
Contents
- What is endometriosis
- Female reproductive system
- Endometriosis complications
- Endometriosis symptoms
- Endometriosis causes
- Endometriosis diagnosis
- Endometriosis treatment
- Endometriosis prognosis
What is endometriosis
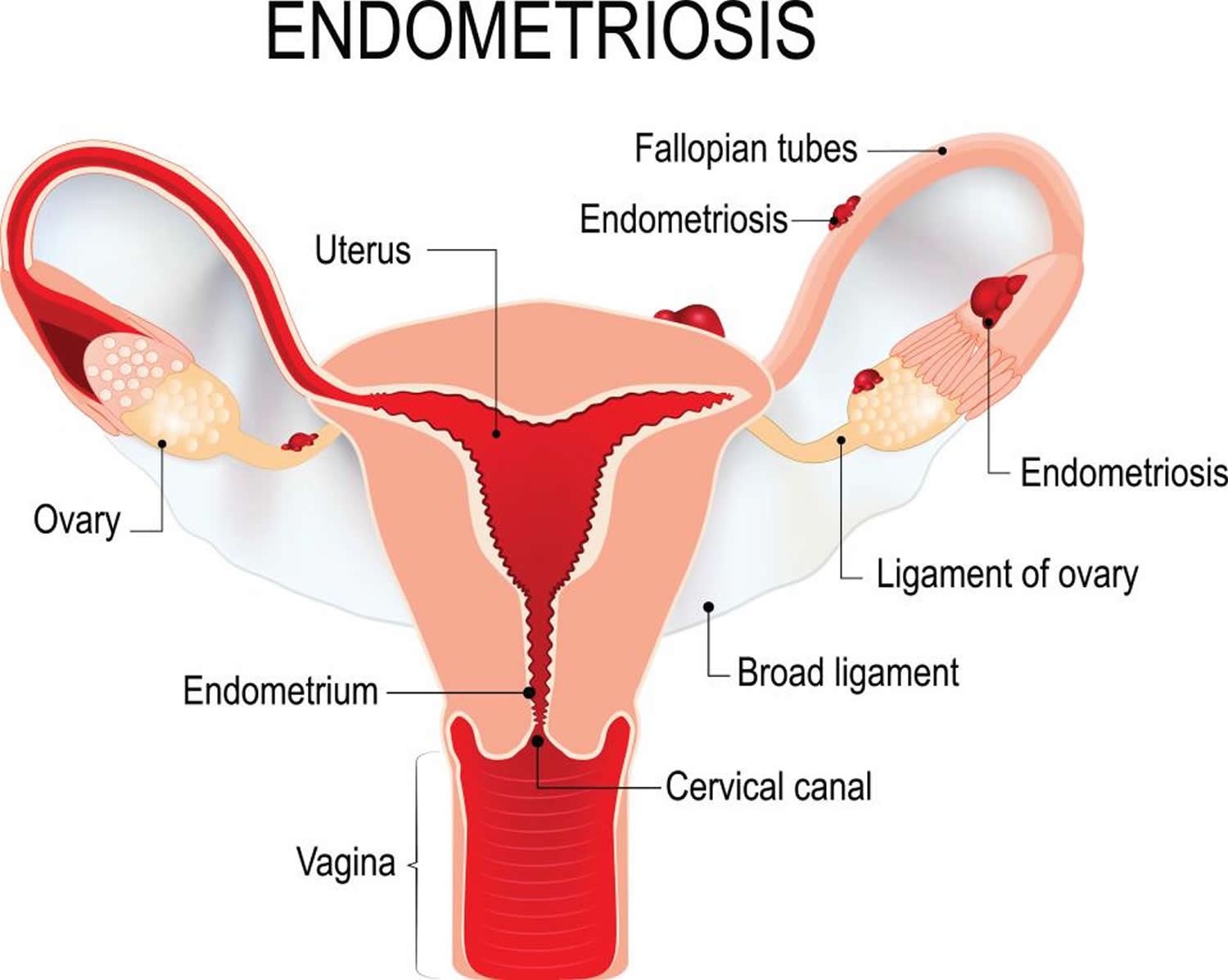
Endometriosis is a condition in which the tissue that is similar to the lining of your uterus called the endometrium (the inner lining of your uterus) that normally grows inside your uterus (womb) grows outside your uterus 1, 2, 3, 4, 5, 6, 7, 8. Your uterus or womb is the place where your baby grows during pregnancy. Endometriosis happens when tissue similar to the lining of your uterus (the endometrium) grows outside of your uterus and on other areas in your body where it doesn’t belong. Endometriosis can grow or implants in the cul-de-sac (the space behind the uterus), outer surfaces of the uterus, on the ovaries, fallopian (uterine) tubes, intestines and rectum, ureters or bladder. Rarely, endometriosis appears in other parts of your body, such as your lungs, brain, and skin 9. With endometriosis, the displaced endometrial tissue continues to act as it normally would — it thickens, breaks down and bleeds with each menstrual cycle. Because the displaced endometrium (the inner lining of your uterus) has no way to exit your body, it becomes trapped. When endometriosis involves the ovaries, cysts called endometriomas may form. Surrounding tissue can become irritated, eventually developing scar tissue and adhesions — abnormal bands of fibrous tissue that can cause pelvic tissues and organs to stick to each other and may make it harder for you to get pregnant. Endometriosis can cause pelvic pain — sometimes severe — especially during your period.
Endometriosis may affect more than 11% of American women between 15 and 44 10. Endometriosis is especially common among women in their 30s and 40s and can cause infertility.
Pelvic pain is the most common symptom of endometriosis. Women with endometriosis may have many different kinds of pain:
- Very painful menstrual cramps. The pain may get worse over time.
- Chronic (long-term) pain in the lower back and pelvis
- Pain during or after sex. This is usually described as a “deep” pain and is different from pain felt at the entrance to the vagina when penetration begins.
- Intestinal pain
- Painful bowel movements or pain when urinating during menstrual periods. In rare cases, you may also find blood in your stool or urine.
Endometriosis implants respond to changes in estrogen, a female hormone. The implants may grow and bleed like the uterine lining does during the menstrual cycle. Surrounding tissue can become irritated, inflamed, and swollen. The breakdown and bleeding of this tissue each month also can cause scar tissue, called adhesions, to form. Sometimes adhesions can cause organs to stick together. The bleeding, inflammation, and scarring can cause pain, especially before and during menstruation.
To diagnose endometriosis and other conditions that can cause pelvic pain, your doctor will ask you to describe your symptoms, including the location of your pain and when it occurs.
Tests to check for clues of endometriosis include:
- Pelvic exam. During a pelvic exam, your doctor manually feels (palpates) areas in your pelvis for abnormalities, such as cysts on your reproductive organs or scars behind your uterus. Often it’s not possible to feel small areas of endometriosis, unless they’ve caused a cyst to form.
- Ultrasound. This test uses high-frequency sound waves to create images of the inside of your body. To capture the images, a device called a transducer is either pressed against your abdomen or inserted into your vagina called transvaginal ultrasound. Both types of ultrasound may be done to get the best view of your reproductive organs. Ultrasound imaging won’t definitively tell your doctor whether you have endometriosis, but it can identify cysts associated with endometriosis (endometriomas).
- Magnetic resonance imaging (MRI). This exam uses a magnetic field and radio waves to make images of the organs and tissues within the body. For some, an MRI helps with surgical planning. It gives your surgeon detailed information about the location and size of endometriosis growths.
- Laparoscopy. Medical management is usually tried first. But to be certain you have endometriosis, your doctor may refer you to a surgeon to look inside your abdomen for signs of endometriosis using a surgical procedure called laparoscopy. A laparoscopy can provide information about the location, extent and size of the endometriosis growths to help determine the best treatment options. While you’re under general anesthesia, your surgeon makes a tiny incision near your navel (belly button) and inserts a slender viewing instrument called a laparoscope, looking for endometrial tissue outside your uterus. Your surgeon may take a tissue sample called biopsy for more testing. With proper planning, a surgeon can often treat endometriosis during the laparoscopy so that you need only one surgery.
Definitive diagnosis requires visualization of lesions during surgery, resulting in a delay in diagnosis that globally averages 7 years from symptom onset 11.
Fortunately, effective treatments are available that can help you manage your symptoms and improve your chances of getting pregnant.
Treatment for endometriosis often involves medicine or surgery. The approach you and your doctor choose will depend on how serious your symptoms are and whether you hope to become pregnant. Typically, medicine is recommended first. If it doesn’t help enough, surgery becomes an option.
How common is endometriosis?
Endometriosis is a common health problem for women. Researchers think that at least 11% of women, or more than 6.5 million women in the United States, have endometriosis 12. According to the findings of systematic reviews, the prevalence of endometriosis is around 3 to 5% in the general female population of reproductive age, but around 30% in women with infertility, 50% in women with pelvic pain 13, 14, 15, and as high as 65 to 75% in symptomatic adolescents who do not respond to medical treatment 16, 17.
Who gets endometriosis?
Endometriosis can happen in any girl or woman who has menstrual periods, but it is more common in women in their 30s and 40s.
You might be more likely to get endometriosis if you have:
- Never had children
- Menstrual periods that last more than seven days
- Short menstrual cycles (27 days or fewer)
- A family member (mother, aunt, sister) with endometriosis
- A medical condition that blocks the normal flow of menstrual blood from your body during your menstrual period.
How can I prevent endometriosis?
You can’t prevent endometriosis. But you can reduce your chances of developing it by lowering the levels of the hormone estrogen in your body. Estrogen helps to thicken the lining of your uterus during your menstrual cycle.
To keep lower estrogen levels in your body, you can:
- Talk to your doctor about hormonal birth control methods, such as pills, patches or rings with lower doses of estrogen.
- Exercise regularly (more than 4 hours a week). This will also help you keep a low percentage of body fat 18. Regular exercise and a lower amount of body fat help decrease the amount of estrogen circulating through the body.
- Avoid large amounts of alcohol. Alcohol raises estrogen levels 19. No more than one drink per day is recommended for women who choose to drink alcohol.
- Avoid large amount of drinks with caffeine. Studies show that drinking more than one caffeinated drink a day, especially sodas and green tea, can raise estrogen levels 20.
Can I get pregnant if I have endometriosis?
Yes. Many women with endometriosis get pregnant. But, you may find it harder to get pregnant. Researchers think endometriosis may affect as many as one in every two women with infertility 21.
No one knows exactly how endometriosis might cause infertility. Some possible reasons include 22:
- Patches of endometriosis block off or change the shape of the pelvis and reproductive organs. This can make it harder for the sperm to find the egg.
- The immune system, which normally helps defend the body against disease, attacks the embryo.
- The endometrium (the layer of the uterine lining where implantation happens) does not develop as it should.
If you have endometriosis and are having trouble getting pregnant, talk to your doctor. He or she can recommend treatments, such as surgery to remove the endometrial growths 22.
What other health conditions are linked to endometriosis?
Research shows a link between endometriosis and other health problems in women and their families. Some of these include:
- Allergies, asthma, and chemical sensitivities 23
- Autoimmune diseases, in which your body’s immune system that fights illness attacks itself instead. These can include multiple sclerosis, lupus, and some types of hypothyroidism 24
- Chronic fatigue syndrome and fibromyalgia 24
- Certain cancers, such as ovarian cancer 25 and breast cancer 26.
Does endometriosis go away on its own?
For some women diagnosed with endometriosis, endometriosis patches go away on their own 27.
Also, after menopause, symptoms of endometriosis typically lessen because there is a drop in the natural hormones and the growths gradually shrink. However, this is not true for all women. If a woman takes hormones for menopausal symptoms, both her pain symptoms and the growths may return.
Women with endometriosis who are experiencing symptoms, especially after menopause, should talk with their healthcare providers about treatment options.
Does endometriosis go away after menopause?
For some women, the painful symptoms of endometriosis improve after menopause. As the body stops making the hormone estrogen, the growths shrink slowly. However, some women who take menopausal hormone therapy may still have symptoms of endometriosis.
If you are having symptoms of endometriosis after menopause, talk to your doctor about your treatment options.
Female reproductive system
The female reproductive system includes parts of the female body that are involved in sexual activity, fertility, pregnancy and childbirth. The female reproductive system is made up of female body parts that include the following:
- Ovaries — There are 2 ovaries, which are about the size and shape of almonds, 1 ovary on each side of the uterus where female hormones (estrogen and progesterone) are produced, and eggs (ova) are stored to mature. Every month, an egg (ovum) is released. This is called ovulation. All the other female reproductive organs are there to transport, nurture and otherwise meet the needs of the egg or developing fetus.
- Fallopian tubes are 2 thin tubes that connect your ovaries to your uterus (womb), allowing the egg (ovum) to travel to your uterus (womb).
- The fallopian tubes are about 10 cm long and begin as funnel-shaped passages next to the ovary. They have a number of finger-like projections known as fimbriae on the end near the ovary. When an egg is released by the ovary it is ‘caught’ by one of the fimbriae and transported along the fallopian tube to the uterus. The egg is moved along the fallopian tube by the wafting action of cilia — hairy projections on the surfaces of cells at the entrance of the fallopian tube — and the contractions made by the tube. It takes the egg about 5 days to reach the uterus and it is on this journey down the fallopian tube that fertilisation may occur if a sperm penetrates and fuses with the egg. The egg, however, is usually viable for only 24 hours after ovulation, so fertilization usually occurs in the top one-third of the fallopian tube.
- Uterus (the womb) — Your uterus also known as the womb is a hollow muscular organ about the size of a pear (in women who have never been pregnant) that exists to house a developing fertilized egg (zygote). The main part of the uterus which sits in the pelvic cavity is called the body of the uterus, while the rounded region above the entrance of the fallopian tubes is the fundus and its narrow outlet, which protrudes into the vagina, is the cervix. The thick wall of your uterus is composed of 3 layers. The inner layer is known as the endometrium. The inner lining of your uterus (endometrium) thickens with blood and other substances every month. If an egg (ovum) has been fertilized (zygote), pregnancy occurs, the fertilized egg (zygote) will burrow into the endometrium in your uterus, where it will stay for the rest of its growth, growing into a fetus and then a baby. Your uterus (womb) will expand during a pregnancy to make room for the growing fetus. A part of the wall of the fertilized egg (zygote), which has burrowed into the endometrium, develops into the placenta. If an egg has not been fertilized, the endometrial lining is shed at the end of each menstrual cycle, this lining flows out of your body. This is known as menstruation or your period.
- The myometrium is the large middle layer of your uterus, which is made up of interlocking groups of muscle. It plays an important role during the birth of a baby, contracting rhythmically to move the baby out of the body via the birth canal (vagina).
- Cervix is the lower part of your uterus, that connects your uterus to your vagina.
- Vagina is a muscular tube connecting your cervix to the outside of your body (the vestibule of the vulva). Your vagina receives the penis and semen during sexual intercourse and also provides a passageway for menstrual blood flow to leave the body.
The female reproductive system also plays an important part in pregnancy and birth.
Figure 1. Uterus anatomy (normal female reproductive system anatomy)
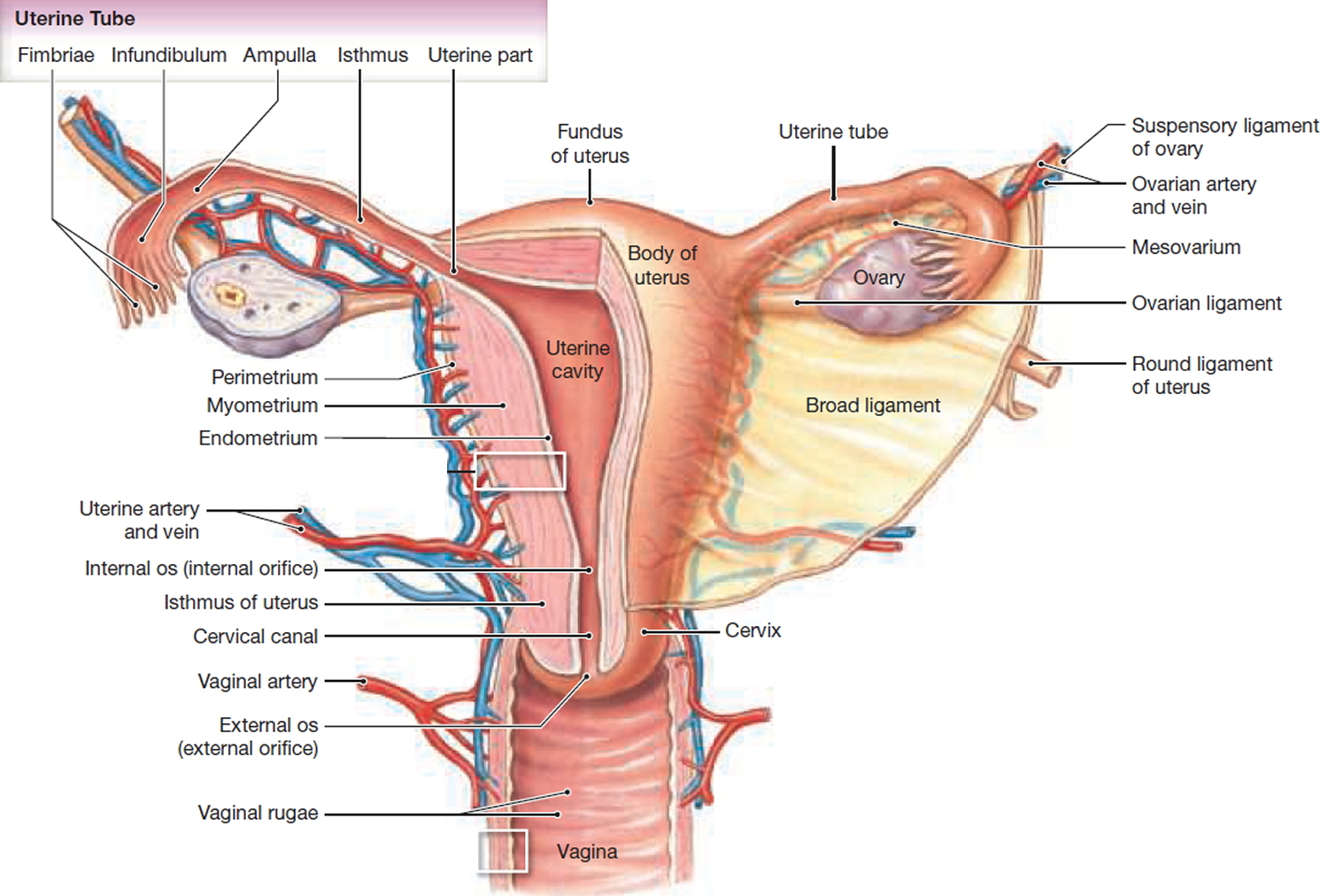
Figure 2. Female reproductive system
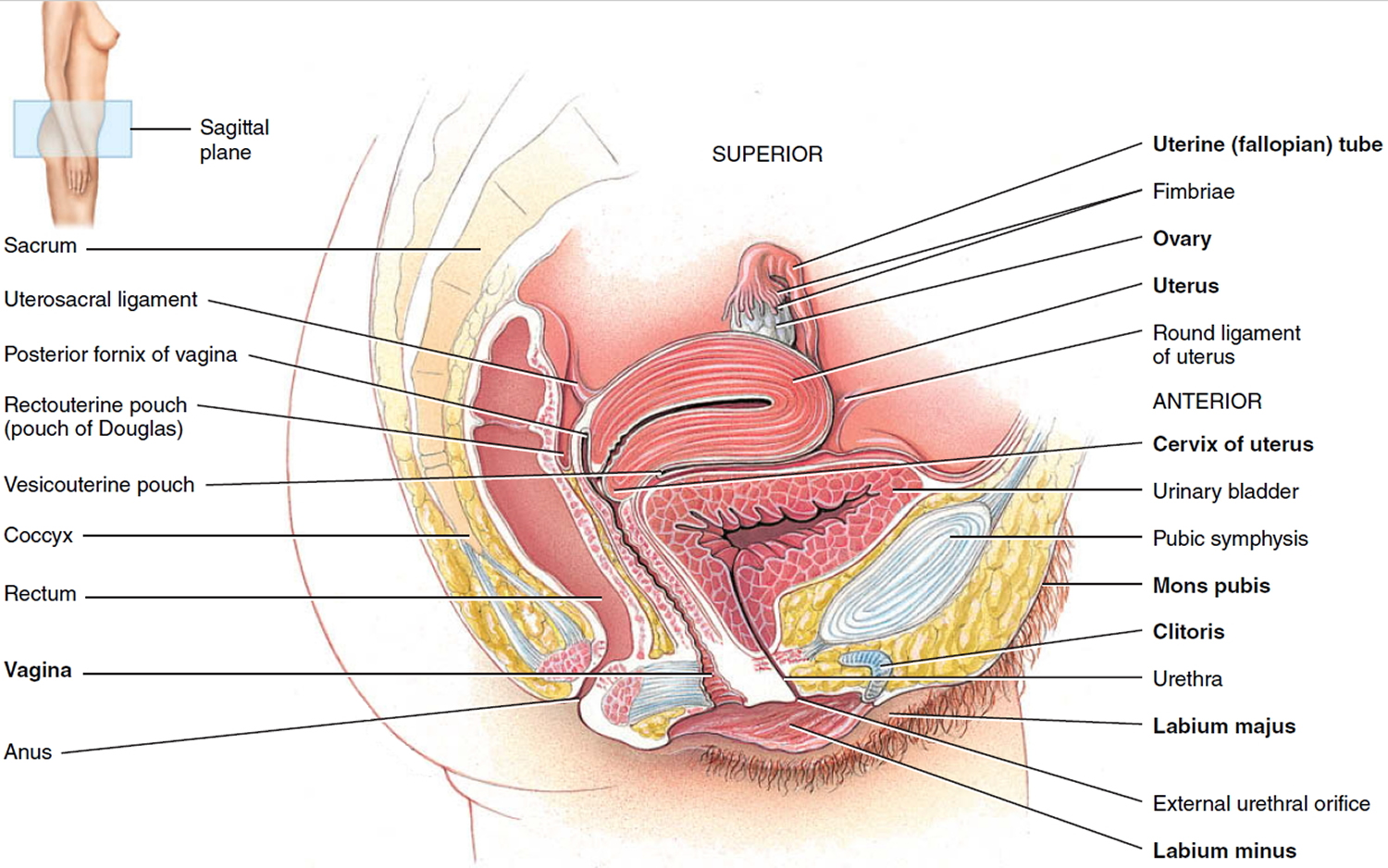
Figure 3. Endometrium of the uterus and its blood supply
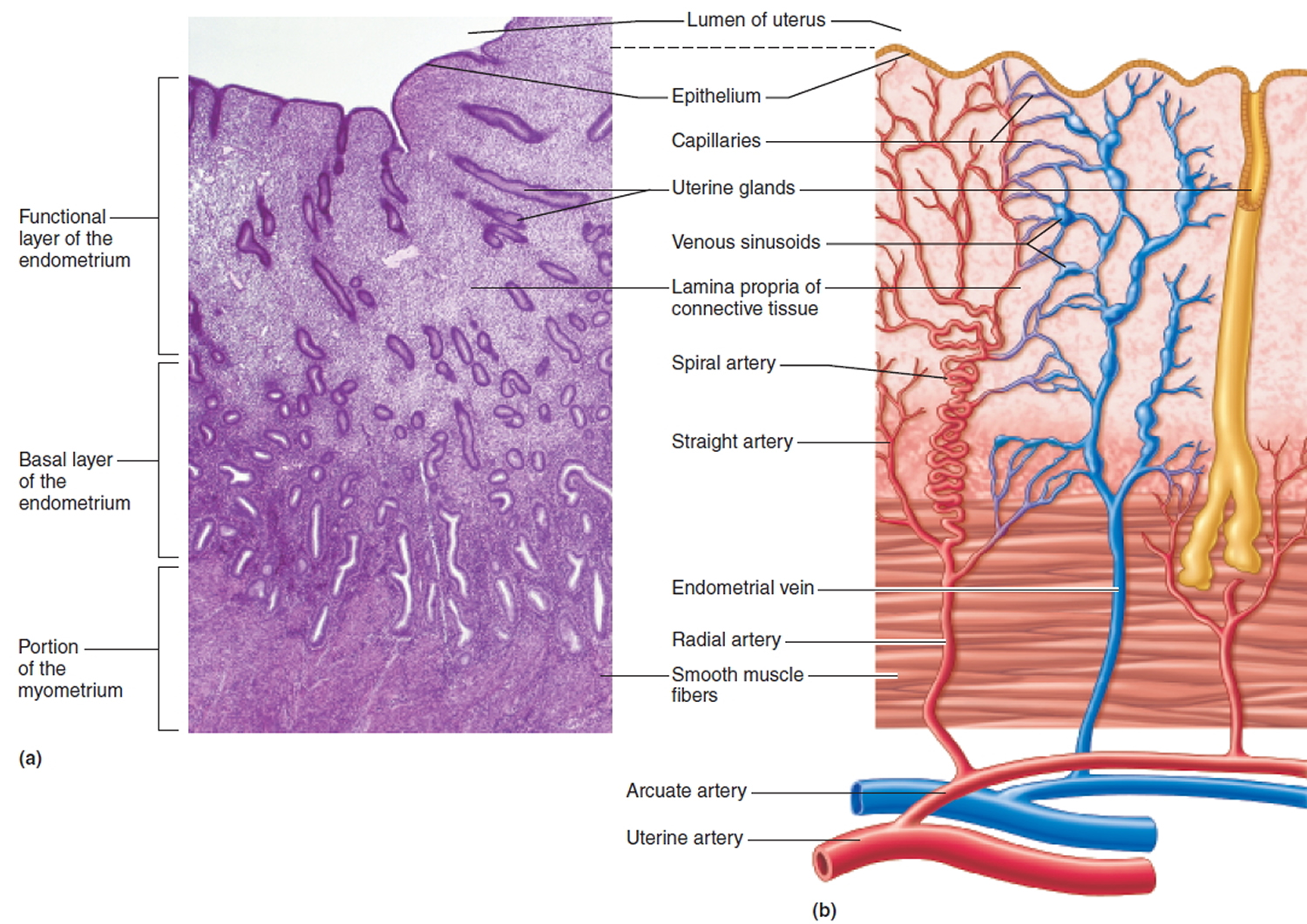
Figure 4. Endometriosis
Endometriosis complications
The main complication of endometriosis is trouble getting pregnant or infertility and chronic pain. Approximately one-third to one-half of women with endometriosis have difficulty getting pregnant. Furthermore, is a chronic condition with a large impact on the woman’s quality of life causing a decrease in the quality of life of patients, complications of surgical procedures, anatomical abnormalities due to possible adhesions, bowel or/and bladder dysfunction, and in the case of ovarian endometriomas could even lead to the development of ovarian, breast and thyroid cancers 28. Additionally, women with endometriosis have higher stress levels, report worse quality of sleep, and lower physical activity compared to healthy women 29. Bowel dysfunction like constipation or other digestive problems can appear in females who have endometriosis as a result of the inflammatory process of irritation of the gastrointestinal system rather than due to the involvement of endometriotic nodules affecting the rectum since patients undergoing surgical treatment for rectal endometriosis might continue experiencing those symptoms 30. Although primarily endometriosis was considered a benign condition, later research findings showed a higher risk for ovarian cancer in patients with endometriosis 31.
Infertility
The main complication of endometriosis is impaired fertility. Approximately one-third to one-half of women with endometriosis have difficulty getting pregnant.
For pregnancy to occur, an egg must be released from an ovary, travel through the neighboring fallopian tube, become fertilized by a sperm cell and attach itself to the uterine wall to begin development. Endometriosis may block the fallopian tube and keep the egg and sperm from uniting. But endometriosis also seems to affect fertility in less-direct ways, such as damage to the sperm or egg.
Even so, many women with mild to moderate endometriosis can still conceive and carry a pregnancy to term. Doctors sometimes advise women with endometriosis not to delay having children because the condition may become worse with time.
What is the link between infertility and endometriosis?
This is one of the most perplexing aspects of endometriosis, confronting researchers and patients alike. Almost 40% of women with infertility have endometriosis. Not only do some of these women have difficulty conceiving and carrying a live birth to term, they are less likely to conceive following assisted reproduction, such as fertility medication, artificial insemination, and in vitro fertilization. Studies to address the link between endometriosis and infertility have just begun. These studies suggest that women with endometriosis may have implantation defects (abnormalities of the environment that make it difficult for the embryo to attach and survive) and/or low quality eggs. These conditions, in turn, could be related to an abnormal immune environment that some suspect exist in women with endometriosis. Furthermore, inflammation from endometriosis may damage the sperm or egg or interfere with their movement through the fallopian tubes and uterus. In severe cases of endometriosis, the fallopian tubes may be blocked by adhesions or scar tissue.
Ovarian cancer
Ovarian cancer does occur at higher than expected rates in women with endometriosis 25. But the overall lifetime risk of ovarian cancer is low to begin with. Some studies suggest that endometriosis increases that risk, but it’s still relatively low. Although rare, another type of cancer — endometriosis-associated adenocarcinoma — can develop later in life in women who have had endometriosis.
Chronic pelvic pain
Chronic pelvic pain is closely associated with endometriosis since endometriosis has been the cause in 71% to 87% of women suffering from chronic pelvic pain 32. Chronic pelvic pain can negatively affect the health-related quality of life and hinder social, emotional, and sexual well-being as well as other domains like daily routines, family planning, or productivity of patients in the work environment 29.
Endometriosis symptoms
The most common symptom of endometriosis is chronic (long-term) pelvic pain, especially just before and during the menstrual period. Although many women experience cramping during their menstrual period, women with endometriosis typically describe menstrual pain that’s far worse than usual. They also tend to report that the pain increases over time.
Pelvic pain also may occur during sex. If endometriosis is present on the bowel, pain during bowel movements can occur. If it affects the bladder, pain may be felt during urination. Heavy menstrual bleeding is another symptom of endometriosis. Many women with endometriosis have no symptoms at all. Having trouble getting pregnant may be the first sign.
Common signs and symptoms of endometriosis may include:
- Painful periods (dysmenorrhea). Pelvic pain and cramping may begin before your period and extend several days into your period. You may also have lower back and abdominal pain.
- Pain with intercourse. Pain during or after sex is common with endometriosis.
- Pain with bowel movements or urination. You’re most likely to experience these symptoms during your menstrual period.
- Excessive bleeding. You may experience occasional heavy periods (menorrhagia) or bleeding between periods (menometrorrhagia).
- Infertility or not being able to get pregnant. Endometriosis is first diagnosed in some women who are seeking treatment for infertility.
- Other symptoms. You may also experience fatigue, diarrhea, constipation, bloating or nausea, especially before or during your menstrual periods.
The severity of your pain isn’t necessarily a reliable indicator of the number or extent of endometriosis growths in your body. Some women with mild endometriosis have intense pain, while others with lots of endometriosis tissue may have little pain or even no pain at all. Still, some women with endometriosis have no symptoms. Often, they find out they have endometriosis when they can’t get pregnant or after they get surgery for another reason.
Endometriosis is sometimes mistaken for other conditions that can cause pelvic pain, such as pelvic inflammatory disease (PID) or ovarian cysts. It may be confused with irritable bowel syndrome (IBS), a condition that causes bouts of diarrhea, constipation and abdominal cramping. Irritable bowel syndrome (IBS) can happen along with endometriosis, which can complicate the diagnosis.
Endometriosis pain
Pelvic pain is the most common symptom of endometriosis. Women with endometriosis may have many different kinds of pain:
- Very painful menstrual cramps. The pain may get worse over time.
- Chronic (long-term) pain in the lower back and pelvis
- Pain during or after sex. This is usually described as a “deep” pain and is different from pain felt at the entrance to the vagina when penetration begins.
- Intestinal pain
- Painful bowel movements or pain when urinating during menstrual periods. In rare cases, you may also find blood in your stool or urine.
Endometriosis implants respond to changes in estrogen, a female hormone. The implants may grow and bleed like the uterine lining does during the menstrual cycle. Surrounding tissue can become irritated, inflamed, and swollen. The breakdown and bleeding of this tissue each month also can cause scar tissue, called adhesions, to form. Sometimes adhesions can cause organs to stick together. The bleeding, inflammation, and scarring can cause pain, especially before and during menstruation.
When to see a doctor
See your doctor if you have signs and symptoms that may indicate endometriosis.
Endometriosis can be a challenging condition to manage. An early diagnosis, a multidisciplinary medical team and an understanding of your diagnosis may result in better management of your symptoms.
Endometriosis causes
Although the exact cause of endometriosis is not certain, possible explanations include:
- Retrograde menstruation. In retrograde menstruation, menstrual blood containing endometrial cells flows back through the fallopian tubes and into the pelvic cavity instead of out of your body. These displaced endometrial cells stick to the pelvic walls and surfaces of pelvic organs, where they grow and continue to thicken and bleed over the course of each menstrual cycle.
- Transformation of peritoneal cells. In what’s known as the “induction theory”, experts propose that hormones or immune factors promote transformation of peritoneal cells — cells that line the inner side of your abdomen — into endometrial cells.
- Embryonic cell transformation. Hormones such as estrogen may transform embryonic cells — cells in the earliest stages of development — into endometrial-like cell implants during puberty.
- Surgical scar implantation. After a surgery, such as a hysterectomy or C-section, endometrial cells may attach to a surgical incision.
- Endometrial cells transport. The blood vessels or tissue fluid (lymphatic) system may transport endometrial cells to other parts of your body.
- Immune system disorder. It’s possible that a problem with your immune system may make the body unable to recognize and destroy endometrial tissue that’s growing outside your uterus.
The retrograde menstruation, based on the implantation of endometrial cells reaching the pelvis via transtubal retrograde flow during menstruation, is supported by the largest body of evidence 33, 34, 35, 36, 7, 37, 38, 39.
Risk factors for developing endometriosis
Several factors place you at greater risk of developing endometriosis, such as:
- Never giving birth
- Mother, sister, or daughter had endometriosis (raises the risk about six times)
- Starting your period at an early age (before age 11)
- Going through menopause at an older age
- Short menstrual cycles — for instance, less than 27 days
- Heavy menstrual periods that last longer than seven days.
- Having higher levels of estrogen in your body or a greater lifetime exposure to estrogen your body produces
- Low body mass index
- Alcohol consumption
- One or more relatives (mother, aunt or sister) with endometriosis 40, 41
- Any medical condition that prevents the blood from flowing out of your body during menstrual periods
- Uterine abnormalities
Endometriosis usually develops several years after the onset of menstruation (menarche). Signs and symptoms of endometriosis end temporarily with pregnancy and end permanently with menopause, unless you’re taking estrogen therapy.
Endometriosis diagnosis
To diagnose endometriosis and other conditions that can cause pelvic pain, your doctor will ask you to describe your symptoms, including the location of your pain and when it occurs.
Tests to check for clues of endometriosis include:
- Pelvic exam. During a pelvic exam, your doctor manually feels (palpates) areas in your pelvis for abnormalities, such as cysts on your reproductive organs or scars behind your uterus. Often it’s not possible to feel small areas of endometriosis, unless they’ve caused a cyst to form.
- Ultrasound. This test uses high-frequency sound waves to create images of the inside of your body. To capture the images, a device called a transducer is either pressed against your abdomen or inserted into your vagina called transvaginal ultrasound. Both types of ultrasound may be done to get the best view of your reproductive organs. Ultrasound imaging won’t definitively tell your doctor whether you have endometriosis, but it can identify cysts associated with endometriosis (endometriomas).
- Magnetic resonance imaging (MRI). This exam uses a magnetic field and radio waves to make images of the organs and tissues within the body. For some, an MRI helps with surgical planning. It gives your surgeon detailed information about the location and size of endometriosis growths.
- Laparoscopy. Medical management is usually tried first. But to be certain you have endometriosis, your doctor may refer you to a surgeon to look inside your abdomen for signs of endometriosis using a surgical procedure called laparoscopy. A laparoscopy can provide information about the location, extent and size of the endometriosis growths to help determine the best treatment options. While you’re under general anesthesia, your surgeon makes a tiny incision near your navel (belly button) and inserts a slender viewing instrument called a laparoscope, looking for endometrial tissue outside your uterus. Your surgeon may take a tissue sample called biopsy for more testing. With proper planning, a surgeon can often treat endometriosis during the laparoscopy so that you need only one surgery.
Endometriosis treatment
Treatment for endometriosis is usually with medications or surgery. The approach you and your doctor choose will depend on the severity of your signs and symptoms and whether you hope to become pregnant.
Generally, doctors recommend trying conservative treatment approaches first, opting for surgery as a last resort.
Finding a doctor with whom you feel comfortable is crucial in managing and treating endometriosis. You may also want to get a second opinion before starting any treatment to be sure you know all of your options and the possible outcomes.
Pain medications
Your doctor may recommend that you take an over-the-counter pain reliever, such as the nonsteroidal anti-inflammatory drugs (NSAIDs) ibuprofen (Advil, Motrin IB, others) or naproxen (Aleve, others), to help ease painful menstrual cramps.
If you find that taking the maximum dose of these medications doesn’t provide full relief, you may need to try another approach to manage your signs and symptoms.
Home remedies for endometriosis
If your pain persists or if finding a treatment that works takes some time, you can try measures at home to relieve your discomfort.
- Apply a hot water bottle or heating pad to your lower stomach. This can get blood flowing and relax your muscles. Warm baths also may help relieve pain.
- Lie down and rest. Place a pillow under your knees when lying on your back. If you prefer to lie on your side, pull your knees up toward your chest. These positions help take the pressure off your back.
- Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Advil, Motrin IB, others) or naproxen (Aleve, others), can help ease painful menstrual cramps. If the pain is worse during your periods, try starting these medicines 1 to 2 days before your period begins.
- Regular exercise may help improve symptoms. Exercise helps improve blood flow. It also triggers your body’s natural painkillers, called endorphins.
- Eat a balanced, healthy diet. Maintaining a healthy weight will help improve your overall health. Eating plenty of fiber can help keep you regular so you don’t have to strain during bowel movements.
Techniques that also offer ways to relax and may help relieve pain include:
- Muscle relaxation
- Deep breathing
- Visualization
- Biofeedback
- Yoga
Some women find that acupuncture helps ease painful periods. Some studies show it also helps with chronic pain.
Hormone therapy
Sometimes, hormone medicine help ease or get rid of your endometriosis pain. The rise and fall of hormones during your menstrual cycle causes endometriosis tissue to thicken, break down and bleed. Hormone medication may slow the growth of this tissue and prevent new endometrial tissue from forming.
However, hormone therapy isn’t a permanent fix for endometriosis. You could experience a return of your symptoms after stopping treatment.
Hormone medications used to treat endometriosis include:
- Hormonal contraceptives. Birth control pills, patches and vaginal rings help control the hormones responsible for the buildup of endometrial tissue each month. Most women have lighter and shorter menstrual flow when they’re using a hormonal contraceptive. Using hormonal contraceptives — especially continuous cycle regimens — may reduce or eliminate the pain of mild to moderate endometriosis. The chances of relief seem to go up if you use birth control pills for a year or more with no breaks.
- Gonadotropin-releasing hormone (Gn-RH) agonists and antagonists. These drugs block the production of ovarian-stimulating hormones, lowering estrogen levels and preventing menstruation. This causes endometrial tissue to shrink. Because these drugs create an artificial menopause, taking a low dose of estrogen or progestin along with Gn-RH agonists and antagonists may decrease menopausal side effects, such as hot flashes, vaginal dryness and bone loss. Your menstrual periods and the ability to get pregnant return when you stop taking the medication.
- Progestin therapy. A progestin-only contraceptive (lab-made version of the progesterone hormone), such as an intrauterine device (Mirena, Skyla, others), a contraceptive rod placed under the skin of the arm (Nexplanon) or contraceptive injection (Depo-Provera) or a progestin-only birth control pill (Camila, Slynd), can stop menstrual periods and the growth of endometrial implants, which may relieve endometriosis signs and symptoms.
- Danazol. This drug suppresses the growth of the endometrium by blocking the production of ovarian-stimulating hormones, preventing menstruation and the symptoms of endometriosis. However, danazol may not be the first choice because it can cause serious side effects and can be harmful to the baby if you become pregnant while taking this medication.
- Aromatase inhibitors. Aromatase inhibitors are a class of medicines that lower the amount of estrogen in your body. Your doctor may recommend an aromatase inhibitor along with a progestin or combination birth control pills to treat your endometriosis.
- Researchers are exploring the use of other hormones for treating endometriosis and the pain related to it. One example is gestrinone, which has been used in Europe but is not available in the United States.
If you are TRYING to get pregnant, your doctor may prescribe a gonadotropin-releasing hormone (GnRH) agonist. This medicine stops your body from making the hormones responsible for ovulation, the menstrual cycle, and the growth of endometriosis. This treatment causes a temporary menopause, but it also helps control the growth of endometriosis. Once you stop taking the medicine, your menstrual cycle returns, but you may have a better chance of getting pregnant.
If you are NOT trying to get pregnant, hormonal birth control is generally the first step in treatment. This may include 9:
- Extended-cycle (you have only a few periods a year) or continuous cycle (you have no periods) birth control. These types of hormonal birth control are available in the pill or the shot and help stop bleeding and reduce or eliminate pain.
- Intrauterine device (IUD) to help reduce pain and bleeding. The hormonal IUD protects against pregnancy for up to 7 years. But the hormonal IUD may not help your pain and bleeding due to endometriosis for that long.
Oral contraceptives or birth control pills
These help make your period lighter, more regular, and shorter. Women prescribed contraceptives also report relief from pain 42.
- In general, the therapy contains two hormones-estrogen and progestin (a man-made progesterone-like hormone). Women who can’t take estrogen because of cardiovascular disease or a high risk of blood clots can use progestin-only pills to reduce menstrual flow.
- Typically, a woman takes the pill for 21 days and then takes sugar pills for 7 days to mimic the natural menstrual cycle. Some women take birth control pills continuously, without using the sugar pills that signal the body to go through menstruation. Taken without the sugar pills, birth control pills may stop the menstrual period altogether, which can reduce or eliminate the pain. There are also birth control pills available that provide only a couple days of sugar pills every 3 months; these also help reduce or eliminate pain.
- Pain relief usually lasts only while taking the pills, while the endometriosis is suppressed. When treatment stops, the symptoms of endometriosis may return (along with the ability to get pregnant). Many women continue treatment indefinitely. Occasionally, some women have no pain for several years after stopping treatment.
- There are some mild side effects from these hormones, such as weight gain, bloating, and bleeding between periods (especially when women first start to take the pills continuously).
Progesterone and progestin
Progesterone and progestin, taken as a pill, by injection, or through an intrauterine device (IUD), improve symptoms by reducing a woman’s period or stopping it completely. This also prevents pregnancy.
- As a pill taken daily, these hormones reduce menstrual flow without causing the uterus lining to grow. As soon as a woman stops taking the progestin pill, symptoms may return and pregnancy is possible.
- An IUD containing progestin, such as Mirena®, may be effective in reducing endometriosis-associated pain. It reduces the size of lesions and reduces menstrual flow (one third of women no longer get their period after a year of use) 43.
- As an Depo-Provera injection taken every 3 months, these hormones usually stop menstrual flow. However, one-third of women bleed several times in the first year of injection use. During these times of bleeding, pain may occur. Additionally, it may take a few months for a period to return after stopping the injections. When menstruation starts again, the ability to get pregnant returns.
- Women taking these hormones may gain weight, feel depressed, or have irregular vaginal bleeding.
Gonadotropin-releasing hormone (GnRH) agonists
Gonadotropin-releasing hormone (GnRH) agonists stop the production of certain hormones to prevent ovulation, menstruation, and the growth of endometriosis. This treatment sends the body into a “menopausal” state.
- GnRH agonists come in a nose spray taken daily, as an injection given once a month, or as an injection given every 3 months.
- The low-dose elagolix (Orilissa) pill should not be taken for more than 24 months and the high‑dose pill should not be taken for more than 6 months because it may cause bone loss 44
- Most health care providers recommend staying on GnRH agonists for only about 6 months at a time, with several months between treatments if they are repeated. The risk for heart complications and bone loss can rise when taking them longer 18. After stopping the GnRH agonist, the body comes out of the menopausal state, menstruation begins, and pregnancy is possible 45.
- As with all hormonal treatments, endometriosis symptoms return after women stop taking GnRH agonists.
- These medications also have side effects, including hot flashes, tiredness, problems sleeping, headache, depression, joint and muscle stiffness, bone loss, and vaginal dryness 44.
Danazol
Danazol also called Danocrine treatment stops the release of hormones that are involved in the menstrual cycle. While taking this drug, women will have a period only now and then or sometimes not at all.
- Common side effects include oily skin, pimples or acne, weight gain, muscle cramps, tiredness, smaller breasts, and sore breasts. Headaches, dizziness, weakness, hot flashes, or a deepening of the voice may also occur while on this treatment. Danazol’s side effects are more severe than those from other hormone treatment options 46.
- Danazol can harm a developing fetus. Therefore, it is important to prevent pregnancy while on this medication. Hormonal birth control methods are not recommended while on danazol. Instead, health care providers recommend using barrier methods of birth control, such as condoms or a diaphragm.
Conservative surgery
Conservative surgery is usually chosen for severe symptoms, when hormones are not providing relief or if you are having fertility problems. If you have endometriosis and are trying to become pregnant, surgery to remove as much endometriosis as possible while preserving your uterus and ovaries (conservative surgery) may increase your chances of success. If you have severe pain from endometriosis, you may also benefit from surgery. After surgery, most women have relief from pain. However, about 40 to 80% of women have pain again within 2 years after surgery. The more severe the disease, the more likely it is to return. Taking birth control pills or other medications after having surgery may help extend the pain-free period.
In some cases, hormone therapy is used before or after surgery to reduce pain and/or continue treatment. Current evidence supports the use of an intrauterine device (IUD) containing progestin after surgery to reduce pain. Currently, the only such device approved by the FDA is Mirena®.
Your doctor may do this procedure laparoscopically or through traditional abdominal surgery in more extensive cases. In laparoscopic surgery, your surgeon inserts a slender viewing instrument (laparoscope) through a small incision near your navel and inserts instruments to remove endometrial tissue through another small incision.
After surgery, your doctor may recommend taking hormone medicine to help improve pain.
Laparoscopy
The surgeon uses an instrument to inflate the abdomen slightly with a harmless gas and then inserts a small viewing instrument with a light, called a laparoscope, into the abdomen through a small cut to see the growths.
To remove the endometriosis, the surgeon makes at least two more small cuts in the abdomen and inserts lasers or other surgical instruments to:
- Remove the lesions, which is a process called excising.
- Destroy the lesions with intense heat and seal the blood vessels without stitches, a process called cauterizing or vaporizing.
- Some surgeons also will remove scar tissue at this time because it may be contributing to endometriosis-associated pain.
- The goal is to treat the endometriosis without harming the healthy tissue around it.
- Although most women have relief from pain with surgery in the short term, pain often returns 46. The excision of deep lesions seems to be associated with long-term pain relief.
- Some evidence shows that surgical treatment for endometriosis-related pain is actually more effective in women who have moderate endometriosis rather than minimal endometriosis. The reason is that women with minimal endometriosis may have changes in their pain perception that persist after the lesions are removed 43, 47.
Laparotomy
In this major abdominal surgery procedure, the surgeon may remove the endometriosis patches. Sometimes, the endometriosis lesions are too small to see in a laparotomy.
- During this procedure, the surgeon may also remove the uterus. Removing the uterus is called hysterectomy.
- If the ovaries have endometriosis on them or if damage is severe, the surgeon may remove the ovaries and fallopian tubes along with the uterus. This process is called total hysterectomy and bilateral (meaning “on both sides”) salpingo-oophorectomy.
- When possible, health care providers will try to leave the ovaries in place because of the important role ovaries play in overall health.
- Doctors recommend major surgery as a last resort for endometriosis treatment.
- Having a hysterectomy or salpingo-oophorectomy does not guarantee that the lesions will not return or that the pain will go away. Endometriosis symptoms and lesions may come back in as many as 15% of women who have a total hysterectomy with bilateral salpingo-oophorectomy 18.
Hysterectomy
In severe cases of endometriosis, surgery to remove the uterus and cervix (total hysterectomy) as well as both ovaries (oophorectomy) may be the best treatment but causes early menopause. Early menopause also carries a risk of heart and blood vessel diseases, certain metabolic conditions and early death. You can’t get pregnant after a hysterectomy. The lack of hormones made by the ovaries may improve endometriosis pain for some. But for others, endometriosis that remains after surgery continues to cause symptoms.
A hysterectomy alone is not effective — the estrogen your ovaries produce can stimulate any remaining endometriosis and cause pain to persist. There is a small chance that pain will come back even if your uterus and ovaries are removed. This may be due to endometriosis that was not visible or could not be removed at the time of surgery.
Taking out your uterus and ovaries was once thought to be the most effective treatment for endometriosis. Today, some experts consider it to be a last resort to ease pain when other treatments haven’t worked. Other experts instead recommend surgery that focuses on the careful and thorough removal of all endometriosis tissue.
Surgery to sever pelvic nerves
If the pain is located in the center of the abdomen, health care providers may recommend cutting nerves in the pelvis to lessen the pain. This can be done during either laparoscopy or laparotomy 18. The American College of Obstetricians and Gynecologists (ACOG) reports several clinical trials that showed these procedures to be ineffective at relieving pain from endometriosis. These procedures are not currently included in the American College of Obstetricians and Gynecologists (ACOG) recommendations for management of endometriosis 18, 42, 43.
Two procedures are used to sever different nerves in the pelvis.
- Presacral neurectomy. This procedure severs the nerves connected to the uterus. Research shows that this procedure can be useful in relieving pain along the center of the abdomen 43.
- Laparoscopic uterine nerve ablation (LUNA). This procedure involves severing nerves in the ligaments that secure the uterus. However, studies have shown that LUNA did not relieve pain any better than laparoscopy alone. For this reason, it is generally not recommended for treatment of endometriosis-associated pain 18, 42.
Treatments for Infertility Related to Endometriosis
Endometriosis can lead to trouble getting pregnant. In most cases, doctor will recommend laparoscopy to remove or vaporize the growths as a way to also improve fertility in women who have mild or minimal endometriosis 43. Although studies show improved pregnancy rates following this type of surgery, the success rate is not clear.
If pregnancy does not occur after laparoscopic treatment, in vitro fertilization (IVF) may be the best option to improve fertility. Taking any other hormonal therapy usually used for endometriosis-associated pain will only suppress ovulation and delay pregnancy. Performing another laparoscopy is not the preferred approach to improving fertility unless symptoms of pain prevent undergoing IVF. Multiple surgeries, especially those that remove cysts from the ovaries, may reduce ovarian function and hamper the success of IVF 43.
IVF makes it possible to combine sperm and eggs in a laboratory to make an embryo. Then the resulting embryos are placed into the woman’s uterus. IVF is one type of assisted reproductive technology (ART) that may be an option for women and families affected by infertility related to endometriosis.
In general, the process of IVF involves the following steps. First, a woman takes hormones to cause “superovulation”, which triggers her body to produce many eggs at one time. Once mature, the eggs are collected from the woman, using a probe inserted into the vagina and guided by ultrasound. The collected eggs are placed in a dish for fertilization with a man’s sperm. The fertilized cells are then placed in an incubator, a machine that keeps them warm and allows them to develop into embryos. After 3 to 5 days, the embryos are transferred to the woman’s uterus. It takes about 2 weeks to know if the process is successful.
Even though the use of hormones in IVF is successful in treating infertility related to endometriosis, other forms of hormone therapy are not as successful. For instance, the American College of Obstetricians and Gynecologists does not recommend using oral contraceptive pills or GnRH agonists to treat endometriosis-related infertility. The use of these hormonal agents prevents ovulation and delays pregnancy 18, 6.
In addition, the hormones used during IVF do not cure the endometriosis lesions, which means that pain may recur after pregnancy and that not all women with endometriosis are able to become pregnant with IVF. Researchers are still looking for hormone treatments for infertility due to endometriosis.
Alternative medicine
Alternative medicine involves treatments that aren’t part of standard medical care. Some people with endometriosis say they get pain relief from alternative therapies such as:
- Acupuncture, in which a trained practitioner places fine needles into your skin. Acupuncture has shown some promise at easing endometriosis pain.
- Chiropractic care, in which a licensed professional adjusts the spine or other body parts.
- Herbs such as cinnamon trig or licorice root.
- Supplements including vitamin B1 (thiamine), magnesium or omega-3 fatty acids.
Overall, there’s little research on much relief women with endometriosis might get from alternative medicine. Always check with your doctor before you try a new alternative therapy to find out if it’s safe for you. For example, supplements and herbs can affect standard treatments such as medicines. If you’re interested in trying acupuncture or chiropractic care, ask your doctor to recommend reputable professionals.
Endometriosis diet
Women with endometriosis are frequently misdiagnosed with irritable bowel syndrome (IBS) for some time before a correct diagnosis is made. A study 48 found women with concurrent endometriosis and IBS report a unique symptom phenotype. The low FODMAP diet appears effective in women with gut symptoms and endometriosis.
For more information of FODMAP diet go here: Fodmap diet
The literature on dietary factors and the risk of developing endometriosis is limited. The few studies conducted in this area are contradictory.
The current scientific evidence suggests that the diet and lifestyle may influence the presence of inflammation in the body, estrogen activity, menstrual cycle, and prostaglandin metabolism. As such, diet and lifestyle can also impact the risk of developing endometriosis 49, 50.
One of the possible pathogenic factors affecting both endometriosis and dysmenorrhea is prostaglandin levels. Omega-6 fatty acids derived from the diet are the precursors of the proinflammatory prostaglandins PGE2 and PGF2α that probably increase uterine cramps and cause the painful symptoms. However, PGE3 and PGE3α derived from the Omega-3 fatty acids were linked to reduced inflammation and thus, lesser pain 51.
High levels of estrogen may be another risk factor for developing endometriosis. Research has demonstrated a connection between diet and the incidence of the estrogen-dependent diseases (e.g. breast and endometrial cancer). We can therefore assume that dietary impact blood estrogen levels may also play a role in the etiology of endometriosis 52, 53.
Food may also contain chemical compounds from contaminated environments, especially chlorinated hydrocarbons including polychlorinated biphenyls (PCBs). Such compounds tend to bioaccumulate in lipids contained particularly in meat, liver, and dairy products. Similarly, pesticides can be consumed together with contaminated fruits and vegetables. The above compounds can also be counted among the risk factors for endometriosis 54, 55.
On the basis of the data presented in this study 56, it can be suggested that the increased consumption of vegetables, fruits 57, Omega-3 fatty acids 50, 58, Omega-6 fatty acids 58, fats 59, soy and phytoestrogens 60 as well as dairy products rich in calcium and vitamin D 61 decreases the risk of developing endometriosis. Conversely, factors identified to increase the risk for endometriosis include fruits 62, dietary fiber 63, fats in general 64 [including vegetable fats, monounsaturated fats, polyunsaturated fats 64, and trans-unsaturated fatty acids 50], pork and beef 57, ham 57, and alcohol 61.
It appears that in developing endometriosis antioxidants, vitamins A, C, and E, and B-group vitamins as well as folic acid also play an important role. Consumption of these vitamins and antioxidants decreases the risk of developing endometriosis, potentially by influencing oxidative stress and steroid hormone metabolism in the body. From 1991 to 2005 a cohort study was conducted on a group of 70,617 women by Darling et al. 65. The experimental group (n = 1.383) consisted of women with the endometriosis confirmed by laparoscopy and the control group (n = 69.234) consisted of the healthy women. On the basis of a questionnaire concerning consumption of products and usage of vitamin supplements, the relationship between vitamins C and E as well as B-group vitamins and endometriosis risk was examined. It has been found that consumption of products rich in vitamins such as folic acid, vitamin C, and vitamin E is inversely proportional to the risk of developing endometriosis. However, supplying these vitamins via dietary supplement had no influence on the occurrence of endometriosis 65. This may suggest that other factors present in food
may modify the risk of endometriosis 65. A similar study was conducted in 2008 by Mier-Cabrera et al. 66 on a group of women suffering from endometriosis (n = 83) compared to a control group of healthy women (n = 80). Disorders in blood serum were defined on the basis of a questionnaire assessing frequency of product consumption and serum testing to assess oxidant-antioxidant balance. The findings of the study showed lower consumption of vitamins A, C, and E, and microelements zinc and copper in the group of women with diagnosed endometriosis 66.
A high fat diet in which more than 45% of daily calorie requirements come from fat can also increase oxidative stress and inflammation in the body, thereby increasing the risk of developing endometriosis. This finding comes from a 2016 study by Heard et al. 67 conducted in mice in which the experimental group was on the diet of 45% of fat and the control group was on a diet of 17% of fat. Another study performed on animals in 2013 by Herington
et al. 68 seems to confirm the positive influence of fish oils on decreasing the risk of developing endometriosis, demonstrating that supplementation with fish oil reduced the development of postoperative adhesions connected with endometriosis.
CONCLUSIONS
Dietary factors that may decrease the risk of endometriosis include consumption of vegetables, antioxidant vitamins, B-group vitamins, dairy products rich in calcium and vitamin D, fish oils, and Omega-3 fatty acids.
The dietary factors that may potentially increase the risk of developing endometriosis include consumption of trans unsaturated fatty acids, red meat and ham, as well as alcohol.
Currently there are no clear connections between the diet and the risk of endometriosis. Further research is needed in order to explain the relationship between consumed foods and development of this disease.
Endometriosis prognosis
Women with endometriosis have fewer chances for childbearing and a higher risk for miscarriages and ectopic pregnancies than those without endometriosis 69. Additionally, endometriotic lesions can spontaneously regress in approximately one-third of affected women who are not receiving any treatment 70. According to different estimates, endometriosis recurrence rates after surgery vary between 6 and 67% 71. Potential risk factors predicting a possible recurrence have not been completely clarified, but the recurrent endometriotic lesions may arise from de novo cells or residual endometriotic tissue 71. Medical treatment can be proven effective, but in 5% to 59% of patients, the pain continues to exist at the end of the therapy 72. Even in cases of treatment cessation, pain recurrence has been reported in 17% to 34% of cases 72.
- Carpinello OJ, Sundheimer LW, Alford CE, et al. Endometriosis. [Updated 2017 Oct 22]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278996[↩]
- Tsamantioti ES, Mahdy H. Endometriosis. [Updated 2023 Jan 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK567777[↩]
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Overview: Endometriosis. [Updated 2021 Mar 24]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279501[↩]
- Becker CM, Bokor A, Heikinheimo O, Horne A, Jansen F, Kiesel L, King K, Kvaskoff M, Nap A, Petersen K, Saridogan E, Tomassetti C, van Hanegem N, Vulliemoz N, Vermeulen N; ESHRE Endometriosis Guideline Group. ESHRE guideline: endometriosis. Hum Reprod Open. 2022 Feb 26;2022(2):hoac009. doi: 10.1093/hropen/hoac009[↩]
- Giudice LC, Oskotsky TT, Falako S, Opoku-Anane J, Sirota M. Endometriosis in the era of precision medicine and impact on sexual and reproductive health across the lifespan and in diverse populations. FASEB J. 2023 Sep;37(9):e23130. doi: 10.1096/fj.202300907[↩]
- Brown J, Farquhar C. Endometriosis: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2014 Mar 10;2014(3):CD009590. doi: 10.1002/14651858.CD009590.pub2[↩][↩]
- Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020 Mar 26;382(13):1244-1256. doi: 10.1056/NEJMra1810764[↩][↩]
- Endometriosis. Medline Plus. https://medlineplus.gov/endometriosis.html[↩]
- Endometriosis. https://womenshealth.gov/a-z-topics/endometriosis[↩][↩]
- Buck, L.G.M., Hediger, M.L., Peterson, C.M., Croughan, M., Sundaram, R., Stanford, J., Chen, Z., et al. (2011). Incidence of endometriosis by study population and diagnostic method: the ENDO study. Fertility and Sterility; 96(2): 360-5. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143230[↩]
- Nnoaham KE, Hummelshoj L, Webster P, d’Hooghe T, de Cicco Nardone F, de Cicco Nardone C, Jenkinson C, Kennedy SH, Zondervan KT; World Endometriosis Research Foundation Global Study of Women’s Health consortium. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril. 2011 Aug;96(2):366-373.e8. doi: 10.1016/j.fertnstert.2011.05.090[↩]
- Buck Louis GM, Hediger ML, Peterson CM, Croughan M, Sundaram R, Stanford J, Chen Z, Fujimoto VY, Varner MW, Trumble A, Giudice LC; ENDO Study Working Group. Incidence of endometriosis by study population and diagnostic method: the ENDO study. Fertil Steril. 2011 Aug;96(2):360-5. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143230[↩]
- Ghiasi M, Kulkarni MT, Missmer SA. Is Endometriosis More Common and More Severe Than It Was 30 Years Ago? J Minim Invasive Gynecol. 2020 Feb;27(2):452-461. doi: 10.1016/j.jmig.2019.11.018[↩]
- Parazzini F, Roncella E, Cipriani S, Trojano G, Barbera V, Herranz B, Colli E.. The frequency of endometriosis in the general and selected populations: a systematic review. J Endometriosis Pelvic Pain Disorders 2020;12:176–189.[↩]
- Sarria-Santamera A, Orazumbekova B, Terzic M, Issanov A, Chaowen C, Asúnsolo-Del-Barco A. Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis. Healthcare (Basel). 2020 Dec 30;9(1):29. doi: 10.3390/healthcare9010029[↩]
- Janssen EB, Rijkers AC, Hoppenbrouwers K, Meuleman C, D’Hooghe TM. Prevalence of endometriosis diagnosed by laparoscopy in adolescents with dysmenorrhea or chronic pelvic pain: a systematic review. Hum Reprod Update. 2013 Sep-Oct;19(5):570-82. doi: 10.1093/humupd/dmt016[↩]
- Hirsch M, Dhillon-Smith R, Cutner AS, Yap M, Creighton SM. The Prevalence of Endometriosis in Adolescents with Pelvic Pain: A Systematic Review. J Pediatr Adolesc Gynecol. 2020 Dec;33(6):623-630. doi: 10.1016/j.jpag.2020.07.011[↩]
- Practice bulletin no. 114: management of endometriosis. Obstet Gynecol. 2010 Jul;116(1):223-236. doi: 10.1097/AOG.0b013e3181e8b073[↩][↩][↩][↩][↩][↩][↩]
- Emanuele MA, Wezeman F, Emanuele NV. Alcohol’s effects on female reproductive function. Alcohol Res Health. 2002;26(4):274-81. https://pmc.ncbi.nlm.nih.gov/articles/PMC6676690[↩]
- Schliep KC, Schisterman EF, Mumford SL, Pollack AZ, Zhang C, Ye A, Stanford JB, Hammoud AO, Porucznik CA, Wactawski-Wende J. Caffeinated beverage intake and reproductive hormones among premenopausal women in the BioCycle Study. Am J Clin Nutr. 2012 Feb;95(2):488-97. doi: 10.3945/ajcn.111.021287[↩]
- Macer ML, Taylor HS. Endometriosis and infertility: a review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet Gynecol Clin North Am. 2012 Dec;39(4):535-49. doi: 10.1016/j.ogc.2012.10.002[↩]
- Endometriosis. https://www.nichd.nih.gov/health/topics/endometriosis[↩][↩]
- Matalliotakis I, Cakmak H, Matalliotakis M, Kappou D, Arici A. High rate of allergies among women with endometriosis. J Obstet Gynaecol. 2012 Apr;32(3):291-3. doi: 10.3109/01443615.2011.644358[↩]
- Sinaii N, Cleary SD, Ballweg ML, Nieman LK, Stratton P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: a survey analysis. Hum Reprod. 2002 Oct;17(10):2715-24. doi: 10.1093/humrep/17.10.2715[↩][↩]
- Sayasneh A, Tsivos D, Crawford R. Endometriosis and ovarian cancer: a systematic review. ISRN Obstet Gynecol. 2011;2011:140310. doi: 10.5402/2011/140310[↩][↩]
- Munksgaard PS, Blaakaer J. The association between endometriosis and gynecological cancers and breast cancer: a review of epidemiological data. Gynecol Oncol. 2011 Oct;123(1):157-63. doi: 10.1016/j.ygyno.2011.06.017[↩]
- Giudice LC. Clinical practice. Endometriosis. N Engl J Med. 2010 Jun 24;362(25):2389-98. doi: 10.1056/NEJMcp1000274[↩]
- Kvaskoff M, Mahamat-Saleh Y, Farland LV, Shigesi N, Terry KL, Harris HR, Roman H, Becker CM, As-Sanie S, Zondervan KT, Horne AW, Missmer SA. Endometriosis and cancer: a systematic review and meta-analysis. Hum Reprod Update. 2021 Feb 19;27(2):393-420. doi: 10.1093/humupd/dmaa045[↩]
- Marinho MCP, Magalhaes TF, Fernandes LFC, Augusto KL, Brilhante AVM, Bezerra LRPS. Quality of Life in Women with Endometriosis: An Integrative Review. J Womens Health (Larchmt). 2018 Mar;27(3):399-408. doi: 10.1089/jwh.2017.6397[↩][↩]
- Roman H, Bridoux V, Tuech JJ, Marpeau L, da Costa C, Savoye G, Puscasiu L. Bowel dysfunction before and after surgery for endometriosis. Am J Obstet Gynecol. 2013 Dec;209(6):524-30. doi: 10.1016/j.ajog.2013.04.015[↩]
- Králíčková M, Laganà AS, Ghezzi F, Vetvicka V. Endometriosis and risk of ovarian cancer: what do we know? Arch Gynecol Obstet. 2020 Jan;301(1):1-10. doi: 10.1007/s00404-019-05358-8[↩]
- Bloski T, Pierson R. Endometriosis and Chronic Pelvic Pain: Unraveling the Mystery Behind this Complex Condition. Nurs Womens Health. 2008 Oct;12(5):382-95. doi: 10.1111/j.1751-486X.2008.00362.x[↩]
- Vercellini P, Aimi G, De Giorgi O, Maddalena S, Carinelli S, Crosignani PG. Is cystic ovarian endometriosis an asymmetric disease? Br J Obstet Gynaecol. 1998 Sep;105(9):1018-21. doi: 10.1111/j.1471-0528.1998.tb10267.x[↩]
- Vercellini P, Abbiati A, Viganò P, Somigliana ED, Daguati R, Meroni F, Crosignani PG. Asymmetry in distribution of diaphragmatic endometriotic lesions: evidence in favour of the menstrual reflux theory. Hum Reprod. 2007 Sep;22(9):2359-67. doi: 10.1093/humrep/dem224[↩]
- Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014 May;10(5):261-75. doi: 10.1038/nrendo.2013.255[↩]
- Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Viganò P. Endometriosis. Nat Rev Dis Primers. 2018 Jul 19;4(1):9. doi: 10.1038/s41572-018-0008-5[↩]
- Bulun SE, Yilmaz BD, Sison C, Miyazaki K, Bernardi L, Liu S, Kohlmeier A, Yin P, Milad M, Wei J. Endometriosis. Endocr Rev. 2019 Aug 1;40(4):1048-1079. doi: 10.1210/er.2018-00242[↩]
- Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021 Feb 27;397(10276):839-852. doi: 10.1016/S0140-6736(21)00389-5[↩]
- Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022 Nov 14;379:e070750. doi: 10.1136/bmj-2022-070750[↩]
- Saha R, Pettersson HJ, Svedberg P, Olovsson M, Bergqvist A, Marions L, Tornvall P, Kuja-Halkola R. Heritability of endometriosis. Fertil Steril. 2015 Oct;104(4):947-952. doi: 10.1016/j.fertnstert.2015.06.035[↩]
- Treloar SA, O’Connor DT, O’Connor VM, Martin NG. Genetic influences on endometriosis in an Australian twin sample. [email protected]. Fertil Steril. 1999 Apr;71(4):701-10. doi: 10.1016/s0015-0282(98)00540-8[↩]
- Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril. 2014 Apr;101(4):927-35. doi: 10.1016/j.fertnstert.2014.02.012. Epub 2014 Mar 13. Erratum in: Fertil Steril. 2015 Aug;104(2):498.[↩][↩][↩]
- Yeung PP Jr, Shwayder J, Pasic RP. Laparoscopic management of endometriosis: comprehensive review of best evidence. J Minim Invasive Gynecol. 2009 May-Jun;16(3):269-81. doi: 10.1016/j.jmig.2009.02.007[↩][↩][↩][↩][↩][↩]
- Drug Trials Snapshots: ORILISSA. https://www.fda.gov/drugs/drug-approvals-and-databases/drug-trials-snapshots-orilissa[↩][↩]
- Limonta, P., Marelli, M. M., Moretti, R., Marzagalli, M., Fontana, F., & Maggi, R. (2018). Chapter two – GnRH in the human female reproductive axis. In G. Litwack (Ed.), Vitamins and hormones Vol. 107, pp. 27–66. Cambridge, MA: Academic Press. https://doi.org/10.1016/bs.vh.2018.01.003[↩]
- American College of Obstetricians and Gynecologists. (2010). Management of endometriosis (Practice Bulletin No. 114). Obstetrics & Gynecology, 116(1), 223-236.[↩][↩]
- Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. 2011 May-Jun;17(3):327-46. doi: 10.1093/humupd/dmq050[↩]
- Endometriosis in patients with irritable bowel syndrome: Specific symptomatic and demographic profile, and response to the low FODMAP diet. Aust N Z J Obstet Gynaecol. 2017 Apr;57(2):201-205. doi: 10.1111/ajo.12594. Epub 2017 Mar 17. http://onlinelibrary.wiley.com/doi/10.1111/ajo.12594/full[↩]
- Darling AM, Chavarro JE, Malspeis S, et al. A prospective cohort study of Vitamins B, C, E, and multivitamin intake and endometriosis. J Endometr. 2013; 5(1): 17–26, doi: 10.5301/je.5000151 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2873173/[↩]
- Missmer SA, Chavarro JE, Malspeis S, et al. A prospective study of dietary fat consumption and endometriosis risk. Hum Reprod. 2010; 25(6): 1528–1535, doi: 10.1093/humrep/deq044 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2873173/[↩][↩][↩]
- Fjerbaek A, Knudsen UB. Endometriosis, dysmenorrhea and diet–what is the evidence? Eur J Obstet Gynecol Reprod Biol. 2007; 132(2): 140–147, doi: 10.1016/j.ejogrb.2006.12.006 https://www.ncbi.nlm.nih.gov/pubmed/17210218[↩]
- Tsubura A, Uehara N, Kiyozuka Y, et al. Dietary factors modifying breast cancer risk and relation to time of intake. J Mammary Gland Biol Neoplasia. 2005; 10(1): 87–100, doi: 10.1007/s10911-005-2543-4, https://www.ncbi.nlm.nih.gov/pubmed/15886889[↩]
- Littman AJ, Beresford SA, White E. The association of dietary fat and plant foods with endometrial cancer (United States). Cancer Causes Control. 2001; 12(8): 691–702, https://www.ncbi.nlm.nih.gov/pubmed/11562109[↩]
- La Rocca C, Mantovani A. From environment to food: the case of PCB. Ann Ist Super Sanita. 2006; 42(4): 410–416. http://www.iss.it/publ/anna/2006/4/424410.pdf[↩]
- Grassi P, Fattore E, Generoso C, et al. Polychlorobiphenyls (PCBs), polychlorinated dibenzo-p-dioxins (PCDDs) and dibenzofurans (PCDFs) in fruit and vegetables from an industrial area in northern Italy. Chemosphere. 2010; 79(3): 292–298, doi: 10.1016/j.chemosphere.2010.01.028 https://www.ncbi.nlm.nih.gov/pubmed/20153014[↩]
- Influence of diet on the risk of developing endometriosis. https://journals.viamedica.pl/ginekologia_polska/article/view/GP.a2017.0017/37603[↩]
- Parazzini F, Chiaffarino F, Surace M, et al. Selected food intake and risk of endometriosis. Hum Reprod. 2004; 19(8): 1755–1759, doi: 10.1093/humrep/deh395, https://www.ncbi.nlm.nih.gov/pubmed/15254009[↩][↩][↩]
- Khanaki K, Nouri M, Ardekani AM, et al. Evaluation of the relationship between endometriosis and omega-3 and omega-6 polyunsaturated fatty acids. Iran Biomed J. 2012; 16(1): 38–43. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3614254/[↩][↩]
- Sesti F, Capozzolo T, Pietropolli A, et al. Recurrence rate of endometrioma after laparoscopic cystectomy: a comparative randomized trial between post-operative hormonal suppression treatment or dietary therapy vs. placebo. Eur J Obstet Gynecol Reprod Biol. 2009; 147(1): 72–77, doi:10.1016/j.ejogrb.2009.07.003 https://www.ncbi.nlm.nih.gov/pubmed/19665279[↩]
- Tsuchiya M, Miura T, Hanaoka T, et al. Effect of soy isoflavones on endometriosis: interaction with estrogen receptor 2 gene polymorphism. Epidemiology. 2007; 18(3): 402–408. https://www.ncbi.nlm.nih.gov/pubmed/17474167[↩]
- Matalliotakis IM, Cakmak H, Fragouli YG, et al. Epidemiological characteristics in women with and without endometriosis in the Yale series. Arch Gynecol Obstet. 2008; 277(5): 389–393, doi: 10.1007/s00404-007-0479-1, https://www.ncbi.nlm.nih.gov/pubmed/17922285[↩][↩]
- Trabert B, Peters U, De Roos AJ, et al. Diet and risk of endometriosis in a population-based case-control study. Br J Nutr. 2011; 105(3): 459–467, doi: 10.1017/S0007114510003661 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374872/[↩]
- Savaris AL, do Amaral VF. Nutrient intake, anthropometric data and correlations with the systemic antioxidant capacity of women with pelvic endometriosis. Eur J Obstet Gynecol Reprod Biol. 2011; 158(2): 314–318,doi: 10.1016/j.ejogrb.2011.05.014 https://www.ncbi.nlm.nih.gov/pubmed/21700380[↩]
- Britton JA, Westhoff C, Howe GR, et al. Diet and benign ovarian tumors (United States). Cancer Causes Control. 2000; 11(5): 389–401, https://www.ncbi.nlm.nih.gov/pubmed/10877332[↩][↩]
- Darling AM, Chavarro JE, Malspeis S, et al. A prospective cohort study of Vitamins B, C, E, and multivitamin intake and endometriosis. J Endometr. 2013; 5(1): 17–26, doi: 10.5301/je.5000151 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3916184/[↩][↩][↩]
- Mier-Cabrera J, Aburto-Soto T, Burrola-Méndez S, et al. Women with endometriosis improved their peripheral antioxidant markers after the application of a high antioxidant diet. Reprod Biol Endocrinol. 2009; 7: 54, doi: 10.1186/1477-7827-7-54 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2693127/[↩][↩]
- Heard ME, Melnyk SB, Simmen FA, et al. High-Fat Diet Promotion of Endometriosis in an Immunocompetent Mouse Model is Associated With Altered Peripheral and Ectopic Lesion Redox and Inflammatory Status. Endocrinology. 2016; 157(7): 2870–2882, doi: 10.1210/en.2016-1092, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4929556/[↩]
- Herington JL, Glore DR, Lucas JA, et al. Dietary fish oil supplementation inhibits formation of endometriosis-associated adhesions in a chimeric mouse model. Fertil Steril. 2013; 99(2): 543–550, doi: 10.1016/j.fertnstert. 2012.10.007 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3582352/[↩]
- Hjordt Hansen MV, Dalsgaard T, Hartwell D, Skovlund CW, Lidegaard O. Reproductive prognosis in endometriosis. A national cohort study. Acta Obstet Gynecol Scand. 2014 May;93(5):483-9. doi: 10.1111/aogs.12373[↩]
- Harrison RF, Barry-Kinsella C. Efficacy of medroxyprogesterone treatment in infertile women with endometriosis: a prospective, randomized, placebo-controlled study. Fertil Steril. 2000 Jul;74(1):24-30. doi: 10.1016/s0015-0282(00)00577-x[↩]
- Selçuk I, Bozdağ G. Recurrence of endometriosis; risk factors, mechanisms and biomarkers; review of the literature. J Turk Ger Gynecol Assoc. 2013 Jun 1;14(2):98-103. doi: 10.5152/jtgga.2013.52385[↩][↩]
- Becker CM, Gattrell WT, Gude K, Singh SS. Reevaluating response and failure of medical treatment of endometriosis: a systematic review. Fertil Steril. 2017 Jul;108(1):125-136. doi: 10.1016/j.fertnstert.2017.05.004[↩][↩]





{kind=link}