Contents
What is tension pneumothorax
Tension pneumothorax is a life-threatening collapsed lung (pneumothorax) that occurs when air builds up and is trapped and can’t get out in your pleural space (the space between your lung and chest wall), the one-way valve effect causes pressure to build up inside of your chest putting pressure on your lungs, major blood vessels and heart disrupting your heart and breathing function 1. A collapsed lung or pneumothorax occurs when air leaks into the pleural space between your lung and chest wall. Tension pneumothorax develops when a lung or chest wall injury is such that it allows air into the pleural space but not out of it (a one-way valve). As a result, air accumulates and compresses your lung, eventually shifting the mediastinum (the central portion of your thoracic cavity between your lungs), compressing the contralateral lung, and increasing intrathoracic pressure enough to decrease venous return to the heart, causing shock. These effects can develop rapidly, particularly in patients undergoing positive pressure ventilation.
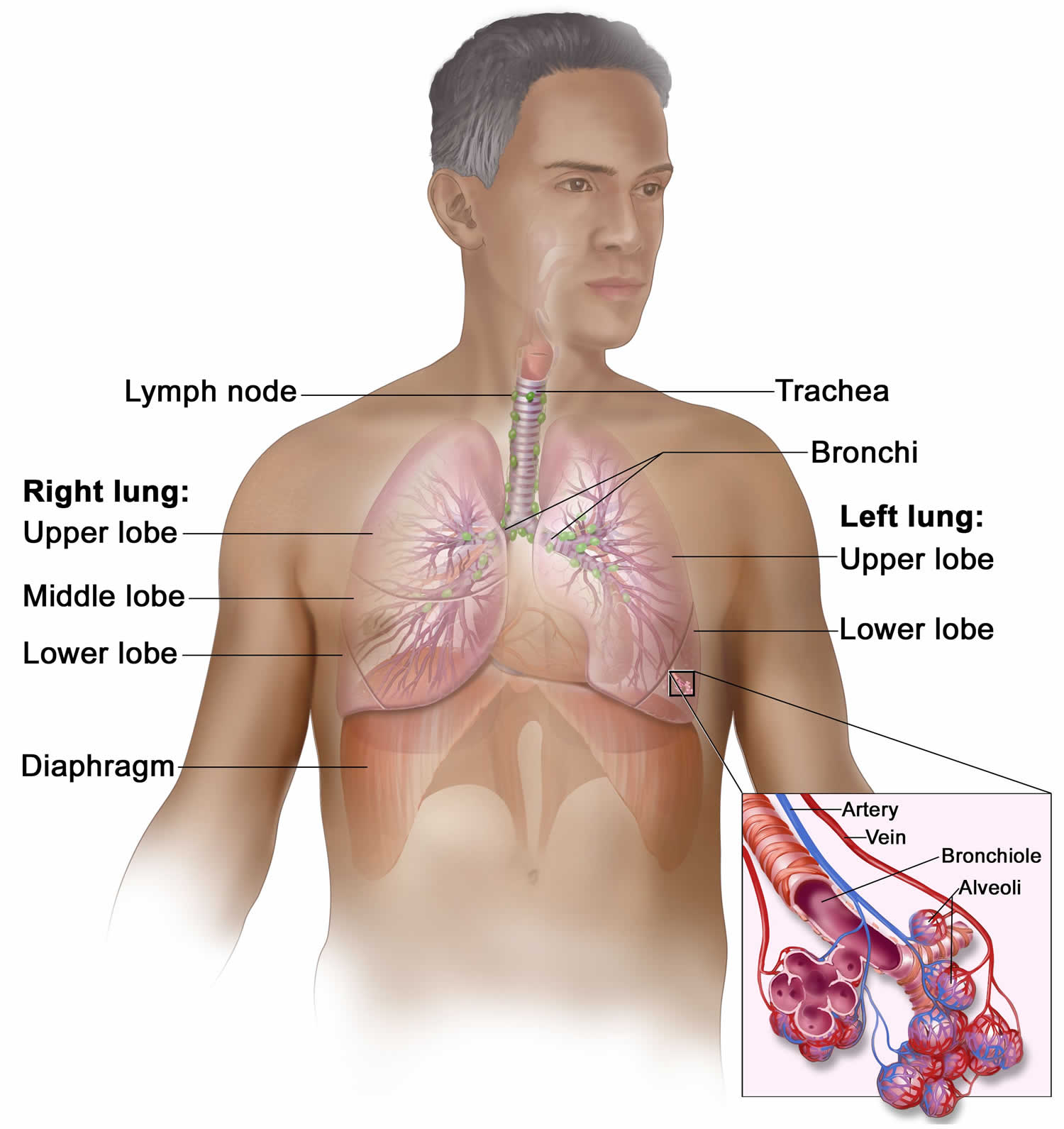
Your mediastinum contains your heart, the major blood vessels connected to your heart and lungs, the trachea (windpipe) and bronchi, the esophagus (foodpipe), the thymus, and lymph nodes but not your lungs. Your right and left lungs are on either side of the mediastinum.
Tension pneumothorax is a medical emergency that requires immediate needle decompression or chest tube drainage to remove air from your chest and might result in death if left untreated 2, 3. People with a tension pneumothorax are usually unstable and will decompensate quickly.
Tension pneumothorax causes include mechanical ventilation (most commonly) and simple (uncomplicated) pneumothorax with lung injury that fails to seal following penetrating or blunt chest trauma or failed central venous cannulation.
A collapsed lung or pneumothorax can be caused by:
- Chest injury. Any blunt or penetrating injury to your chest can cause lung collapse. Some injuries may happen during physical assaults (gunshot wound, stab wound) or car crashes, while others may inadvertently occur during medical procedures that involve the insertion of a needle into your chest for a nerve block, lung biopsy or central venous line placement.
- Lung disease. Damaged lung tissue is more likely to collapse. Lung damage can be caused by many types of underlying diseases, including chronic obstructive pulmonary disease (COPD), cystic fibrosis, asthma, pneumonia, tuberculosis, idiopathic pulmonary fibrosis, emphysema, lung cancer, acute respiratory distress syndrome (ARDS), lymphangioleiomyomatosis or collagen vascular disease (a group of autoimmune disorders that cause the body’s immune system to attack its own tissues).
- Ruptured air blisters. Small air blisters (blebs) can develop on the top of your lung. These blebs sometimes burst — allowing air to leak into the space that surrounds the lungs.
- Mechanical ventilation. A severe type of pneumothorax can occur in people who need mechanical assistance to breathe. The ventilator can create an imbalance of air pressure within the chest. The lung may collapse completely.
- Lifestyle factors such as drug use, especially inhaled drugs, smoking, flying that involves drastic changes in air pressure or scuba or deep-sea diving.
Tension pneumothorax signs and symptoms are usually more dramatic than those seen with a simple pneumothorax, and clinical interpretation of these is crucial for diagnosing and treating the condition. Tension pneumothorax is classically characterized by hypotension (low blood pressure) and hypoxia (low blood oxygen). On examination, breath sounds are absent on the affected lung and the trachea deviates away from the affected side. The chest may also be hyperresonant to percussion and often feels somewhat distended, tense, and poorly compressible to palpation; neck vein distention (jugular venous distention) and fast heart rate (tachycardia) may be present. If on mechanical ventilation, the airway pressure alarms are triggered.
Tension pneumothorax is a clinical diagnosis. Patients with this condition can easily decompensate and go into cardiac arrest if not managed immediately 4. Unconscious patients without respirations or a pulse must be given immediate resuscitation regardless of the cause.
Because of subtle presentations that do not always present with the classically described clinical findings of tension pneumothorax or the complexity of the patient with critical illness or injury to describe a tension pneumothorax, actual case reports include descriptions of the diagnosis of tension pneumothorax being missed or delayed. Nevertheless, tension pneumothorax should always be a consideration when acute breathing and cardiovascular compromise occurs.
Symptoms of tension pneumothorax may include chest pain (90%), dyspnea (80%), anxiety, fatigue, or acute epigastric pain (a rare finding).
Tension pneumothorax should be diagnosed by clinical findings. Treatment should not be delayed pending radiographic confirmation. Although cardiac tamponade also can cause hypotension, neck vein distention, and sometimes respiratory distress, tension pneumothorax can be differentiated clinically by its unilateral absence of breath sounds and hyperresonance chest to percussion.
Treatment of tension pneumothorax is immediate needle decompression by inserting a large-bore (eg, 14- or 16-gauge) needle into the second intercostal space in the midclavicular line above the rib with an angiocatheter. The American College of Surgeons Advanced Trauma Life Support recommends placement in the fourth or fifth intercostal space along the midaxillary line, as it has been associated with improved success at decompression. Air will usually gush out. Because needle decompression causes a simple pneumothorax, tube thoracostomy should be done immediately thereafter.
Figure 1. Tension pneumothorax
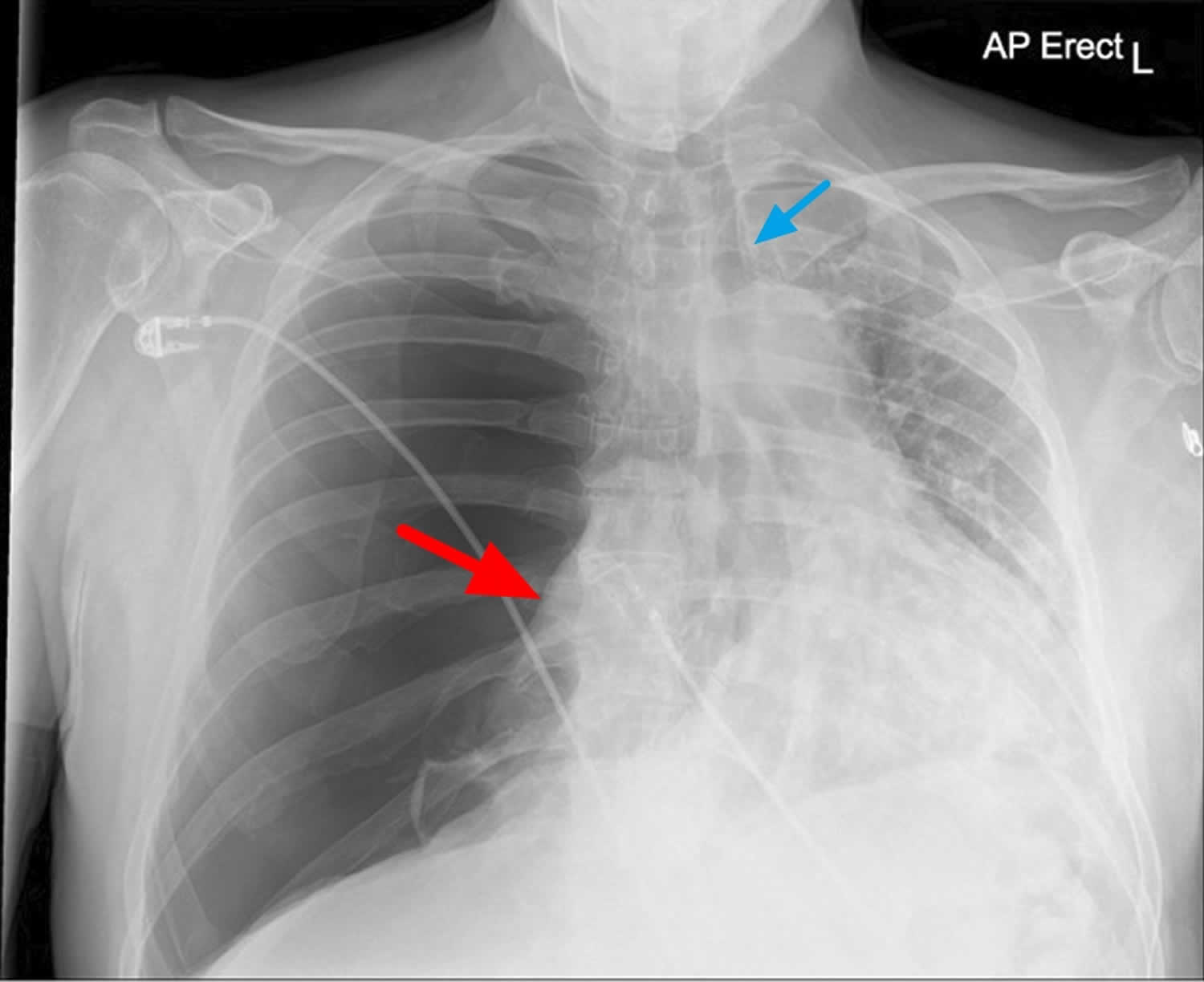
Footnotes: Chest x-ray of tension pneumothorax. Large right-sided tension pneumothorax causing deviation of the mediastinum to the left. The left lung is compressed
[Source 5 ]Figure 2. Tension pneumothorax
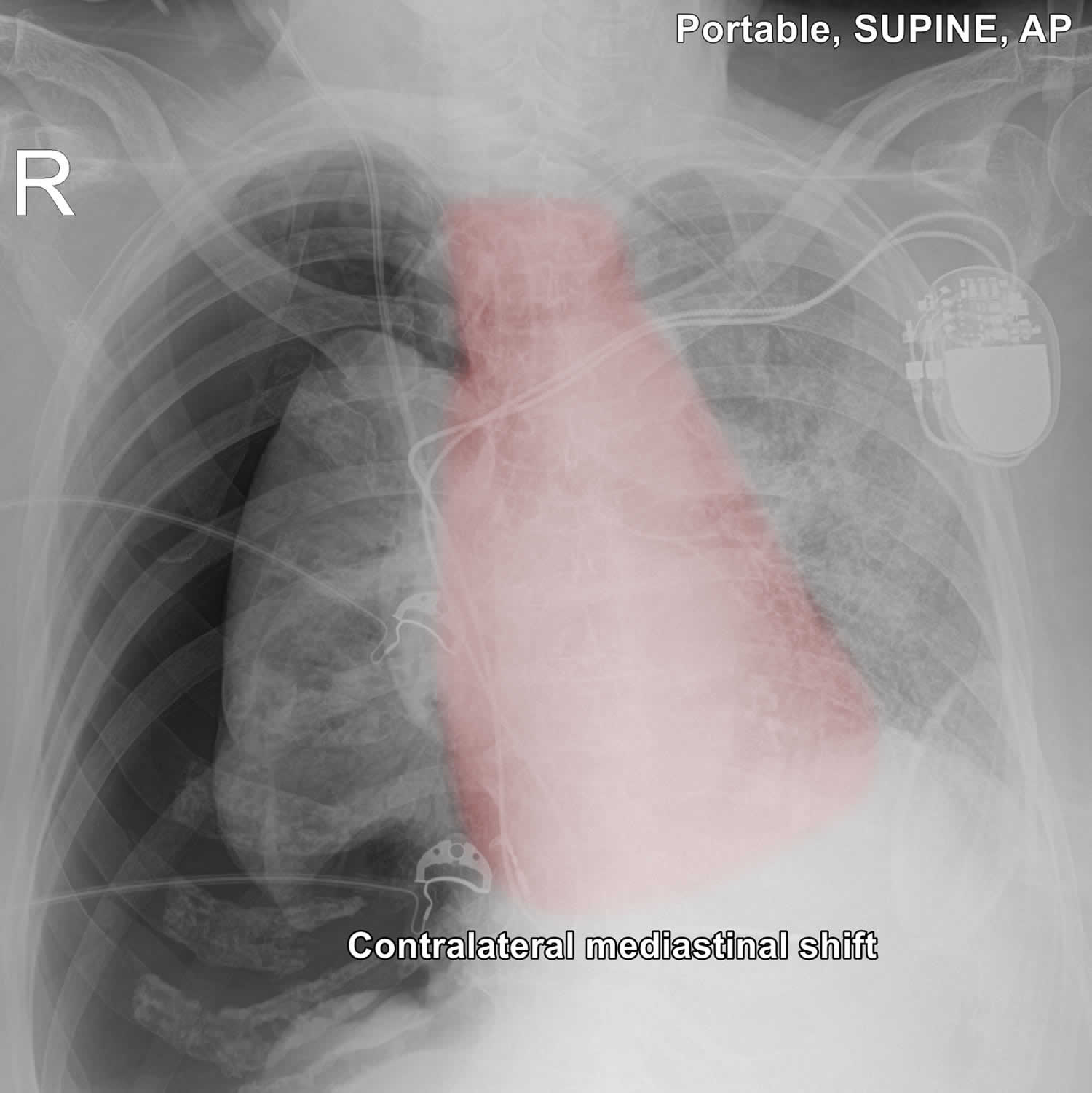
Footnotes: Presence of a large right tension pneumothorax and the resultant collapse of the right lung is evident. Three worrisome features are also present:
- Significant mediastinal shift to the left
- Depressed right hemidiaphragm
- Widened intercostal spaces and marked asymmetric expansion of the right hemithorax
The tracheal tube and right internal jugular vein (IJV) central venous catheter (CVC) line are in a normal position, as well as the leads of the dual chamber pacemaker. Increased interstitial markings on the left, suggestive of decompensated heart failure. Minimally displaced CT-confirmed (not shown) fractures of the anterior aspect of ribs 4-6 on the right.
[Source 6 ]Chest anatomy
Your chest cavity also called the thoracic cavity is formed by the ribs, the muscles of the chest, the sternum (breastbone), and the thoracic portion of the vertebral column. Within your thoracic cavity are 3 smaller cavities: (a) 2 pleural cavities (fluid-filled spaces one around each lung), your left pleural cavity (holds your left lung) and your right pleural cavity (holds your right lung) and (b) a central portion of your thoracic cavity between your lungs called the mediastinum (media- = middle; -stinum = partition). The mediastinum is the central portion of your thoracic cavity between your lungs, extending from the base of your neck (from your first rib and sternum) to the diaphragm. The mediastinum contains your heart (pericardial cavity, peri- = around; -cardial = heart, a fluid-filled space that surrounds your heart), the major blood vessels connected to your heart and lungs, the trachea (windpipe) and bronchi, the esophagus (foodpipe), the thymus, and lymph nodes but not your lungs. Your right and left lungs are on either side of the mediastinum. The diaphragm is a dome-shaped muscle that separates the thoracic cavity from the abdominopelvic cavity.
Your mediastinum is divided into several parts, which researchers call compartments. The traditional or classical model divides your mediastinum into four parts:
- Superior mediastinum: The top part, located superior to (above) your heart.
- Anterior mediastinum: The part anterior to (in front of) your heart, between your heart and your sternum (breastbone).
- Middle mediastinum: The part that contains your heart.
- Posterior mediastinum: The part posterior to (behind) your heart.
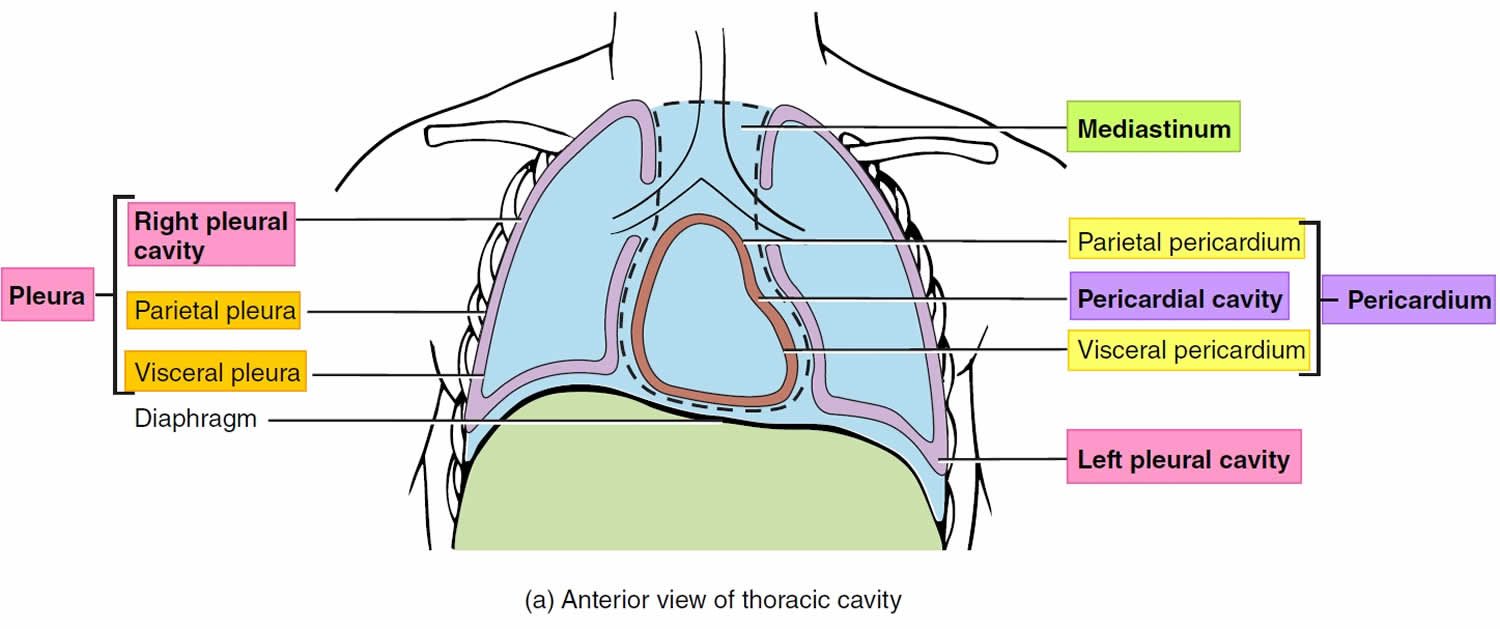
A membrane is a thin, pliable tissue that covers, lines, partitions, or connects internal organs (viscera). One example is a slippery, double-layered membrane associated with body cavities that does not open directly to the exterior called a serous membrane. Serous membrane covers your internal organs (viscera) within the thoracic and abdominal cavities and also lines the walls of the thorax and abdomen. The parts of a serous membrane are (1) the parietal layer (outer layer), a thin epithelium that lines the walls of the cavities, and (2) the visceral layer (inner layer), a thin epithelium that covers and adheres to the viscera within the cavities. Between the two layers is a potential space that contains a small amount of lubricating fluid (serous fluid). The fluid allows the internal organs (viscera) to slide somewhat during movements, such as when the lungs inflate and deflate during breathing.
Within the right and left sides of your thoracic cavity (chest cavity), the compartments that contain your lungs, on either side of the mediastinum, are lined with a membrane called the parietal pleura (outer serous membrane) lining the inside of your rib cage (parietal pleura lines the chest wall) and covering the superior surface of the diaphragm. A similar membrane, called the visceral pleura (inner serous membrane), clings to the surface of your lungs forming the external surface of your lung. The visceral (inner) and parietal (outer) pleural membranes are separated only by a thin film of watery fluid called serous fluid, which is secreted by the parietal and visceral pleural membranes. Although no actual space normally exists between the parietal (outer) and visceral (inner) pleural membranes, the potential space between them is called the pleural cavity. The parietal pleura (outer membrane) and visceral pleura (inner membrane) slide with little friction across the cavity walls as your lungs move, expand and collapse during respiration.
Your heart, which is located in the broadest portion of the mediastinum, is surrounded by pericardial membranes called the pericardium. Your pericardium is a protective, fluid-filled sac that surrounds your heart and helps it function properly.
Normally, your pericardium is flexible and stretchy. It can easily expand with your heart as your heart fills up with blood and then contracts to pump the blood out to your body. Pericardial conditions and disorders prevent your heart from expanding as it should. As a result, your heart can’t fill and pump blood efficiently to the rest of your body. This can lead to dangerous complications, including heart failure and cardiogenic shock.
Figure 3. Chest anatomy

Figure 4. Thoracic cavity
Footnote: The black dashed lines indicate the borders of the mediastinum.
Figure 5. Thoracic cavity transverse section
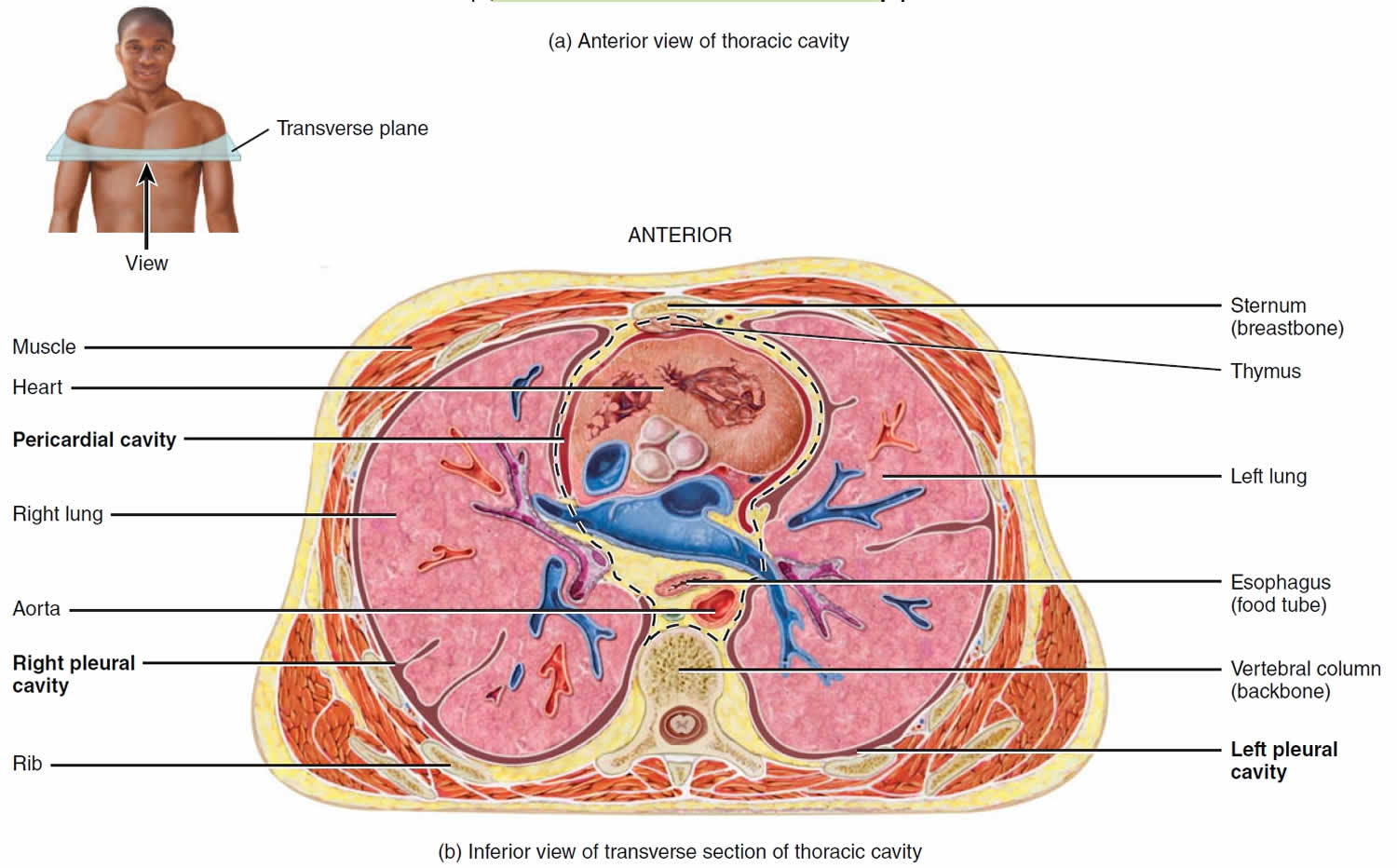
Figure 6. Mediastinum
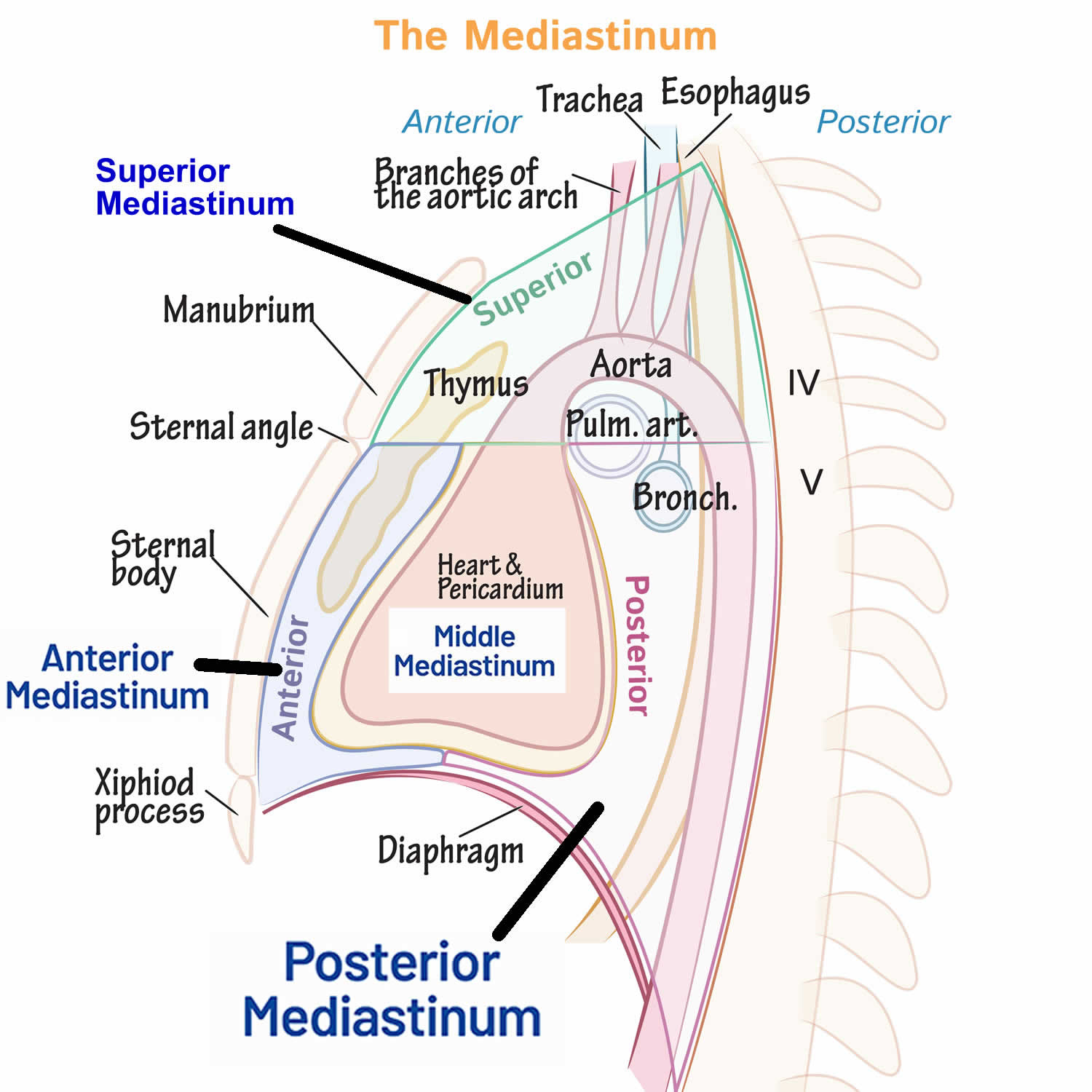
Figure 7. Respiratory system
Tension pneumothorax causes
Tension pneumothorax can be traumatic or atraumatic. Outside of the hospital, traumatic pneumothorax may arise from penetrating or blunt chest trauma, rib fractures, and pulmonary decompression sickness 7, 8. In the hospital setting, traumatic pneumothorax may arise iatrogenically from the following procedures 9:
- Central venous catheterization (CVC) in the subclavian or internal jugular vein
- Lung biopsy
- Barotrauma due to positive pressure ventilation (PPV)
- Percutaneous tracheostomy
- Thoracentesis
- Pacemaker insertion
- Bronchoscopy
- Cardiopulmonary resuscitation
- Intercostal nerve block
Atraumatic pneumothorax may have an unknown cause (primary) or arise as a complication of an underlying lung disease (secondary).
Risk factors for a collapsed lung
Pneumothorax in those over 40 years of age is commonly seen in the background of emphysema or chronic bronchitis. Occasionally, asthma, and other lung disease can cause a pneumothorax.
In younger patients, pneumothorax may occur spontaneously or due to chest trauma. Spontaneous pneumothorax commonly occurs in tall, thin young men (sex ratio: 6:1), due to rupture of small subpleural ‘blebs’. Trauma such as a rib fracture, or penetrating chest wall injury, may also cause pneumothorax.
Risk factors for a pneumothorax include:
- Your sex. In general, men are far more likely to have a pneumothorax than are women.
- Smoking. The risk increases with the length of time and the number of cigarettes smoked, even without emphysema.
- Age. The type of pneumothorax caused by ruptured air blisters is most likely to occur in people between 20 and 40 years old, especially if the person is a very tall and underweight.
- Genetics. Certain types of pneumothorax appear to run in families.
- Lung disease. Having an underlying lung disease — especially chronic obstructive pulmonary disease (COPD) — makes a collapsed lung more likely.
- Mechanical ventilation. People who need mechanical ventilation to assist their breathing are at higher risk of pneumothorax.
- Previous pneumothorax. Anyone who has had one pneumothorax is at increased risk of another, usually within one to two years of the first.
- Pregnancy
- Have a tall, thin body type, especially if you are a man.
- Marfan syndrome.
- Endometriosis.
Tension pneumothorax signs and symptoms
Tension pneumothorax signs and symptoms are usually more dramatic than those seen with a simple pneumothorax, and clinical interpretation of these is crucial for diagnosing and treating the condition. Tension pneumothorax is classically characterized by hypotension (low blood pressure) and hypoxia (low blood oxygen). On examination, breath sounds are absent on the affected lung and the trachea deviates away from the affected side. The chest may also be hyperresonant to percussion and often feels somewhat distended, tense, and poorly compressible to palpation; neck vein distention (jugular venous distention) and fast heart rate (tachycardia) may be present. If on mechanical ventilation, the airway pressure alarms are triggered.
Because of subtle presentations that do not always present with the classically described clinical findings of tension pneumothorax or the complexity of the patient with critical illness or injury to describe a tension pneumothorax, actual case reports include descriptions of the diagnosis of tension pneumothorax being missed or delayed. Nevertheless, tension pneumothorax should always be a consideration when acute breathing and cardiovascular compromise occurs.
Symptoms of tension pneumothorax may include chest pain (90%), dyspnea (80%), anxiety, fatigue, or acute epigastric pain (a rare finding).
Tension pneumothorax complications
Tension pneumothorax is potentially fatal. In patients who survive this condition, complications may arise from the lung injury itself or chest tube thoracostomy, which include the following:
- Pneumopericardium is a condition where air or gas accumulates in the pericardial sac, the sac surrounding the heart. It’s often caused by trauma, but can also occur after certain procedures or due to underlying conditions.
- Pneumoperitoneum refers to the presence of air or gas within the peritoneal cavity, often detected on imaging like X-rays, and is most commonly caused by a perforation of a hollow abdominal organ. In some cases, air can leak from the lungs into the peritoneal cavity, particularly in patients on mechanical ventilation or air from the chest can migrate into the abdomen.
- Hemothorax is a collection of blood in the pleural cavity (the space between the chest wall and the lung) often caused by trauma, but can also occur due to other medical conditions
- Bronchopleural fistula is an abnormal connection between the bronchial tubes and the pleural space, often a complication of lung surgery or other lung conditions, leading to air leaks and potential complications.
- Damage to the neurovascular bundle during chest tube thoracostomy
- Pain and skin infection at the chest tube thoracostomy site
- Empyema
- Pyopneumothorax is a pleural collection of pus and gas, often occurring as a complication of pneumonia, lung abscess, or empyema, and can be a life-threatening emergency
Timely diagnosis and management help improve outcomes in patients with tension pneumothorax.
Tension pneumothorax diagnosis
Tension pneumothorax is a medical emergency. A quick, focused examination will reveal severe respiratory distress in a hypotensive patient. The affected chest is enlarged and has no breath sounds. The trachea and mediastinum shift to the opposite side. Air escaping after large-bore needle insertion in the second intercostal space in the midclavicular line confirms the diagnosis.
History will reveal the cause of the tension pneumothorax. A history of recent trauma or receiving a medical procedure such as positive pressure ventilation (PPV) or central venous catheterization (CVC) is common. Some may have an underlying lung condition like asthma or pneumonia. Besides shortness of breath, patients may complain of sharp, pleuritic chest pain radiating to the ipsilateral back or shoulder.
Other early physical findings include fast breathing (tachypnea), fast heart rate (tachycardia), chest retractions, cyanosis, and jugular venous distension. The affected hemithorax will have reduced tactile fremitus and hyper-resonance. Subcutaneous emphysema may be seen in some cases.
When in doubt about the diagnosis, the patient’s status, whether stable or unstable, determines the next evaluation steps. A bedside ultrasound, if available, can confirm the diagnosis in the presence of hemodynamic instability. Patients should concurrently be stabilized, and the airway, breathing, and circulation assessed.
Ultrasound is 94% sensitive and 100% specific with a skilled operator. Bedside ultrasound can detect pneumothorax, which may be useful in unstable patients. Ultrasound findings include the absence of lung sliding and the presence of a lung point 10, 11, 12, 13, 14. Needle decompression may still be performed if the diagnosis remains doubtful after performing a bedside ultrasound.
Imaging studies is recommended when the patient is hemodynamically stable. The initial assessment involves a chest X-ray (CXR) to confirm the diagnosis 15, 16.
Chest X-ray (CXR) can demonstrate one or more of the following:
- A thin line representing the edge of the visceral pleura
- Effacement of lung markings distally to this line
- Complete ipsilateral lung collapse
- The mediastinal shift away from the pneumothorax in tension pneumothorax
- Subcutaneous emphysema
- Tracheal deviation to the contralateral side of tension pneumothorax
- Flattening of the hemidiaphragm on the ipsilateral side (tension pneumothorax)
A chest computed tomography (CT) can be done if the diagnosis is unclear on chest X-ray (CXR). Chest CT is the most reliable imaging study for diagnosing pneumothorax, though it is not recommended for routine use 1.
Tension pneumothorax differential diagnosis
The differential diagnosis of tension pneumothorax includes the following 1:
- Pulmonary embolism (PE)
- Acute coronary syndrome
- Acute aortic dissection
- Heart attack (myocardial infarction)
- Pneumonia
- Acute pericarditis
- Rib fracture
- Diaphragmatic injuries
The combined physical findings of severe respiratory distress, hypotension, an enlarged hemithorax, ipsilaterally absent breath sounds, and contralateral tracheal deviation will distinguish tension pneumothorax from the other conditions.
Tension pneumothorax treatment
Tension pneumothorax is a medical emergency that is usually managed in the emergency department (ER) or the intensive care unit (ICU). Management strategies depend on the patient’s hemodynamic stability. Airway, breathing, and circulation must be assessed in any patient presenting with chest trauma. Penetrating chest wounds must be covered with an airtight occlusive bandage and clean plastic sheeting.
Administration of 100% supplemental oxygen can help reduce the pneumothorax’s size by decreasing the alveolar nitrogen partial pressure. Oxygen supplementation creates a diffusion gradient for nitrogen, thus accelerating pneumothorax resolution 1. Only 1.25% of the air is absorbed without oxygen in 24 hours 1. Positive pressure ventilation (PPV) should be avoided initially, as it may increase the tension pneumothorax’s size. Patients may be placed on positive pressure ventilation (PPV) after a chest tube is placed 17, 18.
Immediate needle decompression must be performed without delay if the patient is hemodynamically unstable and clinical suspicion is high for pneumothorax. Needle placement is at the 2nd intercostal space in the midclavicular line above the rib with an angiocatheter. The American College of Surgeons Advanced Trauma Life Support recommends placement in the fourth or fifth intercostal space along the midaxillary line, as it has been associated with improved success at decompression. Air will usually gush out. Because needle decompression causes a simple pneumothorax, chest tube thoracostomy should be done immediately thereafter. However, quick lung re-expansion increases the risk of pulmonary edema. A chest X-ray (CXR) is obtained, and chest tube thoracostomy is performed following needle decompression 19.
Serial chest X-rays (CXRs) can help assess pneumothorax resolution. The chest tube is removed when the lung has fully re-expanded, no air leaks are visible, and the patient has clinically improved.
Chest tubes are usually managed by experienced nurses, respiratory therapists, surgeons, and intensive care physicians. Chest tube thoracostomy suffices in 90% of pneumothorax cases. A video-assisted thoracoscopic surgery (VATS) or thoracotomy is performed on patients with pneumothoraces that do not resolve with chest tube thoracostomy 20, 21, 22, 23.
Patients requiring surgical intervention frequently have bilateral pneumothoraces, recurrent ipsilateral pneumothoraces, pulmonary decompression sickness, and more than 7 days of non-resolving air leaks 1. During video-assisted thoracoscopic surgery (VATS), the pneumothorax is treated with pleurodesis, which can be mechanical or chemical. Mechanical pleurodesis options include abrasive scratchpads, dry gauze, and parietal pleura stripping. Chemical pleurodesis is an alternative if the patient cannot tolerate mechanical pleurodesis. Chemical pleurodesis options include talc, minocycline, doxycycline, or tetracycline. Recent studies show that pleurodesis can decrease the rate of pneumothorax recurrence. Mechanical pleurodesis reduces pneumothorax recurrence risk to less than 5% 24, 25.
Tension pneumothorax prognosis
Tension pneumothorax can progress rapidly to respiratory insufficiency, cardiovascular collapse, and death if not recognized and treated immediately 26, 27. Diagnostic and management delays are associated with a poor prognosis. Early recognition and management is life-saving.
Uncomplicated pneumothorax may recur within 6 months to 3 years, especially in smokers and patients with chronic obstructive pulmonary disease (COPD) and acquired immunodeficiency syndrome (AIDS) 28, 29.
Ventilator-related tension pneumothorax has been found to have dire outcomes and frequently results in death 30. By comparison, procedure-related tension pneumothorax has better outcomes than ventilator-related cases 31.
- Jalota Sahota R, Sayad E. Tension Pneumothorax. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559090[↩][↩][↩][↩][↩][↩]
- ATLS Subcommittee; American College of Surgeons’ Committee on Trauma; International ATLS working group. Advanced trauma life support (ATLS®): the ninth edition. J Trauma Acute Care Surg. 2013 May;74(5):1363-6. doi: 10.1097/TA.0b013e31828b82f5[↩]
- Rojas R, Wasserberger J, Balasubramaniam S. Unsuspected tension pneumothorax as a hidden cause of unsuccessful resuscitation. Ann Emerg Med. 1983 Jun;12(6):411-2. doi: 10.1016/s0196-0644(83)80502-2[↩]
- Light RW. Pleural diseases. Dis Mon. 1992 May;38(5):266-331. doi: 10.1016/0011-5029(92)90007-c[↩]
- Tirimanna R, Myerson J, Okorie M, Dorman E. Diagnosis of spontaneous secondary tension pneumothorax following apparent recovery from coronavirus disease 2019 pneumonitis: a case report. J Med Case Rep. 2022 Feb 22;16(1):88. doi: 10.1186/s13256-022-03313-x[↩]
- Tension pneumothorax (annotated signs). https://radiopaedia.org/cases/tension-pneumothorax-annotated-signs#image-51856629[↩]
- Melton LJ 3rd, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota: 1950 to 1974. Am Rev Respir Dis. 1979 Dec;120(6):1379-82. doi: 10.1164/arrd.1979.120.6.1379[↩]
- Gupta D, Hansell A, Nichols T, Duong T, Ayres JG, Strachan D. Epidemiology of pneumothorax in England. Thorax. 2000 Aug;55(8):666-71. https://pmc.ncbi.nlm.nih.gov/articles/instance/1745823/pdf/v055p00666.pdf[↩]
- Sharma A, Jindal P. Principles of diagnosis and management of traumatic pneumothorax. J Emerg Trauma Shock. 2008 Jan;1(1):34-41. doi: 10.4103/0974-2700.41789[↩]
- Gordon R. The deep sulcus sign. Radiology. 1980 Jul;136(1):25-7. doi: 10.1148/radiology.136.1.7384513[↩]
- DORNHORST AC, PIERCE JW. Pulmonary collapse and consolidation; the role of collapse in the production of lung field shadows and the significance of segments in inflammatory lung disease. J Fac Radiol. 1954 Apr;5(4):276-81.[↩]
- Zhang M, Liu ZH, Yang JX, Gan JX, Xu SW, You XD, Jiang GY. Rapid detection of pneumothorax by ultrasonography in patients with multiple trauma. Crit Care. 2006;10(4):R112. doi: 10.1186/cc5004[↩]
- Soldati G, Iacconi P. The validity of the use of ultrasonography in the diagnosis of spontaneous and traumatic pneumothorax. J Trauma. 2001 Aug;51(2):423. doi: 10.1097/00005373-200108000-00045[↩]
- Shostak E, Brylka D, Krepp J, Pua B, Sanders A. Bedside sonography for detection of postprocedure pneumothorax. J Ultrasound Med. 2013 Jun;32(6):1003-9. doi: 10.7863/ultra.32.6.1003[↩]
- Zarogoulidis P, Kioumis I, Pitsiou G, Porpodis K, Lampaki S, Papaiwannou A, Katsikogiannis N, Zaric B, Branislav P, Secen N, Dryllis G, Machairiotis N, Rapti A, Zarogoulidis K. Pneumothorax: from definition to diagnosis and treatment. J Thorac Dis. 2014 Oct;6(Suppl 4):S372-6. doi: 10.3978/j.issn.2072-1439.2014.09.24[↩]
- Arao K, Mase T, Nakai M, Sekiguchi H, Abe Y, Kuroudu N, Oobayashi O. Concomitant Spontaneous Tension Pneumothorax and Acute Myocardial Infarction. Intern Med. 2019 Apr 15;58(8):1131-1135. doi: 10.2169/internalmedicine.1422-18[↩]
- Vallee P, Sullivan M, Richardson H, Bivins B, Tomlanovich M. Sequential treatment of a simple pneumothorax. Ann Emerg Med. 1988 Sep;17(9):936-42. doi: 10.1016/s0196-0644(88)80676-0[↩]
- Henry M, Arnold T, Harvey J; Pleural Diseases Group, Standards of Care Committee, British Thoracic Society. BTS guidelines for the management of spontaneous pneumothorax. Thorax. 2003 May;58 Suppl 2(Suppl 2):ii39-52. doi: 10.1136/thorax.58.suppl_2.ii39[↩]
- Dominguez KM, Ekeh AP, Tchorz KM, Woods RJ, Walusimbi MS, Saxe JM, McCarthy MC. Is routine tube thoracostomy necessary after prehospital needle decompression for tension pneumothorax? Am J Surg. 2013 Mar;205(3):329-32; discussion 332. doi: 10.1016/j.amjsurg.2013.01.004[↩]
- Terada T, Nishimura T, Uchida K, Hagawa N, Esaki M, Mizobata Y. How emergency physicians choose chest tube size for traumatic pneumothorax or hemothorax: a comparison between 28Fr and smaller tube. Nagoya J Med Sci. 2020 Feb;82(1):59-68. doi: 10.18999/nagjms.82.1.59[↩]
- Chen KC, Chen PH, Chen JS. New options for pneumothorax management. Expert Rev Respir Med. 2020 Jun;14(6):587-591. doi: 10.1080/17476348.2020.1740090[↩]
- Eguchi M, Abe T, Tedokon Y, Miyagi M, Kawamoto H, Nakasone Y. [Traumatic Intercostal Lung Hernia Repaired by Video-assisted Thoracoscopic Surgery;Report of a Case]. Kyobu Geka. 2019 Nov;72(12):1038-1041. Japanese.[↩]
- Johnson G. Traumatic pneumothorax: is a chest drain always necessary? J Accid Emerg Med. 1996 May;13(3):173-4. https://pmc.ncbi.nlm.nih.gov/articles/instance/1342681/pdf/jaccidem00012-0021.pdf[↩]
- Paydar S, Ghahramani Z, Ghoddusi Johari H, Khezri S, Ziaeian B, Ghayyoumi MA, Fallahi MJ, Niakan MH, Sabetian G, Abbasi HR, Bolandparvaz S. Tube Thoracostomy (Chest Tube) Removal in Traumatic Patients: What Do We Know? What Can We Do? Bull Emerg Trauma. 2015 Apr;3(2):37-40. https://pmc.ncbi.nlm.nih.gov/articles/PMC4771264[↩]
- van den Brande P, Staelens I. Chemical pleurodesis in primary spontaneous pneumothorax. Thorac Cardiovasc Surg. 1989 Jun;37(3):180-2. doi: 10.1055/s-2007-1020313[↩]
- Barton ED, Rhee P, Hutton KC, Rosen P. The pathophysiology of tension pneumothorax in ventilated swine. J Emerg Med. 1997 Mar-Apr;15(2):147-53. doi: 10.1016/s0736-4679(96)00312-5[↩]
- Nelson D, Porta C, Satterly S, Blair K, Johnson E, Inaba K, Martin M. Physiology and cardiovascular effect of severe tension pneumothorax in a porcine model. J Surg Res. 2013 Sep;184(1):450-7. doi: 10.1016/j.jss.2013.05.057[↩]
- Huang TW, Lee SC, Cheng YL, Tzao C, Hsu HH, Chang H, Chen JC. Contralateral recurrence of primary spontaneous pneumothorax. Chest. 2007 Oct;132(4):1146-50. doi: 10.1378/chest.06-2772[↩]
- British Thoracic Society Fitness to Dive Group, Subgroup of the British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines on respiratory aspects of fitness for diving. Thorax. 2003 Jan;58(1):3-13. https://pmc.ncbi.nlm.nih.gov/articles/instance/1746450/pdf/v058p00003.pdf[↩]
- Hsu CW, Sun SF, Lee DL, Chu KA, Lin HS. Clinical characteristics, hospital outcome and prognostic factors of patients with ventilator-related pneumothorax. Minerva Anestesiol. 2014 Jan;80(1):29-38. https://www.minervamedica.it/en/getfreepdf/MWVaVGQya2hJUGRGdUxSTDVTd0RpeFF2dHNOY2lzQmJabTBZQURFdTBXL3o3WHlpcldDRjd6Nm9aNkpTSzdFYQ%253D%253D/R02Y2014N01A0029.pdf[↩]
- Chen KY, Jerng JS, Liao WY, Ding LW, Kuo LC, Wang JY, Yang PC. Pneumothorax in the ICU: patient outcomes and prognostic factors. Chest. 2002 Aug;122(2):678-83. doi: 10.1378/chest.122.2.678[↩]





{kind=link}