Contents
- Familial hypertriglyceridemia
- Familial hypertriglyceridemia types
- Familial hypertriglyceridemia cause
- Familial hypertriglyceridemia symptoms
- Familial hypertriglyceridemia complications
- Familial hypertriglyceridemia diagnosis
- Familial hypertriglyceridemia treatment
- Familial hypertriglyceridemia prognosis
Familial hypertriglyceridemia
Familial hypertriglyceridemia also called type IV familial dyslipidemia, type IV hyperlipoproteinemia or pure hypertriglyceridemia is a common autosomal dominant inherited disorder passed down through families in which triglyceride levels are elevated with increased plasma concentration of very-low-density lipoprotein (VLDL), typically with low LDL (low density lipoprotein) “bad” cholesterol and low HDL (high-density lipoprotein) “good” cholesterol 1, 2, 3, 4, 5. Triglycerides are a type of fat called lipid that circulate in your blood. Triglycerides are the most common type of fat in your body. Triglycerides come from foods, especially butter, oils, and other fats you eat. Triglycerides also come from extra calories your body does not need right away. Unused calories (energy you don’t need right away) are stored as triglycerides in fat cells, thus triglycerides is a major source of energy for your body. When your body needs energy, it releases the triglycerides. In between meals, triglycerides are released from fat tissue to be used as an energy source for your body. Most triglycerides are carried in the blood by lipoproteins called very low-density lipoproteins (VLDL). Some triglycerides are important for good health. However, high triglyceride levels in your blood or hypertriglyceridemia can raise your risk of heart disease and stroke. How severe familial hypertriglyceridemia is can vary based on sex, age, hormone use, and dietary factors.
Familial hypertriglyceridemia was described by Glueck and co-workers in 1973 6. Familial hypertriglyceridemia is the most common form of primary isolated hypertriglyceridemia. Familial hypertriglyceridemia is characterized by the presence of fasting plasma triglyceride levels >95th population percentile for age and gender, as well as normal to low total cholesterol levels 6. Therefore, the biochemical presentation of familial hypertriglyceridemia is characterized by variable levels of triglycerides (200–700 mg/dL) and the presence of triglyceride rich VLDL particles (type 4 hyperlipidemia).
People with familial hypertriglyceridemia often also have obesity, high blood glucose levels (hyperglycemia), high levels of insulin (hyperinsulinemia), insulin resistance, type 2 diabetes, high blood pressure (hypertension) and hyperuricemia. These factors may cause even higher triglyceride levels. When familial hypertriglyceridemia coexists with other comorbidities, such as type 2 diabetes, the metabolic syndrome or environmental factors such as increased alcohol intake or a high fat diet, the levels of triglycerides can reach values of over 1000 mg/dL with a triglyceride/cholesterol ratio of 5:1, accompanied by the presence of chylomicrons (type 5 hyperlipidemia). Hence, familial hypertriglyceridemia is associated with a life-threatening risk of acute pancreatitis 7. Alcohol, a diet high in carbohydrates, and estrogen use can make familial hypertriglyceridemia worse.
Familial hypertriglyceridemia is asymptomatic (having no symptoms). Some people with familial hypertriglyceridemia may have coronary artery disease (coronary heart disease) at an early age and can present with chylomicronemia syndrome and pancreatitis. Chylomicronemia syndrome is a disorder in which your body does not break down fats (lipids) correctly 8. This causes fat particles called chylomicrons to build up in your blood. Chylomicronemia syndrome is passed down through families. You are more likely to have familial hypertriglyceridemia if you have a family history of hypertriglyceridemia or heart disease before age 50. In most cases, familial hypertriglyceridemia is not noticeable until puberty or early adulthood.
Familial hypertriglyceridemia is most likely caused by genetic defects combined with environmental factors 9, 10. As a result, familial hypertriglyceridemia clusters in families.
Familial hypertriglyceridemia is frequently confused with other causes of HTG. This includes familial chylomicronemia syndrome 11, 12, a condition caused by mutations in the lipoprotein lipase (LPL) gene or other genes that regulate the function of lipoprotein lipase enzyme (i.e APOC2 and the LMF1 [lipase maturation factor 1]) 13, 14, 15, 16, 17.
According to the National Cholesterol Education Program Adult Treatment Panel guidelines, a normal triglyceride level is less than 150 mg/dL (less than 1.7 mmol/L) (see Table 1 below) 18. Plasma triglyceride levels reflect the triglyceride content of multiple lipoprotein particles, primarily chylomicrons and very low density lipoprotein (VLDL). Fasting triglyceride levels less than 150 mg/dL has been generally accepted as “normal” 19, 20. A non-fasting triglyceride of 175mg/dL represents ~75th percentile of the normal range, and levels of ~400mg/dL represent the 97th percentile 21, 22. There is no current widely accepted definition of elevated non-fasting triglyceride levels, but some expert groups have utilized 175mg/dL as a cut point 23, 24, 25. Due to high variability of triglyceride levels, precise definitions for non-fasting triglyceride levels are difficult to establish 26. It is important to note that after-meal triglyceride levels rarely exceed 400mg/dL even after a high fat challenge 26, 22. In the United States, hypertriglyceridemia defined as a triglyceride level greater than 150 mg/dL is prevalent in about 30% of the general population 27. According to the National Health and Nutrition Examination Survey (NHANES), fasting triglycerides of > 150 mg/dL, > 200 mg/dL and > 500 mg/dL are seen in 31%, 16.2%, and 1.1% of US adults, respectively 28.
Moderate elevations of triglycerides usually occur during early adulthood, and a triad of obesity, high blood sugar level (hyperglycemia) and hyperinsulinemia can be seen in affected individuals. In individuals with moderate elevation in plasma triglycerides associated with a normal cholesterol level, the possibility of familial hypertriglyceridemia should be suspected 1. Although patients with familial hypertriglyceridemia usually have moderate elevation of plasma triglycerides, whenever conditions known to elevate triglyceride, such as type 2 diabetes or alcohol or oral contraceptive consumption, concurrently occur, they may develop a profound hypertriglyceridemia and a mixed hyperlipidemia (type 5 lipoprotein pattern). High triglycerides may contribute to hardening of the arteries or thickening of the artery walls (atherosclerosis) — which increases the risk of stroke, heart attack and heart disease. Extremely high triglycerides can also cause acute inflammation of the pancreas (pancreatitis). Hypertension and hyperuricemia have also been frequently observed.
If you are diagnosed with high blood triglycerides, your doctor may recommend that you make heart-healthy lifestyle changes 20:
- Choose heart-healthy foods. Eat more high-fiber foods from plants. Choose 100% whole grains, whole fruits and vegetables.
- Get regular physical activity. Aim for at least 30 minutes of physical activity on most or all days of the week. Regular exercise can lower triglycerides and boost “good” cholesterol. Try to incorporate more physical activity into your daily tasks — for example, climb the stairs at work or take a walk during breaks.
- Lose weight. If you have mild to moderate hypertriglyceridemia, focus on cutting calories. Extra calories are converted to triglycerides and stored as fat. Reducing your calories will reduce triglycerides.
- Manage stress.
- Quit smoking.
- Get enough good quality sleep.
- Limit alcohol. Alcohol is high in calories and sugar and has a particularly potent effect on triglycerides. If your blood triglyceride levels are considered very high, your doctor may tell you not to drink alcohol.
If healthy lifestyle changes aren’t enough to control high triglycerides, your doctor might recommend a few different types of medicines to control or lower your triglyceride levels 20:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. These cholesterol-lowering medications may be recommended if you also have poor cholesterol numbers or a history of blocked arteries or diabetes. Examples of statins include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor).
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can also be used to remove triglycerides from the blood when paired with a healthy diet. Ezetimibe can be used with a statin drug. If statins don’t reduce cholesterol enough, doctors often suggest adding ezetimibe.
- Fibrates. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Fibrates have been shown to markedly reduce triglyceride levels by 50% and beyond. Drugs like fenofibrate and gemfibrozil help activate lipoprotein lipase (LPL) through PPAR-alpha leading to further breakdown of triglycerides. However, fibrates aren’t used if you have severe kidney or liver disease. Furthermore, caution must be noted during polypharmacy. A combination of fibrates with statins can increase the risk of statin side effects 29, 30. This is theorized to be a result of CYP-3A4 inhibition via fibrates. If combined therapy is required, exercise caution and consider statin therapy that is not primarily metabolized through CYP-3A4 (pravastatin) 30.
- Fish oil also known as omega-3 fatty acids. Fish oil or omega-3 fatty acid can help lower your triglycerides. Fish oil has shown a significant reduction of both VLDL and triglyceride levels 31. Prescription fish oil preparations such as Lovaza, contain more-active omega-3 fatty acids than many nonprescription supplements. Fish oil taken at high levels can interfere with blood clotting and cause gastrointestinal symptoms, so talk to your doctor before taking any supplements.
- Niacin also called nicotinic acid or vitamin B3. Niacin can lower your triglycerides and low-density lipoprotein (LDL) cholesterol the “bad” cholesterol. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins. Talk to your doctor before taking over-the-counter niacin because it can interact with other medications and cause significant side effects.
More than one medicine may be necessary to treat very high levels of triglycerides. If your doctor prescribes medication to lower your triglycerides, take the medication as prescribed. And remember the significance of the healthy lifestyle changes you’ve made. Medications can help — but lifestyle matters, too.
Figure 1. Triglyceride
Figure 2. Triglyceride (TG) lipoprotein metabolism
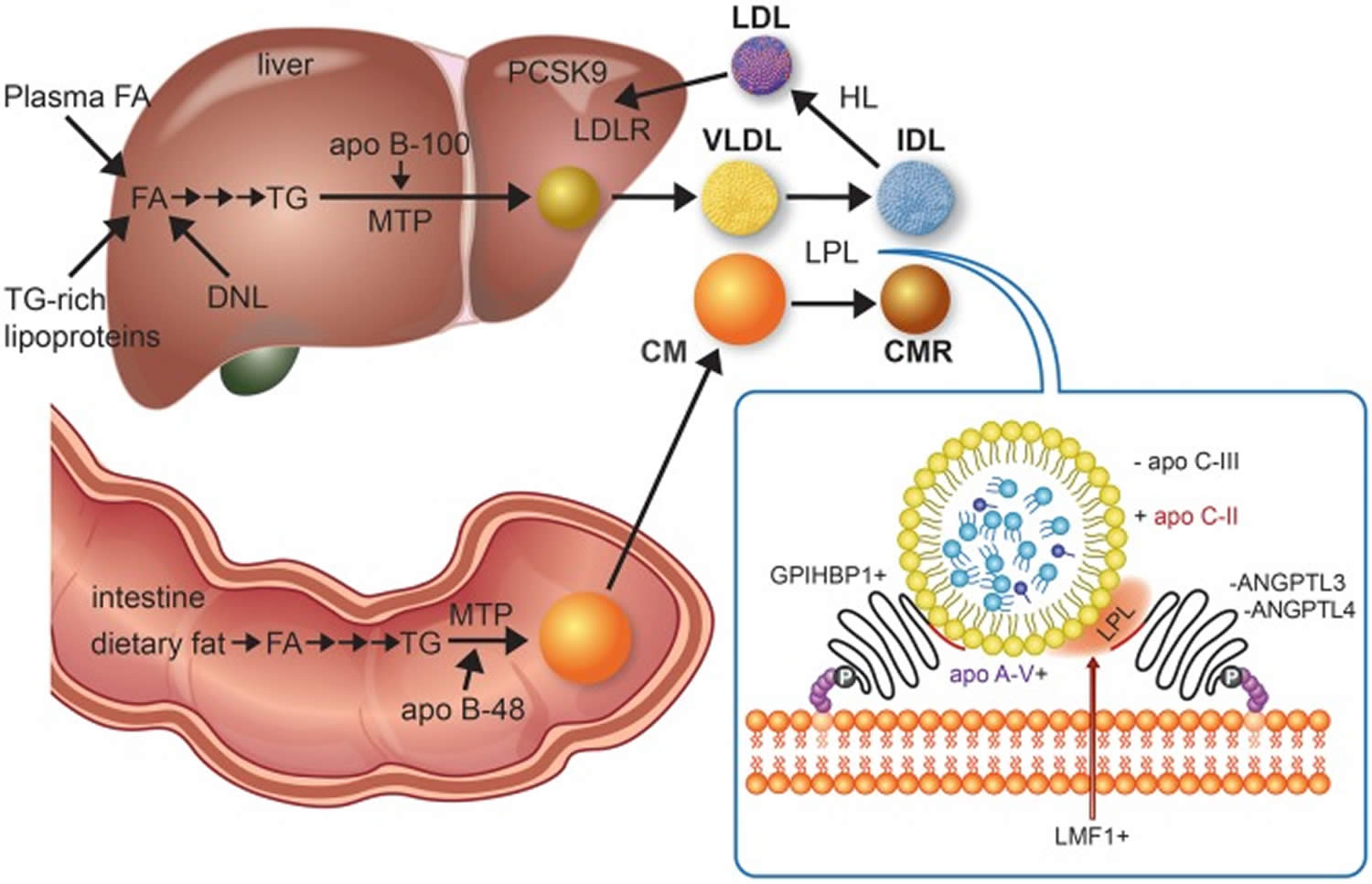
Footnotes: Triglyceride-rich lipoprotein assembly begins with triglyceride synthesis, which derive from fatty acids in the intestine from the diet or in the liver taken up from plasma, fatty acids released from lysosomes after breakdown of endocytosed triglyceride-rich lipoproteins, and fatty acids generated from glucose by de novo lipogenesis. A series of enzymes, culminating in tissue-specific isoforms of diacylglycerol acyltransferase in intestine and liver, produce triglyceride. Microsomal triglyceride transfer protein unites triglyceride, cholesterol, and phospholipids, with tissue-specific isoforms of apolipoprotein (apo) B, i.e. small B-48, shortened as a result of RNA editing in enterocytes and full-length B-100 in hepatocytes, forming chylomicrons and very-low-density lipoprotein, respectively. Chylomicrons formation also requires Sar1 homolog B GTPase (SAR1B gene product, not shown). Chylomicrons enter plasma indirectly through lymphatics while very-low-density lipoprotein is secreted directly into the circulation. Hydrolysis of circulating chylomicrons and very-low-density lipoprotein by lipoprotein lipase releases free fatty acids and produce chylomicron remnant clearance and intermediate-density lipoprotein particles, respectively. Chylomicrons remnant clearance by the liver (not shown) requires apo E, as apo B-48 does not have the low-density lipoprotein receptor binding domain. Intermediate-density lipoprotein can also be removed by the liver (not shown) with apo B-100 and apo E both acting as ligands for the low-density lipoprotein receptor. Intermediate-density lipoprotein can be further lipolyzed by lipoprotein lipase and also remodelled by hepatic lipase to generate low-density lipoprotein, which is cleared by the low-density lipoprotein receptor, whose activity is reduced by proprotein convertase subtilisin kexin 9. The inset depicts lipoprotein lipase activity on a triglyceride-rich lipoprotein particle as well as several interacting proteins at the endothelial surface that affect lipoprotein lipase activity. A plus sign indicates enhancement or stimulation of lipolysis, whereas a minus sign indicates inhibition. Lipase maturation factor 1 (LMF1) is a chaperone protein that ensures that lipoprotein lipase attains functionality and is properly secreted from adipose cells or myocytes. Glycosylphosphatidylinositol-anchored high-density lipoprotein binding protein-1 (GPIHBP1) is necessary for transcytosis of lipoprotein lipase across the endothelium of capillaries in adipose and muscle tissues as well as tethering lipoprotein lipase to the endothelium, thereby stabilizing it. Apo C-II activates lipoprotein lipase, while apo A-V is a stabilizing cofactor. Lipolysis is reduced by apo C-III, which is a component of triglyceride-rich lipoproteins, and by angiopoietin-like proteins 3 and 4 (ANGPTL3 and ANGPTL4), which both operate near the endothelium. Volanesorsen and AKCEA-APOCIII-LRx reduce triglyceride by targeting apo C-III, while evinacumab and IONIS-ANGPTL3-LRx lower triglyceride by targeting ANGPTL3. Peroxisome proliferator-activated receptors (not shown), particularly alpha and delta types, form a regulatory network that influences several of the above target molecules.
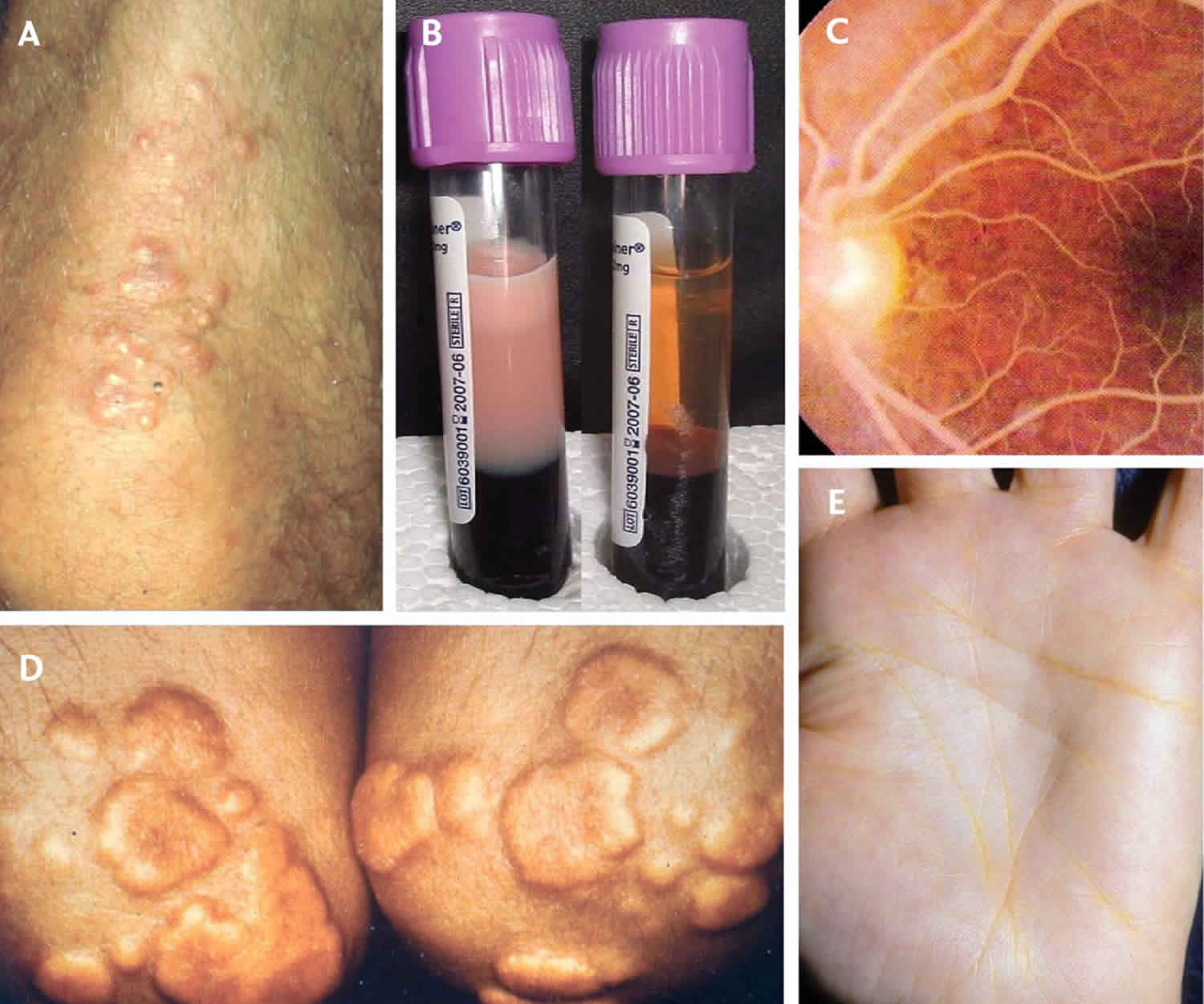
[Source 24 ]Figure 3. Eruptive xanthomas

Footnote: Eruptive xanthomas associated with hypertriglyceridemia and new-onset type 2 diabetes. (Panels A and B) A previously healthy, 38-year-old man with a family history of early cerebrovascular accidents presented with a sudden eruption of pink papules with creamy-colored centers on his arms and upper torso. He was otherwise asymptomatic and had no abdominal pain. The results of laboratory tests performed while the patient was fasting included a total cholesterol level of 1268 mg per deciliter (32.8 mmol per liter), a total triglyceride level of 8869 mg per deciliter (100.1 mmol per liter), a glucose level of 241 mg per deciliter (13.4 mmol per liter), and a glycosylated hemoglobin value of 13.4 percent. Triglyceride-lowering therapy with gemfibrozil was initiated to enhance lipoprotein lipase activity, and insulin therapy was initiated to treat the hyperglycemia. Twenty-four hours later, his total triglyceride level was 6466 mg per deciliter (73.0 mmol per liter). At follow-up visits three and five months later, the patient’s eruptive xanthomas had decreased in size and number. After eight months of treatment with gemfibrozil, glyburide, and glucophage, his total cholesterol level was 218 mg per deciliter (5.6 mmol per liter), his total triglyceride level was 302 mg per deciliter (3.4 mmol per liter), and his glycosylated hemoglobin value was 8.3 percent; the eruptive xanthomas had completely resolved.
[Source 32 ]Figure 4. Hypertriglyceridemia diagnostic and treatment algorithm
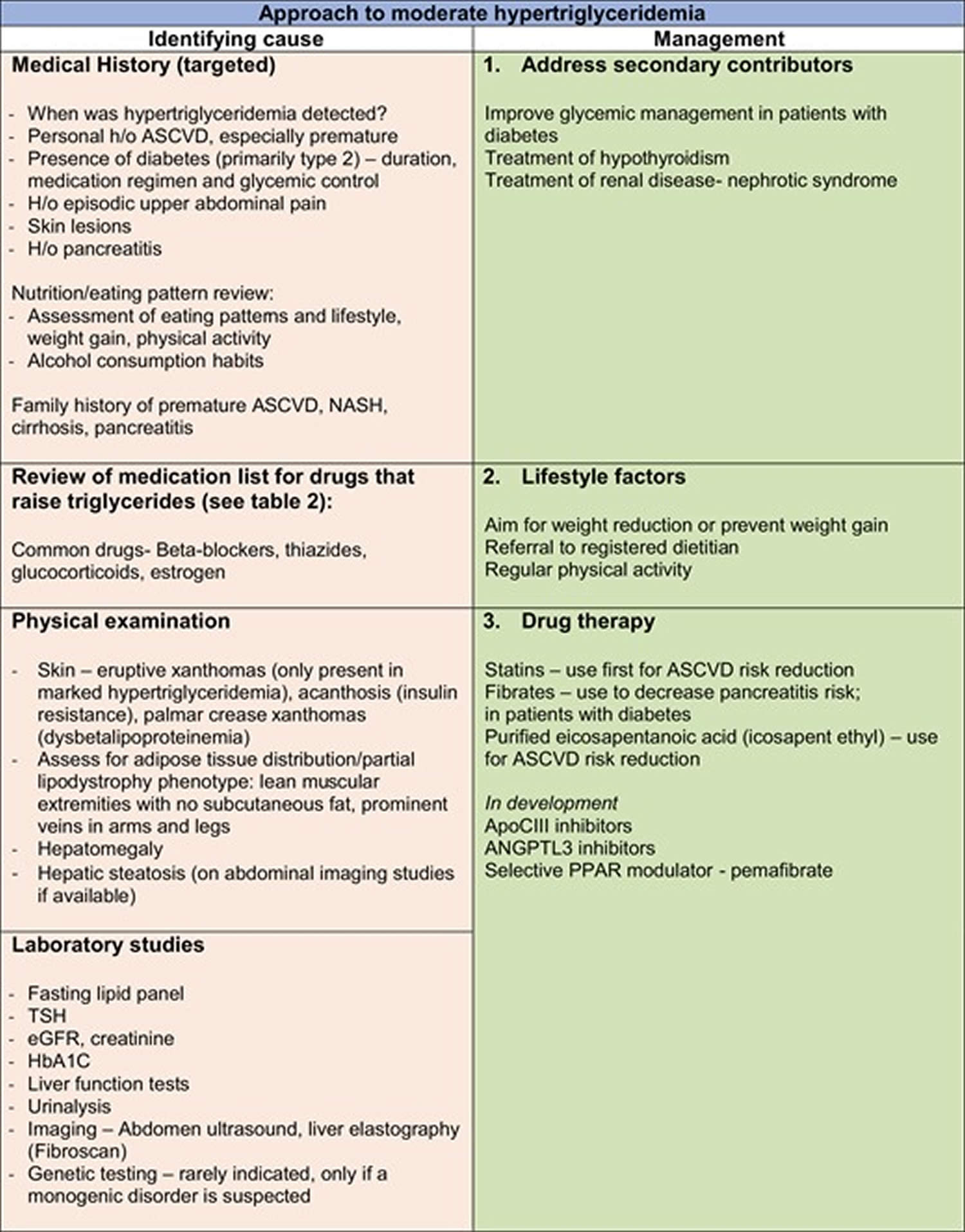
Table 1. Hypertriglyceridemia definition
| Guideline | Classification | Triglyceride Levels |
|---|---|---|
| National Cholesterol Education Program Adult Treatment Panel (NCEP/ ATP III) 33 American Heart Association 34 National Lipid Association 35 |
|
|
| The Endocrine Society 20 |
|
|
| European Society of Cardiology/European Atherosclerosis Society 36 |
|
|
| Hegele et al 19 |
|
|
What’s the difference between triglycerides and cholesterol?
Triglycerides and cholesterol are different types of lipids that circulate in your blood:
- Triglycerides store unused calories and provide your body with energy.
- Cholesterol is used to build cells and certain hormones.
Familial hypertriglyceridemia types
Fredrickson, Levy and Lees classification of lipoprotein disorders identified 5 primary lipoprotein phenotypes (type I to V) based on the lipoprotein patterns on paper electrophoresis and characterized by the presence of hypercholesterolemia and/or hypertriglyceridemia 37, 38, 39, 40 and this classification system was formally adopted by the World Health Organization (WHO) in 1970 41.
Genetic or monogenic hypertriglyceridemia was classified as type 1, and multifactorial hypertriglyceridemia was referred to as type 5 38, 22. This classification does not identify the actual cause or diagnosis of the underlying lipid disorder and has been replaced by categorization based on pathophysiology and/or genetic cause 42. A new algorithm for classification using only the plasma triglycerides and non-HDL-C levels (calculated as total cholesterol minus HDL) has been recently described for identifying dyslipidemias arising from altered apolipoprotein (apo) B metabolism looks promising but will need further validation before widely embraced 43. A comparison of the Fredrickson classification of hyperlipidemias and current terminology is shown in Table 2 below.
Table 2. Hypertriglyceridemia types (Fredrickson’s classification of dyslipidemias and modern classification)
| Fredrickson phenotype | Previous label | Lipoprotein abnormality | Lipid levels | Recommended modern classification |
|---|---|---|---|---|
| I | Primary hyperchylomicronemia | Chylomicrons | ↑↑↑ triglyceride | Monogenic hypertriglyceridemia or Familial chylomicronemia syndrome |
| IIa | Familial hypercholesterolemia | Low-density lipoprotein (LDL) | ↑ total cholesterol Normal triglyceride | Familial hypercholesterolemia, polygenic hypercholesterolemia |
| IIb | Familial combined hyperlipidemia | Very low-density lipoprotein (VLDL) | ↑↑ triglycerides | Polygenic hypertriglyceridemia |
| III | Familial dysbetalipoproteinemia | Remnants of chylomicron and very low-density lipoprotein (VLDL) | ↑-↑↑total cholesterol ↑-↑↑ triglycerides | Familial dysbetalipoproteinemia |
| IV | Familial hypertriglyceridemia | Very low-density lipoprotein (VLDL) | ↑↑ triglycerides | Polygenic hypertriglyceridemia |
| V | Endogenous hypertriglyceridemia | Chylomicron and very low-density lipoprotein (VLDL) | ↑↑↑triglycerides | Multifactorial chylomicronemia syndrome (due to polygenic hypertriglyceridemia) |
Familial hypertriglyceridemia cause
Familial hypertriglyceridemia is most likely caused by genetic defects combined with environmental factors 9, 10, 4, 5. Familial hypertriglyceridemia is commonly associated with an autosomal dominant inheritance with most cases having a multigenic or polygenic inheritance or the result of many genetic factors 3, 44, 45. A common mutation implicated in the development of familial hypertriglyceridemia is a heterozygous inactivating mutation of the lipoprotein lipase (LPL) gene 2. The LPL gene provides instructions for making an enzyme called lipoprotein lipase 46. The lipoprotein lipase (LPL) enzyme is found primarily on the surface of cells that line tiny blood vessels (capillaries) within muscles and in fatty (adipose) tissue. Lipoprotein lipase (LPL) plays a critical role in breaking down fat in the form of triglycerides, which are carried from various organs to the blood by molecules called lipoproteins.
Lipoprotein lipase breaks down triglycerides carried by two different types of lipoproteins, which bring fat to the bloodstream from different organs. Fat from the intestine, which is taken in from the diet, is transported to the bloodstream by lipoproteins called chylomicrons. Another type of lipoprotein called very low density lipoprotein (VLDL) carries triglycerides from the liver to the bloodstream. When lipoprotein lipase breaks down triglycerides, the fat molecules are used by the body as energy or stored in fatty tissue for later use.
Inactivation of the LPL gene creates an inability to hydrolyze the triglycerides within the VLDL core 47. This creates an overall build-up of triglycerides and very low density lipoprotein (VLDL), contributing to pathology.
The main pathophysiological mechanism of hypertriglyceridemia in familial hypertriglyceridemia appears to be abnormal VLDL composition without alteration in VLDL particle number 29. As a result, plasma apo B levels in familial hypertriglyceridemia subjects are normal or low. High triglyceride levels in familial hypertriglyceridemia subjects are not determined by hepatic VLDL-apo B overproduction, it is likely to be a result of decreased triglyceride clearance 29.
More than 220 mutations in the LPL gene have been found to cause familial lipoprotein lipase deficiency 46. This condition disrupts the normal breakdown of triglycerides in the body, resulting in an increase of these fats. The most common mutation in people of European ancestry replaces the protein building block (amino acid) glycine with the amino acid glutamic acid at position 188 in the enzyme (written as Gly188Glu or G188E). Mutations that cause familial lipoprotein lipase deficiency reduce or eliminate lipoprotein lipase activity, which prevents the enzyme from effectively breaking down triglycerides in the bloodstream. As a result, triglycerides attached to lipoproteins accumulate in the blood and tissues, leading to inflammation of the pancreas (pancreatitis), enlarged liver and spleen (hepatosplenomegaly), fatty deposits in the skin (eruptive xanthomas), and the other signs and symptoms of familial lipoprotein lipase deficiency.
Insulin is also a potent activator of lipoprotein lipase in fatty (adipose) tissue. Therefore, insulin resistance can decrease lipoprotein lipase (LPL) activity and ultimately contribute more to hypertriglyceridemia, helping push the amount to a pathologic level 48.
How severe familial hypertriglyceridemia is can vary based on sex, age, hormone use, and dietary factors.
Secondary causes of hypertriglyceridemia 24:
- Diet with high positive energy-intake balance and high fat or high glycemic index (high GI)
- Increased alcohol consumption (hypertriglyceridemia risk increases with > 2 and > 1 drink(s) per day in men and women, respectively)
- Obesity
- Metabolic syndrome
- Insulin resistance
- Diabetes mellitus (predominantly type 2 diabetes)
- Hypothyroidism (underactive thyroid)
- Kidney disease (proteinuria, uremia, or glomerulonephritis)
- Pregnancy (particularly in the third trimester)
- Paraproteinemia
- Systemic lupus erythematosus (SLE)
- Medications, including corticosteroids, oral oestrogen, tamoxifen, thiazides, non-cardioselective beta-blockers and bile acid sequestrants, cyclophosphamide, L-asparaginase, protease inhibitors, and second-generation antipsychotic agents (such as clozapine and olanzapine)
Familial hypertriglyceridemia inheritance
Familial hypertriglyceridemia may follow an autosomal dominant monogenic inheritance with variable penetrance; however, the genes involved in familial hypertriglyceridemia are still largely unknown 4. The frequency of heterozygous carriers of various pathologic mutations in the LPL gene range from 0.06% to 20% while noting different mutations carry different degrees of pathology 49. Due to the complexity of these disorders and the absence of a single gene defect, there is no role for routine genetic testing at this time 22.
Familial hypertriglyceridemia symptoms
Patients with familial hypertriglyceridemia will typically have no symptoms, however they may have elevated cardiovascular disease risk like coronary heart disease and stroke and frequently have other comorbidities such as obesity, metabolic syndrome, and type 2 diabetes 50, 51.
- Borderline high and high blood triglycerides, levels measured without fasting and that stay higher than 175 mg/dL for a long time, can raise the risk for heart complications.
- Very high blood triglycerides, more than 500 mg/dL, can raise the risk for a sudden swelling in the pancreas called acute pancreatitis.
- Very high blood triglycerides levels can also lead to changes in the eye’s blood vessels that make the vessels look different than usual. This condition is called lipemia retinalis.
- Finally, people with very high levels of blood triglycerides may also have damaged skin on their back, chest, arms, and legs.
In hereditary lipid disorders, a patient may present with the variants of cutaneous xanthoma. A xanthoma is a collection of macrophages that are “lipid-laden”. These macrophages have accumulated excessive amounts of free lipids and become coined “foam cells”. More commonly, the eruptive xanthoma variant can be indicative of hypertriglyceridemia. However, it should be noted that triglyceride levels necessary to present with these lesions are well above the typical blood levels of familial hypertriglyceridemia patients. The formation of eruptive xanthomas is commonly less than 5 mm and in a crop formation on the extensor surfaces 32.
Extremely high blood triglyceride levels, greater than 1,500 mg/dL, may cause the body to stop breaking down fats, which is called multifactorial chylomicronemia syndrome. Symptoms include short-term memory loss, swelling of the liver and spleen, stomach pain, and reddening or flushing of the skin with alcohol use.
Familial hypertriglyceridemia complications
Hypertriglyceridemia is responsible for a mild amount of acute pancreatitis. There is a direct correlation with increased risk of pancreatitis as triglyceride levels rise above 500 mg/dL. When values rise above 1000 mg/dL, there is a described 5% risk of pancreatitis that then doubles when values reach more than 2000 mg/dL. Acute pancreatitis treatment includes IV fluid resuscitation and pain control. Treatment of hypertriglyceridemia-induced acute pancreatitis includes standard acute pancreatitis treatment, insulin to reduce triglyceride load, and possibly total plasma exchange 52. Total plasma exchange is indicated initially in settings of severe pancreatitis, which can be determined by clinical evidence of hypocalcemia and lactic acidosis 53. The mechanism relies on the rapid correction of hypertriglyceridemia as well as the successful reduction of inflammatory cytokines. Recent clinical data affirms this treatment as a safe approach in severe hypertriglyceridemia-induced acute pancreatitis cases; unfortunately, a difficult prediction of therapy success may require multiple rounds of treatment 54. Additionally, there is evidence suggesting a relationship between elevated triglycerides with respect to cardiovascular disease, through increased atherosclerotic burden. While a causal relationship has not yet been established, evidence suggests that states of increased triglyceride levels are linked to an increased incidence of coronary heart disease 55. Ruling out secondary causes is essential for these risk factors may also cause an increase in accelerating cardiovascular disease.
Familial hypertriglyceridemia diagnosis
Your doctor will perform a physical exam and ask about your family history and symptoms. If you have a family history of hypertriglyceridemia, you should have blood tests to check very low density lipoprotein (VLDL) and triglyceride levels. You may be asked to fast, or not eat, for 9 to 12 hours before your blood is tested. In addition, alcohol should not be consumed for 24 hours just before the test.
A blood test to check cholesterol levels called a lipid panel or lipid profile typically reports:
- Total cholesterol
- LDL cholesterol
- HDL cholesterol
- Triglycerides
Blood tests most often show a mild to moderate increase in triglycerides (about 200 to 500 mg/dL).
Triglyceride levels usually fall into the following categories 20:
- Healthy: Triglyceride below 150 milligrams per deciliter (mg/dL) for adults; lower than 90 mg/dL for children and teens (ages 10-19)
- Mild hypertriglyceridemia: Triglyceride between 150 and 199 mg/dL
- Moderate hypertriglyceridemia: Triglyceride 200 and 999 mg/dL
- Severe hypertriglyceridemia: Triglyceride 1000 and 1999 mg/dL
- Very severe hypertriglyceridemia: Triglyceride greater than 2000 mg/dL
Your doctor may diagnose you with high blood triglycerides if your fasting blood triglyceride levels are regularly 150 milligrams mg/dL or higher.
Due to the complexity of hypertriglyceridemia and the absence of a single gene defect (ie, no single gene defect is identifiable), there is no role for routine genetic testing at this time 22. Diagnosis of familial hypertriglyceridemia is confirmed when the an individual who is affected by hypertriglyceridemia and one or more of their family members show a similar lipid pattern 56, 57.
Evaluation of hypertriglyceridemia does not stop at the level of a lipid panel. Your doctor must also check and monitor you for other comorbidities development that may augment disease progression. Initially, body-mass-index (BMI) need to be measured as it is an important link to other disease processes like increased insulin resistance, cardiovascular disease, and overall morbidity. Furthermore, the clinical exam can often become the first clue in comorbidity development or increased progression of the hypertriglyceridemia disease state. A common sign of severe triglyceride elevation can often be xanthoma formation on skin exams (see Figure 3 above).
Patients with hypertriglyceridemia commonly can develop comorbid insulin resistance and further progress to type 2 diabetes 58. Therefore, screening appropriately with a hemoglobin A1c (HbA1c) level as well as random blood glucose finger prick testing is necessary for patients with hypertriglyceridemia. Furthermore, insulin resistance can lead to subsequent development of elevated lipid levels 48.
If the diagnosis of hypertriglyceridemia is made, monitoring of cardiovascular risk factors is important due to the increased risk of developing heart disease 55. Initially, blood pressure must be controlled to limit this risk. The physical exam will serve to alert in the setting of increased disease progression. Auscultation of carotids for bruits and heart sounds can provide clues and set baselines as patients become monitored over time. Routine ECGs will help preserve a baseline for comparison if there becomes an incident of heart attack (acute myocardial infarction).
When suspecting elevated triglyceride levels, consideration of other factors can help find a secondary cause of elevated triglyceride from a primary cause of elevated triglyceride. Several drugs and substances can lead to a metabolic syndrome that can mispresent as a primary cause of elevated triglyceride. These substances include estrogen, alcohol, glucocorticoids, beta-blockers, highly active antiretroviral therapy (HAART) therapy, and others 59, 60, 61.
Familial hypertriglyceridemia treatment
Treatments for familial hypertriglyceridemia focus on reducing triglyceride levels. The goal of treatment is to control conditions that can raise your triglyceride levels, conditions such as obesity, underactive thyroid (hypothyroidism), and type 2 diabetes. Your doctor may tell you not to drink alcohol. Certain birth control pills can raise triglyceride levels. Talk to your doctor about your risk when deciding whether to take these medicines.
If you are diagnosed with high blood triglycerides, your doctor may recommend that you make heart-healthy lifestyle changes 20:
- Choose heart-healthy foods. Eat more high-fiber foods from plants. Choose 100% whole grains, whole fruits and vegetables.
- Get regular physical activity. Aim for at least 30 minutes of physical activity on most or all days of the week. Regular exercise can lower triglycerides and boost “good” cholesterol. Try to incorporate more physical activity into your daily tasks — for example, climb the stairs at work or take a walk during breaks.
- Lose weight. If you have mild to moderate hypertriglyceridemia, focus on cutting calories. Extra calories are converted to triglycerides and stored as fat. Reducing your calories will reduce triglycerides.
- Manage stress.
- Quit smoking.
- Get enough good quality sleep.
- Limit alcohol. Alcohol is high in calories and sugar and has a particularly potent effect on triglycerides. If your blood triglyceride levels are considered very high, your doctor may tell you not to drink alcohol.
If healthy lifestyle changes aren’t enough to control high triglycerides, your doctor might recommend a few different types of medicines to control or lower your triglyceride levels 20:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. These cholesterol-lowering medications may be recommended if you also have poor cholesterol numbers or a history of blocked arteries or diabetes. Examples of statins include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor).
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can also be used to remove triglycerides from the blood when paired with a healthy diet. Ezetimibe can be used with a statin drug. If statins don’t reduce cholesterol enough, doctors often suggest adding ezetimibe.
- Fibrates. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Fibrates have been shown to markedly reduce triglyceride levels by 50% and beyond. Drugs like fenofibrate and gemfibrozil help activate lipoprotein lipase (LPL) through PPAR-alpha leading to further breakdown of triglycerides. However, fibrates aren’t used if you have severe kidney or liver disease. Furthermore, caution must be noted during polypharmacy. A combination of fibrates with statins can increase the risk of statin side effects 29, 30. This is theorized to be a result of CYP-3A4 inhibition via fibrates. If combined therapy is required, exercise caution and consider statin therapy that is not primarily metabolized through CYP-3A4 (pravastatin) 30.
- Fish oil also known as omega-3 fatty acids. Fish oil or omega-3 fatty acid can help lower your triglycerides. Fish oil has shown a significant reduction of both VLDL and triglyceride levels 31. Triglyceride lowering by fish oil omega-3 fatty acids are mediated primarily via eicosopentanoic acid (EPA3) and docosahexaenoic acid (DHA), which result in variable, dose-dependent, and modest lowering of triglycerides through chylomicron clearance 62. To achieve triglyceride reduction of 20% to 50%, administration of 3 to 4 g/day of omega-3 fish oil is required. Omega-3 preparations are available by prescription and readily available as over-the-counter (OTC) supplements with variable quantities/purity of EPA and DHA. A generic version of purified EPA alone is also available. Both prescription and OTC supplements can lower triglycerides. Prescription fish oil preparations such as Lovaza, contain more-active omega-3 fatty acids than many nonprescription supplements. Fish oil taken at high levels can interfere with blood clotting and cause gastrointestinal symptoms, so talk to your doctor before taking any supplements.
- Niacin also called nicotinic acid or vitamin B3. Niacin can lower your triglycerides and low-density lipoprotein (LDL) cholesterol the “bad” cholesterol. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. Niacin (nicotinic acid) can decrease plasma triglycerides by up to 40% 63. Niacin decreases adipose tissue lipolysis and free fatty acid delivery to the liver with resultant reduced hepatic VLDL synthesis. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins. Talk to your doctor before taking over-the-counter niacin because it can interact with other medications and cause significant side effects.
More than one medicine may be necessary to treat very high levels of triglycerides. If your doctor prescribes medication to lower your triglycerides, take the medication as prescribed. And remember the significance of the healthy lifestyle changes you’ve made. Medications can help — but lifestyle matters, too.
Familial hypertriglyceridemia medications
Currently available triglyceride-lowering therapies include fibrates, omega-3 fatty acids and niacin can reduce levels up to 45% 22. Primary cholesterol lowering therapies such as statins, ezetimibe, and PCSK9 inhibitors also modestly improve triglyceride levels (averaging 5-25%) 22.
Table 3. Familial hypertriglyceridemia medications
| Fibrates | Omega 3 fish oil |
|---|---|
| Gemfibrozil Doses: 300 mg, 600 mg taken twice daily | Omega -3 fatty acids (Epanova) 850 mg polyunsaturated fatty acids, including eicosapentanoic acid (EPA) and docosahexanoic acid (DHA) |
| Fenofibrate Micronizeda 43, 130 mg or 67, 134, 200 mg | Omega 3 ethyl esters (Lovaza, Omacor) 375 mg DHA and 465 mg EPA |
| Bezafibrate (not available in the United States) 200 mg twice daily or 400 mg extended release once daily | Icosapent ethyl (Vascepa) EPA only—0.5 or 1 g |
Triglyceride lowering for atherosclerotic cardiovascular disease risk reduction
In patients without preexisting atherosclerotic cardiovascular disease, mild to moderate hypertriglyceridemia does increase cardiovascular risk; often a strong family history of premature or early atherosclerotic cardiovascular disease can be discovered suggesting polygenic influence. Therefore, in addition to lifestyle measures, statins are the first line of therapy in patients with and without hypertriglyceridemia. Purified icosapent ethyl (IPE) [trade name: Vascepa] can be added in patients with known atherosclerotic cardiovascular disease or diabetes with 2 or more risk factors. There is lack of clear evidence of addition of fibrates to statins for atherosclerotic cardiovascular disease risk reduction. However, in patients with persistent hypertriglyceridemia (especially for triglycerides > 500 mg/dL) despite lifestyle adjustments and maximized statin therapy, it is reasonable to add fibrates to lower potential risk of pancreatitis 64.
Triglyceride lowering for pancreatitis risk reduction
Fibrates are first-line therapy in combination with healthy lifestyle changes in patients with triglycerides > 1000 mg/dL to decrease risk of pancreatitis and should be considered if triglycerides are in the moderate to severe range of 500 to 999 mg/dL. There is no clinical trial evidence of benefit of omega-3 fish oil on pancreatitis risk reduction. Statin therapy can be added to fibrate therapy if there is persistent cholesterol elevation without increase in rhabdomyolysis risk 65.
Familial hypertriglyceridemia diet
What you eat and drink affects your triglyceride and cholesterol levels. No randomized clinical trial evidence for any specific dietary recommendations for mild to moderate triglyceride exists. The key principle of making changes to eating patterns is to reduce net caloric intake. Replacing refined carbohydrates with complex carbohydrates, limiting dietary saturated fat, avoiding trans fats, and inclusion of mono- or polyunsaturated fats are reasonable approaches 66. Intermittent fasting may decrease triglycerides more than standard hypocaloric diets, but evidence is inconsistent in studies 67, 68. Very low carbohydrate or ketogenic diets also appear to consistently lower triglycerides in patients with mild to moderate hypertriglyceridemia 69; additionally, in some individuals who follow such eating patterns, marked LDL cholesterol elevations can occur 22. In the online “ketogenic world” these individuals are referred to as “lean-mass hyper-responders” 70. Such responses may be related to the higher fat (especially saturated fat) consumption and resultant downregulation of cell surface LDL receptors. Such diets are hard to maintain and cannot be recommended especially in patients with moderate hypertriglyceridemia who have strong history of atherosclerotic cardiovascular disease 71 or in patients with predisposition to marked hypertriglyceridemia with pancreatitis 69.
If you have high triglyceride levels, your doctor may recommend following a heart healthy diet. A heart-healthy diet focuses on plant-based foods, including fruits, vegetables and whole grains while limiting saturated fats, trans fats, salt and sugar. Saturated fats such as those in meat, butter, cheese and other full-fat dairy products can raise your total cholesterol. Decreasing your consumption of saturated fats to less than 7% of your total daily calorie intake can reduce your LDL cholesterol by 8% to 10%. Trans fats sometimes listed on food labels as “partially hydrogenated vegetable oil”, are often used in margarines and store-bought cookies, crackers and cakes. Trans fats raise overall cholesterol levels. The Food and Drug Administration (FDA) banned the use of partially hydrogenated vegetable oils in processed foods sold after January 1, 2020.
Oatmeal, oat bran and high-fiber foods
Oatmeal has soluble fiber, which reduces your low-density lipoprotein (LDL) cholesterol, the “bad” cholesterol. Soluble fiber is also found in such foods as kidney beans, Brussels sprouts, apples and pears. Soluble fiber can reduce the absorption of cholesterol into your bloodstream. Five to 10 grams or more of soluble fiber a day decreases your LDL cholesterol.
One serving of a breakfast cereal with oatmeal or oat bran provides 3 to 4 grams of fiber. If you add fruit, such as a banana or berries, you’ll get even more fiber.
Fish and omega-3 fatty acids
Fatty fish has high levels of omega-3 fatty acids, which can reduce your triglycerides — a type of fat found in blood. These acids also may help lower your blood pressure and risk of developing blood clots. In people who have already had heart attacks, omega-3 fatty acids may reduce the risk of sudden death.
Omega-3 fatty acids don’t affect LDL cholesterol levels but may help lower triglycerides and increase HDL, the good cholesterol. But because of omega-3 fatty acids’ other heart benefits, the American Heart Association recommends eating at least two servings of fish a week. Baking or grilling the fish avoids adding unhealthy fats.
The highest levels of omega-3 fatty acids are in:
- Mackerel
- Herring
- Tuna
- Salmon
- Trout
Foods such as walnuts, flaxseed and canola oil also have small amounts of omega-3 fatty acids.
Omega-3 and fish oil supplements are available. Talk to your doctor before taking any supplements.
Almonds and other nuts
Almonds and other tree nuts can improve blood cholesterol. Studies have shown that walnuts, which have omega-3 fats, may help protect the heart and lower the risk of heart attack for people who already have heart disease. All nuts are high in calories, so a handful added to a salad or eaten as a snack will do.
Avocados
Avocados are a good source of nutrients as well as monounsaturated fatty acids (MUFAs). Research suggests that the fiber from avocados can improve HDL cholesterol levels and the quality of LDL cholesterol. Adding two servings of avocado per week to a heart-healthy diet can lower your risk of heart disease.
People tend to think of avocados in guacamole, which often is eaten with high-fat corn chips. Try adding avocado slices to salads and sandwiches or eating them as a side dish. Also try guacamole with raw cut vegetables, such as cucumber slices.
Replacing saturated fats, such as those found in meats, with monounsaturated fatty acids (MUFAs) are part of what makes the Mediterranean diet heart healthy.
Foods with added plant sterols or stanols
Sterols and stanols are substances found in plants that help block the absorption of cholesterol. Foods that have been fortified with sterols or stanols are available.
Margarines and orange juice with added plant sterols can help lower LDL cholesterol. Adding 2 grams of sterol to your diet every day can lower your LDL cholesterol by 5% to 15%.
It’s not clear whether food with plant sterols or stanols lowers your risk of heart attack or stroke — although experts assume that foods that lower cholesterol do cut the risk. Plant sterols or stanols don’t appear to affect levels of triglycerides or of high-density lipoprotein (HDL) cholesterol, the “good” cholesterol.
Whey protein
Whey protein, which is found in dairy products, may account for many of the health benefits attributed to dairy. Studies have shown that whey protein given as a supplement lowers both LDL and total cholesterol as well as blood pressure. You can find whey protein powders in health food stores and some grocery stores.
Olive oil
Try using olive oil in place of other fats in your diet. You can saute vegetables in olive oil, add it to a marinade or mix it with vinegar as a salad dressing. You can also use olive oil as a substitute for butter when basting meat or as a dip for bread. Extra virgin olive oil also reduces the risk of heart attacks.
Familial hypertriglyceridemia prognosis
When managed, patients with familial hypertriglyceridemia have a good prognosis 2. Commonly, patients with familial hypertriglyceridemia do not have severe elevations of triglycerides and VLDL. However, secondary causes of an elevated lipid profile often coincide. Management of these secondary factors is the best prognostic factor for patient longevity.
- Cox RA, García-Palmieri MR. Cholesterol, Triglycerides, and Associated Lipoproteins. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 31. Available from: https://www.ncbi.nlm.nih.gov/books/NBK351[↩][↩]
- Goyal A, Cusick AS, Reilly E. Familial Hypertriglyceridemia. [Updated 2023 Jan 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556024[↩][↩][↩]
- Hegele RA, Ban MR, Hsueh N, Kennedy BA, Cao H, Zou GY, Anand S, Yusuf S, Huff MW, Wang J. A polygenic basis for four classical Fredrickson hyperlipoproteinemia phenotypes that are characterized by hypertriglyceridemia. Hum Mol Genet. 2009 Nov 1;18(21):4189-94. doi: 10.1093/hmg/ddp361[↩][↩]
- Cruz-Bautista, I., Huerta-Chagoya, A., Moreno-Macías, H. et al. Familial hypertriglyceridemia: an entity with distinguishable features from other causes of hypertriglyceridemia. Lipids Health Dis 20, 14 (2021). https://doi.org/10.1186/s12944-021-01436-6[↩][↩][↩]
- Austin MA, Edwards KL, Monks SA, Koprowicz KM, Brunzell JD, Motulsky AG, Mahaney MC, Hixson JE. Genome-wide scan for quantitative trait loci influencing LDL size and plasma triglyceride in familial hypertriglyceridemia. J Lipid Res. 2003 Nov;44(11):2161-8. doi: 10.1194/jlr.M300272-JLR200[↩][↩]
- Glueck CJ, Tsang R, Fallat R, Buncher CR, Evans G, Steiner P. Familial hypertriglyceridemia: studies in 130 children and 45 siblings of 36 index cases. Metabolism. 1973 Oct;22(10):1287-309. doi: 10.1016/0026-0495(73)90274-6[↩][↩]
- Stefanutti C, Labbadia G, Morozzi C. Severe hypertriglyceridemia-related acute pancreatitis: myth or reality? Ther Apher Dial. 2013 Aug;17(4):464-5. doi: 10.1111/1744-9987.12063[↩]
- Chylomicronemia syndrome. https://medlineplus.gov/ency/article/000405.htm[↩]
- Goldstein JL, Schrott HG, Hazzard WR, Bierman EL, Motulsky AG. Hyperlipidemia in coronary heart disease. II. Genetic analysis of lipid levels in 176 families and delineation of a new inherited disorder, combined hyperlipidemia. J Clin Invest. 1973 Jul;52(7):1544-68. doi: 10.1172/JCI107332[↩][↩]
- Nikkilä EA, Aro A. Family study of serum lipids and lipoproteins in coronary heart-disease. Lancet. 1973 May 5;1(7810):954-9. doi: 10.1016/s0140-6736(73)91598-5[↩][↩]
- Moulin P, Dufour R, Averna M, Arca M, Cefalù AB, Noto D, D’Erasmo L, Di Costanzo A, Marçais C, Alvarez-Sala Walther LA, Banach M, Borén J, Cramb R, Gouni-Berthold I, Hughes E, Johnson C, Pintó X, Reiner Ž, van Lennep JR, Soran H, Stefanutti C, Stroes E, Bruckert E. Identification and diagnosis of patients with familial chylomicronaemia syndrome (FCS): Expert panel recommendations and proposal of an “FCS score”. Atherosclerosis. 2018 Aug;275:265-272. doi: 10.1016/j.atherosclerosis.2018.06.814[↩]
- Davidson M, Stevenson M, Hsieh A, Ahmad Z, Roeters van Lennep J, Crowson C, Witztum JL. The burden of familial chylomicronemia syndrome: Results from the global IN-FOCUS study. J Clin Lipidol. 2018 Jul-Aug;12(4):898-907.e2. doi: 10.1016/j.jacl.2018.04.009[↩]
- Surendran RP, Visser ME, Heemelaar S, Wang J, Peter J, Defesche JC, Kuivenhoven JA, Hosseini M, Péterfy M, Kastelein JJ, Johansen CT, Hegele RA, Stroes ES, Dallinga-Thie GM. Mutations in LPL, APOC2, APOA5, GPIHBP1 and LMF1 in patients with severe hypertriglyceridaemia. J Intern Med. 2012 Aug;272(2):185-96. doi: 10.1111/j.1365-2796.2012.02516.x[↩]
- D’Erasmo L, Di Costanzo A, Cassandra F, Minicocci I, Polito L, Montali A, Ceci F, Arca M. Spectrum of Mutations and Long-Term Clinical Outcomes in Genetic Chylomicronemia Syndromes. Arterioscler Thromb Vasc Biol. 2019 Dec;39(12):2531-2541. doi: 10.1161/ATVBAHA.119.313401[↩]
- Serveaux Dancer M, Di Filippo M, Marmontel O, Valéro R, Piombo Rivarola MDC, Peretti N, Caussy C, Krempf M, Vergès B, Mahl M, Marçais C, Moulin P, Charrière S. New rare genetic variants of LMF1 gene identified in severe hypertriglyceridemia. J Clin Lipidol. 2018 Sep-Oct;12(5):1244-1252. doi: 10.1016/j.jacl.2018.06.018[↩]
- Cefalù AB, Spina R, Noto D, Ingrassia V, Valenti V, Giammanco A, Fayer F, Misiano G, Cocorullo G, Scrimali C, Palesano O, Altieri GI, Ganci A, Barbagallo CM, Averna MR. Identification of a novel LMF1 nonsense mutation responsible for severe hypertriglyceridemia by targeted next-generation sequencing. J Clin Lipidol. 2017 Jan-Feb;11(1):272-281.e8. doi: 10.1016/j.jacl.2017.01.003[↩]
- Wang J, Hegele RA. Homozygous missense mutation (G56R) in glycosylphosphatidylinositol-anchored high-density lipoprotein-binding protein 1 (GPI-HBP1) in two siblings with fasting chylomicronemia (MIM 144650). Lipids Health Dis. 2007 Sep 20;6:23. doi: 10.1186/1476-511X-6-23[↩]
- Alexopoulos AS, Qamar A, Hutchins K, Crowley MJ, Batch BC, Guyton JR. Triglycerides: Emerging Targets in Diabetes Care? Review of Moderate Hypertriglyceridemia in Diabetes. Curr Diab Rep. 2019 Feb 26;19(4):13. doi: 10.1007/s11892-019-1136-3[↩]
- Hegele RA, Ginsberg HN, Chapman MJ, Nordestgaard BG, Kuivenhoven JA, Averna M, Borén J, Bruckert E, Catapano AL, Descamps OS, Hovingh GK, Humphries SE, Kovanen PT, Masana L, Pajukanta P, Parhofer KG, Raal FJ, Ray KK, Santos RD, Stalenhoef AF, Stroes E, Taskinen MR, Tybjærg-Hansen A, Watts GF, Wiklund O; European Atherosclerosis Society Consensus Panel. The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management. Lancet Diabetes Endocrinol. 2014 Aug;2(8):655-66. doi: 10.1016/S2213-8587(13)70191-8[↩][↩]
- Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Sacks F, Murad MH, Stalenhoef AF; Endocrine society. Evaluation and treatment of hypertriglyceridemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012 Sep;97(9):2969-89. doi: 10.1210/jc.2011-3213. Erratum in: J Clin Endocrinol Metab. 2015 Dec;100(12):4685. doi: 10.1210/jc.2015-3649[↩][↩][↩][↩][↩][↩][↩]
- Langlois MR, Nordestgaard BG, Langsted A, et al. European Atherosclerosis Society (EAS) and the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) Joint Consensus Initiative. Quantifying atherogenic lipoproteins for lipid-lowering strategies: consensus-based recommendations from EAS and EFLM. Clin Chem Lab Med. 2020 Mar 26;58(4):496-517. doi: 10.1515/cclm-2019-1253[↩]
- Savitha Subramanian, Approach to the Patient With Moderate Hypertriglyceridemia, The Journal of Clinical Endocrinology & Metabolism, Volume 107, Issue 6, June 2022, Pages 1686–1697, https://doi.org/10.1210/clinem/dgac085[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Virani SS, Morris PB, Agarwala A, Ballantyne CM, Birtcher KK, Kris-Etherton PM, Ladden-Stirling AB, Miller M, Orringer CE, Stone NJ. 2021 ACC Expert Consensus Decision Pathway on the Management of ASCVD Risk Reduction in Patients With Persistent Hypertriglyceridemia: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2021 Aug 31;78(9):960-993. doi: 10.1016/j.jacc.2021.06.011[↩]
- Laufs U, Parhofer KG, Ginsberg HN, Hegele RA. Clinical review on triglycerides. Eur Heart J. 2020 Jan 1;41(1):99-109c. doi: 10.1093/eurheartj/ehz785[↩][↩][↩]
- Pedersen SB, Langsted A, Nordestgaard BG. Nonfasting Mild-to-Moderate Hypertriglyceridemia and Risk of Acute Pancreatitis. JAMA Intern Med. 2016 Dec 1;176(12):1834-1842. doi: 10.1001/jamainternmed.2016.6875. Erratum in: JAMA Intern Med. 2024 Apr 1;184(4):453. doi: 10.1001/jamainternmed.2024.0643[↩]
- Subramanian S. Hypertriglyceridemia: Pathophysiology, Role of Genetics, Consequences, and Treatment. [Updated 2024 Jan 8]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK326743[↩][↩][↩]
- Langlois MR, Nordestgaard BG, Langsted A, Chapman MJ, Aakre KM, Baum H, Borén J, Bruckert E, Catapano A, Cobbaert C, Collinson P, Descamps OS, Duff CJ, von Eckardstein A, Hammerer-Lercher A, Kamstrup PR, Kolovou G, Kronenberg F, Mora S, Pulkki K, Remaley AT, Rifai N, Ros E, Stankovic S, Stavljenic-Rukavina A, Sypniewska G, Watts GF, Wiklund O, Laitinen P; European Atherosclerosis Society (EAS) and the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) Joint Consensus Initiative. Quantifying atherogenic lipoproteins for lipid-lowering strategies: consensus-based recommendations from EAS and EFLM. Clin Chem Lab Med. 2020 Mar 26;58(4):496-517. doi: 10.1515/cclm-2019-1253[↩]
- Cohen JD, Cziraky MJ, Cai Q, Wallace A, Wasser T, Crouse JR, Jacobson TA. 30-year trends in serum lipids among United States adults: results from the National Health and Nutrition Examination Surveys II, III, and 1999-2006. Am J Cardiol. 2010 Oct 1;106(7):969-75. doi: 10.1016/j.amjcard.2010.05.030. Epub 2010 Aug 11. Erratum in: Am J Cardiol. 2010 Dec 15;106(12):1826.[↩]
- Brunzell JD. Clinical practice. Hypertriglyceridemia. N Engl J Med. 2007 Sep 6;357(10):1009-17. doi: 10.1056/NEJMcp070061[↩][↩][↩][↩]
- Athyros VG, Papageorgiou AA, Hatzikonstandinou HA, Didangelos TP, Carina MV, Kranitsas DF, Kontopoulos AG. Safety and efficacy of long-term statin-fibrate combinations in patients with refractory familial combined hyperlipidemia. Am J Cardiol. 1997 Sep 1;80(5):608-13. doi: 10.1016/s0002-9149(97)00430-x[↩][↩][↩][↩]
- Pradhan A, Bhandari M, Vishwakarma P, Sethi R. Triglycerides and Cardiovascular Outcomes-Can We REDUCE-IT ? Int J Angiol. 2020 Mar;29(1):2-11. doi: 10.1055/s-0040-1701639[↩][↩]
- Nayak KR, Daly RG. Images in clinical medicine. Eruptive xanthomas associated with hypertriglyceridemia and new-onset diabetes mellitus. N Engl J Med. 2004 Mar 18;350(12):1235. doi: 10.1056/NEJMicm030676[↩][↩]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001 May 16;285(19):2486-97. doi: 10.1001/jama.285.19.2486[↩]
- Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, Goldberg AC, Howard WJ, Jacobson MS, Kris-Etherton PM, Lennie TA, Levi M, Mazzone T, Pennathur S; American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011 May 24;123(20):2292-333. doi: 10.1161/CIR.0b013e3182160726[↩]
- Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, Wilson DP, Brown WV. National lipid association recommendations for patient-centered management of dyslipidemia: part 1–full report. J Clin Lipidol. 2015 Mar-Apr;9(2):129-69. doi: 10.1016/j.jacl.2015.02.003[↩]
- Authors/Task Force Members:; Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, Hoes AW, Jennings CS, Landmesser U, Pedersen TR, Reiner Ž, Riccardi G, Taskinen MR, Tokgozoglu L, Verschuren WM, Vlachopoulos C, Wood DA, Zamorano JL. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016 Oct;253:281-344. doi: 10.1016/j.atherosclerosis.2016.08.018[↩]
- Fredrickson DS. An international classification of hyperlipidemias and hyperlipoproteinemias. Ann Intern Med. 1971 Sep;75(3):471-2. doi: 10.7326/0003-4819-75-3-471[↩]
- Fredrickson DS, Levy RI, Lees RS. Fat transport in lipoproteins–an integrated approach to mechanisms and disorders. N Engl J Med. 1967 Feb 2;276(5):273-81 concl. doi: 10.1056/NEJM196702022760507[↩][↩]
- FREDRICKSON DS, LEES RS. A SYSTEM FOR PHENOTYPING HYPERLIPOPROTEINEMIA. Circulation. 1965 Mar;31:321-7. doi: 10.1161/01.cir.31.3.321[↩]
- Brahm A, Hegele RA. Hypertriglyceridemia. Nutrients. 2013 Mar 22;5(3):981-1001. doi: 10.3390/nu5030981[↩]
- Beaumont JL, Carlson LA, Cooper GR, Fejfar Z, Fredrickson DS, Strasser T. Classification of hyperlipidaemias and hyperlipoproteinaemias. Bull World Health Organ. 1970;43(6):891-915. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2427808/pdf/bullwho00210-0126.pdf[↩]
- S Wong, A Al-Sarraf, A Ignaszewski, J Frohlich. Dr D.S. Fredrickson: founding father of the field of lipidology. BCMJ 2012;45(7):336-340. https://bcmj.org/sites/default/files/public/BCMJ_54_Vol7_Fredrickson.pdf[↩]
- Sampson M, Ballout RA, Soffer D, Wolska A, Wilson S, Meeusen J, Donato LJ, Fatica E, Otvos JD, Brinton EA, Rosenson RS, Wilson P, Amar M, Shamburek R, Karathanasis SK, Remaley AT. A new phenotypic classification system for dyslipidemias based on the standard lipid panel. Lipids Health Dis. 2021 Nov 27;20(1):170. doi: 10.1186/s12944-021-01585-8[↩]
- Gill PK, Dron JS, Berberich AJ, Wang J, McIntyre AD, Cao H, Hegele RA. Combined hyperlipidemia is genetically similar to isolated hypertriglyceridemia. J Clin Lipidol. 2021 Jan-Feb;15(1):79-87. doi: 10.1016/j.jacl.2020.11.006[↩]
- Gill PK, Hegele RA. Familial combined hyperlipidemia is a polygenic trait. Curr Opin Lipidol. 2022 Apr 1;33(2):126-132. doi: 10.1097/MOL.0000000000000796[↩]
- LPL gene. https://medlineplus.gov/genetics/gene/lpl[↩][↩]
- Föger B, Ritsch A, Doblinger A, Wessels H, Patsch JR. Relationship of plasma cholesteryl ester transfer protein to HDL cholesterol. Studies in normotriglyceridemia and moderate hypertriglyceridemia. Arterioscler Thromb Vasc Biol. 1996 Dec;16(12):1430-6. doi: 10.1161/01.atv.16.12.1430[↩]
- Goldberg IJ. Lipoprotein lipase and lipolysis: central roles in lipoprotein metabolism and atherogenesis. J Lipid Res. 1996 Apr;37(4):693-707.[↩][↩]
- Laskarzewski PM, Khoury P, Kelly K, Mellies MJ, Morrison JA, Glueck CJ. Prevalence of familial hypertriglyceridemia: the Princeton School District Family Study. Prev Med. 1982 May;11(3):317-45. doi: 10.1016/0091-7435(82)90057-3[↩]
- Hegele RA, Pollex RL. Hypertriglyceridemia: phenomics and genomics. Mol Cell Biochem. 2009 Jun;326(1-2):35-43. doi: 10.1007/s11010-008-0005-1[↩]
- Yuan G, Al-Shali KZ, Hegele RA. Hypertriglyceridemia: its etiology, effects and treatment. CMAJ. 2007 Apr 10;176(8):1113-20. doi: 10.1503/cmaj.060963[↩]
- Mikhail N, Trivedi K, Page C, Wali S, Cope D. Treatment of severe hypertriglyceridemia in nondiabetic patients with insulin. Am J Emerg Med. 2005 May;23(3):415-7. doi: 10.1016/j.ajem.2005.02.036[↩]
- Ipe TS, Pham HP, Williams LA 3rd. Critical updates in the 7th edition of the American Society for Apheresis guidelines. J Clin Apher. 2018 Feb;33(1):78-94. doi: 10.1002/jca.21562[↩]
- Fei F, Boshell N, Williams LA 3rd. Predictability and efficacy of therapeutic plasma exchange for hypertriglyceridemia induced acute pancreatitis. Transfus Apher Sci. 2020 Apr;59(2):102699. doi: 10.1016/j.transci.2019.102699[↩]
- Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration; Sarwar N, Sandhu MS, Ricketts SL, Butterworth AS, Di Angelantonio E, Boekholdt SM, Ouwehand W, Watkins H, Samani NJ, Saleheen D, Lawlor D, Reilly MP, Hingorani AD, Talmud PJ, Danesh J. Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010 May 8;375(9726):1634-9. doi: 10.1016/S0140-6736(10)60545-4. Erratum in: Lancet. 2010 Jul 10;376(9735):90. Kastelein, J J [added].[↩][↩]
- Dron JS, Wang J, Cao H, McIntyre AD, Iacocca MA, Menard JR, Movsesyan I, Malloy MJ, Pullinger CR, Kane JP, Hegele RA. Severe hypertriglyceridemia is primarily polygenic. J Clin Lipidol. 2019 Jan-Feb;13(1):80-88. doi: 10.1016/j.jacl.2018.10.006[↩]
- Lewis GF, Xiao C, Hegele RA. Hypertriglyceridemia in the genomic era: a new paradigm. Endocr Rev. 2015 Feb;36(1):131-47. doi: 10.1210/er.2014-1062[↩]
- Smellie WS. Hypertriglyceridaemia in diabetes. BMJ. 2006 Dec 16;333(7581):1257-60. doi: 10.1136/bmj.39043.398738.DE[↩]
- Aljenedil S, Hegele RA, Genest J, Awan Z. Estrogen-associated severe hypertriglyceridemia with pancreatitis. J Clin Lipidol. 2017 Jan-Feb;11(1):297-300. doi: 10.1016/j.jacl.2016.12.006[↩]
- Kim Y, Miller M. Marked hypertriglyceridemia in a woman receiving metoprolol succinate. J Clin Lipidol. 2014 Nov-Dec;8(6):640-643. doi: 10.1016/j.jacl.2014.07.009[↩]
- Feeney ER, Mallon PW. HIV and HAART-Associated Dyslipidemia. Open Cardiovasc Med J. 2011;5:49-63. doi: 10.2174/1874192401105010049[↩]
- Park Y, Harris WS. Omega-3 fatty acid supplementation accelerates chylomicron triglyceride clearance. J Lipid Res. 2003 Mar;44(3):455-63. doi: 10.1194/jlr.M200282-JLR200[↩]
- Kamanna VS, Kashyap ML. Mechanism of action of niacin. Am J Cardiol. 2008 Apr 17;101(8A):20B-26B. doi: 10.1016/j.amjcard.2008.02.029[↩]
- Newman CB, Blaha MJ, Boord JB, Cariou B, Chait A, Fein HG, Ginsberg HN, Goldberg IJ, Murad MH, Subramanian S, Tannock LR. Lipid Management in Patients with Endocrine Disorders: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2020 Dec 1;105(12):dgaa674. doi: 10.1210/clinem/dgaa674. Erratum in: J Clin Endocrinol Metab. 2021 May 13;106(6):e2465. doi: 10.1210/clinem/dgab175[↩]
- Geng Q, Ren J, Chen H, Lee C, Liang W. Adverse events following statin-fenofibrate therapy versus statin alone: a meta-analysis of randomized controlled trials. Clin Exp Pharmacol Physiol. 2013 Mar;40(3):219-26. doi: 10.1111/1440-1681.12053[↩]
- De Natale C, Annuzzi G, Bozzetto L, Mazzarella R, Costabile G, Ciano O, Riccardi G, Rivellese AA. Effects of a plant-based high-carbohydrate/high-fiber diet versus high-monounsaturated fat/low-carbohydrate diet on postprandial lipids in type 2 diabetic patients. Diabetes Care. 2009 Dec;32(12):2168-73. doi: 10.2337/dc09-0266[↩]
- Meng H, Zhu L, Kord-Varkaneh H, O Santos H, Tinsley GM, Fu P. Effects of intermittent fasting and energy-restricted diets on lipid profile: A systematic review and meta-analysis. Nutrition. 2020 Sep;77:110801. doi: 10.1016/j.nut.2020.110801[↩]
- Yang F, Liu C, Liu X, Pan X, Li X, Tian L, Sun J, Yang S, Zhao R, An N, Yang X, Gao Y, Xing Y. Effect of Epidemic Intermittent Fasting on Cardiometabolic Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Nutr. 2021 Oct 18;8:669325. doi: 10.3389/fnut.2021.669325[↩]
- Kirkpatrick CF, Bolick JP, Kris-Etherton PM, Sikand G, Aspry KE, Soffer DE, Willard KE, Maki KC. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J Clin Lipidol. 2019 Sep-Oct;13(5):689-711.e1. doi: 10.1016/j.jacl.2019.08.003[↩][↩]
- Goldberg IJ, Ibrahim N, Bredefeld C, Foo S, Lim V, Gutman D, Huggins LA, Hegele RA. Ketogenic diets, not for everyone. J Clin Lipidol. 2021 Jan-Feb;15(1):61-67. doi: 10.1016/j.jacl.2020.10.005[↩]
- Seidelmann SB, Claggett B, Cheng S, Henglin M, Shah A, Steffen LM, Folsom AR, Rimm EB, Willett WC, Solomon SD. Dietary carbohydrate intake and mortality: a prospective cohort study and meta-analysis. Lancet Public Health. 2018 Sep;3(9):e419-e428. doi: 10.1016/S2468-2667(18)30135-X[↩]





{kind=link}