
Contents
- What is indigestion or dyspepsia?
- What is functional dyspepsia
- Functional dyspepsia cause
- Functional dyspepsia pathophysiology
- Functional dyspepsia symptoms
- Functional dyspepsia types
- Functional dyspepsia complications
- Functional dyspepsia diagnosis
- Functional dyspepsia differential diagnosis
- Functional dyspepsia treatment
- Functional dyspepsia prognosis
What is indigestion or dyspepsia?
Indigestion also known as dyspepsia or an upset stomach is a general term used to describe one or more gastrointestinal symptoms that occur together such as a feeling of fullness during a meal, uncomfortable fullness after a meal, and a feeling of discomfort or a burning feeling in your upper middle part of abdomen (mid upper abdomen). You may also feel nauseated, or even throw up. Indigestion is not a disease, but rather some gastrointestinal symptoms you experience, including abdominal pain and a feeling of fullness soon after you start eating. Indigestion is pain or discomfort after eating, while your stomach is digesting. If you get a stomachache or upset tummy after eating, something in your digestive process isn’t going quite right. It’s not always a problem with your body, though. Sometimes it just means you ate the wrong thing or ate too fast. However, indigestion may be a sign of certain digestive tract diseases or conditions. Indigestion is not always related to eating.
Sometimes the term dyspepsia or indigestion is used to describe the symptom of heartburn, but these are two different conditions. Dyspepsia or indigestion is not the same as heartburn. Dyspepsia or indigestion is not related to stomach acid. Heartburn is a painful, burning feeling in your chest that radiates toward your neck or back. Heartburn is caused by stomach acid rising out of your stomach and back into your food pipe (esophagus) and may be a symptom of gastroesophageal reflux disease (GERD). You can have symptoms of both indigestion and heartburn at the same time.
Symptoms of indigestion vary between individuals. Symptoms may include:
- Early fullness during a meal. You haven’t eaten much of your meal, but you already feel full and may not be able to finish eating.
- Uncomfortable fullness after a meal. You feel overly full after a meal—it may feel like the food is staying in your stomach too long. Fullness lasts longer than it should.
- Discomfort in the upper abdomen. You feel a mild to severe pain in the area between the bottom of your breastbone and your navel also known as the epigastric area (the area between the lower end of your chest bone and the navel).
- Burning in the upper abdomen. You feel an uncomfortable heat or burning sensation between the bottom of your breastbone and your navel (the epigastric area). You may experience epigastric pain ranging from mild to severe.
- Bloating in the upper abdomen. You feel an uncomfortable sensation of tightness.
- Nausea. You feel as though you want to vomit.
Other, less frequent symptoms that may occur with indigestion are nausea and bloating (an unpleasant tightness in your stomach). Nausea and bloating could be due to causes other than indigestion.
Experts generally agree that the symptoms of indigestion include:
- Epigastric pain. Your epigastrium is your central, upper abdominal region. This is where your stomach is.
- Burning sensation. Burning may come from stomach acids and enzymes in your GI tract, or from inflammation.
- Early or late-lasting satiety. Feeling full soon after eating, or long after, suggests your stomach is overwhelmed.
But people who experience indigestion often report other symptoms along with it, such as:
- Bloating.
- Gas.
- Nausea.
- Burping.
- Regurgitation (when swallowed food comes back up).
- Acid reflux.
- Heartburn.
Indigestion may be 1:
- Occasional—happening once in a while
- Chronic—happening regularly for a few weeks or months
- Functional—having chronic symptoms without a specific cause
The symptoms of indigestion may look like other health problems. Always see your doctor to be sure.
Because indigestion can be a sign of a more serious condition, you should see a doctor right away if you experience:
- frequent vomiting
- blood in vomit
- weight loss or loss of appetite
- black tarry stools
- difficult or painful swallowing
- abdominal pain in a nonepigastric area (the area between the lower end of your chest bone and the navel)
- indigestion accompanied by shortness of breath, sweating, or pain that radiates to the jaw, neck, or arm
- symptoms that persist for more than 2 weeks.
Sometimes digestive tract diseases such as peptic ulcer disease, gastritis, and stomach cancer cause chronic indigestion. However, most often doctors do not know what causes chronic indigestion. Chronic indigestion without a health problem or digestive tract disease that could explain symptoms is called functional dyspepsia. The vast majority of people who see doctors for dyspeptic symptoms are ultimately diagnosed as having functional dyspepsia (having chronic indigestion symptoms without a specific cause) 2.
Indigestion is common in adults and can occur once in a while or as often as every day. People of any age can get indigestion. Both men and women get it. About 1 of every 4 persons gets indigestion at some time 3.
Indigestion is not a disease, but rather some gastrointestinal symptoms you experience, including abdominal pain and a feeling of fullness soon after you start eating. Although indigestion is common, each person may experience indigestion in a slightly different way. Symptoms of indigestion may be felt occasionally or as often as daily.
Indigestion can be a symptom of another digestive disease, lifestyle issues, or medicines.
- Indigestion can be caused by health problems or diseases include:
- Sores or ulcers in your stomach or small intestine (peptic ulcer disease)
- Redness and swelling or inflammation in your stomach (gastritis)
- Acid flowing back from your stomach into your esophagus (gastroesophageal reflux disease [GERD])
- Bacterial infection in your stomach (Helicobacter pylori [H. pylori] infection)
- Inflammation of your gallbladder (cholecystitis)
- Lumps of solid material (gallstones) in your gallbladder (cholelithiasis)
- Swelling of your pancreas (pancreatitis)
- Food moving too slowly out of your stomach (gastroparesis) (common in people with diabetes)
- Indigestion can be caused by lifestyle issues include:
- Smoking
- Having too much caffeine
- Drinking too much alcohol
- Eating too fast
- Eating too much
- Eating spicy, fatty, or greasy foods
- Eating high-fiber foods
- Feeling very stressed
- Indigestion can be caused by medicines include:
- Antibiotics
- Aspirin and over-the-counter pain and fever medicines (nonsteroidal anti-inflammatory drugs [NSAIDs])
Indigestion that isn’t caused by an underlying disease may be eased with lifestyle changes and medication. Indigestion that is mild and occasional can usually be managed with lifestyle changes and over-the-counter medications. In more serious cases, other treatment may be needed.
To diagnose indigestion, your doctor asks about your current symptoms and medical history and performs a physical examination. Your doctor may order x rays of the stomach and small intestine. Your doctor may perform blood, breath, or stool tests if the Helicobacter pylori (H. pylori) bacteria that causes peptic ulcer disease is suspected as the cause of indigestion.
Your doctor may also perform an upper endoscopy. After giving a sedative to help the person become drowsy, your doctor passes an endoscope—a long, thin tube that has a light and small camera on the end—through the mouth and gently guides it down the esophagus into the stomach. Your doctor can look at your esophagus and stomach with the endoscope to check for any abnormalities. Your doctor may perform biopsies—removing small pieces of tissue for examination with a microscope—to look for possible damage from gastroesophageal reflux disease (GERD) or a Helicobacter pylori (H. pylori) infection.
Figure 1. Digestive system
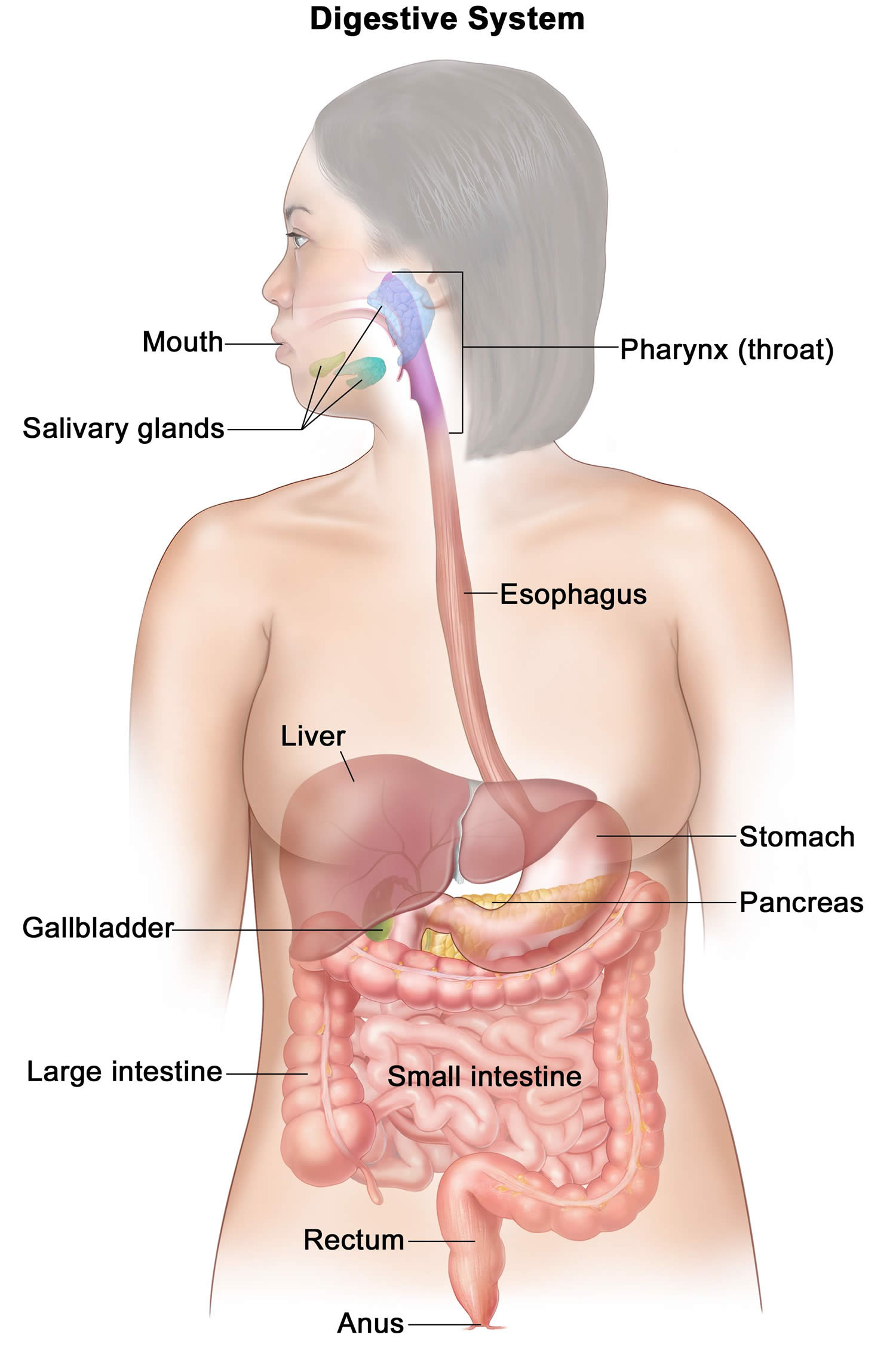
Footnotes: Your digestive system processes nutrients in foods that you have eaten and helps pass waste material out of your body. Food moves from your throat to your stomach through a tube called the esophagus. After food enters your stomach, it is broken down by stomach acid and muscles that mix the food and liquid with digestive juices. After leaving your stomach, partly digested food passes into your small intestine and then into your large intestine. The end of the large intestine, called the rectum, stores the waste from the digested food until it is pushed out of the anus during a bowel movement.
Mild indigestion is usually nothing to worry about. See your doctor if discomfort persists for more than two weeks.
Contact your doctor right away if pain is severe or accompanied by:
- If you are 55 or over
- Unintentional weight loss or loss of appetite
- Difficulty swallowing (dysphagia)
- Repeated vomiting or vomiting with blood
- Black, tarry stools
- Trouble swallowing that gets progressively worse
- Fatigue or weakness, which may indicate anemia
Seek immediate medical attention if you have:
- Shortness of breath, sweating or chest pain radiating to the jaw, neck or arm
- Chest pain on exertion or with stress
These symptoms can be a sign of something more serious.
IMPORTANT: Sometimes a heart attack can masquerade as indigestion. Seek medical attention right away if your indigestion is accompanied by sweating, shortness of breath or a tight, clenching feeling in your upper abdominal area.
Who is more likely to get indigestion?
You are more likely to get indigestion if you:
- Drink
- too many alcoholic beverages
- too much coffee or too many drinks containing caffeine
- Eat
- too fast or too much during a meal
- spicy, fatty, or greasy foods
- foods that contain a lot of acid, such as tomatoes, tomato products, and oranges
- Feel stressed
- Have certain health problems or digestive tract diseases
- Smoke
- Take certain medicines e.g., antibiotics, bisphosphonates, acarbose, corticosteroids, iron, metformin, nonsteroidal anti-inflammatory drugs (NSAIDs), opiates, orlistat, potassium chloride, theophylline.
What foods and drinks should I avoid if I have indigestion?
You can help prevent indigestion by changing what you eat and drink. You may need to avoid foods and drinks that cause indigestion.
If you have indigestion, avoid foods and drinks that may make your symptoms worse, such as
- alcoholic beverages
- carbonated, or fizzy, drinks
- foods and drinks that contain caffeine
- foods that contain a lot of acid, such as tomatoes, tomato products, and oranges
- spicy, fatty, or greasy foods
What can I eat if I have indigestion?
You should eat a healthy, well-balanced diet. A healthy diet can improve your overall health, help manage certain diseases and conditions, and reduce the chance of disease.
Indigestion causes
Indigestion has many possible causes. Often, indigestion is related to your lifestyle and may be triggered by food, drink or medication.
Causes of occasional indigestion can be simple. For example, many people get indigestion after an especially large or rich meal. That’s easy to explain: your digestive system is working harder than usual to accommodate a heavy load. Your stomach is stretching, your gallbladder and pancreas are contracting, and they’re all producing strong digestive juices, which may be irritating your tissues.
But indigestion that lasts longer than one meal, or that comes and goes chronically, is often less simple. There may be a variety of factors involved. Sometimes there’s an organic cause, like a disease.
In general, causes of indigestion fall into three categories:
- Your eating habits:
- Eating
- too fast or too much during a meal
- spicy, fatty, or greasy foods
- foods that contain a lot of acid, such as tomatoes, tomato products, and oranges
- Drinking
- too many alcoholic beverages
- too much coffee or too many drinks containing caffeine
- too many carbonated, or fizzy, drinks
- Eating
- How your digestive system is functioning.
- Your perception of pain and discomfort.
Often, indigestion is caused by a stomach ulcer or acid reflux disease. If you have acid reflux disease, stomach acid backs up into your esophagus (the tube leading from your mouth to your stomach). This causes pain in your chest. Your doctor may do some tests to find out if you have an ulcer or acid reflux disease. Some medicines, like anti-inflammatory medicines, can cause dyspepsia. Sometimes no cause of dyspepsia can be found. This is called functional dyspepsia. Functional gastrointestinal disorders occur when the nerves in your gastrointestinal tract are hypersensitized, which lowers your threshold for discomfort.
Table 1. Health problems and digestive tract diseases and conditions that can cause indigestion
| Health problems and digestive tract diseases and conditions that can cause indigestion | Approximate prevalence* |
|---|---|
| Functional (nonulcer) dyspepsia | Up to 70 percent |
| Peptic ulcer disease | 15 to 25 percent |
| Reflux esophagitis | 5 to 15 percent |
| Gastric or esophageal cancer | < 2 percent |
| Abdominal cancer, especially pancreatic cancer | Rare |
| Biliary tract disease | Rare |
| Carbohydrate malabsorption (lactose, sorbitol, fructose, mannitol) | Rare |
| Gastroparesis | Rare |
| Hepatoma | Rare |
| Infiltrative diseases of the stomach (Crohn disease, sarcoidosis) | Rare |
| Intestinal parasites (Giardia species, Strongyloides species) | Rare |
| Ischemic bowel disease | Rare |
| Medication effects | Rare |
| Metabolic disturbances (hypercalcemia, hyperkalemia) | Rare |
| Pancreatitis | Rare |
| Systemic disorders (diabetes mellitus, thyroid and parathyroid disorders, connective tissue disease) | Rare |
Footnote: * Based on the occurrence of the disorders in patients with indigestion who are evaluated with endoscopy.
[Source 4 ]Table 2. Medicines that can cause indigestion
| Acarbose (Precose) |
| Alcohol |
| Antibiotics, oral (e.g., erythromycin) |
| Bisphosphonates |
| Corticosteroids (e.g., prednisone) |
| Herbs (e.g., garlic, ginkgo, saw palmetto, feverfew, chaste tree berry, white willow) |
| Iron |
| Metformin (Glucophage) |
| Miglitol (Glyset) |
| Nonsteroidal anti-inflammatory drugs, including cyclooxygenase-2 inhibitors |
| Opiates |
| Orlistat (Xenical) |
| Potassium chloride |
| Theophylline |
Common causes of indigestion include:
- Overeating or eating too quickly
- Fatty, greasy or spicy foods
- Too much caffeine, alcohol, chocolate or carbonated beverages
- Smoking
- Anxiety or depression
- Certain antibiotics, pain relievers and iron supplements
Sometimes indigestion is caused by other digestive conditions, including:
- Acid reflux (GER and GERD)
- Gastritis
- Peptic ulcer disease
- Celiac disease
- Gastroparesis
- Gallstones (cholelithiasis) or gallbladder inflammation (cholecystitis)
- Constipation
- Helicobacter pylori (H. pylori) infection
- Irritable bowel syndrome (IBS)
- Lactose intolerance
- Pancreas inflammation (pancreatitis)
- Stomach cancer
- Intestinal blockage
- Reduced blood flow in the intestine (intestinal ischemia)
Indigestion with no obvious cause is known as functional dyspepsia or nonulcer dyspepsia.
Common triggers for indigestion
Some people experience indigestion regardless of what they eat. Others find they only get it after eating certain foods or meals. Common triggers for indigestion include:
- large meals
- fatty or spicy foods
- coffee and cola drinks
- citrus foods
- alcohol
- chocolate
- cigarettes
- peppermints.
Other things that can increase your risk of indigestion are:
- being overweight or obese
- being pregnant
- taking certain medications (check with your doctor).
- eating a large meal
- exercising too soon after eating.
Indigestion symptoms
Symptoms of indigestion vary between individuals. Symptoms may include:
- Early fullness during a meal. You haven’t eaten much of your meal, but you already feel full and may not be able to finish eating.
- Uncomfortable fullness after a meal. You feel overly full after a meal—it may feel like the food is staying in your stomach too long. Fullness lasts longer than it should.
- Discomfort in the upper abdomen. You feel a mild to severe pain in the area between the bottom of your breastbone and your navel also known as the epigastric area (the area between the lower end of your chest bone and the navel).
- Burning in the upper abdomen. You feel an uncomfortable heat or burning sensation between the bottom of your breastbone and your navel (the epigastric area). You may experience epigastric pain ranging from mild to severe.
- Bloating in the upper abdomen. You feel an uncomfortable sensation of tightness.
- Nausea. You feel as though you want to vomit.
Other, less frequent symptoms that may occur with indigestion are nausea and bloating (an unpleasant tightness in your stomach). Nausea and bloating could be due to causes other than indigestion.
Indigestion may involve several different symptoms, but it always involves some level of abdominal pain or discomfort. Your abdomen is where most of the organs in your digestive system live, so if your digestive system are having difficulties while doing their jobs, that’s where you’ll feel it. Indigestion symptoms always occur after eating, when your stomach is digesting — what doctors call the postprandial period. You may have symptoms of indigestion for a few minutes to a few hours after eating. It takes 3 to 5 hours for your stomach to digest a meal before passing it on to your intestines. During that time, your pancreas and gallbladder send bile and enzymes to your stomach to help with digestion. These are the organs in your epigastric region (upper middle abdomen), where indigestion symptoms occur.
Experts generally agree that the symptoms of indigestion include:
- Epigastric pain. Your epigastrium is your central, upper abdominal region. This is where your stomach is.
- Burning sensation. Burning may come from stomach acids and enzymes in your GI tract, or from inflammation.
- Early or late-lasting satiety. Feeling full soon after eating, or long after, suggests your stomach is overwhelmed.
But people who experience indigestion often report other symptoms along with it, such as:
- Bloating.
- Gas.
- Nausea.
- Burping.
- Regurgitation (when swallowed food comes back up).
- Acid reflux.
- Heartburn.
These symptoms can overlap with indigestion, but they can also occur separately from it.
The symptoms of indigestion may look like other health problems. Always see your doctor to be sure.
Sometimes people with indigestion also experience heartburn, but heartburn and indigestion are two separate conditions. Heartburn is a pain or burning feeling in the center of your chest that may radiate into your neck or back during or after eating.
Indigestion complications
Although indigestion doesn’t usually have serious complications, it can affect your quality of life by making you feel uncomfortable and causing you to eat less. You might miss work or school because of your symptoms. When indigestion is caused by an underlying condition, that condition can also have its own complications.
Sometimes indigestion can be the sign of a serious problem–for example, a deep stomach ulcer. Rarely, indigestion is caused by stomach cancer. If you have indigestion, talk to your family doctor. This is especially important if any one of the following is true for you:
- You’re older than 50 years of age
- You recently lost weight without trying to
- You have trouble swallowing
- You have severe vomiting
- You have black, tarry bowel movements
Indigestion diagnosis
Your doctor is likely to start with a health history and a thorough physical exam. Those evaluations may be sufficient if your indigestion is mild and you’re not experiencing certain symptoms, such as weight loss and repeated vomiting.
But if your indigestion began suddenly, and you are experiencing severe symptoms or are older than age 55, your doctor may recommend:
- Laboratory tests, to check for thyroid problems or other metabolic disorders.
- Breath and stool tests, to check for Helicobacter pylori (H. pylori), the bacterium associated with peptic ulcers, which can cause indigestion. H. pylori testing is controversial because studies suggest limited benefit from treating the bacterium.
- Urea breath test. Your doctor may use a urea breath test to check for H. pylori infection. You will swallow a capsule, liquid, or pudding that contains urea—a waste product the body produces as it breaks down protein. The urea is “labeled” with a special carbon atom. If H. pylori are present, the bacteria will convert the urea into carbon dioxide. After a few minutes, you will breathe into a container, exhaling carbon dioxide. A health care professional will test your exhaled breath for labeled carbon dioxide. If the test detects the labeled carbon atoms, the health care professional will confirm an H. pylori infection in your digestive tract. A doctor can also use this test to see if treatment has worked to get rid of H. pylori.
- Stool test. Your doctor may use stool tests to look for signs of H. pylori infection. Your doctor may also use a stool test to see if treatment has worked to get rid of H. pylori.
- Upper gastrointestinal (GI) endoscopy, to check for abnormalities in your upper digestive tract. A tissue sample (biopsy) may be taken for analysis.
- Imaging tests (X-ray or CT scan), to check for intestinal obstruction.
In an upper gastrointestinal (GI) endoscopy, a small tube with a camera inside it is put into your mouth and down into your stomach. Then your doctor can look inside your stomach to try to find a cause for your pain. During an upper gastrointestinal (GI) endoscopy, your doctor can use tiny tools passed through the endoscope to take small pieces of tissue from the lining of your stomach and duodenum. This procedure is called an upper GI biopsy. A doctor will examine the tissue samples to look for digestive tract diseases and conditions, including Helicobacter pylori (H. pylori) infection.
Your doctor may recommend an upper gastrointestinal (GI) endoscopy for people with indigestion who are older than 55 or for people with indigestion of any age who have:
- a family history of cancer
- difficulty swallowing
- evidence of bleeding in the digestive tract
- frequent vomiting
- weight loss
If initial testing fails to provide a cause, your doctor may diagnose functional dyspepsia.
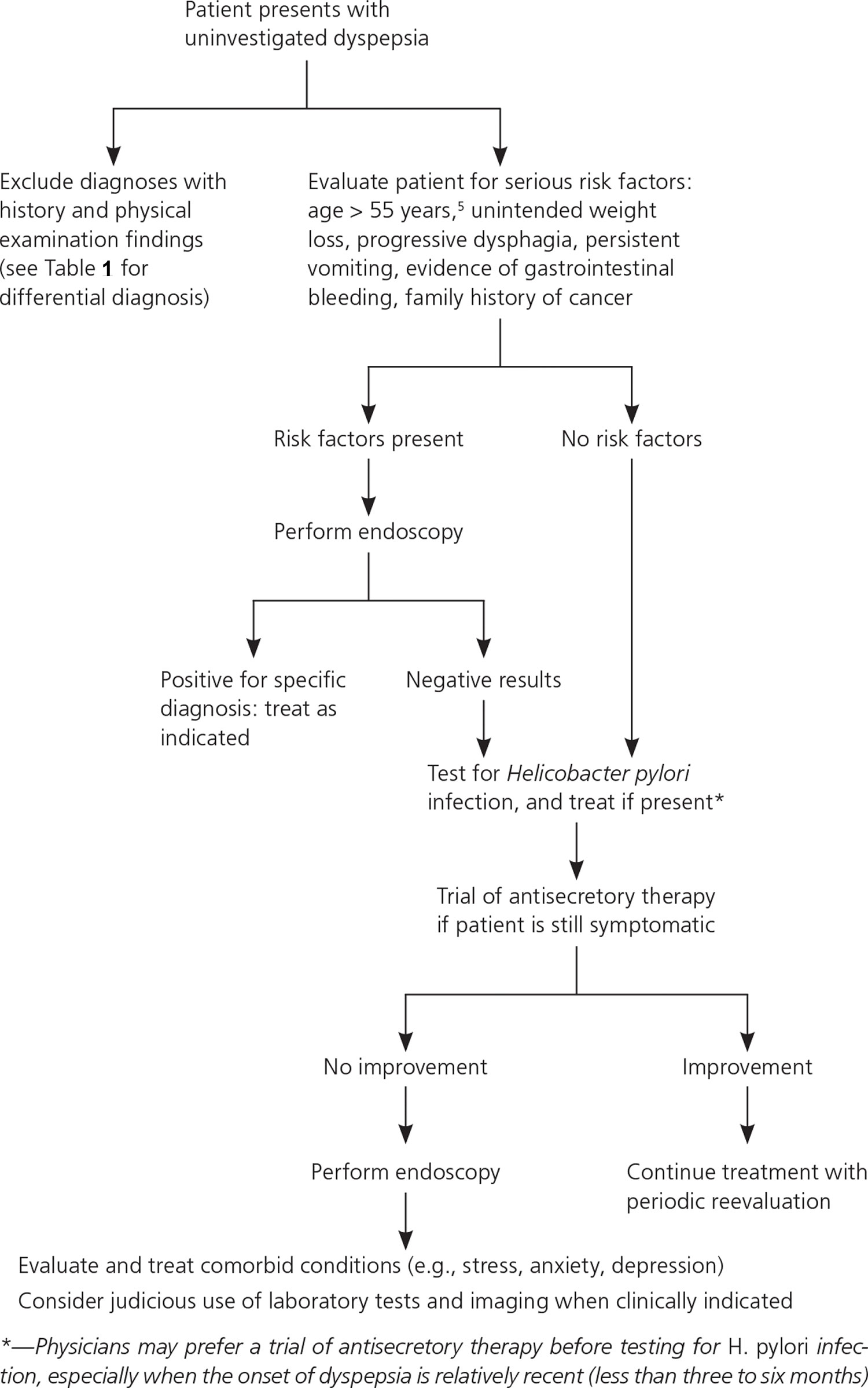
Figure 2. Evaluation and Management of indigestion
How to get rid of indigestion
Treatment for indigestion depends on the cause and may include:
- over-the-counter and prescription medicines
- changing what you eat and drink
- psychological therapies
Your treatment will depend on what is causing your dyspepsia, but medicine is the most common treatment. If you have a stomach ulcer, it can be cured. You may need to take an acid-blocking medicine. If you have an infection in your stomach, you may also need to take an antibiotic. If your doctor thinks that a medicine you’re taking causes your dyspepsia, you might take another medicine. A medicine that cuts down on the amount of acid in your stomach might help your pain. This medicine can also help if you have acid reflux disease. Your doctor might want you to have an upper gastrointestinal (GI) endoscopy if you are older than 55 or you have indigestion and the following:
- a family history of cancer
- difficulty swallowing
- evidence of bleeding in the digestive tract
- frequent vomiting
- weight loss
Some people may experience relief from symptoms of indigestion by:
- eating several small, low-fat meals throughout the day at a slow pace
- refraining from smoking
- abstaining from consuming coffee, carbonated beverages, and alcohol
- stopping use of medications that may irritate the stomach lining—such as aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs)
- getting enough rest
- finding ways to decrease emotional and physical stress, such as relaxation therapy or yoga.
Indigestion treatment at home
Lifestyle changes may help ease indigestion.
You can do quite a bit to help yourself feel better:
- If you smoke, stop smoking.
- Losing weight, if you are overweight. Excess pounds put pressure on your abdomen, pushing up your stomach and causing acid to back up into your esophagus.
- Exercising regularly. Exercise helps you keep off extra weight and promotes better digestion.
- If some foods bother your stomach, try to avoid eating them.
- Managing stress. Create a calm environment at mealtime. Practice relaxation techniques, such as deep breathing, meditation or yoga. Spend time doing things you enjoy.
- Get plenty of sleep.
- If you have acid reflux, don’t eat right before bedtime.
- Raising the head of your bed with blocks under two legs may also help.
- Unless your doctor tells you otherwise, don’t take a lot of anti-inflammatory medicines like ibuprofen (one brand: Motrin), aspirin, naproxen (brand name: Aleve) and ketoprofen (brand name: Orudis). Acetaminophen (brand name: Tylenol) is a better choice for pain, because it doesn’t hurt your stomach.
- Changing your medications. With your doctor’s approval, stop or cut back on pain relievers or other medications that may irritate your stomach lining. If that’s not an option, be sure to take these medications with food.
Mild indigestion can often be helped with lifestyle changes, including:
- Avoiding foods that trigger indigestion. Fatty and spicy foods, processed foods, carbonated beverages, caffeine, alcohol, and smoking can trigger indigestion.
- Eating five or six small meals a day instead of three large meals. Chew your food slowly and thoroughly.
- Reducing or eliminating the use of alcohol and caffeine
- Avoiding certain pain relievers, such as aspirin, ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve)
- Finding alternatives for medications that trigger indigestion
- Controlling stress and anxiety
- Cut down on tea, coffee, cola or alcohol.
Alternative medicine
Alternative and complementary treatments may help ease indigestion, although none of these treatments has been well-studied. These treatments include:
- Herbal therapies such as peppermint and caraway.
- Psychological treatment, including behavior modification, relaxation techniques, cognitive behavioral therapy and hypnotherapy.
- Acupuncture, which may work by blocking the pathways of nerves that carry sensations of pain to the brain.
- Mindfulness meditation.
- STW 5 (Iberogast), a liquid supplement that contains extracts of herbs including bitter candytuft, peppermint leaves, caraway and licorice root. STW 5 may work by reducing the production of gastric acid.
Always check with your doctor before taking any supplements to be sure you’re taking a safe dose and that the supplement won’t adversely interact with any other medications you’re taking.
Reduce stress in your daily life
Chronic stress can be bad for your body and mind. It can put you at risk for health problems such as high blood pressure, stomachaches, headaches, anxiety, and depression. Using stress-reduction techniques or relaxation therapy can help you feel calm and manage your symptoms.
When you feel stress, your body responds by releasing hormones that increase your blood pressure and raise your heart rate. This is called the stress response.
Relaxation techniques can help your body relax and lower your blood pressure and heart rate. This is called a relaxation response.
There are many healthy ways to manage stress. Try a few and see which ones work best for you.
Deep breathing
One of the simplest ways to relax is by practicing deep breathing. You can do deep breathing almost anywhere.
- Sit still or lie down and place one hand on your stomach. Put your other hand over your heart.
- Inhale slowly until you feel your stomach rise.
- Hold your breath for a moment.
- Exhale slowly, feeling your stomach fall.
There are also many other types of breathing techniques you can learn. In many cases, you do not need much instruction to do them on your own.
Meditation
Meditation involves focusing your attention to help you feel more relaxed. Practicing meditation may help you react in a calmer way to your emotions and thoughts, including those that cause stress. Meditation has been practiced for thousands of years, and there are several different styles.
Most types of meditation usually include:
- Focused attention. You might focus on your breath, an object, or a set of words.
- Quiet. Most meditation is done in a quiet area to limit distractions.
- Body position. Most people think meditation is done while sitting, but it can also be done lying down, walking, or standing.
- An open attitude. This means that you stay open to thoughts that come into your mind during meditation. Instead of judging these thoughts, you let them go by bringing your attention back to your focus.
- Relaxed breathing. During meditation, you breathe slowly and calmly. This also helps you relax.
Biofeedback
Biofeedback teaches you how to control some of your body’s functions, such as your heart rate or certain muscles.
In a typical session, a biofeedback therapist attaches sensors to different areas of your body. These sensors measure your skin temperature, brain waves, breathing, and muscle activity. You can see these readings on a monitor. Then you practice changing your thoughts, behaviors, or emotions to help control your body’s responses. Over time, you can learn to change them without using the monitor.
Progressive relaxation
This is another simple technique that you can do almost anywhere. Starting with your toes and feet, focus on tightening your muscles for a few moments and then releasing them. Continue with this process, working your way up your body, focusing on one group of muscles at a time.
Yoga
Yoga is an ancient practice rooted in Indian philosophy. The practice of yoga combines postures or movements with focused breathing and meditation. The postures are meant to increase strength and flexibility. Postures range from simple poses lying on the floor to more complex poses that may require years of practice. You can modify most yoga postures based on your own ability.
There are many different styles of yoga that range from slow to vigorous. If you are thinking about starting yoga, look for a teacher who can help you practice safely. Make sure to tell your teacher about any recent or past injuries.
Tai Chi
Tai chi was first practiced in ancient China for self-defense. Today, it is used mainly to improve health. It is a low-impact, gentle type of exercise that is safe for people of all ages.
There are many styles of tai chi, but all involve the same basic principles:
- Slow, relaxed movements. The movements in tai chi are slow, but your body is always moving.
- Careful postures. You hold specific postures as you move your body.
- Concentration. You are encouraged to put aside distracting thoughts while you practice.
- Focused breathing. During tai chi, your breathing should be relaxed and deep.
If you are interested in tai chi for stress relief, you may want to start with a class. For many people, it is the easiest way to learn the proper movements. You can also find books and videos about tai chi.
Exercise
Getting physical activity every day is one of the easiest and best ways to cope with stress. When you exercise, your brain releases chemicals that make you feel good. It can also help you release built-up energy or frustration. Find something you enjoy, whether it is walking, cycling, softball, swimming, or dancing, and do it for at least 30 minutes on most days.
Indigestion medicine
If your indigestion won’t go away after trying lifestyle changes and home remedies, indigestion medication may help. Your doctor may recommend over-the-counter antacids (nonprescription antacids) or medications that reduce acid production or help the stomach move food more quickly into the small intestine. Many of these medications can be purchased without a prescription. Nonprescription medications should only be used at the dose and for the length of time recommended on the label unless advised differently by a doctor. Informing the doctor when starting a new medication is important. If you are pregnant, check with your doctor or pharmacist if these medications are safe for you to take. Pregnant women often get indigestion. It’s very common from 27 weeks onwards. It can be caused by hormonal changes and the growing baby pressing against the stomach.
- Antacids, such as Alka-Seltzer, Maalox, Mylanta, Rolaids, and Riopan, are usually the first drugs recommended to relieve symptoms of indigestion. Many brands on the market use different combinations of three basic salts—magnesium, calcium, and aluminum—with hydroxide or bicarbonate ions to neutralize the acid in the stomach. Antacids, however, can have side effects. Magnesium salt can lead to diarrhea, and aluminum salt may cause constipation. Aluminum and magnesium salts are often combined in a single product to balance these effects. Calcium carbonate antacids, such as Tums, Titralac, and Alka-2, can also be a supplemental source of calcium, though they may cause constipation.
- Gas-relieving medicine. Gas-relieving medicine that are available without a prescription. An ingredient called simethicone may provide some relief by reducing intestinal gas. Simethicone is used to relieve painful pressure caused by excess gas in the stomach and intestines. Simethicone is a silicone compound that functions as a non-systemic surfactant, decreasing the surface tension of gas bubbles in the gastrointestinal (GI) tract 6. This action results in coalescence and dispersion of the gas bubbles allowing their removal from the gastrointestinal tract as flatulence or belching. Simethicone causes the gas bubbles to accumulate and therefore pass more easily either through the upper gastrointestinal or lower gastrointestinal opening 6. Simethicone does not appear to reduce the actual production of gas in the GI tract 7 Examples of gas-relieving medicines include Mylanta, Maalox, Alka-Seltzer Anti-Gas and Gas-X.
- H2-receptor blockers (Histamine Type-2 Receptor Antagonists) include ranitidine (Zantac), cimetidine (Tagamet HB), famotidine (Pepcid AC), and nizatidine (Axid AR) and are available both by prescription and over-the-counter. H2-receptor blockers treat symptoms of indigestion by reducing the amount of stomach acid released into your digestive tract, which relieves ulcer pain and encourages healing. Stronger versions of these medicines also are available by prescription.. They work longer than but not as quickly as antacids. Side effects of H2-receptor blockers may include headache, nausea, vomiting, constipation, diarrhea, and unusual bleeding or bruising.
- Proton pump inhibitors (PPIs) reduce stomach acid by blocking the action of the parts of cells that produce acid. Proton pump inhibitors (PPIs), which are stronger than H2-receptor blockers, also treat indigestion symptoms by reducing stomach acid. Proton pump inhibitors (PPIs) are most effective in treating symptoms of indigestion in people who also have GERD. Proton pump inhibitors (PPIs) include the prescription and over-the-counter medications omeprazole (Prilosec, Zegerid), lansoprazole (Prevacid), rabeprazole (Aciphex), esomeprazole (Nexium), dexlansoprazole (Dexilant) and pantoprazole (Protonix). There are very few medical differences between these drugs. However, long-term use of proton pump inhibitors (PPIs), particularly at high doses, may increase your risk of hip, wrist and spine fracture. Ask your doctor whether a calcium supplement may reduce this risk. In patients whose symptoms improve with proton pump inhibitors (PPIs), PPI (proton pump inhibitor) therapy should be discontinued every 6 to 12 months to reduce the long-term risk of therapy. Side effects of PPIs may include back pain, aching, cough, headache, dizziness, abdominal pain, gas, nausea, vomiting, constipation, and diarrhea. The standard dosages of orally administered proton pump inhibitors are as follows:
- Lansoprazole 30 mg daily
- Omeprazole 20 mg daily
- Pantoprazole 40 mg daily
- Rabeprazole 20 mg daily
- Esomeprazole 20 mg daily
- Proton pump inhibitors (PPIs) require a meal to activate them. You should eat a meal within 30 minutes to 1 hour after taking this medication for the acid suppression therapy to work most effectively. Waiting later than this time can decrease the positive effect of this medication. This might delay healing or even result in the failure of the ulcer to heal.
- Prokinetics help your stomach empty faster and tighten the valve between your stomach and esophagus (the lower esophageal sphincter). This helps to reduce upper abdominal pain. Prescription prokinetics such as bethanechol (Urecholine) and metoclopramide (Reglan) may be helpful for people who have a problem with the stomach emptying too slowly. Metoclopramide also improves muscle action in the digestive tract. Prokinetics have frequent side effects that limit their usefulness, including fatigue, sleepiness, depression, anxiety, and involuntary muscle spasms or movements. Metoclopramide 5 to 10 mg is usually given one-half hour before meals and at night. A 4 to 8 week course is recommended and may be repeated when symptoms recur. However, in some patients, adverse effects may lead to discontinuation of therapy 8.
- Medicines to relieve nausea or anti-emetics. If you feel like throwing up after eating, anti-emetics may help. These include promethazine, prochlorperazine and meclizine.
- Low-dose antidepressants. Your doctor may prescribe low doses of tricyclic antidepressants (TCAs) and antidepressants known as selective serotonin reuptake inhibitors (SSRIs). These medicines may inhibit the activity of neurons that control intestinal pain. In patients whose symptoms are refractory to the initial 8 weeks of proton pump inhibitor (PPI) therapy, a tricyclic antidepressant (TCA) is suggested 9. For those who respond partially to proton pump inhibitors (PPIs), tricyclic antidepressants (TCAs) may be given in combination therapy with PPIs. The following approach is recommended:
- Start with either of the following low-dose tricyclic antidepressants (TCAs) at night:
- Amitriptyline 10 mg 10
- Nortriptyline 10 mg
- Desipramine 25 mg
- Doses may be titrated up modestly according to symptoms.
- Higher doses may cause sedation and still not be more effective.
- Tricyclic antidepressant (TCA) is initially administered for 8 to 12 weeks and then continued for 6 months if the patient responds appropriately.
- Doses are slowly tapered.
- Tricyclic antidepressants (TCAs) may be resumed if symptoms recur.
- Start with either of the following low-dose tricyclic antidepressants (TCAs) at night:
- Mirtazapine has shown benefits in patients with functional dyspepsia and the associated weight loss that may be due to a central mechanism of action 11. As with tricyclic antidepressants (TCAs), an initial low dose is recommended. The dose is titrated from 7.5 mg an hour before bedtime to 45 mg daily.
If testing shows H. pylori bacteria that causes peptic ulcer disease is found in your digestive tract, your doctor may recommend a combination of antibiotics to kill the bacterium. These may include amoxicillin (Amoxil), clarithromycin (Biaxin), metronidazole (Flagyl), tinidazole (Tindamax), tetracycline and levofloxacin. The antibiotics used will be determined by where you live and current antibiotic resistance rates. You’ll likely need to take antibiotics for two weeks, as well as additional medications to reduce stomach acid, including a proton pump inhibitor (PPI) and possibly bismuth subsalicylate (Pepto-Bismol). To find out if the antibiotics worked, your doctor may recommend testing you for H. pylori at least 4 weeks after you’ve finished taking the antibiotics 12. If you still have an H. pylori infection, your doctor may prescribe a different combination of antibiotics and other medicines to treat the infection. Making sure that all of the H. pylori bacteria have been killed is important.
Psychological therapy
Patients with functional dyspepsia score higher than those without gastrointestinal symptoms for depression, anxiety, and somatization, which are more strongly associated with decreased quality of life than are the clinical symptoms themselves 13, 14. Your doctor may recommend a type of psychological therapy called “talk therapy” also called psychotherapy to help treat anxiety and depression that may be causing your indigestion. If stress is causing your indigestion, your doctor may recommend ways to help you reduce your stress, such as meditation, relaxation exercises or counseling. Talk therapy can also help you learn how to reduce your stress. A counselor or therapist can show you relaxation techniques to help you cope with your symptoms 15. You may also learn ways to reduce stress to help manage your symptoms.
What is functional dyspepsia
Functional dyspepsia, also known as nonulcer dyspepsia or “irritable stomach syndrome”, is a medical term for recurring symptoms of an upset stomach or indigestion (dyspepsia) that cannot be fully explained by another medical condition and when no cause can be found after a thorough physical examination and appropriate investigations 16, 17, 18, 19, 20, 21, 14, 22, 13, 23, 24. Functional dyspepsia symptoms resemble those of an upset stomach or indigestion. Functional dyspepsia is one of the most common functional gastrointestinal disorders and affects more than 20% of the population 25, 13. Functional dyspepsia is more common in women than in men. This difference is due to inherent sex-specific differences in gastrointestinal function. For example, sex-specific variation exists in hormone mechanisms, pain signaling, and healthcare maintenance 14.
Functional dyspepsia symptoms include:
- upper abdominal pain or discomfort
- frequently include symptoms of burning, pressure, or fullness often, but not necessarily, related to meals.
- early feeling of fullness (satiety)
- nausea
- belching
- bloating
Functional dyspepsia is common. It is a constant condition but symptoms don’t happen all the time.
Functional dyspepsia can be divided into 3 categories 26:
- Ulcer-like functional dyspepsia,
- Dysmotility-like functional dyspepsia,
- Unspecified.
Ulcer-like functional dyspepsia has upper abdominal pain as its predominant symptom. This pain is accompanied by several other symptoms, including 26:
- hunger pain that is sometimes relieved by eating,
- pain relieved by antacids,
- night pain,
- periodic pain, and
- pain which may be very localized in the upper middle region of the abdomen.
Dysmotility-like functional dyspepsia has upper abdominal discomfort, not pain, as its predominant symptom. It is accompanied by several other symptoms, including 26:
- early feeling of having enough to eat,
- fullness after a meal,
- nausea,
- recurrent retching and/or vomiting,
- upper abdominal bloating, and
- upper abdominal discomfort aggravated by food.
No one knows what causes functional dyspepsia. Experts consider it a functional disorder. That means it can’t be explained by a medical condition, so routine testing may not show any problems or causes. As a result, the diagnosis is based on your symptoms. However, care must be taken not to confuse functional dyspepsia with other common gastrointestinal (GI) disorders that may cause upper gastrointestinal distress, like heartburn, irritable bowel syndrome (IBS), gastroesophageal reflux disease (GERD), functional abdominal bloating, and functional biliary disorders.
Confirmation of the diagnosis of functional dyspepsia rests on 27, 8, 28:
- The typical symptoms and the patient’s history
- The exclusion of other diseases of the upper gastrointestinal tract and upper abdominal organs that may present with similar dyspeptic symptoms.
Functional dyspepsia is diagnosed based on the Rome IV (4) criteria. The diagnosis of functional dyspepsia must include one or more of the following for at least 4 days per month 29, 27:
- Bothersome after eating a meal fullness (satiety)
- Bothersome early satiation
- Bothersome epigastric pain not associated with defecation
- Bothersome epigastric burning not associated with defecation
- After appropriate evaluation, the symptoms cannot be fully explained by another medical condition
These criteria should be fulfilled for the last two months before diagnosis 29.
The current Rome IV (4) criteria divide functional dyspepsia into two subgroups according to the cardinal symptoms (Figure 2) 29, 27:
- Epigastric pain syndrome (EPS) — predominant epigastric pain or burning.
- Postprandial distress syndrome (PDS) — feeling of fullness and early satiation.
Functional dyspepsia that can’t be managed with lifestyle changes may need treatment. Functional dyspepsia may be treated with changes in your diet or with medications. Although studies have not proven that dietary changes help, individual dietary experimentation may prove helpful for some.
- Avoiding spicy and fatty food may reduce symptoms of fullness after eating.
- Eating six small, low-fat meals per day may reduce early feelings of fullness, bloating after a meal, or nausea.
- Avoidance of caffeine, alcohol or smoking may also help.
In patients who fail to respond to treatment, specialized diagnostic procedures should be carried out on an individual basis. In the presence of accompanying symptoms of reflux, 24-h monitoring of esophageal pH/impedance may be helpful 30. C13 Urea Breath tests and gastric emptying scintigraphy may detect an underlying gastric emptying disorder or gastroparesis 13.
In the case of accompanying severe flatulence, further breath tests for carbohydrate intolerance and abnormal bacterial colonization may be useful 13. Patients whose symptoms do not respond to treatment should be screened for mental disorders such as anxiety, depression, and stress 14, 31, 32, 33.
Figure 1. Digestive system
Footnotes: Your digestive system processes nutrients in foods that you have eaten and helps pass waste material out of your body. Food moves from your throat to your stomach through a tube called the esophagus. After food enters your stomach, it is broken down by stomach acid and muscles that mix the food and liquid with digestive juices. After leaving your stomach, partly digested food passes into your small intestine and then into your large intestine. The end of the large intestine, called the rectum, stores the waste from the digested food until it is pushed out of the anus during a bowel movement.
Figure 2. Functional dyspepsia
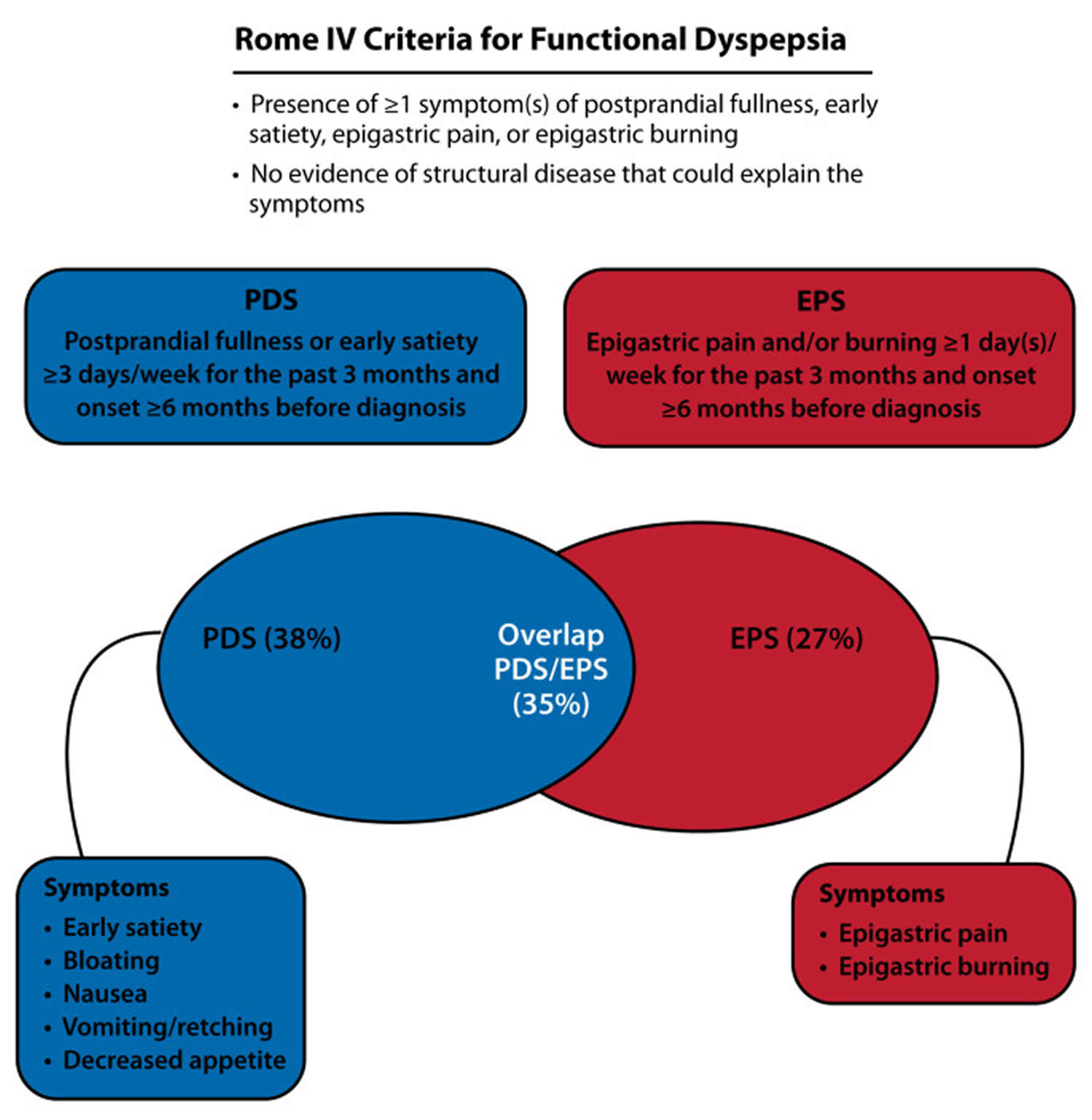
Footnote: Rome IV criteria for functional dyspepsia and its subclassifications.
Abbreviations: EPS, epigastric pain syndrome; PDS, postprandial distress syndrome.
[Source 20 ]Figure 3. Functional dyspepsia types
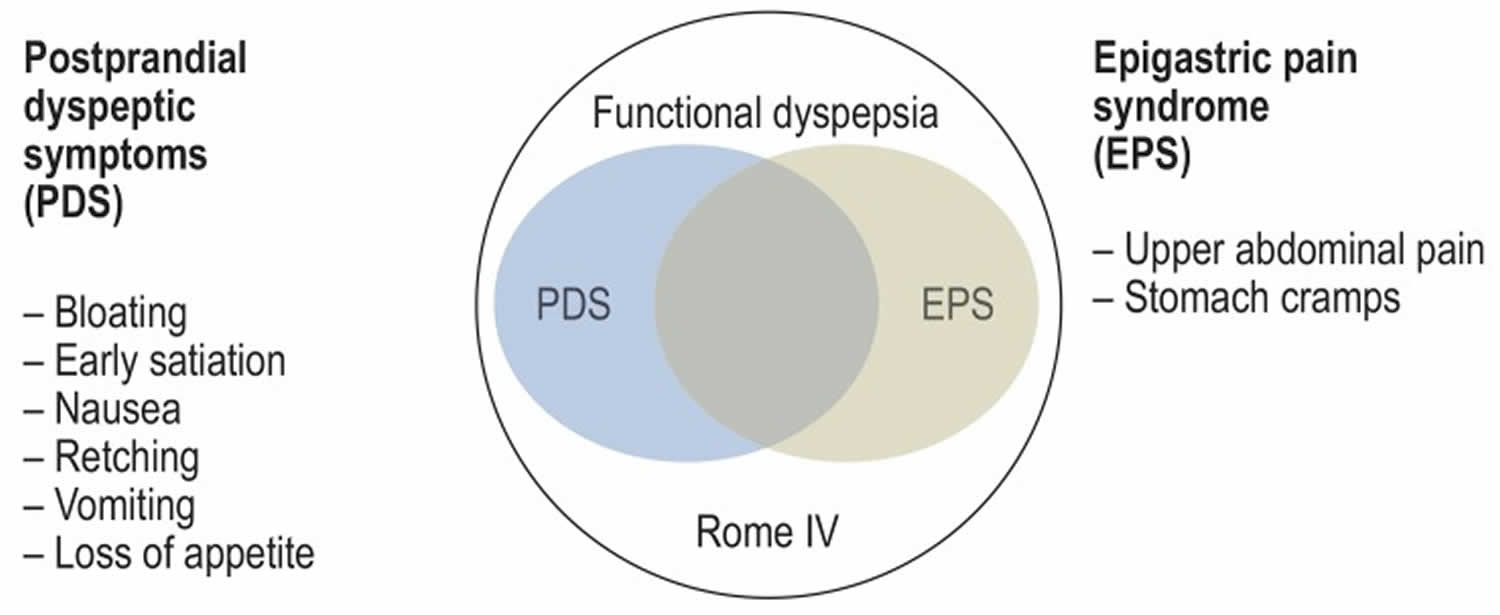
Footnote: Definition of functional dyspepsia according to the Rome IV criteria. Functional dyspepsia is divided into two subgroups according to the cardinal symptoms 27:
- Epigastric pain syndrome (EPS): predominant epigastric pain or burning
- Postprandial distress syndrome (PDS): feeling of fullness and early satiation.
Figure 4. Functional dyspepsia diagnostic algorithm
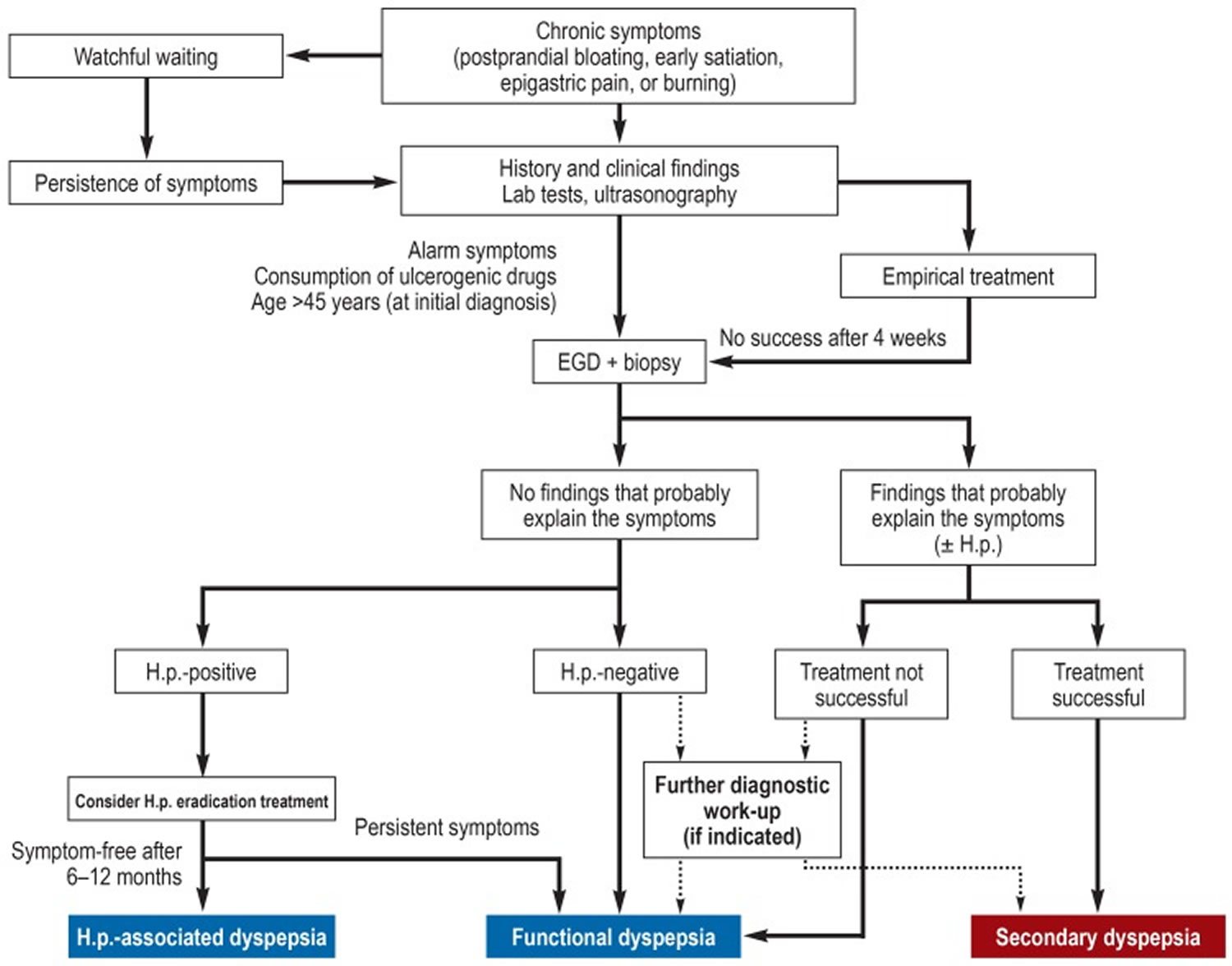
Abbreviations: H.p. = Helicobacter pylori; EGD = esophagogastroduodenoscopy
[Source 13 ]See your doctor if you experience persistent symptoms that worry you.
See your doctor right away if you have any of the following:
- Bloody vomit.
- Vomiting, with or without blood
- Trouble swallowing or pain while swallowing
- Decreased appetite (loss of appetite) or feeling full sooner than usual
- Continued heartburn while taking the medicine
- Shortness of breath.
- Pain in your jaw, neck or arm.
- Weight loss for no known reason (without trying)
- Blood in the stool or dark, tarry stools.
- Yellowing of the skin and eyes (jaundice), if the cancer spreads to the liver
- Ascites (swelling or fluid build-up in the abdomen)
- Trouble swallowing
- Feeling tired or weak, as a result of having too few red blood cells (anemia)
Functional dyspepsia cause
The causes of functional dyspepsia are largely unknown and likely involving or dependent on a number of factors (multifactorial), especially genetic or environmental factors 20. Functional dyspepsia is currently considered to be a bio-psychosocial disorder with disturbances of motor function, heightened visceral sensitivity, and possibly a central nervous system disturbance 34, 35. Psychosocial factors can alter motility and/or enhance sensation and influence the timing of patients’ presentation to physicians 34, 35. Some evidence exists to implicate a genetic predisposition. Although Helicobacter pylori (H. pylori) infection may produce dyspeptic symptoms in a small subset of patients, there is little data to support this bacteria as a cause of symptoms in a majority of patients. Psychological factors may influence the symptom experience in some patients with functional dyspepsia.
Changes in gastric function have been identified in many patients with functional dyspepsia. In approximately 40% of patients with dyspepsia, the stomach does not relax normally in response to a meal 36, 37, 38. This is known as “impaired accommodation” and may be associated with symptoms of fullness and pressure in some patients. Impaired stomach contractions and abnormal stomach emptying may also be seen in a similar percentage of patients.
Impaired stomach emptying has been associated with symptoms of bloating and early feeling of fullness. As many as two-thirds of patients with functional dyspepsia have heightened perception of stomach activity, which is termed visceral hypersensitivity. While frequently seen, visceral hypersensitivity in functional dyspepsia has not been strongly associated with any specific symptoms.
Both with an empty stomach and after a meal, patients with functional dyspepsia suffer from visceral hypersensitivity when the gastric fundus is expanded 39, 40. The proportion of patients found to have this hypersensitivity depends on the diagnostic criteria and on whether hypersensitivity is defined as abnormal pain projection, allodynia, and/or hyperalgesia. In any case the hypersensitivity correlates with the severity of the symptoms 41. Even patients with normal fundus accommodation may react hypersensitively to expansion of the stomach 42 and some patients with functional dyspepsia also react hypersensitively to expansion of the duodenum, jejunum, or rectum 43. This finding points to generalized rather than local visceral sensitization of the efferent or afferent enteric nerves or of the sensory nerves connecting the gut with the central nervous system (gut–brain axis). The hypersensitivity following stomach expansion is ameliorated by inhibition of cholinergic tone but not by active muscle relaxation by means of the NO donor nitroglycerin 44. This shows the predominant role of the cholinergic enteric innervation in the origin of hypersensitivity.
Symptoms of functional dyspepsia occur after infusion of acid into the duodenum 45 and probably result from sensitized pH sensors or insufficient removal of the acid due to impaired motor function of the proximal duodenum 46. This is in accordance with the elevated sensitivity to capsaicin 47. Capsaicin is a TRPV1 agonist (transient receptor potential cation channel subfamily V member 1) that is stimulated by, among other factors, decreased pH.
The presence of fat in the duodenum triggers the symptoms of functional dyspepsia due to direct neural action, increased sensitivity of enteroendocrine cells, systemic or local elevation of cholecystokinin concentration, and/or increased sensitivity of the cholecystokinin-A receptors 48.
Risk factors for functional dyspepsia
Some factors can increase the risk of functional dyspepsia. They include:
- Being female.
- Using certain pain relievers that are available without a prescription. These include aspirin and ibuprofen (Advil, Motrin IB, others), which can cause stomach problems.
- Smoking.
- Anxiety or depression.
- History of childhood physical or sexual abuse.
- Helicobacter pylori infection.
Functional dyspepsia pathophysiology
Although the exact mechanism is not well understood, the pathophysiology of functional dyspepsia is complex. Several different mechanisms are thought to contribute to each subtype. Traditionally, functional dyspepsia has been attributed to disturbances in gastric physiologic factors divided into macroscopic and microscopic mechanisms.
- Macroscopic mechanisms include the following:
- Gastroesophageal reflux (GERD)
- Delayed gastric emptying, rapid gastric emptying, gastric dysrhythmias, and antral hypomotility 49
- Visceral hypersensitivity alterations in the nervous system 50:
- Lower threshold for pain in the presence of normal gastric compliance
- Contributed to abnormal processing of afferent input in the spinal cord or brain as well as dysfunction of mechanoreceptors.
- Microscopic mechanisms include the following:
- Impaired barrier function
- Altered sensitivity to duodenal acid or lipids impairs mucosal integrity.
- Gastroduodenal inflammation 51
- Characterized by altered lymphocytes, including “gut-homing” lymphocytes, increased eosinophils, and mast cells 52
- Altered gut microbiome and Helicobacter pylori infection 53
- Impaired barrier function
Additional mechanisms include environmental insults like food-inducing gastroduodenal physiologic changes, infections causing inflammation, and allergen exposure can lead to eosinophil recruitment in genetically predisposed patients.
Psychological factors like anxiety and depression can cause increased activation of the amygdala, and the dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis suggests that there is central processing of visceral stimuli from sensations in the gastrointestinal tract 54. Acute stress also increases salivary cortisol levels and intestinal permeability in healthy individuals 55. A higher prevalence of functional gastrointestinal disorders is present in patients with a history of childhood abuse 56.
Functional dyspepsia symptoms
When you have indigestion or dyspepsia, you may have one or more of the following symptoms:
- Pain or burning in the stomach, bloating, excessive belching, or nausea after eating
- An early feeling of fullness when eating. The feeling of fullness also is called satiety.
- Stomach pain that occurs unrelated to meals or goes away when eating.
- Feeling uncomfortably full after eating a meal
- Bloating
- Burping
Other symptoms may include:
- burping up food or liquid
- loud growling or gurgling in your stomach
- nausea
- gas
Sometimes when you have indigestion, you may also have heartburn. However, heartburn and indigestion are two separate conditions.
Functional dyspepsia types
Functional dyspepsia is divided into two subgroups according to the cardinal symptoms 27:
- Epigastric pain syndrome (EPS): predominant epigastric pain or burning
- Postprandial distress syndrome (PDS): feeling of fullness and early satiation.
Epigastric pain syndrome
Epigastric pain syndrome with no evidence of systemic, organic, or metabolic disease is diagnosed with at least one of the following symptoms (severe enough to impact usual activities) occurring at least once per week, for 3 or more months with onset at least 6 months before diagnosis: epigastric burning (severe enough to impact usual activities) or epigastric pain.
Supportive criteria include the following 27:
- Postprandial epigastric bloating, nausea, and belching may also be present.
- Pain does not meet biliary pain criteria.
- Pain may be provoked or relieved by ingesting meals and can also occur while fasting.
- Persistent vomiting is suggestive of another condition.
- Heartburn may coexist.
- Symptoms relieved by flatus or defecation are typically not considered part of dyspepsia.
Postprandial distress syndrome
Postprandial distress syndrome with no evidence of systemic, organic, or metabolic disease is diagnosed with at least one of the following symptoms (severe enough to impact usual activities) occurring at least 3 days per week, for 3 or more months with onset at least 6 months before diagnosis: postprandial fullness (severe enough to impact usual activities) or early satiation that prevents finishing a regular-size meal.
Supportive symptoms include the following 27:
- Nausea
- Postprandial epigastric pain or burning
- Epigastric bloating
- Excessive belching
- Heartburn
Symptoms relieved by flatus or defecation are typically not considered part of dyspepsia. Persistent vomiting could be suggestive of a coexisting condition. Reflux symptoms and irritable bowel syndrome may also be present.
Functional dyspepsia complications
Although functional dyspepsia is not associated with increased mortality, it does cause physical and mental distress affecting the patient’s quality of life 25. Patients with functional dyspepsia score higher on psychometric tests for symptoms of anxiety, depression, and somatization. About 10% to 25% of patients report the social impact of their symptoms is significant enough to seek a physician, leading to more healthcare visits, greater health impairment, and a worsening quality of life 25.
Functional dyspepsia diagnosis
Your doctor will review your symptoms, medical history and perform a physical exam. He or she will ask you about your eating and drinking habits, your use of over-the-counter and prescription medicines, and whether you smoke.
Several tests can help find the cause of your discomfort and rule out other disorders. These may include:
- Blood tests. Blood tests may help rule out other diseases that can cause symptoms like those of functional dyspepsia.
- Laboratory tests for H. pylori. Your doctor may recommend tests to determine whether the bacterium H. pylori is present in your body. He or she may look for H. pylori using a blood, stool or breath test. The breath test is the most accurate.
- Urea breath test. Doctors may use a urea breath test to check for H. pylori infection. For the breath test, you will swallow a capsule, liquid, or pudding that contains urea “labeled” with a special carbon atom (radioactive carbon). H. pylori breaks down the substance in your stomach. If H. pylori is present, the bacteria will convert the urea into carbon dioxide. After a few minutes, you will breathe into a bag, exhaling carbon dioxide, which is then sealed. If you’re infected with H. pylori, your breath sample will contain the radioactive carbon in the form of carbon dioxide (CO2). If you are taking an antacid prior to the testing for H. pylori, make sure to let your doctor know. Depending on which test is used, you may need to discontinue the medication for a period of time because antacids can lead to false-negative results.
- Blood test. Doctors may use blood tests to check for signs of H. pylori infection or complications of peptic ulcers. For a blood test, a health care professional will take a blood sample from you and send the sample to a lab.
- Stool test. Doctors may use stool tests to check for H. pylori infection. Your doctor will give you a container for catching and holding a stool sample. You will receive instructions on where to send or take the kit for testing.
- Upper gastrointestinal endoscopyy also called EsophagoGastroDuodenoscopy (EGD). Your doctor is more likely to recommend endoscopy if you are older, have signs of bleeding, or have experienced recent weight loss or difficulty eating and swallowing. Your doctor may use a scope to examine your upper digestive system (endoscopy). During upper endoscopy (EGD), your doctor passes a hollow tube equipped with a lens (endoscope) down your throat and into your esophagus, stomach and small intestine. Using the endoscope, your doctor looks for ulcers. If your doctor detects an ulcer, a small tissue sample (biopsy) may be removed for examination in a lab. A biopsy can also identify whether H. pylori is in your stomach lining. If the endoscopy shows an ulcer in your stomach, a follow-up endoscopy should be performed after treatment to show that it has healed, even if your symptoms improve.
The American College of Gastroenterology (ACG) recommends the routine use of upper endoscopy in patients older than 60 to rule out malignancy, especially in the setting of red flag signs 25. If patients do not respond to treatment, pursuing more specialized testing specific to the symptoms is reasonable 13. Confirmation of the diagnosis is based on the patient’s history by excluding other diseases with similar presentations 13.
In some cases, you may have other tests to see how well your stomach empties its contents.
Confirmation of the diagnosis of functional dyspepsia rests on 27, 8, 28:
- The typical symptoms and the patient’s history
- The exclusion of other diseases of the upper gastrointestinal tract and upper abdominal organs that may present with similar dyspeptic symptoms.
Functional dyspepsia diagnostic criteria
Functional dyspepsia is diagnosed based on the Rome IV (4) criteria. The diagnosis of functional dyspepsia must include one or more of the following for at least 4 days per month 29, 27:
- Bothersome after eating a meal fullness (satiety)
- Bothersome early satiation
- Bothersome epigastric pain not associated with defecation
- Bothersome epigastric burning not associated with defecation
- After appropriate evaluation, the symptoms cannot be fully explained by another medical condition
These criteria should be fulfilled for the last two months before diagnosis 29.
Functional dyspepsia differential diagnosis
These conditions should be considered in functional dyspepsia differential diagnosis.
- GERD
- H. pylori infection
- Gastritis
- Peptic ulcer disease
- Celiac disease
- Irritable bowel syndrome
- Small intestinal bacterial overgrowth
- Chronic pancreatitis
- Gastroparesis
- Acute cholecystitis
- Gastric carcinoma
Functional dyspepsia treatment
Functional dyspepsia treatment depends on your symptoms. It may combine medicines and behavior therapy. Patients whose symptoms do not respond to treatment should be screened for mental disorders such as anxiety, depression, and stress 14, 31, 32, 33.
Diet for functional dyspepsia
Most patients with functional dyspepsia have symptoms associated with the ingestion of food. As such, a variety of dietary recommendations are often made, although no clinical trials have formally evaluated specific dietary interventions for the treatment of functional dyspepsia 57. There are limited data to suggest that dietary fat may induce or worsens symptoms and patients often report improvement by eating low-fat meals, and more frequent, smaller meals.
Changes to what you eat and how you eat might help control your symptoms. Try to:
- Eat smaller, more-frequent meals. Having an empty stomach sometimes contributes to functional dyspepsia. Nothing but acid in your stomach may make you feel sick. Try eating a small snack such as a cracker or a piece of fruit. Try not to skip meals. Avoid large meals and overeating. Eat smaller meals more often.
- Stay away from trigger foods. Some foods may trigger functional dyspepsia. These may include fatty and spicy foods, carbonated beverages, caffeine, and alcohol.
- Chew your food slowly and completely. Allow time to enjoy your meals.
Reduce stress in your daily life
Chronic stress can be bad for your body and mind. It can put you at risk for health problems such as high blood pressure, stomachaches, headaches, anxiety, and depression. Using stress-reduction techniques or relaxation therapy can help you feel calm and manage your symptoms.
When you feel stress, your body responds by releasing hormones that increase your blood pressure and raise your heart rate. This is called the stress response.
Relaxation techniques can help your body relax and lower your blood pressure and heart rate. This is called a relaxation response.
There are many healthy ways to manage stress. Try a few and see which ones work best for you.
Deep breathing
One of the simplest ways to relax is by practicing deep breathing. You can do deep breathing almost anywhere.
- Sit still or lie down and place one hand on your stomach. Put your other hand over your heart.
- Inhale slowly until you feel your stomach rise.
- Hold your breath for a moment.
- Exhale slowly, feeling your stomach fall.
There are also many other types of breathing techniques you can learn. In many cases, you do not need much instruction to do them on your own.
Meditation
Meditation involves focusing your attention to help you feel more relaxed. Practicing meditation may help you react in a calmer way to your emotions and thoughts, including those that cause stress. Meditation has been practiced for thousands of years, and there are several different styles.
Most types of meditation usually include:
- Focused attention. You might focus on your breath, an object, or a set of words.
- Quiet. Most meditation is done in a quiet area to limit distractions.
- Body position. Most people think meditation is done while sitting, but it can also be done lying down, walking, or standing.
- An open attitude. This means that you stay open to thoughts that come into your mind during meditation. Instead of judging these thoughts, you let them go by bringing your attention back to your focus.
- Relaxed breathing. During meditation, you breathe slowly and calmly. This also helps you relax.
Biofeedback
Biofeedback teaches you how to control some of your body’s functions, such as your heart rate or certain muscles.
In a typical session, a biofeedback therapist attaches sensors to different areas of your body. These sensors measure your skin temperature, brain waves, breathing, and muscle activity. You can see these readings on a monitor. Then you practice changing your thoughts, behaviors, or emotions to help control your body’s responses. Over time, you can learn to change them without using the monitor.
Progressive relaxation
This is another simple technique that you can do almost anywhere. Starting with your toes and feet, focus on tightening your muscles for a few moments and then releasing them. Continue with this process, working your way up your body, focusing on one group of muscles at a time.
Yoga
Yoga is an ancient practice rooted in Indian philosophy. The practice of yoga combines postures or movements with focused breathing and meditation. The postures are meant to increase strength and flexibility. Postures range from simple poses lying on the floor to more complex poses that may require years of practice. You can modify most yoga postures based on your own ability.
There are many different styles of yoga that range from slow to vigorous. If you are thinking about starting yoga, look for a teacher who can help you practice safely. Make sure to tell your teacher about any recent or past injuries.
Tai Chi
Tai chi was first practiced in ancient China for self-defense. Today, it is used mainly to improve health. It is a low-impact, gentle type of exercise that is safe for people of all ages.
There are many styles of tai chi, but all involve the same basic principles:
- Slow, relaxed movements. The movements in tai chi are slow, but your body is always moving.
- Careful postures. You hold specific postures as you move your body.
- Concentration. You are encouraged to put aside distracting thoughts while you practice.
- Focused breathing. During tai chi, your breathing should be relaxed and deep.
If you are interested in tai chi for stress relief, you may want to start with a class. For many people, it is the easiest way to learn the proper movements. You can also find books and videos about tai chi.
Exercise
Getting physical activity every day is one of the easiest and best ways to cope with stress. When you exercise, your brain releases chemicals that make you feel good. It can also help you release built-up energy or frustration. Find something you enjoy, whether it is walking, cycling, softball, swimming, or dancing, and do it for at least 30 minutes on most days.
Functional dyspepsia medication
Some medicines may help manage symptoms of functional dyspepsia. They include:
Gas-relieving medicine
Gas-relieving medicine that are available without a prescription. An ingredient called simethicone may provide some relief by reducing intestinal gas. Simethicone is used to relieve painful pressure caused by excess gas in the stomach and intestines. Simethicone is a silicone compound that functions as a non-systemic surfactant, decreasing the surface tension of gas bubbles in the gastrointestinal (GI) tract 6. This action results in coalescence and dispersion of the gas bubbles allowing their removal from the gastrointestinal tract as flatulence or belching. Simethicone causes the gas bubbles to accumulate and therefore pass more easily either through the upper gastrointestinal or lower gastrointestinal opening 6. Simethicone does not appear to reduce the actual production of gas in the GI tract 7 Examples of gas-relieving medicines include Mylanta, Maalox, Alka-Seltzer Anti-Gas and Gas-X.
Medications to reduce acid production
Acid blockers also called H2-receptor blockers (Histamine Type-2 Receptor Antagonists) reduce the amount of stomach acid released into your digestive tract, which relieves ulcer pain and encourages healing. Available by prescription or over the counter, acid blockers include the medications famotidine (Pepcid AC), cimetidine (Tagamet HB) and nizatidine (Axid AR). Stronger versions of these medicines also are available by prescription.
Medications that block acid production and promote healing. Proton pump inhibitors (PPIs) reduce stomach acid by blocking the action of the parts of cells that produce acid. These drugs include the prescription and over-the-counter medications omeprazole (Prilosec, Zegerid), lansoprazole (Prevacid), rabeprazole (Aciphex), esomeprazole (Nexium), dexlansoprazole (Dexilant) and pantoprazole (Protonix). There are very few medical differences between these drugs. However, long-term use of proton pump inhibitors (PPIs), particularly at high doses, may increase your risk of hip, wrist and spine fracture. Ask your doctor whether a calcium supplement may reduce this risk.
In patients whose symptoms improve with proton pump inhibitors (PPIs), PPI (proton pump inhibitor) therapy should be discontinued every 6 to 12 months to reduce the long-term risk of therapy. The standard dosages of orally administered proton pump inhibitors are as follows:
- Lansoprazole 30 mg daily
- Omeprazole 20 mg daily
- Pantoprazole 40 mg daily
- Rabeprazole 20 mg daily
- Esomeprazole 20 mg daily
Proton pump inhibitors (PPIs) require a meal to activate them. You should eat a meal within 30 minutes to 1 hour after taking this medication for the acid suppression therapy to work most effectively. Waiting later than this time can decrease the positive effect of this medication. This might delay healing or even result in the failure of the ulcer to heal.
Antibiotic medications to kill H. pylori
If H. pylori is found in your digestive tract, your doctor may recommend a combination of antibiotics to kill the bacterium. These may include amoxicillin (Amoxil), clarithromycin (Biaxin), metronidazole (Flagyl), tinidazole (Tindamax), tetracycline and levofloxacin. The antibiotics used will be determined by where you live and current antibiotic resistance rates. You’ll likely need to take antibiotics for two weeks, as well as additional medications to reduce stomach acid, including a proton pump inhibitor (PPI) and possibly bismuth subsalicylate (Pepto-Bismol). To find out if the antibiotics worked, your doctor may recommend testing you for H. pylori at least 4 weeks after you’ve finished taking the antibiotics 12. If you still have an H. pylori infection, your doctor may prescribe a different combination of antibiotics and other medicines to treat the infection. Making sure that all of the H. pylori bacteria have been killed is important.
Low-dose antidepressants
Your doctor may prescribe low doses of tricyclic antidepressants (TCAs) and antidepressants known as selective serotonin reuptake inhibitors (SSRIs). These medicines may inhibit the activity of neurons that control intestinal pain.
In patients whose symptoms are refractory to the initial 8 weeks of proton pump inhibitor (PPI) therapy, a tricyclic antidepressant (TCA) is suggested 9. For those who respond partially to proton pump inhibitors (PPIs), tricyclic antidepressants (TCAs) may be given in combination therapy with PPIs. The following approach is recommended:
- Start with either of the following low-dose tricyclic antidepressants (TCAs) at night:
- Amitriptyline 10 mg 10
- Nortriptyline 10 mg
- Desipramine 25 mg
- Doses may be titrated up modestly according to symptoms.
- Higher doses may cause sedation and still not be more effective.
- Tricyclic antidepressant (TCA) is initially administered for 8 to 12 weeks and then continued for 6 months if the patient responds appropriately.
- Doses are slowly tapered.
- Tricyclic antidepressants (TCAs) may be resumed if symptoms recur.
Mirtazapine has shown benefits in patients with functional dyspepsia and the associated weight loss that may be due to a central mechanism of action 11. As with tricyclic antidepressants (TCAs), an initial low dose is recommended. The dose is titrated from 7.5 mg an hour before bedtime to 45 mg daily.
Prokinetics
These medicines help your stomach empty faster and tighten the valve between your stomach and esophagus (the lower esophageal sphincter). This helps to reduce upper abdominal pain. Prescription prokinetics include bethanechol (Urecholine) and metoclopramide (Reglan). Metoclopramide 5 to 10 mg is usually given one-half hour before meals and at night.
A 4 to 8 week course is recommended and may be repeated when symptoms recur. However, in some patients, adverse effects may lead to discontinuation of therapy 8.
Medicines to relieve nausea or anti-emetics
If you feel like throwing up after eating, anti-emetics may help. These include promethazine, prochlorperazine and meclizine.
Psychological therapy
Patients with functional dyspepsia score higher than those without gastrointestinal symptoms for depression, anxiety, and somatization, which are more strongly associated with decreased quality of life than are the clinical symptoms themselves 13, 14. Your doctor may recommend a type of psychological therapy called “talk therapy” also called psychotherapy to help treat anxiety and depression that may be causing your indigestion. If stress is causing your indigestion, your doctor may recommend ways to help you reduce your stress, such as meditation, relaxation exercises or counseling. Talk therapy can also help you learn how to reduce your stress. A counselor or therapist can show you relaxation techniques to help you cope with your symptoms 15. You may also learn ways to reduce stress to help manage your symptoms.
Lifestyle and home remedies
Your doctor may recommend lifestyle changes to help you control your functional dyspepsia.
You are more likely to get indigestion (dyspepsia) if you:
- drink too many alcoholic beverages
- drink too much coffee or too many drinks containing caffeine
- eat too fast or too much during a meal
- eat spicy, fatty, or greasy foods
- eat foods that contain a lot of acid, such as tomatoes, tomato products, and oranges
- feel stressed
- have certain health problems or digestive tract diseases
- smoke
- take certain medicines e.g., nonsteroidal anti-inflammatory drugs (NSAIDs), antibiotics
In addition to making changes in what you eat and drink, you can help prevent indigestion by making lifestyle changes such as: 58
- avoiding exercise right after eating
- chewing food carefully and completely
- losing weight
- not eating late-night snacks
- not taking a lot of nonsteroidal anti-inflammatory drugs
- quitting smoking
- trying to reduce stress in your life
- waiting 2 to 3 hours after eating before you lie down
Get enough sleep
Getting a good night’s sleep can help you think more clearly and have more energy. This will make it easier to handle any problems that crop up. Aim for about 7 to 9 hours each night.
Maintain a healthy diet
Eating healthy foods helps fuel your body and mind. Skip the high-sugar snack foods and load up on vegetables, fruits, whole grains, low-fat or nonfat dairy, and lean proteins.
Avoid stressful situations
When you can, remove yourself from the source of stress. For example, if your family squabbles during the holidays, give yourself a breather and go out for a walk or drive.
Do something you enjoy
When stress has you down, do something you enjoy to help pick you up. It could be as simple as reading a good book, listening to music, watching a favorite movie, or having dinner with a friend. Or, take up a new hobby or class. Whatever you choose, try to do at least one thing a day that’s just for you.
Complementary and alternative treatments
People with functional dyspepsia often turn to complementary and alternative medicines to help them cope. Further studies are needed before complementary and alternative medicines can be recommended. But they may provide some symptom relief when used with other approaches suggested by your health care provider.
If you’re interested in complementary and alternative treatments, talk to your doctor about:
- Herbal supplements. A combination of peppermint and caraway oils may offer some benefit for functional dyspepsia. Together, they relieved pain symptoms in a l-week trial. Iberogast contains extracts of nine herbs. It may relieve gastrointestinal spasms and improve the intestine’s ability to move food. A Japanese herbal remedy called rikkunshito (a kampo herbal medicine) also may be helpful 18. Researchers found it improved abdominal pain, heartburn and bloating better than placebo 59, 60. A placebo is a treatment with no therapeutic effect that looks the same as, and is given the same way as, the medicine or treatment being tested in a study. Preliminary studies have suggested that rikkunshito (TJ-43, Tsumura and Co) promotes gastric accommodation and expedites gastric emptying time 61, 62, 63. Three randomized control trials have also demonstrated that rikkunshito (a kampo herbal medicine) improves dyspepsia symptoms, including abdominal pain, postprandial fullness, and bloating 64, 65, 60. Artichoke leaf extract may reduce symptoms of functional dyspepsia.
Functional dyspepsia prognosis
Functional dyspepsia is a benign common gastrointestinal disorder 25. Functional dyspepsia is relapsing and remitting 66. In a European study of patients with functional dyspepsia, dyspepsia symptoms recurred within 3 months in 20% of the patients whose symptoms had disappeared after 4 weeks of treatment with a proton pump inhibitor (PPI) or placebo 67. Similarly, in a Japanese study of patients with functional dyspepsia whose symptoms improved with a prokinetic drug called acotiamide, functional dyspepsia was found to have recurred in 25% of the patients at 1 year 68.
Population studies have shown that 15% to 20% of patients have persistent symptoms during extended follow-up, while 50% have complete resolution of symptoms 25. In a population-based cohort study in the United States of the impact of functional gastrointestinal disorders (FGIDs) on survival with over 30,000 person-years of follow-up, no association with overall survival was detected for dyspepsia, IBS, chronic diarrhea, or abdominal pain 69. Likewise, a population-based cohort study in the United Kingdom with over 84,000 person-years of follow-up also found that dyspepsia did not increase mortality 70. Taken together, these studies indicate that functional dyspepsia does not appear to increase mortality.
- Indigestion (Dyspepsia). https://generalsurgery.ucsf.edu/conditions–procedures/indigestion.aspx[↩]
- Talley NJ, Ford AC. Functional Dyspepsia. N Engl J Med. 2015 Nov 5;373(19):1853-63. doi: 10.1056/NEJMra1501505[↩]
- Longstreth GF, Lacy BE. Approach to the adult with dyspepsia. https://www.uptodate.com/contents/approach-to-the-adult-with-dyspepsia[↩]
- Update on the Evaluation and Management of Functional Dyspepsia. Am Fam Physician. 2011 Mar 1;83(5):547-552. https://www.aafp.org/afp/2011/0301/p547.html[↩]
- Dickerson LM, King DE. Evaluation and management of nonulcer dyspepsia. Am Fam Physician. 2004;70(1):109.[↩]
- Ingold CJ, Akhondi H. Simethicone. [Updated 2023 Jul 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555997[↩][↩][↩][↩]
- Voepel-Lewis TD, Malviya S, Burke C, D’Agostino R, Hadden SM, Siewert M, Tait AR. Evaluation of simethicone for the treatment of postoperative abdominal discomfort in infants. J Clin Anesth. 1998 Mar;10(2):91-4. doi: 10.1016/s0952-8180(97)00249-3[↩][↩]
- Moayyedi P, Lacy BE, Andrews CN, Enns RA, Howden CW, Vakil N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am J Gastroenterol. 2017 Jul;112(7):988-1013. doi: 10.1038/ajg.2017.154. Epub 2017 Jun 20. Erratum in: Am J Gastroenterol. 2017 Sep;112(9):1484.[↩][↩][↩][↩]
- Lacy BE, Saito YA, Camilleri M, Bouras E, DiBaise JK, Herrick LM, Szarka LA, Tilkes K, Zinsmeister AR, Talley NJ. Effects of Antidepressants on Gastric Function in Patients with Functional Dyspepsia. Am J Gastroenterol. 2018 Feb;113(2):216-224. doi: 10.1038/ajg.2017.458[↩][↩]
- Talley NJ, Locke GR, Saito YA, Almazar AE, Bouras EP, Howden CW, Lacy BE, DiBaise JK, Prather CM, Abraham BP, El-Serag HB, Moayyedi P, Herrick LM, Szarka LA, Camilleri M, Hamilton FA, Schleck CD, Tilkes KE, Zinsmeister AR. Effect of Amitriptyline and Escitalopram on Functional Dyspepsia: A Multicenter, Randomized Controlled Study. Gastroenterology. 2015 Aug;149(2):340-9.e2. doi: 10.1053/j.gastro.2015.04.020[↩][↩]
- Carbone F, Vanuytsel T, Tack J. The effect of mirtazapine on gastric accommodation, gastric sensitivity to distention, and nutrient tolerance in healthy subjects. Neurogastroenterol Motil. 2017 Dec;29(12). doi: 10.1111/nmo.13146[↩][↩]
- Vakil NB. Peptic ulcer disease: treatment and secondary prevention. https://www.uptodate.com/contents/peptic-ulcer-disease-treatment-and-secondary-prevention[↩][↩]
- Madisch A, Andresen V, Enck P, Labenz J, Frieling T, Schemann M. The Diagnosis and Treatment of Functional Dyspepsia. Dtsch Arztebl Int. 2018 Mar 30;115(13):222-232. doi: 10.3238/arztebl.2018.0222[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Enck P, Azpiroz F, Boeckxstaens G, Elsenbruch S, Feinle-Bisset C, Holtmann G, Lackner JM, Ronkainen J, Schemann M, Stengel A, Tack J, Zipfel S, Talley NJ. Functional dyspepsia. Nat Rev Dis Primers. 2017 Nov 3;3:17081. doi: 10.1038/nrdp.2017.81[↩][↩][↩][↩][↩][↩]
- Soo S, Moayyedi P, Deeks JJ, Delaney B, Lewis M, Forman D. WITHDRAWN: Psychological interventions for non-ulcer dyspepsia. Cochrane Database Syst Rev. 2011 Feb 16;2011(2):CD002301. doi: 10.1002/14651858.CD002301.pub5[↩][↩]
- Black CJ, Paine PA, Agrawal A, Aziz I, Eugenicos MP, Houghton LA, Hungin P, Overshott R, Vasant DH, Rudd S, Winning RC, Corsetti M, Ford AC. British Society of Gastroenterology guidelines on the management of functional dyspepsia. Gut. 2022 Sep;71(9):1697-1723. doi: 10.1136/gutjnl-2022-327737[↩]
- Li H, Page AJ. Altered Vagal Signaling and Its Pathophysiological Roles in Functional Dyspepsia. Front Neurosci. 2022 Apr 22;16:858612. doi: 10.3389/fnins.2022.858612[↩]
- Miwa H, Nagahara A, Asakawa A, Arai M, Oshima T, Kasugai K, Kamada K, Suzuki H, Tanaka F, Tominaga K, Futagami S, Hojo M, Mihara H, Higuchi K, Kusano M, Arisawa T, Kato M, Joh T, Mochida S, Enomoto N, Shimosegawa T, Koike K. Evidence-based clinical practice guidelines for functional dyspepsia 2021. J Gastroenterol. 2022 Feb;57(2):47-61. doi: 10.1007/s00535-021-01843-7[↩][↩]
- Wauters L, Dickman R, Drug V, et al. United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) consensus on functional dyspepsia. United European Gastroenterol J. 2021 Apr;9(3):307-331. doi: 10.1002/ueg2.12061[↩]
- Harer KN, Hasler WL. Functional Dyspepsia: A Review of the Symptoms, Evaluation, and Treatment Options. Gastroenterol Hepatol (N Y). 2020 Feb;16(2):66-74. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8132673[↩][↩][↩]
- Sperber AD, Bangdiwala SI, Drossman DA, Ghoshal UC, Simren M, Tack J, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome foundation global study. Gastroenterology. 2020;S0016‐5085:30487. 10.1053/j.gastro.2020.04.014[↩]
- Park JK, Huh KC, Shin CM, Lee H, Yoon YH, Song KH, Min BH, Choi KD; Korean Society of Neurogastroenterology and Motility. [Current issues in functional dyspepsia]. Korean J Gastroenterol. 2014 Sep 25;64(3):133-41. Korean. doi: 10.4166/kjg.2014.64.3.133[↩]
- Functional Dyspepsia. https://aboutgimotility.org/learn-about-gi-motility/disorders-of-the-stomach/functional-dyspepsia[↩]
- Functional dyspepsia. https://www.mayoclinic.org/diseases-conditions/functional-dyspepsia/symptoms-causes/syc-20375709[↩]
- Francis P, Zavala SR. Functional Dyspepsia. [Updated 2023 Aug 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554563[↩][↩][↩][↩][↩][↩]
- Dyspepsia. https://iffgd.org/gi-disorders/upper-gi-disorders/dyspepsia[↩][↩][↩]
- Stanghellini V, Chan FK, Hasler WL, Malagelada JR, Suzuki H, Tack J, Talley NJ. Gastroduodenal Disorders. Gastroenterology. 2016 May;150(6):1380-92. doi: 10.1053/j.gastro.2016.02.011[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Talley NJ, Walker MM, Holtmann G. Functional dyspepsia. Curr Opin Gastroenterol. 2016 Nov;32(6):467-473. doi: 10.1097/MOG.0000000000000306[↩][↩]
- Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Functional Disorders: Children and Adolescents. Gastroenterology. 2016 Feb 15:S0016-5085(16)00181-5. doi: 10.1053/j.gastro.2016.02.015[↩][↩][↩][↩][↩]
- Labenz J, Koop H. Gastroösophageale Refluxkrankheit – was tun, wenn PPI nicht ausreichend wirksam, verträglich oder erwünscht sind? [Gastro-Oesophageal Reflux Disease – How to Manage if PPI are not Sufficiently Effective, not Tolerated, or not Wished?]. Dtsch Med Wochenschr. 2017 Mar;142(5):356-366. German. doi: 10.1055/s-0042-121021[↩]
- Van Oudenhove L, Aziz Q. The role of psychosocial factors and psychiatric disorders in functional dyspepsia. Nat Rev Gastroenterol Hepatol. 2013 Mar;10(3):158-67. doi: 10.1038/nrgastro.2013.10[↩][↩]
- Jones MP, Tack J, Van Oudenhove L, Walker MM, Holtmann G, Koloski NA, Talley NJ. Mood and Anxiety Disorders Precede Development of Functional Gastrointestinal Disorders in Patients but Not in the Population. Clin Gastroenterol Hepatol. 2017 Jul;15(7):1014-1020.e4. doi: 10.1016/j.cgh.2016.12.032[↩][↩]
- Pinto-Sanchez MI, Ford AC, Avila CA, Verdu EF, Collins SM, Morgan D, Moayyedi P, Bercik P. Anxiety and Depression Increase in a Stepwise Manner in Parallel With Multiple FGIDs and Symptom Severity and Frequency. Am J Gastroenterol. 2015 Jul;110(7):1038-48. doi: 10.1038/ajg.2015.128[↩][↩]
- Talley NJ, Silverstein MD, Agréus L, Nyrén O, Sonnenberg A, Holtmann G. AGA technical review: evaluation of dyspepsia. American Gastroenterological Association. Gastroenterology. 1998 Mar;114(3):582-95. doi: 10.1016/s0016-5085(98)70542-6[↩][↩]
- Talley NJ, Stanghellini V, Heading RC, Koch KL, Malagelada JR, Tytgat GN. Functional gastroduodenal disorders. Gut. 1999 Sep;45 Suppl 2(Suppl 2):II37-42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1766695/pdf/v045p0II37.pdf[↩][↩]
- Bortolotti M, Bolondi L, Santi V, Sarti P, Brunelli F, Barbara L. Patterns of gastric emptying in dysmotility-like dyspepsia. Scand J Gastroenterol. 1995 May;30(5):408-10. doi: 10.3109/00365529509093299[↩]
- Kim DY, Delgado-Aros S, Camilleri M, Samsom M, Murray JA, O’Connor MK, Brinkmann BH, Stephens DA, Lighvani SS, Burton DD. Noninvasive measurement of gastric accommodation in patients with idiopathic nonulcer dyspepsia. Am J Gastroenterol. 2001 Nov;96(11):3099-105. doi: 10.1111/j.1572-0241.2001.05264.x[↩]
- Coffin B, Azpiroz F, Guarner F, Malagelada JR. Selective gastric hypersensitivity and reflex hyporeactivity in functional dyspepsia. Gastroenterology. 1994 Nov;107(5):1345-51. doi: 10.1016/0016-5085(94)90536-3[↩]
- Troncon LE, Thompson DG, Ahluwalia NK, Barlow J, Heggie L. Relations between upper abdominal symptoms and gastric distension abnormalities in dysmotility like functional dyspepsia and after vagotomy. Gut. 1995 Jul;37(1):17-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1382761/pdf/gut00526-0033.pdf[↩]
- Mertz H, Fullerton S, Naliboff B, Mayer EA. Symptoms and visceral perception in severe functional and organic dyspepsia. Gut. 1998 Jun;42(6):814-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1727129/pdf/v042p00814.pdf[↩]
- Simrén M, Törnblom H, Palsson OS, van Tilburg MAL, Van Oudenhove L, Tack J, Whitehead WE. Visceral hypersensitivity is associated with GI symptom severity in functional GI disorders: consistent findings from five different patient cohorts. Gut. 2018 Feb;67(2):255-262. doi: 10.1136/gutjnl-2016-312361[↩]
- Mearin F, Cucala M, Azpiroz F, Malagelada JR. The origin of symptoms on the brain-gut axis in functional dyspepsia. Gastroenterology. 1991 Oct;101(4):999-1006. doi: 10.1016/0016-5085(91)90726-2[↩]
- Grundy D, Al-Chaer ED, Aziz Q, Collins SM, Ke M, Taché Y, Wood JD. Fundamentals of neurogastroenterology: basic science. Gastroenterology. 2006 Apr;130(5):1391-411. doi: 10.1053/j.gastro.2005.11.060[↩]
- Bouin M, Lupien F, Riberdy-Poitras M, Poitras P. Tolerance to gastric distension in patients with functional dyspepsia: modulation by a cholinergic and nitrergic method. Eur J Gastroenterol Hepatol. 2006 Jan;18(1):63-8. doi: 10.1097/00042737-200601000-00011[↩]
- Lee KJ, Demarchi B, Demedts I, Sifrim D, Raeymaekers P, Tack J. A pilot study on duodenal acid exposure and its relationship to symptoms in functional dyspepsia with prominent nausea. Am J Gastroenterol. 2004 Sep;99(9):1765-73. doi: 10.1111/j.1572-0241.2004.30822.x[↩]
- Samsom M, Verhagen MA, vanBerge Henegouwen GP, Smout AJ. Abnormal clearance of exogenous acid and increased acid sensitivity of the proximal duodenum in dyspeptic patients. Gastroenterology. 1999 Mar;116(3):515-20. doi: 10.1016/s0016-5085(99)70171-x[↩]
- Hammer J, Führer M, Pipal L, Matiasek J. Hypersensitivity for capsaicin in patients with functional dyspepsia. Neurogastroenterol Motil. 2008 Feb;20(2):125-33. doi: 10.1111/j.1365-2982.2007.00997.x[↩]
- Feinle-Bisset C. Upper gastrointestinal sensitivity to meal-related signals in adult humans – relevance to appetite regulation and gut symptoms in health, obesity and functional dyspepsia. Physiol Behav. 2016 Aug 1;162:69-82. doi: 10.1016/j.physbeh.2016.03.021[↩]
- Park SY, Acosta A, Camilleri M, Burton D, Harmsen WS, Fox J, Szarka LA. Gastric Motor Dysfunction in Patients With Functional Gastroduodenal Symptoms. Am J Gastroenterol. 2017 Nov;112(11):1689-1699. doi: 10.1038/ajg.2017.264[↩]
- Farré R, Vanheel H, Vanuytsel T, Masaoka T, Törnblom H, Simrén M, Van Oudenhove L, Tack JF. In functional dyspepsia, hypersensitivity to postprandial distention correlates with meal-related symptom severity. Gastroenterology. 2013 Sep;145(3):566-73. doi: 10.1053/j.gastro.2013.05.018[↩]
- Ye Y, Wang XR, Zheng Y, Yang JW, Yang NN, Shi GX, Liu CZ. Choosing an Animal Model for the Study of Functional Dyspepsia. Can J Gastroenterol Hepatol. 2018 Feb 12;2018:1531958. doi: 10.1155/2018/1531958[↩]
- Du L, Shen J, Kim JJ, Yu Y, Ma L, Dai N. Corrigendum: Increased Duodenal Eosinophil Degranulation in Patients with Functional Dyspepsia: A Prospective Study. Sci Rep. 2017 Apr 7;7:46121. doi: 10.1038/srep46121. Erratum for: Sci Rep. 2016 Oct 06;6:34305[↩]
- Rahman MM, Ghoshal UC, Sultana S, Kibria MG, Sultana N, Khan ZA, Ahmed F, Hasan M, Ahmed T, Sarker SA. Long-Term Gastrointestinal Consequences are Frequent Following Sporadic Acute Infectious Diarrhea in a Tropical Country: A Prospective Cohort Study. Am J Gastroenterol. 2018 Sep;113(9):1363-1375. doi: 10.1038/s41395-018-0208-3[↩]
- Vanner S, Greenwood-Van Meerveld B, Mawe G, Shea-Donohue T, Verdu EF, Wood J, Grundy D. Fundamentals of Neurogastroenterology: Basic Science. Gastroenterology. 2016 Feb 18:S0016-5085(16)00184-0. doi: 10.1053/j.gastro.2016.02.018[↩]
- Vanuytsel T, van Wanrooy S, Vanheel H, Vanormelingen C, Verschueren S, Houben E, Salim Rasoel S, Tόth J, Holvoet L, Farré R, Van Oudenhove L, Boeckxstaens G, Verbeke K, Tack J. Psychological stress and corticotropin-releasing hormone increase intestinal permeability in humans by a mast cell-dependent mechanism. Gut. 2014 Aug;63(8):1293-9. doi: 10.1136/gutjnl-2013-305690[↩]
- Dibaise JK, Islam RS, Dueck AC, Roarke MC, Crowell MD. Psychological distress in Rome III functional dyspepsia patients presenting for testing of gastric emptying. Neurogastroenterol Motil. 2016 Feb;28(2):196-205. doi: 10.1111/nmo.12709[↩]
- Duncanson K, Burns G, Pryor J, Keely S, Talley NJ. Mechanisms of Food-Induced Symptom Induction and Dietary Management in Functional Dyspepsia. Nutrients. 2021 Mar 28;13(4):1109. doi: 10.3390/nu13041109[↩]
- Treatment of Indigestion. https://www.niddk.nih.gov/health-information/digestive-diseases/indigestion-dyspepsia/treatment[↩]
- Tominaga K, Arakawa T. Kampo medicines for gastrointestinal tract disorders: a review of basic science and clinical evidence and their future application. J Gastroenterol. 2013 Apr;48(4):452-62. doi: 10.1007/s00535-013-0788-z[↩]
- Tominaga K, Sakata Y, Kusunoki H, Odaka T, Sakurai K, Kawamura O, Nagahara A, Takeuchi T, Fujikawa Y, Oshima T, Kato M, Furuta T, Murakami K, Chiba T, Miwa H, Kinoshita Y, Higuchi K, Kusano M, Iwakiri R, Fujimoto K, Tack JF, Arakawa T. Rikkunshito simultaneously improves dyspepsia correlated with anxiety in patients with functional dyspepsia: A randomized clinical trial (the DREAM study). Neurogastroenterol Motil. 2018 Jul;30(7):e13319. doi: 10.1111/nmo.13319[↩][↩]
- Hayakawa T, Arakawa T, Kase Y, Akiyama S, Ishige A, Takeda S, Sasaki H, Uno H, Fukuda T, Higuchi K, Kobayashi K. Liu-Jun-Zi-Tang, a kampo medicine, promotes adaptive relaxation in isolated guinea pig stomachs. Drugs Exp Clin Res. 1999;25(5):211-8.[↩]
- Kido T, Nakai Y, Kase Y, Sakakibara I, Nomura M, Takeda S, Aburada M. Effects of rikkunshi-to, a traditional Japanese medicine, on the delay of gastric emptying induced by N(G)-nitro-L-arginine. J Pharmacol Sci. 2005 Jun;98(2):161-7. doi: 10.1254/jphs.fpj04056x[↩]
- Tominaga K, Kido T, Ochi M, Sadakane C, Mase A, Okazaki H, Yamagami H, Tanigawa T, Watanabe K, Watanabe T, Fujiwara Y, Oshitani N, Arakawa T. The Traditional Japanese Medicine Rikkunshito Promotes Gastric Emptying via the Antagonistic Action of the 5-HT(3) Receptor Pathway in Rats. Evid Based Complement Alternat Med. 2011;2011:248481. doi: 10.1093/ecam/nep173[↩]
- Togawa K, Matsuzaki J, Kobayakawa M, Fukushima Y, Suzaki F, Kasugai K, Nishizawa T, Naito Y, Hayakawa T, Kamiya T, Andoh T, Yoshida H, Tokura Y, Nagata H, Mori M, Kato K, Hosoda H, Takebayashi T, Miura S, Uemura N, Joh T, Hibi T, Suzuki H. Association of baseline plasma des-acyl ghrelin level with the response to rikkunshito in patients with functional dyspepsia. J Gastroenterol Hepatol. 2016 Feb;31(2):334-41. doi: 10.1111/jgh.13074[↩]
- Tominaga K, Iwakiri R, Fujimoto K, Fujiwara Y, Tanaka M, Shimoyama Y, Umegaki E, Higuchi K, Kusano M, Arakawa T; GERD 4 Study Group. Rikkunshito improves symptoms in PPI-refractory GERD patients: a prospective, randomized, multicenter trial in Japan. J Gastroenterol. 2012 Mar;47(3):284-92. doi: 10.1007/s00535-011-0488-5[↩]
- Talley NJ, Ford AC. Functional Dyspepsia. N Engl J Med. 2016 Mar 3;374(9):896. doi: 10.1056/NEJMc1515497[↩]
- Meineche-Schmidt V, Talley NJ, Pap A, Kordecki H, Schmid V, Ohlsson L, Wahlqvist P, Wiklund I, Bolling-Sternevald E. Impact of functional dyspepsia on quality of life and health care consumption after cessation of antisecretory treatment. A multicentre 3-month follow-up study. Scand J Gastroenterol. 1999 Jun;34(6):566-74. doi: 10.1080/003655299750026010[↩]
- Shinozaki S, Osawa H, Sakamoto H, Hayashi Y, Miura Y, Lefor AK, Yamamoto H. Adherence to an acotiamide therapeutic regimen improves long-term outcomes in patients with functional dyspepsia. J Gastrointestin Liver Dis. 2017 Dec;26(4):345-350. doi: 10.15403/jgld.2014.1121.264.ski[↩]
- Chang JY, Locke GR 3rd, McNally MA, Halder SL, Schleck CD, Zinsmeister AR, Talley NJ. Impact of functional gastrointestinal disorders on survival in the community. Am J Gastroenterol. 2010 Apr;105(4):822-32. doi: 10.1038/ajg.2010.40[↩]
- Ford AC, Forman D, Bailey AG, Axon AT, Moayyedi P. Effect of dyspepsia on survival: a longitudinal 10-year follow-up study. Am J Gastroenterol. 2012 Jun;107(6):912-21. doi: 10.1038/ajg.2012.69[↩]





{kind=link}