
What is SSRI
SSRIs is short for selective serotonin reuptake inhibitors, which are a class of antidepressant medications that works by increasing serotonin levels in your brain, that are commonly prescribed to treat depression, anxiety disorders, obsessive-compulsive disorder (OCD), panic disorders, and eating disorder bulimia nervosa and other mental health conditions 1, 2. Selective serotonin reuptake inhibitors (SSRIs) work by blocking the reabsorption (reuptake) of serotonin, a neurotransmitter (a chemical messenger) in your brain, which increases the amount of serotonin available to nerve cells (neurons) in the brain which is associated with their antidepressant effect. Serotonin also known as 5-hydroxytryptamine or 5-HT, is one of the a biochemical messengers and regulators, synthesized from the essential amino acid L-Tryptophan that nerve cells (neurons) in your brain use to communicate 3, 4, 5. Raising serotonin levels can help regulate mood, appetite, digestion, sleep, and many other bodily functions. Selective serotonin reuptake inhibitors (SSRIs) include drugs such as citalopram, escitalopram, fluoxetine, paroxetine, and sertraline.
SSRIs drugs include:
- Citalopram (Celexa)
- Escitalopram (Lexapro)
- Fluoxetine (Prozac®, Prozac Weekly®, Rapuflux®, Selfemra®, and Sarafem®)
- Paroxetine (Paxil®, Aropax®, Brisdelle®, Pexeva® and Seroxat®)
- Sertraline (Zoloft)
- Vilazodone (Viibryd)
SSRIs common uses:
- Major depressive disorder
- Anxiety disorders, including generalized anxiety disorder (GAD) and panic disorder
- Severe phobias such as agoraphobia and social anxiety disorder (social phobia)
- Obsessive-compulsive disorder (OCD)
- Post-traumatic stress disorder (PTSD)
- Bulimia nervosa
- Bipolar depression 6
SSRIs can sometimes be used to treat other conditions, such as:
SSRIs are only available orally and come in multiple forms, including tablets, capsules, or liquid suspension/solution. There are currently no parenteral (IV, IM, SubQ), rectal, or other forms of SSRIs. SSRI administration is typically once-daily medication in the morning or nighttime. Except for vilazodone, SSRIs may be taken without regard to food. Take vilazodone with food 7.
SSRIs are usually taken in tablet form. When they’re prescribed, you’ll start on the lowest possible dose thought necessary to improve your symptoms. SSRIs usually need to be taken for 2 to 4 weeks before the benefit is felt. You may experience mild side effects early on, but it’s important that you don’t stop taking the medicine. These effects will usually wear off quickly.
If you take an SSRI for 4 to 6 weeks without feeling any benefit, speak to your doctor or mental health specialist. Your doctor or mental health specialist may recommend increasing your dose or trying an alternative antidepressant. This is because SSRIs differ in how well they block serotonin reuptake and in how quickly they break down and are cleared from the body.
An SSRI that is best for you depends on several factors, such as your symptoms and any other health conditions you may have.
A course of treatment usually continues for at least 6 months after you feel better, although longer courses are sometimes recommended and some people with recurrent problems may be advised to take them indefinitely.
SSRIs also need to be used with caution if you have certain underlying health problems, including diabetes, epilepsy and kidney disease.
Some SSRIs can react unpredictably with other medicines, including some over-the-counter painkillers and herbal remedies, such as St John’s wort. Always read the information leaflet that comes with your SSRI medicine to check if there are any medicines you need to avoid.
SSRIs are generally considered safe and effective, but they can cause side effects, including:
- Upset stomach, vomiting or diarrhea.
- Insomnia
- Headaches
- Sexual dysfunction
- Sweating
- Sleepiness or trouble sleeping.
- Dry mouth.
- Nervousness, anxiety or restlessness.
- Shakiness.
- Sexual problems, such as lessened sexual desire, trouble reaching orgasm or trouble getting and keeping an erection.
- Changes in appetite, leading to weight loss or weight gain.
Taking your SSRI with food may lessen the risk of an upset stomach. Also, so long as your SSRI medicien doesn’t keep you from sleeping, taking it at bedtime may lessen an upset stomach.
SSRIs are generally safe for most people. But some can cause safety issues. For example, citalopram can cause dangerous irregular heart rhythms if the dose is too high. The U.S. Food and Drug Administration (FDA) and the manufacturer recommend that the dose should be no more than 40 milligrams (mg) a day, but no more than 20 mg of citalopram a day for people over age 60.
Before you take an SSRI, talk with your doctor about:
- Interactions with other medicines and supplements. When taking an antidepressant, tell your doctor about any other prescription or nonprescription medicines, herbs, or other supplements you’re taking. Some antidepressants can interfere with the effectiveness of other medicines. Some antidepressants can cause dangerous reactions when combined with certain medicines or herbal supplements. For example, SSRIs may raise your risk of bleeding. The risk is higher when you also take other medicines that raise the risk of bleeding, for example, a nonsteroidal anti-inflammatory drug, such as aspirin or ibuprofen (Advil, Motrin IB, others), or warfarin (Jantoven) and other blood thinners.
- Serotonin syndrome. Rarely, an antidepressant can cause high levels of serotonin to build up in your body. Serotonin syndrome most often occurs when two medicines that raise the level of serotonin are combined. These include, for example, other antidepressants, some pain or headache medicines, and the herbal supplement St. John’s wort. Symptoms of serotonin syndrome include anxiety, being nervous or jittery, high fever, sweating, confusion, shaking, restlessness, lack of coordination, major changes in blood pressure, and a fast heartbeat. Get medical help right away if you have any of these symptoms.
- Antidepressants and pregnancy. Talk to your doctor about the risks and benefits of using specific antidepressants. Some antidepressants may harm your baby if you take them during pregnancy or while you’re breastfeeding. If you’re taking an antidepressant and you’re thinking about getting pregnant, talk with your doctor about the possible risks. Don’t stop taking your medicine without talking with your doctor first, as stopping puts you at risk.
- Suicide risk and antidepressants. Most antidepressants are generally safe. But the U.S. Food and Drug Administration (FDA) requires that all antidepressants carry boxed warnings, the strictest warnings for prescriptions. In some cases, children, teenagers and young adults under 25 may have an increase in suicidal thoughts or behavior when taking antidepressants. This may be more likely in the first few weeks after starting or when the dose is changed. Anyone taking an antidepressant should be watched closely for worsening depression or unusual behavior. If you or someone you know has suicidal thoughts when taking an antidepressant, call your doctor right away or get emergency help. Keep in mind that depression that’s not treated is a more concerning risk of suicide. And antidepressants may lessen suicide risk in the long run by improving mood for many people.
- Stopping treatment with SSRIs. SSRIs aren’t habit-forming. However, stopping antidepressant treatment suddenly or missing several doses can cause withdrawal-like symptoms. This is sometimes called discontinuation syndrome. Work with your doctor to slowly and safely lower your dose.
- SSRI withdrawal-like symptoms can include:
- Restlessness and anxiety.
- Nausea.
- Dizziness.
- Feeling sluggish or sleepy.
- Flu-like symptoms, such as chills, sweating and muscle aches.
- SSRI withdrawal-like symptoms can include:
Finding the right antidepressant
Different people may react differently to the same antidepressant. For example, one medicine may work better — or not as well — for you than for another person. Or you may have more, or fewer, side effects from taking a specific antidepressant than someone else does.
Traits passed down in your family play a role in how antidepressants affect you. If a relative responded well to a particular antidepressant, tell your doctor. This may be a good medicine for you to try first.
In some cases, results of special blood tests, where available, may offer clues about how your body may respond to a particular antidepressant. But other factors can affect your response to medicine. For example, people with a history of bipolar disorder typically aren’t given SSRIs for depression. That’s because SSRIs may worsen their symptoms.
When choosing an antidepressant, your doctor considers your symptoms, any health conditions you may have, other medicines you take and what has worked for you in the past.
It may take several weeks or more before an antidepressant is fully effective and for early side effects to ease up. Your doctor may recommend some dose changes or different antidepressants. With patience, you and your doctor can find a medicine that works well for you.
How selective serotonin reuptake inhibitor (SSRI) drugs work
The therapeutic actions of selective serotonin reuptake inhibitors (SSRIs) have their basis on increasing serotonin that researchers hypothesize as the cause of depression in the monoamine hypothesis 1. Serotonin is a neurotransmitter (a messenger chemical that carries signals between nerve cells in the brain). It’s thought to have a good influence on mood, emotion and sleep. After carrying a message, serotonin is usually reabsorbed by the nerve cells (known as “reuptake”). Selective serotonin reuptake inhibitors (SSRIs) work by blocking (“inhibiting”) the reuptake of serotonin in the brain, thereby increasing serotonin activity, meaning more serotonin is available to pass further messages between nearby nerve cells. SSRIs inhibit the serotonin transporter (SERT) at the presynaptic axon terminal. By inhibiting serotonin transporter (SERT), an increased amount of serotonin (5-hydroxytryptamine or 5HT) remains in the synaptic cleft and can stimulate postsynaptic receptors for a more extended period 8, 9, 10, 7. However, it would be too simplistic to say that depression and related mental health conditions are caused by low serotonin levels, but a rise in serotonin levels can improve symptoms and make people more responsive to other types of treatment, such as Cognitive Behavioral Therapy (CBT).
Unlike other classes of antidepressants, SSRIs have little effect on other neurotransmitters, such as dopamine or norepinephrine. SSRIs also have relatively fewer side effects than tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) due to fewer effects on adrenergic, cholinergic, and histaminergic receptors.
Selective serotonin reuptake inhibitor (SSRI) drugs uses
Selective serotonin reuptake inhibitors (SSRIs) are a widely used type of antidepressant (medicine used to treat clinical depression). SSRIs are usually the first choice medicine for depression because they generally have fewer side effects than most other types of antidepressant 1. SSRIs are mainly prescribed to treat depression, particularly persistent or severe cases, and are often used in combination with a talking therapy such as cognitive behavioral therapy (CBT).
Selective serotonin reuptake inhibitors (SSRIs) are approved for use in both adult and children 11, 12
SSRIs in use in the United States are:
- Fluoxetine
- Sertraline
- Paroxetine
- Fluvoxamine
- Citalopram
- Escitalopram
- Vilazodone
SSRIs currently with FDA labeled indications to treat the following conditions 1:
- Major depressive disorder
- Generalized anxiety disorder (GAD)
- Bulimia nervosa
- Bipolar depression 6
- Obsessive-compulsive disorder (OCD)
- Panic disorder
- Premenstrual dysphoric disorder (PMDD)
- Treatment-resistant depression
- Post-traumatic stress disorder (PTSD)
- Social anxiety disorder (social phobia)
- Severe phobias such as agoraphobia
Other off-label uses of SSRI include but are not limited to 13, 1:
- Binge eating disorder
- Body dysmorphic disorder
- Fibromyalgia
- Premature ejaculation
- Paraphilias: Paraphilia is an experience of recurring or intense sexual arousal to atypical objects, situations, fantasies, behaviors and/or targets (eg, children, corpses, animals) 14. Paraphilia has also been defined as a sexual interest in anything other than a legally consenting human partner. A total of eight Paraphilias are listed in the DSM V and include pedophilia, exhibitionism, voyeurism, sexual sadism, sexual masochism, frotteurism, fetishism, and transvestic fetishism 15. Although not innately pathological, a paraphilic disorder can evolve if paraphilia invokes harm, distress, or functional impairment on the lives of the affected individual or others.
- Pedophilia is any sexual activity with a prepubescent child, where the offender/patient is at least sixteen years of age, and the victim is at least five years younger 16.
- Exhibitionism is the exposure of an individual’s genitalia to unsuspecting strangers for sexual satisfaction 17
- Voyeurism is the viewing of an unsuspecting person engaging in disrobing or sexual activity 18.
- Sexual sadism is when sexual arousal is gained from inflicting mental or physical suffering on a nonconsenting person 19.
- Sexual masochism is the derivation of sexual arousal from being the recipient of physical or mental abuse and/or humiliation 20.
- Frotteurism is the touching of or rubbing against a nonconsenting person 21.
- Fetishism is the use of nonliving objects, most commonly shoes and undergarments, for sexual pleasure 22.
- Transvestic fetishism is the derivation of sexual arousal from cross-dressing or dressing in clothes of the opposite sex 23.
- Autism spectrum disorder (ASD) is a developmental disability that causes a complex range of behavioural symptoms.
- Raynaud phenomenon also called Raynaud’s disease is a condition that causes blood vessels in the extremities, particularly fingers and toes, to narrow in response to cold or stress, leading to reduced blood flow and a characteristic color change (white, then blue, then red)
- Vasomotor symptoms (hot flushes) associated with menopause.
SSRI Contraindications
SSRIs are contraindicated with the concurrent use of monoamine oxidase inhibitors (MAOIs), linezolid, and other medications that increase serotonin levels and could put patients at risk for life-threatening serotonin syndrome. Do not use SSRI if you have used an monoamine oxidase (MAO) inhibitor in the past 14 days. A dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate). Wait at least 14 days after stopping an monoamine oxidase (MAO) inhibitor before you take SSRI.
Paroxetine is contraindicated in pregnancy and is classified as category D/X due to its teratogenic effects in causing cardiovascular defects, specifically heart malformations if prescribed in the first trimester 24.
Pregnancy and SSRI
SSRIs can be prescribed if you’re pregnant, breastfeeding or under 18, but this depends if your doctor thinks that the benefits outweigh the risks. Talk to your doctor about what’s best for you or your child.
Babies of women who are taking an SSRI at the time of delivery may have some difficulties in the first few days of life. Reported symptoms include jitteriness, increased muscle tone, irritability, constant crying, changes in sleeping patterns, tremors, difficulty eating, and problems with breathing. Not every baby will experience these symptoms. For the SSRI medications, it is estimated that 10-30% of babies will be affected.
Some babies with symptoms of withdrawal may need to spend time in the neonatal intensive care unit (NICU) to receive additional care. However, in most cases the symptoms are mild and go away within two weeks. Reassuringly, there does not seem to be a dose-response relationship, which means that women who need a higher amount of medication to manage their anxiety are not expected to have babies who are at a higher risk for withdrawal.
SSRI side effects
Most people will only experience a few mild side effects when taking SSRIs. These can be troublesome at first, but they’ll generally improve with time 25, 26.
Common side effects of SSRIs can include 27, 28:
- feeling agitated, shaky or anxious
- diarrhea and feeling or being sick
- gastrointestinal distress
- dizziness
- blurred vision
- headache
- loss of libido (reduced sex drive)
- difficulty achieving orgasm during sex or masturbation
- in men, difficulty obtaining or maintaining an erection (erectile dysfunction)
- sleep disturbances
- weight changes
- xerostomia
SSRIs also have the potential to prolong the QT interval, which can lead to fatal arrhythmia, torsade de pointes. Citalopram has correlations with a longer QT duration, or QT prolongation than the other medications in this class 29, 30. Coagulopathy (bleeding disorder) also correlates with SSRI use 31. Although infrequent, as with all medications that increase serotonin activity, it is important to be aware of the risk of serotonin syndrome, particularly when prescribing multiple medications that may have serotonergic effects.
In 2004, the FDA issued a black box warning for SSRIs and other antidepressant medications due to a possible increased risk of suicidality among pediatric and young adult (up to age 25) populations 32, 33. The risk and benefits of initiating SSRI therapy on acutely suicidal patients must be weighed, keeping in mind that depression itself is a large risk factor for the risk of suicide (usually indicated by suicidal ideation or intent) and requires treatment.
SSRIs are brokendown (metabolized) by and have effects on the cytochrome P450 system. Fluoxetine, paroxetine, sertraline, citalopram, and escitalopram are inhibitors of CYP2D6. Fluoxetine and fluvoxamine are inhibitors of CYP2C19. Fluvoxamine is an inhibitor of CYP1A2 7.
You’ll usually need to see your doctor every few weeks when you first start taking SSRIs to discuss how well the medicine is working. You can also contact your doctor at any point if you experience any troublesome or persistent side effects.
SSRI Overdose
Symptoms of SSRI (selective serotonin reuptake inhibitors) overdose may include the following:
- dizziness
- drowsiness
- sweating
- agitation, hallucinations, fever, sweating, confusion, fast heartbeat, shivering, severe muscle stiffness or twitching, loss of coordination, nausea, vomiting, or diarrhea
- nausea
- vomiting
- uncontrollable shaking of a part of the body
- drowsiness
- fast, irregular, or pounding heartbeat
- memory loss
- confusion
- seizures
- coma (loss of consciousness)
- fast breathing
- bluish color around mouth, fingers, or fingernails
- muscle pain
- dark-colored urine.
Out of all the SSRIs, citalopram and escitalopram are more likely to cause overdose due to differences in their structures. Citalopram and escitalopram have an increased risk of heart toxicity due to QT prolongation, which can progress to serious arrhythmias such as Torsades de pointes, a type of very fast heart rhythm (tachycardia) that starts in your heart’s lower chambers (ventricles).
Serotonin syndrome
Serotonin syndrome also called serotonin toxicity is a potentially life threatening condition due to excessive serotonin in your body 34, 35. Serotonin syndrome most often occurs when two medicines that affect the body’s level of serotonin are taken together at the same time. The medicines cause too much serotonin to be released or to remain in the brain area. Serotonin syndrome (serotonin toxicity) can occur when you increase the dose of such a drug or add a new drug to your regimen. Certain illegal drugs and dietary supplements also are associated with serotonin syndrome. For example, you can develop serotonin syndrome if you take migraine medicines called triptans together with antidepressants called selective serotonin reuptake inhibitors (SSRIs), and selective serotonin/norepinephrine reuptake inhibitors (SSNRIs).
Serotonin syndrome symptoms and their severity vary from person to person. They can be mild to severe to even fatal.
If you’re taking a medication that affects serotonin and experience any of the following symptoms, call your doctor or visit an urgent or emergency care facility right away.
Mild symptoms
- Nervousness.
- Nausea, vomiting.
- Diarrhea.
- Dilated pupils.
- Tremor.
Moderate symptoms
- Agitation, restlessness.
- Muscle twitching, involuntary muscle contractions, muscle spasms, muscle rigidity.
- Sweating, shivering.
- Abnormal (side-to-side) eye movements.
Severe symptoms
- Confusion, disorientation, delirium.
- Rapid heart rate.
- High blood pressure.
- High body temperature (greater than 101.3° Fahrenheit [38.5° Celsius]).
- Seizures.
- Abnormal heartbeat.
- Passing out, fainting.
Symptoms usually begin within a few hours of taking a new medication that affects serotonin levels or increasing the dose of a drug you’re already taking. Nearly all people will experience symptoms within 24 hours of starting, adding or increasing the dosage of a serotonergic medication or product.
Serotonin syndrome generally doesn’t cause any problems once serotonin levels are back to their original levels.
Without treatment, serotonin symptoms can cause:
- Seizures.
- Trouble breathing.
- Kidney failure. The breakdown products of muscle (from spasms) are released into your blood, which is filtered through your kidneys. If left untreated, these products can cause severe kidney damage.
- Coma.
- Death.
If left untreated, severe serotonin syndrome can lead to unconsciousness and death.
There aren’t any tests to diagnose serotonin syndrome symptoms. Your doctor usually makes the diagnosis based on the results of your physical exam, review of your symptoms and history of medications you take that affect serotonin levels.
You can assist your doctor by telling them all the products you take, including prescription medicines, over-the-counter medicines, supplements, herbal products and illegal drugs. Be honest. Don’t worry. Your doctor is here to help you, not judge you.
To make sure your symptoms are caused by serotonin syndrome and not due to another cause, your doctor may use tests to:
- Measure levels of any drugs you’re using
- Check for signs of infection
- Check body functions that may be affected by serotonin syndrome
A number of conditions can cause symptoms similar to those of serotonin syndrome. Minor symptoms can be caused by several conditions. Moderate and severe symptoms similar to those of serotonin syndrome could be caused by:
- A serious reaction to certain medications, such as some anesthetics, antipsychotic drugs and other agents known to produce these severe reactions
- An overdose of illicit drugs, antidepressant medications or other medications that increase serotonin levels
- Damage associated with illicit drug use
- Severe alcohol withdrawal
Your doctor may order additional tests to rule out other causes of your symptoms. Tests may include:
- Blood and urine tests
- Chest X-ray
- Computerized Tomography (CT) scan
- Spinal tap (lumbar puncture)
Treatment of serotonin syndrome depends on the severity of your symptoms.
- If your symptoms are minor, a visit to the doctor and stopping the medication causing the problem may be enough.
- If you have symptoms that concern your doctor, you may need to go to the hospital. Your doctor may have you stay in the hospital for several hours to make sure your symptoms are improving.
- If you have severe serotonin syndrome, you’ll need intensive treatment in a hospital.
Depending on your symptoms, you may receive the following treatments:
- Muscle relaxants. Benzodiazepines, such as diazepam (Valium, Diastat) or lorazepam (Ativan), can help control agitation, seizures and muscle stiffness.
- Serotonin antagonists. If other treatments aren’t working, serotonin antagonists such as the medicine cyproheptadine may help. These medicines work by blocking certain serotonin receptors, lessening the activity that causes the symptoms.
- Oxygen and intravenous (IV) fluids. Breathing oxygen through a mask helps maintain oxygen levels in your blood, and IV fluids are used to treat dehydration and fever.
- Drugs that control heart rate and blood pressure. These may include esmolol (Brevibloc) or nitroprusside (Nitropress) to reduce a high heart rate or high blood pressure. If your blood pressure is too low, your doctor may give you phenylephrine (Vazculep) or epinephrine (Adrenalin, Epipen, others).
- A breathing tube and machine and medication to paralyze your muscles. You may need this treatment if you have a high fever (106° Fahrenheit [41.1° Celsius]).
Milder forms of serotonin syndrome usually go away within 24 to 72 hours of stopping medications that increase serotonin. You may need to take medications to block the effects of serotonin already in your system.
However, symptoms of serotonin syndrome caused by some antidepressants could take several weeks to go away completely. These medications remain in your system longer than do other medications that can cause serotonin syndrome.
List of selective serotonin reuptake inhibitors (SSRIs)
Common selective serotonin reuptake inhibitors (SSRIs) include:
- Citalopram (Celexa)
- Escitalopram (Lexapro)
- Fluoxetine (Prozac®, Prozac Weekly®, Rapuflux®, Selfemra®, and Sarafem®)
- Paroxetine (Paxil®, Aropax®, Brisdelle®, Pexeva® and Seroxat®)
- Sertraline (Zoloft)
- Vilazodone (Viibryd)
Citalopram
Citalopram belongs to the class of antidepressants known as selective serotonin reuptake inhibitors (SSRIs) 36, 37, 38, 39. Citalopram works by increasing the amount of serotonin, a natural substance in your brain that helps maintain mental balance. Citalopram is a medication that has been used to treat depression, including major depressive disorder. Citalopram is also sometimes used to treat obsessive-compulsive disorder [OCD] (with bothersome thoughts that won’t go away and the need to perform certain actions over and over), eating disorders, alcoholism, panic disorder (condition that causes sudden attacks of extreme fear with no apparent cause), premenstrual dysphoric disorder [PMDD] (a group of physical and emotional symptoms that occur before the menstrual period each month), social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life), post traumatic stress disorder (PTSD), tingling in the hands and feet caused by diabetes nerve damage (diabetic neuropathy), and certain male sexual problems. Citalopram may be prescribed for other uses; ask your doctor for more information.
Citalopram was approved for use in the United States in 1998 and Citalopram has become one of the most widely used antidepressant medications, with more than 16 million prescriptions being written yearly 39, 40.
Citalopram is available as tablets of 10, 20 and 40 mg and in an oral solution (liquid) of 10 mg/5 mL in several generic forms and under the brand name of Celexa. Citalopram is usually taken once a day, in the morning or in the evening, with or without food. The recommended dosage of citalopram in adults is 20 mg once daily, increasing to 40 mg daily if necessary. Take citalopram at around the same time every day. Your doctor may start you on a low dose of citalopram and gradually increase your dose, not more often than once a week. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take citalopram exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Your doctor may order certain laboratory tests and electrocardiograms (ECG; a test to monitor your heart rate and rhythm) before you start taking citalopram and during your treatment with citalopram.
It may take 1 to 4 weeks before you notice the full benefit of citalopram. Continue to take citalopram even if you feel well. Do not stop taking citalopram without talking to your doctor. Your doctor will probably decrease your dose gradually. If you suddenly stop taking citalopram, you may experience withdrawal symptoms such as mood changes, irritability, agitation, dizziness, numbness, tingling or electric shock-like sensations in the hands or feet, anxiety, confusion, headache, tiredness, nausea, sweating, shaking, frenzied or abnormally excited mood, and difficulty falling asleep or staying asleep. Tell your doctor if you experience any of these symptoms while you are decreasing your dose of citalopram or soon after you stop taking citalopram.
Common side effects of Citalopram are drowsiness, dyspepsia, nausea, headache, increased sweating and sexual dysfunction. Rare, but potentially severe adverse events include suicidal ideation and behavior, prolongation of the QTc interval, serotonin syndrome, precipitation of acute mania and acute glaucoma.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as citalopram during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, experts are not sure about how great this risk is and how much it should be considered in deciding whether a child or teenager should take an antidepressant. Children younger than 18 years of age should not normally take citalopram, but in some cases, a doctor may decide that citalopram is the best medication to treat a child’s condition.
You should know that your mental health may change in unexpected ways when you take citalopram or other antidepressants even if you are an adult over 24 years of age. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; and frenzied abnormal excitement. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking citalopram, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
The doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with citalopram. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. This risk is higher if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood), or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
Citalopram mechanism of action
Citalopram is a racemic dicyclic phthalane derivative designated (±)‐1‐(3‐dimethylaminopropyl)‐1‐(4‐fluorophenyl)‐1,3‐dihydroisobenzofuran‐5carbonitrile and its antidepressant effect is due to a specific inhibition of the re‐uptake of serotonin in the brain thereby increasing serotonergic activity in the central nervous system (brain and spinal cord) 41. Multiple studies confirm that citalopram hydrobromide is a highly selective and potent SSRI with minimal effects on the neuronal reuptake of norepinephrine (NE) and dopamine (DA) 42. Citalopram has no or very low affinity for a series of receptors including serotonin 5‐HT1A, 5‐HT2, dopamine D1, and D2, a1‐, a2‐, alpha- or beta-adrenergic receptors, histamine H1, muscarinic acetylcholine receptors, benzodiazepine receptors, gamma aminobutyric acid (GABA) and opioid receptors 43, 44, 45. Citalopram is a racemic mixture of both (R)- and (S)-enantiomers, whereas escitalopram consists solely of the (S)-enantiomer 46.
The neurotrophic hypothesis of depression emphasizes that depression results from reduced brain-derived neurotrophic factor (BDNF), leading to neuronal loss and reduced hippocampal neurogenesis. Antidepressants elevate brain-derived neurotrophic factor (BDNF) levels, counteracting neuronal and cellular loss. Extensive research in both preclinical and clinical depression studies reveals reduced serum brain-derived neurotrophic factor (BDNF) levels in depressed individuals. Antidepressants, including citalopram, raise the expression of brain-derived neurotrophic factor (BDNF) in the hippocampus and preferential cortex 47.
Pharmacokinetics
Citalopram onset of action for depression is about 1 to 4 weeks. However, the complete response may take 8 to 12 weeks after treatment initiation.
Bioavailability is 80%. Citalopram tablets and oral solutions are bioequivalent. Half-life is 24 to 48 hours (average, 35 hours). However, in patients with liver impairment, mild-to-moderate kidney impairment, older age (60 or older), and those who are poor CYP2C19 metabolizers, Citalopram’s half-life notably increases. Citalopram is metabolized primarily by CYP450 3A4 and 2C19, and it exhibits weak inhibitory effects on CYP450 2D6 48.
Citalopram uses
Citalopram hydrobromide is a selective serotonin reuptake inhibitor (SSRI). The primary FDA-approved clinical use for citalopram hydrobromide is for treating depression in adults. Off-label uses include alcohol use disorder, coronary arteriosclerosis, obsessive-compulsive disorder, panic disorder, postmenopausal flushing, and premenstrual dysphoric disorder. Citalopram is listed in the WHO model list of essential medicines to treat depressive disorders. According to the 2022 National Institute for Health and Care Excellence (NICE) guidelines, SSRIs should be considered the initial choice for pharmacotherapy in patients with depression 49.
FDA-Approved Indication for Citalopram
Citalopram is used for the treatment of depression in adults 18 years or older 50, 51, 52. In terms of efficacy, citalopram was more efficacious than other reference compounds like paroxetine or reboxetine, but worse than escitalopram. In terms of side effects, citalopram was more acceptable than older antidepressants, like tricyclic antidepressants 53.
Off-Label Use of Citalopram
- Obsessive-compulsive disorder (OCD) 54, 55
- Panic disorder 56
- Generalized anxiety disorder (GAD) 57
- Social anxiety disorder (social phobia)
- Separation anxiety disorder a mental health condition characterized by excessive fear or anxiety when separated from, or anticipating separation from, a close attachment figure, often a parent or caregiver, that is out of proportion to the situation and interferes with daily life.
- Premenstrual dysphoric disorder is a severe form of premenstrual syndrome (PMS) characterized by significant mood disturbances, irritability, and other symptoms that interfere with daily life, occurring in the week or two before menstruation 58
- Binge eating disorder is an eating disorder characterized by frequent and recurrent binge eating episodes with associated negative psychological and social problems 59
- Posttraumatic stress disorder (PTSD) 60
- Premature ejaculation 61
- Poststroke depression 62
The advantages and disadvantages of off-label use of Citalopram depend on the patient’s condition and the clinician’s judgment.
Before taking Citalopram
You should not use Citalopram if you are allergic to citalopram or escitalopram (Lexapro), or if you also take pimozide. Do not take pimozide (Orap) while you are taking Citalopram. Using these medicines together can cause very serious heart problems.
You should know that citalopram is very similar to another SSRI, escitalopram (Lexapro). You should not take these two medications together.
Do not use citalopram if you have used an monoamine oxidase (MAO) inhibitor in the past 14 days. A dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate). Wait at least 14 days after stopping an monoamine oxidase (MAO) inhibitor before you take citalopram.
Tell your doctor if you also use stimulant medicine, opioid medicine, herbal products, or medicine for depression, mental illness, Parkinson’s disease, migraine headaches, serious infections, or prevention of nausea and vomiting. An interaction with citalopram could cause a serious condition called serotonin syndrome.
To make sure citalopram is safe for you, tell your doctor if you have ever had:
- heart problems, high blood pressure, long QT syndrome (a rare heart problem that may cause irregular heartbeat, fainting, or sudden death),
- a heart attack, or if you have or have ever had a slow or irregular heartbeat, heart failure (condition in which the heart cannot pump enough blood to other parts of the body) or other heart conditions.
- a stroke
- bleeding problems
- sexual problems
- narrow-angle glaucoma. You should know that citalopram may cause angle-closure glaucoma, a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision. Talk to your doctor about having an eye examination before you start taking this medication. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, call your doctor or get emergency medical treatment right away.
- seizures or epilepsy
- bipolar disorder (manic depression) in you or a family member
- an electrolyte imbalance such as low levels of potassium, magnesium, or sodium in your blood.
- Liver disease: According to product labeling, the dosage needs to be reduced to 20 mg daily for patients with liver impairment.
- Kidney disease: No dose adjustment is necessary for patients with mild-to-moderate kidney impairment. Patients with severe kidney impairments should be closely monitored for possible adverse reactions.
The following nonprescription or herbal products may interact with citalopram: St. John’s wort; tryptophan; cimetidine (Tagamet); aspirin and nonsteroidal anti-inflammatory drugs (NSAIDS) such as ibuprofen (Advil, Motrin, others) and naproxen (Aleve). Be sure to let your doctor and pharmacist know that you are taking these medications before you start taking citalopram. Do not start any of these medications while taking citalopram without discussing with your doctor.
People with depression or mental illness may have thoughts about suicide. Some young people may have increased suicidal thoughts when first starting a medicine to treat depression. Stay alert to changes in your mood or symptoms. Your family or caregivers should also watch for sudden changes in your behavior.
Tell your doctor if you are pregnant, especially if you are in the last few months of your pregnancy, or if you plan to become pregnant or are breast-feeding. Taking citalopram during the last 3 months of pregnancy may harm the unborn baby, but stopping the medicine may not be safe for you. Citalopram may cause problems in newborns following delivery if it is taken during the last months of pregnancy. Do not start or stop citalopram without asking your doctor.
If you are pregnant, your name may be listed on a pregnancy registry to track the effects of citalopram on the baby.
Ask a doctor if it is safe to breastfeed while using Citalopram.
You should know that citalopram may make you drowsy and may affect your judgment, thinking, and movements. Do not drive a car or operate machinery until you know how Citalopram affects you. Alcohol can make the side effects of citalopram worse.
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to Citalopram or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies have not been performed on the relationship of age to the effects of citalopram in the pediatric population. Safety and efficacy have not been established.
Elderly
Citalopram capsules is not recommended for use in the elderly because an adjustment in the dose is not possible with the available dose strength of Citalopram.
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of citalopram in the elderly. However, elderly patients are more likely to have hyponatremia (low sodium in the blood) or syndrome of inappropriate antidiuretic hormone secretion (SIADH), which may require caution and an adjustment in the dose for patients receiving citalopram 63.
Pregnancy
It is not known if citalopram can make it harder for a woman to get pregnant 64. Studies in animals found that citalopram might cause some reduced fertility (ability to get pregnant) 64.
Miscarriage is common and can occur in any pregnancy for many different reasons. There have been some studies that suggested taking antidepressant medications might slightly increase the chance of miscarriage. However, a study on citalopram and escitalopram did not find an increased chance of miscarriage in women taking these medications 64.
Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. There are reports of more than 15,000 pregnancies exposed to citalopram or escitalopram. Overall, the available data do not suggest that citalopram or escitalopram increases the chance of birth defects. While some reports have suggested an increased chance of heart defects or other birth defects, most studies have not found an increased chance of birth defects 64.
Some studies suggest that taking citalopram or escitalopram throughout the pregnancy might increase the chance of pregnancy-related problems such as preterm birth (birth before 37 weeks of pregnancy) and low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth). However, research has also shown that when depression is left untreated during pregnancy, there could be an increased chance of pregnancy complications. This makes it hard to know if it is the medication, untreated depression, or other factors that are increasing the chance for these problems.
Some, but not all, studies have suggested that when pregnant women take SSRIs such as escitalopram or citalopram during the second half of the pregnancy, their babies might have an higher chance for a serious lung condition called persistent pulmonary hypertension. Persistent pulmonary hypertension happens in 1 or 2 out of 1,000 births. Among the studies looking at this, the overall chance for pulmonary hypertension when an SSRI was used in pregnancy was less than 1/100 (less than 1%).
One small study followed eleven babies exposed to citalopram during pregnancy. At one year of age there was no difference in their development compared to children who were not exposed to citalopram. Most studies find no increase in attention deficit hyperactivity disorder (ADHD) in children exposed to SSRIs during pregnancy. Most studies also find that SSRIs do not appear to increase the chance of autism spectrum disorder (ASD) after considering the effects of maternal depression or other factors.
Some medications taken during pregnancy are associated with withdrawal symptoms in a newborn after delivery. If you are taking escitalopram or citalopram at the time of delivery, your baby might have irritability, jitteriness, tremors (shivering), constant crying, different sleep patterns, problems with eating and controlling body temperature, and some problems with breathing. In most cases, these symptoms are mild and go away within a couple weeks with no treatment. Some babies may need to stay in the nursery or neonatal intensive care unit (NICU) until the symptoms go away. Most babies exposed to escitalopram or citalopram in late pregnancy do not have these symptoms. It is important that your doctor know you are taking these medications so that if symptoms occur your baby can get the care that is best for them.
Breastfeeding
Several studies have shown that small amounts of citalopram are found in breast milk 64. There have been a few case reports of sleepiness and weight loss, but in most studies no harmful effects were seen in breastfed babies 64. Studies also showed no difference in the intellectual development of babies exposed to citalopram during breastfeeding. A nursing infant should be monitored for being very sleepy (hard to wake for feeds), poor feeding and poor weight gain, especially in younger, exclusively breastfed infants and when a combination of medications for mental health are used. Be sure to talk to your doctor about all your breastfeeding questions. An alternative to Citalopram should be prescribed or you should stop breastfeeding while using citalopram.
Drug Interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking Citalopram, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using Citalopram with any of the following medicines is not recommended. Your doctor may decide not to treat you with this medication or change some of the other medicines you take.
- Bepridil
- Bromopride
- Cisapride
- Dronedarone
- Fluconazole
- Isocarboxazid
- Levoketoconazole
- Linezolid
- Mesoridazine
- Methylene Blue
- Metoclopramide
- Ozanimod
- Phenelzine
- Pimozide
- Piperaquine
- Posaconazole
- Procarbazine
- Rasagiline
- Safinamide
- Selegiline
- Sparfloxacin
- Terfenadine
- Thioridazine
- Tranylcypromine
- Ziprasidone
Using Citalopram with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Abciximab
- Aceclofenac
- Acemetacin
- Acenocoumarol
- Adagrasib
- Alfentanil
- Alfuzosin
- Almotriptan
- Amineptine
- Amiodarone
- Amisulpride
- Amitriptyline
- Amitriptylinoxide
- Amoxapine
- Amphetamine
- Amtolmetin Guacil
- Anagrelide
- Anileridine
- Apixaban
- Apomorphine
- Ardeparin
- Argatroban
- Aripiprazole
- Aripiprazole Lauroxil
- Armodafinil
- Arsenic Trioxide
- Artemether
- Asenapine
- Aspirin
- Astemizole
- Atazanavir
- Azathioprine
- Azithromycin
- Bedaquiline
- Bemiparin
- Benzhydrocodone
- Benzphetamine
- Betrixaban
- Bivalirudin
- Bromfenac
- Plus many more not on this list.
Using Citalopram with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Ginkgo
- Irinotecan
- Mavacamten
- Rifampin.
Citalopram Contraindications
Citalopram is contraindicated with the concomitant use of monoamine oxidase inhibitors (MAOIs). Evidence suggests that concurrent use of citalopram alongside an monoamine oxidase (MAO) inhibitor can result in serotonin syndrome (serotonergic toxicity). Symptoms of serotonin syndrome include rigidity, hyperthermia, autonomic instability, mental status changes, and coma. Similar adverse reactions are possible in patients who abruptly switched from an SSRI to an MAOI; therefore, the recommendation is to wait 14 days after discontinuing citalopram to initiate an monoamine oxidase (MAO) inhibitor 65.
Citalopram is also contraindicated in patients with hypersensitivity to the drug or excipient 66. Secondary to Citalopram inhibitory effects on CYP 2D6, it could hypothetically increase thioridazine concentrations, inducing dangerous arrhythmias 67. Canadian labeling for citalopram includes additional contraindications, specifically mentioning known QT interval prolongation or congenital long QT syndrome, which are not listed in the United States labeling 68. Citalopram should not be administered in patients using urokinase, pimozide, methylene blue, linezolid, or dapoxetine. Linezolid is a reversible, nonselective monoamine oxidase inhibitor that can lead to serotonin syndrome if administered with serotonergic drugs 69, 70.
Citalopram Dosage
The dose of Citalopram will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of Citalopram. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
For oral dosage forms (capsules)
- For depression
- Adults: 30 milligrams (mg) once a day. Your doctor may adjust your dose as needed. Do not start treatment with citalopram capsules because the only available dose strength is 30 mg. Use another dosage form of citalopram (eg, solution or tablets) for starting treatment and adjusting doses other than 30 mg once a day.
- Older adults: Use is not recommended.
- Children: Use and dose must be determined by your doctor.
For oral dosage forms (solution or tablets)
- For depression
- Adults: At first, 20 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg per day.
- Older adults: 20 mg once a day, taken either in the morning or evening.
- Children: Use and dose must be determined by your doctor.
Missed Dose
If you miss a dose of Citalopram, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Monitoring Before Treatment
Electrolytes, especially potassium and sodium, should be monitored and evaluated. Reevaluating electrolytes in patients at risk for electrolyte disturbances during the treatment is recommended.
QT-prolongation should be monitored. ECG is necessary for patients with congenital long QT syndrome, bradycardia, hypokalemia or hypomagnesemia, recent acute myocardial infarction, uncompensated heart failure, or concomitant use of other QT-prolonging drugs 71.
Monitoring During Treatment
- Patients need to be assessed and monitored for worsening depression, suicidality, or unusual changes in behavior during the initial few months of therapy or when the dose increases or decreases. Weekly face-to-face contact with patients during the initial first month of treatment, followed by visits every other week for the next month and ultimately at 3-month intervals, is recommended.
- Weight and growth should be monitored regularly by a clinician during treatment in children and adolescents.
- According to the Beers Criteria, monitor sodium levels closely when starting or adjusting the dose of citalopram in patients aged 65 and older 63, 63
Psychiatric Assessment for Depression and Anxiety
- Various scales in clinical practice can assist in screening anxiety disorder and depression and response to citalopram therapy.
- Patient Health Questionnaire (PHQ-9) 72
- Montgomery-Asberg Depression Rating Scale(MADRS) 73
- Hamilton Rating Scale for Depression(HDRS-17) 74
- Generalized Anxiety Disorder 7 score (GAD-7) 75
- Hamilton Anxiety Scale (HAM-A) 76
Citalopram side effects
Citalopram may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- nausea
- diarrhea
- constipation
- vomiting
- stomach pain
- heartburn
- decreased appetite
- weight loss
- increased sweating
- increased thirst
- frequent urination
- difficulty falling asleep or staying asleep
- drowsiness
- excessive tiredness
- yawning
- weakness
- uncontrollable shaking of a part of the body
- muscle or joint pain
- dry mouth
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or inability to have an orgasm
- heavy menstrual periods
- runny nose
Some side effects can be serious. If you experience any of the following symptoms, or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS sections, see your doctor immediately or get emergency medical treatment:
- chest pain
- shortness of breath
- dizziness
- fainting
- fever, sweating, confusion, fast or irregular heartbeat, severe muscle stiffness or twitching, agitation, hallucinations, loss of coordination, nausea, vomiting, or diarrhea
- coma (loss of consciousness)
- hives or blisters
- rash
- itching
- difficulty breathing or swallowing
- swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs
- hoarseness
- unusual bleeding or bruising
- nose bleeding
- headache
- unsteadiness
- problems with thinking, concentration, or memory
- seizures
Citalopram may decrease appetite and cause weight loss in children. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight while he or she is taking this medication. Talk to your child’s doctor about the risks of giving citalopram to your child.
Citalopram may cause other side effects. Call your doctor if you have any unusual problems while taking citalopram.
Citalopram Toxicity
Studies reveal that citalopram toxicity is not common, even at doses up to 100 mg. However, there is a chance of developing serotonin syndrome at therapeutic doses, primarily if using another serotonergic medication concomitantly.
In the event of an intentional Citalopram overdose, the ingestion of more than 600 mg of citalopram requires 8 hours of cardiac monitoring. At the end of the observation period, the patient can be discharged if the patient is asymptomatic and QTc is less than 450 milliseconds. However, continued inpatient cardiac monitoring is necessary for patients with QTc greater than 450 milliseconds at the end of the observation period 77. Case reports also describe recurrent seizures associated with massive citalopram overdose. Seizures should be treated with benzodiazepines 78.
Management of serotonin syndrome requires withdrawal of the citalopram and aggressive supportive treatment for hyperthermia and autonomic dysfunction. Cyproheptadine, a serotonin antagonist (5HT2 receptors), can be administered 79.
Escitalopram
Escitalopram belongs to the class of antidepressants known as selective serotonin reuptake inhibitors (SSRIs) 80. Escitalopram contains the same active medication as citalopram. These two drugs act in a very similar way by increasing the amount of serotonin, a natural substance in the brain that helps maintain mental balance. Escitalopram has been used to treat depression in adults and children and teenagers 12 years of ago or older. Escitalopram is also used to treat generalized anxiety disorder (GAD, excessive worry and tension that disrupts daily life and lasts for 6 months or longer) in adults, teenagers, and children 7 years of age and older.
Escitalopram was approved for use in the United States in 2002 and is available in tablets of 5, 10, and 20 mg and a solution (liquid) under the brand name Lexapro. It is usually taken once a day with or without food. The recommended dosage of escitalopram is 10 mg once daily, increasing to 20 mg daily if necessary. To help you remember to take escitalopram, take it at around the same time every day, in the morning or in the evening. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take escitalopram exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Your doctor may start you on a low dose of escitalopram and increase your dose after 1 week in adults and after 2 or 3 weeks in teenagers and children 7 years of age and older.
It may take 1 to 4 weeks or longer before you feel the full benefit of escitalopram. Continue to take escitalopram even if you feel well. Do not stop taking escitalopram without talking to your doctor. Your doctor will probably decrease your dose gradually. If you suddenly stop taking escitalopram, you may experience withdrawal symptoms such as mood changes, irritability, agitation, nausea, dizziness, burning, numbness, or tingling in the hands or feet, anxiety, confusion, headache, sweating, shaking, frenzied or abnormally excited mood, tiredness, and difficulty falling asleep or staying asleep. Tell your doctor if you experience any of these symptoms while you are decreasing your dose of escitalopram or soon after you stop taking escitalopram.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as escitalopram during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, experts are not sure about how great this risk is and how much it should be considered in deciding whether a child or teenager should take an antidepressant. Children younger than 12 years of age should not normally take escitalopram, but in some cases, a doctor may decide that escitalopram is the best medication to treat a child’s condition.
You should know that your mental health may change in unexpected ways when you take escitalopram or other antidepressants even if you are an adult over 24 years of age. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; and frenzied abnormal excitement. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking escitalopram, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
The doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with escitalopram. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. Tell your doctor if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood) or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
How does escitalopram work?
Selective serotonin reuptake inhibitors (SSRIs) exert their mechanism of action by binding to the sodium-dependent serotonin transporter protein (SERT) in the presynaptic neuron. Sodium-dependent serotonin transporter protein (SERT) is responsible for reuptaking serotonin from the synaptic cleft into the presynaptic neuron. Inactivation of sodium-dependent serotonin transporter protein (SERT) by escitalopram leads to an elevation in synaptic serotonin levels 81.
Serotonin also known as 5-hydroxytryptamine (5-HT), is a crucial neurotransmitter that regulates various human behavioral processes, including mood, perception, memory, anger, aggression, fear, stress response, appetite, addiction, and sexuality. The expression of multiple serotonin receptors in brain regions, such as the cortex, limbic system, midbrain, and hindbrain, orchestrates these processes 82. The brain has 5 primary serotonin receptors, 5-HT1A, 5-HT1B, 5-HT4, 5-HT6, and 5-HT7 83. In total, there are 15 known serotonin receptors, which are also found outside the central nervous system (brain and spinal cord) 82.
Pharmacokinetics
- Absorption: The pharmacokinetics of escitalopram demonstrate linearity and dose proportionality within the 10 to 30 mg/d dosage range. Notably, food does not affect the absorption of the drug. Peak plasma concentration is typically attained in approximately 5 hours, and steady-state plasma concentrations are achieved within 1 to 2 weeks 84
- Distribution: Escitalopram has a high volume of distribution (12 L/kg) and a low plasma protein binding (56%). Consequently, it is unlikely to provoke interactions with highly protein-bound drugs.
- Metabolism: Escitalopram undergoes hepatic metabolism via CYP3A4 and CYP2C19, yielding S-desmethyl-citalopram (S-DCT) and S-di-desmethyl citalopram (S-DDCT).
- Elimination: The terminal half-life of escitalopram varies from 27 to 33 hours. Escitalopram and its metabolites are exerted in the urine 85
How should escitalopram be used?
Escitalopram comes as a tablet and a solution (liquid) to take by mouth. It is usually taken once a day with or without food. To help you remember to take escitalopram, take it at around the same time every day, in the morning or in the evening. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take escitalopram exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Your doctor may start you on a low dose of escitalopram and increase your dose after 1 week.
It may take 1 to 4 weeks or longer before you feel the full benefit of escitalopram. Continue to take escitalopram even if you feel well. Do not stop taking escitalopram without talking to your doctor. If you suddenly stop taking escitalopram, you may experience withdrawal symptoms such as mood changes, irritability, agitation, dizziness, numbness or tingling in the hands or feet, anxiety, confusion, headache, tiredness, and difficulty falling asleep or staying asleep. Your doctor will probably decrease your dose gradually.
Who can and can’t take escitalopram
Escitalopram can be taken by adults over the age of 18.
Escitalopram isn’t suitable for some people. Check with your doctor before starting to take escitalopram if you:
- have had an allergic reaction to escitalopram or any other medicines in the past
- have epilepsy – as escitalopram can increase your seizures
- have a heart problem – as escitalopram can speed up or change your heartbeat
- have a low heart rate plus you have had severe diarrhoea and vomiting for a long time or take water tablets
- have liver or kidney problems – your doctor may need to change your dose
- have been told you have low sodium (salt) levels
- bruise or bleed easily
- are having electroconvulsive treatment
- have ever taken any other medicines for depression – some rarely used antidepressants can interact with escitalopram to cause very high blood pressure
- even when they’ve been stopped for a few weeks
- are trying to become pregnant, are already pregnant or are breastfeeding
- have an eye problem called glaucoma because escitalopram can increase the pressure in your eye
If you have diabetes, escitalopram can make it more difficult to keep your blood sugar stable. Monitor your blood sugar more often for the first few weeks of treatment with escitalopram and adjust your diabetes treatment if necessary.
Before taking Escitalopram
You should not use escitalopram if you are allergic to escitalopram or citalopram (Celexa), or if you also take pimozide.
Do not use escitalopram within 14 days before or 14 days after you have used an monoamine oxidase (MAO) inhibitor. A dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate). You must wait at least 14 days after stopping an monoamine oxidase (MAO) inhibitor before you take escitalopram.
You should know that escitalopram is very similar to another SSRI, citalopram (Celexa). You should not take these two medications together.
Some young people have thoughts about suicide when first taking an antidepressant. Stay alert to changes in your mood or symptoms. Report any new or worsening symptoms to your doctor.
Seek medical attention right away if you have symptoms of serotonin syndrome, such as: agitation, hallucinations, fever, sweating, shivering, fast heart rate, muscle stiffness, twitching, loss of coordination, nausea, vomiting, or diarrhea.
To make sure escitalopram is safe for you, tell your doctor if you have ever had:
- Bipolar disorder (mood disorder with mania and depression)
- Bleeding problems
- Drug addiction
- Angle-closure glaucoma (a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision). Talk to your doctor about having an eye examination before you start taking this medication. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, call your doctor or get emergency medical treatment right away.
- Hyponatremia (low sodium in the blood)
- Heart disease or heart attack
- High blood pressure
- Kidney disease
- Liver disease—Use with caution. The effects may be increased because of slower removal of the medicine from the body.
- Mania
- Seizures
- Sexual problems—Use with caution. May make these conditions worse.
- Stroke
- Suicidal thoughts.
Some medications should not be taken with escitalopram. Other medications may cause dosing changes or extra monitoring when taken with escitalopram. Make sure you have discussed any medications you are currently taking or plan to take before starting escitalopram with your doctor and pharmacist. Before starting, stopping, or changing any medications while taking escitalopram, please get the advice from your doctor or pharmacist.
The following nonprescription or herbal products may interact with escitalopram: aspirin, ibuprofen (Advil, Motrin IB), naproxen (Aleve), St. John’s wort, or tryptophan. Be sure to let your doctor and pharmacist know that you are taking these medications before you start taking escitalopram. Do not start any of these medications while taking escitalopram without discussing with your doctor.
Be sure your doctor knows if you also take stimulant medicine, opioid medicine, herbal products, or medicine for depression, mental illness, Parkinson’s disease, migraine headaches, serious infections, or prevention of nausea and vomiting. These medicines may interact with escitalopram and cause a serious condition called serotonin syndrome.
You should know that escitalopram may make you drowsy and may affect your judgment, thinking, and movements. Do not drive a car or operate machinery until you know how escitalopram affects you. Remember that alcohol can add to the drowsiness caused by escitalopram.
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to Escitalopram or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies performed to date have not demonstrated pediatric-specific problems that would limit the usefulness of escitalopram in children 12 years of age and older with depression. However, safety and efficacy have not been established in children less than 12 years of age. Escitalopram may cause weight loss or a decrease in appetite. Teenagers who will be taking it for a long time should have their weight and growth measured on a regular basis.
Appropriate studies have not been performed on the relationship of age to the effects of escitalopram in children younger than 7 years of age with generalized anxiety disorder. Safety and efficacy have not been established.
Elderly
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of escitalopram in the elderly. However, elderly patients are more likely to have hyponatremia (low sodium in the blood) and age-related liver problems, which may require caution and an adjustment in the dose for patients receiving escitalopram.
Pregnancy
It is not known if escitalopram can make it harder for a woman to get pregnant 64. Studies in animals found that escitalopram might cause some reduced fertility (ability to get pregnant) 64.
Miscarriage is common and can occur in any pregnancy for many different reasons. There have been some studies that suggested taking antidepressant medications might slightly increase the chance of miscarriage. However, a study on citalopram and escitalopram did not find an increased chance of miscarriage in women taking these medications 64.
Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. There are reports of more than 15,000 pregnancies exposed to citalopram or escitalopram. Overall, the available data do not suggest that citalopram or escitalopram increases the chance of birth defects. While some reports have suggested an increased chance of heart defects or other birth defects, most studies have not found an increased chance of birth defects 64.
Some studies suggest that taking citalopram or escitalopram throughout the pregnancy might increase the chance of pregnancy-related problems such as preterm birth (birth before 37 weeks of pregnancy) and low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth). However, research has also shown that when depression is left untreated during pregnancy, there could be an increased chance of pregnancy complications. This makes it hard to know if it is the medication, untreated depression, or other factors that are increasing the chance for these problems.
Some, but not all, studies have suggested that when pregnant women take SSRIs such as escitalopram or citalopram during the second half of the pregnancy, their babies might have an higher chance for a serious lung condition called persistent pulmonary hypertension. Persistent pulmonary hypertension happens in 1 or 2 out of 1,000 births. Among the studies looking at this, the overall chance for pulmonary hypertension when an SSRI was used in pregnancy was less than 1/100 (less than 1%).
Some medications taken during pregnancy are associated with withdrawal symptoms in a newborn after delivery. If you are taking escitalopram or citalopram at the time of delivery, your baby might have irritability, jitteriness, tremors (shivering), constant crying, different sleep patterns, problems with eating and controlling body temperature, and some problems with breathing. In most cases, these symptoms are mild and go away within a couple weeks with no treatment. Some babies may need to stay in the nursery or neonatal intensive care unit (NICU) until the symptoms go away. Most babies exposed to escitalopram or citalopram in late pregnancy do not have these symptoms. It is important that your doctor know you are taking these medications so that if symptoms occur your baby can get the care that is best for them.
Breastfeeding
Several studies have shown that small amounts of escitalopram are found in breast milk. There have been a few case reports of sleepiness and weight loss, but in most studies no harmful effects were seen in breastfed babies. Studies also showed no difference in the intellectual development of babies exposed to citalopram or escitalopram during breastfeeding. A nursing infant should be monitored for being very sleepy (hard to wake for feeds), poor feeding and poor weight gain, especially in younger, exclusively breastfed infants and when a combination of medications for mental health are used. Be sure to talk to your doctor about all your breastfeeding questions. An alternative to this medication should be prescribed or you should stop breastfeeding while using Escitalopram.
Drug Interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking Escitalopram, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using Escitalopram with any of the following medicines is not recommended. Your doctor may decide not to treat you with Escitalopram or change some of the other medicines you take.
- Bepridil
- Bromopride
- Cisapride
- Clorgyline
- Dronedarone
- Fluconazole
- Isocarboxazid
- Lazabemide
- Levoketoconazole
- Linezolid
- Mesoridazine
- Methylene Blue
- Metoclopramide
- Nialamide
- Ozanimod
- Phenelzine
- Pimozide
- Piperaquine
- Procarbazine
- Rasagiline
- Safinamide
- Saquinavir
- Selegiline
- Sparfloxacin
- Terfenadine
- Tranylcypromine
- Ziprasidone
Using Escitalopram with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Abciximab
- Aceclofenac
- Acemetacin
- Acenocoumarol
- Adagrasib
- Alfentanil
- Alfuzosin
- Almotriptan
- Amineptine
- Amiodarone
- Amisulpride
- Amitriptyline
- Amitriptylinoxide
- Amoxapine
- Amphetamine
- Amtolmetin Guacil
- Anagrelide
- Anileridine
- Apixaban
- Apomorphine
- Ardeparin
- Argatroban
- Aripiprazole
- Arsenic Trioxide
- Asenapine
- Aspirin
- Astemizole
- Atazanavir
- Atomoxetine
- Azathioprine
- Azithromycin
- Bedaquiline
- Bemiparin
- Benzhydrocodone
- Benzphetamine
- Betrixaban
- Bivalirudin
- Bromfenac
- Brompheniramine
- Bufexamac
- Plus many more not on this list.
Using Escitalopram with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Boceprevir
- Ginkgo
- Lamotrigine
- Mavacamten.
What is escitalopram used for?
Escitalopram is approved by the U.S. Food and Drug Administration (FDA) for treating major depressive disorder (unipolar depression) in adults and adolescents (ages 12 to 17) for both acute and maintenance phases 86. The FDA recently approved escitalopram for the treatment of generalized anxiety disorder (GAD) in both adults and children aged 7 and older 87, 88. Escitalopram is also used off-label for conditions such as social anxiety disorder, obsessive-compulsive disorder (OCD), panic disorder, posttraumatic stress disorder (PTSD), premenstrual dysphoric disorder (PMDD) and the management of hot flushes associated with menopause 89, 90, 91, 92.
Escitalopram Dosage
The dose of Escitalopram will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of Escitalopram. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
Escitalopram tablets come in different strengths ranging from 5 mg to 20mg.
The usual dose of escitalopram is 10mg a day in adults. However, you may start on a lower dose and increase to a maximum dose of 20mg a day. If you have liver problems, the maximum recommended dose is 10mg a day.
With liquid drops of escitalopram, 1 drop is equivalent to 1mg, 10 drops is 10mg, 20 drops is 20mg.
For oral dosage forms (solution or tablets)
- For depression
- Adults and children 12 years of age and older: 10 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 20 mg per day.
- Older adults: 10 mg once a day, taken either in the morning or evening.
- Children younger than 12 years of age: Use and dose must be determined by your doctor.
- For generalized anxiety disorder (GAD)
- Adults and children 7 years of age and older: At first, 10 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 20 mg per day.
- Older adults: 10 mg once a day, taken either in the morning or evening.
- Children younger than 7 years of age: Use and dose must be determined by your doctor.
Adult Dose for Generalized Anxiety Disorder
Use: Acute treatment of generalized anxiety disorder
- Initial dose: 10 mg orally once a day; increase if necessary after at least 1 week of treatment to 20 mg once a day
- Maintenance dose: 10 to 20 mg orally once a day
- Maximum dose: 20 mg orally once a day
Comment: Treatment should be periodically reassessed to determine the need for ongoing treatment; efficacy beyond 8 weeks has not been systematically studied.
Adult Dose for Depression
Use: Acute and maintenance treatment of major depressive disorder
- Initial dose: 10 mg orally once a day; increase if necessary after at least 1 week of treatment to 20 mg once a day
- Maintenance dose: 10 to 20 mg orally once a day
- Maximum dose: 20 mg orally once a day
Comments:
- Acute episodes may require several months or longer of sustained pharmacological therapy beyond response to the acute episode.
- Patients should be periodically reassessed to determine the need for maintenance treatment.
Geriatric Dose for Depression
Use: Acute and maintenance treatment of major depressive disorder
- Recommended dose: 10 mg orally once a day
Pediatric Dose for Depression
Use: Acute and maintenance treatment of major depressive disorder
12 years and older:
- Initial dose: 10 mg orally once a day; increase if necessary after at least 3 weeks of treatment to 20 mg once a day
- Maintenance dose: 10 to 20 mg orally once a day
- Maximum dose: 20 mg orally once a day
Comments:
- Acute episodes may require several months or longer of sustained pharmacological therapy beyond response to the acute episode.
- Patients should be periodically reassessed to determine the need for maintenance treatment.
Renal Dose Adjustments
- Mild to moderate renal dysfunction: No adjustment recommended
- Severe renal dysfunction: Use with caution
Liver Dose Adjustments
- Liver dysfunction: 10 mg orally once a day
Missed Dose
If you miss a dose of Escitalopram, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Escitalopram side effects
Escitalopram may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- nausea
- diarrhea
- constipation
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or unable to have an orgasm
- drowsiness
- yawning
- shaking
- difficulty falling asleep or staying asleep
- increased sweating
- dizziness
- heartburn
- stomach pain
- excessive tiredness
- dry mouth
- decreased appetite
- weight loss
- flu-like symptoms
- runny nose
- sneezing
Some side effects can be serious. If you experience either of the following symptoms or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS sections, see your doctor immediately:
- unusual excitement
- seeing things or hearing voices that do not exist (hallucinating)
- rash
- hives or blisters
- itching
- fever
- joint pain
- difficulty breathing or swallowing
- swelling of the face, throat, tongue, lips, or eyes
- fever, sweating, confusion, fast or irregular heartbeat, severe muscle stiffness or twitching, agitation, hallucinations, loss of coordination, nausea, vomiting, or diarrhea
- abnormal bleeding or bruising
- nose bleeding
- headache
- unsteadiness
- problems with thinking, concentration, or memory
- seizures
- difficult or painful urination
Escitalopram may decrease appetite and cause weight loss and height in children. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight while he or she is taking this medication. Talk to your child’s doctor about the risks of giving escitalopram to your child.
Escitalopram may cause other side effects. See your doctor if you have any unusual problems while taking Escitalopram.
Escitalopram withdrawal
Case reports of escitalopram discontinuation syndrome involved 2 patients 93. One subject gradually reduced escitalopram (over 3 weeks) 93, while the other first missed a few doses and then reduced the drug very gradually (over 9 months) 94. Both experienced electric-shock sensations a few days after drug stoppage, which lasted from 5 days 93 to 4 weeks 94.
Despite the limited literature available, the results of this systematic review indicate that withdrawal symptoms may occur with any type of SSRI (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline), even though they are exceedingly more frequent with paroxetine 95.
The pathophysiological mechanisms of withdrawal phenomena are still hypothetical and in need of proper neurobiological investigations 95. A number of mechanisms have been suggested: a decrease in serotonin availability when treatment ends 96, a behavioral stress response that is associated with increased hippocampal N-methyl-D-aspartate (NMDA) receptor density 97, and genetic vulnerabilities 98. Animal studies concerned with the long-term use of antidepressant drug have limited implications, since clear discontinuation-like behaviors in animal models are not available 99. Fava and Offidani 100 have interpreted the withdrawal phenomena according to the oppositional model of tolerance. Continued drug treatment may recruit processes that oppose the initial acute effects of a drug and may lead to a loss of efficacy and/or to a treatment-unresponsive course. When drug treatment ends, oppositional processes may operate for some time, resulting in the appearance of withdrawal symptoms and/or an increased vulnerability to relapse and/or resistance to treatment (if it is reinstituted) and/or switching to a bipolar course 100. The appearance of withdrawal symptoms after SSRI discontinuation may thus be potentially related to a number of important clinical phenomena 101.
Escitalopram overdose
In clinical trials of escitalopram, there were reports of escitalopram overdose, including overdoses of up to 600 mg, with no associated fatalities. During the postmarketing evaluation of escitalopram, escitalopram oxalate overdoses involving overdoses of over 1000 mg have been reported. As with other SSRIs, a fatal outcome in a patient who has taken an overdose of escitalopram has been rarely reported.
Symptoms most often accompanying escitalopram overdose, alone or in combination with other drugs and/or alcohol, included convulsions, coma, dizziness, hypotension, insomnia, nausea, vomiting, sinus tachycardia, somnolence, and ECG changes (including QT prolongation and very rare cases of torsade de pointes). Acute renal failure has been very rarely reported accompanying overdose.
Symptoms of overdose may include:
- dizziness
- sweating
- nausea
- vomiting
- tremor
- drowsiness
- fast or pounding heartbeat
- seizures
- confusion
- forgetfulness
- fast breathing
- coma (loss of consciousness for a period of time)
Management of escitalopram overdose
Establish and maintain an airway to ensure adequate ventilation and oxygenation. Gastric evacuation by lavage and use of activated charcoal should be considered. Careful observation and cardiac and vital sign monitoring are recommended, along with general symptomatic and supportive care. Due to the large volume of distribution of escitalopram, forced diuresis, dialysis, hemoperfusion, and exchange transfusion are unlikely to be of benefit. There are no specific antidotes for escitalopram oxalate.
In managing overdosage, consider the possibility of multiple-drug involvement. The physician should consider contacting a poison control center for additional information on the treatment of any overdose.
Fluoxetine
Fluoxetine belongs to the class of antidepressants known as selective serotonin reuptake inhibitors (SSRIs) 102, 103, 104. Fluoxetine works by increasing the amount of serotonin, a natural substance in the brain that helps maintain mental balance. Fluoxetine is a medication that has been used to treat depression, obsessive-compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), Tourette’s syndrome, bulimia nervosa, panic disorder (a type of anxiety disorder characterized by recurring, unexpected panic attacks, which are sudden episodes of intense fear or discomfort, often accompanied by physical symptoms, and persistent worry about future attacks), and premenstrual dysphoric disorder [PMDD] symptoms (a more severe form of premenstrual syndrome [PMS] characterized by extreme mood swings, bloating, irritability, breast tenderness and depression, occurring in the week or two before menstruation). Fluoxetine has also been used to treat body dysmorphic disorder, borderline personality disorder, hot flushes of menopause, post traumatic stress disorder (PTSD), alcoholism, attention-deficit/hyperactivity disorder (ADHD), sleep disorders, headaches, mental illness, sexual problems, phobias and Raynaud’s phenomenon. Fluoxetine is also used along with olanzapine (Zyprexa) to treat depression that did not respond to other medications and episodes of depression in people with bipolar disorder type 1 (manic-depressive disorder; a disease that causes episodes of depression, episodes of mania, and other abnormal moods). Fluoxetine may be prescribed for other uses; ask your doctor for more information.
Fluoxetine was approved for use in the United States in 1987 and it became one of the most widely used antidepressant medications, more than 20 million prescriptions being written yearly 103.
Fluoxetine is available as tablets, delayed-release (releases the medication in the intestine) capsules of 10, 20 and 40 mg and in an oral solution (liquid) of 20 mg/5 mL, in multiple generic forms and under the brand names of Prozac and Sarafem. Fixed combinations of fluoxetine with olanzapine (Symbyax and generic forms) are also available. A long acting formulation of 90 mg of fluoxetine has been developed for once weekly dosing (Prozac weekly).
Fluoxetine may be taken with or without food. Fluoxetine capsules, tablets, and liquid are usually taken once a day in the morning or twice a day in the morning and at noon. The recommended dosage of standard formulations of fluoxetine in adults is 20 mg once daily, increasing to 40 mg daily if necessary and not exceeding 80 mg daily.
Fluoxetine delayed-released capsules are usually taken once a week. Take fluoxetine at around the same time(s) every day. Swallow the delayed-release capsules whole; do not cut, crush, or chew them. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take fluoxetine exactly as directed. Your doctor may start you on a low dose of fluoxetine and gradually increase your dose. Do not take more or less of it or take it more often than prescribed by your doctor.
It may take 4 to 5 weeks or longer before you feel the full benefit of fluoxetine. Continue to take fluoxetine even if you feel well. Do not stop taking fluoxetine without talking to your doctor. If you suddenly stop taking fluoxetine, you may experience withdrawal symptoms such as mood changes, irritability, agitation, dizziness, numbness or tingling in the hands or feet, anxiety, sweating, confusion, headache, tiredness, and difficulty falling asleep or staying asleep. Your doctor will probably decrease your dose gradually.
Common side effects of fluoxetine are drowsiness, dyspepsia, nausea, headache, increased sweating, increased appetite, weight gain and sexual dysfunction.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as fluoxetine during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, experts are not sure about how great this risk is and how much it should be considered in deciding whether a child or teenager should take an antidepressant.
You should know that your mental health may change in unexpected ways when you take fluoxetine or other antidepressants even if you are an adult over 24 years of age. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; and frenzied abnormal excitement. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking fluoxetine, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
The doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with fluoxetine. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. This risk is higher if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood) or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
How does Fluoxetine work?
Fluoxetine belongs to the class of antidepressants known as selective serotonin reuptake inhibitors (SSRIs) 102, 103, 104. Fluoxetine exerts its antidepressant effects by blocking the reuptake of serotonin in the presynaptic serotonin neurons by blocking the reuptake transporter protein in the presynaptic terminal. Due to Fluoxetine’s action on the reuptake of serotonin, fluoxetine produces an activating effect, and due to its long half-life, the initial antidepressant effect emerges within 2 to 4 weeks. Fluoxetine also has mild activity at the serotonin 5-HT2A and 5-HT2C receptors.
Fluoxetine has minimal activity on noradrenergic reuptake.
Pharmacokinetics
- Absorption: Peak plasma concentrations of fluoxetine are attained after 6 to 8 hours. Fluoxetine is well absorbed with a bioavailability of 70% to 90%. Food does not appear to impact the bioavailability of fluoxetine, but it may slow its absorption by 1 to 2 hours, which is not clinically significant. Thus, fluoxetine may be administered with or without food.
- Distribution: Fluoxetine has plasma protein binding of approximately 94.5%, bound to albumin and alpha-1 glycoprotein. Fluoxetine readily crosses the blood-brain barrier, with a brain-to-plasma ratio of 2.6:1 in humans. The volume of distribution (Vd) of fluoxetine and its metabolite ranges between 20 to 42 L/kg. Some studies report that fluoxetine has the maximum volume of distribution (Vd) of any SSRI (between 14 and 100 L/kg) 105
- Metabolism: Fluoxetine’s active metabolite is norfluoxetine, produced when the cytochrome P450 enzyme (CYP2D6) acts on it. Prescribers must remember that fluoxetine has several drug-drug interactions due to its metabolism through the CYP2D6 isoenzyme. Additionally, norfluoxetine can have an inhibitory effect on CYP3A4. Fluoxetine has a half-life of 2 to 4 days, and its active metabolite norfluoxetine has a half-life of 7 to 9 days 106, 107. Approximately 7% of individuals definitively exhibit poor metabolism of fluoxetine due to reduced activity of CYP2D6 108.
- Elimination: Fluoxetine and norfluoxetine have long elimination half-lives, leading to the presence of the drug in the body for several weeks, even after stopping its use. This has important implications when discontinuing fluoxetine and prescribing medications that may interact with fluoxetine and norfluoxetine after discontinuation. The metabolism of fluoxetine is extensive, resulting in approximately 2.5% of the administered dose being excreted unchanged in the urine 109.
What is Fluoxetine used for?
Fluoxetine is a SSRI medication that has received FDA approval to treat major depressive disorder (8 years of age and older), obsessive-compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over) (7 years of age and older), panic disorder (a type of anxiety disorder characterized by recurring, unexpected panic attacks, which are sudden episodes of intense fear or discomfort, often accompanied by physical symptoms, and persistent worry about future attacks with or without agoraphobia), bulimia nervosa 110, 111, 112. The American Psychiatric Association guidelines recommend fluoxetine as first-line pharmacotherapy along with cognitive behavioral therapy (CBT) for patients with bulimia nervosa 113. Fluoxetine is also used as an add-on with olanzapine (Zyprexa) to treat depression that did not respond to other medications and episodes of depression in people with bipolar disorder type 1 (a mental health condition characterized by at least one manic episode, which may be followed by depressive or hypomanic episodes, and can involve psychosis).
Non-FDA-approved uses for fluoxetine include Tourette’s syndrome, binge eating disorder, social anxiety disorder, body dysmorphic disorder, premenstrual dysphoric disorder [PMDD] symptoms (a more severe form of premenstrual syndrome [PMS] characterized by extreme mood swings, bloating, irritability, breast tenderness and depression, occurring in the week or two before menstruation), borderline personality disorder, Raynaud’s phenomenon, and selective mutism 114, 115.
The American Psychological Association endorses fluoxetine for post traumatic stress disorder (PTSD) 116.
Fluoxetine has also been used to treat hot flushes of menopause, alcoholism, attention-deficit/hyperactivity disorder (ADHD), sleep disorders, headaches, mental illness, sexual problems and phobias. Fluoxetine may be prescribed for other uses; ask your doctor for more information.
Fluoxetine Contraindications
Contraindications to fluoxetine include hypersensitivity to fluoxetine or any component in its formulation. This drug is also contraindicated with the concurrent use of monoamine oxidase inhibitors (current use of monoamine oxidase (MAO) inhibitor or within 2 weeks of discontinuing the monoamine oxidase (MAO) inhibitor) due to the risk of serotonin syndrome.
Never initiate fluoxetine in a patient receiving linezolid 117.
Do not give fluoxetine with pimozide or thioridazine due to the risk of QT prolongation 118.
Use Fluoxetine with caution in those with a history of seizures or elderly patients.
Before taking Fluoxetine
You should not use Fluoxetine if you are allergic to fluoxetine, if you also take pimozide or thioridazine. Tell your doctor and pharmacist if you are allergic to fluoxetine, any other medications, or any of the ingredients in fluoxetine capsules, tablets, or solution. Ask your pharmacist for a list of the ingredients.
Do not use fluoxetine if you have used an monoamine oxidase (MAO) inhibitor in the past 14 days. A dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate). You must wait at least 14 days after stopping an monoamine oxidase (MAO) inhibitor before you take fluoxetine. You must wait 5 weeks after stopping fluoxetine before you can take thioridazine or an monoamine oxidase (MAO) inhibitor.
Tell your doctor about all other antidepressants you take, especially Celexa, Cymbalta, Desyrel, Effexor, Lexapro, Luvox, Oleptro, Paxil, Pexeva, Symbyax, Viibryd, or Zoloft.
To make sure fluoxetine is safe for you, tell your doctor if you have ever had:
- Bipolar disorder (mood disorder with mania and depression)
- Bleeding problems
- Diabetes
- Drug abuse
- Angle-closure glaucoma. You should know that fluoxetine may cause angle-closure glaucoma, a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision. Talk to your doctor about having an eye examination before you start taking fluoxetine. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, see your doctor or get emergency medical treatment right away.
- Hyponatremia (low sodium in the blood)
- Mania
- Seizures or epilepsy
- Sexual problems—Use with caution. May make these conditions worse.
- Heart attack or stroke
- Heart failure
- Heart rhythm problems such as prolonged QT interval (a rare heart problem that may cause irregular heartbeat, fainting, or sudden death)
- Cirrhosis of the liver or liver disease—Use with caution. The effects may be increased because of slower removal of the medicine from the body.
- Urination problems
- Suicidal thoughts
- Electroconvulsive therapy (ECT), procedure in which small electric shocks are administered to the brain to treat certain mental illnesses.
- Hypokalemia (low potassium in the blood) or
- Hypomagnesemia (low magnesium in the blood)—May cause side effects to become worse.
Also tell your doctor if you have a low level of potassium, magnesium, or sodium in your blood.
Tell your doctor if you have recently had a heart attack and if you have or have ever had a slow or irregular heartbeat, heart failure, or any other heart problems; high blood pressure; bleeding problems; a stroke; liver or kidney disease.
The following nonprescription or herbal products may interact with fluoxetine: St. John’s wort; tryptophan. Be sure to let your doctor and pharmacist know that you are taking these medications before you start taking fluoxetine. Do not start any of these medications while taking fluoxetine without discussing with your doctor.
Some young people have thoughts about suicide when first taking an antidepressant. Your doctor should check your progress at regular visits. Your family or other caregivers should also be alert to changes in your mood or symptoms.
Older adults may be more sensitive to the effects of fluoxetine.
Ask your doctor about taking fluoxetine if you are pregnant, especially if you are in the last few months of your pregnancy, or if you plan to become pregnant or are breastfeeding. Taking an SSRI antidepressant during late pregnancy may cause serious medical complications in the baby if it is taken during the last months of pregnancy. However, you may have a relapse of depression if you stop taking your antidepressant. Tell your doctor right away if you become pregnant. If you are pregnant, your name may be listed on a pregnancy registry to track the effects of fluoxetine on the baby.
If you are breastfeeding, tell your doctor if you notice agitation, fussiness, feeding problems, or poor weight gain in the nursing baby.
You should know that fluoxetine may make you drowsy and may affect your judgment, thinking, and movements. Do not drive a car or operate machinery until you know how fluoxetine affects you. Remember that alcohol can add to the drowsiness caused by fluoxetine.
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to Fluoxetine or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies performed to date have not demonstrated pediatric-specific problems that would limit the usefulness of fluoxetine in children. However, safety and efficacy have not been established to treat depression in children younger than 8 years of age, to treat obsessive-compulsive disorder in children younger than 7 years of age, and to treat depression that is part of bipolar disorder in children younger than 10 years of age.
Appropriate studies have not been performed on the relationship of age to the effects of fluoxetine in children with bulimia nervosa, panic disorder, or treatment resistant depression. Safety and efficacy have not been established.
Fluoxetine is FDA-approved for administration in pediatric patients with major depressive disorder (clinical depression) and obsessive-compulsive disorder (OCD). As with other SSRIs, decreased weight gain is associated with administering fluoxetine in children and adolescent patients. The dose for children with major depressive disorder (clinical depression) and obsessive-compulsive disorder (OCD) is 10 mg once daily. According to the American Academy of Child and Adolescent Psychiatry (AACAP), it is recommended to offer selective serotonin reuptake inhibitor (SSRI) medication, particularly fluoxetine, to children and adolescents diagnosed with major depressive disorder. For those who respond positively to acute treatment with fluoxetine, the American Academy of Child and Adolescent Psychiatry (AACAP) suggests continuing with fluoxetine alone or combining it with cognitive-behavioral therapy to prevent the relapse or recurrence of major depressive disorder 119.
Extensive metareview study results show that fluoxetine offers a strong risk-benefit ratio compared to other antidepressants in youth. This finding suggests that fluoxetine could be recommended as the initial treatment of choice for depressive disorders in children and adolescents 120.
Elderly
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of fluoxetine in the elderly 121. However, elderly patients are more likely to have hyponatremia (low sodium in the blood) than younger adults, which may require caution and an adjustment in the dose for patients receiving fluoxetine.
Pregnancy
Fluoxetine has been studied in women having medical treatments because they were already having a hard time getting pregnant. In these studies, those who took fluoxetine got pregnant at the same rate as those who did not take fluoxetine 122.
Out of all babies born each year, about 3 out of 100 (3%) will have a birth defect. Doctors look at research studies to try to understand if an exposure, like fluoxetine, might increase the chance of birth defects in a pregnancy. Fluoxetine use is not expected to increase the chance of birth defects. There are reports of over 10,000 pregnancies exposed to fluoxetine in the first trimester (when many major birth defects can happen). No pattern of birth defects has been found and most studies have not found an increased chance of birth defects related to fluoxetine use.
Some studies have suggested an increased chance of heart defects or other birth defects. However, there is no proven increased chance of birth defects directly related to fluoxetine.
Some studies suggest a higher chance of preterm delivery (birth before week 37) or low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth) with the use of fluoxetine in pregnancy. However, research has also shown that when conditions such as depression or anxiety are untreated or undertreated during pregnancy, there could be an increased chance of pregnancy complications. This makes it hard to know if it is the medication, the underlying condition, or other factors that might increase the chance for these problems.
Some, but not all, studies have suggested that when women who are pregnant take SSRIs during the second half of pregnancy, their babies might have an increased chance for a serious lung condition called persistent pulmonary hypertension (PPH). Persistent pulmonary hypertension happens in 1 or 2 out of 1,000 births. A recent report that combined results from several studies suggested the chance for persistent pulmonary hypertension might be increased if an SSRI was used during pregnancy. However, it was not clear if this was due to medication exposure or to other exposures that people who take SSRIs have in common, such as higher rates of smoking. Data from studies suggest the overall chance for persistent pulmonary hypertension when an SSRI is used in pregnancy is less than 1/100 (less than 1%).
The use of fluoxetine during pregnancy and/or in the third trimester can cause temporary symptoms in newborns soon after birth. These symptoms are sometimes referred to as withdrawal. Symptoms include being irritable and/or jittery, crying, tight muscles, trouble breathing, unusual sleep patterns, tremors (shivers), and/or trouble eating. In most cases symptoms are mild and go away in a few weeks with no treatment, or with only supportive care. Not all babies exposed to fluoxetine will have these symptoms. There might be a higher chance for withdrawal symptoms if other psychiatric medications are also taken with fluoxetine during pregnancy. It is important that your doctor know you are taking fluoxetine so that if symptoms occur your baby can get the care that is best for them.
Does taking fluoxetine in pregnancy affect future behavior or learning for the child?
A few studies have looked at the development of children from age 16 months to 7 years and did not find differences between children who were exposed to fluoxetine during pregnancy and those who were not. Most studies found no increase in attention deficit hyperactivity disorder (ADHD) in children exposed to SSRIs like fluoxetine during pregnancy. Most studies also find that SSRIs like fluoxetine do not appear to increase the chance of autism spectrum disorders (ASD) after adjusting for factors such as maternal illness.
Breastfeeding
Fluoxetine gets into breast milk and most reports find no side effects in breastfed babies 122. In a small number of cases, irritability, vomiting, diarrhea, and less sleep have been reported. One study noted slightly less weight gain in infants exposed to fluoxetine via breast milk; however, this would likely only be an issue if the infant’s weight gain was already a concern 122. One study showed that mental and physical development was normal for infants exposed to fluoxetine in breast milk in their first year of life 122. Studies in women breastfeeding have demonstrated harmful infant effects 123. If you suspect the baby has any symptoms (such as irritability, vomiting, diarrhea, trouble sleeping, or trouble gaining weight) contact the child’s doctor.
The product label for fluoxetine recommends women who are breastfeeding not use this medication. But the benefit of treating your condition might outweigh possible risks. Your doctor can talk with you about using fluoxetine and what treatment is best for you. Be sure to talk to your doctor about all your breastfeeding questions.
An alternative to Fluoxetine should be prescribed or you should stop breastfeeding while using Fluoxetine.
If a man takes fluoxetine, could it affect fertility or increase the chance of birth defects?
Fluoxetine and other SSRIs have been reported to cause some sexual side effects, such as lower sexual desire or problems with ejaculation. This can affect a man’s fertility (ability to get a woman pregnant). Studies looking at fluoxetine in a small number of men have reported that sperm quality can be affected (but still within the normal range) with long-term fluoxetine use. The sperm quality improved when fluoxetine was stopped. In general, exposures that men have are unlikely to increase risks to a pregnancy.
Drug Interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking Fluoxetine, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using Fluoxetine with any of the following medicines is not recommended. Your doctor may decide not to treat you with Fluoxetine or change some of the other medicines you take.
- Bepridil
- Bromopride
- Cisapride
- Clorgyline
- Dronedarone
- Isocarboxazid
- Levoketoconazole
- Levomethadyl
- Linezolid
- Mavacamten
- Mavorixafor
- Mesoridazine
- Methylene Blue
- Nialamide
- Ozanimod
- Phenelzine
- Pimozide
- Piperaquine
- Procarbazine
- Rasagiline
- Safinamide
- Saquinavir
- Selegiline
- Sparfloxacin
- Terfenadine
- Thioridazine
- Toloxatone
- Tranylcypromine
- Ziprasidone
Using Fluoxetine with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Abciximab
- Abiraterone Acetate
- Abiraterone Acetate, Micronized
- Aceclofenac
- Acemetacin
- Acenocoumarol
- Adagrasib
- Alfentanil
- Alfuzosin
- Almotriptan
- Amineptine
- Amiodarone
- Amisulpride
- Amitriptyline
- Amitriptylinoxide
- Amoxapine
- Amphetamine
- Amtolmetin Guacil
- Anagrelide
- Anileridine
- Apixaban
- Apomorphine
- Aprindine
- Ardeparin
- Argatroban
- Aripiprazole
- Aripiprazole Lauroxil
- Arsenic Trioxide
- Asenapine
- Aspirin
- Astemizole
- Atazanavir
- Atomoxetine
- Azithromycin
- Bedaquiline
- Belzutifan
- Bemiparin
- Benzhydrocodone
- Benzphetamine
- Betrixaban
- Plus many more not on this list.
Using Fluoxetine with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Alprazolam
- Cyproheptadine
- Delavirdine
- Diazepam
- Ginkgo
- Metoprolol.
Fluoxetine Dosage
The dose of Fluoxetine will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of Fluoxetine. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
For oral dosage forms (capsules, delayed-release capsules, pulvules, or solution)
- For bulimia nervosa
- Adults: 60 milligrams (mg) once a day in the morning.
- Children: Use and dose must be determined by your doctor.
- For depression
- Adults: At first, 20 milligrams (mg) once a day in the morning. Your doctor may adjust your dose as needed. If you are taking more than 20 mg per day, you may take the capsule once a day in the morning or 2 times a day (eg, morning and noon). However, the dose is usually not more than 80 mg per day.
- Children 8 years of age and older: At first, 10 or 20 mg once a day in the morning. Your doctor may adjust your dose as needed.
- Children younger than 8 years of age: Use and dose must be determined by your doctor.
Major depressive disorder
The typical starting dose of fluoxetine for major depressive disorder (clinical depression) is 20 mg daily. The maximum recommended dose of fluoxetine for major depressive disorder is 80 mg daily 124.
Depression associated with bipolar disorder (combination with olanzapine)
- Adults: At first, 20 milligrams (mg) of fluoxetine and 5 mg of olanzapine once a day, taken in the evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg of fluoxetine and 12 mg of olanzapine per day.
- Children 10 years of age and older: At first, 20 milligrams (mg) of fluoxetine and 2.5 mg of olanzapine once a day, taken in the evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg of fluoxetine and 12 mg of olanzapine per day.
- Children younger than 10 years of age: Use and dose must be determined by your doctor.
Treatment resistant depression (combination with olanzapine)
- Adults: At first, 20 milligrams (mg) of fluoxetine and 5 mg of olanzapine once a day, taken in the evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg of fluoxetine and 20 mg of olanzapine per day.
- Children: Use and dose must be determined by your doctor.
Obsessive-compulsive disorder (OCD)
- Adults: At first, 20 milligrams (mg) once a day in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 80 mg per day. The typical maintenance dose for obsessive-compulsive disorder (OCD) is 20 to 60 mg.
- Children 7 years of age and older: At first, 10 mg once a day in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 60 mg per day.
- Children younger than 7 years of age: Use and dose must be determined by your doctor.
Panic disorder
- Adults: At first, 10 milligrams (mg) once a day in the morning. Your doctor may adjust your dose as needed. After 1 week, consider increasing the fluoxetine to 20 mg daily. The maximum recommended dose of fluoxetine for panic disorder is 60 mg daily.
- Children: Use and dose must be determined by your doctor.
Premenstrual dysphoric disorder (PMDD)
- Adults: At first, 20 milligrams (mg) once a day in the morning. Your doctor may have you take 20 mg every day of your menstrual cycle or for only 15 days of your cycle. Your doctor may adjust your dose as needed. However, the dose is usually not more than 80 mg per day.
- Children: Use and dose must be determined by your doctor.
Bulimia nervosa
The American Psychiatric Association guidelines recommend cognitive-behavioral therapy (CBT) as the primary treatment for adults with bulimia nervosa. If there is minimal or no response to psychotherapy alone within 6 weeks, prescribing 60 mg of fluoxetine daily is recommended 113.
Missed Dose
If you miss a dose of Fluoxetine, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Monitoring
A thorough assessment of depression and suicidal risk, particularly at the beginning of Fluoxetine therapy or when doses are changed, anxiety/panic attacks, social functioning, mania/mood lability, and features of serotonin syndrome 125, 126. The Patient Health Questionnaire-9 (PHQ-9) and Hamilton Depression Rating Scale (HAM-D/HDRS) should be monitored 127, 128, 129.
No routine laboratory testing is necessary for healthy individuals. However, in older and population-specific patients, clinicians may order blood glucose and liver function tests. In addition, prescribers may order an ECG for patients with risk factors for QT prolongation and ventricular arrhythmias. Pediatric patients’ height and weight should be monitored periodically when receiving fluoxetine.
The American Society of Regional Anesthesia (ASRA) suggests a washout period of approximately 5 weeks before interventional spine and pain procedures due to the long half-life of fluoxetine to decrease the risk of bleeding 130.
Fluoxetine side effects
Fluoxetine may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- nervousness
- anxiety
- difficulty falling asleep or staying asleep
- nausea
- diarrhea
- dry mouth
- heartburn
- yawning
- weakness
- uncontrollable shaking of a part of the body
- loss of appetite
- weight loss
- unusual dreams
- stuffy nose
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or unable to have an orgasm
- excessive sweating
- headache, confusion, weakness, difficulty concentrating, or memory problems
Some side effects can be serious. If you experience any of the following symptoms or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS section, see your doctor immediately:
- rash
- hives or blisters
- itching
- fever
- joint pain
- swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs
- difficulty breathing or swallowing
- agitation, fever, sweating, confusion, fast or irregular heartbeat, shivering, severe muscle stiffness or twitching, hallucinations, loss of coordination, nausea, vomiting, or diarrhea
- fast, slow, or irregular heartbeat
- shortness of breath
- dizziness or fainting
- seizures
- abnormal bleeding or bruising
Fluoxetine may decrease appetite and cause weight loss in children. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight while he or she is taking this medication. Talk to your child’s doctor about the risks of giving fluoxetine to your child.
Fluoxetine may cause other side effects. See your doctor if you have any unusual problems while taking fluoxetine.
Fluoxetine Toxicity
Fluoxetine is rarely lethal in monotherapy overdose. However, when taken with alcohol, it may cause ataxia and respiratory depression. Fluoxetine may cause serotonin syndrome (also knownn as serotonin toxicity, which is a potentially life-threatening drug reaction that results from having too much serotonin in your body) when taken in excessive amounts or combined with other agents that increase serotonin levels 131, 132.
Management of Fluoxetine Overdose
In the case of SSRI overdose, the goal is to provide supportive therapy. This support can be in the form of airway protection, serial ECGs to monitor for cardiotoxicity, administration of benzodiazepines for sedation, and GI decontamination with activated charcoal. Serotonin syndrome is treatable with the administration of cyproheptadine 2, 133.
Paroxetine
Paroxetine is a selective serotonin reuptake inhibitor (SSRI) that has been used to treat depression, generalized anxiety disorder (GAD, excessive worrying that is difficult to control), social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life), obsessive compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), premenstrual dysphoric disorder (PMDD, physical and psychological symptoms that occur before the onset of the menstrual period each month), post-traumatic stress disorder (PTSD, disturbing psychological symptoms that develop after a frightening experience), and panic disorder (sudden, unexpected attacks of extreme fear and worry about these attacks) 134. Paroxetine is also used to treat chronic headaches, diabetic neuropathy (numbness in the hands and feet caused by diabetes), premature ejaculation and hot flashes (sudden feelings of warmth, especially in the face, neck, and chest) in women who are experiencing menopause (stage of life when menstrual periods become less frequent and stop and women may experience other symptoms and body changes) 135. There is not enough information available at this time to know how paroxetine works to treat hot flashes in menopause. Paroxetine is also sometimes used with other medications to treat bipolar disorder (mood that changes from depressed to abnormally excited). Paroxetine may be prescribed for other uses; ask your doctor or pharmacist for more information.
Paroxetine was approved for use in the United States in 1992 and it remains in wide use, with more than 15 million prescriptions being filled yearly 136.
Paroxetine is available as tablets of 10, 20, 30 and 40 mg and an oral suspension (liquid) in generic forms and under the brand names of Paxil and Pexeva. The recommended dosage for depression in adults is 20 mg once daily, increasing the dosage by 10 mg increments weekly to a maximum of 50 mg. Controlled release or extended-release (long-acting) tablets are also available that have slightly different dosing recommendations.
The tablets, suspension, and controlled-release tablets are usually taken once daily in the morning or evening, with or without food. The capsules are usually taken once a day at bedtime with or without food. You may want to take paroxetine with food to prevent stomach upset. Take paroxetine at around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take paroxetine exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Shake the liquid well before each use to mix the medication evenly.
Swallow the extended-release and regular tablets whole; do not chew or crush them.
If you are taking paroxetine tablets, suspension, or controlled-release tablets, your doctor may start you on a low dose of paroxetine and gradually increase your dose, not more than once a week.
Paroxetine capsules contain a lower dose of paroxetine than is needed to treat depression and other forms of mental illness. Do not take paroxetine capsules to treat a mental illness. If you think you have depression or another mental illness, talk to your doctor about treatment.
Paroxetine may help control your symptoms but will not cure your condition. It may take several weeks or longer before you feel the full benefit of paroxetine. Continue to take paroxetine even if you feel well. Do not stop taking paroxetine without talking to your doctor. Your doctor may decrease your dose gradually. If you suddenly stop taking paroxetine tablets, suspension, or controlled-release tablets, you may experience withdrawal symptoms such as depression; mood changes; frenzied or abnormally excited mood; irritability; anxiety; confusion; dizziness; headache; tiredness; numbness or tingling in the arms, legs, hands, or feet; unusual dreams; difficulty falling asleep or staying asleep; nausea; or sweating. Tell your doctor if you experience any of these symptoms when your dose of paroxetine is decreased.
Common side effects of Paroxetine are drowsiness, dyspepsia, nausea, headache, increased sweating, increased appetite, weight gain and sexual dysfunction. Rare but potentially severe adverse events include suicidal ideation and behavior, activation of mania, serotonin syndrome, discontinuation syndrome, increased risk of bleeding, seizures, acute glaucoma, hypersensitivity reactions and embryo-fetal toxicity.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as paroxetine during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, there are also risks when depression is not treated in children and teenagers. Talk to your child’s doctor about these risks and whether your child should take an antidepressant, Children younger than 18 years of age should not normally take paroxetine, but in some cases, a doctor may decide that paroxetine is the best medication to treat a child’s condition.
You should know that your mental health may change in unexpected ways when you take paroxetine or other antidepressants to treat depression or other mental illness even if you are an adult over 24 years of age. You may also experience changes in your mental health if you are a woman taking a low dose of paroxetine to treat hot flashes and you have never had depression or another mental illness. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; and frenzied abnormal excitement. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking paroxetine, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
The doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with paroxetine. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter what your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. This risk is higher if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood) or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
How does Paroxetine work?
Paroxetine is a selective serotonin reuptake inhibitor (SSRI) that works by blocking the serotonin reuptake transporter (SERT) and thus increasing the concentration of synaptic serotonin. Current theory suggests that the diminished serotonin concentration in the depressed brain induces the upregulation of serotonergic receptors. By increasing the synaptic serotonin concentration, paroxetine thus induces the downregulation of the previously upregulated serotonin receptors, thus normalizing the receptor concentration 137. Furthermore, in a radioligand study, paroxetine showed some affinity for muscarinic, adrenergic (alpha and beta), dopaminergic (D2), serotonergic (5-HT2), and histaminergic (H1) receptors 138. These receptors have also appeared to contribute to Paroxetine’s antidepressant effects and its side effect profile 134.
Paroxetine undergoes metabolism via liver CYPP450 2D6 and Paroxetine is 62% metabolized over a 10-day post-dosing period 134. Paroxetine inhibits CYP2D6 and, thus, its own metabolism; plasma concentrations can potentially double following dosage increases of 50% 139. The urine excretes 2% Paroxetine and 36% excreted in the feces.
What is Paroxetine used for?
Paroxetine is a selective serotonin reuptake inhibitor (SSRI) that is FDA approved to treat depression (major depressive disorder), generalized anxiety disorder (GAD, excessive worrying that is difficult to control), social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life), obsessive compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), panic disorder (sudden, unexpected attacks of extreme fear and worry about these attacks), premenstrual dysphoric disorder (PMDD, physical and psychological symptoms that occur before the onset of the menstrual period each month) and post-traumatic stress disorder (PTSD, disturbing psychological symptoms that develop after a frightening experience) 134. Paroxetine is not FDA approved for use in children and adolescents less than 18 years of age; however, clinicians use it off-label in this group.
Paroxetine is also used to treat chronic headaches, diabetic neuropathy (numbness in the hands and feet caused by diabetes), premature ejaculation and hot flashes (sudden feelings of warmth, especially in the face, neck, and chest) in women who are experiencing menopause (stage of life when menstrual periods become less frequent and stop and women may experience other symptoms and body changes) 135. There is not enough information available at this time to know how paroxetine works to treat hot flashes in menopause. Paroxetine is also sometimes used with other medications to treat bipolar disorder (mood that changes from depressed to abnormally excited). Paroxetine may be prescribed for other uses; ask your doctor or pharmacist for more information.
Paroxetine Off-Label Use
- Obsessive-compulsive disorder (in children and adolescents)
- Social anxiety disorder (in children and adolescents)
- Separation anxiety
- Dysthymia also known as persistent depressive disorder, which is a chronic, low-grade form of depression characterized by persistent feelings of sadness and hopelessness, lasting for at least two years
- Body dysmorphic disorder
- Postpartum depression
- Premature ejaculation
- Cancer causing itch that is unresponsive to standard treatment.
Paroxetine Contraindications
There are only a few absolute contraindications for the use of paroxetine. Absolute contraindications include concurrent use of monoamine oxidase inhibitors (MAOIs), thioridazine, and pimozide. Concomitant use of monoamine oxidase (MAO) inhibitors and paroxetine can precipitate serotonin syndrome. Concurrent use of thioridazine and paroxetine can induce cardiac arrhythmias; similar effects can occur with pimozide and paroxetine 140.
Precautions that should be acknowledged when prescribing paroxetine include concurrent tricyclic antidepressant (TCA) use, concomitant tamoxifen use, and drugs affecting liver metabolism. Paroxetine inhibits tricyclic antidepressant (TCA) metabolism, leading to possible tricyclic antidepressant (TCA) toxicity. Tamoxifen is active once metabolized by CYP4502D6; thus, paroxetine essentially inactivates tamoxifen.
Paroxetine is not recommended for use during pregnancy or if breastfeeding. Based on epidemiological studies, infants exposed to paroxetine during the first trimester had an increased risk for cardiovascular malformations 140.
Before taking Paroxetine
You should not use Paroxetine if you are allergic to paroxetine, or if you are also taking pimozide or thioridazine.
Do not use Paroxetine if you have used an monoamine oxidase (MAO) inhibitor in the past 14 days. A dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate). You must wait at least 14 days after stopping an monoamine oxidase (MAO) inhibitor before you take Paroxetine.
To make sure paroxetine is safe for you, tell your doctor if you have:
- Bipolar disorder (mood disorder with mania and depression)
- Bleeding problems
- Bone problems
- Angle-closure glaucoma. You should know that Paroxetine may cause angle-closure glaucoma, a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision. Talk to your doctor about having an eye examination before you start taking Paroxetine. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, see your doctor or get emergency medical treatment right away.
- Drug addiction
- Hyponatremia (low sodium in the blood)
- Hyponatremia (low sodium in the blood)
- Mania, history of or
- Seizures, history of or
- Sexual problems: Use with caution. May make these conditions worse.
- Kidney disease, severe or
- Liver disease, severe: Use with caution. The effects may be increased because of slower removal of the medicine from the body.
- Suicidal thoughts.
Be sure your doctor knows if you also take stimulant medicine, opioid medicine, herbal products, or medicine for depression, mental illness, Parkinson’s disease, migraine headaches, serious infections, or prevention of nausea and vomiting. These medicines may interact with paroxetine and cause a serious condition called serotonin syndrome.
Some young people have thoughts about suicide when first taking an antidepressant. Your doctor should check your progress at regular visits. Your family or other caregivers should also be alert to changes in your mood or symptoms.
Taking an SSRI antidepressant during pregnancy may cause serious lung problems or other complications in the baby. However, you may have a relapse of depression if you stop taking your antidepressant. Tell your doctor right away if you become pregnant. Do not start or stop taking Paroxetine without your doctor’s advice.
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to Paroxetine or any other medicines. Also tell your doctor if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies have not been performed on the relationship of age to the effects of paroxetine in the pediatric population. Safety and efficacy have not been established.
Use of Brisdelle® or paroxetine capsules is not indicated in the pediatric population.
Elderly
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of paroxetine in the elderly. However, elderly patients may be more sensitive to the effects of Paroxetine than younger adults, and are more likely to have hyponatremia (low sodium in the blood), which may require caution and an adjustment in the dose for patients receiving paroxetine.
Pregnancy
Paroxetine is contraindicated in pregnancy and is classified as category D/X due to its teratogenic effects in causing cardiovascular defects, specifically heart malformations if prescribed in the first trimester 24.
In some women, paroxetine may raise the levels of a hormone called prolactin 141. High levels of prolactin can stop ovulation (part of the menstrual cycle when an ovary releases an egg). This can make it harder to get pregnant. Paroxetine has also been associated with changes in sexual function such as less desire to have sex 141.
Miscarriage is common and can occur in any pregnancy for many different reasons. Some studies suggest that taking paroxetine may slightly increase the chance of miscarriage. However, research also shows that depression itself may increase the chance of miscarriage. This makes it hard to know if an increased chance of miscarriage is due to medication, the underlying condition, or other factors.
Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. Some studies suggest that exposure to paroxetine in the first trimester might be associated with a small increased chance for heart defects. Other studies did not find a possible increased risk. The background rate of heart defects for any pregnancy is about 1 in 100 (1%). If there is an increased chance of birth defects with paroxetine use in the first trimester, it is expected to be small. Paroxetine exposure in pregnancy has not been shown to increase the chance of other birth defects.
Some studies suggest a higher chance for preterm delivery (birth before week 37) with the use of an SSRI such as paroxetine, while others do not. Conditions such as depression may increase the chance of pregnancy-related problems, such as preterm delivery. This makes it hard to know if it is the medication, the condition being treating, or other factors that are increasing the chance of pregnancy-related problems.
Some, but not all, studies have suggested that when women who are pregnant take SSRIs during the second half of the pregnancy, their babies might have a higher chance for a serious lung condition called persistent pulmonary hypertension 141. Persistent pulmonary hypertension happens in 1 or 2 out of 1,000 births. Among the studies looking at this, the overall chance for pulmonary hypertension when an SSRI was used in pregnancy was less than 1/100 (less than 1%).
The use of paroxetine during pregnancy can cause temporary symptoms in newborns soon after birth. These symptoms are sometimes referred to as withdrawal. Symptoms may include jitteriness, increased muscle tone, irritability, changes in sleep patterns, tremors, trouble eating, and trouble breathing. These symptoms are usually mild and go away on their own. Some babies may need to stay in a special care nursery for several days. Not all babies exposed to paroxetine will have these symptoms. It is important that your doctor know you are taking paroxetine so that if symptoms occur your baby can get the care that’s best for them.
It is not known if paroxetine can increase the chance for behavior or learning issues. One study looking at prescriptions for SSRIs including paroxetine suggested an increased chance of autism spectrum disorder. Studies based on filled prescriptions/prescription records cannot tell if a person took the medication, so it is hard to know if the outcomes are related to the medication or other factors. Also, this study did not look at factors such as other exposures, paternal mental illness, or other family history of autism. Another prescription study did not report an increased chance for autism spectrum disorder.
One study looking at pregnancies exposed at least during the third trimester to SSRIs including paroxetine reported no differences in developmental outcomes between the exposed 46 infants or the unexposed 23 infants at 2 and 8 months of age. A follow-up study on some of these children found no difference in behaviors such as emotional reactivity, withdrawal, irritability, depression, or anxiety in the exposed group (22 children) when compared to the group that was not exposed to paroxetine (14 children).
Breastfeeding
Paroxetine passes into breastmilk in small amounts. In some cases, mild side effects have been reported. If you suspect the baby has any symptoms (trouble sleeping, restlessness, or increased crying), contact the child’s doctor. Be sure to talk to your doctor about all your breastfeeding questions. An alternative to Paroxetine should be prescribed or you should stop breastfeeding while using Paroxetine.
Drug Interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking Paroxetine, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using Paroxetine with any of the following medicines is not recommended. Your doctor may decide not to treat you with this medication or change some of the other medicines you take.
- Bepridil
- Bromopride
- Cisapride
- Colchicine
- Dronedarone
- Isocarboxazid
- Levoketoconazole
- Linezolid
- Mavorixafor
- Mesoridazine
- Methylene Blue
- Ozanimod
- Phenelzine
- Pimozide
- Piperaquine
- Potassium Chloride
- Potassium Citrate
- Procarbazine
- Rasagiline
- Safinamide
- Saquinavir
- Selegiline
- Sparfloxacin
- Terfenadine
- Thioridazine
- Tranylcypromine
- Ziprasidone
Using Paroxetine with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Abciximab
- Abiraterone Acetate
- Abiraterone Acetate, Micronized
- Aceclofenac
- Acemetacin
- Acenocoumarol
- Adagrasib
- Alfentanil
- Alfuzosin
- Almotriptan
- Amantadine
- Amineptine
- Amiodarone
- Amisulpride
- Amitriptyline
- Amitriptylinoxide
- Amoxapine
- Amphetamine
- Amtolmetin Guacil
- Anagrelide
- Anileridine
- Apixaban
- Apomorphine
- Ardeparin
- Argatroban
- Aripiprazole
- Aripiprazole Lauroxil
- Arsenic Trioxide
- Asenapine
- Aspirin
- Astemizole
- Atazanavir
- Atomoxetine
- Azathioprine
- Azithromycin
- Bedaquiline
- Bemiparin
- Benzhydrocodone
- Benzphetamine
- Betrixaban
- Plus many more not on this list.
Using Paroxetine with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Amprenavir
- Cimetidine
- Cyproheptadine
- Fluphenazine
- Fosamprenavir
- Ginkgo
- Metoprolol
- Phenytoin
Paroxetine dosage
The dose of Paroxetine will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of Paroxetine. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
Oral dosage form (capsules)
- For moderate to severe hot flashes caused by menopause
- Adults: 7.5 milligrams (mg) once a day, at bedtime.
- Children: Use is not recommended.
Oral dosage form (suspension)
Depression
- Adults: At first, 20 milligrams (mg) (10 milliliters [mL]) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg (25 mL) per day.
- Older adults: At first, 10 mg (5 mL) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg (20 mL) per day.
- Children: Use and dose must be determined by your doctor.
Generalized anxiety disorder (GAD)
- Adults: At first, 20 milligrams (mg) (10 milliliters [mL]) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg (25 mL) per day.
- Older adults: At first, 10 mg (5 mL) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg (20 mL) per day.
- Children: Use and dose must be determined by your doctor.
Obsessive-compulsive disorder (OCD)
- Adults: At first, 20 milligrams (mg) (10 milliliters [mL]) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 60 mg (30 mL) per day.
- Older adults: At first, 10 mg (5 mL) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg (20 mL) per day.
- Children: Use and dose must be determined by your doctor.
Panic disorder
- Adults: At first, 10 milligrams (mg) (5 milliliters [mL]) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 60 mg (30 mL) per day.
- Older adults: At first, 10 mg (5 mL) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg (20 mL) per day.
- Children: Use and dose must be determined by your doctor.
Post traumatic stress disorder (PTSD)
- Adults: At first, 20 milligrams (mg) (10 milliliters [mL]) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg (25 mL) per day.
- Older adults: At first, 10 mg (5 mL) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 40 mg (20 mL) per day.
- Children: Use and dose must be determined by your doctor.
Social anxiety disorder
- Adults: At first, 20 milligrams (mg) (10 milliliters [mL]) once a day, usually taken in the morning.
- Older adults: At first, 10 mg (5 mL) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 20 mg (10 mL) per day.
- Children: Use and dose must be determined by your doctor.
Oral dosage form (tablets)
Depression
- Adults: At first, 20 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg per day.
- Older adults: At first, 10 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg per day.
- Children: Use and dose must be determined by your doctor.
Generalized anxiety disorder (GAD)
- Adults: At first, 20 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg per day.
- Older adults: At first, 10 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 40 mg per day.
- Children: Use and dose must be determined by your doctor.
Obsessive-compulsive disorder (OCD)
- Adults: At first, 20 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 60 mg per day.
- Older adults: At first, 10 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg per day.
- Children: Use and dose must be determined by your doctor.
Panic disorder
- Adults: At first, 10 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 60 mg per day.
- Older adults: At first, 10 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg per day.
- Children: Use and dose must be determined by your doctor.
Post traumatic stress disorder (PTSD)
- Adults: At first, 20 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 50 mg per day.
- Older adults: At first, 10 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 40 mg per day.
- Children: Use and dose must be determined by your doctor.
Social anxiety disorder
- Adults: At first, 20 milligrams (mg) once a day, usually taken in the morning.
- Older adults: At first, 10 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 20 mg per day.
- Children: Use and dose must be determined by your doctor.
Oral dosage form (extended-release tablets)
Depression
- Adults: At first, 25 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 62.5 mg per day.
- Older adults: At first, 12.5 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg per day.
- Children: Use and dose must be determined by your doctor.
Panic disorder
- Adults: At first, 12.5 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose usually is not more than 75 mg per day.
- Older adults: At first, 12.5 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 50 mg per day.
- Children: Use and dose must be determined by your doctor.
Premenstrual dysphoric disorder (PMDD)
- Adults: At first, 12.5 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 25 mg per day.
- Older adults and children: Use and dose must be determined by your doctor.
Social anxiety disorder
- Adults: At first, 12.5 milligrams (mg) once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 37.5 mg per day.
- Older adults: At first, 12.5 mg once a day, usually taken in the morning. Your doctor may adjust your dose as needed. However, the dose is usually not more than 37.5 mg per day.
- Children: Use and dose must be determined by your doctor.
Missed Dose
If you miss a dose of Paroxetine, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Kidney impairment
For patients with kidney impairment, Paroxetine dosage is based on Creatinine clearance (CrCl), as shown below.
- If the Creatinine clearance (CrCl) is 30 to 60 ml per minute: No need to change the dosing.
- If Creatinine clearance (CrCl) is less than 30 ml per minute:
- Immediate release formulation: 10 mg per day; increase if needed by 10 mg per day increments at an interval of at least a week; maximum dose: 40 mg per day.
- Controlled release formulation: 12.5 mg per day; increase if needed by 12.5 mg per day increments at interval one week; maximum dose: 50 mg per day.
Liver impairment
In liver impairment, Paroxetine plasma concertation of two times normal can occur.
- If mild to moderate liver impairment: no change in dosage.
- If severe liver impairment:
- Immediate-release formulations: 10 mg per day and, if needed, increase by 10 mg per day at intervals of 1 week; maximum dose of 40 mg per day.
- Controlled release formulation: 12.5 mg per day; increase if needed by 12.5 mg per day increments at intervals of 1 week; maximum dose is 50 mg per day.
Monitoring
Patients initiated on paroxetine should initially receive close observation and be monitored for worsening clinical symptoms, behavior changes (mania, social function, anxiety), or suicidal ideations. Labs should include serum sodium concentration to rule out syndrome of inappropriate antidiuretic hormone secretion (SIADH) 142. Vital signs should be monitored for signs of serotonin syndrome (serotonergic toxicity). Serotonin syndrome precipitates via the manifestation of changes in mental status, autonomic instability, gastrointestinal symptoms, hyperreflexia, and myoclonus. Serotonin syndrome is treated by discontinuing any of the offending agents. If symptoms continue to escalate, the clinician can administer cyproheptadine 143.
Paroxetine side effects
Paroxetine may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- headache
- dizziness
- weakness
- difficulty concentrating
- nervousness
- forgetfulness
- confusion
- sleepiness
- nausea
- vomiting
- diarrhea
- constipation
- gas
- stomach pain
- heartburn
- changes in ability to taste food
- decreased appetite
- weight loss or gain
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or unable to have an orgasm
- dry mouth
- sweating
- yawning
- pain in the back, muscles, bones, or anywhere in the body
- tenderness or swelling of joints
Some side effects can be serious. If you experience any of the following symptoms or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS sections, call your doctor immediately or get emergency medical treatment:
- seeing things or hearing voices that do not exist (hallucinating)
- fainting
- rapid, pounding, or irregular heartbeat
- chest pain
- difficulty breathing
- seizures
- agitation, fever, sweating, confusion, fast or irregular heartbeat, and severe muscle stiffness or twitching, hallucinations, loss of coordination, nausea, vomiting, or diarrhea
- abnormal bleeding or bruising
- tiny red spots directly under the skin
- peeling or blistering of skin
- sore throat, fever, chills, cough, and other signs of infection
- uncontrollable shaking of a part of the body
- unsteady walking that may cause falling
- numbness or tingling in your hands, feet, arms, or legs
- painful erection that lasts for hours
- sudden nausea, vomiting, weakness, cramping, bloating, swelling, tightness in hands and feet, dizziness, headache and/or confusion
- hives
- rash
- itching
- swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs
- hoarseness
- black and tarry stools
- red blood in stools
- bloody vomit
- vomit that looks like coffee grounds
- bone pain or fracture
- tenderness, swelling, or bruising of one part of your body
Paroxetine may decrease appetite and cause weight loss in children. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight while he or she is taking this medication. Talk to your child’s doctor about the risks of giving paroxetine to your child.
Paroxetine may cause other side effects. See your doctor if you have any unusual problems while taking Paroxetine.
Paroxetine discontinuation syndrome
Discontinuation syndrome is more common and more severe with paroxetine than with other SSRIs; this may be due in part to the fact that it inhibits its own metabolism 134. Withdrawal symptoms from Paroxetine discontinuation include dizziness, lethargy, nausea, vomiting, headache, fever, chills, vivid dreams, electric shock-like-sensation, dyskinesia, anxiety, crying, irritability, and depersonalization 144.
Paroxetine Toxicity
Paroxetine is rarely lethal in overdose. In Paroxetine overdose, patients can develop somnolence, nausea, tremor, heart rhythm disturbances, confusion, vomiting, dizziness, and mydriasis. During Paroxetine overdose, a patient’s airway, oxygenation, and ventilation require evaluation first. The treatment for Paroxetine overdose includes symptomatic supportive treatment. There is no specific treatment for paroxetine toxicity 134.
Sertraline
Sertraline is a selective serotonin reuptake inhibitor (SSRI) medication that has been used to treat depression, obsessive-compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), panic attacks (sudden, unexpected attacks of extreme fear and worry about these attacks), and major anxiety disorders including social anxiety disorder, post-trauma stress disorder (PTSD, disturbing psychological symptoms that develop after a frightening experience) and generalized anxiety disorder (GAD), panic disorder, premenstrual dysphoric disorder [PMDD] (a severe form of premenstrual syndrome [PMS] with mood swings, irritability, bloating, and breast tenderness), and social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life) 145. Sertraline is also used for headache, diabetic neuropathy and premature ejaculation. Sertraline works by blocking the reuptake of serotonin in your brain neurons, thus increasing serotonin levels in your brain which is associated with its psychiatric effects.
Sertraline was approved for use in the United States in 1991, and it remains in wide use, with almost 40 million prescriptions being filled yearly 146.
Sertraline is available as tablets of 25, 50 and 100 mg and as an oral suspension (liquid) in multiple generic forms and under the brand name of Zoloft. Sertraline is usually taken once daily in the morning or evening. The recommended dosage for depression in adults is 50 or 100 mg once daily, increasing the dosage by 25 or 50 mg increments to a maximum of 200 mg. Take sertraline at around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take sertraline exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
To treat premenstrual dysphoric disorder (PMDD), sertraline is taken once a day, either every day of the month or on certain days of the month.
Sertraline concentrate must be diluted before use. Immediately before taking it, use the provided dropper to remove the amount of concentrate your doctor has told you to take. Mix the concentrate with 4 ounces (1/2 cup [120 milliliters]) of water, ginger ale, lemon or lime soda, lemonade, or orange juice. After mixing, the diluted solution may be hazy; this is normal. Do not mix the concentrate with any liquids other than the ones listed. Drink the diluted solution immediately.
Your doctor may start you on a low dose of sertraline and gradually increase your dose, not more than once a week.
It may take a few weeks or longer before you feel the full benefit of sertraline. Continue to take sertraline even if you feel well. Do not stop taking sertraline without talking to your doctor. If you suddenly stop taking sertraline, you may experience withdrawal symptoms such as nausea, sweating, depression, mood changes, frenzied or abnormally excited mood, irritability, anxiety, confusion, dizziness, headache, tiredness, seizures, ringing in the ears, numbness or tingling in the arms, legs, hands, or feet, difficulty falling asleep or staying asleep.
Common side effects of Sertraline are drowsiness, dyspepsia, nausea, headache, increased sweating, increased appetite, weight gain and sexual dysfunction. Rare but potentially severe adverse events include suicidal ideation and behavior, activation of mania, serotonin syndrome, discontinuation syndrome, increased risk of bleeding, seizures, acute glaucoma, hypersensitivity reactions and embryo-fetal toxicity.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as sertraline during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, experts are not sure about how great this risk is and how much it should be considered in deciding whether a child or teenager should take an antidepressant.
You should know that your mental health may change in unexpected ways when you take sertraline or other antidepressants even if you are an adult over 24 years of age. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; new or worsening anxiety; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; and frenzied abnormal excitement. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking sertraline, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
The doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with sertraline. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter what your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. This risk is higher if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood) or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
How does Sertraline work?
Sertraline is an antidepressant medication within the selective serotonin reuptake inhibitors (SSRIs) class. Sertraline is an antidepressant with primarily inhibitory effects on presynaptic serotonin reuptake. This inhibition of serotonin reuptake results in an accumulation of serotonin in your brain neurons. Serotonin in the central nervous system plays a role in regulating mood, personality, and wakefulness, which is why blocking serotonin reuptake is beneficial in disorders such as major depression 147.
Sertraline also has minimal effects on norepinephrine and dopamine uptake, and research has shown that Sertraline has more dopaminergic activity than other medications in the same SSRI class. Sertraline’s mechanism of action makes it highly efficacious when used in the treatment of various psychiatric conditions 148, 87.
What is Sertraline used for?
Sertraline is a selective serotonin reuptake inhibitor (SSRI) medication that has been used to treat depression, obsessive-compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), panic attacks (sudden, unexpected attacks of extreme fear and worry about these attacks), and major anxiety disorders including social anxiety disorder, post-trauma stress disorder (PTSD, disturbing psychological symptoms that develop after a frightening experience) and generalized anxiety disorder (GAD), panic disorder, premenstrual dysphoric disorder [PMDD] (a severe form of premenstrual syndrome [PMS] with mood swings, irritability, bloating, and breast tenderness), and social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life) 145. Sertraline is also used for headache, diabetic neuropathy and premature ejaculation. Sertraline works by blocking the reuptake of serotonin in your brain neurons, thus increasing serotonin levels in your brain which is associated with its psychiatric effects.
FDA-approved uses
- Sertraline is an antidepressant used as a first-line treatment of major depressive disorder 147
- Obsessive-compulsive disorder (OCD) 149, 150
- Panic disorder 151
- Post-traumatic stress disorder (PTSD) 152
- Premenstrual dysphoric disorder (PMDD), a severe form of premenstrual syndrome (PMS) characterized by significant mood disturbances, irritability, and other symptoms that interfere with daily life, occurring in the week or two before menstruation
- Social anxiety disorder (social phobia)
Non-FDA-approved uses
- Binge eating disorder 153
- Body dysmorphic disorder
- Bulimia nervosa 153
- Generalized anxiety disorder (GAD)
- Premature ejaculation.
Sertraline Contraindications
Sertraline is contraindicated in patients with documented hypersensitivity to the drug or its components. The coadministration of sertraline with thioridazine, pimozide, or monoamine oxidase inhibitors (MAOIs), including linezolid or methylene blue, is also contraindicated. Patients who are taking other serotonergic medications should receive education regarding the risks of coadministration with sertraline 154.
Sertraline solution is contraindicated with disulfiram as solution form contains 12% alcohol, and it may cause an alcohol-disulfiram reaction.
Sertraline therapy should not start within two weeks of discontinuing any monoamine oxidase (MAO) inhibitor such as isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate) to prevent toxicity with serotonin syndrome 154. Wait at least 14 days after stopping an MAO inhibitor before you take sertraline.
There is a US black box warning for use in children and young adults. Use caution in patients ages 18 to 24 years old due to the risk of an increase in suicidal ideation 155.
Before taking Sertraline
You should not use sertraline if you are allergic to it, or if you also take pimozide. Do not use the liquid form of Sertraline if you take disulfiram (Antabuse).
if you have used an MAO inhibitor in the past 14 days, a dangerous drug interaction could occur. MAO inhibitors include isocarboxazid, linezolid, methylene blue injection, phenelzine, and tranylcypromine. Wait at least 14 days after stopping an MAO inhibitor before you take sertraline.
Tell your doctor if you also take stimulant medicine, opioid medicine, herbal products, or medicine for depression, mental illness, Parkinson’s disease, migraine headaches, serious infections, or prevention of nausea and vomiting. An interaction with sertraline could cause a serious condition called serotonin syndrome.
To make sure sertraline is safe for you, tell your doctor if you have ever had:
- An allergy or sensitivity to aspirin or tartrazine (food dye) or latex (Zoloft oral solution – the dropper dispenser contains natural rubber)
- Bipolar disorder (mood disorder with mania and depression)
- Bleeding problems or if you take warfarin (Coumadin, Jantoven)
- Diabetes
- Angle-closure glaucoma. You should know that Paroxetine may cause angle-closure glaucoma, a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision. Talk to your doctor about having an eye examination before you start taking Paroxetine. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, see your doctor or get emergency medical treatment right away.
- Heart rhythm problems (eg, long QT syndrome)
- High blood pressure
- Hyponatremia (low sodium in the blood)
- Mania or hypomania
- Purpura (purplish or brownish-red discoloration of the skin)
- Seizures
- Sexual problems: Use with caution. May make these conditions worse.
- Kidney disease: Product labeling does not report any dose adjustment based on the patient’s renal function.
- Liver disease: Use with caution. The effects may be increased because of slower removal of the medicine from the body.
- Stroke
Some young people may have increased suicidal thoughts when first starting a medicine to treat depression. Your doctor will need to check your progress on a regular basis. Your family or caregivers should also watch for sudden changes in your behavior.
Sertraline is approved for use in children at least 6 years old, only to treat obsessive-compulsive disorder but not depression.
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to Sertraline or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies have not been performed on the relationship of age to the effects of sertraline in children with depression, panic disorder, premenstrual dysphoric disorder (PMDD), posttraumatic stress disorder (PTSD), and social anxiety disorder (SAD), and in children younger than 6 years of age with obsessive-compulsive disorder. Safety and efficacy have not been established.
Elderly
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of sertraline in the elderly. However, elderly patients are more likely to have hyponatremia (low sodium in the blood), age-related kidney, liver, or heart problems which may require caution and an adjustment in the dose for patients receiving sertraline.
Pregnancy
It is not known if sertraline can make it harder to get pregnant. One study found that women who take SSRIs have a slightly lower chance of getting pregnant. However, some conditions, including depression, can make it harder to get pregnant. This makes it hard to know if the medication, the condition being treated, or other factors might affect fertility.
Miscarriage is common and can occur in any pregnancy for many different reasons. Use of sertraline and the chance of miscarriage has not been well studied. One study found no differences in the chance of miscarriage in women who filled prescriptions for sertraline during the first 35 days of pregnancy and those who stopped filling prescriptions before pregnancy. Also, some conditions, including depression, may increase the chance of miscarriage. This makes it hard to know if the medication, the condition being treated, or other factors might affect the chance of miscarriage.
Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. There are reports of more than 25,000 pregnancies exposed to sertraline. Some studies have suggested an increased chance for heart defects or other birth defects. However, most studies have not found an increased chance of birth defects when sertraline is used in pregnancy. Overall, the available data does not suggest that sertraline increases the chance of birth defects above the background risk.
Some studies suggest a higher chance for pregnancy-related problems, such as preterm delivery (birth before week 37) or low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth) with the use of sertraline in pregnancy. However, research has also shown that when conditions such as depression or anxiety are untreated or undertreated during pregnancy, there could be an increased chance for pregnancy complications. This makes it hard to know if it is the medication, the underlying condition, or other factors that might increase the chance for these problems.
Some, but not all, studies have suggested that when women who are pregnant take SSRIs during the second half of pregnancy, their babies might have an increased chance for a serious lung condition called persistent pulmonary hypertension (PPH). Persistent pulmonary hypertension happens in 1 or 2 out of 1,000 births. A recent report that combined results from several studies suggested the chance for persistent pulmonary hypertension might be increased if an SSRI was used during pregnancy. However, it was not clear if this was due to medication exposure or to other exposures that people who take SSRIs have in common, such as higher rates of smoking. Data from studies suggest the overall chance for persistent pulmonary hypertension when an SSRI is used in pregnancy is less than 1/100 (less than 1%).
The use of sertraline during pregnancy can cause temporary symptoms in newborns soon after birth. These symptoms are sometimes referred to as withdrawal. Symptoms can include irritability, jitteriness, tremors (shivering), constant crying, changes in sleep patterns, lower muscle tone (hypotonia), skin discoloration (cyanosis), problems with eating, trouble controlling body temperature, and problems with breathing (apnea). In most cases, these symptoms are mild and go away within a couple weeks with no treatment required. Some babies may need to stay in the nursery or neonatal intensive care unit (NICU) until the symptoms go away. Not all babies exposed to sertraline will have these symptoms. It is important that your doctor know you are taking sertraline so that if symptoms do occur, your baby can get the care that is best for them.
One study on a small number of children who were exposed to SSRIs during pregnancy reported a lower score on motor skill tests than other children. Another small study looked at behaviors in children ages 4-5 years old. This study found no difference in behavior between children who were exposed to sertraline or other SSRIs during pregnancy and those children who were not.
Breastfeeding
Sertraline gets into breastmilk in small amounts 156. Most reports show no problems for babies who are exposed to sertraline through breast milk 157. Babies who were also exposed to sertraline in the third trimester of pregnancy may have a lower chance of withdrawal after birth if they are breastfed. Most reviewers consider sertraline a preferred antidepressants during breastfeeding 158, 159, 160, 161, 162, 157, 163, 164, 165. Be sure to talk to your doctor about all your breastfeeding questions.
Drug Interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking Sertraline, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using Sertraline with any of the following medicines is not recommended. Your doctor may decide not to treat you with this medication or change some of the other medicines you take.
- Bepridil
- Bromopride
- Cisapride
- Dronedarone
- Fluconazole
- Furazolidone
- Iproniazid
- Isocarboxazid
- Ketoconazole
- Levoketoconazole
- Linezolid
- Mesoridazine
- Methylene Blue
- Metoclopramide
- Ozanimod
- Phenelzine
- Pimozide
- Piperaquine
- Posaconazole
- Procarbazine
- Rasagiline
- Safinamide
- Saquinavir
- Selegiline
- Sparfloxacin
- Terfenadine
- Thioridazine
- Toloxatone
- Tranylcypromine
- Ziprasidone
Using Sertraline with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Abciximab
- Aceclofenac
- Acemetacin
- Acenocoumarol
- Adagrasib
- Alfentanil
- Alfuzosin
- Almotriptan
- Amineptine
- Amiodarone
- Amisulpride
- Amitriptyline
- Amitriptylinoxide
- Amoxapine
- Amphetamine
- Amtolmetin Guacil
- Anagrelide
- Anileridine
- Apixaban
- Apomorphine
- Ardeparin
- Argatroban
- Aripiprazole
- Aripiprazole Lauroxil
- Arsenic Trioxide
- Asenapine
- Aspirin
- Astemizole
- Atazanavir
- Atomoxetine
- Avacopan
- Azithromycin
- Bedaquiline
- Bemiparin
- Benzhydrocodone
- Benzphetamine
- Betrixaban
- Bivalirudin
- Bromfenac
- Brompheniramine
- Plus many more not on this list.
Using Sertraline with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Alprazolam
- Cimetidine
- Fluphenazine
- Ginkgo
- Lamotrigine
- Mavacamten
- Rifampin
Sertraline dosage
The dose of Sertraline will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of Sertraline. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
For oral dosage forms (solution or tablets)
- For depression
- Adults: At first, 50 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children: Use and dose must be determined by your doctor.
- For obsessive-compulsive disorder (OCD)
- Adults and teenagers: At first, 50 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children 6 to 12 years of age: At first, 25 mg once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children younger than 6 years of age: Use and dose must be determined by your doctor.
- For panic disorder, posttraumatic stress disorder (PTSD) or social anxiety disorder
- Adults: At first, 25 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children: Use and dose must be determined by your doctor.
- For premenstrual dysphoric disorder (PMDD)
- Adults: At first, 50 milligrams (mg) once a day throughout your menstrual cycle or just during the premenstrual time. Your doctor may adjust your dose as needed. However, the dose is usually not more than 150 mg per day throughout your menstrual cycle or 100 mg per day if you are only taking it during your premenstrual time.
- Children: Use and dose must be determined by your doctor.
Missed Dose
If you miss a dose of Sertraline, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Monitoring
It is essential to monitor patients for unusual changes in behavior, anxiety, suicidality, or any other clinical signs of worsening illness. Regularly evaluate for depression and suicidality, especially when changing the dose of sertraline. Sertraline may also precipitate mania in patients at risk for bipolar disorder. Monitor for symptoms of mania in patients who are started on sertraline, especially if they have a family history of mania or bipolar disorder 166.
Monitor for abnormal bleeding, adverse effects of medication use, or withdrawal symptoms from abrupt discontinuation in patients taking sertraline. The abnormal bleeding may primarily occur if used concurrently with aspirin, non-steroidal anti-inflammatory drugs (NSAIDs), warfarin, or other anticoagulants, as sertraline may impair platelet aggregation and cause bruising, epistaxis, or hemorrhage 167.
For geriatric patients, monitor for changes in mental status, and check their sodium concentration regularly due to the risk of syndrome of inappropriate antidiuretic hormone secretion (SIADH) or hyponatremia.
Sertraline is considered safe in patients with a history of myocardial infarction, heart failure, and other cardiac conditions. However, due to the minor effect of QT prolongation, it may benefit the provider to monitor the QT interval with electrocardiograms 168, 169.
When treating pregnant women with sertraline during the third trimester, the physician should consider tapering sertraline in the third trimester by risk-benefit analysis 170, 157.
Sertraline side effects
Sertraline may cause side effects. See your doctor if any of these symptoms are severe or do not go away:
- nausea
- diarrhea
- constipation
- vomiting
- difficulty falling asleep or staying asleep
- dry mouth
- heartburn
- loss of appetite
- weight changes
- dizziness
- excessive tiredness
- headache
- nervousness
- uncontrollable shaking of a part of the body
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or unable to have an orgasm
- excessive sweating
Some side effects can be serious. If you experience any of the following symptoms or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS section, see your doctor immediately:
- seizures
- abnormal bleeding or bruising
- agitation, hallucinations, fever, sweating, confusion, fast heartbeat, shivering, severe muscle stiffness or twitching, loss of coordination, nausea, vomiting, or diarrhea
- headache, weakness, unsteadiness, confusion, or memory problems
- rash
- hives
- swelling
- difficulty breathing
Sertraline may decrease appetite and cause weight loss in children. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight while he or she is taking this medication. Talk to your child’s doctor about the risks of giving sertraline to your child.
Sertraline may cause other side effects. Call your doctor if you have any unusual problems while taking Sertraline.
Sertraline Withdrawal
Discontinuation of serotonergic antidepressants may cause adverse reactions, particularly when the discontinuation is abrupt. Symptoms include nausea, diaphoresis, dysphoric mood, irritability, agitation, vertigo, sensory disturbances (e.g., paresthesia, electric shock sensations), tremor, anxiety, confusion, cephalgia, lethargy, emotional lability, sleep disorder, hypomania, tinnitus, and seizures. Therefore, it is preferable to reduce the dosage gradually rather than stop immediately whenever possible.
Sertraline Overdose
The overdose of sertraline is generally well-tolerated. Sertraline overdose may result in serotonin syndrome, resulting in myoclonus, muscle rigidity, diaphoresis, tremor, hyperreflexia, agitated delirium, and hyperthermia. Treatment of serotonin syndrome requires discontinuing the medication and supportive care. Consider antiemetics (non-serotonergic), benzodiazepines, and standard cooling measures for symptom relief. The patient can also receive serotonin antagonists such as cyproheptadine. If severe serotonin syndrome and the patient develops muscular rigidity and hyperthermia with body temperatures higher than 41 degrees C, consider sedation, endotracheal intubation, external cooling, and neuromuscular paralysis. It is important to note that antipyretics are likely not beneficial to patients experiencing hyperthermia due to serotonin syndrome 171.
Vilazodone
Vilazodone is a serotonin reuptake inhibitor (SSRI) and partial serotonin (5-HT1A) receptor agonist that is used in treatment of major depressive disorder 172, 173, 174, 175, 176, 177. Vilazodone is an antidepressant that is thought to work through the modulation of serotonin neurotransmission in the central nervous system (brain and spinal cord), including the inhibition of serotonin reuptake at the serotonin transporter (SERT), an increased amount of serotonin (5-hydroxytryptamine or 5HT) remains in the synaptic cleft and can stimulate postsynaptic receptors for a more extended period 178. Because of these characteristics, vilazodone has been termed a serotonin partial agonist–reuptake inhibitor (SPARI) 178, 175.
Vilazodone was approved for use in the United States in 2011 for use in treatment of major depressive disorder 179, 180, 176. However, there is limited clinical experience with its use.
Vilazodone is available as tablets of 10, 20 and 40 mg under the brand name Viibryd 180. Take vilazodone at around the same time every day. The recommended starting dosage of vilazodone in adults is 10 mg per day for adults younger than 65 years of age, and 5 mg per day for adults 65 and older, which can then be increased to the typical maintenance dose of 40 mg once daily. Vilazodone is usually taken with food once a day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take vilazodone exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Your doctor will probably start you on a low dose of vilazodone and gradually increase your dose, not more than once every 7 days.
Vilazodone controls depression but does not cure it. It may take several weeks before you feel the full benefit of vilazodone. Continue to take vilazodone even if you feel well. Do not stop taking vilazodone without talking to your doctor. Your doctor will probably decrease your dose gradually. If you suddenly stop taking vilazodone, you may experience withdrawal symptoms such as dizziness; nausea; headache; confusion; irritability; agitation; difficulty falling asleep or staying asleep; anxiety; extreme tiredness; seizures; pain, burning, or tingling in the hands or feet; frenzied or abnormally excited mood; or sweating. Tell your doctor if you experience any of these symptoms while you are decreasing your dose of vilazodone or soon after you stop taking vilazodone.
Common, non-serious side effects of Vilazodone include diarrhea, nausea, fatigue, drowsiness, headache, insomnia, weight gain and sexual dysfunction. Vilazodone overdose is associated with acute serotonin syndrome. Rare, but potentially severe adverse effects include suicidal thinking and behavior, activation of symptoms of mania, serotonin syndrome, sexual dysfunction, hyponatremia and hypersensitivity reactions.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as vilazodone during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, experts are not sure about how great this risk is and how much it should be considered in deciding whether a child or teenager should take an antidepressant. Children younger than 18 years of age should not normally take vilazodone, but in some cases, a doctor may decide that vilazodone is the best medication to treat a child’s condition.
You should know that your mental health may change in unexpected ways when you take vilazodone or other antidepressants, even if you are an adult over 24 years of age. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; frenzied abnormal excitement; or any other changes in your usual thoughts, mood, or behavior. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking vilazodone, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with vilazodone and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. This risk is higher if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood) or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
Vilazodone mechanism of action
The mechanism of the antidepressant effect of Vilazodone is thought to be related to its enhancement of serotonergic activity in the brain through selective inhibition of serotonin reuptake 178. Vilazodone binds with high affinity to the serotonin reuptake site but not to the norepinephrine or dopamine reuptake site. As a result, vilazodone potently and selectively inhibits the reuptake of serotonin 175.
Even though vilazodone is also a partial agonist at serotonergic 5-HT1A receptors, the net result of this activity on serotonergic transmission and its role in the antidepressant effect of vilazodone are not fully understood 175.
The half-life of vilazodone is approximately 25 hours 175.
When vilazodone is taken with food, the drug’s absolute bioavailability is 72% 175. After daily dosing of vilazodone 40 mg under fed conditions, the mean maximum plasma concentration (Cmax) at steady state was 156 ng/mL, and the mean area-under-the-curve (AUC 0–24 hr) concentration was 1,645 ng • hours/mL. When vilazodone was administered with a high-fat or light meal, the mean maximum plasma concentration (Cmax) was increased by approximately 147% to 160%, and the area-under-the-curve concentration was increased by approximately 64% to 85% 175.
If vomiting occurs within 7 hours after administration, vilazodone’s absorption is decreased by about 25%; however, a replacement dose is not required 175.
Vilazodone has a large volume of distribution (value unknown). It is approximately 96% to 99% protein-bound 175.
Vilazodone is extensively metabolized in the liver, primarily via the cytochrome P450 (CYP) 3A4 isoenzyme. CYP2C19 and CYP2D6 are minor metabolic pathways. Non-CYP450 metabolism also occurs, possibly by carboxylesterase. Only 1% and 2% of the dose are recovered in urine and feces, respectively, as unchanged vilazodone.
The presence of mild or moderate kidney and liver impairment does not affect the clearance of vilazodone 175.
Vilazodone Contraindications
Because of the risk of serious, sometimes fatal, interactions with serotonergic drugs, vilazodone is contraindicated in patients taking concomitant monoamine oxidase (MAO) inhibitors or in those who have taken them within 14 days preceding vilazodone therapy 175.
What is vilazodone used for?
Vilazodone is a serotonin reuptake inhibitor (SSRI) and partial serotonin (5-HT1A) receptor agonist that is used to treat major depressive disorder 172, 173, 174, 175, 176, 177, 181, 182, 183, 184, 185, 186, 187.
Before taking Vilazodone
Before taking vilazodone:
- Tell your doctor and pharmacist if you are allergic to vilazodone, any other medications, or any of the ingredients in vilazodone tablets. Ask your pharmacist or check the Medication Guide for a list of the ingredients.
- Do not use an monoamine oxidase (MAO) inhibitor within 14 days before or 14 days after you take vilazodone. A dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate). You must wait at least 14 days after stopping an monoamine oxidase (MAO) inhibitor before you take vilazodone.
- Tell your doctor if you also take stimulant medicine, opioid medicine, herbal products, or medicine for depression, mental illness, Parkinson’s disease, migraine headaches, serious infections, or prevention of nausea and vomiting. An interaction with vilazodone could cause a serious condition called serotonin syndrome.
- Vilazodone is not approved for use by anyone younger than 18 years old.
- Some young people have thoughts about suicide when first taking an antidepressant. Your doctor should check your progress at regular visits. Your family or other caregivers should also be alert to changes in your mood or symptoms.
- Some medications should not be taken with vilazodone. Other medications may cause dosing changes or extra monitoring when taken with vilazodone. Make sure you have discussed any medications you are currently taking or plan to take before starting vilazodone with your doctor and pharmacist. Before starting, stopping, or changing any medications while taking vilazodone, please get the advice of your doctor or pharmacist.
- The following nonprescription or herbal products may interact with vilazodone: St. John’s wort; tryptophan; aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Advil, Motrin) and naproxen (Aleve). Be sure to let your doctor and pharmacist know that you are taking these medications before you start taking vilazodone. Do not start any of these medications while taking vilazodone without discussing with your doctor.
- Tell your doctor if you have a low level of sodium in your blood (hyponatremia) or glaucoma (increased pressure in the eye that may cause loss of sight), and if you drink or have ever drunk large amounts of alcohol, Also tell your doctor if you have or have ever had bleeding problems, seizures, or liver disease.
- Tell your doctor if you are pregnant, especially if you are in the last few months of your pregnancy, or if you plan to become pregnant or are breast-feeding. If you become pregnant while taking vilazodone, call your doctor. Vilazodone may cause problems in newborns following delivery if it is taken during the last months of pregnancy. If you are pregnant, your name may be listed on a pregnancy registry to track the effects of vilazodone on the baby.
- If you are having surgery, including dental surgery, tell the doctor or dentist that you are taking vilazodone.
- You should know that vilazodone may make you drowsy and affect your judgment and thinking. Do not drive a car or operate machinery until you know how this medication affects you.
- Ask your doctor about the safe use of alcoholic beverages while you are taking vilazodone. Alcohol can make the side effects from vilazodone worse.
- You should know that vilazodone may cause angle-closure glaucoma (a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision). Talk to your doctor about having an eye examination before you start taking this medication. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, call your doctor or get emergency medical treatment right away.
Tell your doctor about all your current medicines. Many drugs can affect vilazodone, especially:
- any other antidepressants
- mephenytoin
- St. John’s wort
- tramadol
- a diuretic or “water pill”
- medicine to treat anxiety, mood disorders, or mental illness such as schizophrenia
- a blood thinner: warfarin, Coumadin, Jantoven
- migraine headache medicine: sumatriptan, Imitrex, Maxalt, Treximet, and others.
This list is not complete and many other drugs may affect vilazodone. This includes prescription and over-the-counter medicines, vitamins, and herbal products. Not all possible drug interactions are listed here.
Pregnancy
It is not known if vilazodone can make it harder to get pregnant 188.
Miscarriage is common and can occur in any pregnancy for many different reasons. Studies have not been done to see if vilazodone increases the chance for miscarriage. However, depression itself might increase the chance for miscarriage.
Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. Animal studies did not find an increased chance of birth defects. We have been unable to locate studies on the use of vilazodone in human pregnancies.
Studies have not been done to see if vilazodone can cause other pregnancy-related problems, such as preterm delivery (birth before week 37) or low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth).
It is not known if the use of vilazodone during pregnancy can cause withdrawal symptoms in a baby after birth. The use of other antidepressants during pregnancy has been associated with temporary symptoms in some newborns after birth. These symptoms are sometimes referred to as withdrawal. Symptoms may include jitteriness, increased muscle tone, irritability, changes in sleep patterns, tremors, trouble eating, and trouble breathing. These symptoms are usually mild and go away on their own. Some babies may need to stay in a special care nursery for several days. Not all babies exposed to an antidepressant will have these symptoms. It is important that your doctor know you are taking vilazodone so that if symptoms occur your baby can get the best care.
Studies have not been done to see if vilazodone use in pregnancy can cause behavior or learning issues for the child.
Breastfeeding
It is not known if vilazodone gets into breast milk or causes side effects for a baby who receives the milk. The benefit of continuing vilazodone while breastfeeding may outweigh the risks of an untreated mental health condition or the risks of not breastfeeding. Your doctor can talk with you about vilazodone and what treatment is best for you. Be sure to talk to your doctor about all of your breastfeeding questions.
Vilazodone dosage
Adult Dose for Depression
- Initial dose: 10 mg orally once a day for 7 days, followed by 20 mg orally once a day for an additional 7 days
- Maintenance dose: 40 mg orally once a day
Take vilazodone with food 7.
Missed Dose
If you miss a dose of vilazodone, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Monitoring
Patients who are taking vilazodone should be monitored for clinical worsening and for suicidal thinking or behavior, especially during the initial few months and at times of dose increases or decreases).
Serotonergic drugs such as vilazodone have been associated with withdrawal symptoms upon discontinuation, including dysphoric mood, irritability, agitation, anxiety, and confusion. Patients should be monitored for these symptoms when discontinuing vilazodone.
The most severe form of serotonin syndrome resembles neuroleptic malignant syndrome (NMS) and is characterized by hyperthermia, muscle rigidity, autonomic instability with possible rapid fluctuation of vital signs, and alterations in mental status. Patients should be monitored for the emergence of serotonin syndrome or neuroleptic malignant syndrome (NMS) -like signs and symptoms.
Because of the potential for increased bleeding, patients receiving warfarin therapy should be carefully monitored when vilazodone is initiated or discontinued.
Vilazodone side effects
Vilazodone may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- dry mouth
- increased appetite
- heartburn
- gas
- dizziness
- pain, burning, or tingling in the hands or feet
- uncontrollable shaking of a part of the body
- unusual dreams
- tiredness
- joint pain
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or unable to have an orgasm
Some side effects can be serious. If you experience any of these symptoms or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS sections, see your doctor immediately:
- rash
- hives
- swelling
- difficulty breathing
- loss of consciousness
- seizures
- fever, sweating, confusion, fast or irregular heartbeat, and severe muscle stiffness or twitching, agitation, hallucinations, loss of coordination, nausea, vomiting, or diarrhea
- unusual bleeding or bruising
- nosebleeds
- small red or purple dots on the skin
- hallucinations (seeing things or hearing voices that do not exist)
- headache
- difficulty concentrating
- memory problems
- weakness
- problems with coordination
- increased falls
- fainting
Vilazodone may cause other side effects. See your doctor if you have any unusual problems while taking Vilazodone.
- Chu A, Wadhwa R. Selective Serotonin Reuptake Inhibitors. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554406[↩][↩][↩][↩][↩]
- Bruggeman C, O’Day CS. Selective Serotonin Reuptake Inhibitor Toxicity. [Updated 2023 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534815[↩][↩]
- Bakshi A, Tadi P. Biochemistry, Serotonin. [Updated 2022 Oct 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560856[↩]
- Smith C, Smith M, Cunningham R, Davis S. Recent Advances in Antiemetics: New Formulations of 5-HT3 Receptor Antagonists in Adults. Cancer Nurs. 2020 Jul/Aug;43(4):E217-E228. doi: 10.1097/NCC.0000000000000694[↩]
- David DJ, Gardier AM. Les bases de pharmacologie fondamentale du système sérotoninergique : application à la réponse antidépressive [The pharmacological basis of the serotonin system: Application to antidepressant response]. Encephale. 2016 Jun;42(3):255-63. French. doi: 10.1016/j.encep.2016.03.012[↩]
- Antosik-Wójcińska AZ, Stefanowski B, Święcicki Ł. Efficacy and safety of antidepressant’s use in the treatment of depressive episodes in bipolar disorder – review of research. Psychiatr Pol. 2015;49(6):1223-39. English, Polish. doi: 10.12740/PP/37914[↩][↩]
- Preskorn SH. Clinically relevant pharmacology of selective serotonin reuptake inhibitors. An overview with emphasis on pharmacokinetics and effects on oxidative drug metabolism. Clin Pharmacokinet. 1997;32 Suppl 1:1-21. doi: 10.2165/00003088-199700321-00003[↩][↩][↩][↩]
- Feighner JP. Mechanism of action of antidepressant medications. J Clin Psychiatry. 1999;60 Suppl 4:4-11; discussion 12-3. https://www.psychiatrist.com/pdf/mechanism-of-action-of-antidepressant-medications-pdf/[↩]
- Delgado PL. How antidepressants help depression: mechanisms of action and clinical response. J Clin Psychiatry. 2004;65 Suppl 4:25-30. https://www.psychiatrist.com/pdf/how-antidepressants-help-depression-mechanisms-of-action-and-clinical-response-pdf/[↩]
- Xue W, Wang P, Li B, Li Y, Xu X, Yang F, Yao X, Chen YZ, Xu F, Zhu F. Identification of the inhibitory mechanism of FDA approved selective serotonin reuptake inhibitors: an insight from molecular dynamics simulation study. Phys Chem Chem Phys. 2016 Jan 28;18(4):3260-71. doi: 10.1039/c5cp05771j[↩]
- DeLucia V, Kelsberg G, Safranek S. Which SSRIs most effectively treat depression in adolescents? J Fam Pract. 2016 Sep;65(9):632-4. https://www.mdedge.com/jfponline/article/111448/mental-health/which-ssris-most-effectively-treat-depression-adolescents[↩]
- Rohde C, Hieronymus F, Østergaard SD. A target trial emulation comparing the antidepressant effectiveness of selective serotonin reuptake inhibitors (SSRIs) highlighting the importance of patent-related confounding by indication. Acta Psychiatr Scand. 2024 Oct;150(4):198-208. doi: 10.1111/acps.13729[↩]
- Coleiro B, Marshall SE, Denton CP, Howell K, Blann A, Welsh KI, Black CM. Treatment of Raynaud’s phenomenon with the selective serotonin reuptake inhibitor fluoxetine. Rheumatology (Oxford). 2001 Sep;40(9):1038-43. doi: 10.1093/rheumatology/40.9.1038[↩]
- Fisher KA, Marwaha R. Paraphilia. [Updated 2023 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554425[↩]
- Seto MC, Kingston DA, Bourget D. Assessment of the paraphilias. Psychiatr Clin North Am. 2014 Jun;37(2):149-61. doi: 10.1016/j.psc.2014.03.001[↩]
- Seto MC. Pedophilia. Annu Rev Clin Psychol. 2009;5:391-407. doi: 10.1146/annurev.clinpsy.032408.153618[↩]
- PODOLSKY E. Exhibitionism. J Natl Med Assoc. 1960 Sep;52(5):343-4. https://pmc.ncbi.nlm.nih.gov/articles/instance/2641763/pdf/jnma00699-0033.pdf[↩]
- Balon R. Lack of Clarity in the DSM-5 Criteria of Voyeuristic Disorder. J Sex Marital Ther. 2016 Jul 3;42(5):391-2. doi: 10.1080/0092623X.2016.1158760[↩]
- Palermo GB. The various faces of sadism. Int J Offender Ther Comp Criminol. 2013 Apr;57(4):399-401. doi: 10.1177/0306624X13480125[↩]
- Civitarese G. Masochism and its Rhythm. J Am Psychoanal Assoc. 2016 Oct;64(5):885-916. doi: 10.1177/0003065116674442[↩]
- Långström N. The DSM diagnostic criteria for exhibitionism, voyeurism, and frotteurism. Arch Sex Behav. 2010 Apr;39(2):317-24. doi: 10.1007/s10508-009-9577-4[↩]
- Kafka MP. The DSM diagnostic criteria for fetishism. Arch Sex Behav. 2010 Apr;39(2):357-62. doi: 10.1007/s10508-009-9558-7[↩]
- Anupama M, Gangadhar KH, Shetty VB, Dip PB. Transvestism as a Symptom: A Case Series. Indian J Psychol Med. 2016 Jan-Feb;38(1):78-80. doi: 10.4103/0253-7176.175131[↩]
- Susser LC, Sansone SA, Hermann AD. Selective serotonin reuptake inhibitors for depression in pregnancy. Am J Obstet Gynecol. 2016 Dec;215(6):722-730. doi: 10.1016/j.ajog.2016.07.011[↩][↩]
- Hirschfeld RM. Efficacy of SSRIs and newer antidepressants in severe depression: comparison with TCAs. J Clin Psychiatry. 1999 May;60(5):326-35. doi: 10.4088/jcp.v60n0511 https://www.psychiatrist.com/jcp/efficacy-ssris-newer-antidepressants-severe-depression[↩]
- Kocsis JH. Review: SSRIs and TCAs equally effective at treating chronic depression and dysthemia; SSRIs are associated with fewer adverse events than TCAs. Evid Based Ment Health. 2013 Aug;16(3):82. doi: 10.1136/eb-2013-101268[↩]
- David DJ, Gourion D. Antidépresseurs et tolérance : déterminants et prise en charge des principaux effets indésirables [Antidepressant and tolerance: Determinants and management of major side effects]. Encephale. 2016 Dec;42(6):553-561. French. doi: 10.1016/j.encep.2016.05.006[↩]
- Hu XH, Bull SA, Hunkeler EM, Ming E, Lee JY, Fireman B, Markson LE. Incidence and duration of side effects and those rated as bothersome with selective serotonin reuptake inhibitor treatment for depression: patient report versus physician estimate. J Clin Psychiatry. 2004 Jul;65(7):959-65. doi: 10.4088/jcp.v65n0712[↩]
- Funk KA, Bostwick JR. A comparison of the risk of QT prolongation among SSRIs. Ann Pharmacother. 2013 Oct;47(10):1330-41. doi: 10.1177/1060028013501994[↩]
- Beach SR, Kostis WJ, Celano CM, Januzzi JL, Ruskin JN, Noseworthy PA, Huffman JC. Meta-analysis of selective serotonin reuptake inhibitor-associated QTc prolongation. J Clin Psychiatry. 2014 May;75(5):e441-9. doi: 10.4088/JCP.13r08672[↩]
- Laporte S, Chapelle C, Caillet P, Beyens MN, Bellet F, Delavenne X, Mismetti P, Bertoletti L. Bleeding risk under selective serotonin reuptake inhibitor (SSRI) antidepressants: A meta-analysis of observational studies. Pharmacol Res. 2017 Apr;118:19-32. doi: 10.1016/j.phrs.2016.08.017[↩]
- Suicidality in Children and Adolescents Being Treated With Antidepressant Medications. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/suicidality-children-and-adolescents-being-treated-antidepressant-medications[↩]
- Friedman RA. Antidepressants’ black-box warning–10 years later. N Engl J Med. 2014 Oct 30;371(18):1666-8. doi: 10.1056/NEJMp1408480[↩]
- Watson WA, Litovitz TL, Rodgers GC, Jr, Klein-Schwartz W, Youniss J, Rose SR, et al. 2002 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med. 2003;21(5):353–421. http://www.ajemjournal.com/article/S0735-6757(03)00088-3/fulltext[↩]
- Simon LV, Torrico TJ, Keenaghan M. Serotonin Syndrome. [Updated 2024 Mar 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482377[↩]
- Sharbaf Shoar N, Fariba KA, Padhy RK. Citalopram. [Updated 2023 Nov 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482222[↩]
- Citalopram. https://medlineplus.gov/druginfo/meds/a699001.html[↩]
- Citalopram (oral route). https://www.mayoclinic.org/drugs-supplements/citalopram-oral-route/description/drg-20062980[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Citalopram. [Updated 2017 Oct 12]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548395[↩][↩]
- Lochmann D, Richardson T. Selective Serotonin Reuptake Inhibitors. Handb Exp Pharmacol. 2019;250:135-144. doi: 10.1007/164_2018_172[↩]
- Stahl S. 5HT1A receptors and pharmacotherapy. Is serotonin receptor down-regulation linked to the mechanism of action of antidepressant drugs? Psychopharmacol Bull. 1994;30(1):39-43.[↩]
- Luo Y, Chaimani A, Kataoka Y, Ostinelli EG, Ogawa Y, Cipriani A, Salanti G, Furukawa TA. Evidence synthesis, practice guidelines and real-world prescriptions of new generation antidepressants in the treatment of depression: a protocol for cumulative network meta-analyses and meta-epidemiological study. BMJ Open. 2018 Dec 9;8(12):e023222. doi: 10.1136/bmjopen-2018-023222[↩]
- Hyttel J. Citalopram–pharmacological profile of a specific serotonin uptake inhibitor with antidepressant activity. Prog Neuropsychopharmacol Biol Psychiatry. 1982;6(3):277-95. doi: 10.1016/s0278-5846(82)80179-6[↩]
- Baumann P. Pharmacokinetic-pharmacodynamic relationship of the selective serotonin reuptake inhibitors. Clin Pharmacokinet. 1996 Dec;31(6):444-69. doi: 10.2165/00003088-199631060-00004[↩]
- Stahl SM. Mechanism of action of serotonin selective reuptake inhibitors. Serotonin receptors and pathways mediate therapeutic effects and side effects. J Affect Disord. 1998 Dec;51(3):215-35. doi: 10.1016/s0165-0327(98)00221-3[↩]
- Edinoff AN, Akuly HA, Hanna TA, Ochoa CO, Patti SJ, Ghaffar YA, Kaye AD, Viswanath O, Urits I, Boyer AG, Cornett EM, Kaye AM. Selective Serotonin Reuptake Inhibitors and Adverse Effects: A Narrative Review. Neurol Int. 2021 Aug 5;13(3):387-401. doi: 10.3390/neurolint13030038[↩]
- Chakrapani S, Eskander N, De Los Santos LA, Omisore BA, Mostafa JA. Neuroplasticity and the Biological Role of Brain Derived Neurotrophic Factor in the Pathophysiology and Management of Depression. Cureus. 2020 Nov 9;12(11):e11396. doi: 10.7759/cureus.11396[↩]
- Ji Y, Schaid DJ, Desta Z, Kubo M, Batzler AJ, Snyder K, Mushiroda T, Kamatani N, Ogburn E, Hall-Flavin D, Flockhart D, Nakamura Y, Mrazek DA, Weinshilboum RM. Citalopram and escitalopram plasma drug and metabolite concentrations: genome-wide associations. Br J Clin Pharmacol. 2014 Aug;78(2):373-83. doi: 10.1111/bcp.12348[↩]
- Kendrick T, Pilling S, Mavranezouli I, Megnin-Viggars O, Ruane C, Eadon H, Kapur N; Guideline Committee. Management of depression in adults: summary of updated NICE guidance. BMJ. 2022 Jul 20;378:o1557. https://doi.org/10.1136/bmj.o1557[↩]
- Citalopram. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/020822s055lbl.pdf#page=22[↩]
- Citalopram (marketed as Celexa) Information. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/citalopram-marketed-celexa-information[↩]
- FDA Drug Safety Communication: Revised recommendations for Celexa (citalopram hydrobromide) related to a potential risk of abnormal heart rhythms with high doses. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-revised-recommendations-celexa-citalopram-hydrobromide-related[↩]
- Cipriani A, Purgato M, Furukawa TA, Trespidi C, Imperadore G, Signoretti A, Churchill R, Watanabe N, Barbui C. Citalopram versus other anti-depressive agents for depression. Cochrane Database Syst Rev. 2012 Jul 11;2012(7):CD006534. doi: 10.1002/14651858.CD006534.pub2[↩]
- Bezchlibnyk-Butler K, Aleksic I, Kennedy SH. Citalopram–a review of pharmacological and clinical effects. J Psychiatry Neurosci. 2000 May;25(3):241-54. https://pmc.ncbi.nlm.nih.gov/articles/instance/1407724/pdf/jpn00086-0027.pdf[↩]
- Thomsen PH. Child and adolescent obsessive-compulsive disorder treated with citalopram: findings from an open trial of 23 cases. J Child Adolesc Psychopharmacol. 1997;7(3):157-66. doi: 10.1089/cap.1997.7.157[↩]
- Perna G, Bertani A, Caldirola D, Smeraldi E, Bellodi L. A comparison of citalopram and paroxetine in the treatment of panic disorder: a randomized, single-blind study. Pharmacopsychiatry. 2001 May;34(3):85-90. doi: 10.1055/s-2001-14283[↩]
- Varia I, Rauscher F. Treatment of generalized anxiety disorder with citalopram. Int Clin Psychopharmacol. 2002 May;17(3):103-7. doi: 10.1097/00004850-200205000-00002[↩]
- Nevatte T, O’Brien PM, Bäckström T, Brown C, Dennerstein L, Endicott J, Epperson CN, Eriksson E, Freeman EW, Halbreich U, Ismail K, Panay N, Pearlstein T, Rapkin A, Reid R, Rubinow D, Schmidt P, Steiner M, Studd J, Sundström-Poromaa I, Yonkers K; Consensus Group of the International Society for Premenstrual Disorders. ISPMD consensus on the management of premenstrual disorders. Arch Womens Ment Health. 2013 Aug;16(4):279-91. doi: 10.1007/s00737-013-0346-y[↩]
- McElroy SL, Hudson JI, Malhotra S, Welge JA, Nelson EB, Keck PE Jr. Citalopram in the treatment of binge-eating disorder: a placebo-controlled trial. J Clin Psychiatry. 2003 Jul;64(7):807-13. doi: 10.4088/jcp.v64n0711[↩]
- English BA, Jewell M, Jewell G, Ambrose S, Davis LL. Treatment of chronic posttraumatic stress disorder in combat veterans with citalopram: an open trial. J Clin Psychopharmacol. 2006 Feb;26(1):84-8. doi: 10.1097/01.jcp.0000195043.39853.bc[↩]
- Saleh R, Majzoub A, Abu El-Hamd M. An update on the treatment of premature ejaculation: A systematic review. Arab J Urol. 2021 Aug 4;19(3):281-302. doi: 10.1080/2090598X.2021.1943273[↩]
- Towfighi A, Ovbiagele B, El Husseini N, Hackett ML, Jorge RE, Kissela BM, Mitchell PH, Skolarus LE, Whooley MA, Williams LS; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; and Council on Quality of Care and Outcomes Research. Poststroke Depression: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2017 Feb;48(2):e30-e43. doi: 10.1161/STR.0000000000000113[↩]
- By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2019 Apr;67(4):674-694. doi: 10.1111/jgs.15767[↩][↩][↩]
- Citalopram | Escitalopram (Celexa® | Lexapro®). https://mothertobaby.org/fact-sheets/citalopramescitalopram-celexalexapro-pregnancy[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Ferguson JM. SSRI Antidepressant Medications: Adverse Effects and Tolerability. Prim Care Companion J Clin Psychiatry. 2001 Feb;3(1):22-27. doi: 10.4088/pcc.v03n0105[↩]
- Herstowska M, Komorowska O, Cubała WJ, Jakuszkowiak-Wojten K, Gałuszko-Węgielnik M, Landowski J. Severe skin complications in patients treated with antidepressants: a literature review. Postepy Dermatol Alergol. 2014 May;31(2):92-7. doi: 10.5114/pdia.2014.40930[↩]
- Beach SR, Celano CM, Noseworthy PA, Januzzi JL, Huffman JC. QTc prolongation, torsades de pointes, and psychotropic medications. Psychosomatics. 2013 Jan-Feb;54(1):1-13. doi: 10.1016/j.psym.2012.11.001[↩]
- Shah SR, Park K, Alweis R. Long QT Syndrome: A Comprehensive Review of the Literature and Current Evidence. Curr Probl Cardiol. 2019 Mar;44(3):92-106. doi: 10.1016/j.cpcardiol.2018.04.002[↩]
- Gatti M, Raschi E, De Ponti F. Serotonin syndrome by drug interactions with linezolid: clues from pharmacovigilance-pharmacokinetic/pharmacodynamic analysis. Eur J Clin Pharmacol. 2021 Feb;77(2):233-239. doi: 10.1007/s00228-020-02990-1[↩]
- Alotaibi MS, Yousuf AZ, Khan A, Alshammari NS. Late Presentation of Linezolid-Induced Serotonin Syndrome After Maprotiline and Mirtazapine Therapy: A Case Report. Clin Neuropharmacol. 2021 Mar-Apr 01;44(2):71-74. doi: 10.1097/WNF.0000000000000431[↩]
- Montgomery SA, Rasmussen JG, Lyby K, Connor P, Tanghøj P. Dose response relationship of citalopram 20 mg, citalopram 40 mg and placebo in the treatment of moderate and severe depression. Int Clin Psychopharmacol. 1992 Jun;6 Suppl 5:65-70. doi: 10.1097/00004850-199206005-00007[↩]
- Ford J, Thomas F, Byng R, McCabe R. Use of the Patient Health Questionnaire (PHQ-9) in Practice: Interactions between patients and physicians. Qual Health Res. 2020 Nov;30(13):2146-2159. doi: 10.1177/1049732320924625[↩]
- Hengartner MP, Jakobsen JC, Sørensen A, Plöderl M. Efficacy of new-generation antidepressants assessed with the Montgomery-Asberg Depression Rating Scale, the gold standard clinician rating scale: A meta-analysis of randomised placebo-controlled trials. PLoS One. 2020 Feb 26;15(2):e0229381. doi: 10.1371/journal.pone.0229381[↩]
- Bobo WV, Angleró GC, Jenkins G, Hall-Flavin DK, Weinshilboum R, Biernacka JM. Validation of the 17-item Hamilton Depression Rating Scale definition of response for adults with major depressive disorder using equipercentile linking to Clinical Global Impression scale ratings: analysis of Pharmacogenomic Research Network Antidepressant Medication Pharmacogenomic Study (PGRN-AMPS) data. Hum Psychopharmacol. 2016 May;31(3):185-92. doi: 10.1002/hup.2526[↩]
- Moore MT, Anderson NL, Barnes JM, Haigh EA, Fresco DM. Using the GAD-Q-IV to identify generalized anxiety disorder in psychiatric treatment seeking and primary care medical samples. J Anxiety Disord. 2014 Jan;28(1):25-30. doi: 10.1016/j.janxdis.2013.10.009[↩]
- Stein DJ, Khoo JP, Ahokas A, Jarema M, Van Ameringen M, Vavrusova L, Hӧschl C, Bauer M, Bitter I, Mosolov SN, Olivier V, Matharan S, Picarel-Blanchot F, de Bodinat C. 12-week double-blind randomized multicenter study of efficacy and safety of agomelatine (25-50 mg/day) versus escitalopram (10-20 mg/day) in out-patients with severe generalized anxiety disorder. Eur Neuropsychopharmacol. 2018 Aug;28(8):970-979. doi: 10.1016/j.euroneuro.2018.05.006[↩]
- Macaluso M, Preskorn SH. Knowledge of the Pharmacology of Antidepressants and Antipsychotics Yields Results Comparable With Pharmacogenetic Testing. J Psychiatr Pract. 2018 Nov;24(6):416-419. doi: 10.1097/PRA.0000000000000345[↩]
- Zoofaghari S, Wong A, Kiarasi P, Gheshlaghi F. Massive Citalopram Overdose Associated with Recurrent Seizures and Bilateral Shoulder Dislocations. J Res Pharm Pract. 2020 Oct 8;9(3):161-164. doi: 10.4103/jrpp.JRPP_20_24[↩]
- Iqbal MM, Basil MJ, Kaplan J, Iqbal MT. Overview of serotonin syndrome. Ann Clin Psychiatry. 2012 Nov;24(4):310-8. https://www.aacp.com/article/buy_now/?id=207[↩]
- Escitalopram. https://medlineplus.gov/druginfo/meds/a603005.html[↩]
- Kasper S, Sacher J, Klein N, Mossaheb N, Attarbaschi-Steiner T, Lanzenberger R, Spindelegger C, Asenbaum S, Holik A, Dudczak R. Differences in the dynamics of serotonin reuptake transporter occupancy may explain superior clinical efficacy of escitalopram versus citalopram. Int Clin Psychopharmacol. 2009 May;24(3):119-25. doi: 10.1097/YIC.0b013e32832a8ec8[↩]
- Berger M, Gray JA, Roth BL. The expanded biology of serotonin. Annu Rev Med. 2009;60:355-66. doi: 10.1146/annurev.med.60.042307.110802[↩][↩]
- Yohn CN, Gergues MM, Samuels BA. The role of 5-HT receptors in depression. Mol Brain. 2017 Jun 24;10(1):28. doi: 10.1186/s13041-017-0306-y[↩]
- Rao N. The clinical pharmacokinetics of escitalopram. Clin Pharmacokinet. 2007;46(4):281-90. doi: 10.2165/00003088-200746040-00002[↩]
- Keks N, Hope J, Keogh S. Switching and stopping antidepressants. Aust Prescr. 2016 Jun;39(3):76-83. doi: 10.18773/austprescr.2016.039[↩]
- Landy K, Rosani A, Estevez R. Escitalopram. [Updated 2023 Nov 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557734[↩]
- Sanchez C, Reines EH, Montgomery SA. A comparative review of escitalopram, paroxetine, and sertraline: Are they all alike? Int Clin Psychopharmacol. 2014 Jul;29(4):185-96. doi: 10.1097/YIC.0000000000000023[↩][↩]
- Strawn JR, Moldauer L, Hahn RD, Wise A, Bertzos K, Eisenberg B, Greenberg E, Liu C, Gopalkrishnan M, McVoy M, Knutson JA. A Multicenter Double-Blind, Placebo-Controlled Trial of Escitalopram in Children and Adolescents with Generalized Anxiety Disorder. J Child Adolesc Psychopharmacol. 2023 Apr;33(3):91-100. doi: 10.1089/cap.2023.0004. Erratum in: J Child Adolesc Psychopharmacol. 2023 Jun;33(5):200. doi: 10.1089/cap.2023.0004.correx[↩]
- Baldwin DS, Asakura S, Koyama T, Hayano T, Hagino A, Reines E, Larsen K. Efficacy of escitalopram in the treatment of social anxiety disorder: A meta-analysis versus placebo. Eur Neuropsychopharmacol. 2016 Jun;26(6):1062-9. doi: 10.1016/j.euroneuro.2016.02.013[↩]
- Bandelow B, Reitt M, Röver C, Michaelis S, Görlich Y, Wedekind D. Efficacy of treatments for anxiety disorders: a meta-analysis. Int Clin Psychopharmacol. 2015 Jul;30(4):183-92. doi: 10.1097/YIC.0000000000000078[↩]
- Stubbs C, Mattingly L, Crawford SA, Wickersham EA, Brockhaus JL, McCarthy LH. Do SSRIs and SNRIs reduce the frequency and/or severity of hot flashes in menopausal women. J Okla State Med Assoc. 2017 May;110(5):272-274[↩]
- Jespersen C, Lauritsen MP, Frokjaer VG, Schroll JB. Selective serotonin reuptake inhibitors for premenstrual syndrome and premenstrual dysphoric disorder. Cochrane Database Syst Rev. 2024 Aug 14;8(8):CD001396. doi: 10.1002/14651858.CD001396.pub4[↩]
- Feth N, Cattapan-Ludewig K, Jaquenoud-Sirot E: Electric sensations: neglected symptom of escitalopram discontinuation. Am J Psychiatry 2006;163:160.[↩][↩][↩]
- Prakash O, Dhar V: Emergence of electric shock-like sensations on escitalopram discontinuation. J Clin Psychopharmacol 2008;28:359-360.[↩][↩]
- Withdrawal Symptoms after Selective Serotonin Reuptake Inhibitor Discontinuation: A Systematic Review. Psychother Psychosom 2015;84:72-81 https://doi.org/10.1159/000370338[↩][↩]
- Blier P, Tremblay P: Physiologic mechanisms underlying the antidepressant discontinuation syndrome. J Clin Psychiatry 2006;67:8-13.[↩]
- Harvey BH, McEwen BS, Stein DJ: Neurobiology of antidepressant withdrawal: implications for longitudinal outcome of depression. Biol Psychiatry 2003;54:1105-1117.[↩]
- Murata Y, Kobayashi D, Imuta N, Haraguchi K, Ieiri I, Nishimura R, Koyama S, Mine K: Effects of serotonin 1A, 2A, 2C, 3A and 3B and serotonin transporter gene polymorphisms on the occurrence of paroxetine discontinuation syndrome. J Clin Psychopharmacol 2010;30:11-17.[↩]
- Renoir T: Selective serotonin reuptake inhibitor antidepressant treatment discontinuation syndrome: a review of the clinical evidence and the possible mechanisms involved. Front Pharmacol 2013;4:1-10.[↩]
- Fava GA, Offidani E: The mechanisms of tolerance in antidepressant action. Prog Neuropsychopharmacol Biol Psychiatry 2011;35:1593-1602.[↩][↩]
- Fava GA: Rational use of antidepressant drugs. Psychother Psychosom 2014;83:197-204.[↩]
- Sohel AJ, Shutter MC, Patel P, et al. Fluoxetine. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459223[↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Fluoxetine. [Updated 2018 Feb 2]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548010[↩][↩][↩]
- Fluoxetine. https://medlineplus.gov/druginfo/meds/a689006.html[↩][↩]
- Hiemke C, Härtter S. Pharmacokinetics of selective serotonin reuptake inhibitors. Pharmacol Ther. 2000 Jan;85(1):11-28. doi: 10.1016/s0163-7258(99)00048-0[↩]
- Robertson OD, Coronado NG, Sethi R, Berk M, Dodd S. Putative neuroprotective pharmacotherapies to target the staged progression of mental illness. Early Interv Psychiatry. 2019 Oct;13(5):1032-1049. doi: 10.1111/eip.12775[↩]
- Cao B, Zhu J, Zuckerman H, Rosenblat JD, Brietzke E, Pan Z, Subramanieapillai M, Park C, Lee Y, McIntyre RS. Pharmacological interventions targeting anhedonia in patients with major depressive disorder: A systematic review. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Jun 8;92:109-117. doi: 10.1016/j.pnpbp.2019.01.002[↩]
- Delavenne X, Magnin M, Basset T, Piot M, Mallouk N, Ressnikoff D, Garcin A, Laporte S, Garnier P, Mismetti P. Investigation of drug-drug interactions between clopidogrel and fluoxetine. Fundam Clin Pharmacol. 2013 Dec;27(6):683-9. doi: 10.1111/fcp.12021[↩]
- Deodhar M, Rihani SBA, Darakjian L, Turgeon J, Michaud V. Assessing the Mechanism of Fluoxetine-Mediated CYP2D6 Inhibition. Pharmaceutics. 2021 Jan 23;13(2):148. doi: 10.3390/pharmaceutics13020148[↩]
- Mikocka-Walus A, Prady SL, Pollok J, Esterman AJ, Gordon AL, Knowles S, Andrews JM. Adjuvant therapy with antidepressants for the management of inflammatory bowel disease. Cochrane Database Syst Rev. 2019 Apr 12;4(4):CD012680. doi: 10.1002/14651858.CD012680.pub2[↩]
- Dhenain T, Côté F, Coman T. Serotonin and orthodontic tooth movement. Biochimie. 2019 Jun;161:73-79. doi: 10.1016/j.biochi.2019.04.002[↩]
- Burch R. Antidepressants for Preventive Treatment of Migraine. Curr Treat Options Neurol. 2019 Mar 21;21(4):18. doi: 10.1007/s11940-019-0557-2[↩]
- Crone C, Fochtmann LJ, Attia E, Boland R, Escobar J, Fornari V, Golden N, Guarda A, Jackson-Triche M, Manzo L, Mascolo M, Pierce K, Riddle M, Seritan A, Uniacke B, Zucker N, Yager J, Craig TJ, Hong SH, Medicus J. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders. Am J Psychiatry. 2023 Feb 1;180(2):167-171. doi: 10.1176/appi.ajp.23180001[↩][↩]
- Li X, Li J, Li X, Wang J, Dai H, Wang J. Effectiveness and safety of fluoxetine for premature ejaculation: Protocol for a systematic review. Medicine (Baltimore). 2019 Feb;98(7):e14481. doi: 10.1097/MD.0000000000014481[↩]
- Slee A, Nazareth I, Bondaronek P, Liu Y, Cheng Z, Freemantle N. Pharmacological treatments for generalised anxiety disorder: a systematic review and network meta-analysis. Lancet. 2019 Feb 23;393(10173):768-777. doi: 10.1016/S0140-6736(18)31793-8. Epub 2019 Jan 31. Erratum in: Lancet. 2019 Apr 27;393(10182):1698. doi: 10.1016/S0140-6736(19)30857-8[↩]
- Martin A, Naunton M, Kosari S, Peterson G, Thomas J, Christenson JK. Treatment Guidelines for PTSD: A Systematic Review. J Clin Med. 2021 Sep 15;10(18):4175. doi: 10.3390/jcm10184175[↩]
- Mazhar F, Akram S, Haider N, Ahmed R. Overlapping of Serotonin Syndrome with Neuroleptic Malignant Syndrome due to Linezolid-Fluoxetine and Olanzapine-Metoclopramide Interactions: A Case Report of Two Serious Adverse Drug Effects Caused by Medication Reconciliation Failure on Hospital Admission. Case Rep Med. 2016;2016:7128909. doi: 10.1155/2016/7128909[↩]
- Tisdale JE. Drug-induced QT interval prolongation and torsades de pointes: Role of the pharmacist in risk assessment, prevention and management. Can Pharm J (Ott). 2016 May;149(3):139-52. doi: 10.1177/1715163516641136[↩]
- Walter HJ, Abright AR, Bukstein OG, Diamond J, Keable H, Ripperger-Suhler J, Rockhill C. Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents With Major and Persistent Depressive Disorders. J Am Acad Child Adolesc Psychiatry. 2023 May;62(5):479-502. doi: 10.1016/j.jaac.2022.10.001[↩]
- Solmi M, Fornaro M, Ostinelli EG, Zangani C, Croatto G, Monaco F, Krinitski D, Fusar-Poli P, Correll CU. Safety of 80 antidepressants, antipsychotics, anti-attention-deficit/hyperactivity medications and mood stabilizers in children and adolescents with psychiatric disorders: a large scale systematic meta-review of 78 adverse effects. World Psychiatry. 2020 Jun;19(2):214-232. doi: 10.1002/wps.20765[↩]
- Gutsmiedl K, Krause M, Bighelli I, Schneider-Thoma J, Leucht S. How well do elderly patients with major depressive disorder respond to antidepressants: a systematic review and single-group meta-analysis. BMC Psychiatry. 2020 Mar 4;20(1):102. doi: 10.1186/s12888-020-02514-2[↩]
- Fluoxetine (Prozac®). https://mothertobaby.org/fact-sheets/fluoxetine-prozac-pregnancy[↩][↩][↩][↩]
- Baudat M, de Kort AR, van den Hove DLA, Joosten EA. Early-life exposure to selective serotonin reuptake inhibitors: Long-term effects on pain and affective comorbidities. Eur J Neurosci. 2022 Jan;55(1):295-317. doi: 10.1111/ejn.15544[↩]
- Wagstaff AJ, Goa KL. Once-weekly fluoxetine. Drugs. 2001;61(15):2221-8; discussion 2229-30. doi: 10.2165/00003495-200161150-00006[↩]
- Selph SS, McDonagh MS. Depression in Children and Adolescents: Evaluation and Treatment. Am Fam Physician. 2019 Nov 15;100(10):609-617. https://www.aafp.org/pubs/afp/issues/2019/1115/p609.html[↩]
- Lee-Kelland R, Zehra S, Mappa P. Fluoxetine overdose in a teenager resulting in serotonin syndrome, seizure and delayed onset rhabdomyolysis. BMJ Case Rep. 2018 Oct 8;2018:bcr2018225529. doi: 10.1136/bcr-2018-225529[↩]
- Sharp R. The Hamilton Rating Scale for Depression. Occup Med (Lond). 2015 Jun;65(4):340. doi: 10.1093/occmed/kqv043[↩]
- Arroll B, Goodyear-Smith F, Crengle S, Gunn J, Kerse N, Fishman T, Falloon K, Hatcher S. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med. 2010 Jul-Aug;8(4):348-53. doi: 10.1370/afm.1139[↩]
- Beard C, Hsu KJ, Rifkin LS, Busch AB, Björgvinsson T. Validation of the PHQ-9 in a psychiatric sample. J Affect Disord. 2016 Mar 15;193:267-73. doi: 10.1016/j.jad.2015.12.075[↩]
- Narouze S, Benzon HT, Provenzano D, Buvanendran A, De Andres J, Deer T, Rauck R, Huntoon MA. Interventional Spine and Pain Procedures in Patients on Antiplatelet and Anticoagulant Medications (Second Edition): Guidelines From the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Reg Anesth Pain Med. 2018 Apr;43(3):225-262. doi: 10.1097/AAP.0000000000000700[↩]
- Nelson LS, Erdman AR, Booze LL, Cobaugh DJ, Chyka PA, Woolf AD, Scharman EJ, Wax PM, Manoguerra AS, Christianson G, Caravati EM, Troutman WG. Selective serotonin reuptake inhibitor poisoning: An evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila). 2007 May;45(4):315-32. doi: 10.1080/15563650701285289[↩]
- Patel DD, Galarneau D. Serotonin Syndrome With Fluoxetine: Two Case Reports. Ochsner J. 2016 Winter;16(4):554-557. https://pmc.ncbi.nlm.nih.gov/articles/PMC5158166[↩]
- Barbey JT, Roose SP. SSRI safety in overdose. J Clin Psychiatry. 1998;59 Suppl 15:42-8. https://www.psychiatrist.com/wp-content/uploads/2021/02/17841_ssri-safety-overdose.pdf[↩]
- Shrestha P, Fariba KA, Abdijadid S. Paroxetine. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526022[↩][↩][↩][↩][↩][↩]
- Germann D, Ma G, Han F, Tikhomirova A. Paroxetine hydrochloride. Profiles Drug Subst Excip Relat Methodol. 2013;38:367-406. doi: 10.1016/B978-0-12-407691-4.00008-3[↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Paroxetine. [Updated 2020 Apr 8]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548306[↩]
- Amidfar M, Kim YK. Recent Developments on Future Antidepressant-related Serotonin Receptors. Curr Pharm Des. 2018;24(22):2541-2548. doi: 10.2174/1381612824666180803111240[↩]
- van Harten J. Clinical pharmacokinetics of selective serotonin reuptake inhibitors. Clin Pharmacokinet. 1993 Mar;24(3):203-20. doi: 10.2165/00003088-199324030-00003[↩]
- Uttamsingh V, Gallegos R, Liu JF, Harbeson SL, Bridson GW, Cheng C, Wells DS, Graham PB, Zelle R, Tung R. Altering metabolic profiles of drugs by precision deuteration: reducing mechanism-based inhibition of CYP2D6 by paroxetine. J Pharmacol Exp Ther. 2015 Jul;354(1):43-54. doi: 10.1124/jpet.115.223768[↩]
- Hieronymus F, Lisinski A, Nilsson S, Eriksson E. Efficacy of selective serotonin reuptake inhibitors in the absence of side effects: a mega-analysis of citalopram and paroxetine in adult depression. Mol Psychiatry. 2018 Aug;23(8):1731-1736. doi: 10.1038/mp.2017.147[↩][↩]
- Paroxetine. https://mothertobaby.org/fact-sheets/paroxetine-paxil-pregnancy/[↩][↩][↩]
- Magalhães P, Alves G, Llerena A, Falcão A. Therapeutic Drug Monitoring of Fluoxetine, Norfluoxetine and Paroxetine: A New Tool Based on Microextraction by Packed Sorbent Coupled to Liquid Chromatography. J Anal Toxicol. 2017 Sep 1;41(7):631-638. doi: 10.1093/jat/bkx043[↩]
- Fitzgerald KT, Bronstein AC. Selective serotonin reuptake inhibitor exposure. Top Companion Anim Med. 2013 Feb;28(1):13-7. doi: 10.1053/j.tcam.2013.03.003[↩]
- Bahar MA, Wang Y, Bos JHJ, Wilffert B, Hak E. Discontinuation and dose adjustment of metoprolol after metoprolol-paroxetine/fluoxetine co-prescription in Dutch elderly. Pharmacoepidemiol Drug Saf. 2018 Jun;27(6):621-629. doi: 10.1002/pds.4422[↩]
- Singh HK, Saadabadi A. Sertraline. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547689[↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Sertraline. [Updated 2020 Apr 8]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548513[↩]
- Cipriani A, La Ferla T, Furukawa TA, Signoretti A, Nakagawa A, Churchill R, McGuire H, Barbui C. Sertraline versus other antidepressive agents for depression. Cochrane Database Syst Rev. 2010 Apr 14;(4):CD006117. doi: 10.1002/14651858.CD006117.pub4[↩][↩]
- Kitaichi Y, Inoue T, Nakagawa S, Boku S, Kakuta A, Izumi T, Koyama T. Sertraline increases extracellular levels not only of serotonin, but also of dopamine in the nucleus accumbens and striatum of rats. Eur J Pharmacol. 2010 Nov 25;647(1-3):90-6. doi: 10.1016/j.ejphar.2010.08.026[↩]
- Fenske JN, Schwenk TL. Obsessive compulsive disorder: diagnosis and management. Am Fam Physician. 2009 Aug 1;80(3):239-45. https://www.aafp.org/pubs/afp/issues/2009/0801/p239-s1.html[↩]
- Semenya AM, Bhatnagar P. Diagnosis and Management of Obsessive-Compulsive Disorder in the Primary Care Setting. Am Fam Physician. 2024 Oct;110(4):385-392. https://www.aafp.org/pubs/afp/issues/2024/1000/obsessive-compulsive-disorder.html[↩]
- Hobgood CD, Clayton AH. Sertraline in the treatment of panic disorder. Drugs Today (Barc). 2009 May;45(5):351-61. doi: 10.1358/dot.2009.45.5.1362066[↩]
- Buhmann CB, Andersen HS. [Diagnosing and treating post-traumatic stress disorder]. Ugeskr Laeger. 2017 Jun 12;179(24):V12160914. Danish.[↩]
- Aigner M, Treasure J, Kaye W, Kasper S; WFSBP Task Force On Eating Disorders. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of eating disorders. World J Biol Psychiatry. 2011 Sep;12(6):400-43. doi: 10.3109/15622975.2011.602720[↩][↩]
- Sola CL, Bostwick JM, Hart DA, Lineberry TW. Anticipating potential linezolid-SSRI interactions in the general hospital setting: an MAOI in disguise. Mayo Clin Proc. 2006 Mar;81(3):330-4. doi: 10.4065/81.3.330[↩][↩]
- DeVane CL, Liston HL, Markowitz JS. Clinical pharmacokinetics of sertraline. Clin Pharmacokinet. 2002;41(15):1247-66. doi: 10.2165/00003088-200241150-00002[↩]
- Drugs and Lactation Database (LactMed®) [Internet]. Bethesda (MD): National Institute of Child Health and Human Development; 2006-. Sertraline. [Updated 2025 Feb 15]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK501191[↩]
- Pinheiro E, Bogen DL, Hoxha D, Ciolino JD, Wisner KL. Sertraline and breastfeeding: review and meta-analysis. Arch Womens Ment Health. 2015 Apr;18(2):139-146. doi: 10.1007/s00737-015-0499-y[↩][↩][↩]
- Weissman AM, Levy BT, Hartz AJ, Bentler S, Donohue M, Ellingrod VL, Wisner KL. Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants. Am J Psychiatry. 2004 Jun;161(6):1066-78. doi: 10.1176/appi.ajp.161.6.1066[↩]
- Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol #18: use of antidepressants in nursing mothers. Breastfeed Med. 2008 Mar;3(1):44-52. doi: 10.1089/bfm.2007.9978[↩]
- Berle JO, Spigset O. Antidepressant Use During Breastfeeding. Curr Womens Health Rev. 2011 Feb;7(1):28-34. doi: 10.2174/157340411794474784[↩]
- Larsen ER, Damkier P, Pedersen LH, Fenger-Gron J, Mikkelsen RL, Nielsen RE, Linde VJ, Knudsen HE, Skaarup L, Videbech P; Danish Psychiatric Society; Danish Society of Obstetrics and Gynecology; Danish Paediatric Society; Danish Society of Clinical Pharmacology. Use of psychotropic drugs during pregnancy and breast-feeding. Acta Psychiatr Scand Suppl. 2015;(445):1-28. doi: 10.1111/acps.12479[↩]
- Orsolini L, Bellantuono C. Serotonin reuptake inhibitors and breastfeeding: a systematic review. Hum Psychopharmacol. 2015 Jan;30(1):4-20. doi: 10.1002/hup.2451[↩]
- McAllister-Williams RH, Baldwin DS, Cantwell R, Easter A, Gilvarry E, Glover V, Green L, Gregoire A, Howard LM, Jones I, Khalifeh H, Lingford-Hughes A, McDonald E, Micali N, Pariante CM, Peters L, Roberts A, Smith NC, Taylor D, Wieck A, Yates LM, Young AH; endorsed by the British Association for Psychopharmacology. British Association for Psychopharmacology consensus guidance on the use of psychotropic medication preconception, in pregnancy and postpartum 2017. J Psychopharmacol. 2017 May;31(5):519-552. doi: 10.1177/0269881117699361[↩]
- Molenaar NM, Kamperman AM, Boyce P, Bergink V. Guidelines on treatment of perinatal depression with antidepressants: An international review. Aust N Z J Psychiatry. 2018 Apr;52(4):320-327. doi: 10.1177/0004867418762057[↩]
- Uguz F. A New Safety Scoring System for the Use of Psychotropic Drugs During Lactation. Am J Ther. 2021 Jan-Feb 01;28(1):e118-e126. doi: 10.1097/MJT.0000000000000909[↩]
- Leverich GS, Altshuler LL, Frye MA, Suppes T, McElroy SL, Keck PE Jr, Kupka RW, Denicoff KD, Nolen WA, Grunze H, Martinez MI, Post RM. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry. 2006 Feb;163(2):232-9. doi: 10.1176/appi.ajp.163.2.232[↩]
- Andrade C, Sandarsh S, Chethan KB, Nagesh KS. Serotonin reuptake inhibitor antidepressants and abnormal bleeding: a review for clinicians and a reconsideration of mechanisms. J Clin Psychiatry. 2010 Dec;71(12):1565-75. doi: 10.4088/JCP.09r05786blu[↩]
- Glassman AH, O’Connor CM, Califf RM, Swedberg K, Schwartz P, Bigger JT Jr, Krishnan KR, van Zyl LT, Swenson JR, Finkel MS, Landau C, Shapiro PA, Pepine CJ, Mardekian J, Harrison WM, Barton D, Mclvor M; Sertraline Antidepressant Heart Attack Randomized Trial (SADHEART) Group. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA. 2002 Aug 14;288(6):701-9. doi: 10.1001/jama.288.6.701. Erratum in: JAMA 2002 Oct 9;288(14):1720.[↩]
- O’Connor CM, Jiang W, Kuchibhatla M, Silva SG, Cuffe MS, Callwood DD, Zakhary B, Stough WG, Arias RM, Rivelli SK, Krishnan R; SADHART-CHF Investigators. Safety and efficacy of sertraline for depression in patients with heart failure: results of the SADHART-CHF (Sertraline Against Depression and Heart Disease in Chronic Heart Failure) trial. J Am Coll Cardiol. 2010 Aug 24;56(9):692-9. doi: 10.1016/j.jacc.2010.03.068[↩]
- Paulzen M, Goecke TW, Stickeler E, Gründer G, Schoretsanitis G. Sertraline in pregnancy – Therapeutic drug monitoring in maternal blood, amniotic fluid and cord blood. J Affect Disord. 2017 Apr 1;212:1-6. doi: 10.1016/j.jad.2017.01.019[↩]
- Wang RZ, Vashistha V, Kaur S, Houchens NW. Serotonin syndrome: Preventing, recognizing, and treating it. Cleve Clin J Med. 2016 Nov;83(11):810-817. doi: 10.3949/ccjm.83a.15129[↩]
- Laughren TP, Gobburu J, Temple RJ, Unger EF, Bhattaram A, Dinh PV, Fossom L, Hung HM, Klimek V, Lee JE, Levin RL, Lindberg CY, Mathis M, Rosloff BN, Wang SJ, Wang Y, Yang P, Yu B, Zhang H, Zhang L, Zineh I. Vilazodone: clinical basis for the US Food and Drug Administration’s approval of a new antidepressant. J Clin Psychiatry. 2011 Sep;72(9):1166-73. doi: 10.4088/JCP.11r06984[↩][↩]
- Hughes Z.A., Starr K.R., Langmead C.J., Hill M., Bartoszyk G.D., Hagan J.J., Middlemiss D.N., Dawson L.A. Neurochemical evaluation of the novel 5-HT1A receptor partial agonist/serotonin reuptake inhibitor, vilazodone. Eur. J. Pharmacol. 2005;510:49–57. doi: 10.1016/j.ejphar.2005.01.018[↩][↩]
- Owen R.T. Vilazodone: A new treatment option for major depressive disorder. Drugs Today (Barc) 2011;47:531–537. doi: 10.1358/dot.2011.47.7.1622076[↩][↩]
- Cruz MP. Vilazodone HCl (Viibryd): A Serotonin Partial Agonist and Reuptake Inhibitor For the Treatment of Major Depressive Disorder. P T. 2012 Jan;37(1):28-31. https://pmc.ncbi.nlm.nih.gov/articles/PMC3278186[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Vilazodone. [Updated 2020 Apr 8]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548223[↩][↩][↩]
- Vilazodone. https://medlineplus.gov/druginfo/meds/a611020.html[↩][↩]
- Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, Hasnain M, Jollant F, Levitt AJ, MacQueen GM, McInerney SJ, McIntosh D, Milev RV, Müller DJ, Parikh SV, Pearson NL, Ravindran AV, Uher R; CANMAT Depression Work Group. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments. Can J Psychiatry. 2016 Sep;61(9):540-60. doi: 10.1177/0706743716659417. Epub 2016 Aug 2. Erratum in: Can J Psychiatry. 2017 May;62(5):356. doi: 10.1177/0706743717708346[↩][↩][↩]
- FDA-Approved Drugs. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=208212[↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/022567s025lbl.pdf#page=17[↩][↩]
- Pae CU, Wang SM, Han C, Lee SJ, Patkar AA, Masand PS, Serretti A. Vortioxetine: a meta-analysis of 12 short-term, randomized, placebo-controlled clinical trials for the treatment of major depressive disorder. J Psychiatry Neurosci. 2015 May;40(3):174-86. doi: 10.1503/jpn.140120[↩]
- Viswanathan M, Kennedy SM, McKeeman J, et al. Treatment of Depression in Children and Adolescents: A Systematic Review [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2020 Apr. (Comparative Effectiveness Review, No. 224.) Chapter 1, Introduction. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555846[↩]
- Durgam S, Chen C, Migliore R, Prakash C, Edwards J, Findling RL. A Phase 3, Double-Blind, Randomized, Placebo-Controlled Study of Vilazodone in Adolescents with Major Depressive Disorder. Paediatr Drugs. 2018 Aug;20(4):353-363. doi: 10.1007/s40272-018-0290-4[↩]
- Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Int Clin Psychopharmacol. 2012 Jul;27(4):215-23. doi: 10.1097/YIC.0b013e3283542457[↩]
- Mahableshwarkar AR, Zajecka J, Jacobson W, Chen Y, Keefe RS. A Randomized, Placebo-Controlled, Active-Reference, Double-Blind, Flexible-Dose Study of the Efficacy of Vortioxetine on Cognitive Function in Major Depressive Disorder. Neuropsychopharmacology. 2015 Jul;40(8):2025-37. doi: 10.1038/npp.2015.52. Epub 2015 Feb 17. Erratum in: Neuropsychopharmacology. 2016 Nov;41(12):2961. doi: 10.1038/npp.2016.181[↩]
- Rosenblat JD, Kakar R, McIntyre RS. The Cognitive Effects of Antidepressants in Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int J Neuropsychopharmacol. 2015 Jul 25;19(2):pyv082. doi: 10.1093/ijnp/pyv082. Erratum in: Int J Neuropsychopharmacol. 2016 Apr 27;19(10):pyw031. doi: 10.1093/ijnp/pyw031[↩]
- McIntyre RS, Lophaven S, Olsen CK. A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults. Int J Neuropsychopharmacol. 2014 Oct;17(10):1557-67. doi: 10.1017/S1461145714000546[↩]
- Vilazodone (Viibryd®). https://mothertobaby.org/fact-sheets/vilazodone-viibryd[↩]
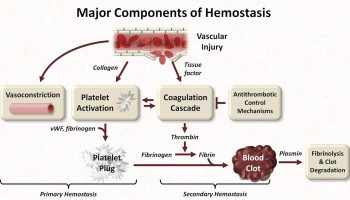

{kind=link}