






What is black seed oil
Black seed (Nigella sativa) often called black cumin or black-caraway, also known as nigella or kalonji, is an annual flowering plant in the family Ranunculaceae, native to south and southwest Asia 1. Nigella sativa plant can grow to 20-90 cm tall, with finely divided leaves, the leaf segments narrowly linear to threadlike. The flowers are delicate, and usually colored white, yellow, pink, pale blue or pale purple, with 5-10 petals. The fruit is a large and inflated capsule composed of 3-7 united follicles, each containing numerous seeds 2.
Black seeds are used as a spice in Indian and Middle Eastern cuisines. The black seeds taste like a combination of onions, black pepper and oregano, depending on whom you ask 3. The seeds have a slightly bitter flavor and resemble cumin or oregano, depending on whom you ask. They have a pungent bitter taste and smell 4.
The dry-roasted black seeds flavor curries, vegetables and pulses. Black seed can be used as a “pepper” in recipes with pod fruit, vegetables, salads and poultry. In some cultures, the black seeds are used to flavor bread products. It is also used as part of the spice mixture panch phoron (meaning a mixture of five spices) and by itself in many recipes in Bengali cuisine and most recognizably in naan bread 3. Black seed is also used in Armenian string cheese, a braided string cheese called majdouleh or majdouli in the Middle East.
Black seeds reported to contain a fatty oil rich in unsaturated fatty acids, mainly linoleic acid (50-60%), oleic acid (20%), eicodadienoic acid (3%) and dihomolinoleic acid (10%) 5. Saturated fatty acids (palmitic, stearic acid) amount to about 30% or less. α-sitosterol is a major sterol, which accounts for 44% and 54% of the total sterols in Tunisian and Iranian varieties of black seed oils respectively, followed by stigmasterol (6.57-20.92% of total sterols) 6.
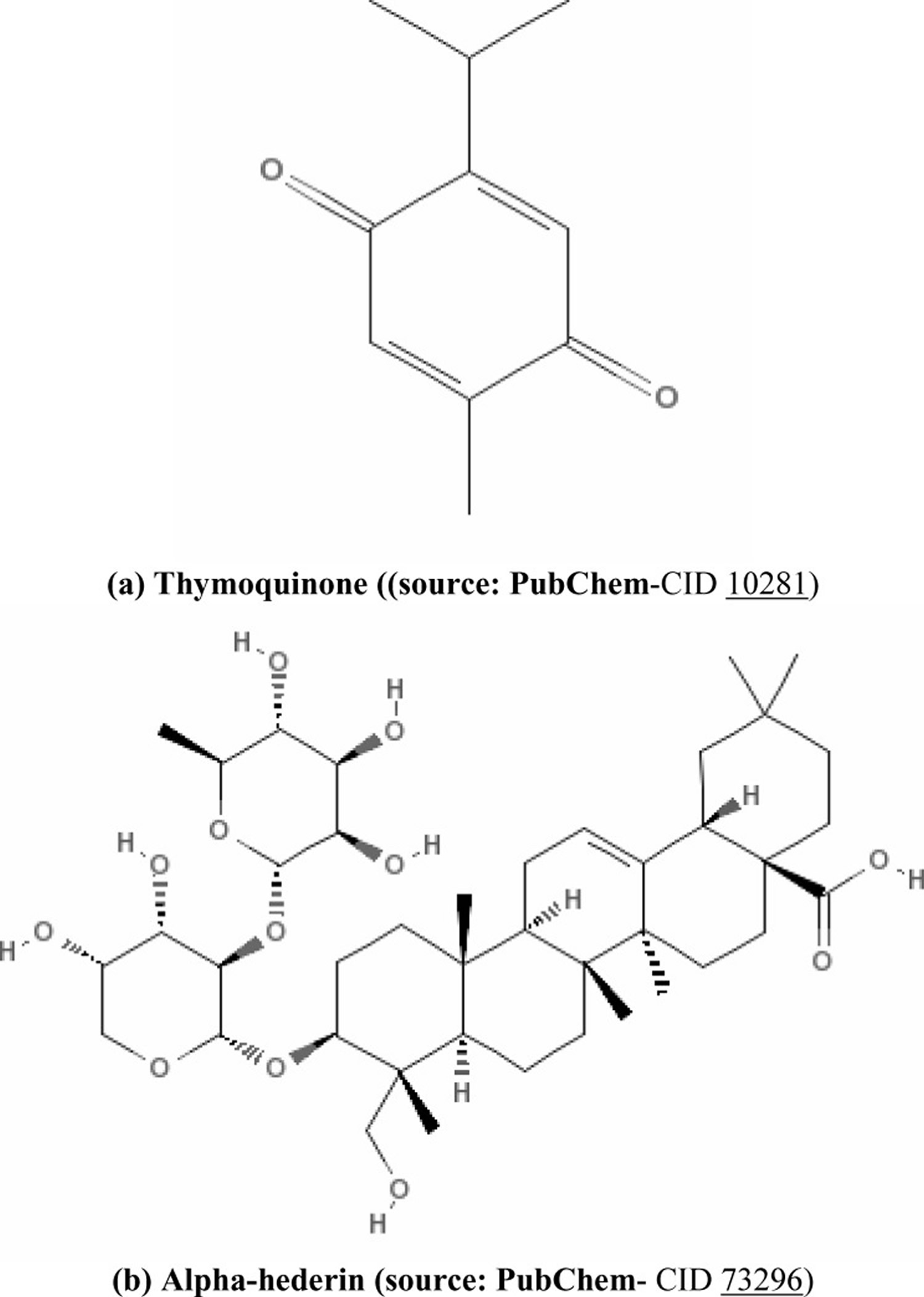
Black seeds contain both fixed and essential oils, proteins, alkaloids and saponin 7. Many active compounds have been isolated, identified and reported so far in different varieties of black seeds. The most important active compounds are thymoquinone (30%-48%), thymohydroquinone, dithymoquinone, p-cymene (7%-15%), carvacrol (6%-12%), 4-terpineol (2%-7%), t-anethol (1%-4%), sesquiterpene longifolene (1%-8%) α-pinene and thymol etc. Black seeds also contain some other compounds in trace amounts. Seeds contain two different types of alkaloids; i.e. isoquinoline alkaloids e.g. nigellicimine and nigellicimine-N-oxide, and pyrazol alkaloids or indazole ring bearing alkaloids which include nigellidine and nigellicine. Moreover, black seeds also contain alpha-hederin, a water soluble pentacyclic triterpene and saponin, a potential anticancer agent 8.
Some other compounds e.g. carvone, limonene, citronellol were also found in trace amounts. Most of the pharmacological properties of black seed are mainly attributed to quinine constituents, of which thymoquinone is the most abundant. On storage, thymoquinone yields dithymoquinone and higher oligocondensation products. Black seeds contain protein (26.7%), fat (28.5%), carbohydrates (24.9%), crude fibre (8.4%) and total ash (4.8 %). Black seeds are also containing good amount of various vitamins and minerals like Cu, P, Zn and Fe etc. The seeds contain carotene which is converted by the liver to vitamin A. Root and shoot are reported to contain vanillic acid 9.
Ghosheh et al. 10 described the quantification of four pharmacologically important components: thymoquinone, dithymoquinone, thymohydroquinone, and thymol, in the black seed oil by high performance liquid chromatography. Much of the biological activities of black seeds have been shown to be due to thymoquinone, the major component of the essential oil, which is also present in the fixed oil 7. Thymoquinone is considered as potent anti-oxidant 11, anti-carcinogenic and anti-mutagenic agent 12 (structure of thymoquinone is shown in Figure 1). Moreover, thymoquinone is a relatively safe compound, particularly when given orally to experimental animals 13. Alpha (α)-hederin, a pentacyclic triterpene saponin (structure: Figure 1b) isolated from the black cumin seeds of N. sativa, was also reported to have potent in vivo antitumor activity 14.
Many studies showed that black seed oil or thymoquinone has antioxidant activity and increases the activities of antioxidant enzymes such as superoxide dismutase, catalase, glutathione peroxidase etc 15. And antioxidant enzymes are clearly related to cancer- mostly their increased activities are beneficial against different types of cancer 16. Administration of black seed oil or thymoquinone can lower the toxicity of other anticancer drugs (for example, cyclophosphamide) by an up-regulation of antioxidant mechanisms, indicating a potential clinical application for these agents to minimize the toxic effects of treatment with anticancer drugs 17.
Figure 1. Thymoquinone and Alpha (α)-hederin chemical structure
Traditional uses of black seed in folk remedies
Black seed has been traditionally used for the treatment of a variety of disorders, diseases and conditions pertaining to respiratory system, digestive tract, kidney and liver function, cardio vascular system and immune system support, as well as for general well-being 18, 19.
Avicenna refers to black seeds in the “The Canon of Medicine”, as seeds stimulate the body’s energy and helps recovery from fatigue and dispiritedness. Black seeds and their oil have a long history of folklore usage in Indian and Arabian civilization as food and medicine 2, 20. The seeds have been traditionally used in Southeast Asian and the Middle East countries for the treatment of several diseases and ailments including asthma, bronchitis, rheumatism and related inflammatory diseases. Its many uses have earned Nigella the Arabic approbation ‘Habbatul barakah’, meaning the seed of blessing. A tincture prepared from the seeds is useful in indigestion, loss of appetite, diarrhoea, dropsy, amenorrhoea and dysmenorrhoea and in the treatment of worms and skin eruptions. Externally the oil is used as an antiseptic and local anesthetic. Roasted black seeds are given internally to stop the vomiting 21.
Black cumin seed oil benefits
Black seeds of Nigella sativa (family: Ranunculaceae), commonly known Black Cumin, or “Habbatul Barakah”, have long been used in folk medicine in the Arabian Gulf region, Far East Asia, and Europe 22.
In the traditional system of medicine practised in the Arabian Gulf region, Black Seed is recommended for a wide range of ailments, including fever, cough, bronchitis, asthma, chronic headache, migraine, dizziness, chest congestion, dysmenorrhea, obesity, diabetes, paralysis, hemiplagia, back pain, infection, inflammation, rheumatism, hypertension, and gastrointestinal problems such as dyspepsia, flatulence, dysentery, and diarrhea. It has been used as a stimulant, diuretic, emmenagogue, lactagogue, anthelmintic, and carminative 23. Black Seed has also been used externally where it is applied directly to abscesses, nasal ulcers, orchitis, eczema, and swollen joints.
Many of the folk medicinal claims of Black Seed use have been scientifically tested 22. Over 150 studies have been conducted over the last five decades to investigate chemical and pharmacological properties of Black Seeds 22. Phytochemical studies of Black Seed showed the presence of >100 constituents. Many of these compounds have not been chemically identified nor have they been pharmacologically tested. A combination of fatty acids, volatile oils, and trace elements are believed to contribute to the pharmacological activity of Black Seeds 22.
This randomized, double blind clinical trial 24 comparing the effect of black seed oil and fish oil in the treatment an autoimmune skin disease, vitiligo, where the body’s immune system destroy the melanocytes of the skin. The study found that skin application in 52 patients (40% female and 60% male of average age 45 years), the highest percentage of improvement in the black seed oil group was observed in the lower extremities, trunk, head, and neck; and in the fish oil group in the head and neck, trunk, and feet. The lowest percentage of improvement in the black seed oil group was observed in the head, neck, and hands; and in the fish oil group in the hands and lower extremities. No specific side effects were reported by patients during six months of treatment 24. Both black seed oil and fish oil were effective in reduction the size of patient’s lesions (vitiligo) 24. Most of the percent improvement observed in upper extremities, trunk, head, and neck of those who received black seed oil and head, neck, trunk, and feet for those who received fish oil.
The results of extensive pharmacological studies (in test tubes and on animal) on black seed and black seed oil found Black Seed have:
- Aanalgesic 25,
- Antilipemic 26, 27,
- Postcoital contraceptive 28,
- Diuretic and antihypertensive 29,
- Bronchodilator and calcium antagonist 30,
- Histamine release inhibitor 31, hepatoprotective 32,
- Anthelmintic 33,
- Antifungal 34,
- Antimicrobial (against a wide range of organisms) 35,
- Anticancer 36,
- Diminishing the risk of atherosclerosis by decreasing the serum low density lipoprotein cholesterol level and increasing the serum high density lipoprotein cholesterol levels 37,
- Exerts therapeutic and protective effect in diabetes by decreasing morphological changes and preserving pancreatic beta-cell integrity 38 and by beneficially changing the hepatic enzyme activities 39,
- Effective against hypertension 40,
- Has a potent antihistaminic effect on airways of asthmatic patients 41,
- Its components are promising agents to complement schistosomiasis specific treatment 42,
- Black seed oil protects kidney tissue against oxygen free radicals, preventing renal dysfunction and morphological abnormalities 43 and
- Anti-inflammatory activities 44.
Anticancer Activities of Black Seed (Black Cumin Seed)
Blood Cancer
El-Mahdy et al. 45 reported that Thymoquinone exhibits anti-proliferative effect in human myeloblastic leukemia HL-60 cells. Derivatives of thymoquinone bearing terpene-terminated 6-alkyl residues were tested in HL-60 cells and 518A2 melanoma by Effenberger et al. 46. They found the derivatives induce apoptosis associated with DNA laddering, a decrease in mitochondrial membrane potential and a slight increase in reactive oxygen species. Swamy and Huat 14 observed that α-hederin also induced death of murine leukemia P388 cells by a dose- and time-dependent increase in apoptosis.
Breast Cancer
Aqueous and alcohol extracts of black cumin seeds were found to be effective in vitro in inactivating MCF-7 breast cancer cells 47. Black cumin seeds, in combination with melatonin and retinoic acid reduced the carcinogenic effects of DMBA (7, 12-di-methylbenz(a)anthracene) in mammary carcinoma of rats 48. Terpene-terminated 6-alkyl residues of Thymoquinone were tested in MCF-7/Topo breast carcinoma by Effenberger et al. 46. They found the derivatives inducing cell death by apoptosis.
Colon Cancer
Gali-Muhtasib et al. 49 suggested that thymoquinone is anti-neoplastic and pro-apoptotic against colon cancer cell line HCT116. Salim and Fukushima 50 demonstrated that the volatile oil of black seed has the ability to inhibit colon carcinogenesis of rats in the post-initiation stage, with no evident adverse side effects. Norwood et al. 51 suggested thymoquinone as chemotherapeutic agent on SW-626 colon cancer cells, in potency, which is similar to 5-flurouracil in action. However, on HT-29 (colon adenocarcinoma) cell, no effect of thymoquinone was found 52.
Pancreatic Cancer
Chehl et al. 53 showed that thymoquinone, the major constituent of N. sativa oil extract, induced apoptosis and inhibited proliferation in PDA (pancreatic ductal adenocarcinoma) cells. They also suggested thymoquinone as a novel inhibitor of pro-inflammatory pathways, which provides a promising strategy that combines anti-inflammatory and proapoptotic modes of action. Thymoquinone also can abrogate gemcitabine- or oxaliplatin-induced activation of NF-kappa B, resulting in the chemosensitization of pancreatic tumors to conventional therapeutics 54. The high molecular weight glycoprotein mucin 4 (MUC4) is aberrantly expressed in pancreatic cancer and contributes to the regulation of differentiation, proliferation, metastasis, and the chemoresistance of pancreatic cancer cells. Torres et al. 55 evaluated the down-regulatory effect of thymoquinone on MUC4 in pancreatic cancer cells. But in a study, Rooney and Ryan 52 did not find any preventive role of thymoquinone on MIA PaCa-2 (pancreas carcinoma) cells.
Hepatic Cancer
The cytotoxic activity of N. sativa seed was tested on the human hepatoma HepG2 cell line by Thabrew et al. 56, and 88% inhibitory effect on HepG2 was found after 24-hr incubation with different concentrations (0–50 mg/ml) of the N. sativa extract. Nagi and Almakki 57 reported that oral administration of thymoquinone is effective in increasing the activities of quinone reductase and glutathione transferase and makes thymoquinone a promising prophylactic agent against chemical carcinogenesis and toxicity in hepatic cancer
Lung Cancer
Swamy and Huat 14 mentioned the antitumor activity of α-hederin from black cumin seed against LL/2 (Lewis Lung carcinoma) in BDF1 mice. Also, Mabrouk et al. 58 showed that supplementation of diet with honey and N. sativa has a protective effect against MNU (methylnitrosourea)-induced oxidative stress, inflammatory response and carcinogenesis in lung, skin and colon. However, Rooney and Ryan 52 reported that α-hederin and thymoquinone, the two principal bioactive constituents of N. sativa enhance neither cytotoxicity nor apoptosis in A549 (lung carcinoma), HEp-2 (larynx epidermoid carcinoma) cells.
Skin cancer
Topical application of black cumin seed extract inhibited two-stage initiation/promotion [dimethylbenz[a]anthracene (DMBA)/croton oil] skin carcinogenesis in mice. Again, intraperitoneal administration of black cumin seed (100 mg/kg body wt) 30 days after subcutaneous administration of MCA (20-methylcholanthrene) restricted soft tissue sarcomas to 33.3% compared with 100% in MCA-treated controls 59.
Fibrosarcoma
Thymoquinone from black cumin seed was administrated (0.01% in drinking water) one week before and after MCA treatment significantly inhibited the tumor incidence (fibrosarcoma) and tumor burden by 43% and 34%, respectively, compared with the results in the group receiving MCA alone. Moreover, Thymoquinone delayed the onset of MCA-induced fibrosarcoma tumors. Also in vitro studies showed that Thymoquinone inhibited the survival of fibrosarcoma cells with IC50 of 15 mM 60. Black cumin seed oil also decreased the fibrinolytic potential of the human fibrosarcoma cell line (HT1080) in vitro 61.
Renal Cancer
Khan and Sultana 62 reported the chemo-preventive effect of black seed against ferric nitrilotriacetate (Fe-NTA)-induced renal oxidative stress, hyper-proliferative response and renal carcinogenesis. Treatment of rats orally with black cumin seed (50 100 mg/kg body wt) resulted in significant decrease in H2O2 generation, DNA synthesis and incidence of tumors.
Prostate Cancer
Thymoquinone, from black seed, inhibited DNA synthesis, proliferation, and viability of cancerous (LNCaP, C4-B, DU145, and PC-3) but not non-cancerous (BPH-1) prostate epithelial cells by down-regulating AR (androgen receptor) and E2F-1 (a transcription factor) 63. In this study, they suggested thymoquinone as effective in treating hormone-sensitive as well as hormone-refractory prostate cancer. Yi et al. 64 found that thymoquinone blocked angiogenesis in vitro and in vivo, prevented tumor angiogenesis in a xenograft human prostate cancer (PC3) model in mouse, and inhibited human prostate tumor growth at low dosage with almost no chemotoxic side effects. Furthermore, they observed that endothelial cells were more sensitive to thymoquinone-induced cell apoptosis, cell proliferation, and migration inhibition compared with PC3 cancer cells. Thymoquinone also inhibited vascular endothelial growth factor-induced extracellular signal-regulated kinase activation but showed no inhibitory effects on vascular endothelial growth factor receptor 2 activation.
Cervical Cancer
Shafi et al. 65 reported that methanol, n-Hexane and chloroform extracts of black seed effectively killed HeLa (human epithelial cervical cancer) cells by inducing apoptosis. Effenberger et al. 46 tested terpene-terminated 6-alkyl residues of thymoquinone on multidrug-resistant KB-V1/Vb1 cervical carcinoma and found the derivatives inducing cell death by apoptosis.
Black seed oil side effects
Many toxicological studies have been carried out on black seeds. It has been shown that no toxic effects were reported when black seed oil was given to mice via the stomach in an acute study. In a chronic toxicity study rats treated daily with an oral dose for 3 months caused no changes in key hepatic enzyme levels particularly aspartate-aminotransferase, alanine-aminotranferase, and gammaglutamyl-transferase 66. Moreover, the histopathological results also showed to be normal for the tissues of heart, liver, kidneys and pancreas LD50 (LD 50 is a lethal dose, the amount of an ingested substance that kills 50 percent of a test sample. It is expressed in mg/kg, or milligrams of substance per kilogram of body weight) values of black seed oil of N. sativa obtained by single doses orally and intraperitoneally in mice, were reported to be 26.2-31.6 mg/kg and 1.86-2.26 mg/kg, respectively. The low toxicity of black seed oil, evidenced by high LD50 values, key hepatic enzyme stability and organ integrity, suggests a wide margin of safety for therapeutic doses of black seed oil 67. In another study, the LD50 of thymoquinone was found to be 104.7 mg/kg (89.7-119.7) and 870.9 mg/kg (647.1-1 094.8) after intra-peritoneal injection and oral ingestion respectively. Whereas, LD50 in rats was found to be 57.5 mg/kg (45.6-69.4) and 794.3 mg/kg (469.8-1 118.8) after intra-peritoneal injection and oral ingestion respectively. The LD50 values presented here after intra-peritoneal injection and oral gavages are 10-15 times and 100-150 times greater than doses of thymoquinone reported for its anti-inflammatory, anti-oxidant and anti-cancer effects. These observations revealed that thymoquinone is a relatively safe compound, particularly when given orally to experimental animals 68, 69.
- Nigella sativa. Wikipedia. https://en.wikipedia.org/wiki/Nigella_sativa[↩]
- Warrier PK, Nambiar VPK, Ramankutty . Chennai: Orient Longman Pvt Ltd; 2004. Indian medicinal plants-a compendium of 500 species; pp. 139–142.[↩][↩]
- https://www.smithsonianmag.com/arts-culture/nigella-seeds-what-the-heck-do-i-do-with-those-29298883[↩][↩]
- Bharat B Aggarwal. Molecular Targets and Therapeutic Uses of Spices. Google Books. p. 259. ISBN 978-981-4468-95-4.[↩]
- Bharat B Aggarwal. Molecular Targets and Therapeutic Uses of Spices. Google Books. p. 259. ISBN 978-981-4468-95-4. [↩]
- Phenolic composition and biological activities of Tunisian Nigella sativa L. shoots and roots. Bourgou S, Ksouri R, Bellila A, Skandrani I, Falleh H, Marzouk B. C R Biol. 2008 Jan; 331(1):48-55. https://www.ncbi.nlm.nih.gov/pubmed/18187122/[↩]
- Pharmacological and toxicological properties of Nigella sativa. Ali BH, Blunden G. Phytother Res. 2003 Apr; 17(4):299-305. https://www.ncbi.nlm.nih.gov/pubmed/12722128/[↩][↩]
- Atta-Ur-Rahman Nigellidine-a new indazole alkaloid from the seed of Nigella sativa. Tetrahedron Lett. 1995;36(12):1993–1994.[↩]
- Chemical composition of the fixed and volatile oils of Nigella sativa L. from Iran. Nickavar B, Mojab F, Javidnia K, Amoli MA. Z Naturforsch C. 2003 Sep-Oct; 58(9-10):629-31. https://www.ncbi.nlm.nih.gov/pubmed/14577620/[↩]
- High performance liquid chromatographic analysis of the pharmacologically active quinones and related compounds in the oil of the black seed (Nigella sativa L.). Ghosheh OA, Houdi AA, Crooks PA. J Pharm Biomed Anal. 1999 Apr; 19(5):757-62. https://www.ncbi.nlm.nih.gov/pubmed/10698539/[↩]
- Thymoquinone is a potent superoxide anion scavenger. Badary OA, Taha RA, Gamal el-Din AM, Abdel-Wahab MH. Drug Chem Toxicol. 2003 May; 26(2):87-98. https://www.ncbi.nlm.nih.gov/pubmed/12816394/[↩]
- Antimutagenic effects of ethanolic extracts from selected Palestinian medicinal plants. Khader M, Bresgen N, Eckl PM. J Ethnopharmacol. 2010 Feb 3; 127(2):319-24. https://www.ncbi.nlm.nih.gov/pubmed/19913082/[↩]
- Oral and intraperitoneal LD50 of thymoquinone, an active principle of Nigella sativa, in mice and rats. Al-Ali A, Alkhawajah AA, Randhawa MA, Shaikh NA. J Ayub Med Coll Abbottabad. 2008 Apr-Jun; 20(2):25-7. https://www.ncbi.nlm.nih.gov/pubmed/19385451/[↩]
- Intracellular glutathione depletion and reactive oxygen species generation are important in alpha-hederin-induced apoptosis of P388 cells. Swamy SM, Huat BT. Mol Cell Biochem. 2003 Mar; 245(1-2):127-39. https://www.ncbi.nlm.nih.gov/pubmed/12708752/[↩][↩][↩]
- Nigella sativa thymoquinone-rich fraction greatly improves plasma antioxidant capacity and expression of antioxidant genes in hypercholesterolemic rats. Ismail M, Al-Naqeep G, Chan KW. Free Radic Biol Med. 2010 Mar 1; 48(5):664-72. https://www.ncbi.nlm.nih.gov/pubmed/20005291/[↩]
- Khan MA, Tania M, Zhang DZ, Chen HC. Antioxidant enzymes and cancer. Chin J Cancer Res. 2010;22:87–92.[↩]
- Protective effects of Nigella sativa oil and thymoquinone against toxicity induced by the anticancer drug cyclophosphamide. Alenzi FQ, El-Bolkiny Yel-S, Salem ML. Br J Biomed Sci. 2010; 67(1):20-8. https://www.ncbi.nlm.nih.gov/pubmed/20373678/[↩]
- Sharma PC, Yelne MB, Dennis TJ. Database on medicinal plants used in Ayurveda. New Delhi: 2005. pp. 420–440.[↩]
- Goreja WG. Black seed: nature’s miracle remedy. New York, NY: Amazing Herbs Press; 2003.[↩]
- Yarnell E, Abascal K. Nigella sativa: holy herb of the middle East. Altern Compl Therap. 2011;17(2):99–105.[↩]
- From here to eternity – the secret of Pharaohs: Therapeutic potential of black cumin seeds and beyond. Padhye S, Banerjee S, Ahmad A, Mohammad R, Sarkar FH. Cancer Ther. 2008; 6(b):495-510. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2583426/[↩]
- Tariq M. Nigella Sativa Seeds: Folklore Treatment in Modern Day Medicine. Saudi Journal of Gastroenterology : Official Journal of the Saudi Gastroenterology Association. 2008;14(3):105-106. doi:10.4103/1319-3767.41725. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2702918/[↩][↩][↩][↩]
- Nadkarni AK. Indian materia medica. 3rd ed. Mumbai: Popular Prakashan Pvt. Ltd; 1976. pp. 301–40.[↩]
- Ghorbanibirgani A, Khalili A, Rokhafrooz D. Comparing Nigella sativa Oil and Fish Oil in Treatment of Vitiligo. Iranian Red Crescent Medical Journal. 2014;16(6):e4515. doi:10.5812/ircmj.4515. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4102993/[↩][↩][↩]
- Abdel-Fattah AM, Matsumoto K, Watanabe H. Antinociceptive effects of Nigella sativa oil and its major component, thymoquinone, in mice. Eur J Pharmacol. 2000;400:89–97.[↩]
- Bashandy SA. Effects of Nigella sativa oil on liver and kidney functions of adult and senile rats. Egypt J Pharm Sci. 1996;37:313–27.[↩]
- Hassanim NI, Hassan FM. A preliminary study on the effect of Nigella sativa seeds on hypoglycemia. Vet Med J Giza. 1996;44:699–708.[↩]
- Keshri G, Singh MM, Lakshmi V, Kamboj VP. Post-coital contraceptive efficacy of the seeds of Nigella sativa in rats. Indian J Physiol Pharmacol. 1995;39:59–62.[↩]
- Zaoui A, Cherrah Y, Lacaille-Dubois MA, Settaf A, Amarouch H, Hassar M. Diuretic and hypotensive effects of Nigella sativa in the spontaneously hypertensive rat. Therapie. 2000;55:379–82.[↩]
- Gilani AH, Aziz N, Khurram IM, Chaudhary KS, Iqbal A. Bronchodilator, spasmolytic and calcium anatagonist activities of Nigella sativa seeds (Kalonji): A traditional herbal product with multiple medicinal uses. J Pak Med Assoc. 2001;51:115–20.[↩]
- Chakravarty N. Inhibition of histamine release from mast cells by nigellone. Ann Allergy. 1993;70:237–42.[↩]
- Daba MH, Abdel-Rahman MS. Hepatoprotective activity of thymoquinone in isolated rat hepatocytes. Toxicol Let. 1998;95:23–9.[↩]
- Akhtar MS, Riffat S. Field trial of Saussurea lappa roots against nematodes and Nigella sativa seeds against cestodes in children. J Pakistan Med Assoc. 1991;41:185–7.[↩]
- Khan MA, Ashfaq MK, Zuberi HS, Mahmood MS, Gilani AH. The in vivo antifungal activity of the aqueous extract from Nigella sativa seeds. Phytother Res. 2003;17:183–6.[↩]
- Sokmen A, Jones BM, Erturk M. The in vitro antibacterial activity of Turkish medicinal plants. J Ethnopharmacol. 1999;67:79–86.[↩]
- Worthen DR, Ghosheh OA, Crooks PA. The in vitro anti-tumour activity of some crude and purified components of black seeds, Nigella sativa L. Anticancer Res. 1998;18:1527–32.[↩]
- Protective effects of propolis and thymoquinone on development of atherosclerosis in cholesterol-fed rabbits. Nader MA, el-Agamy DS, Suddek GM. Arch Pharm Res. 2010 Apr; 33(4):637-43. https://www.ncbi.nlm.nih.gov/pubmed/20422375/[↩]
- Protective effects of the volatile oil of Nigella sativa seeds on beta-cell damage in streptozotocin-induced diabetic rats: a light and electron microscopic study. Kanter M, Akpolat M, Aktas C. J Mol Histol. 2009 Oct; 40(5-6):379-85. https://www.ncbi.nlm.nih.gov/pubmed/20049514/[↩]
- Beneficial effects of thymoquinone on hepatic key enzymes in streptozotocin-nicotinamide induced diabetic rats. Pari L, Sankaranarayanan C. Life Sci. 2009 Dec 16; 85(23-26):830-4. https://www.ncbi.nlm.nih.gov/pubmed/19903489/[↩]
- Antihypertensive effect of Nigella sativa seed extract in patients with mild hypertension. Dehkordi FR, Kamkhah AF. Fundam Clin Pharmacol. 2008 Aug; 22(4):447-52. https://www.ncbi.nlm.nih.gov/pubmed/18705755/[↩]
- Antiasthmatic effect of Nigella sativa in airways of asthmatic patients. Boskabady MH, Mohsenpoor N, Takaloo L. Phytomedicine. 2010 Aug; 17(10):707-13. https://www.ncbi.nlm.nih.gov/pubmed/20149611/[↩]
- The effect of antioxidant properties of aqueous garlic extract and Nigella sativa as anti-schistosomiasis agents in mice. El Shenawy NS, Soliman MF, Reyad SI. Rev Inst Med Trop Sao Paulo. 2008 Jan-Feb; 50(1):29-36. https://www.ncbi.nlm.nih.gov/pubmed/18327484/[↩]
- The protective effect of thymoquinone, an anti-oxidant and anti-inflammatory agent, against renal injury: a review. Ragheb A, Attia A, Eldin WS, Elbarbry F, Gazarin S, Shoker A. Saudi J Kidney Dis Transpl. 2009 Sep; 20(5):741-52. https://www.ncbi.nlm.nih.gov/pubmed/19736468/[↩]
- Mutabagani A, El-Mahdy , Samiha HM. A study of anti-inflammatory activity of Nigella sativa L and thymoquinone in rats. Saudi Pharm J. 1997;5:110–3.[↩]
- Thymoquinone induces apoptosis through activation of caspase-8 and mitochondrial events in p53-null myeloblastic leukemia HL-60 cells. El-Mahdy MA, Zhu Q, Wang QE, Wani G, Wani AA. Int J Cancer. 2005 Nov 10; 117(3):409-17. https://www.ncbi.nlm.nih.gov/pubmed/15906362/[↩]
- Terpene conjugates of the Nigella sativa seed-oil constituent thymoquinone with enhanced efficacy in cancer cells. Effenberger K, Breyer S, Schobert R. Chem Biodivers. 2010 Jan; 7(1):129-39. https://www.ncbi.nlm.nih.gov/pubmed/20087986/[↩][↩][↩]
- Effect of Nigella sativa (N. sativa L.) and oxidative stress on the survival pattern of MCF-7 breast cancer cells. Farah IO, Begum RA. Biomed Sci Instrum. 2003; 39():359-64. https://www.ncbi.nlm.nih.gov/pubmed/12724920/[↩]
- The biochemical and morphological alterations following administration of melatonin, retinoic acid and Nigella sativa in mammary carcinoma: an animal model. el-Aziz MA, Hassan HA, Mohamed MH, Meki AR, Abdel-Ghaffar SK, Hussein MR. Int J Exp Pathol. 2005 Dec; 86(6):383-96. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2517452/[↩]
- Thymoquinone extracted from black seed triggers apoptotic cell death in human colorectal cancer cells via a p53-dependent mechanism. Gali-Muhtasib H, Diab-Assaf M, Boltze C, Al-Hmaira J, Hartig R, Roessner A, Schneider-Stock R. Int J Oncol. 2004 Oct; 25(4):857-66. https://www.ncbi.nlm.nih.gov/pubmed/15375533/[↩]
- Chemopreventive potential of volatile oil from black cumin (Nigella sativa L.) seeds against rat colon carcinogenesis. Salim EI, Fukushima S. Nutr Cancer. 2003; 45(2):195-202. https://www.ncbi.nlm.nih.gov/pubmed/12881014/[↩]
- Comparison of potential chemotherapeutic agents, 5-fluoruracil, green tea, and thymoquinone on colon cancer cells. Norwood AA, Tan M, May M, Tucci M, Benghuzzi H. Biomed Sci Instrum. 2006; 42():350-6. https://www.ncbi.nlm.nih.gov/pubmed/16817633/[↩]
- Modes of action of alpha-hederin and thymoquinone, active constituents of Nigella sativa, against HEp-2 cancer cells. Rooney S, Ryan MF. Anticancer Res. 2005 Nov-Dec; 25(6B):4255-9. http://ar.iiarjournals.org/content/25/6B/4255.long[↩][↩][↩]
- Anti-inflammatory effects of the Nigella sativa seed extract, thymoquinone, in pancreatic cancer cells. Chehl N, Chipitsyna G, Gong Q, Yeo CJ, Arafat HA. HPB (Oxford). 2009 Aug; 11(5):373-81. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2742606/[↩]
- Antitumor activity of gemcitabine and oxaliplatin is augmented by thymoquinone in pancreatic cancer. Banerjee S, Kaseb AO, Wang Z, Kong D, Mohammad M, Padhye S, Sarkar FH, Mohammad RM. Cancer Res. 2009 Jul 1; 69(13):5575-83. http://cancerres.aacrjournals.org/content/69/13/5575.long[↩]
- Effects of thymoquinone in the expression of mucin 4 in pancreatic cancer cells: implications for the development of novel cancer therapies. Torres MP, Ponnusamy MP, Chakraborty S, Smith LM, Das S, Arafat HA, Batra SK. Mol Cancer Ther. 2010 May; 9(5):1419-31. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2906253/[↩]
- Cytotoxic effects of a decoction of Nigella sativa, Hemidesmus indicus and Smilax glabra on human hepatoma HepG2 cells. Thabrew MI, Mitry RR, Morsy MA, Hughes RD. Life Sci. 2005 Aug 5; 77(12):1319-30. https://www.ncbi.nlm.nih.gov/pubmed/15916774/[↩]
- Thymoquinone supplementation induces quinone reductase and glutathione transferase in mice liver: possible role in protection against chemical carcinogenesis and toxicity. Nagi MN, Almakki HA. Phytother Res. 2009 Sep; 23(9):1295-8. https://www.ncbi.nlm.nih.gov/pubmed/19277968/[↩]
- Inhibition of methylnitrosourea (MNU) induced oxidative stress and carcinogenesis by orally administered bee honey and Nigella grains in Sprague Dawely rats. Mabrouk GM, Moselhy SS, Zohny SF, Ali EM, Helal TE, Amin AA, Khalifa AA. J Exp Clin Cancer Res. 2002 Sep; 21(3):341-6. https://www.ncbi.nlm.nih.gov/pubmed/12385575/[↩]
- Inhibitory effects of Nigella sativa and saffron (Crocus sativus) on chemical carcinogenesis in mice. Salomi MJ, Nair SC, Panikkar KR. Nutr Cancer. 1991; 16(1):67-72. https://www.ncbi.nlm.nih.gov/pubmed/1923908/[↩]
- Inhibitory effects of thymoquinone against 20-methylcholanthrene-induced fibrosarcoma tumorigenesis. Badary OA, Gamal El-Din AM. Cancer Detect Prev. 2001; 25(4):362-8. https://www.ncbi.nlm.nih.gov/pubmed/11531013/[↩]
- In vitro decreases of the fibrinolytic potential of cultured human fibrosarcoma cell line, HT1080, by Nigella sativa oil. Awad EM. Phytomedicine. 2005 Jan; 12(1-2):100-7. https://www.ncbi.nlm.nih.gov/pubmed/15693715/[↩]
- Inhibition of two stage renal carcinogenesis, oxidative damage and hyperproliferative response by Nigella sativa. Khan N, Sultana S. Eur J Cancer Prev. 2005 Apr; 14(2):159-68. https://www.ncbi.nlm.nih.gov/pubmed/15785320/[↩]
- Androgen receptor and E2F-1 targeted thymoquinone therapy for hormone-refractory prostate cancer. Kaseb AO, Chinnakannu K, Chen D, Sivanandam A, Tejwani S, Menon M, Dou QP, Reddy GP. Cancer Res. 2007 Aug 15; 67(16):7782-8. http://cancerres.aacrjournals.org/content/67/16/7782.long[↩]
- Thymoquinone inhibits tumor angiogenesis and tumor growth through suppressing AKT and extracellular signal-regulated kinase signaling pathways. Yi T, Cho SG, Yi Z, Pang X, Rodriguez M, Wang Y, Sethi G, Aggarwal BB, Liu M. Mol Cancer Ther. 2008 Jul; 7(7):1789-96. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2587125/[↩]
- Induction of apoptosis in HeLa cells by chloroform fraction of seed extracts of Nigella sativa. Shafi G, Munshi A, Hasan TN, Alshatwi AA, Jyothy A, Lei DK. Cancer Cell Int. 2009 Nov 27; 9():29. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2794855/[↩]
- Ahmad A, Husain A, Mujeeb M, et al. A review on therapeutic potential of Nigella sativa: A miracle herb. Asian Pacific Journal of Tropical Biomedicine. 2013;3(5):337-352. doi:10.1016/S2221-1691(13)60075-1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3642442/[↩]
- Zaoui A, Cherrah Y, Mahassini N, Alaoui K, Amarouch H, Hassar M. Acute and chronic toxicity of Nigella sativa fixed oil. Phytomedicine. 2002;9(1):69–74. https://www.ncbi.nlm.nih.gov/pubmed/11924767[↩]
- Khader M, Bresgen N, Eckl PM. In vitro toxicological properties of thymoquinone. Food Chem Toxicol. 2009;47(1):129–133. https://www.ncbi.nlm.nih.gov/pubmed/19010375[↩]
- Al-Ali A, Alkhawajah AA, Randhawa MA, Shaikh NA. Oral and intraperitoneal LD50 of thymoquinone, an active principle of Nigella sativa, in mice and rats. J Ayub Med Coll Abbottabad. 2008;20(2):25–27. https://www.ncbi.nlm.nih.gov/pubmed/19385451[↩]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}