
Ozempic
Ozempic is a brand name for a weekly subcutaneous injection medicine called Semaglutide that is used together with diet and exercise to treat type 2 diabetes in adults to help control blood sugar levels 1, 2. Ozempic is also used to lower the risk of heart attack, stroke, or death in patients with type 2 diabetes, obesity, and heart or blood vessel disease. Ozempic is also used to lower the risk of worsening of kidney disease, kidney failure (end-stage kidney disease), and death caused by heart or blood vessel disease in adults with type 2 diabetes and chronic kidney disease (CKD). Other brand names for Semaglutide are Rybelus (daily oral tablet) and Wegovy (subcutaneous weekly injection) including Ozempic are all made by Novo Nordisk 3, 2. Semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist also called glucagon-like peptide-1 (GLP-1) analogue, is approved by the U.S. Food and Drug Administration (FDA) as 3 separate brand name medications—Ozempic, Wegovy, and Rybelsus. Note that each brand name comes with its own uses (indications), preparations, and dosages to consider.
- Ozempic (semaglutide) injection
- Ozempic is used to treat type 2 diabetes in adults to help control blood sugar (glucose) levels used together with balanced diet and exercise 4, 5.
- Ozempic is also used for reducing major cardiovascular event risks such as heart attack, stroke, or death in adults with type 2 diabetes with known heart disease.
- Ozempic is also used to reduce the risk of kidney function decline, kidney failure, and death due to cardiovascular disease, in adults with chronic kidney disease (CKD) and type 2 diabetes
- Ozempic injection is given 1 time a week under your skin (subcutaneous) of your stomach (belly), your thigh, or your upper arm, using an autoinjector (pen).
- Wegovy (semaglutide) injection
- Wegovy (semaglutide) injection is used for weight loss and weight maintenance in patients 12 years and older with obesity 6, 7.
- Wegovy is also used for reducing major cardiovascular event risks such as heart attack, stroke, or death in adults with type 2 diabetes with known heart disease
- Wegovy injection is given 1 time a week under your skin (subcutaneous) of your stomach (belly), your thigh, or your upper arm, using an autoinjector (pen)
- Wegovy injection should be used in addition to a reduced-calorie diet and increased physical activity
- Rybelsus (semaglutide) oral tablets
- Rybelsus tablets are used to treat type 2 diabetes in adults to help control blood sugar (glucose) levels.
- Rybelsus oral tablet is taken daily
- Rybelsus tablets should be used in addition to a reduced-calorie diet and increased physical activity.
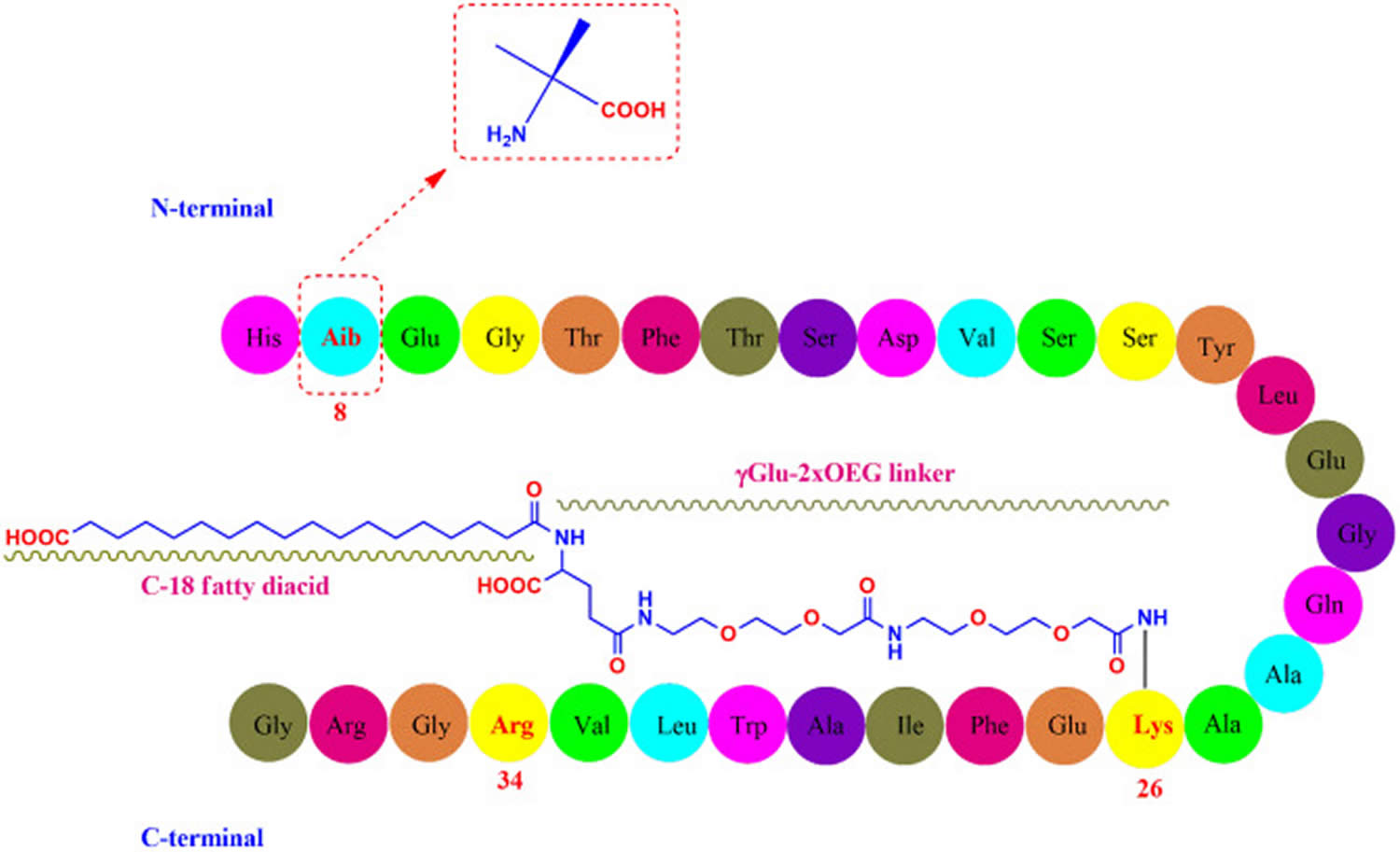
Semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist that acts like the native gut hormone (an incretin) to increase insulin secretion. Semaglutide is a recombinant DNA-produced polypeptide that is 94% homologous to endogenous human GLP-1 and differs only by minor amino acid substitutions and other structural modifications at positions 8, 26, and 34, which prolong its half-life (T1/2) and make it resistant to degradation by dipeptidyl peptidase 4 (DPP4) 8, 9. Semaglutide, like other glucagon-like peptide-1 (GLP-1) receptor agonists, is given parenterally, but its long half-life allows weekly dosing. Semaglutide has been shown to improve blood sugar control in patients with type 2 diabetes was approved as an add-on to diet and exercise for use use in the United States in 2017 under the brand name Ozempic, the sixth GLP-1 receptor agonist to be approved for treatment of diabetes. Indications for Ozempic were later expanded to include reduction of the risk of major adverse cardiovascular events and risk of end-stage kidney disease in patients with type 2 diabetes and established cardiovascular or chronic kidney disease disease. Semaglutide is available in single-patient-use, multi-dose pens of 2, 4 and 8 mg in 3 mL. The recommended starting dose is 0.25 mg by subcutaneous injection once weekly with subsequent increases at 4-week intervals to 0.5 and then 1 mg once weekly.
Figure 1. Semaglutide molecular structure
Recent studies indicated that semaglutide is absorbed orally to some degree and high doses (7 to 14 mg) are as effective as parenteral doses (0.25 to 1.0 mg) in improving blood sugar control and inducing weight loss 9, 11. Oral semaglutide was approved as an adjunct to diet and exercise for treatment of type 2 diabetes in 2024 under the brand name Rybelsus. Rybelsus is available in two formulations: R1 formulations in tablets of 3, 7, and 14 mg, and R2 formulations as tablets of 1.5, 4 and 9 mg. The starting dose for Rybelsus R1 is 3 mg, and for Rybelsus R2 is 1.5 mg daily for the first 30 days followed by dose escalations at 30-day intervals to as high as 14 for R1 and 9 mg daily for R2.
Semaglutide also causes weight loss particularly when given in high doses 2. Semaglutide appears to cause weight loss by decreasing hunger and increasing satiety as well as by delaying gastric emptying 12. Weight loss can be profound resulting in a 10 to 15% decline in body weight 12. However, relapse is common when semaglutide is discontinued and its long-term safety and efficacy remain uncertain. Semaglutide was approved as a weight loss agent for persons who are overweight or obese in 2021 under the brand name Wegovy. Since initial approval, indications for Wegovy have been expanded to include children with obesity who are above the age of 12 years and for overweight or obese adults with established cardiovascular disease to reduce the risk of major adverse cardiovascular events. For all indications it is described as an adjunct to diet and exercise. For weight loss, semaglutide is available in prefilled single dose pens that deliver doses of 0.25, 0.5, 1.0, 1.7 and 2.4 mg. The usual starting dose is 0.25 mg by subcutaneous injection once weekly, which can be increased at 4-week intervals to 0.5, 1.0, 1.7 and 2.4 mg weekly based upon efficacy and tolerance.
The SUSTAIN clinical trials have exhibited favorable outcomes in reducing hemoglobin A1C (HbA1c) in patients with type 2 diabetes through the weekly subcutaneous semaglutide brand name Ozempic 2. These trials compared semaglutide injection to placebo (SUSTAIN 1), sitagliptin (SUSTAIN 2), exenatide extended-release (SUSTAIN 3), daily insulin glargine with metformin and/or a sulfonylurea (SUSTAIN 4), and basal insulin with or without metformin (SUSTAIN 5) 13, 14, 15, 16, 17. Each trial demonstrated statistically significant reductions in HbA1c (hemoglobin A1C) with semaglutide.
Upon further examination of signals indicating cardiovascular benefits identified in the first 5 SUSTAIN trials, the SUSTAIN 6 trial examined the effects of semaglutide (Ozempic) versus placebo over 2 years on a composite outcome comprising cardiovascular death, nonfatal heart attack, and nonfatal stroke in patients with type 2 diabetes 18. The estimated hazard ratio for the time-to-first event of the composite outcome was 0.74, indicating semaglutide (Ozempic) therapy has reduced the hazard of cardiovascular death, nonfatal heart attack, and nonfatal stroke by 26% over placebo.
Following the positive findings from the SUSTAIN clinical trial program, the FDA approved weekly subcutaneous semaglutide (Ozempic) as an add-on to diet and exercise for managing type 2 diabetes in adults. In addition, Ozempic is approved for reducing the risk of major cardiovascular events, including cardiovascular death, nonfatal heart attack, and nonfatal stroke, in adults with type 2 diabetes and established cardiovascular disease.
The PIONEER clinical trials program has demonstrated the effectiveness of oral semaglutide (Rybelsus) in managing type 2 diabetes compared to placebo (PIONEER 1), empagliflozin (PIONEER 2), sitagliptin with or without metformin and/or a sulfonylurea (PIONEER 3 and PIONEER 7), liraglutide (PIONEER 4), and basal insulin with or without metformin (PIONEER 8) 19, 20, 21, 22, 23, 24, 25. The PIONEER 6 trial examined the benefits of oral semaglutide (Rybelsus) on the risk of major cardiovascular events similar to the SUSTAIN 6 trial in patients with type 2 diabetes. In the PIONEER 6 trial, noninferiority with placebo was demonstrated in the composite outcome of cardiovascular death, nonfatal heart attack, and nonfatal stroke in patients with type 2 diabetes 26.
Based on the favorable results observed in the type 2 diabetes trials, the FDA has approved oral semaglutide (Rybelsus) as an add-on to diet and exercise for managing type 2 diabetes. This marks the first approval of an oral GLP-1 receptor agonist for type 2 diabetes management. Unlike injectable semaglutide (Ozempic), oral semaglutide (Rybelsus) does not decrease major cardiovascular events.
The Semaglutide Treatment Effect in People with Obesity (STEP) clinical trial investigated the effects of weekly subcutaneous Semaglutide under the brand name Wegovy on weight loss in adult patients with obesity (BMI ≥30 kg/m²) or in patients who are overweight (BMI ≥27 kg/m²) with comorbidities 27, 28, 29, 30, 31. Following the positive outcomes observed in the 4 STEP trials (STEPs 1, 2, 3, and 4), the FDA has approved the use of 2.4 mg weekly subcutaneous semaglutide (Wegovy) for weight management in adult patients with obesity and in patients who are overweight with at least 1 weight-related condition, such as high blood pressure (hypertension), type 2 diabetes, or dyslipidemia (high cholesterol or high triglycerides). The recommended approach for weight management includes the integration of semaglutide with a balanced diet and regular exercise.
Another active comparator trial, the STEP 8 trial, compared subcutaneous weekly semaglutide (Wegovy) to subcutaneous daily liraglutide injection (another anti-diabetic medication used to treat type 2 diabetes, and obesity), revealing semaglutide’s superiority in the primary outcome of mean percentage change in body weight 32. In this randomized clinical trial that included 338 participants, mean body weight change from baseline to 68 weeks was –15.8% with semaglutide vs –6.4% with liraglutide, a statistically significant difference 32.
The STEP TEENS trial examined the efficacy and safety of semaglutide (Wegovy) compared to placebo in adolescents aged 12 to less than 18 with obesity. The STEP TEENS trial revealed that subcutaneous semaglutide (Wegovy) at a dosage of 2.4 mg weekly, along with lifestyle interventions, provided superior reductions in body mass index (BMI) in adolescents than placebo and lifestyle interventions 33.
Semaglutide is moderately well tolerated, but side effects can be dose limiting and include injection site reactions, diarrhea, nausea, vomiting, abdominal pain, dizziness, headache, fatigue and hypoglycemia. Rare potential adverse events include pancreatitis, thyroid C-cell tumors, and hypersensitivity reactions. Recently, long-term semaglutide therapy (greater than 2 years) has been linked to ischemic optic neuropathy particularly in persons with diabetes and hypertension.
In rodents study, Semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. The thyroid gland has 2 main types of cells: (1) Follicular cells use iodine from the blood to make thyroid hormones. These hormones help regulate your metabolism. (2) C cells also called parafollicular cells make calcitonin, a hormone that helps control how your body uses calcium.
It is unknown whether Ozempic causes thyroid C-cell tumors, including medullary thyroid cancer also known as medullary thyroid carcinoma, in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined 34, 3.
Ozempic is contraindicated in patients with a personal or family history of medullary thyroid cancer and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for medullary thyroid cancer with the use of Ozempic and inform them of symptoms of thyroid tumors (eg, a mass in the neck, dysphagia [difficulty swallowing], dyspnea [shortness of breath], persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of medullary thyroid cancer in patients treated with Ozempic.
Precautions
Suicidal behavior has been reported with other medications prescribed for weight management. Therefore, it is advisable to avoid the use of Semaglutide in individuals with a history of suicidal attempts or current suicidal ideation. Patients with suicidal ideations should seek immediate assistance.
Semaglutide can potentially slow gastric emptying and impede the absorption of other medications.
The multiple-dose injection pen (Ozempic) should not be shared among individuals to mitigate the risk of infection transmitting infections.
Semaglutide is contraindicated in patients with type 1 diabetes.
As the effectiveness of semaglutide in combination with other weight loss medications is not established, concurrent use of this drug with other weight loss medications should be avoided.
Patients with a history of weight loss surgery face an increased risk of gastrointestinal complications when using semaglutide. Therefore, regular monitoring for such complications is recommended.
If Semaglutide is discontinued after attaining weight loss, a risk of rebound weight gain exists. This was demonstrated in an extension of the STEP 1 trial, where participants, after discontinuing weekly subcutaneous semaglutide 2.4 mg and lifestyle interventions for 1 year, experienced a regain of approximately two-thirds of their initial weight loss 35.
What is the difference between Ozempic, Wegovy, and Rybelsus?
Ozempic, Wegovy, and Rybelsus are 3 brand names of the same drug Semaglutide that is approved by the US Food and Drug Administration (FDA) 2:
- Ozempic injection: Ozempic injection is FDA-approved to treat type 2 diabetes in adults to help control blood sugar levels to be used together with diet and exercise. Ozempic injection also provides an additional indication of reducing the risk of major adverse cardiovascular events, such as cardiovascular death, nonfatal heart attack, or nonfatal stroke, in patients with and without 2 diabetes mellitus and established cardiovascular disease.
- Wegovy injection: In a recent development, semaglutide received FDA approval for promoting weight loss in individuals dealing with obesity and overweight under the brand name Wegovy. Wegovy injection is used in combination with a reduced-calorie diet and increased physical activity for long-term weight management in adults with obesity, defined by an initial body mass index (BMI) of 30 kg/m² or higher. Wegovy injection is also approved for those who are overweight, with a BMI of 27 kg/m² or higher, in the presence of at least a weight-related comorbid condition such as high blood pressure (hypertension), type 2 diabetes, or dyslipidemia (abnormal levels of lipids or fats in your blood, including high cholesterol and high triglycerides). The FDA has also approved Wegovy injection for use in children aged 12 and older with an initial BMI at or above the 95th percentile for their age and sex.
- Rybelsus tablets: Rybelsus tablet has received FDA approval in addition to diet and exercise for enhancing blood sugar in adults with type 2 diabetes mellitus.
If you are wondering whether to choose Wegovy or Ozempic injection, you might compare their FDA-approved uses, side effects and costs. Both Wegovy and Ozempic contain semaglutide (the active drug), Ozempic is used to control blood sugar levels in adults with type 2 diabetes, while Wegovy is prescribed long-term weight loss in adults and children. Both Wegovy and Ozempic injection lower the risk for heart-related complications, but they differ in other FDA-approved uses, doses, target populations and costs.
Ozempic can also help protect your kidneys. Ozempic is approved to reduce the risk of worsening kidney disease and cardiovascular death in patients with type 2 diabetes and chronic kidney disease. Wegovy does not have this FDA-approval.
- Ozempic is used to improve blood sugar control in adults with type 2 diabetes.
- Ozempic is used to reduce the risk of major cardiovascular events (e.g., heart attack, stroke, heart-related death) in adults with type 2 diabetes and heart disease
- Ozempic is used to reduce the risk of worsening kidney disease and cardiovascular death in patients with type 2 diabetes and chronic kidney disease.
- Wegovy is used to help adults and children aged 12 years and older with obesity, or adults who are overweight and have weight-related medical problems (for example: high blood pressure, high cholesterol, or diabetes) lose weight and keep the weight off long-term. If you are only looking for a weight loss medicine, studies have shown that Wegovy can lead to significant weight loss whether you have type 2 diabetes or not.
- Wegovy is also used to reduce the risk of major heart-related events such as death, heart attack or stroke in adults with known heart disease and with either obesity or overweight.
While Wegovy or Ozempic injection have lots of similarities, they have some important differences, too. Furthermore, there are no Ozempic vs Wegovy comparison studies for weight loss, but studies suggest that higher doses of semaglutide may lead to greater weight loss. Overall, you may lose more weight with Wegovy because it’s typically prescribed at a higher dose than Ozempic. In addition, separate studies looking at both drugs have shown greater weight loss with Wegovy over the long-term.
The Wegovy brand of semaglutide contains a higher maximum dose of semaglutide (2.4 mg) which may result in a greater weight loss for you. In studies with Wegovy, adults lost around 15% of their body weight, equal to about 35 lb (16 kg) over 68 weeks. With Ozempic, people have lost on average about 14 lbs (6.4 kgs) over 40 weeks using the 2 mg weekly dose of Ozempic to treat type 2 diabetes. Ozempic has also resulted in significantly more weight loss when compared to other type 2 diabetes treatments like Bydureon (exenatide), Januvia (sitagliptin) or Trulicity (dulaglutide). You and your doctor can work together to weigh the pros and cons and determine which treatment is right for you.
People respond to medicines differently, so your weight loss may be more or less than those in the studies. However, most people who continue on treatment respond well to Ozempic or Wegovy. These treatments are also used in addition to a low calorie diet and increased exercise for best effect.
Table 1. Ozempic, Wegovy, and Rybelsus Uses, Dosage
| Semaglutide brand | Ozempic | Wegovy | Rybelsus |
|---|---|---|---|
| Form | Subcutaneous injection | Subcutaneous injection | Tablet |
| Strength | 0.25 mg or 0.5 mg dose pen, 1 mg dose pen, 2mg dose pen. | 0.25 mg dose pen, 0.5 mg dose pen, 1 mg dose pen, 1.7 mg dose pen, 2.4 mg dose pen | R1 formulation: 3 mg tablet, 7 mg tablet, and 14 mg tablet R2 formulation: 1.5 mg, 4 mg, and 9 mg tablet |
| Dose | Weekly | Weekly | Daily |
| Uses |
|
|
|
Footnotes: Semaglutide brand names. Each brand is FDA-approved for different conditions. Semaglutide FDA approval was first granted on December 5, 2017, for the brand Ozempic.
How does Ozempic work?
Semaglutide is a recombinant DNA produced polypeptide analogue of human glucagon-like peptide-1 (GLP-1) also called glucagon-like peptide-1 (GLP-1) receptor agonist, sharing a remarkable 94% structural homology with human glucagon-like peptide-1 (GLP-1) 38, 39. The mechanisms through which semaglutide delivers its benefits in lowering blood glucose levels and promoting weight loss involve the activation of glucagon-like peptide-1 (GLP-1) receptors primarily located in the gastrointestinal tract, pancreas, and brain 2. Upon activation of the GLP-1 receptor (GLP-1R), semaglutide enhances glucose-dependent insulin secretion, providing a physiological response to elevated blood glucose levels after a meal 40. Simultaneously, semaglutide slows gastric emptying, increasing pancreatic beta-cell proliferation, and reduces glucagon release, contributing to an overall reduction in appetite 40, 41.
Furthermore, semaglutide’s interaction with glucagon-like peptide-1 (GLP-1) receptors in the hypothalamus may mitigate sensations of hunger, alleviate food cravings, and enhance the feelings of satiety 42, 43. These multifaceted actions contribute to the metabolic effects of semaglutide in managing blood glucose levels and facilitating weight loss 2.
Semaglutide is also considered a “long-acting” glucagon-like peptide-1 (GLP-1) receptor agonist, alongside extended-release exenatide and dulaglutide 44. The extended half-life of semaglutide may be attributed to 2 structural modifications—one modification promotes albumin binding, leading to prolonged kidney clearance, whereas the other shields it from metabolic degradation by the dipeptidyl peptidase-4 (DPP-4) enzyme 44.
Absorption
Subcutaneous semaglutide has high bioavailability (89%), with peak concentration achieved within 1 to 3 days of initiation 45. Achieving steady-state exposure typically occurs after 4 to 5 weeks of weekly subcutaneous administration, demonstrating a proportional increase with escalating doses up to 2.4 mg 2.
Due to the high homology to human GLP-1 peptide, oral semaglutide possesses properties inherent to peptide-like compounds. These include high molecular weight, susceptibility to enzymatic degradation, hydrophilicity, and low permeability, resulting in minimal bioavailability of approximately 0.01% 46, 47, 48, 49. To address this limitation, an absorption enhancer called sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC) is incorporated, enhancing the transcellular absorption of oral semaglutide across the gastric mucosa 46. The commercially available oral semaglutide exhibits an improved, although still minimal, bioavailability range of 0.4% to 1% 50. Gastric fluid composition, influenced by food and increased water volumes, significantly affects oral semaglutide absorption 46, 51. After oral administration, the maximum concentration of semaglutide is typically reached within 1 hour post-dose. Steady-state exposure is typically achieved after 4 to 5 weeks of daily administration 52.
Distribution
Following subcutaneous administration, the mean apparent volume of distribution for semaglutide is approximately 12.5 L 53. In healthy subjects, the volume of distribution is approximately 8 L following oral administration 52.
Metabolism
Semaglutide undergoes metabolism through the proteolytic cleavage of the peptide backbone, followed by sequential beta-oxidation of the fatty acid sidechain 54.
Elimination
Both oral and subcutaneous semaglutide have an elimination half-life of approximately 1 week, remaining in circulation for about 5 weeks after the last dose 2. The clearance of subcutaneous semaglutide in individuals with type 2 diabetes or obesity or those who are overweight is approximately 0.05 L/hour 2. In comparison, the clearance of oral semaglutide in healthy subjects is approximately 0.04 L/hour 52, 53. Semaglutide is primarily eliminated in the urine (3% as an unchanged drug) and feces 52, 55.
Ozempic uses
Ozempic injection is used to 34, 3:
- improve blood sugar control in adults with type 2 diabetes.
- reduce the risk of major cardiovascular events (e.g., heart attack, stroke, heart-related death) in adults with type 2 diabetes and heart disease
- reduce the risk of worsening kidney disease and cardiovascular death in patients with type 2 diabetes and chronic kidney disease.
Wegovy injection is used to 36, 37:
- help adults and children aged 12 years and older with obesity, or adults who are overweight and have weight-related medical problems (for example: high blood pressure, high cholesterol, or diabetes) lose weight and keep the weight off long-term.
- Wegovy injection is used in combination with a reduced-calorie diet and increased physical activity for long-term weight management in adults with obesity, defined by an initial body mass index (BMI) of 30 kg/m² or higher. Wegovy injection is also approved for those who are overweight, with a BMI of 27 kg/m² or higher, in the presence of at least a weight-related comorbid condition such as hypertension, type 2 diabetes, or dyslipidemia. The FDA has also approved its use in children aged 12 and older with an initial BMI at or above the 95th percentile for their age and sex.
- reduce the risk of major heart-related events such as death, heart attack or stroke in adults with known heart disease and with either obesity or overweight.
Ozempic for weight loss
The FDA has approved using semaglutide for weight loss, marketed under the brand name Wegovy. The recommended standard maintenance dosage for weight management is 2.4 mg, administered through weekly subcutaneous self-injections. With growing interest in semaglutide for weight control, healthcare professionals are responding to the demand by occasionally prescribing alternative brands of semaglutide, such as Ozempic and Rybelsus, for off-label use meaning using a drug approved by the FDA for a different purpose. Differences in insurance coverage between Wegovy versus Ozempic and Rybelsus may also fuel this off-label use.
The FDA issued a postmarket drug safety alert regarding the prevalence of compounded and counterfeit preparations of semaglutide. The increasing popularity of semaglutide for weight loss is a driving force behind compounded and counterfeit preparations. You “should only obtain drugs containing semaglutide with a prescription from a licensed health care provider, and obtain medicines only from state-licensed pharmacies or outsourcing facilities registered with FDA”.
Ozempic for type 2 diabetes
Ozempic injection is FDA-approved as an add-on to balanced diet and exercise to improve blood sugar control in adults with type 2 diabetes. Ozempic injection also provides an additional indication of reducing the risk of major adverse cardiovascular events, such as cardiovascular death, nonfatal heart attack, or nonfatal stroke, in patients with and without type 2 diabetes and established cardiovascular disease.
Ozempic dosage
Ozempic injection comes as a prefilled, multi-dose pen, meaning each pen delivers several doses and you will reuse the pen throughout the month, but use a new needle for each injection. Your box from the pharmacy comes with one multi-dose pen and NovoFine Plus needles. Each pen usually lasts one month 34, 3.
- 2 mg/3 mL (3 mL) (0.68mg/mL); available in single-patient-use pen that delivers 0.25 mg or 0.5 mg per injection.
- 4 mg/3 mL (1.34mg/mL); available in single-patient-use pen that delivers 1 mg per injection.
- 8 mg/3 mL (2.68 mg/mL); available in single-patient-use pen that delivers 2 mg per injection
Dosage: You Start at 0.25 mg Ozempic once weekly at the beginning of treatment at any time of day, with or without meals. After 4 weeks, increase Ozempic dosage to 0.5 mg once weekly. If additional glycemic control is needed, increase Ozempic dosage to 1mg once weekly after at least 4 weeks on the 0.5mg dose. If additional glycemic control is needed, increase Ozempic dosage to 2mg once weekly after at least 4 weeks on the 1mg dosage. The maximum recommended dosage is 2 mg weekly.
Note: To reduce the risk of sustained estimated Glomerular Filtration Rate (eGFR) decline, end-stage kidney disease and cardiovascular death, increase Ozempic dosage to 1 mg once weekly after at least 4 weeks on the 0.5 mg dosage.
- If you missed a dose, administer within 5 days of missed dose then the regular schedule should be resumed. If more than 5 days have passed, the missed dose can be skipped, and administration can be resumed at the next scheduled weekly dose.
- When changing the weekly subcutaneous semaglutide administration day, ensuring a minimum of 48 hours between 2 consecutive doses is essential.
- Inject Ozempic subcutaneously in the abdomen, thigh, or upper arm.
- Blood glucose should be closely monitored when converting to or from oral semaglutide.
Wegovy injection, prefilled, single-dose pen
Wegovy injection comes as a prefilled, single-dose pen. You will use a new pen for each dose. Your box from the pharmacy comes with 4 pens (a month’s supply). The needle is already attached to the pen, but you cannot see the needle 36, 37.
- 0.25mg/0.5mL
- 0.5mg/0.5mL
- 1mg/0.5mL
- 1.7mg/0.75mL
- 2.4mg/0.75mL
Dosage: You will start with a dose of 0.25 mg of Wegovy injected subcutaneously once weekly for 4 weeks. Wegovy dosage should be increased to 0.5 mg weekly for weeks 5 through 8. Wegovy dosage should be further increased to 1 mg weekly for weeks 9 through 12. Wegovy dosage should be further progressed to 1.7 mg weekly for weeks 13 through 16. Finally, Wegovy should be maintained at a dosage of 2.4 mg weekly thereafter.
Your doctor will slowly increase your dose to the recommended maintenance dose of 1.7 mg or 2.4 mg once weekly. The maintenance dosage of Wegovy is either 2.4 mg (recommended) or 1.7 mg once weekly. Inject Wegovy subcutaneously in your abdomen, thigh, or upper arm on the same day each week, at any time of day, with or without meals.
Administer Wegovy once weekly as an adjunct to diet and increased physical activity.
In patients with type 2 diabetes, monitor blood glucose prior to starting and during Wegovy treatment.
Special considerations for subcutaneous semaglutide (Wegovy)
- If you are experiencing difficulty with a dosage increase, your doctor should consider postponing the dose increase for an additional 4 weeks.
- If the 2.4 mg weekly dosage is not well tolerated, your doctor may consider reducing the dose to 1.7 mg weekly for a maximum of 4 weeks. After this period, the dosage should be increased to 2.4 mg weekly. If you continue to experience intolerance, discontinuing semaglutide (Wegovy) should be considered.
- If a dose is missed and the next scheduled dose is more than 2 days away (48 hours), it should be administered as soon as possible. However, if a dose is missed and the next scheduled dose is less than 2 days away (48 hours), it should not be administered. In such cases, you should resume dosing on the regularly scheduled day of the week.
- If 2 or more consecutive doses are missed, you should resume dosing as scheduled. If necessary, they may reinitiate and follow the dose escalation schedule, which may help reduce the occurrence of gastrointestinal symptoms associated with restarting treatment.
Special Precautions
Liver impairment
No dosage adjustment is needed for subcutaneous or oral semaglutide in patients with liver impairment 56, 57.
Kidney impairment
No dosage adjustment is necessary for subcutaneous or oral semaglutide in mild-to-severe impairment 54, 58. Caution should be exercised when initiating or escalating doses.
The manufacturer advises against adjusting the dosage of subcutaneous and oral Semaglutide for patients undergoing three or more weekly hemodialysis sessions. However, due to limited clinical evidence, caution is advised. Furthermore, the manufacturer recommends against adjusting the subcutaneous and oral semaglutide dosage for patients undergoing peritoneal dialysis. Again, caution is advised due to limited clinical evidence.
Pregnancy
Current clinical trial data and pharmacovigilance reports on semaglutide use in pregnant women are insufficient to ascertain its association with significant congenital defects, miscarriage, or adverse outcomes for both the mother and the fetus. However, findings from animal reproduction studies indicate potential risks to the fetus with semaglutide exposure during pregnancy. In addition, the weight loss effects of semaglutide are not deemed beneficial for pregnant individuals and may pose a risk of harm to the fetus. As a result, the manufacturer recommends against the use of semaglutide during pregnancy due to the potential fetal risks.
For the management of diabetes mellitus or weight loss, discontinuation of semaglutide is advised for a minimum of 2 months before a planned pregnancy. According to the 2021 guidelines from the American College of Obstetricians and Gynecologists (ACOG), weight loss medications are not recommended during pregnancy 59.
Breastfeeding
Insufficient data exist regarding semaglutide or its metabolites in human milk and the potential effects on breastfed infants and milk production. Semaglutide was identified in milk at levels 3 to 12 times lower than in maternal plasma in lactating rats. Although information on the impact of semaglutide in human milk is unavailable, it may be present in human milk if present in animal milk. The decision to use injectable semaglutide while breastfeeding should carefully consider the potential risk of infant exposure versus the benefits of breastfeeding.
Regarding the oral formulation containing sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC), it is unclear whether SNAC is excreted in breast milk. Due to this uncertainty, oral semaglutide is not recommended during breastfeeding, as the unknown risk of sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC) accumulation in infants is a concern.
Children
The safety and efficacy of subcutaneous semaglutide (Ozempic) and oral semaglutide (Rybelsus) have not been established in individuals aged 18 or younger. However, Wegovy, specifically indicated for weight loss, is approved for use in children aged 12 and older with a body mass index (BMI) corresponding to ≥95th percentile standardized for age and sex. This approval is based on a 68-week, double-blind, placebo-controlled clinical trial (STEP TEENS) involving 201 children aged 12 and older with a BMI corresponding to ≥95th percentile for age and sex 33.
The approved dosage for chronic weight management in the children and adolescent age groups of ≥12 and ≤18 is similar to the adult dosing outlined earlier, with the following exceptions:
- If patients do not tolerate the 2.4 mg weekly, the maintenance dosage may be reduced to 1.7 mg indefinitely.
- If the 1.7 mg weekly dose is not tolerated, semaglutide should be discontinued.
Cholelithiasis (gallstones), cholecystitis (gallbladder inflammation), hypotension (low blood pressure), rash, and urticaria were more prevalent in this younger age group than in adults treated with Wegovy 2. Meticulous attention to the dose escalation strategy may help mitigate the incidence of adverse events.
Older patients
No overall differences in safety and efficacy have been observed in patients aged 65 and older 2.
Monitoring
Monitoring for complications should be conducted collaboratively by the patient and their clinician, focusing on the following aspects:
- Vigilance for hypoglycemia is essential, especially when semaglutide is used with other glucose-lowering agents.
- Due to a heightened risk of gastrointestinal adverse effects such as nausea, vomiting, diarrhea, and constipation, close monitoring of patients for these adverse reactions is essential, with meticulous adherence to dose escalation.
- Dehydration resulting from gastrointestinal adverse effects poses a potential risk of renal failure. Therefore, monitoring renal function is paramount, especially in individuals experiencing gastrointestinal adverse effects.
- Doctors should assess the risk of gallbladder or bile duct disease and pancreatitis in patients using semaglutide who exhibit characteristic signs or symptoms.
- A potential risk of diabetic retinopathy complications underscores the importance of monitoring for any changes in vision and providing exceptional care to patients with baseline retinopathy.
- Although the risk of thyroid tumors in humans remains unclear, patients and doctors should remain vigilant for the development of any signs, such as a neck lump, hoarseness, dyspnea, or dysphagia while on semaglutide.
Ozempic Contraindications
Ozempic is contraindicated in patients with a personal or family history of medullary thyroid cancer also known as medullary thyroid carcinoma or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), and in patients with a hypersensitivity reaction to semaglutide or to any of the excipients in Ozempic. Serious hypersensitivity reactions including anaphylaxis and angioedema have been reported with Ozempic.
Is Ozempic safe?
In rodents study, Semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. The thyroid gland has 2 main types of cells: (1) Follicular cells use iodine from the blood to make thyroid hormones. These hormones help regulate your metabolism. (2) C cells also called parafollicular cells make calcitonin, a hormone that helps control how your body uses calcium.
It is unknown whether Ozempic causes thyroid C-cell tumors, including medullary thyroid cancer also known as medullary thyroid carcinoma, in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined 34, 3.
Ozempic is contraindicated in patients with a personal or family history of medullary thyroid cancer and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for medullary thyroid cancer with the use of Ozempic and inform them of symptoms of thyroid tumors (eg, a mass in the neck, dysphagia [difficulty swallowing], dyspnea [shortness of breath], persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of medullary thyroid cancer in patients treated with Ozempic.
Ozempic (Semaglutide) Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including semaglutide. Observe patients carefully for signs and symptoms of pancreatitis (persistent severe abdominal pain, sometimes radiating to the back with or without vomiting). If pancreatitis is suspected, discontinue Ozempic and initiate appropriate management.
- Diabetic Retinopathy Complications: In a 2-year trial involving patients with type 2 diabetes and high cardiovascular risk, more events of diabetic retinopathy complications occurred in patients treated with Ozempic (3.0%) compared with placebo (1.8%). The absolute risk increase for diabetic retinopathy complications was larger among patients with a history of diabetic retinopathy at baseline than among patients without a known history of diabetic retinopathy. Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. The effect of long-term glycemic control with semaglutide on diabetic retinopathy complications has not been studied. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy.
- SUSTAIN-6 has reported 76% higher risk for retinopathy related complications (blindness, vitreous haemorrhage, necessity of photocoagulation, and use of intravitreal agents) in semaglutide treatment group as compared to placebo 18. Rapid control of hyperglycaemia or decline in HbA1c was responsible for deteriorating retinopathy during initial few weeks of treatment, as proposed by post hoc analysis of SUSTAIN 1–6 and Japanese trials. Moreover, the retinopathy complications were more prevailing in patients receiving insulin therapy but it needs further evidences to confirm 60.
- Never Share an Ozempic Pen Between Patients: Ozempic pens must never be shared between patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens
- Hypoglycemia (low blood sugar level): Patients receiving Ozempic in combination with sulfonylurea (a class of medication used to treat type 2 diabetes by stimulating the pancreas to release more insulin, which helps lower blood sugar levels) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. Inform patients using these medications together increase the risk of hypoglycemia and educate them on the signs and symptoms of hypoglycemia. When semaglutide is administered alongside insulins or sulfonylureas, it is recommended to consider reducing the dosage of these medications to mitigate the risk of hypoglycemia. Medications that have the potential to augment the hypoglycemic effects of semaglutide include beta-blockers, monoamine oxidase inhibitors, androgens, quinolones, salicylates, selective serotonin reuptake inhibitors (SSRIs), and other antidiabetic medications.
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Ozempic that could lead to volume depletion, especially during dosage initiation and escalation.
- Severe Gastrointestinal Adverse Reactions: Use of Ozempic has been associated with gastrointestinal adverse reactions, sometimes severe. In Ozempic clinical trials, severe gastrointestinal adverse reactions were reported more frequently among patients receiving Ozempic (0.5 mg 0.4%, 1 mg 0.8%) than placebo (0%). Ozempic is not recommended in patients with severe gastroparesis (a condition where the stomach takes too long to empty its contents, leading to delayed gastric emptying).
- Hypersensitivity: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported in patients treated with Ozempic. If hypersensitivity reactions occur, discontinue use of Ozempic; treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of angioedema or anaphylaxis with another GLP-1 receptor agonist
- Acute Gallbladder Disease: Acute events of gallbladder disease such as cholelithiasis (gallstones) or cholecystitis (gallbladder inflammation) have been reported in GLP-1 receptor agonist trials and postmarketing. In placebo-controlled trials, cholelithiasis (gallstones) was reported in 1.5% and 0.4% of patients treated with Ozempic 0.5 mg and 1 mg, respectively, and not reported in placebo-treated patients. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Inhalation of foreign material, like food, liquid, or vomit, into the lungs (Pulmonary Aspiration) During General Anesthesia or Deep Sedation: Ozempic delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Tell all your health care providers that you are taking Ozempic before you are scheduled to have surgery or other procedures.
- Drug Interactions. Medications that may diminish the therapeutic effects of semaglutide include furosemide, thiazide diuretics, and ritodrine. Semaglutide may increase the serum concentrations of levothyroxine.
- Semaglutide causes a delay of gastric emptying, which may lead to delayed absorption of concurrently administered oral medications, so caution should be exercised. However, clinical pharmacology trials with subcutaneously administered semaglutide have demonstrated no significant impact on the absorption of orally administered medications. Nonetheless, cautious monitoring of the effects of oral medications is recommended when used concurrently with semaglutide, especially those with a narrow therapeutic window.
- Semaglutide should not be used with other GLP-1 receptor agonists or tirzepatide, as they are contraindicated.
Ozempic side effects
The most common side effects or adverse reactions reported in ≥5% of patients treated with Ozempic (Semaglutide) are nausea, vomiting, diarrhea, abdominal pain, and constipation 34, 3. Other reported adverse reactions associated with semaglutide include fatigue, headache, rash, alopecia, vitreous hemorrhage in patients with diabetic retinopathy, anxiety, dizziness, discomfort at the injection site, and erythema at the injection site. There are limited data with Ozempic (Semaglutide) use in pregnant women to inform a drug-associated risk for adverse developmental outcomes. Discontinue Ozempic (Semaglutide) in women at least 2 months before a planned pregnancy due to the long washout period for semaglutide 34, 3.
- Hypoglycemia (low blood sugar level): Ozempic (Semaglutide) or glucagon-like peptide-1 receptor agonist lowers blood glucose and may cause hypoglycemia. The risk of hypoglycemia significantly increases with escalating doses and when semaglutide is administered with other anti-hyperglycemic medications such as sulfonylureas, metformin, or insulin.
- Gastrointestinal side effects: The adverse effects most frequently reported and most associated with discontinuation of Semaglutide include nausea, vomiting, abdominal pain, constipation, and diarrhea 61. Nearly one-fifth of all patients in clinical trials with Ozempic and Rybelsus experienced nausea, which is the most prevalent adverse effect, whereas 44% of patients treated with Wegovy reported the same adverse effects 61. In addition, decreased appetite, altered taste (dysgeusia), and indigestion (dyspepsia) have been documented. Although the precise mechanism behind these effects is not entirely clarified, it may stem from delayed gastric emptying or the activation of brain centers implicated in appetite regulation, satiety, and nausea 62. Higher doses and dose escalations are associated with the risk of these adverse effects.
- Kidney disorders: Semaglutide can result in acute kidney injury. People who experienced nausea, vomiting, diarrhea, or dehydration during the treatment were at the highest risk of acute kidney injury, with volume depletion being the suspected link. Discontinuation or dose reduction of semaglutide is recommended rather than relying solely on symptomatic treatment of volume depletion.
- Gallbladder disorders: Semaglutide has been associated with gallbladder and biliary tract issues, including gallstones (cholelithiasis) and gallbladder inflammation (cholecystitis) 63. The exact mechanism behind this adverse effect is not entirely understood. Animal studies and test tube study data suggest that GLP-1 enhances cholangiocyte proliferation and functional activity, which could contribute to gallbladder diseases 64. Some authors have proposed that semaglutide can potentially suppress cholecystokinin secretion, reduce gallbladder emptying, and prolong gallbladder refilling, or a combination of these factors contributing to gallbladder disease 65.
- Anaphylaxis and angioedema: GLP-1 receptor agonists (GLP-1 RAs) can induce severe type 1 hypersensitivity reactions, such as anaphylaxis (life-threatening allergic reaction) and angioedema (a condition where small blood vessels leak fluid into the tissues under the skin, causing swelling in different parts of the body often around the face, lips, and throat, but it can also affect other areas like the limbs and abdomen) 66, 67. A possibility of cross-reactivity among different GLP-1 receptor agonists exists. Therefore, caution is advised when prescribing semaglutide to patients with a history of anaphylaxis or angioedema in response to other GLP-1 receptor agonists, pending further studies.
- Pancreatitis (inflammation of the pancreas): Although cases of acute pancreatitis have been associated with semaglutide use, findings from the SUSTAIN 6 trial indicate a similar incidence rate of pancreatitis with semaglutide compared to the placebo group 18. The causal relationship between semaglutide and acute pancreatitis has not been definitively established. GLP-1 receptor agonists directly stimulate GLP-1 receptors in pancreatic islet beta cells and exocrine duct cells. Researchers suggest that this stimulation may lead to the overgrowth of cells covering smaller ducts, causing hyperplasia, increased pancreatic weight, duct occlusion, back pressure, and subsequent acute and chronic pancreatitis 68.
- Diabetic retinopathy (a complication of diabetes that damages the blood vessels in the retina): Semaglutide use may potentially elevate the risk of diabetic retinopathy, particularly in patients with retinopathy at baseline. The exact relationship between semaglutide and the development or exacerbation of diabetic retinopathy remains incompletely understood. However, it may be associated with rapid improvements in glucose control, as identified in other studies 69.
- Risk of thyroid C-cell tumors: During the initial phases of drug development, animal studies involving semaglutide revealed the development of thyroid C-cell tumors. However, the potential association between semaglutide and thyroid cancers in humans remains unclear. Individuals with a personal or family history of medullary thyroid carcinoma (medullary thyroid cancer) or those diagnosed with multiple endocrine neoplasia type 2 (MEN 2) syndrome may face an elevated risk. The manufacturer acknowledges reported cases of medullary thyroid cancer associated with liraglutide, which is another GLP-1 receptor agonist.
Overdose
Overdose with oral or subcutaneous semaglutide can cause severe nausea, vomiting, and hypoglycemia.
Oral semaglutide is often co-administered with sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC) to increase gastric absorbability. Animal studies have indicated that higher sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC) exposure can result in lethargy, abnormal respiration, ataxia, and reduced activity.
Management of Overdose
In case of an overdose with oral or subcutaneous semaglutide, management involves implementing suitable supportive measures according to observed signs and symptoms. Consultation with poison control or a toxicologist is recommended. Due to the long half-life of semaglutide, an extended period of observation and treatment may be necessary.
- Dhillon S. Semaglutide: First Global Approval. Drugs. 2018 Feb;78(2):275-284. doi: 10.1007/s40265-018-0871-0[↩]
- Kommu S, Whitfield P. Semaglutide. [Updated 2024 Feb 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603723[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- https://www.novo-pi.com/ozempic.pdf[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/209637s020s021lbl.pdf[↩]
- https://www.ema.europa.eu/en/medicines/human/EPAR/ozempic[↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215256s007lbl.pdf[↩]
- https://www.ema.europa.eu/en/documents/overview/wegovy-epar-medicine-overview_en.pdf[↩]
- Lau J, Bloch P, Schäffer L, et al. Discovery of the once-weekly glucagon-like peptide-1 (GLP-1) analogue semaglutide. J Med Chem. 2015;58:7370–7380. doi: 10.1021/acs.jmedchem.5b00726[↩]
- MacIsaac RJ. Semaglutide: a key medication for managing cardiovascular-kidney-metabolic syndrome. Future Cardiol. 2025 Jul;21(9):663-683. doi: 10.1080/14796678.2025.2511412[↩][↩]
- Mahapatra MK, Karuppasamy M, Sahoo BM. Semaglutide, a glucagon like peptide-1 receptor agonist with cardiovascular benefits for management of type 2 diabetes. Rev Endocr Metab Disord. 2022 Jun;23(3):521-539. doi: 10.1007/s11154-021-09699-1[↩]
- Kalra S, Sahay R. A review on semaglutide: an oral glucagon-like peptide 1 receptor agonist in management of type 2 diabetes mellitus. Diabetes Ther. 2020;11(9):1965–1982. doi: 10.1007/s13300-020-00894-y[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Semaglutide. [Updated 2025 Jun 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548574[↩][↩]
- Sorli C, Harashima SI, Tsoukas GM, Unger J, Karsbøl JD, Hansen T, Bain SC. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol. 2017 Apr;5(4):251-260. doi: 10.1016/S2213-8587(17)30013-X[↩]
- Ahrén B, Masmiquel L, Kumar H, Sargin M, Karsbøl JD, Jacobsen SH, Chow F. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017 May;5(5):341-354. doi: 10.1016/S2213-8587(17)30092-X[↩]
- Ahmann AJ, Capehorn M, Charpentier G, Dotta F, Henkel E, Lingvay I, Holst AG, Annett MP, Aroda VR. Efficacy and Safety of Once-Weekly Semaglutide Versus Exenatide ER in Subjects With Type 2 Diabetes (SUSTAIN 3): A 56-Week, Open-Label, Randomized Clinical Trial. Diabetes Care. 2018 Feb;41(2):258-266. doi: 10.2337/dc17-0417[↩]
- Aroda VR, Bain SC, Cariou B, Piletič M, Rose L, Axelsen M, Rowe E, DeVries JH. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017 May;5(5):355-366. doi: 10.1016/S2213-8587(17)30085-2[↩]
- Rodbard HW, Lingvay I, Reed J, de la Rosa R, Rose L, Sugimoto D, Araki E, Chu PL, Wijayasinghe N, Norwood P. Semaglutide Added to Basal Insulin in Type 2 Diabetes (SUSTAIN 5): A Randomized, Controlled Trial. J Clin Endocrinol Metab. 2018 Jun 1;103(6):2291-2301. doi: 10.1210/jc.2018-00070[↩]
- Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, Lingvay I, Rosenstock J, Seufert J, Warren ML, Woo V, Hansen O, Holst AG, Pettersson J, Vilsbøll T; SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2016 Nov 10;375(19):1834-1844. doi: 10.1056/NEJMoa1607141[↩][↩][↩]
- Aroda VR, Rosenstock J, Terauchi Y, Altuntas Y, Lalic NM, Morales Villegas EC, Jeppesen OK, Christiansen E, Hertz CL, Haluzík M; PIONEER 1 Investigators. PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes. Diabetes Care. 2019 Sep;42(9):1724-1732. doi: 10.2337/dc19-0749[↩]
- Rodbard HW, Rosenstock J, Canani LH, Deerochanawong C, Gumprecht J, Lindberg SØ, Lingvay I, Søndergaard AL, Treppendahl MB, Montanya E; PIONEER 2 Investigators. Oral Semaglutide Versus Empagliflozin in Patients With Type 2 Diabetes Uncontrolled on Metformin: The PIONEER 2 Trial. Diabetes Care. 2019 Dec;42(12):2272-2281. doi: 10.2337/dc19-0883[↩]
- Rosenstock J, Allison D, Birkenfeld AL, Blicher TM, Deenadayalan S, Jacobsen JB, Serusclat P, Violante R, Watada H, Davies M; PIONEER 3 Investigators. Effect of Additional Oral Semaglutide vs Sitagliptin on Glycated Hemoglobin in Adults With Type 2 Diabetes Uncontrolled With Metformin Alone or With Sulfonylurea: The PIONEER 3 Randomized Clinical Trial. JAMA. 2019 Apr 16;321(15):1466-1480. doi: 10.1001/jama.2019.2942[↩]
- Pratley R, Amod A, Hoff ST, Kadowaki T, Lingvay I, Nauck M, Pedersen KB, Saugstrup T, Meier JJ; PIONEER 4 investigators. Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4): a randomised, double-blind, phase 3a trial. Lancet. 2019 Jul 6;394(10192):39-50. doi: 10.1016/S0140-6736(19)31271-1. Epub 2019 Jun 8. Erratum in: Lancet. 2019 Jul 6;394(10192):e1. doi: 10.1016/S0140-6736(19)31519-3[↩]
- Mosenzon O, Blicher TM, Rosenlund S, Eriksson JW, Heller S, Hels OH, Pratley R, Sathyapalan T, Desouza C; PIONEER 5 Investigators. Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5): a placebo-controlled, randomised, phase 3a trial. Lancet Diabetes Endocrinol. 2019 Jul;7(7):515-527. doi: 10.1016/S2213-8587(19)30192-5. Epub 2019 Jun 9. Erratum in: Lancet Diabetes Endocrinol. 2019 Sep;7(9):e21. doi: 10.1016/S2213-8587(19)30246-3[↩]
- Pieber TR, Bode B, Mertens A, Cho YM, Christiansen E, Hertz CL, Wallenstein SOR, Buse JB; PIONEER 7 investigators. Efficacy and safety of oral semaglutide with flexible dose adjustment versus sitagliptin in type 2 diabetes (PIONEER 7): a multicentre, open-label, randomised, phase 3a trial. Lancet Diabetes Endocrinol. 2019 Jul;7(7):528-539. doi: 10.1016/S2213-8587(19)30194-9. Epub 2019 Jun 9. Erratum in: Lancet Diabetes Endocrinol. 2019 Sep;7(9):e21. doi: 10.1016/S2213-8587(19)30247-5[↩]
- Zinman B, Aroda VR, Buse JB, Cariou B, Harris SB, Hoff ST, Pedersen KB, Tarp-Johansen MJ, Araki E; PIONEER 8 Investigators. Efficacy, Safety, and Tolerability of Oral Semaglutide Versus Placebo Added to Insulin With or Without Metformin in Patients With Type 2 Diabetes: The PIONEER 8 Trial. Diabetes Care. 2019 Dec;42(12):2262-2271. doi: 10.2337/dc19-0898[↩]
- Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR, Jeppesen OK, Lingvay I, Mosenzon O, Pedersen SD, Tack CJ, Thomsen M, Vilsbøll T, Warren ML, Bain SC; PIONEER 6 Investigators. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2019 Aug 29;381(9):841-851. doi: 10.1056/NEJMoa1901118[↩]
- Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, McGowan BM, Rosenstock J, Tran MTD, Wadden TA, Wharton S, Yokote K, Zeuthen N, Kushner RF; STEP 1 Study Group. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021 Mar 18;384(11):989-1002. doi: 10.1056/NEJMoa2032183[↩]
- Wadden TA, Bailey TS, Billings LK, Davies M, Frias JP, Koroleva A, Lingvay I, O’Neil PM, Rubino DM, Skovgaard D, Wallenstein SOR, Garvey WT; STEP 3 Investigators. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 2021 Apr 13;325(14):1403-1413. doi: 10.1001/jama.2021.1831[↩]
- Rubino D, Abrahamsson N, Davies M, Hesse D, Greenway FL, Jensen C, Lingvay I, Mosenzon O, Rosenstock J, Rubio MA, Rudofsky G, Tadayon S, Wadden TA, Dicker D; STEP 4 Investigators. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021 Apr 13;325(14):1414-1425. doi: 10.1001/jama.2021.3224[↩]
- Garvey WT, Batterham RL, Bhatta M, Buscemi S, Christensen LN, Frias JP, Jódar E, Kandler K, Rigas G, Wadden TA, Wharton S; STEP 5 Study Group. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022 Oct;28(10):2083-2091. doi: 10.1038/s41591-022-02026-4[↩]
- Davies M, Færch L, Jeppesen OK, Pakseresht A, Pedersen SD, Perreault L, Rosenstock J, Shimomura I, Viljoen A, Wadden TA, Lingvay I; STEP 2 Study Group. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021 Mar 13;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0[↩]
- Rubino DM, Greenway FL, Khalid U, O’Neil PM, Rosenstock J, Sørrig R, Wadden TA, Wizert A, Garvey WT; STEP 8 Investigators. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022 Jan 11;327(2):138-150. doi: 10.1001/jama.2021.23619[↩][↩]
- Weghuber D, Barrett T, Barrientos-Pérez M, Gies I, Hesse D, Jeppesen OK, Kelly AS, Mastrandrea LD, Sørrig R, Arslanian S; STEP TEENS Investigators. Once-Weekly Semaglutide in Adolescents with Obesity. N Engl J Med. 2022 Dec 15;387(24):2245-2257. doi: 10.1056/NEJMoa2208601[↩][↩]
- https://www.novomedlink.com/diabetes/products/treatments/ozempic.html[↩][↩][↩][↩][↩][↩][↩][↩]
- Wilding JPH, Batterham RL, Davies M, Van Gaal LF, Kandler K, Konakli K, Lingvay I, McGowan BM, Oral TK, Rosenstock J, Wadden TA, Wharton S, Yokote K, Kushner RF; STEP 1 Study Group. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022 Aug;24(8):1553-1564. doi: 10.1111/dom.14725[↩]
- https://www.novomedlink.com/obesity/products/treatments/wegovy.html[↩][↩][↩]
- https://www.novo-pi.com/wegovy.pdf[↩][↩][↩]
- Yang XD, Yang YY. Clinical Pharmacokinetics of Semaglutide: A Systematic Review. Drug Des Devel Ther. 2024 Jun 25;18:2555-2570. doi: 10.2147/DDDT.S470826[↩]
- Røder ME. Clinical potential of treatment with semaglutide in type 2 diabetes patients. Drugs Context. 2019 Dec 2;8:212585. doi: 10.7573/dic.212585[↩]
- Meier JJ. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat Rev Endocrinol. 2012 Dec;8(12):728-42. doi: 10.1038/nrendo.2012.140[↩][↩]
- Al-Massadi O, Fernø J, Diéguez C, Nogueiras R, Quiñones M. Glucagon Control on Food Intake and Energy Balance. Int J Mol Sci. 2019 Aug 11;20(16):3905. doi: 10.3390/ijms20163905[↩]
- Drucker DJ. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 2018 Apr 3;27(4):740-756. doi: 10.1016/j.cmet.2018.03.001[↩]
- Knudsen LB, Lau J. The Discovery and Development of Liraglutide and Semaglutide. Front Endocrinol (Lausanne). 2019 Apr 12;10:155. doi: 10.3389/fendo.2019.00155[↩]
- Guja C, Dănciulescu Miulescu R. Semaglutide-the “new kid on the block” in the field of glucagon-like peptide-1 receptor agonists? Ann Transl Med. 2017 Dec;5(23):475. doi: 10.21037/atm.2017.10.09[↩][↩]
- Overgaard RV, Delff PH, Petri KCC, Anderson TW, Flint A, Ingwersen SH. Population Pharmacokinetics of Semaglutide for Type 2 Diabetes. Diabetes Ther. 2019 Apr;10(2):649-662. doi: 10.1007/s13300-019-0581-y[↩]
- Buckley ST, Bækdal TA, Vegge A, et al. Transcellular stomach absorption of a derivatized glucagon-like peptide-1 receptor agonist. Sci Transl Med. 2018 Nov 14;10(467):eaar7047. doi: 10.1126/scitranslmed.aar7047[↩][↩][↩]
- Aroda VR, Blonde L, Pratley RE. A new era for oral peptides: SNAC and the development of oral semaglutide for the treatment of type 2 diabetes. Rev Endocr Metab Disord. 2022 Oct;23(5):979-994. doi: 10.1007/s11154-022-09735-8[↩]
- Kalra S, Das S, Zargar AH. A Review of Oral Semaglutide Available Evidence: A New Era of Management of Diabetes with Peptide in a Pill Form. Indian J Endocrinol Metab. 2022 Mar-Apr;26(2):98-105. doi: 10.4103/ijem.ijem_522_21[↩]
- Aguirre TA, Teijeiro-Osorio D, Rosa M, Coulter IS, Alonso MJ, Brayden DJ. Current status of selected oral peptide technologies in advanced preclinical development and in clinical trials. Adv Drug Deliv Rev. 2016 Nov 15;106(Pt B):223-241. doi: 10.1016/j.addr.2016.02.004[↩]
- Lewis AL, McEntee N, Holland J, Patel A. Development and approval of rybelsus (oral semaglutide): ushering in a new era in peptide delivery. Drug Deliv Transl Res. 2022 Jan;12(1):1-6. doi: 10.1007/s13346-021-01000-w[↩]
- Overgaard RV, Navarria A, Ingwersen SH, Bækdal TA, Kildemoes RJ. Clinical Pharmacokinetics of Oral Semaglutide: Analyses of Data from Clinical Pharmacology Trials. Clin Pharmacokinet. 2021 Oct;60(10):1335-1348. doi: 10.1007/s40262-021-01025-x[↩]
- Chan M, Dimitriou A, Lam S. Semaglutide: A Novel Oral Glucagon-Like Peptide Receptor Agonist for the Treatment of Type 2 Diabetes Mellitus. Cardiol Rev. 2021 Mar-Apr 01;29(2):100-108. doi: 10.1097/CRD.0000000000000351[↩][↩][↩][↩]
- Carlsson Petri KC, Ingwersen SH, Flint A, Zacho J, Overgaard RV. Semaglutide s.c. Once-Weekly in Type 2 Diabetes: A Population Pharmacokinetic Analysis. Diabetes Ther. 2018 Aug;9(4):1533-1547. doi: 10.1007/s13300-018-0458-5[↩][↩]
- Granhall C, Søndergaard FL, Thomsen M, Anderson TW. Pharmacokinetics, Safety and Tolerability of Oral Semaglutide in Subjects with Renal Impairment. Clin Pharmacokinet. 2018 Dec;57(12):1571-1580. doi: 10.1007/s40262-018-0649-2[↩][↩]
- Jensen L, Helleberg H, Roffel A, van Lier JJ, Bjørnsdottir I, Pedersen PJ, Rowe E, Derving Karsbøl J, Pedersen ML. Absorption, metabolism and excretion of the GLP-1 analogue semaglutide in humans and nonclinical species. Eur J Pharm Sci. 2017 Jun 15;104:31-41. doi: 10.1016/j.ejps.2017.03.020[↩]
- Jensen L, Kupcova V, Arold G, Pettersson J, Hjerpsted JB. Pharmacokinetics and tolerability of semaglutide in people with hepatic impairment. Diabetes Obes Metab. 2018 Apr;20(4):998-1005. doi: 10.1111/dom.13186[↩]
- Baekdal TA, Thomsen M, Kupčová V, Hansen CW, Anderson TW. Pharmacokinetics, Safety, and Tolerability of Oral Semaglutide in Subjects With Hepatic Impairment. J Clin Pharmacol. 2018 Oct;58(10):1314-1323. doi: 10.1002/jcph.1131[↩]
- Marbury TC, Flint A, Jacobsen JB, Derving Karsbøl J, Lasseter K. Pharmacokinetics and Tolerability of a Single Dose of Semaglutide, a Human Glucagon-Like Peptide-1 Analog, in Subjects With and Without Renal Impairment. Clin Pharmacokinet. 2017 Nov;56(11):1381-1390. doi: 10.1007/s40262-017-0528-2[↩]
- Obesity in Pregnancy: ACOG Practice Bulletin, Number 230. Obstet Gynecol. 2021 Jun 1;137(6):e128-e144. doi: 10.1097/AOG.0000000000004395[↩]
- Vilsbøll T, Bain SC, Leiter LA, Lingvay I, Matthews D, Simó R, Helmark IC, Wijayasinghe N, Larsen M. Semaglutide, reduction in glycated haemoglobin and the risk of diabetic retinopathy. Diabetes Obes Metab. 2018 Apr;20(4):889-897. doi: 10.1111/dom.13172[↩]
- Htike ZZ, Zaccardi F, Papamargaritis D, Webb DR, Khunti K, Davies MJ. Efficacy and safety of glucagon-like peptide-1 receptor agonists in type 2 diabetes: A systematic review and mixed-treatment comparison analysis. Diabetes Obes Metab. 2017 Apr;19(4):524-536. doi: 10.1111/dom.12849[↩][↩]
- Filippatos TD, Panagiotopoulou TV, Elisaf MS. Adverse Effects of GLP-1 Receptor Agonists. Rev Diabet Stud. 2014 Fall-Winter;11(3-4):202-30. doi: 10.1900/RDS.2014.11.202[↩]
- He L, Wang J, Ping F, Yang N, Huang J, Li Y, Xu L, Li W, Zhang H. Association of Glucagon-Like Peptide-1 Receptor Agonist Use With Risk of Gallbladder and Biliary Diseases: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. 2022 May 1;182(5):513-519. doi: 10.1001/jamainternmed.2022.0338[↩]
- Marzioni M, Alpini G, Saccomanno S, Candelaresi C, Venter J, Rychlicki C, Fava G, Francis H, Trozzi L, Glaser S, Benedetti A. Glucagon-like peptide-1 and its receptor agonist exendin-4 modulate cholangiocyte adaptive response to cholestasis. Gastroenterology. 2007 Jul;133(1):244-55. doi: 10.1053/j.gastro.2007.04.007[↩]
- Gether IM, Nexøe-Larsen C, Knop FK. New Avenues in the Regulation of Gallbladder Motility-Implications for the Use of Glucagon-Like Peptide-Derived Drugs. J Clin Endocrinol Metab. 2019 Jul 1;104(7):2463-2472. doi: 10.1210/jc.2018-01008[↩]
- Pérez E, Martínez-Tadeo J, Callero A, Hernández G, Rodríguez-Plata E, García-Robaina JC. A case report of allergy to exenatide. J Allergy Clin Immunol Pract. 2014 Nov-Dec;2(6):822-3. doi: 10.1016/j.jaip.2014.05.011[↩]
- Pradhan R, Montastruc F, Rousseau V, Patorno E, Azoulay L. Exendin-based glucagon-like peptide-1 receptor agonists and anaphylactic reactions: a pharmacovigilance analysis. Lancet Diabetes Endocrinol. 2020 Jan;8(1):13-14. doi: 10.1016/S2213-8587(19)30382-1[↩]
- Knapen LM, de Jong RG, Driessen JH, Keulemans YC, van Erp NP, De Bruin ML, Leufkens HG, Croes S, de Vries F. Use of incretin agents and risk of acute and chronic pancreatitis: A population-based cohort study. Diabetes Obes Metab. 2017 Mar;19(3):401-411. doi: 10.1111/dom.12833[↩]
- Ntentakis DP, Correa VSMC, Ntentaki AM, Delavogia E, Narimatsu T, Efstathiou NE, Vavvas DG. Effects of newer-generation anti-diabetics on diabetic retinopathy: a critical review. Graefes Arch Clin Exp Ophthalmol. 2024 Mar;262(3):717-752. doi: 10.1007/s00417-023-06236-5[↩]


{kind=link}