | 0.4 ± 0.1b | 0.4 ± 0.0b | 0.2 ± 0.0b | 1.4 ± 0.3a | 1.1 ± 0.1a | 1.1 ± 0.2a | 0.6 ± 0.1b |
| Ash (%) | 2.1 ± 0.3a | 1.8 ± 0.3ab | 1.5 ± 0.3b | 1.5 ± 0.1b | 3.4 ± 0.2a | 1.4 ± 0.1b | 1.2 ± 0.1c | 1.0 ± 0.1c |
| Fiber, total dietary (%) | 6.4 ± 0.4a | 4.2 ± 0.1b | 3.5 ± 0.3c | 3.6 ± 0.3bc | 9.7 ± 1.0a | 5.4 ± 0.9b | 4.9 ± 1.0b | 4.2 ± 0.2c |
| Carbohydrates, total (%) | 7.1 ± 1.7a | 6.6 ± 1.4ab | 6.3 ± 0.8b | 6.2 ± 1.2b | 16.5 ± 1.6a | 8.9 ± 0.7b | 8.1 ± 1.1b | 4.2 ± 0.6c |
| Other carbohydrates (%) | 2.7 ± 0.2ab | 2.9 ± 0.3a | 2.5 ± 0.1b | 2.7 ± 0.1a | 6.2 ± 1.0a | 3.5 ± 0.7b | 3.3 ± 0.5b | 2.0 ± 0.1c |
| Calories, total (kcal/100 g) | 45.7 ± 3.1a | 42.6 ± 2.1a | 44.7 ± 2.5a | 36.5 ± 2.3b | 99.7 ± 2.5a | 62.0 ± 1.0b | 57.3 ± 1.5c | 32.0 ± 1.0d |
| Calories from fat (kcal/100 g) | 5.0 ± 1.0a | 4.3 ± 0.6ab | 2.7 ± 0.5bc | 2.3 ± 0.6c | 12.3 ± 1.6a | 10.0 ± 1.0ab | 8.7 ± 3.1b | 4.0 ± 1.0c |
| Vitamins and minerals | ||||||||
| Vitamin A, total (IU/100 g) | 4935 ± 104a | 4851 ± 56a | 4548 ± 53b | 4362 ± 78b | 11403 ± 1333a | 6470 ± 222bc | 6021 ± 90c | 7872 ± 354b |
| Vitamin A, as β-carotene (IU/100 g) | 5035 ± 213a | 4689 ± 37b | 4549 ± 130b | 4062 ± 39c | 7860 ± 460a | 4811 ± 88b | 5028 ± 65b | 4154 ± 148c |
| Vitamin C (mg/100 g) | 1.1 ± 0.1a | 0.6 ± 0.1b | 0.6 ± 0.1b | 0.5 ± 0.1b | 0.5 ± 0.0a | 0.5 ± 0.0a | 0.5 ± 0.0a | 0.5 ± 0.0a |
| Calcium (mg/100 g) | 278 ± 9c | 441 ± 12a | 376 ± 9ab | 318 ± 52bc | 788 ± 41a | 464 ± 10b | 430 ± 10b | 316 ± 7c |
| Iron (mg/100 g) | 1.2 ± 0.1c | 1.8 ± 0.2b | 2.6 ± 0.1a | 2.5 ± 0.3a | 3.4 ± 0.3a | 2.1 ± 0.2b | 2.1 ± 0.3b | 1.6 ± 0.1c |
| Sodium (mg/100 g) | 5.7 ± 0.1b | 6.3 ± 0.4b | 6.5 ± 0.3b | 87.7 ± 6.0a | 5.5 ± 0.6b | 7.0 ± 0.2b | 6.7 ± 0.2b | 81.1 ± 2.9a |
| Fatty acid profile | ||||||||
| Saturated fat (%) | 35.5 ± 2.6a | 25.7 ± 2.5b | 23.6 ± 4.1 c | 21.7 ± 1.9d | 32.7 ± 2.8a | 16.5 ± 1.5bc | 17.3 ± 1.2b | 15.7 ± 1.4c |
| Monounsaturated (%) | 2.7 ± 0.2c | 3.3 ± 0.2a | 4.8 ± 0.3a | 3.2 ± 0.1b | 7.5 ± 0.6a | 5.3 ± 0.3b | 5.8 ± 1.1b | 4.6 ± 0.2c |
| Polyunsaturated (%) | 61.8 ± 3.5c | 71.0 ± 2.0b | 71.6 ± 1.2c | 75.1 ± 1.9a | 59.8 ± 2.7d | 78.2 ± 4.4b | 76.9 ± 2.5c | 79.7 ± 2.6a |
| Cholesterol (mg/100 g) | 1.0 ± 0.0a | 1.0 ± 0.0a | 1.0 ± 0.0a | 1.0 ± 0.0a | 1.0 ± 0.0a | 1.0 ± 0.0a | 1.0 ± 0.0a | 1.0 ± 0.0a |
Footnotes: Approximate composition, vitamins, minerals, and fatty acid profile of raw and processed stinging nettle (Urtica dioica L.) shoots harvested from field plots in the fall of 2011 and spring of 2012.
[Source 10)]Stinging nettle is often sold as an herbal supplement. There are no regulated manufacturing standards in place for many herbal compounds and some marketed supplements have been found to be contaminated with toxic metals or other drugs. Herbal/health supplements should be purchased from a reliable source to minimize the risk of contamination.
Stinging nettle (Urtica dioica) is widespread through Europe and North America, and also occurs in North Africa and parts of Asia. There are naturalized populations in several other parts of the world. The stinging nettle plant has an erect stalk that grows up to 2 m in height.The soft, serrated leaves are opposite each other in pairs on the stem. The leaves and the rest of the plant are coated in stinging and non-stinging hairs. The plant spreads by underground roots which are noticeably yellow. The tiny greenish-white flowers, each with four petals, are densely clustered on elongated inflorescences towards the top of the stem. Stinging nettle (Urtica dioica) is divided into at least five subspecies, each of which is slightly different 11). The stinging nettle is well known for its toothed, hairy leaves and for its sting. The painful sensation of nettle stings occurs when toxins from specialized hairs are delivered into the skin. Each stinging hair has a bulbous tip which breaks off to leave a sharp, needle-like tube that pierces the skin and injects histamine and acetylcholine, causing itching and burning that may last up to 12 hours 12).
Figure 1. Stinging nettle

Several preclinical studies demonstrating the anti-inflammatory therapeutic potential and proposed mechanism of action of stinging nettle have been reported 13), most notably its inhibition of myeloid dendritic cells 14) as well as targets in the NF-kB pathway 15), however stinging nettle’s precise mechanism of action is not clear. Ten clinical trials evaluating stinging nettle use for the treatment of osteoarthritis have been conducted and generated mixed results in terms of their efficacy 16), 17). The root extracts of stinging nettle have also been studied clinically for treatment of benign prostatic hyperplasia (BPH) 18). Also noteworthy is that the bioactive compound(s) responsible for these reported activities remains poorly understood.
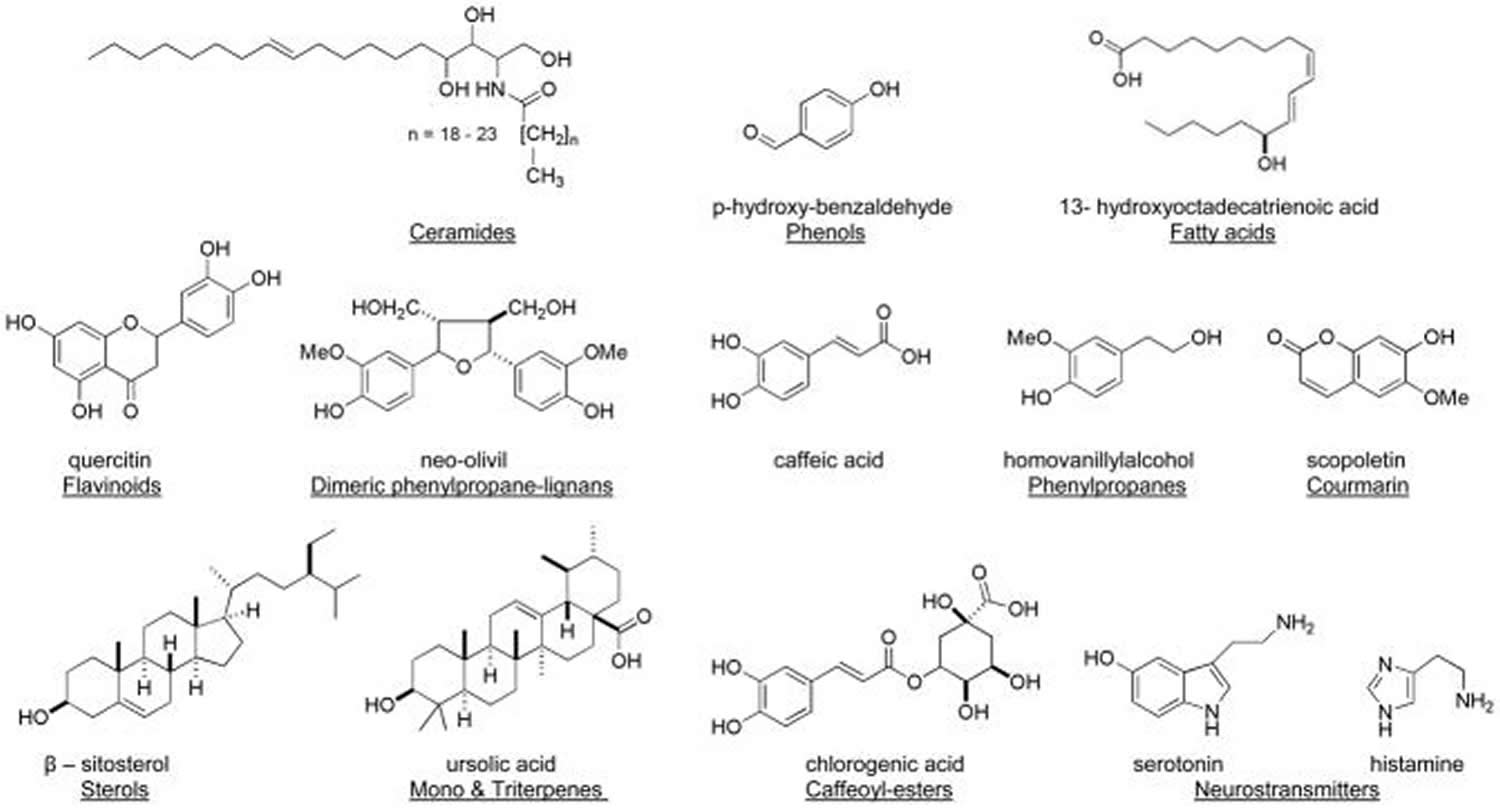
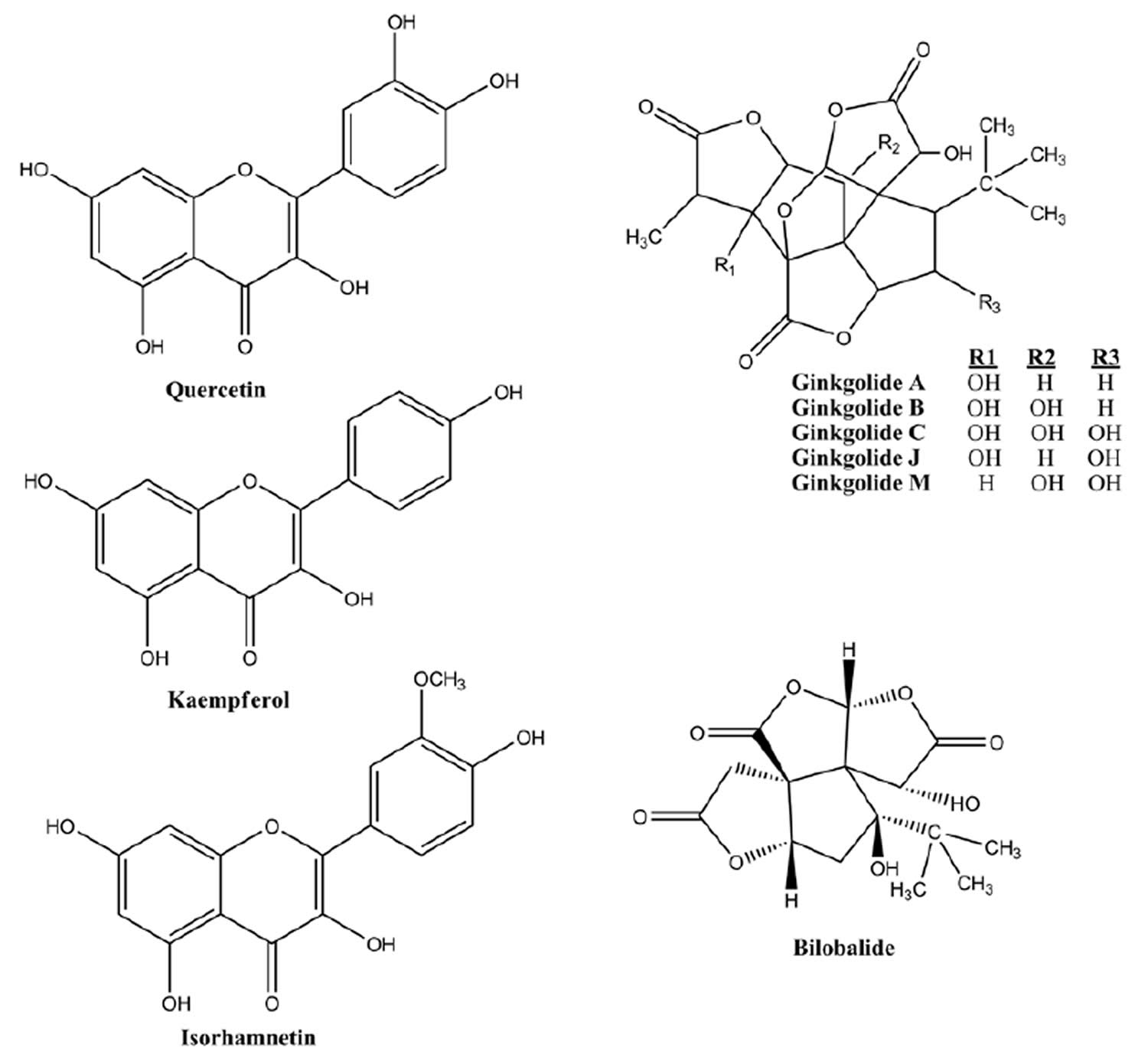
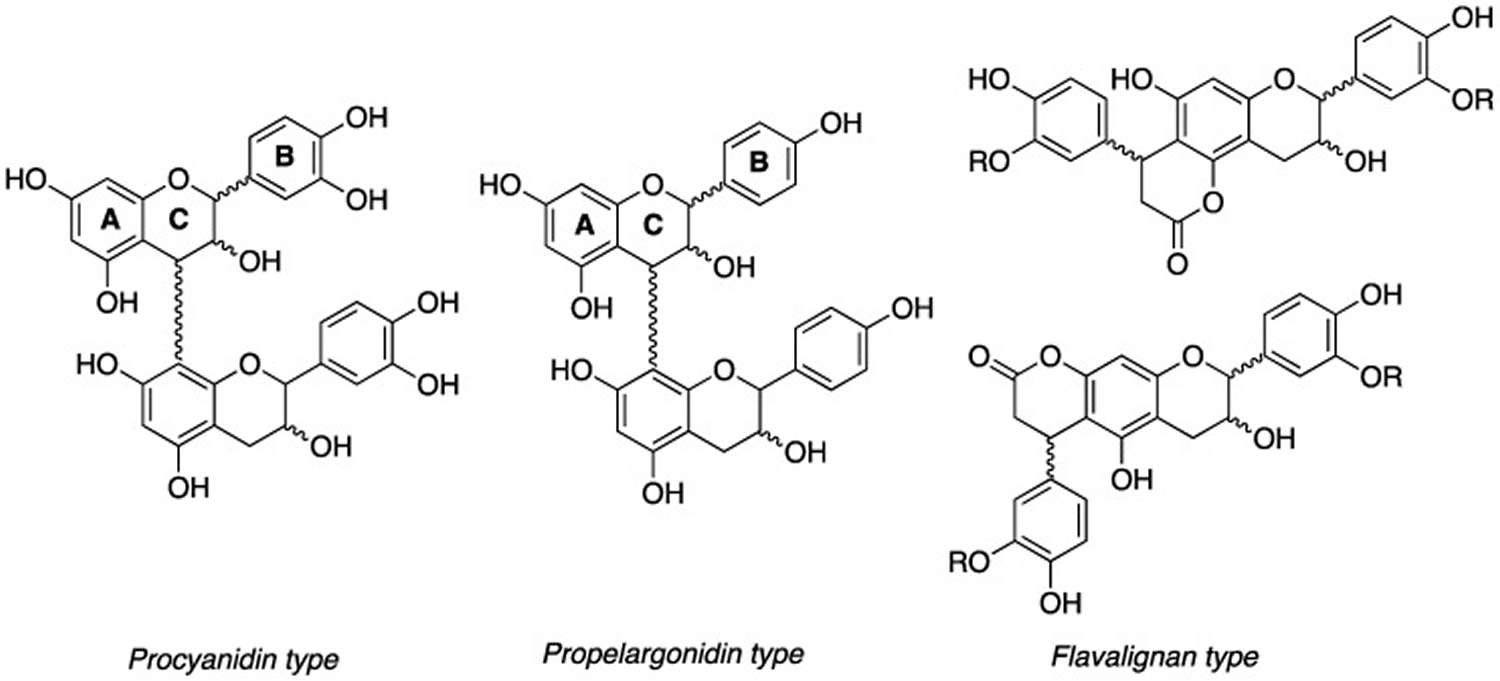
A number of structural classes have been reported from extracts of stinging nettle and selected examples are shown in Figure 2 19). Surprisingly, definitive reports using bioassay guided fractionation to link any potent anti-inflammatory compound(s) derived from stinging nettle for treating osteoarthritis are lacking 20). In addition several different extract preparations (e.g. water, ethanol, propanol) have exhibited success clinically, making it difficult to pinpoint the overall active chemistry and further compare the efficacy of clinical studies side-by-side 21). Traditionally water and ethanol soluble extracts of stinging nettle have been used to investigate its anti-inflammatory effects. Unfortunately, standardized stinging nettle extracts of the more polar constituents have failed to agree with clinical efficacy 22). Interestingly, few investigators have looked closely into the lipophilic extracts of stinging nettle despite previous reports of anti-inflammatory activity with potentially undefined chemistry 23).
Investigation of the stinging nettle extracts found the polar water (H2O) extracts demonstrated no ability to reduce inflammation. In fact stinging nettle water extracts of the stems and leaves demonstrated noticeable cytotoxicity in the MTT assay. Second, most of the polar stinging nettle methanol extracts including the roots, stems and leaves were far less effective than the standard anti-inflammatory agent celastrol and were comparable to a commercial ethanol extract of stinging nettle in terms of their activity 24). Third, in accordance with reports by others 25), the stinging nettle methanol extract extract of the flowering portion of nettle displayed significant anti-inflammatory activity however moderate cytotoxicity was also observed. Lastly and of particular note, the lipophilic extracts of the stinging nettle roots, stems and leaves were equivalent to or more potent than the standard endotoxin lipopolysaccharide induced inflammation in the NFkB luciferase assay and were the least cytotoxic.
Figure 2. Stinging nettle bioactive compounds
Stinging nettle uses
Stinging nettles have been used for centuries for a multitude of purposes, and continue to be harvested from the wild for food and medicine today.
Stinging nettles are eaten as a vegetable; cooking will destroy the stings. The tender, young shoots and leaves – the most palatable parts – are the main ingredient in nettle soup, which has a reputation for ‘cleansing the blood’. Historically, puddings and beer were made with stinging nettles. Today, the mature leaves are used in the production of cheese (notably Cornish Yarg) and in pesto, cordials and herbal tea. Stinging nettleshave also been used to yield vegetable protein similar to tofu made from soya ( Glycine max ). In some parts of Britain (e.g., Orkney) the leaves are traditionally fed to pigs to fatten them.
Stinging nettles have been used for a variety of medicinal purposes. A tonic prepared from the leaves is still among the most popular plant remedies used today. One traditional remedy for rheumatism involves deliberately stinging the afflicted area with nettle leaves! While this may seem strange, research has shown that nettle stings have anti-inflammatory properties that disrupt the NF-κB pathway and inhibit other inflammatory responses. Extracts of the stinging nettle root are used to treat benign prostate hyperplasia (BPH). Scientists have identified a variety of biochemical properties in extracts of nettles that support their uses in herbal medicine.
Stinging nettle stems contain tough fibers and can be used in textiles; the fiber was widely used to this effect in Germany and Austria during the First World War. Nettles can also be used for dyeing fabric. Horticulturalists sometimes use stinging nettles, which are rich in nutrients, to produce a type of liquid plant feed. The leaves are used in cosmetics.
Benign Prostatic Hyperplasia
The roots of stinging nettle have been used for urination disorders associated with benign prostate hyperplasia (BPH), as well as for joint problems, as a diuretic, and as an astringent. There is some limited evidence that stinging nettle may improve some symptoms of benign prostate hyperplasia (BPH), including lower urinary tract symptoms. There is also some limited evidence that stinging nettle and saw palmetto (Serenoa repens) may be efficacious for lower urinary tract symptoms associated with benign prostate hyperplasia (BPH).
The evidence base on efficacy of stinging nettle for benign prostate hyperplasia consists of only a few randomized controlled trials and reviews.
- A 2005 double-blind, placebo-controlled, randomized trial of stinging nettle 27) for treatment of benign prostate hyperplasia in 620 patients found significant improvement in International Prostate Symptom Score (IPSS), maximum urinary flow rate, and relief of lower urinary tract symptoms compared with placebo, over 6 months of treatment. These improvements were also maintained after 18 months of treatment.
- Other studies have examined the effects of a combination of Serenoa repens and stinging nettle. A 2007 randomized controlled trial in 257 patients with moderate and severe symptoms of benign prostate hyperplasia 28) found that the combination treatment over the course of 6 months was superior to placebo for attenuation of inflammatory and obstructive symptoms. Another study in Germany 29) compared the effects of the same combination to tamsulosin in 140 men for 15 months and found both treatments to be efficacious for lower urinary tract symptoms caused by benign prostate hyperplasia.
Stinging nettle contraindications
Due to the effects on androgen and estrogen metabolism, stinging nettle preparations are contraindicated in pregnancy and lactation and should not be used in children younger than 12 years.
Stinging nettle dosage
Freeze-dried stinging nettle leaf 600 mg has been used in a clinical trial for allergic rhinitis. Clinical trials for benign prostatic hyperplasia (BPH) have used aqueous stinging nettle root extracts 360 mg daily over 6 months and methanol root extract 600 to 1,200 mg daily for 6 to 9 weeks.
Stinging nettle allergies
Stinging nettles are known primarily for their ability to induce topical irritation following contact with exposed skin. The painful sensation of nettle stings occurs when toxins from specialized hairs of the stinging nettle leaves and stem are delivered into the skin. Each stinging hair has a bulbous tip which breaks off to leave a sharp, needle-like tube that pierces the skin and injects histamine and acetylcholine, causing acute urticaria, itching and burning that generally resolves spontaneously within 12 hours 30).
A 17-day-old exclusively breastfed infant was admitted to the hospital with an urticarial rash on the chest, back, and upper extremities 31). The infant’s mother had reportedly applied water boiled with stinging nettles for cracked nipple twice a day before and after each breastfeeding for 2 days. Total IgE and specific IgE levels for stinging nettle were high in the mother and infant. The infant’s rash improved upon cessation of breastfeeding. Breastfeeding was resumed 2 days later without the use of stinging nettle on the nipple and the rash did not recur. At 2 months of age, skin prick testing in the infant was positive for stinging nettle, but no other allergen tested positive. Stinging nettle exposure was the probable cause of the rash 32).
Stinging nettle side effects
Although not all side effects are known, stinging nettle is thought to be possibly safe when taken for a short period of time (no longer than 6 months).
Common side effects of stinging nettle supplement or extract may include:
- sweating;
- skin irritation; or
- stomach discomfort including diarrhea, gastric pain, and nausea.
Case reports of hypoglycemia 33) due to consumption of nettle preparations for prostatic hypertrophy exist, as well as gynaecomastia and galactorrhea 34). Due to the effects on androgen and estrogen metabolism, stinging nettle preparations are contraindicated in pregnancy and lactation and should not be used in children younger than 12 35).
Single cases of gynecomastia in a man and galactorrhea in a woman were reported after ingesting stinging nettle as a tea for 4 weeks prior to seeking medical advice 36). Serum hormones were normal in the man, but serum estradiol was very high, prolactin was slightly elevated, and LH and FSH were low in the woman. Both conditions reversed 4 to 6 weeks after stopping the tea. The case reports were from Turkey where ingestion of nettle is common. No analysis of the tea was performed to test for foreign substances. The relevance of these findings with respect to breastfeeding are not known. The prolactin level in a mother with established lactation may not affect her ability to breastfeed.
A randomized trial assigned mothers of preterm infants to receive either a purported herbal galactogogue tea twice daily, a fruit tea twice daily or nothing. The galactogogue tea contained stinging nettle, lemon balm, caraway, anise, fennel, goat’s rue, and lemon grass 37). All received similar breastfeeding advice from the same nurse and two groups were told that the tea would increase milk production, but compliance with the study teas was not assessed. The study was not blinded, and not analyzed on an intent-to-treat basis. Mother used breast pumps to extract and measure their milk output on day 1 and day 7 of the study. Although the volume of extracted milk was greater in the galactogogue tea group, there was no difference in infant weight gain nor in maternal serum prolactin between the groups at 7 days 38).
This is not a complete list of side effects and others may occur. Call your doctor for medical advice about side effects.
Get emergency medical help if you have any of these signs of an allergic reaction: hives; difficult breathing; swelling of your face, lips, tongue, or throat.
What other drugs will affect stinging nettle?
Taking stinging nettle with any medicines that make you sleepy can worsen this effect. Ask your doctor before taking stinging nettle with a sleeping pill, narcotic pain medicine, muscle relaxer, or medicine for anxiety, depression, or seizures.
Do not take stinging nettle without medical advice if you are using any of the following medications:
- lithium;
- blood pressure medication;
- insulin or oral diabetes medicine; or
- warfarin (Coumadin, Jantoven).
A 2015 review 39) noted that stinging nettle contains tannins, which can interact with a concomitant intake of iron, causing a reduction of the effects in patients who need iron supplements.
This list is not complete. Other drugs may interact with stinging nettle, including prescription and over-the-counter medicines, vitamins, and herbal products. Not all possible interactions are listed here.
Toxicology
The acute oral LD 50 (lethal dose 50 is the dose where 50% of the test subjects die) in rats has been estimated to be greater than 30 g/kg for the aqueous stinging nettle leaf extract and 1.3 g/kg for the stinging nettle root 40), 41). Liver function tests in rats fed aqueous nettle extracts for 30 days were normal 42). Older mutagenicity and carcinogenicity studies have been negative for the aqueous stinging nettle extract 43).
References [ + ]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}