 Afrikaans
Afrikaans Albanian
Albanian Amharic
Amharic Arabic
Arabic Armenian
Armenian Azerbaijani
Azerbaijani Basque
Basque Belarusian
Belarusian Bengali
Bengali Bosnian
Bosnian Bulgarian
Bulgarian Catalan
Catalan Cebuano
Cebuano Chichewa
Chichewa Chinese (Simplified)
Chinese (Simplified) Chinese (Traditional)
Chinese (Traditional) Corsican
Corsican Croatian
Croatian Czech
Czech Danish
Danish Dutch
Dutch English
English Esperanto
Esperanto Estonian
Estonian Filipino
Filipino Finnish
Finnish French
French Frisian
Frisian Galician
Galician Georgian
Georgian German
German Greek
Greek Gujarati
Gujarati Haitian Creole
Haitian Creole Hausa
Hausa Hawaiian
Hawaiian Hebrew
Hebrew Hindi
Hindi Hmong
Hmong Hungarian
Hungarian Icelandic
Icelandic Igbo
Igbo Indonesian
Indonesian Irish
Irish Italian
Italian Japanese
Japanese Javanese
Javanese Kannada
Kannada Kazakh
Kazakh Khmer
Khmer Korean
Korean Kurdish (Kurmanji)
Kurdish (Kurmanji) Kyrgyz
Kyrgyz Lao
Lao Latin
Latin Latvian
Latvian Lithuanian
Lithuanian Luxembourgish
Luxembourgish Macedonian
Macedonian Malagasy
Malagasy Malay
Malay Malayalam
Malayalam Maltese
Maltese Maori
Maori Marathi
Marathi Mongolian
Mongolian Myanmar (Burmese)
Myanmar (Burmese) Nepali
Nepali Norwegian
Norwegian Pashto
Pashto Persian
Persian Polish
Polish Portuguese
Portuguese Punjabi
Punjabi Romanian
Romanian Russian
Russian Samoan
Samoan Scottish Gaelic
Scottish Gaelic Serbian
Serbian Sesotho
Sesotho Shona
Shona Sindhi
Sindhi Sinhala
Sinhala Slovak
Slovak Slovenian
Slovenian Somali
Somali Spanish
Spanish Sundanese
Sundanese Swahili
Swahili Swedish
Swedish Tajik
Tajik Tamil
Tamil Telugu
Telugu Thai
Thai Turkish
Turkish Ukrainian
Ukrainian Urdu
Urdu Uzbek
Uzbek Vietnamese
Vietnamese Welsh
Welsh Xhosa
Xhosa Yiddish
Yiddish Yoruba
Yoruba Zulu
ZuluContents [hide]
- Aortic valve stenosis
- How your heart works
- What are heart valves?
- Aortic valve stenosis causes
- Aortic valve stenosis prevention
- Aortic valve stenosis symptoms
- Aortic valve stenosis complications
- Aortic valve stenosis diagnosis
- Aortic valve stenosis staging
- Aortic valve stenosis treatment
- Surgery and other procedures
- What happens during the aortic valve stenosis surgery
- What to expect after the aortic valve stenosis surgery
- What can go wrong with aortic valve stenosis surgery?
- Aortic valve stenosis treatment without surgery
- Physical Activity Restrictions
- Lifestyle and home remedies
- Pregnancy
- Aortic valve stenosis prognosis
- Aortic valve stenosis life expectancy
Aortic valve stenosis
Aortic valve stenosis or aortic stenosis is a heart condition where the heart’s aortic valve narrows making it harder for the heart to pump blood through the aortic valve. The word stenosis means constriction or narrowing. In aortic stenosis, the aortic valve is narrowed.
The aortic valve is like a one-way door leading out of the heart. The aortic valve sits between the left ventricle and the aorta, which is the artery that carries blood from the heart to the rest of the body. The aortic valve must open fully and close fully with each heartbeat so the heart can pump enough blood around the body.
About 4 in 1,000 people have a congenital valvular disease most commonly a valve with two cusps called a bicuspid aortic valve, which may lead to the development of aortic valve stenosis by a younger age – e.g. around 30 years of age. The relative prevalence of aortic stenosis in patients with tri-leaflet versus congenitally abnormal aortic valves varies with age 1. Approximately 40% of patients with rheumatic heart disease will have aortic valve involvement. In addition, many elderly people (> 65 years of age) can have degenerative aortic valve stenosis caused by atherosclerosis and calcification of the aortic valve, although only some will have symptoms 2, 3.
The causes of aortic stenosis vary geographically as calcific stenosis is more common in North America and Europe, while rheumatic valve disease is more common in developing countries. The number is expected to increase twofold or threefold in the coming decades with the aging of the population 4. The prevalence of calcific aortic sclerosis is about 1% to 2% in patients aged 65 or less and 29% in patients aged 65 or more 5. About 2 to 9% of patients aged greater than 75 have severe aortic stenosis 6, 7. The prevalence of aortic sclerosis ranges from 9 to 45% in patients with a mean age of 54 to 81 and increases with age 8.
In aortic valve stenosis the opening is narrowed, the heart must work much harder to try and deliver enough blood to the body and can become overworked. As a result of all this strain on your heart, this in turn leads to increased demand for blood and oxygen from the heart and possibly leads to subsequent angina, irregular heart rhythms or heart failure. Arrhythmias such as atrial fibrillation are often precipitated by the changes to the left ventricle. The end result is left ventricular failure. Symptoms of heart failure usually begin to occur when the valvular orifice size is reduced to less than 1/3 of normal. Your heart might be straining if you are short of breath, tired or notice a build-up of fluid in the body.
Many people with aortic stenosis or aortic valve stenosis don’t experience noticeable symptoms until the amount of restricted blood flow becomes greatly reduced.
Symptoms of aortic stenosis in adults may include:
- Chest pain
- Rapid, fluttering heartbeat
- Trouble breathing or feeling short of breath
- Feeling dizzy or light-headed, even fainting
- Difficulty walking short distances
- Decline in activity level or reduced ability to do normal activities
It may be important to note someone with aortic valve stenosis may not complain of symptoms. However, if you or your family members notice a decline in routine physical activities or significant fatigue, it’s worth a visit to your doctor to check your heart function.
Infants and children who have aortic stenosis due to a congenital defect may exhibit symptoms such as:
- Fatigue upon exertion
- Failure to gain weight
- Poor or inadequate feeding
- Breathing problems.
Your doctor might suspect aortic valve stenosis if they hear a murmur or click while checking your heart with a stethoscope.
To confirm aortic valve stenosis diagnosis, they might refer you for the following tests:
- Echocardiogram (or echo). This is an ultrasound of your heart. It shows how well your valves are working.
- Transesophageal echocardiogram (TEE). This is another type of echo that shows more details about how your valves are working.
- Exercise testing. This test shows if you get any symptoms when doing exercise and helps doctors to diagnose you.
- Heart MRI or CT scan. In some cases, your doctor might recommend a heart MRI or CT scan to see your heart more clearly.
The best treatment for aortic valve stenosis is surgery or transcatheter aortic valve replacement (TAVR) 9. So far medicines have not been shown to work when treating aortic valve stenosis 4, 10, 11. The right surgery for you depends on the type of aortic valve stenosis you have and how severe it is.
If you have any questions about what treatment is best for you, you should speak to your heart surgeon and heart doctor.
- Balloon valvuloplasty. This is a procedure where the doctor inserts a thin tube (also known as a catheter) into an artery in your leg and guides it to your heart. The tube (catheter) has a balloon at the end of it. Once the tube reaches your heart, the balloon is inflated to open up the narrowed valve. The balloon is then deflated and the tube is removed.
- Valve replacement. Your aortic valve might need to be replaced if a balloon valvuloplasty is not suitable for you. Valve replacement is an open-heart procedure meaning the surgeon will work directly on your heart. Your aortic valve may be replaced by a mechanical valve or a biological valve. A mechanical valve will last longer but you need to take anticoagulant medicines for the rest of your life to prevent blood from clumping up around the valve.
- Transcatheter aortic valve replacement (TAVR). Doctors may perform a less invasive procedure called transcatheter aortic valve replacement (TAVR) instead of open-heart valve surgery to replace a narrowed aortic valve. Transcatheter aortic valve replacement (TAVR) may be an option for people who are considered to be at intermediate or high risk of complications from surgical aortic valve replacement.
- The Ross procedure also known as pulmonary autograft procedure. The Ross procedure is a type of aortic valve replacement where your own pulmonary valve (pulmonary autograft) replaces the diseased aortic valve, and your pulmonary valve is then replaced with a donor valve (pulmonary homograft) from a cadaver or a stentless xenograft, offering a living valve substitute for aortic valve replacement 12. The Ross procedure is used to treat severe aortic valve disease, such as aortic stenosis or regurgitation, in children and young adults. It’s particularly beneficial for individuals with congenital aortic valve disease. It can also be used for patients with a bicuspid aortic valve.
How your heart works
Your heart is a muscular organ about the size of the palm of your hand that pumps blood to your body. Your heart, the center of your circulatory system, consists of four chambers, two on the right and two on the left 13. The two upper chambers (atria) receive blood. The two lower chambers (ventricles) pump blood. The upper chambers, the right and left atria, receive incoming blood. The lower chambers, the more muscular right and left ventricles, with right ventricle pumping blood out of your heart to your lungs and the left ventricle pumping blood out of your heart to other parts of your body. Your heart has two pumps separated by an inner wall called the septum. The right side of the heart pumps blood to the lungs to pick up oxygen. The left side of the heart receives the oxygen-rich blood from the lungs and pumps it to the body. The heart valves, which keep blood flowing in the right direction, are gates at the chamber openings. Four heart valves open and close to let blood flow in only one direction through your heart. The mitral valve — which lies between the two chambers on the left side of your heart — comprises two flaps of tissue called leaflets.
Heart 4 Chambers
- 2 upper chambers are called atrium (two is called an atria). The atria collect blood as it flows into your heart.
- 2 lower chambers are called ventricles.
- Right ventricle (RV) pumps Deoxygenated blood out of your heart to your lungs. Deoxygenated blood, also known as venous blood, is blood that has a lower oxygen concentration and a higher concentration of carbon dioxide than oxygenated blood.
- Left ventricle (LV) pumps Oxygenated blood out of your heart to other parts of your body. Oxygenated blood, also known as arterial blood, is blood rich in oxygen, typically bright red, that is pumped from the left ventricle of your heart to your body through arteries (aorta) after picking up oxygen in your lungs.
The circulatory system consists of a network of blood vessels, such as arteries, veins, and capillaries. These blood vessels carry blood to and from all areas of your body. Your body depends on your heart’s pumping action to deliver oxygen- and nutrient-rich blood to the body’s cells. When your body’s cells are nourished properly, your body can function normally. Just like an engine makes a car go, your heart keeps your body running.
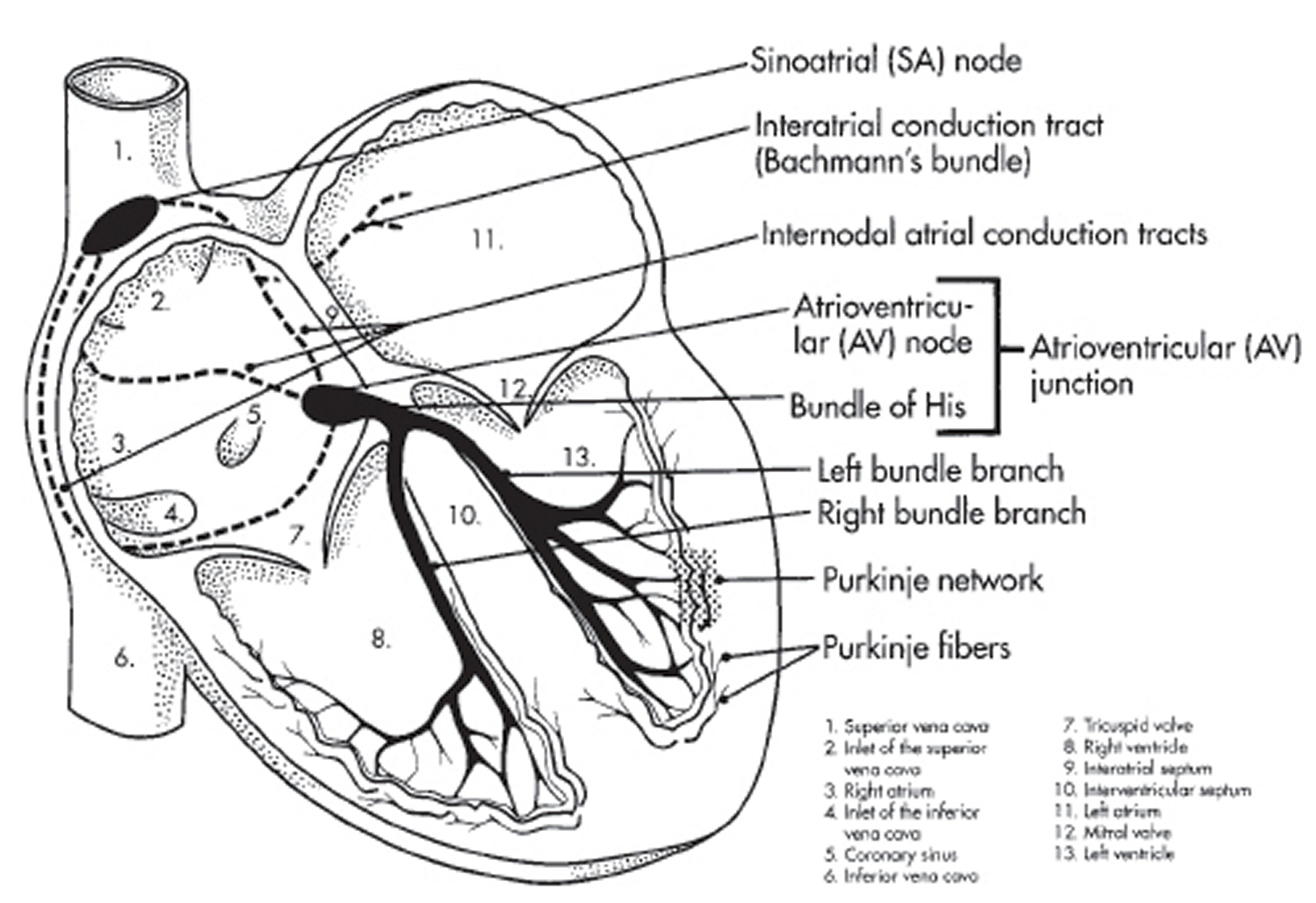
An electrical system controls your heart and uses electrical signals to contract the heart’s walls. When the heart walls contract, blood is pumped into your circulatory system. Inlet and outlet valves in your heart chambers ensure that blood flows in the right direction.
Your heart is vital to your health and nearly everything that goes on in your body. Without your heart’s pumping action, blood can’t move throughout your body.
Your blood carries the oxygen and nutrients that your organs need to work well. Blood also carries carbon dioxide (a waste product) to your lungs so you can breathe it out.
A healthy heart supplies your body with the right amount of blood and oxygen at the rate needed to work well. If disease or injury weakens your heart, your body’s organs won’t receive enough blood to work normally.
Your heart has 2 sides, separated by an inner wall called the septum. The right side of the heart pumps blood to your lungs to pick up oxygen. The left side of your heart receives the oxygen-rich blood from the lungs and pumps it to the body.
Figure 1. Human heart anatomy
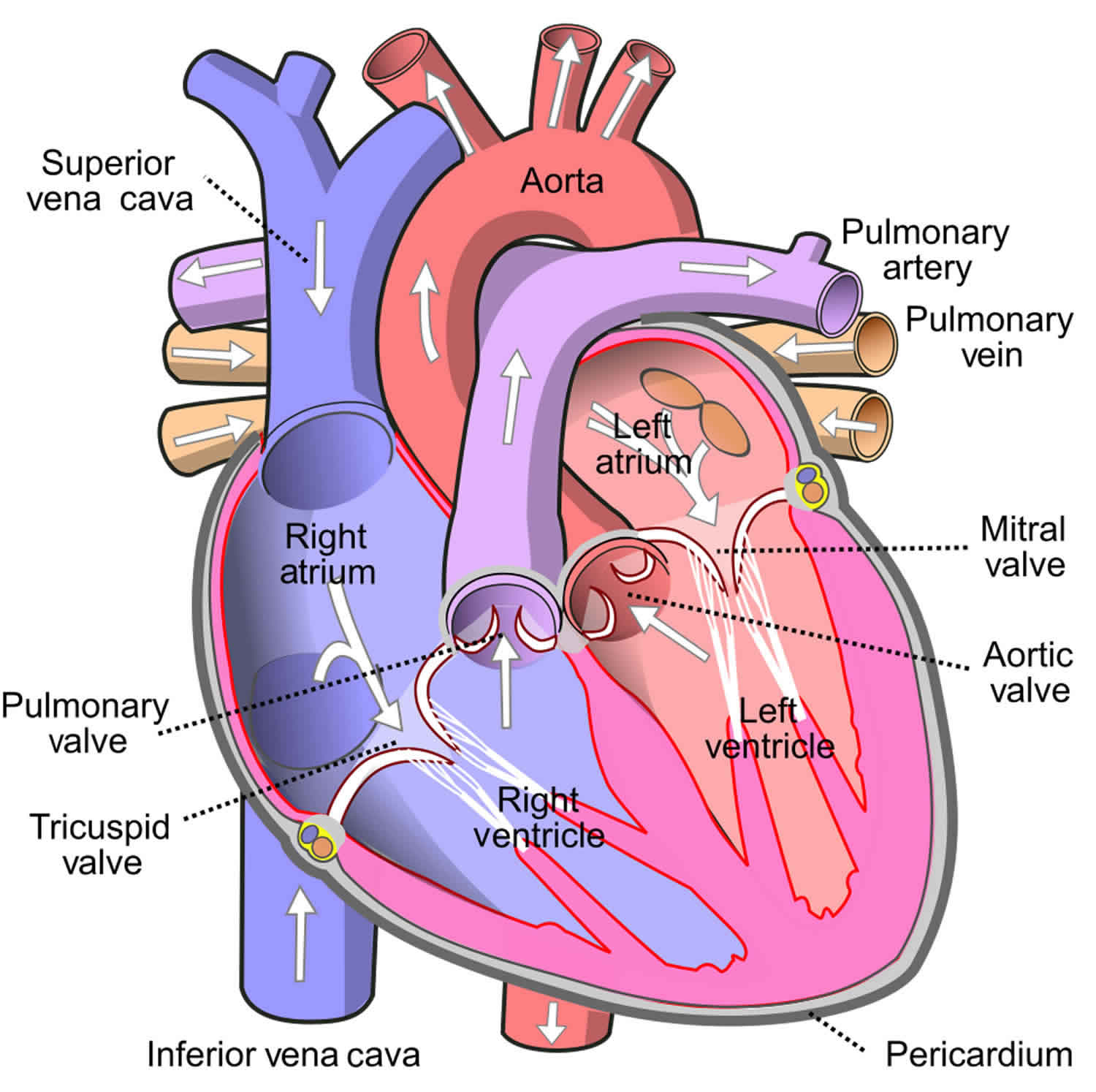
Figure 2. The anatomy of the heart chambers

Figure 3. Normal heart blood flow

Figure 4. The heart’s electrical system

What are heart valves?
Your heart also has 4 valves that open and close to let blood flow from the atria to the ventricles and from the ventricles into the two large arteries connected to the heart in only one direction when the heart contracts (beats). The four heart valves are:
- Tricuspid valve, located between the right atrium and right ventricle
- Pulmonary or pulmonic valve, between the right ventricle and the pulmonary artery. The pulmonary artery carries blood from your heart to your lungs.
- Mitral valve, between the left atrium and left ventricle
- Aortic valve, between the left ventricle and the aorta. This aorta carries blood from the heart to the body.
Each valve has a set of flaps also called leaflets or cusps. The mitral valve has two flaps; the others have three. Valves are like doors that open and close. They open to allow blood to flow through to the next chamber or to one of the arteries. Then they shut to keep blood from flowing backward. Blood flow occurs only when there’s a difference in pressure across the valves, which causes them to open. Under normal conditions, the valves permit blood to flow in only one direction.
Your heart 4 chambers and 4 valves and is connected to various blood vessels. Veins are blood vessels that carry blood from the body to your heart. Arteries are blood vessels that carry blood away from your heart to your body.
Your heart pumps blood to your lungs and to all the body’s tissues by a sequence of highly organized contractions of the four chambers. For your heart to function properly, the four chambers must beat in an organized way.
When your heart’s valves open and close, they make a “lub-DUB” sound that a doctor can hear using a stethoscope 14.
- The First heart sound (S1) — the “lub” —is made by the mitral and tricuspid valves closing at the beginning of systole. Systole is when the ventricles contract, or squeeze, and pump blood out of the heart.
- The Second heart sound (S2) — the “DUB” —is made by the aortic and pulmonary valves closing at the beginning of diastole. Diastole is when the ventricles relax and fill with blood pumped into them by the atria.
Figure 5. The anatomy of the heart valves
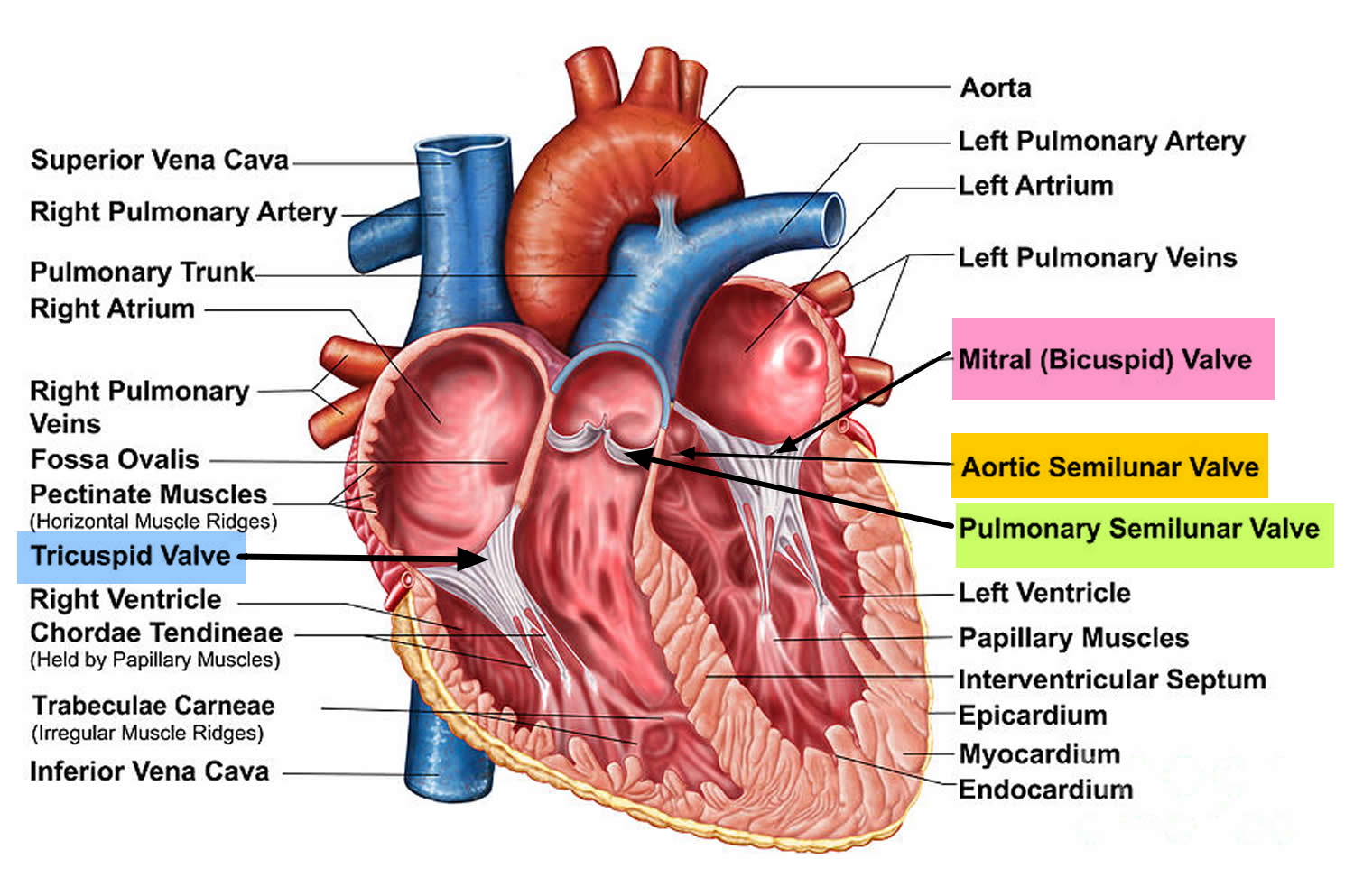
Figure 6. Top view of the 4 heart valves
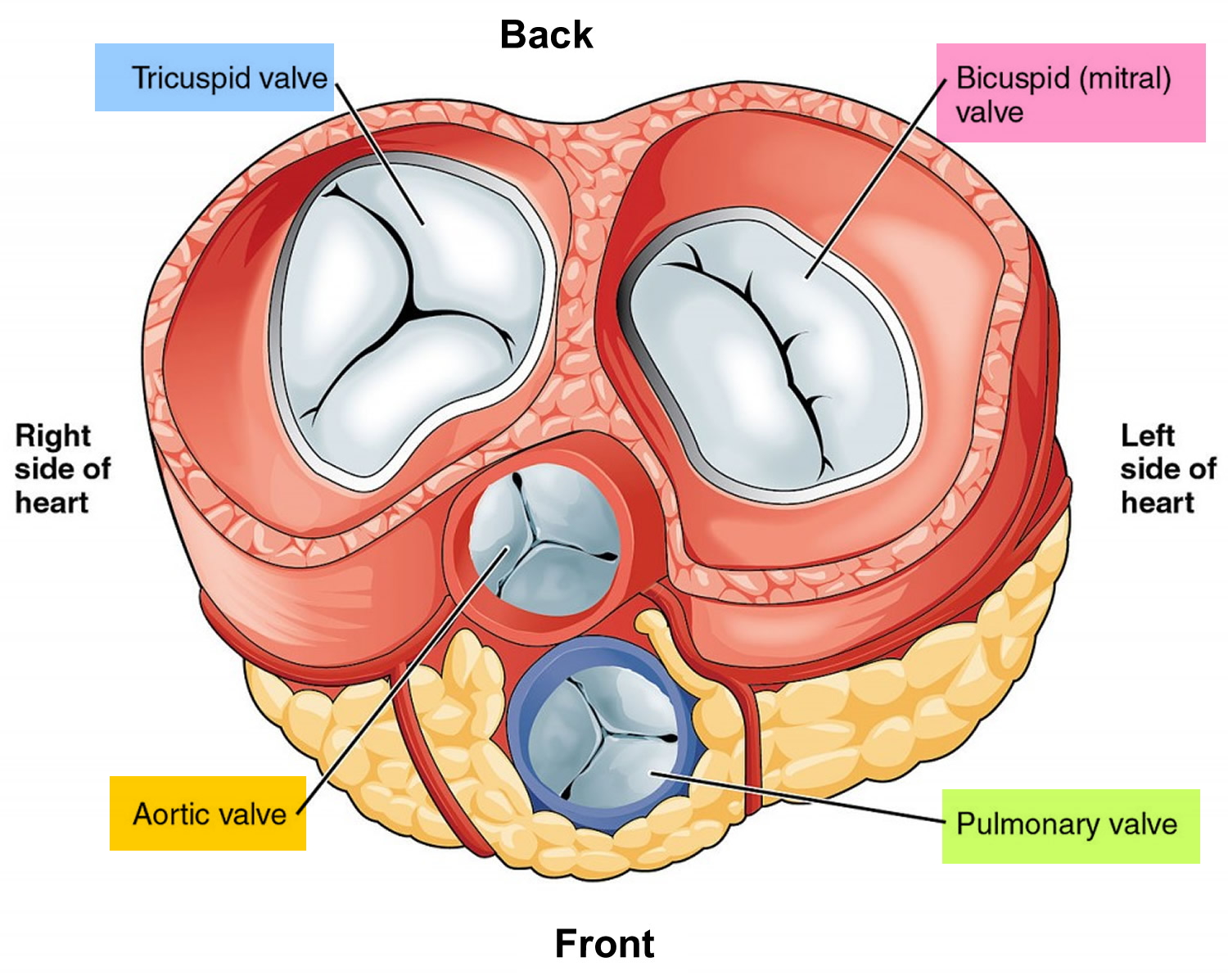 Footnote: The mitral valve has 2 flaps; tricuspid, pulmonary and aortic valves have three flaps.
Footnote: The mitral valve has 2 flaps; tricuspid, pulmonary and aortic valves have three flaps.Figure 7. Normal heart blood flow
Figure 8. Heart valves function
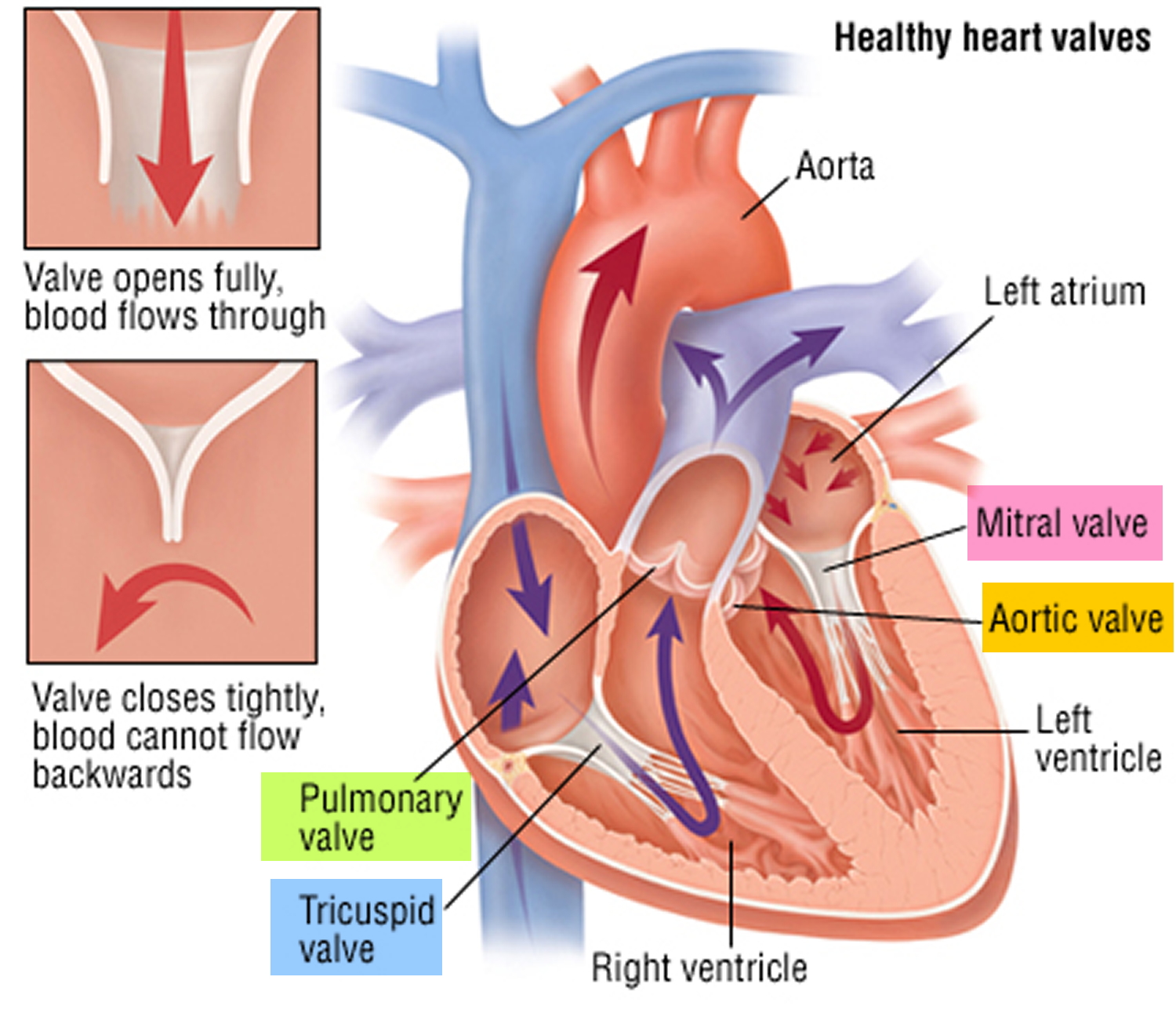
Footnotes: Heart valves are like doors that open and close. Heart valves open to allow blood to flow through to the next chamber or to one of the arteries. Then they shut to keep blood from flowing backward. Blood flow occurs only when there’s a difference in pressure across the valves, which causes them to open. Under normal conditions, heart valves permit blood to flow in only one direction.
Figure 9. Aortic valve stenosis
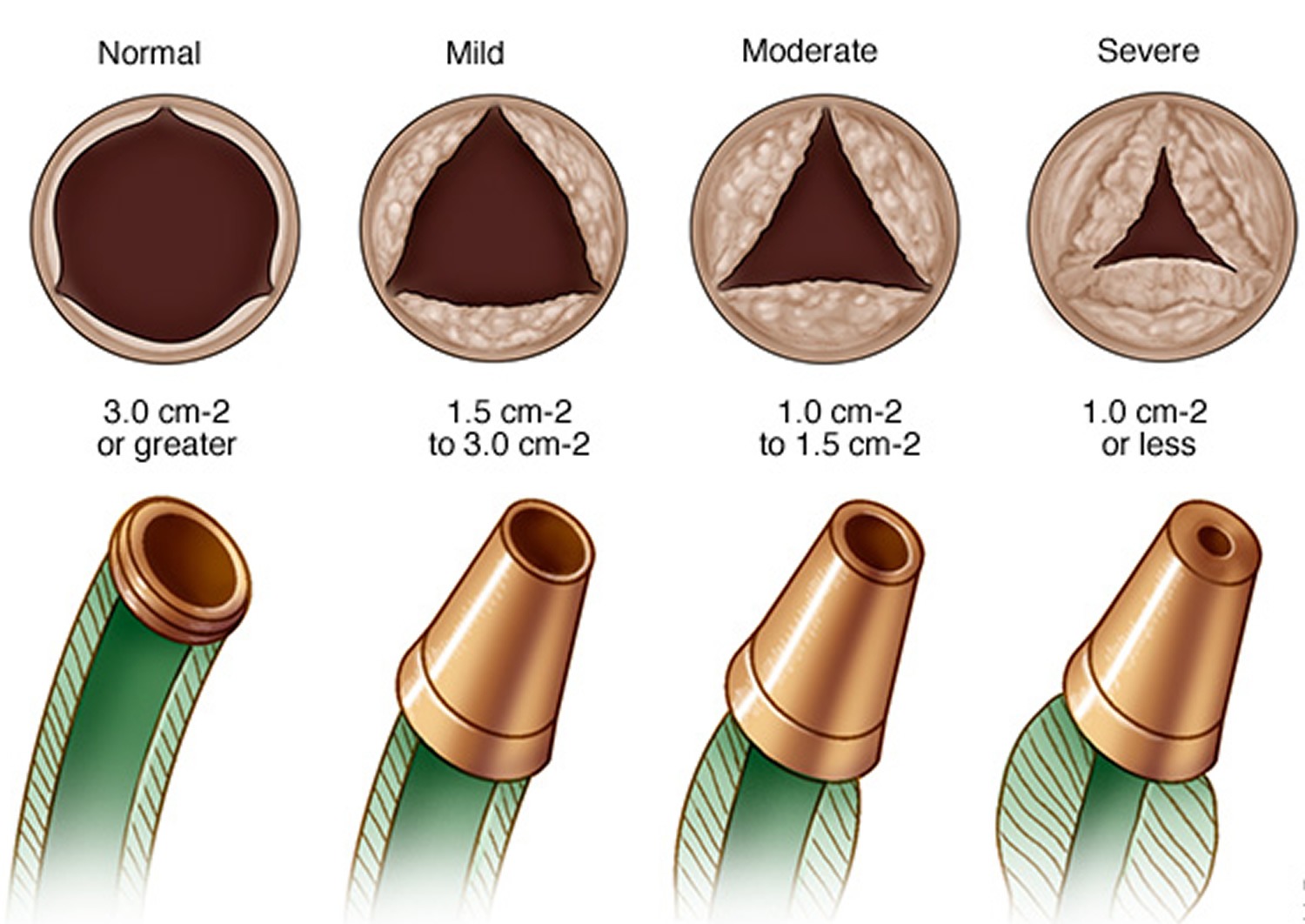
Footnotes: In aortic valve stenosis, there is progressive narrowing of the aortic valve opening over time (top row), which results in increased pressure within the heart and reduced capacity to pump blood to the body. This is similar to attaching smaller and smaller nozzles to the end of a garden hose (bottom row). The narrowing from the nozzle slows the forward flow of water and results in progressive pressure buildup within the garden hose.
Blood Flow
The Right Side of Your Heart
In figure 7 above, the superior vena cava (SVC) and inferior vena cava (IVC) are shown in blue to the left of the heart muscle as you look at the picture. The superior vena cava (SVC) and inferior vena cava (IVC) are the largest veins in your body.
After your body’s organs and tissues have used the oxygen in your blood, the vena cavae carry the oxygen-poor blood (deoxygenated blood or venous blood) back to the right atrium of your heart.
- The superior vena cava (SVC) carries oxygen-poor blood from the upper parts of your body, including your head, chest, arms, and neck.
- The inferior vena cava (IVC) carries oxygen-poor blood from the lower parts of your body from the abdomen and lower extremities back to the right side of your heart for oxygenation.
The oxygen-poor blood (deoxygenated blood or venous blood) from the vena cavae flows into your heart’s right atrium. From the right atrium, blood is pumped into the right ventricle. And then from the right ventricle, blood is pumped to your lungs through the pulmonary arteries (shown in blue in the center of figure 7).
Once in the lungs, the blood travels through many small, thin blood vessels called capillaries. There, the blood picks up more oxygen and transfers carbon dioxide to the lungs—a process called gas exchange.
The oxygen-rich blood passes from your lungs back to your heart through the pulmonary veins (shown in red to the left of the right atrium in figure 7).
The Left Side of Your Heart
Oxygen-rich blood from your lungs passes through the pulmonary veins (shown in red to the right of the left atrium in figure 7 above). The blood enters the left atrium and is pumped into the left ventricle.
From the left ventricle, the oxygen-rich blood is pumped to the rest of your body through the aorta. The aorta is the main artery that carries oxygen-rich blood to your body.
Like all of your organs, your heart needs oxygen-rich blood. As blood is pumped out of your heart’s left ventricle, some of it flows into the coronary arteries (shown in red in figure 7).
Your coronary arteries are located on your heart’s surface at the beginning of the aorta. They carry oxygen-rich blood to all parts of your heart.
For the heart to work well, your blood must flow in only one direction. Your heart’s valves make this possible. Both of your heart’s ventricles have an “in” (inlet) valve from the atria and an “out” (outlet) valve leading to your arteries.
Healthy valves open and close in exact coordination with the pumping action of your heart’s atria and ventricles. Each valve has a set of flaps called leaflets or cusps that seal or open the valve. This allows blood to pass through the chambers and into your arteries without backing up or flowing backward.
What is ejection fraction?
Ejection fraction (EF) is a measurement of your heart’s ability to pump oxygen-rich blood out to your body, expressed as a percentage (%), of how much oxygen-rich blood the left ventricle (LV) pumps out with each heart contraction 15. Ejection fraction (EF) refers to how well your heart pumps blood. Ejection fraction (EF) is the amount of blood pumped out of your heart’s lower chambers (ventricles) each time it contracts. An ejection fraction (EF) of 60 percent means that 60 percent of the total amount of blood in the left ventricle (LV) is pushed out with each heartbeat. A normal heart’s ejection fraction (normal EF) is between 50 and 70 percent 15. With each heartbeat, 50% to 70% of the blood in your left ventricle gets pumped out to your body. However, it is important to note that you can have a normal ejection fraction measurement and still have heart failure. This is called heart failure with preserved ejection fraction (HFpEF) previously known as diastolic heart failure. Heart failure with preserved ejection fraction (HFpEF) happens when your heart’s muscle has become so thick and stiff that the ventricle holds a smaller than usual volume of blood. In this case, your heart might still have an ejection fraction that falls in the normal range (EF≥50%) because your heart is pumping out a normal percentage of the blood that enters it. But in heart failure with preserved ejection fraction (HFpEF), the total amount of blood pumped isn’t enough to meet your body’s needs.
To understand ejection fraction (EF), it’s helpful to understand how blood flows through your heart:
- Blood enters your heart through the top right section (right atrium).
- Between heartbeats, there’s a short pause (diastole, the phase of the heartbeat when your heart muscle relaxes and allows heart chambers to fill with blood). This is when blood flows through a valve down to the left ventricle.
- Once the ventricle is full, the next heartbeat pumps out (ejects) a portion of the blood out to the body. Also called systole, the phase of the heartbeat when your heart muscle contracts and pumps blood from the heart chambers into the arteries.
The simplest classification of left ventricular ejection fraction (LVEF) as per the American College of Cardiology (ACC) that is used clinically as follows 16:
- Hyperdynamic = left ventricular ejection fraction (LVEF) greater than 70%
- Normal = LVEF 50% to 70% (midpoint 60%)
- Mild dysfunction = LVEF 40% to 49% (midpoint 45%)
- Moderate dysfunction = LVEF 30% to 39% (midpoint 35%)
- Severe dysfunction = LVEF less than 30%
Table 1. Ejection Fraction Percentage
| Sex | Normal | Mildly Abnormal | Moderately Abnormal | Severely Abnormal |
|---|---|---|---|---|
| Male | 52% to 72% | 41% to 51% | 30% to 40% | Below 30% |
| Female | 54% to 74% | 41% to 53% | 30% to 40% | Below 30% |
Types of ejection fraction
There are 2 types of ejection fraction: left ventricular ejection fraction (LVEF) and right ventricular ejection fraction (RVEF). Left ventricular ejection fraction (LVEF) measures how much blood gets pumped from the left ventricle with each contraction. Typically, ejection fraction refers to left ventricular. Right ventricular ejection fraction (RVEF) measures how much blood is pumped out of the right side of the heart, to the lungs.
Left ventricular ejection fraction (LVEF)
Ejection fraction (EF) typically refers to the left side of your heart or left ventricular ejection fraction (LVEF). It shows how much oxygen-rich blood is pumped out of the left ventricle (LV) to most of your body’s organs with each contraction. Left ventricular ejection fraction (LVEF) helps determine the severity of dysfunction on the left side of your heart.
Right ventricular ejection fraction (RVEF)
Right ventricular ejection fraction (RVEF) measures the amount of oxygen-poor blood or deoxygenated blood or venous blood pumped out of the right side of your heart to your lungs for oxygen. Right ventricular ejection fraction (RVEF) is important if you have right-sided heart failure. But this condition is not as common as left-sided heart failure.
What’s an unhealthy ejection fraction?
Ejection fraction (EF) refers to how well your heart pumps blood. The ejection fraction is the percentage of blood pumped out of the ventricle after a heart contraction. Ejection fraction (EF) is the amount of blood pumped out of your heart’s lower chambers (ventricles) each time it contracts. Your ejection fraction is an indicator of how well your heart is working. A low ejection fraction typically means you have or are at risk for heart failure. An ejection fraction (EF) from 41 to 49 percent (EF from 41% to 49%) might be considered too low. The lower your heart’s ejection fraction, the weaker your heart’s pumping action is. This occurs in people with severe heart failure. You can also have a low ejection fraction in the earlier stages of heart failure. However, ejection fraction (EF) does not always indicate that a person is developing heart failure, but it could indicate damage, perhaps from a previous heart attack. Some people with a normal ejection fraction also have heart failure. This is known as heart failure with preserved ejection fraction (HFpEF). An ejection fraction measurement under 40 percent (EF<40%) might be evidence of heart failure or cardiomyopathy (disease of the heart muscle that makes it harder for the heart to pump blood). In severe cases, ejection fraction (EF) can be even lower than 40.
According to the American Heart Association:
- Ejection fraction 50 to 70% (EF = 50% to 70%): Normal heart function.
- Ejection fraction 41 to 49% (EF = 41% to 49%): A mildly reduced left ventricle (LV) ejection fraction. Can indicate previous heart damage from heart attack or cardiomyopathy. You might not experience heart failure symptoms. Or, you may have symptoms with physical activity but not at rest.
- Ejection fraction less than 40% (EF < 40%): Your heart pumping ability is below normal. The lower the ejection fraction, the higher the risk of life-threatening complications, like cardiac arrest. Symptoms may be severe and may affect you even when sitting still.
- Ejection fraction greater than 75% (EF > 75%): Can indicate a heart condition like hypertrophic cardiomyopathy (HCM), a genetic heart condition where the heart muscle thickens, making it harder for the heart to pump blood effectively. This thickening can lead to various symptoms and complications, including shortness of breath, chest pain, and an increased risk of arrhythmias and a common cause of sudden cardiac arrest.
The lower your ejection fraction, the more severe your heart failure symptoms may be. You might experience:
- Confusion.
- Fatigue.
- Heart palpitations.
- Nausea.
- Shortness of breath (dyspnea).
- Water retention in your abdomen or feet.
- Weakness.
Some things that may cause a reduced ejection fraction are:
- Weakness of the heart muscle, such as cardiomyopathy.
- Heart attack that damaged the heart muscle.
- Heart valve disease.
- Long-term, uncontrolled high blood pressure.
What is the formula for ejection fraction?
The ejection fraction (EF) formula equals the amount of blood pumped out of the ventricle with each contraction (stroke volume or SV) divided by the end-diastolic volume (EDV), the total amount of blood in the ventricle. To express as a percentage, you would multiply by 100.
- Ejection fraction (EF) = (stroke volume [SV]/end-diastolic volume [EDV]) x 100
Stroke volume (SV) is the volume of blood pumped out of the heart’s left ventricle during each systolic cardiac contraction. Ventricular stroke volume (SV) is often thought of as the amount of blood (mL) ejected per beat by the left ventricle into the aorta (or from the right ventricle into the pulmonary artery). Moreover, a more precise definition for stroke volume (SV) and one that is used in echocardiography when assessing ventricular function is the difference between the ventricular end-diastolic volume (EDV) and the end-systolic volume (ESV). The end-diastolic volume (EDV) is the filled volume of the ventricle before contraction, and the end-systolic volume (ESV) is the residual volume of blood remaining in the ventricle after ejection. In a typical heart, the end-diastolic volume (EDV) is about 120 mL of blood and the end-systolic volume (ESV) is about 50 mL of blood 18. The difference in the end-diastolic volume (EDV) and the end-systolic volume (ESV), 70 mL, that is Stroke volume (SV) = end-diastolic volume (EDV) – end-systolic volume (ESV). Therefore, any factor that alters either the EDV or the ESV will change the SV. For example, an increase in EDV increases SV, whereas an increase in ESV decreases SV.
Aortic valve stenosis causes
Around 4 in 1000 people are born with an aortic valve that is shaped differently, with only two cusps (flaps) instead of three (see Figure 6) 19. These people can get aortic stenosis earlier in life. But the most common cause of aortic stenosis is that the aortic valve can get hardened or scarred as people get older. Aortic valve stenosis occurs in about 2% of people over 65 years of age with more than 13% of Americans 75 and older having aortic stenosis. It occurs more often in men than in women.
Calcium buildup of the aortic valve happens sooner in people who are born with abnormal aortic or bicuspid valves. In rare cases, calcium buildup can develop more quickly when a person has received chest radiation (such as for cancer treatment).
After a bicuspid aortic valve has been diagnosed, you’ll need lifelong care from a pediatric cardiologist as a child, and then from an adult congenital cardiologist as an adult, including regular follow-up appointments to monitor for any changes in your condition.
A bicuspid aortic valve can be inherited in families. Because of this, doctors often recommend that all first-degree relatives — parents, children and siblings — of people with a bicuspid aortic valve be screened with an echocardiogram.
A less common cause of aortic stenosis is rheumatic heart disease. Rheumatic heart disease can develop after strep throat or scarlet fever. Valve problems do not develop for 5 to 10 years or longer after rheumatic fever occurs. Rheumatic fever is becoming rarer in the United States. However, rheumatic valve disease is the most common cause of aortic stenosis in developing countries 19.
Other rare causes of aortic stenosis include calcification of the tri-leaflet valve, alkaptonuria, systemic lupus erythematosus (SLE), ochronosis (a condition characterized by a blue-black or gray-blue pigmentation of the skin and other tissues, caused by the accumulation of a dark pigment in connective tissues, often due to a metabolic disorder or exposure to certain substances), radiation therapy, homozygous type 2 lipoproteinemia, and metabolic diseases such as Fabry disease 20, 21. Mineral metabolism disturbances, such as end-stage renal disease, have also been shown to contribute to the calcification of the heart valves 22. Obstruction to the left ventricular (LV) outflow can occur above or below the aortic valve, causing supravalvular stenosis and subvalvular stenosis, respectively. Hypertrophic cardiomyopathy (HCM), rare a genetic heart condition where the heart muscle thickens, making it harder for the heart to pump blood effectively, can cause dynamic subvalvular stenosis.
Congenital aortic valve stenosis
There are 3 types of congenital aortic stenosis, you will be diagnosed depending on where the narrowing or stenosis is. Speak to your heart doctor if you have any questions about what type of aortic stenosis you have.
Valvular aortic stenosis
This is a type of aortic valve stenosis where the aortic valve is narrowed. It is the most common type of aortic valve stenosis and is usually caused by a bicuspid valve (a valve with 2 flaps instead of 3).
Supravalvular aortic valve stenosis
This is where the aorta is narrowed just after the aortic valve. This can also cause problems with the aortic valve. This type of aortic valve stenosis is usually caused by another genetic condition called William’s syndrome.
Subaortic stenosis
This type of aortic valve stenosis occurs below the aortic valve.
Risk Factors for aortic valve stenosis
The most common predisposing factors are:
- Certain heart conditions present at birth (congenital heart disease) such as a bicuspid aortic valve;
- Rheumatic heart disease;
- Old age;
- History of infections that can affect the heart;
- Having cardiovascular risk factors, such as diabetes, high cholesterol and high blood pressure;
- Chronic kidney disease;
- History of radiation therapy to the chest.
It should be noted that a clinically similar picture can be produced by obstruction to left ventricular outflow at either above or below the valve.
Bicuspid aortic valve
Some people are born with a bicuspid aortic valve, in which the aortic valve — located between the lower left heart chamber (left ventricle) and the main artery that leads to the body (aorta) — has only two (bicuspid) cusps instead of three. People may also be born with one (unicuspid) or four (quadricuspid) cusps, but these are rare.
A bicuspid aortic valve may cause the heart’s aortic valve to narrow (aortic valve stenosis). This narrowing prevents the valve from opening fully, which reduces or blocks blood flow from the heart to the body. In some cases, the aortic valve doesn’t close tightly, causing blood to leak backward into the left ventricle (aortic valve regurgitation). Most people with a bicuspid aortic valve aren’t affected by valve problems until they’re adults, and some may not be affected until they’re older adults. Some children with bicuspid aortic valves may have valve problems.
Some people with a bicuspid aortic valve may have an enlarged aorta — the main blood vessel leading from the heart. There is also an increased risk of aortic dissection.
Children and adults with a bicuspid aortic valve will require regular monitoring for any changes in their condition, such as valve problems or an enlarged aorta, by doctors trained in congenital heart disease (congenital cardiologists).
You may eventually need treatment for valve problems such as aortic valve stenosis, aortic valve regurgitation or an enlarged aorta.
Calcium buildup on the valve
With age, heart valves may accumulate deposits of calcium (aortic valve calcification). Calcium is a mineral found in your blood. As blood repeatedly flows over the aortic valve, deposits of calcium can build up on the valve’s cusps. These calcium deposits aren’t linked to taking calcium tablets or drinking calcium-fortified drinks.
These deposits may never cause any problems. However, in some people — particularly those with a congenitally abnormal aortic valve, such as a bicuspid aortic valve — calcium deposits result in stiffening of the cusps of the valve. This stiffening narrows the aortic valve and can occur at a younger age.
However, aortic valve stenosis that is related to increasing age and the buildup of calcium deposits on the aortic valve is most common in older people. It usually doesn’t cause symptoms until ages 70 or 80.
Rheumatic fever
A complication of strep throat infection, rheumatic fever may result in scar tissue forming on the aortic valve. Scar tissue alone can narrow the aortic valve and lead to aortic valve stenosis. Scar tissue can also create a rough surface on which calcium deposits can collect, contributing to aortic valve stenosis later in life.
Rheumatic fever may damage more than one heart valve, and in more than one way. A damaged heart valve may not open fully or close fully — or both. While rheumatic fever is rare in the United States, some older adults had rheumatic fever as children.
Aortic valve stenosis prevention
Some possible ways to prevent aortic valve stenosis include:
- Taking steps to prevent rheumatic fever. You can do this by making sure you see your doctor when you have a sore throat. Untreated strep throat can develop into rheumatic fever. Fortunately, strep throat can usually be easily treated with antibiotics. Rheumatic fever is more common in children and young adults.
- Addressing risk factors for coronary artery disease. These include high blood pressure, obesity and high cholesterol levels. These factors may be linked to aortic valve stenosis, so it’s a good idea to keep your weight, blood pressure and cholesterol levels under control if you have aortic valve stenosis.
- Taking care of your teeth and gums. There may be a link between infected gums (gingivitis) and infected heart tissue (endocarditis). Inflammation of heart tissue caused by infection can narrow arteries and aggravate aortic valve stenosis.
Once you know that you have aortic valve stenosis, your doctor may recommend that you limit strenuous activity to avoid overworking your heart.
Aortic valve stenosis symptoms
Some people with aortic stenosis don’t have any symptoms, especially if the aortic valve is only a little narrower.
Most people with aortic stenosis do not develop symptoms until the disease is advanced. The diagnosis may have been made when a doctor heard a heart murmur and performed tests.
Others have:
- Palpitations (heart racing or skipping a beat)
- Fainting, weakness, or dizziness with exercise
- Feeling tired or worn out
- Chest pain
- Feeling short of breath
- Chest discomfort: The chest pain may get worse with activity and reach into the arm, neck, or jaw. The chest may also feel tight or squeezed.
- Cough, possibly bloody.
- Breathing problems when exercising.
- Becoming easily tired.
In infants and children, symptoms include:
- Becoming easily tired with exertion (in mild cases)
- Failure to gain weight
- Poor feeding
- Serious breathing problems that develop within days or weeks of birth (in severe cases)
Children with mild or moderate aortic stenosis may get worse as they get older. They are also at risk for a heart infection called bacterial endocarditis.
People with aortic stenosis may have a past history of rheumatic fever and have symptoms of atrial fibrillation – palpitations. Early in the disease, they may experience:
- Exercise-induced fainting;
- Angina; and
- Dyspnea (shortness of breath).
Later in the aortic valve stenosis disease, these progress to frank heart failure with dyspnea, orthopnoea (shortness of breath while lying flat), and paroxysmal nocturnal dyspnea (waking up gasping for breath).
Occasionally, they may present with myocardial infarction (heart attack). If you’re having symptoms like this, it’s a good idea to see your doctor.
Aortic valve stenosis complications
- Heart failure
- Stroke
- Blood clots
- Bleeding
- Heart rhythm abnormalities (arrhythmias)
- Infections that affect the heart, such as endocarditis
- Death
Aortic valve stenosis diagnosis
Your doctor will ask you questions and examine you. They might or might not hear a heart murmur when they listen to your heart.
A heart murmur, click, or other abnormal sound is almost always heard through a stethoscope. Your doctor may be able to feel a vibration or movement when placing a hand over the heart. There may be a faint pulse or changes in the quality of the pulse in the neck.
Blood pressure may be low.
Depending on what your doctor find, you might be asked to have tests such as an ECG (electrocardiogram), a chest X-ray and an echocardiogram, which is an ultrasound of the heart.
A chest X-ray can sometimes show a scarred aortic valve. An ECG gives valuable information about your heart, including if your left ventricle is enlarged from the effort of pumping blood through a narrowed valve.
- Echocardiography (echo). The echocardiogram is the most common test to diagnose a problem with the heart valves. An echocardiogram shows how efficiently your heart is pumping and whether any of the valves are narrowed. Echocardiography is a painless test that uses sound waves to create moving pictures of your heart. The pictures show the size and shape of your heart and how well your heart is pumping blood. A type of echo called Doppler ultrasound shows how well blood flows through your heart’s chambers and valves.
- There are different types of echocardiograms. The type you have depends on the information your heart doctor needs. A standard echocardiogram is done from outside the body. An ultrasound device moves over the skin of the chest above the heart. If more details are needed about the heart, a transesophageal echocardiogram (TEE) may be done. This type creates pictures of the heart from inside the body. The ultrasound device attaches to a tube that goes down the throat and into the esophagus.
- Electrocardiogram (ECG). In this test, wires (electrodes) attached to pads on your skin measure the electrical activity of your heart. An ECG can detect enlarged chambers of your heart, heart disease and abnormal heart rhythms.
- Chest X-ray. A chest X-ray can help your doctor determine whether your heart is enlarged, which can occur in aortic valve stenosis. It can also show whether you have an enlarged blood vessel (aorta) leading from your heart or any calcium buildup on your aortic valve. A chest X-ray can also help doctors determine the condition of your lungs.
- Exercise tests or stress tests. Exercise tests help doctors see whether you have signs and symptoms of aortic valve disease during physical activity, and these tests can help determine the severity of your condition. These tests often involve walking on a treadmill or riding a stationary bike while the heart’s activity is checked. If you are unable to exercise, medications that have similar effects as exercise on your heart may be used.
- Cardiac computerized tomography (CT) scan or heart CT. A cardiac CT scan uses a series of X-rays to create detailed images of your heart and heart valves. Doctors may use this test to measure the size of your aorta and look at your aortic valve more closely. A heart CT scan may be done to see how much calcium buildup is on the valve. It also can show how severe the aortic valve stenosis is.
- Cardiac MRI or heart MRI. A cardiac MRI uses magnetic fields and radio waves to create detailed images of your heart. This test may be used to determine the severity of your condition and evaluate the size of your aorta.
- Cardiac catheterization. This test isn’t often used to diagnose aortic valve disease, but it may be used if other tests aren’t able to diagnose the condition or to determine its severity. In this procedure, your doctor threads a thin tube (catheter) through a blood vessel in your arm or groin and guides it to an artery in your heart. Doctors may inject a dye through the catheter, which helps your arteries become visible on an X-ray (coronary angiogram). This provides your doctor with a detailed picture of your heart arteries and how your heart functions. It can also measure the pressure inside your heart chambers.
Aortic valve stenosis staging
After testing confirms a diagnosis of aortic valve disease or other heart valve disease, your heart doctor (cardiologist) may tell you the stage or severity of your heart condition. Staging helps determine the most appropriate treatment for you.
The stage of heart valve disease depends on many things, including your symptoms, the disease severity, the structure of the heart valve or valves, and blood flow through the heart and lungs 23. The definition of “severe” aortic valve stenosis is based on the severity of symptoms, as well as the severity at which intervention will improve symptoms 23.
Table 2. Aortic Valve Stenosis Stages
| Stage | Definition | Valve Anatomy | Valve Hemodynamics | Hemodynamic Consequences | Symptoms |
|---|---|---|---|---|---|
| A | At risk of aortic stenosis |
| Aortic maximum velocity <2 m/s with normal leaflet motion |
|
|
| B | Progressive aortic stenosis |
OR
|
|
|
|
| C: Asymptomatic severe aortic stenosis | |||||
| C1 | Asymptomatic severe aortic stenosis |
|
|
|
|
| C2 | Asymptomatic severe aortic stenosis with left ventricular systolic dysfunction |
|
|
|
|
| D: Symptomatic severe aortic stenosis | |||||
| D1 | Symptomatic severe high-gradient aortic stenosis |
|
|
|
|
| D2 | Symptomatic severe low-flow, low-gradient aortic stenosis with reduced left ventricular ejection fraction (LVEF) |
|
|
|
|
| D3 | Symptomatic severe low-gradient aortic stenosis with normal left ventricular ejection fraction (LVEF) or paradoxical low-flow severe aortic stenosis |
|
AND
|
|
|
Footnotes: Each stage of aortic valve stenosis is defined by patient symptoms, valve anatomy, valve hemodynamics, and changes in the left ventricle (LV) and vasculature. Hemodynamic severity is best characterized by the transaortic maximum velocity (or mean pressure gradient) when the transaortic volume flow rate is normal. Some patients with aortic valve stenosis have a low transaortic volume flow rate that is either because of left ventricle systolic dysfunction with a low left ventricular ejection fraction (LVEF) or because of a small, hypertrophied left ventricle with a low stroke volume. Severe aortic valve stenosis with low flow is designated D2 (with a low LVEF) or D3 (with a normal LVEF). Meticulous attention to detail is required during assessment of aortic valve hemodynamics, either with Doppler echocardiography or cardiac catheterization, and the inherent variability of the measurements and calculations should always be considered in clinical decision-making.
Aortic valve stenosis treatment
Treatment for aortic valve stenosis depends on your symptoms and how severe the aortic valve stenosis is. Aortic valve stenosis ranges from mild to severe (see Stage of aortic valve stenosis in Table 2).
If you have no symptoms or just mild ones from your aortic stenosis, your doctor may just want you to have regular check-ups. The latest European guidelines recommend follow-up every 2 to 3 years in younger patients with mild aortic stenosis and low aortic valve calcification, yearly in moderate aortic stenosis, and every 6 months in patients with severe aortic stenosis to timely identify patients with an indication for valve replacement 9. American guidelines are slightly less stringent and recommend follow-up every 3 to 5 years in mild aortic stenosis, every 1 to 2 years in moderate aortic stenosis, and every 6 to 12 months in severe aortic stenosis 24. However, the rate of aortic valve stenosis progression may vary considerably between individual patients, and a fixed follow-up interval may be too long for one patient and too short for another 25, 26, 27.
Some people need medicines to treat valve disease symptoms or reduce the risk of complications. You may eventually need a surgery to repair or replace the narrowed aortic valve, even if you don’t have symptoms. Aortic valve surgery may be done at the same time as other types of heart surgery.
Other treatments for aortic valve disease may include:
- Heart-healthy lifestyle changes. Eat healthy, get regular exercise and stay active, and do not smoke.
- Medicines to treat symptoms or reduce the risk of complications.
- Surgery to fix or replace the aortic valve.
If you are affected by aortic stenosis, your doctor might advise you not to overexert yourself.
People with severe aortic stenosis may be told not to play competitive sports, even if they have no symptoms. If symptoms do occur, strenuous activity must often be limited.
Some people with aortic stenosis need an operation to remove the aortic valve and replace it with an artificial one. Another operation is sometimes done where your own valve is opened up with a tiny balloon. But this doesn’t work as well as replacing the valve.
Children with aortic stenosis can sometimes get their aortic valve repaired. However, if the valve is very abnormal it is better to replace it with a new one. Using a balloon to stretch the valve can help for a while, but over time the valve can become narrow again, meaning another operation might need to be done.
General treatment:
- Avoidance of strenous activity as this increases demand on the heart.
- Treating angina with beta blockers such as vasodilators may aggravate syncope.
- Antibiotic prophylaxis against infective endocarditis.
Surgery and other procedures
Surgery to repair or replace the aortic valve is often done for adults or children who develop symptoms. Even if symptoms are not very bad, your doctor may recommend surgery based on test results. The results of aortic valve replacement are often excellent. To get the best treatment, go to a center that regularly performs this type of surgery.
Surgery to repair or replace an aortic valve is usually done through a cut in the chest. Less invasive approaches may be available. Ask your heart doctor which type of aortic valve treatment is best for you.
A less invasive procedure called balloon valvuloplasty may be done instead of or before surgery.
- A balloon is placed into an artery in the groin, threaded to the heart, placed across the valve, and inflated. However, narrowing often occurs again after this procedure.
- A newer procedure done at the same time as valvuloplasty can implant an artificial valve. This procedure is most often done in patients who cannot have surgery, but it is becoming more common.
Some children may need aortic valve repair or replacement. Children with mild aortic stenosis may be able to take part in most activities.
Surgery and procedures for aortic valve stenosis include:
Aortic valve replacement (AVR)
Aortic valve replacement (AVR) is often needed to treat aortic valve stenosis. Aortic valve replacement is recommended in adults with symptomatic aortic stenosis, even if the symptoms are mild 5. Aortic valve replacement (AVR) is also recommended in asymptomatic patients with severe aortic stenosis with 28, 11, 29:
- Left ventricular ejection fraction less than 50% (LVEF <50%),
- Who are undergoing coronary artery bypass grafting (CABG) or any other form of heart surgery
- Abnormal exercise treadmill test,
- Peak velocity (Vmax) greater than 5 m/sec and mean pressure gradient greater than 60, and
- Annual progression of peak velocity of greater than 0.3 m/s/year.
In aortic valve replacement, your surgeon removes the damaged aortic valve and replaces it with a mechanical valve or a valve made from cow, pig or human heart tissue (biological tissue valve). Another type of biological tissue valve replacement that uses your own pulmonary valve is sometimes possible. The pulmonary valve is replaced with a biological lung tissue valve from a deceased donor. This more complicated surgery is called the Ross procedure or pulmonary autograft procedure.
Symptoms such as shortness of breath during physical activity (exertional dyspnea) and angina (chest pain or discomfort caused by reduced blood flow to the heart) are relieved in most of the patients, and a majority will experience an increase in exercise tolerance 5. Left ventricular ejection fraction (LVEF) often improves after the surgery, but longitudinal strain might still be impaired 30.
The operative mortality in surgical aortic valve replacement is about 3.2% in patients undergoing isolated aortic valve replacement 31, 32. It is less than 1% in patients aged less than 70 and having minimal comorbidities. Advanced age should not be considered a contraindication to aortic valve replacement surgery, and 30-day mortality is about 4.2% 5.
Ross procedure
The Ross procedure is a type of aortic valve replacement where your own pulmonary valve (pulmonary autograft) replaces the diseased aortic valve, and your pulmonary valve is then replaced with a donor valve (pulmonary homograft) from a cadaver or a stentless xenograft, offering a living valve substitute for aortic valve replacement 12. The Ross procedure is used to treat severe aortic valve disease, such as aortic stenosis or regurgitation, in children and young adults. It’s particularly beneficial for individuals with congenital aortic valve disease. It can also be used for patients with a bicuspid aortic valve. However, the long-term durability of the pulmonary autograft is a concern, and some patients may require reintervention later in life.
Biological tissue valves degenerate over time and may eventually need to be replaced. People with mechanical valves will need to take blood-thinning medications (blood thinners or anticoagulants) for life to prevent blood clots. Your doctor will discuss with you the benefits and risks of each type of valve and discuss which valve may be appropriate for you.
How Ross procedure or pulmonary autograft procedure works 12:
- Removal of the diseased aortic valve: The surgeon removes the diseased or damaged aortic valve.
- Pulmonary valve replacement: The patient’s own healthy pulmonary valve is then removed and placed in the aortic position.
- Pulmonary valve reconstruction: The pulmonary valve position is reconstructed with a pulmonary homograft
Benefits of the Ross procedure:
- Avoids the need for long-term medication: Unlike mechanical valve replacements, the Ross procedure generally doesn’t require lifelong anticoagulation (blood thinners).
- Favorable blood flow dynamics: The pulmonary autograft provides a more natural blood flow compared to mechanical valves.
- Allows for valve growth: In children, the pulmonary autograft can grow with the child, unlike a mechanical valve.
- Reduced risk of endocarditis: The pulmonary autograft is less prone to infection compared to mechanical valves.
- Long-term viability: The Ross procedure is known for its long-term durability and has shown to restore a normal life expectancy in young and middle-aged adults.
Transcatheter aortic valve replacement (TAVR)
Doctors may perform a less invasive procedure called transcatheter aortic valve replacement (TAVR) instead of open-heart valve surgery to replace a narrowed aortic valve. Transcatheter aortic valve replacement (TAVR) may be an option for people who are considered to be at intermediate or high risk of complications from surgical aortic valve replacement. Transcatheter aortic valve replacement (TAVR) was initially shown to be superior to medical therapy in patients who are not candidates for surgery. But later, it turned out to be superior to the surgical aortic valve replacement in high-risk and also intermediate-risk patients. Transcatheter aortic valve replacement (TAVR) has transformed the treatment of patients in calcific aortic stenosis over the last decade.
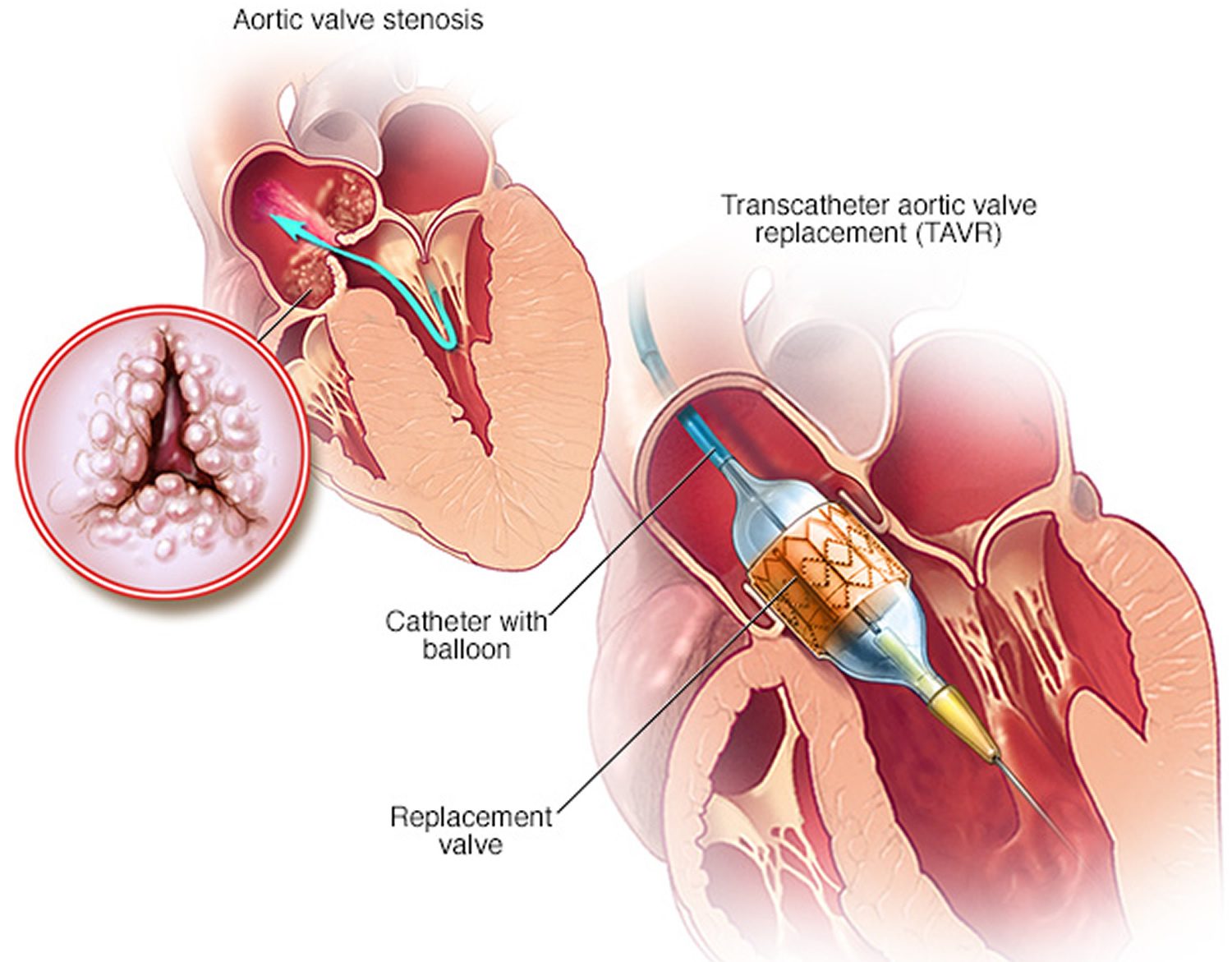
In transcatheter aortic valve replacement, doctors insert a catheter in your leg or chest and guide it to your heart. The most common approach used is the transfemoral approach, especially as there is a progressive decrease in the sheath size. A heart valve team of cardiac surgeons, interventional cardiologists, clinical and imaging experts in valve disease, as well as anesthetists, and geriatricians, are essential to recommend the choice of surgical aortic valve replacement versus transcatheter aortic valve replacement (TAVR), given the complexity of the procedure. A replacement valve made of cow or pig tissue is then inserted through the catheter and guided to the aortic valve area. A balloon on the catheter’s tip inflates to press the new valve into place. Some valves can self-expand. When the valve is implanted, doctors remove the catheter from your blood vessel.
Doctors may also conduct a catheter procedure to insert a replacement valve into a failing biological tissue valve that is no longer working properly. Other catheter procedures to repair or replace aortic valves continue to be researched.
The long-term durability of the transcatheter aortic valve replacement (TAVR) procedure is yet to be determined.
Figure 9. Transcatheter aortic valve replacement (TAVR)
Balloon valvuloplasty
In a balloon valvuloplasty, a heart doctor inserts a catheter with a balloon on the tip into an artery in your groin or arm and guides it to the aortic valve. Once in place, a balloon on the tip of the catheter is inflated. This makes the valve opening wider. The balloon is then deflated. The catheter and balloon are removed. The balloon valvuloplasty procedure can treat aortic valve stenosis in infants and children with aortic valve stenosis, but in adults, the aortic valve tends to narrow again in adults who have had the balloon valvuloplasty procedure. So it’s usually done only if an adult is too sick for surgery or if an adult is waiting for a aortic valve replacement.
Along with relief of aortic stenosis, some people who have had balloon valvuloplasty may have an increased amount of aortic regurgitation after the balloon valvuloplasty procedure.
Aortic valve repair
Aortic valve repair isn’t often performed to treat a bicuspid aortic valve. To repair an aortic valve, surgeons may separate valve flaps (cusps) that have fused, or reshape or remove excess valve tissue so that the cusps can close tightly. However, valve repair is rarely used to treat aortic valve stenosis. Generally aortic valve stenosis requires aortic valve replacement.
Aortic root and ascending aorta surgery
In this procedure, surgeons remove the enlarged section of the aorta located near the heart. Surgeons then replace it with a synthetic tube (graft), which is sewn into place. The aortic valve can also be replaced or repaired during this procedure.
In some cases, doctors may replace the enlarged section of the aorta and the aortic valve remains in place.
What happens during the aortic valve stenosis surgery
The standard procedure is done under a general anesthetic, so you will be completely unconscious.
The surgeon will cut through your breastbone to reach your heart and a machine will take over the working of your heart and lungs during surgery.
The faulty valve will be replaced with a biological valve made of human or animal tissue, or a mechanical valve made of metal. During the surgery you may need a blood transfusion.
Newer techniques involve smaller cuts or no cuts to the chest wall. Your doctor will be able to discuss the risks and benefits of each procedure with you.
What to expect after the aortic valve stenosis surgery
You will be taken to the intensive care unit for monitoring, then to a ward until you are ready to leave hospital.
Full recovery from aortic valve replacement can take from several weeks to months, during which you may have pain and tiredness.
You will need to take anti-clotting medication for life if you receive a mechanical valve, or for a few months after receiving a biological valve.
What can go wrong with aortic valve stenosis surgery?
Possible risks include:
- bleeding
- infection
- poor healing of the wound
- changes to your heart rhythm
- damage to your heart
- problems with your kidneys or lungs, particularly if you have a pre-existing condition.
Aortic valve stenosis treatment without surgery
Some people with aortic valve stenosis may need medicines to treat symptoms or reduce the risk of complications. Medicines are used to treat symptoms of heart failure or abnormal heart rhythms most commonly atrial fibrillation. These include diuretics (water pills), nitrates, and beta-blockers. High blood pressure should also be treated. If aortic stenosis is severe, this treatment must be done carefully so blood pressure does not drop too far.
People with even mildly abnormal aortic valves are at risk for bacterial endocarditis. That’s why it’s important for you to keep your mouth clean and healthy with regular dental check ups. Getting antibiotics before dental procedures isn’t proven to be beneficial and so isn’t universally recommended any more. But if you have a prosthetic valve, you’ll need to take antibiotics before dental work. Your cardiologist can provide you more information and can answer your questions about preventing endocarditis.
In the past, most people with heart valve problems were given antibiotics before dental work or a procedure such as colonoscopy. The antibiotics were given to prevent an infection of the damaged heart. However, antibiotics are now used much less often before dental work and other procedures. Check with your health care provider to find out whether you need antibiotics.
People with aortic valve stenosis and other heart conditions should stop smoking and be tested for high cholesterol.
Physical Activity Restrictions
Physical exercise has many benefits and should be a regular part of almost anyone’s life. That includes most people with congenital heart disease.
- If you have a severely obstructed valve, vigorous exercise is not a good idea. Your cardiologist may tell you to limit your activity if this is the case. Ask your cardiologist about your exercise limits.
There is no proven link between exercise and harmful outcome from aortic valve stenosis causing an enlarged aorta, but many physicians feel that such patients shouldn’t engage in strenuous exercise, particularly activity that involves straining or grunting like heavy weight lifting 33.
- It’s likely that for most patients, the benefits of exercise outweigh the perceived risks. Low-intensity activity is still preferred. If you have any questions about the appropriateness of exercise for you, talk to your doctor.
If you’ve been inactive for a long time and want to start a regular exercise routine, it’s often wise to talk with your doctor about how to get started safely. Your doctor may recommend an exercise test which can provide you with guidelines for exercise.
Physical activities for children
If the aortic valve is abnormally formed but has no important obstruction or leak, your child may not need any special precautions regarding physical activities and may be able to participate in normal activities without increased risk. Some children with obstruction, leak or heart muscle abnormalities may have to limit how much they do some kinds of exercise. Check with your child’s pediatric cardiologist about this.
What types of exercise and how much?
You should speak to your heart doctor before starting or making any changes to your exercise routine no matter what your level of aortic valve stenosis is. You may be able to exercise normally, but it depends on how severe your aortic valve stenosis is, and if you’ve had it repaired.
The best and safest types of exercise are “aerobic” activities. These increase the heart rate and make you breath heavily. Examples include brisk walking, swimming, biking, jogging, rowing, cross-country skiing, hiking or stair climbing. Team or court sports such as basketball, soccer, football, tennis, squash and volleyball are also aerobic activities.
A good rule of thumb is to increase your activity so you breathe hard and fast but can still carry on a conversation with someone. If you can speak in full sentences but still feel your heart pounding, you’re likely benefiting from a safe level of activity.
Often patients are trained to check their heart rate during or immediately after activity. Their target heart rate is 70-80 percent of their predicted maximal heart rate (defined as 220 minus age).
It’s best to avoid activities that cause grunting or straining (medically referred to as a “valsalva maneuver”). This happens when a person bears down against a closed throat to increase the strength of arm or abdominal muscles. There’s often a tendency to do this when lifting heavy weights, doing sit-ups, push-ups or chin-ups, etc., but it may be harmful. Straining causes a sudden rise in blood pressure, which adds strain on the heart; it increases the pressure in the lungs, which can affect blood flow from the body into the lungs; and it often means there’s more force on the chest wall, and many congenital heart patients have surgical scars in the chest that can be damaged, particularly in the first year after surgery.
Intensely physical sports such as football, boxing or hockey may increase the chance for injury and unnecessary strain on the cardiovascular system.
Any amount of activity is better than none, and the more physically active a person is, the greater the anticipated cardiovascular benefit. Guidelines for the general population suggest at least 30 minutes of dedicated aerobic activity a day for five or more days a week. This is a good target for congenital heart patients too. If it seems like too much, start with a more modest goal and build from there.
Lifestyle and home remedies
You’ll have regular follow-up appointments with your doctor to monitor your condition. You’ll need to continue taking all your medications as prescribed.
Your doctor may suggest you incorporate several heart-healthy lifestyle changes into your life, including:
- Eating a heart-healthy diet. Eat a variety of fruits and vegetables, low-fat or fat-free dairy products, poultry, fish, and whole grains. Avoid saturated and trans fat, and excess salt and sugar.
- Maintaining a healthy weight. Aim to keep a healthy weight. If you’re overweight or obese, your doctor may recommend that you lose weight.
- Getting regular physical activity. Aim to include about 30 minutes of physical activity, such as brisk walks, into your daily fitness routine. Talk with your heart doctor about the amount and type of exercise that’s best for you. If you have aortic valve stenosis, your doctor may recommend that you limit strenuous activity to avoid overworking your heart.
- Managing stress. Find ways to help manage your stress, such as through relaxation activities, meditation, physical activity, and spending time with family and friends.
- Avoiding tobacco or do not smoke or use tobacco. Smoking is a major risk factor for heart disease. If you smoke, quit. Ask your doctor about resources to help you quit smoking. Joining a support group may be helpful.
- Control blood pressure, blood sugar and cholesterol. Make lifestyle changes and take medicines as directed. Get regular health checkups.
- Limit alcohol. If you choose to drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women and up to two drinks a day for men.
- Get good sleep. Poor sleep may increase the risk of heart disease and other health conditions. Adults should aim for 7 to 9 hours daily.
For women with aortic valve stenosis, it’s important to talk with your doctor before you become pregnant. Your doctor can discuss with you which medications you can safely take, and whether you may need a procedure to treat your valve condition prior to pregnancy.
You’ll likely require close monitoring by your doctor during pregnancy. Doctors may recommend that women with severe valve stenosis avoid pregnancy to avoid the risk of complications.
Pregnancy
The risk from pregnancy depends on how severely the aortic valve is obstructed or how much it’s leaking.
If you have mild or moderate aortic stenosis and your left heart muscle (left ventricle) is functioning normally, you can have a safe pregnancy, but you need medical supervision throughout the pregnancy. Sometimes balloon valvuloplasty can be done to relieve symptoms if they occur during pregnancy but only when symptoms can’t be controlled by medication and bed rest.
If your aortic stenosis is severe and you have symptoms, avoid conception until you’ve had your heart valve repaired or replaced. If you’re considering pregnancy and you have aortic valve stenosis, you should meet with a multidisciplinary medical team that can give you more information about the risk of pregnancy to you and your baby.
Pregnancy in aortic regurgitation is better tolerated, but if the regurgitation has weakened your heart muscle and signs of heart failure are present before pregnancy, the risk posed by pregnancy is higher.
In patients who have had their heart valve replaced with a metal (mechanical) heart valve, they may be taking warfarin (Coumadin) which can cause risk to the fetus and alternative means of blood thinning may be required. In aortic insufficiency, women may be taking medicines such as ACE inhibitors such as lisinopril (Zestril) or enalapril (Vasotec). These drugs are dangerous to the developing fetus (see the section on Pregnancy) and need to be changed before conception.
It’s best to talk with your doctor before you plan to become pregnant.
Aortic valve stenosis prognosis
It is difficult to predict aortic stenosis rate of progression as it is highly variable 5. However, older age, severe leaflet calcification, hypertension, obesity, smoking, hyperlipidemia, renal insufficiency, metabolic syndrome, elevated circulating levels of lipoprotein A, and increased activity of lipoprotein-A are associated with rapid hemodynamic regression 4, 34, 35. In asymptomatic patients, repeat imaging is typically performed every 3 to 5 years for mild, 1 to 2 years for moderate, and 6 to 12 months for severe aortic stenosis unless they become symptomatic 36, 37, 29.
Doppler aortic jet velocity is the strongest predictor of symptom progression in asymptomatic aortic stenosis patients 38, 39. Prognosis remains excellent in asymptomatic aortic stenosis patients with moderate to severe aortic stenosis 40. Lack of contractile reserve in patients with low-flow, low-gradient, low ejection fraction aortic stenosis, very elevated B-type natriuretic peptide (BNP), frailty, very low mean gradient (less than 20 mm Hg), oxygen-dependent lung disease, advanced renal dysfunction, and very high Society of Thoracic Surgeons (STS) risk score are the factors useful for risk stratification in predicting symptom onset and event-free survival in symptomatic patients 5. The Society of Thoracic Surgeons (STS) risk score is widely used as a starting point to stratify patients in need of aortic valve replacement, both at the clinical and research levels. When aortic stenosis severity is moderate or symptoms are indeterminate, an elevated B-type natriuretic peptide (BNP) level can be helpful, but its role in disease progression has not been fully defined 41. Survival is poor in symptomatic aortic stenosis patients, even while the symptoms are mild, unless the outflow obstruction is relieved. Average survival without aortic valve replacement is only about 1 to 3 years after the symptom onset 38, 42, 43.
Aortic valve stenosis life expectancy
The outcome and life expectancy varies. The aortic valve stenosis may be mild and not produce symptoms (asymptomatic aortic stenosis). Over time, the aortic valve may become narrower. This may result in more severe heart problems such as:
- Atrial fibrillation and atrial flutter
- Blood clots to the brain (embolic stroke), intestines, kidneys, or other areas
- Fainting spells (syncope)
- Heart failure is one of the most common complications of aortic stenosis. Most patients will have left ventricular hypertrophy with normal systolic function. Diastolic dysfunction develops secondary to hypertrophy and fibrosis and often persists even after aortic valve replacement. However, some patients can present with systolic dysfunction secondary to the afterload mismatch, resulting in a low ejection fraction.
- High blood pressure in the arteries of the lungs (pulmonary hypertension). Pulmonary hypertension due to chronic elevation in left ventricular diastolic filling pressure. Another complication associated with aortic stenosis is conduction abnormalities. They occur due to hypertrophy, calcium extension from the valve to the interventricular septum, or existing heart disease.
- Patients with aortic stenosis are also at an increased risk for infective endocarditis, particularly patients with the bicuspid aortic valve.
Severe symptomatic aortic stenosis patients are at a high risk of sudden death. Hence, these patients need to be promptly referred for aortic valve replacement. Although sudden death is common in symptomatic patients, it can occasionally occur in asymptomatic aortic stenosis patients as well.
The prognosis of untreated aortic valve stenosis once symptoms have begun is poor, with the average life expectancy of a few years. However surgical treatments can usually halt the natural history of the disease before end stage heart failure has set in.
- Roberts WC, Ko JM. Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation. 2005 Feb 22;111(7):920-5. doi: 10.1161/01.CIR.0000155623.48408.C5[
 ]
] - Coffey S., Roberts-Thomson R., Brown A., et al. Global epidemiology of valvular heart disease. Nat Rev Cardiol. 2021;18:853–864. doi: 10.1038/s41569-021-00570-z[]
- Messika-Zeitoun D., Baumgartner H., Burwash I.G., et al. Unmet needs in valvular heart disease. Eur Heart J. 2023;44:1862–1873. doi: 10.1093/eurheartj/ehad121[]
- Lindman BR, Clavel MA, Mathieu P, Iung B, Lancellotti P, Otto CM, Pibarot P. Calcific aortic stenosis. Nat Rev Dis Primers. 2016 Mar 3;2:16006. doi: 10.1038/nrdp.2016.6[][][]
- Pujari SH, Agasthi P. Aortic Stenosis. [Updated 2023 Apr 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557628[][][][][][]
- d’Arcy JL, Coffey S, Loudon MA, Kennedy A, Pearson-Stuttard J, Birks J, Frangou E, Farmer AJ, Mant D, Wilson J, Myerson SG, Prendergast BD. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE Population Cohort Study. Eur Heart J. 2016 Dec 14;37(47):3515-3522. doi: 10.1093/eurheartj/ehw229[]
- Osnabrugge RL, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, Bogers AJ, Piazza N, Kappetein AP. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. 2013 Sep 10;62(11):1002-12. doi: 10.1016/j.jacc.2013.05.015[]
- Coffey S, Cox B, Williams MJ. The prevalence, incidence, progression, and risks of aortic valve sclerosis: a systematic review and meta-analysis. J Am Coll Cardiol. 2014 Jul 1;63(25 Pt A):2852-61. doi: 10.1016/j.jacc.2014.04.018[]
- Vahanian A., Beyersdorf F., Praz F., et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561–632. doi: 10.1093/eurheartj/ehab395[][]
- Otto CM, Prendergast B. Aortic-valve stenosis–from patients at risk to severe valve obstruction. N Engl J Med. 2014 Aug 21;371(8):744-56. doi: 10.1056/NEJMra1313875[]
- Lindman BR, Bonow RO, Otto CM. Current management of calcific aortic stenosis. Circ Res. 2013 Jul 5;113(2):223-37. doi: 10.1161/CIRCRESAHA.111.300084[][]
- Brown KN, Kanmanthareddy A. Ross Procedure for Aortic Valve Replacement. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537249[][][]
- American Heart Association. About Arrhythmia. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/About-Arrhythmia_UCM_002010_Article.jsp[]
- Centers for Disease Control and Prevention. Division of Birth Defects and Developmental Disabilities. Congenital Heart Defects (CHDs). https://www.cdc.gov/ncbddd/heartdefects/index.html[]
- Ejection Fraction Heart Failure Measurement. https://www.heart.org/en/health-topics/heart-failure/diagnosing-heart-failure/ejection-fraction-heart-failure-measurement[][]
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015 Jan;28(1):1-39.e14. doi: 10.1016/j.echo.2014.10.003[]
- Kosaraju A, Goyal A, Grigorova Y, et al. Left Ventricular Ejection Fraction. [Updated 2023 Apr 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459131 []
- Regulation of Stroke Volume. https://cvphysiology.com/cardiac-function/cf002[]
- Ross J Jr, Braunwald E. Aortic stenosis. Circulation. 1968 Jul;38(1 Suppl):61-7. doi: 10.1161/01.cir.38.1s5.v-61[][]
- Kiani AN, Fishman EK, Petri M. Aortic valve calcification in systemic lupus erythematosus. Lupus. 2006;15(12):873-6. doi: 10.1177/0961203306071709[]
- Senechal M, Germain DP. Fabry disease: a functional and anatomical study of cardiac manifestations in 20 hemizygous male patients. Clin Genet. 2003 Jan;63(1):46-52. doi: 10.1034/j.1399-0004.2003.630107.x[]
- Umana E, Ahmed W, Alpert MA. Valvular and perivalvular abnormalities in end-stage renal disease. Am J Med Sci. 2003 Apr;325(4):237-42. doi: 10.1097/00000441-200304000-00010[]
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Feb 2;143(5):e72-e227. doi: 10.1161/CIR.0000000000000923 Erratum in: Circulation. 2024 Sep 17;150(12):e267. doi: 10.1161/CIR.0000000000001284[][][]
- Otto C.M., Nishimura R.A., Bonow R.O., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;77(4):e25–e197. doi: 10.1016/j.jacc.2020.11.018[]
- Venema CS, van Bergeijk KH, Hadjicharalambous D, Andreou T, Tromp J, Staal L, Krikken JA, van der Werf HW, van den Heuvel AFM, Douglas YL, Lipsic E, Voors AA, Wykrzykowska JJ. Prediction of the Individual Aortic Stenosis Progression Rate and its Association With Clinical Outcomes. JACC Adv. 2024 Mar 6;3(4):100879. doi: 10.1016/j.jacadv.2024.100879[]
- Otto C.M., Burwash I.G., Legget M.E., et al. Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic, and exercise predictors of outcome. Circulation. 1997;95:2262–2270. doi: 10.1161/01.cir.95.9.2262[]
- Willner N., Prosperi-Porta G., Lau L., et al. Aortic stenosis progression: a systematic review and meta-analysis. J Am Coll Cardiol. 2023;16:314–328. doi: 10.1016/j.jcmg.2022.10.009[]
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD; ACC/AHA Task Force Members. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Jun 10;129(23):e521-643. doi: 10.1161/CIR.0000000000000031. Epub 2014 Mar 3. Erratum in: Circulation. 2014 Jun 10;129(23):e651. Erratum in: Circulation. 2014 Sep 23;130(13):e120. Dosage error in article text.[]
- Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC); European Association for Cardio-Thoracic Surgery (EACTS); Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Barón-Esquivias G, Baumgartner H, Borger MA, Carrel TP, De Bonis M, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schäfers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, Von Oppell UO, Windecker S, Zamorano JL, Zembala M. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012 Oct;33(19):2451-96. doi: 10.1093/eurheartj/ehs109[][]
- Kafa R, Kusunose K, Goodman AL, Svensson LG, Sabik JF, Griffin BP, Desai MY. Association of Abnormal Postoperative Left Ventricular Global Longitudinal Strain With Outcomes in Severe Aortic Stenosis Following Aortic Valve Replacement. JAMA Cardiol. 2016 Jul 1;1(4):494-6. doi: 10.1001/jamacardio.2016.1132[]
- Shahian DM, O’Brien SM, Filardo G, Ferraris VA, Haan CK, Rich JB, Normand SL, DeLong ER, Shewan CM, Dokholyan RS, Peterson ED, Edwards FH, Anderson RP; Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 3–valve plus coronary artery bypass grafting surgery. Ann Thorac Surg. 2009 Jul;88(1 Suppl):S43-62. doi: 10.1016/j.athoracsur.2009.05.055[]
- O’Brien SM, Shahian DM, Filardo G, Ferraris VA, Haan CK, Rich JB, Normand SL, DeLong ER, Shewan CM, Dokholyan RS, Peterson ED, Edwards FH, Anderson RP; Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2–isolated valve surgery. Ann Thorac Surg. 2009 Jul;88(1 Suppl):S23-42. doi: 10.1016/j.athoracsur.2009.05.056[]
- Congenital Heart Defects and Physical Activity. http://www.heart.org/HEARTORG/Conditions/CongenitalHeartDefects/CareTreatmentforCongenitalHeartDefects/Congenital-Heart-Defects-and-Physical-Activity_UCM_307738_Article.jsp[]
- Capoulade R, Mahmut A, Tastet L, Arsenault M, Bédard É, Dumesnil JG, Després JP, Larose É, Arsenault BJ, Bossé Y, Mathieu P, Pibarot P. Impact of plasma Lp-PLA2 activity on the progression of aortic stenosis: the PROGRESSA study. JACC Cardiovasc Imaging. 2015 Jan;8(1):26-33. doi: 10.1016/j.jcmg.2014.09.016[]
- Capoulade R, Chan KL, Yeang C, Mathieu P, Bossé Y, Dumesnil JG, Tam JW, Teo KK, Mahmut A, Yang X, Witztum JL, Arsenault BJ, Després JP, Pibarot P, Tsimikas S. Oxidized Phospholipids, Lipoprotein(a), and Progression of Calcific Aortic Valve Stenosis. J Am Coll Cardiol. 2015 Sep 15;66(11):1236-1246. doi: 10.1016/j.jacc.2015.07.020[]
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Fleisher LA, Jneid H, Mack MJ, McLeod CJ, O’Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017 Jun 20;135(25):e1159-e1195. doi: 10.1161/CIR.0000000000000503[]
- Généreux P, Stone GW, O’Gara PT, Marquis-Gravel G, Redfors B, Giustino G, Pibarot P, Bax JJ, Bonow RO, Leon MB. Natural History, Diagnostic Approaches, and Therapeutic Strategies for Patients With Asymptomatic Severe Aortic Stenosis. J Am Coll Cardiol. 2016 May 17;67(19):2263-2288. doi: 10.1016/j.jacc.2016.02.057[]
- Stewart RA, Kerr AJ, Whalley GA, Legget ME, Zeng I, Williams MJ, Lainchbury J, Hamer A, Doughty R, Richards MA, White HD; New Zealand Heart Valve Study Investigators. Left ventricular systolic and diastolic function assessed by tissue Doppler imaging and outcome in asymptomatic aortic stenosis. Eur Heart J. 2010 Sep;31(18):2216-22. doi: 10.1093/eurheartj/ehq159[][]
- Capoulade R, Le Ven F, Clavel MA, Dumesnil JG, Dahou A, Thébault C, Arsenault M, O’Connor K, Bédard É, Beaudoin J, Sénéchal M, Bernier M, Pibarot P. Echocardiographic predictors of outcomes in adults with aortic stenosis. Heart. 2016 Jun 15;102(12):934-42. doi: 10.1136/heartjnl-2015-308742[]
- Dal-Bianco JP, Khandheria BK, Mookadam F, Gentile F, Sengupta PP. Management of asymptomatic severe aortic stenosis. J Am Coll Cardiol. 2008 Oct 14;52(16):1279-92. doi: 10.1016/j.jacc.2008.07.020[]
- Clavel MA, Malouf J, Michelena HI, Suri RM, Jaffe AS, Mahoney DW, Enriquez-Sarano M. B-type natriuretic peptide clinical activation in aortic stenosis: impact on long-term survival. J Am Coll Cardiol. 2014 May 20;63(19):2016-25. doi: 10.1016/j.jacc.2014.02.581[]
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S; PARTNER Trial Investigators. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010 Oct 21;363(17):1597-607. doi: 10.1056/NEJMoa1008232[]
- Bach DS, Siao D, Girard SE, Duvernoy C, McCallister BD Jr, Gualano SK. Evaluation of patients with severe symptomatic aortic stenosis who do not undergo aortic valve replacement: the potential role of subjectively overestimated operative risk. Circ Cardiovasc Qual Outcomes. 2009 Nov;2(6):533-9. doi: 10.1161/CIRCOUTCOMES.109.848259[]





{kind=link}