Contents
Atopic keratoconjunctivitis
Atopic keratoconjunctivitis also called AKC is the most severe form of chronic allergic conjunctivitis or eye allergic reaction caused by immunoglobulin E (IgE) mediated mechanisms, which has been shown to involve both T-helper-1 (Th1) lymphocyte and T-helper-2 (Th2) lymphocyte inflammatory cascades, and that usually affects people with atopic disease, including atopic dermatitis, eczema, asthma, and food allergies and seasonal allergies, including a family history of allergies and hay fever 1, 2, 3, 4, 5, 6. Atopic keratoconjunctivitis is the chronic eye surface and eyelids (the conjunctiva and cornea) inflammation suffered by patients with atopic dermatitis (eczema). Atopic dermatitis also called atopic eczema, the most common inflammatory skin disease worldwide, presents as generalized skin dryness, itch, and rash 7. Atopic keratoconjunctivitis is the non-infectious inflammation of the conjunctiva (the transparent membrane that lines inside your eyelid and covers the white part of your eyeball) lining your eyelids (palpebral conjunctiva) which is red and swollen. The lower eyelid generally is affected more than the upper eyelid 4. This is a differentiating symptom from vernal keratoconjunctivitis (a severe type of seasonal allergic conjunctivitis) where the upper eyelid is most often affected. Atopy is a genetic condition where your immune system produces higher than normal antibodies in response to a given allergen. Allergic conjunctivitis is caused by contact with something to which a person may be sensitive or allergic to (allergens). However, 45% of the people with atopic keratoconjunctivitis do not display a hypersensitivity reaction to common allergens 8. Conjunctivitis is the inflammation or infection of the conjunctiva, which is the transparent membrane that lines inside your eyelid and covers the white part of your eyeball. The conjunctiva is a thin translucent mucous membrane that can be divided based on the location into palpebral conjunctiva (inside of the eyelids) and bulbar conjunctiva (begins at the edge of the cornea and covers the visible part of the sclera) (Figure 2). The conjunctiva contains nonkeratinizing, squamous epithelium and a thin, richly vascularized substantia propria containing lymphatic vessels and cells, such as lymphocytes, plasma cells, mast cells, and macrophages. The conjunctiva also has accessory lacrimal glands and goblet cells. When the small blood vessels in the conjunctiva become inflamed or infected, they’re more visible. This is what causes the whites of your eyes to appear reddish or pink. Atopic keratoconjunctivitis is a chronic eye surface inflammation with a relatively low expectation of resolution and can have low visual morbidity. If left untreated, atopic keratoconjunctivitis can progress to ulceration, scarring, cataract, keratoconus, and corneal vascularization (the process of growing blood vessels into a tissue).
Although atopic keratoconjunctivitis is a perennial (year round) disease, your symptoms may worsen in the winter. Unlike atopic dermatitis, which is generally seen early in childhood, atopic keratoconjunctivitis appears during late adolescence and early adulthood but may occur at all ages and there is a prevalence peak in patients between 20 and 50 years of age, with a personal or family history of atopic dermatitis or other allergic diseases such as eczema, asthma and/or urticaria 1, 9. The percentage of people with atopic dermatitis that develop atopic keratoconjunctivitis ranges from 25% to 42% 1. Men are more commonly affected than women with a ratio between 2 to 1 and 3 to 1 4. Approximately 5% of atopic keratoconjunctivitis patients have a history of childhood vernal keratoconjunctivitis (a severe type of seasonal allergic conjunctivitis) 10.
People with atopic keratoconjunctivitis usually show atopic dermatitis in the eyelids (see Figure 3A & 5). Eyelid dermatitis results in eyelid hyperpigmentation (panda eyes), swelling that causes horizontal eyelid creases (Dennie-Morgan lines), and absence of the lateral end of the eyebrows (Hertoghe’s sign) 1. More advanced chronic atopic keratoconjunctivitis may also cause keratinization of the eyelid margins, inflammation of the eyelid margins (blepharitis), the loss of eyelashes, and sometimes eyebrows (madarosis), thickening and fissuring of the skin (tylosis), eyelid deformities, and reactive droopy eyelids (ptosis) 1. People with atopic keratoconjunctivitis also show redness of the eyes, chemosis (a swelling of the conjunctiva), and tarsal papillae, typically in the inferior tarsal conjunctiva and sometimes even Horner-Trantas dots in the limbus (Figure 7), especially in more acute phases 1. Conjunctival scarring can lead to conjunctiva of the eyelid to stick to the conjunctiva of the eyeball (symblepharon) and shortening of the inferior conjunctival sac 1. The corneal involvement seems to be secondary to the conjunctival and palpebral involvement and may vary from superficial punctate keratitis to corneal ulcers, corneal scarring, and pannus 1.
People with atopic keratoconjunctivitis complain of severe itching most of the year that is usually more severe during the winter months and in colder climates. There is also discharge that tends to be more aqueous than in vernal keratoconjunctivitis (a severe type of seasonal allergic conjunctivitis), but it may also be mucous 1.
People with atopic keratoconjunctivitis may also complain of dry eyes that exacerbates itchiness and perpetuates conjunctival inflammation 1.
Chronic atopic keratoconjunctivitis leads to numerous complications: infections such as staphylococcal blepharoconjunctivitis and herpes simplex keratitis, cataracts (typically anterior subcapsular but also others), limbal stem-cell deficiency, keratoconus, glaucoma, retinal detachment, and corneoconjunctival tumors 1.
Atopic keratoconjunctivitis usually is diagnosed by clinical exam and a medical and family history, although a conjunctival biopsy may be helpful in distinguishing atopic keratoconjunctivitis from other conditions.
Atopic conjunctivitis treatment is complicated, often requiring input from multiple specialists such as cornea specialist, skin specialist (dermatologist) and doctor specializing in the diagnosis and treatment of allergies (allergist) to determine the most successful management.
The primary goal in managing allergic conjunctivitis, including vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis (AKC), is to avoid exposure to the allergen that triggers the allergic response 11.
If the allergen is known, steps can be taken to minimize exposure to it or, in some cases, get rid of it completely. For example, someone with an allergy to:
- House dust mites may find that minimisation measures such as removing carpet, using dust mite covers for pillows and mattresses, use of hypoallergenic bedding and washing bedding in hot water are enough to reduce symptoms.
- Animal dander may find the best option is to remove the animal or a pet from the house altogether, particularly if symptoms are severe.
- Use of air filtering devices, and dietary changes in cases of food sensitivity.
Mild to moderate symptoms of allergic conjunctivitis usually respond well to simple home treatments such as bathing eyes with cold water, ice packs and cold water compresses. Non-medicated eye drops can also help to lubricate the eye and gently flush allergens from the surface 6, 12, 13. More severe symptoms will usually require treatment with medication.
In some cases, eye patching may be required, and prevent complications that lead to vision loss. It is also important to balance this with limiting side effects of treatment.
- Cold compresses (mild cases): Cold compresses can be used as relief when you feel itchy and the urge to rub your eyes. Consistent eye itching and rubbing can cause thinning of the cornea, leading to keratoconus (corneal disease caused by the steepening and thinning of the cornea).
- Eye lubricants (mild cases): Artificial tear drops to soothe the eye surface, replenish the tear film and dilute the allergen.
- Antihistamine eye drops (mild cases): Antihistamine eye drops (e.g., Ketotifen ophthalmic such as Zaditor or Alaway, relieves itchiness) effective but should not be used for longer than 6 weeks without medical advice.
- Antihistamine tablets or syrups (mild cases): Antihistamine tablets or syrups help some people when it is difficult to avoid the allergen. Some side effects may include dryness of the eyes, nose, and mouth, and blurred vision. Antihistamines are usually contraindicated for people with glaucoma, advice should be sought from an eye specialist.
- Antihistamine eye drops containing a vasoconstrictor (mild cases): Minimize itch and remove redness by narrowing the swollen blood vessels in the eye. They should not be used for longer than 14 days without medical advice.
- Mast cell stabilizer eye drops (mild cases): Mast cell stabilizer eye drops (i.e., Olopatadine ophthalmic [Pataday, over the counter] or [Pazeo, prescription only], relieves itchiness, best used to prevent symptoms from occurring as they can take three to seven days to work. These can be used as long as necessary.
- Mast cell stabiliser eye drops with antihistamines (dual acting agents): These agents block histamine-1 (H1) receptors for acute therapy (antihistamine action) and inhibit mast cell degranulation for prophylaxis (mast cell stabilizer action). Compared with antihistamines and mast cell stabilizers, topical dual-activity agents are clinically superior in both symptom relief and tolerability 14. They are considered first-line therapies and are the most commonly prescribed treatment 14. They’re fast acting, effective and generally well tolerated. Dual acting agents include bepotastine, epinastine, azelastine, alcaftadine, and ketotifen, which are approved for itch treatment, and olopatadine, which is approved for all signs and symptoms of ocular hypersensitivity disorders 6. Olopatadine is safe, effective, and clinically superior to ketotifen, whilst some studies show that alcaftadine appears to be superior to olopatadine in reducing ocular itch 12, 2.
- Steroids: Steroid eye drops (moderate cases) or steroid oral medication (severe cases) effective in relieving symptoms quickly, but are associated with cataract formation, glaucoma and bacterial and viral infections of the cornea and conjunctiva. Steroid use needs to be monitored closely by your ophthalmologist and used only as directed to prevent serious eye problems and should never be used in the presence of herpes infections. Use of steroid drops for a long time or at a large amount can cause serious vision problems, including glaucoma, cataracts and eye infections (keratitis). Only ophthalmologists (eye specialists) who can monitor for side effects should prescribe steroids for allergic conjunctivitis. Talk with your ophthalmologist if you have questions about steroid drops.
- Immunomodulators such as Tacrolimus or Cyclosporine (moderate-severe cases): The topical calcineurin inhibitors cyclosporine A and tacrolimus are very effective in the treatment of atopic keratoconjunctivitis and may serve as steroid-sparing agents when these forms of chronic allergic conjunctivitis become steroid-dependent 1, 6. The concentrations of cyclosporine A in the different ophthalmic formulations range between 0.01% and 2% and therefore the administration varies between 1 and 6 times per day 12. Tacrolimus may also be prepared as suspension by pharmacies and exists as an ointment for dermatological purposes in most countries at a concentration of 0.03-0.1%. Recent research shows that tacrolimus may have similar if not superior effectivity than cyclosporine A for the treatment of vernal keratoconjunctivitis. Moreover, dermatologic ointment containing tacrolimus is effective for the treatment of lid eczema in atopic keratoconjunctivitis 1, 6. Topical treatment with calcineurin inhibitors has side effects such as stinging/burning sensation and the possibility of molluscum contagiosum virus, papillomavirus, or herpesvirus infection, although there is evidence from studies on dry eye syndrome that treatment with cyclosporine A can be topically administered long term and without systemic absorption 12, 6. 2, 15. At present, tacrolimus is generally administered topically in cases that do not respond to cyclosporine A 1. Finally, in very severe cases, allergic conjunctivitis such as vernal keratoconjunctivitis and atopic keratoconjunctivitis may require systemic immunosuppression that is usually achieved with cyclosporine A, tacrolimus, or mycophenolate mofetil 16, 1, 6.
- Allergen-specific immunotherapy. Allergen-specific immunotherapy is only recommended when clearly defined systemic hypersensitivity to an identified allergen exists. Patients requiring allergen-specific immunotherapy should be referred to an allergist or specialist ophthalmologist. Allergen immunotherapy for specific allergens may benefit people with persistent, severe allergic conjunctivitis. However, relief of allergic conjunctivitis symptoms will not happen straight away.
- Surgery, oral corticosteroids (short pulses) or corticosteroid lid injection, or systemic treatment with immunomodulators or biologics may be appropriate options for use by corneal specialists in selected patients with ocular complications or persisting symptoms following prior treatments. Insunakinra (EBI-005) is the first inmunophilin synthesized for topical ophthalmologic use. It is an antagonist of the IL-1 receptor and binds to it, blocking the rest of the pathway. It has been documented to diminish ocular surface symptoms such as itching, inflammation, and discomfort 17. Another molecule called liftitegrast (Shire Pharmaceuticals) has both activity as an antagonist of the IL-1 receptor and as antagonist of the lymphocyte functional antigen-1 and has proven effective for treatment of ocular surface symptoms 18. In very recalcitrant cases of vernal keratoconjunctivitis and atopic keratoconjunctivitis, eye surgery may be needed. Papillae resection, in some cases with grafting of autologous conjunctiva, amniotic membrane or mucous membrane are effective in the treatment of severe forms of vernal keratoconjunctivitis with corneal ulcers 19, 20, 21. In atopic keratoconjunctivitis, surgery may be needed for eyelid and conjunctival scarring. Atopic disease and atopic keratoconjunctivitis can be complicated by subcapsular cataracts and/or severe ocular surface disease that may require complex surgery such as superficial keratectomy, limbal transplantation, or keratoprosthesis implantation 22.
Usually combinations of oral and topical antihistamines and mast cell stabilizers usually are effective in controlling atopic keratoconjunctivitis symptoms. In more severe cases, there is potential for damage to the eye caused by scratching and rubbing. A eye doctor (ophthalmologist) may advise you to wear cotton gloves at night to prevent unintentional damage to your eye surface. Cold compresses and saline irrigation to lower the elevated tear pH also may be helpful. Only in severe cases should topical steroid therapy be considered and under the supervision of your eye doctor (ophthalmologist). Other steroid-sparing agents may be helpful, including cyclosporine or tacrolimus. Oral medications may be very helpful in some atopic conjunctivitis cases.
Figure 1. Human eye
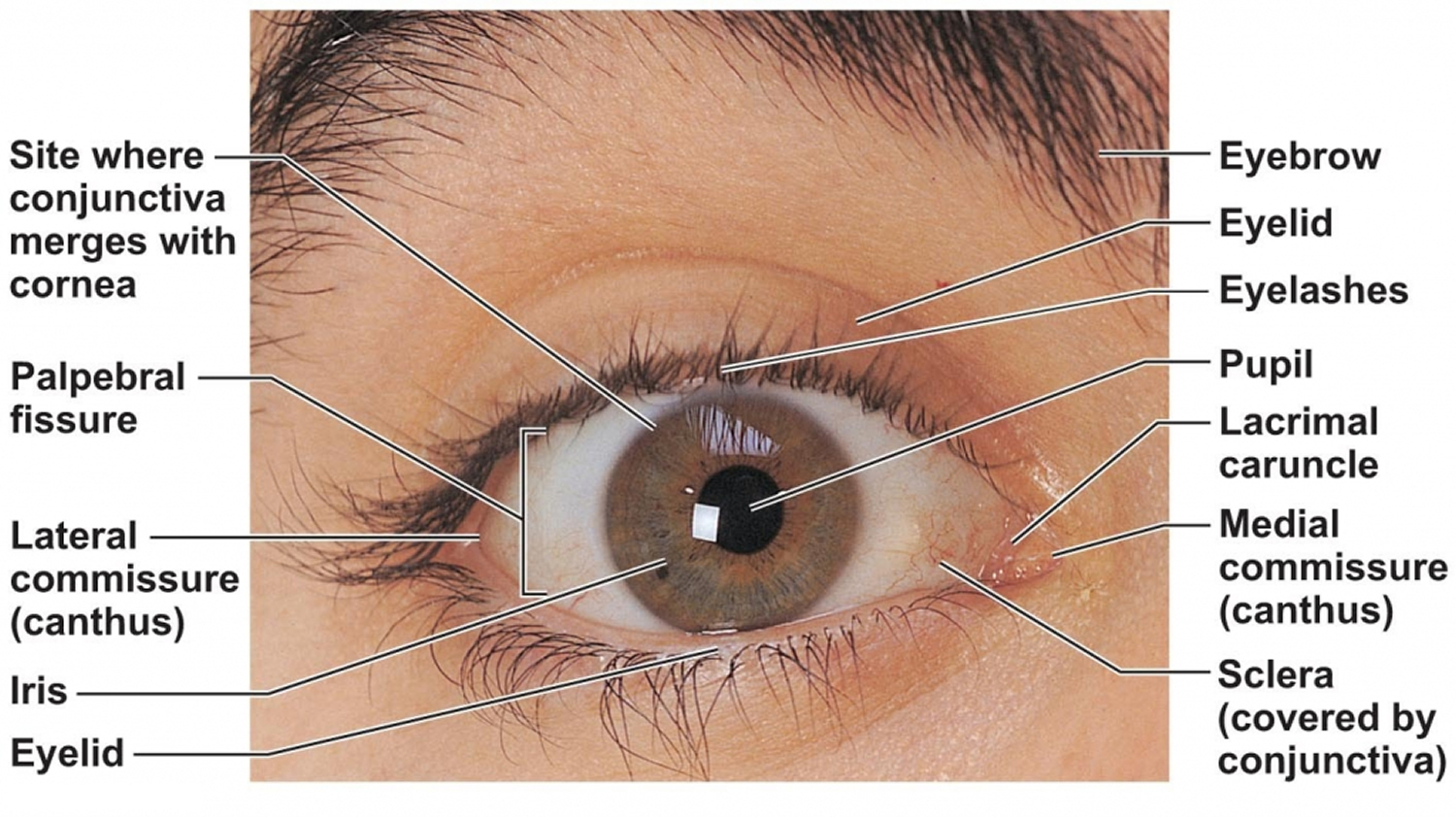
Figure 2. Eye anatomy
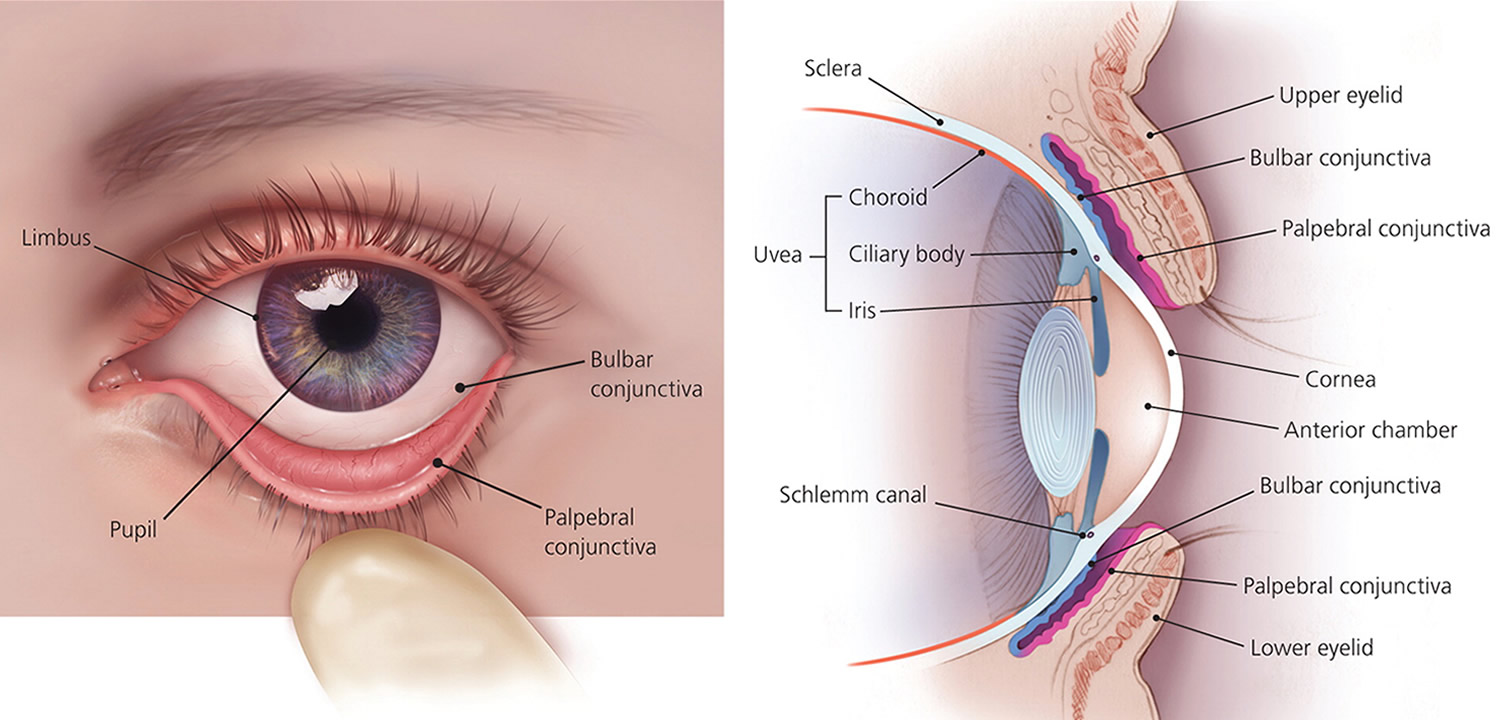
Figure 3. Atopic keratoconjunctivitis
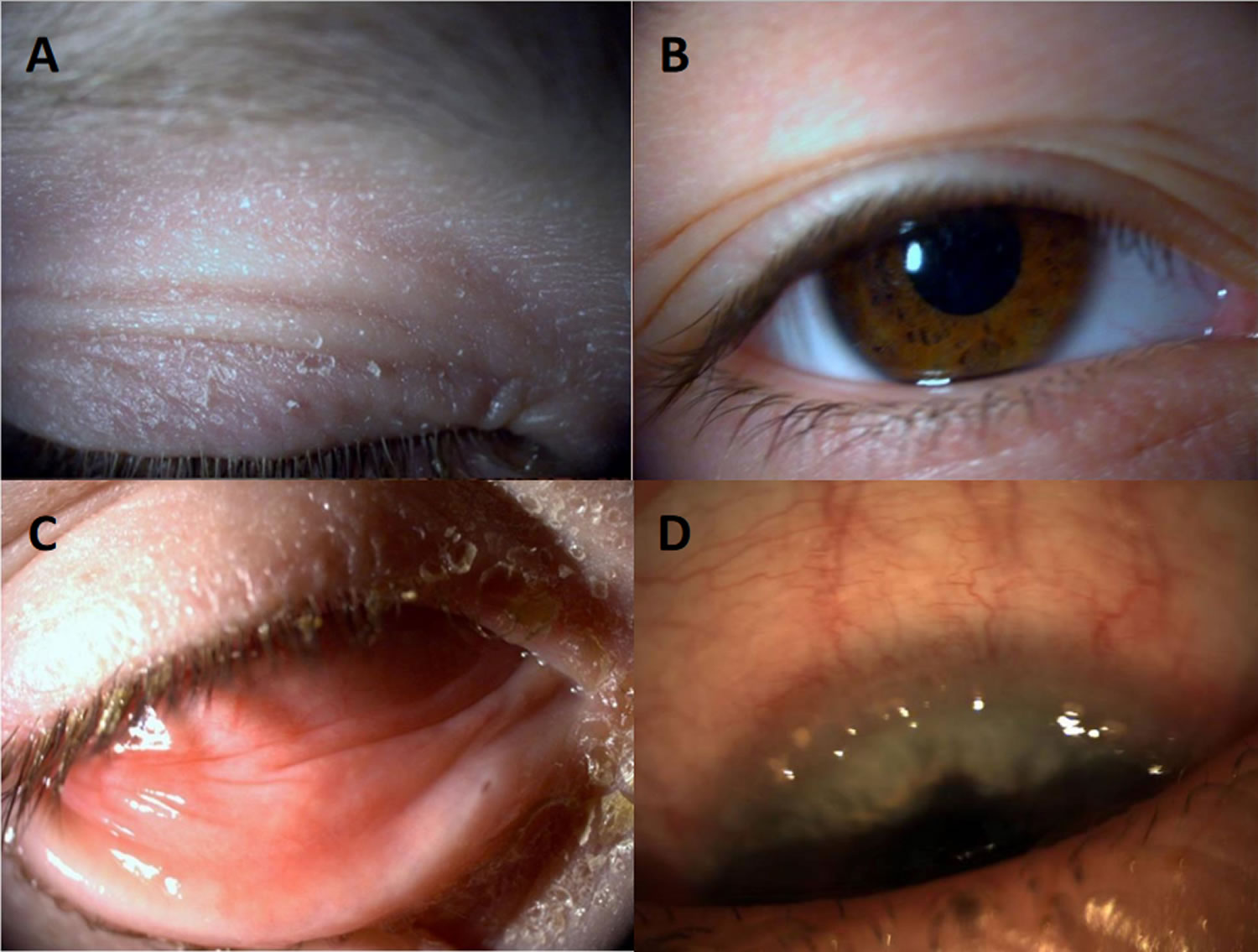
Footnotes: Atopic keratoconjunctivitis. (A) Eczema of the eyelid; (B) Pseudoptosis and Dennie–Morgan double fold of the upper and lower lid; (C) Infiltration of the inferior conjunctiva and blepharitis; (D) Limbal infiltration with Horner–Trantas dots.
[Source 23 ]Figure 4. Atopic blepharokeratoconjunctivitis
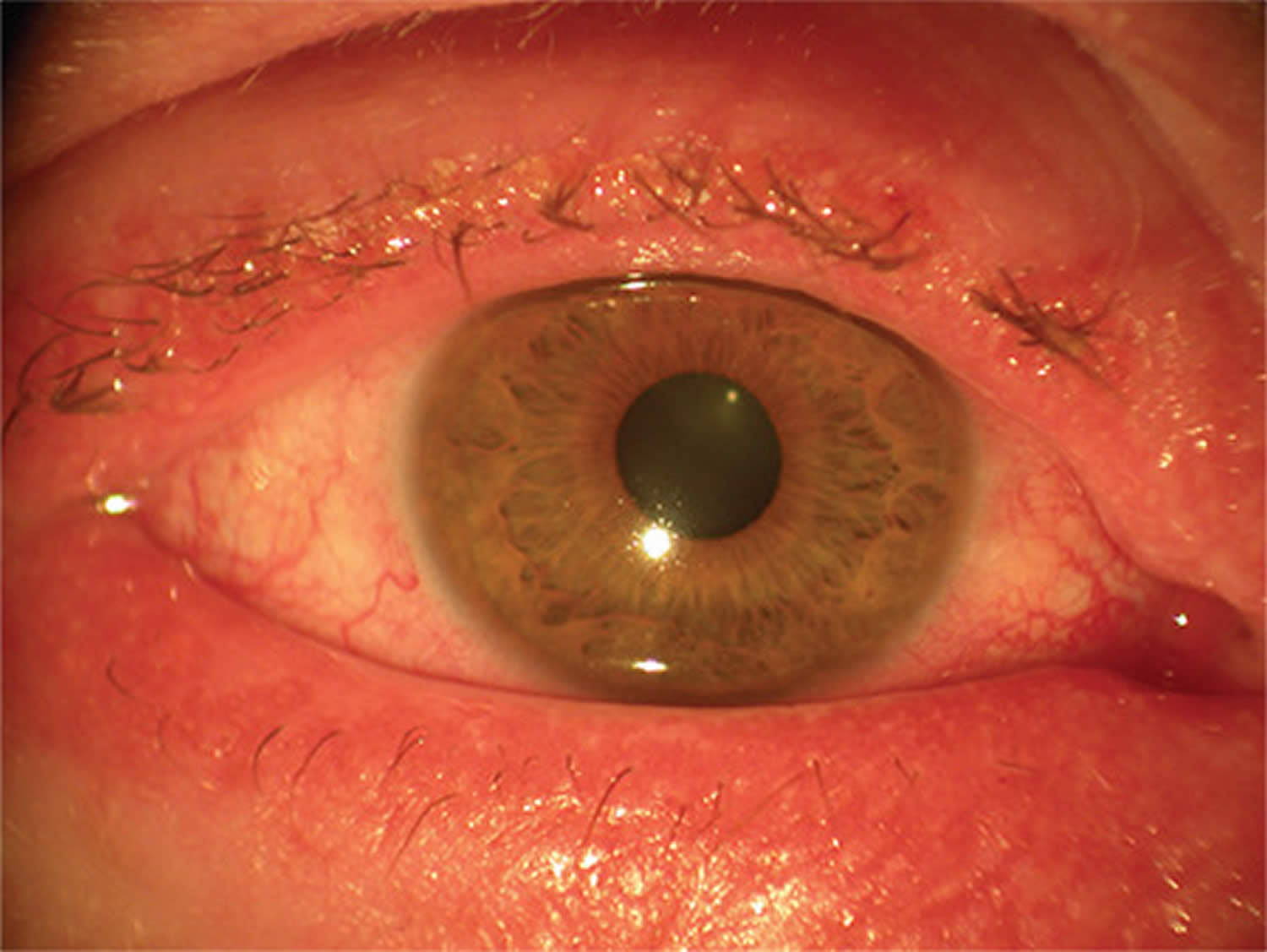
Figure 5. Eyelid atopic dermatitis

Footnote: Atopic dermatitis of the eyelids in a child with characteristic lichenification (skin thickening, hyperpigmentation and exaggerated skin lines caused by sudden itching and excessive rubbing and scratching) and fine scaling 25.
[Source 7 ]Figure 6. Atopic dermatitis

Figure 7. Horner–Trantas dots

Footnote: Peri-limbal Horner–Trantas dots are focal white dots consisting of degenerated epithelial cells and eosinophils and are indicative of vernal keratoconjunctivitis.
[Source 27 ]What is atopy?
Atopy refers to genetic predisposition of experiencing an exaggerated immune response (hypersensitivity) to allergens via the overproduction of immunoglobulin E (IgE) 28. The term “atopy” is derived from the Greek word meaning “the state of being out of place” 28. Atopy typically consists of atopic dermatitis (skin), asthma (airways), and allergic rhinitis (nasal mucosa). Other atopic conditions include food allergy and drug allergy, allergic conjunctivitis, urticaria, angioedema, and anaphylaxis (a severe, life-threatening allergic reaction that requires immediate medical attention).
Individuals with atopy often have environmental allergies, allergic asthma, rhinitis, and atopic dermatitis or eczema. Less commonly, these individuals exhibit food allergies, urticaria, and nonhereditary angioedema.
While the specific cause of atopy is not well understood, a gene-environment interaction is thought to play an important role. Triggers that have been identified include viral respiratory infections, exercise, certain drugs, climatic factors, and psychological factors. Multiple genes with effects on immunoglobulin E (IgE) synthesis are also likely involved as well as changes in the skin microbiome potentially affecting skin barrier function.
The pathophysiology of atopy involves mast cell activation which leads to an inflammatory cascade of lipid mediators, cytokines, and histamine.
Atopic conjunctivitis causes
The exact cause of atopic keratoconjunctivitis is incompletely understood 10, 1, 3. Atopic keratoconjunctivitis is believed to arise from various factors, including allergen exposure, atopic dermatitis (present in more than 90% of cases), genetic predisposition and a combination of immune imbalance involving immediate type 1 hypersensitivity immune reactions (immunoglobulin E [IgE] mediated) and type 4 delayed hypersensitivity immune reactions to eye allergen exposure 29, 6. The tears of atopic keratoconjunctivitis patients will often contain high levels of immunoglobulin E (IgE) suggesting a type 1 hypersensitivity immune reaction 30, 10. However, 45% of the people with atopic keratoconjunctivitis do not display a hypersensitivity reaction to common allergens 8. Atopic keratoconjunctivitis tends to be more perennial (all year round), often worsening in the winter season, and individuals with atopic keratoconjunctivitis are sensitive to a wide range of airborne environmental pathogens 24. Recent studies suggest that microbes and especially colonization of the conjunctiva with Staphylococcus aureus may have a role in the disease 1.
The pathophysiology of atopic keratoconjunctivitis involves the release of cytokines by mast cells, eosinophils, T cells especially T-helper-1 (Th1) cells that produce chemotaxis and stimulate eosinophil production and conjunctival epithelial cells 31. Eosinophils initiate cytokine production, which heightens the inflammatory response 1. The release of allergic mediators leads to activation of T helper cells and chronic mast cell degranulation 32. Atopic keratoconjunctivitis patients have also been shown to have decreased corneal sensitivity and conjunctival goblet cell density compared to controls 33. The tears of patients who suffer from atopic keratoconjunctivitis have been shown to have elevated inflammatory cytokines and chemokines 34.
Conjunctival inflammation with eosinophil infiltrates in atopic keratoconjunctivitis, sometimes extending to the cornea and leading to corneal ulcer, scar formation and, ultimately, to vision loss 35, 36.
Risk factors for atopic keratoconjunctivitis
Atopic keratoconjunctivitis is a multifactorial disease with genetic and environmental risk factors 3. The strongest associations are genetic predisposition for poor skin barrier function and dysregulation of the immune system, asthma, allergic rhinitis, and environmental allergens 3. The presence of food allergies and food sensitivities in infancy and childhood is associated with a more severe form of atopic dermatitis 37. Allergy and sensitivity to pollen, pets and dust mites have also been associated with atopic keratoconjunctivitis 3.
Environmental factors such as climate, diet, urban living including pollution exposure, tobacco smoke, duration of breastfeeding during infancy, and obesity have been suggested as risk factors for atopic keratoconjunctivitis 37. It has also been proposed that antibiotic use may increase the risk of developing atopic disease via alterations to the gut microbiome 38.
Atopic conjunctivitis signs and symptoms
Atopic conjunctivitis signs and symptoms can vary greatly.
Atopic conjunctivitis usually affects both eyes and makes them:
- Bloodshot
- Puffy eyes or swelling of the eyelids
- Burn or gritty feeling in one or both eyes
- Itchy eyes
- Watery eyes
- Sensitive to light called photophobia.
The symptoms described above may not necessarily mean that you have atopic keratoconjunctivitis. If you experience one or more of these symptoms, contact your eye doctor (ophthalmologist) for a complete eye exam. Blurred vision or any change in the appearance of the cornea (clear part of the eye that covers the pupil) requires urgent referral to an eye specialist. Speak to your doctor or optometrist for a referral.
The main symptoms of atopic keratoconjunctivitis are usually perennial (all year round) and include bilateral itching of the conjunctiva, eyelids, and periorbital skin. Tearing, burning, photophobia, blurry vision and a foreign body sensation in the eyes are commonly encountered symptoms. Patients with atopic keratoconjunctivitis can have copious mucoid discharge, often described as rope-like 39.
In comparison to vernal keratoconjunctivitis, the symptoms of atopic keratoconjunctivitis are typically less severe but persistent. The skin changes in atopic keratoconjunctivitis are more pronounced, including eczema, redness, dryness, and scaly skin, often associated with thickening. Epidermal integrity is disrupted, leading to fissures, scratches (excoriation), cracks, and intense itching 34.
Other associated signs in atopic keratoconjunctivitis include chronic staphylococcal blepharitis, madarosis, keratinization of the lid margin, Hertoghe sign (absence of the lateral portion of eyebrows), and Dennie Morgan folds (skin folds on the lower eyelids due to regular itching) 10. Facial skin may have folds, ectropion, and epiphora. Patients can develop ptosis. In atopic keratoconjunctivitis, inferior palpebral conjunctival involvement is more common than superior involvement seen in vernal keratoconjunctivitis. The discharge in atopic keratoconjunctivitis is watery compared to the stringy mucoid discharge typically seen in vernal keratoconjunctivitis.
Hyperemia, inflammation, and chemosis may be present during active acute episodes 10. The papillae are smaller than in vernal keratoconjunctivitis, although marcopapillae can also develop. Diffuse conjunctival infiltration and scarring can give a whitish and featherless appearance. In cicatricial disease, symblepharon formation, shortening of the fornix, and caruncular keratinization may occur. Limbal papillae similar to those seen in vernal keratoconjunctivitis and Horner-Trantas dots can also arise in atopic keratoconjunctivitis 34.
In atopic keratoconjunctivitis, punctate epithelial erosions are commonly observed, particularly in the inferior part of the cornea, and these erosions can be significant 10. Persistent epithelial defects can occur, leading to cornea thinning, perforation, and descemetocele formation 10. Corneal plaque formation can also be observed. Another common finding feature in atopic keratoconjunctivitis is stromal scarring and peripheral vascularization, which tends to be more prevalent than vernal keratoconjunctivitis 10.
Atopic conjunctivitis complications
Untreated or refractory cases of atopic keratoconjunctivitis have a higher risk of developing sight threatening corneal complications such as bacterial and fungal keratitis, and occasionally, herpetic keratitis 40.
- Cataract: Patients with atopic keratoconjunctivitis may develop cataracts, particularly anterior or posterior subcapsular cataracts, secondary to long-term steroid therapy 41. Cataract is a condition that causes the cornea to become cloudy, resulting in blurred vision. These cataracts can be a side effect of using corticosteroid medications to manage the chronic inflammation associated with atopic keratoconjunctivitis 10. It is thought that 8-10% of people with a severe form of atopic dermatitis are at risk of developing cataract.
- Retina: Atopic keratoconjunctivitis has an increased risk of developing endophthalmitis due to a high lid margin and an increased concentration of Staphylococcus aureus in the lid margins 10. Additionally, atopic keratoconjunctivitis patients at high risk for cataract surgery may also face an increased risk of retinal detachment 42.
- Keratoconus: Keratoconus can be secondary to longterm rubbing of the eyes and herpes simplex keratitis in patients with atopic keratoconjunctivitis 43. The continuous eye rubbing associated with atopic keratoconjunctivitis can weaken and thin the corneal structure, predisposing the cornea to develop keratoconus, characterized by progressive bulging and thinning of the cornea. Additionally, herpes simplex keratitis, an infection caused by the herpes simplex virus, can contribute to corneal thinning and deformation, further increasing the risk of keratoconus development in atopic keratoconjunctivitis patients.
Corneal findings range from punctate epithelial erosions to ulcers (infectious or sterile), neovascularization, and lipid keratopathy. Herpes simplex keratitis is more common in patients with atopic keratoconjunctivitis and often more severe 39. Patients with atopic keratoconjunctivitis are also more likely to get bilateral herpetic keratitis, which is relatively unusual in the absence of atopy 44, 45. As with other eye allergic diseases, people with atopic keratoconjunctivitis are at increased risk of keratoconus due to chronic eye rubbing. Therefore, patients with atopic keratoconjunctivitis should be counseled to limit eye rubbing as much as possible and should be provided with treatment to reduce or eliminate itch. Due to common use of topical and oral corticosteroids, glaucoma is a potential complication of treatment. There are various case reports of conjunctival squamous cell carcinoma (SCC) in patients with atopic keratoconjunctivitis 46, 47.
Figure 8. Cataracts
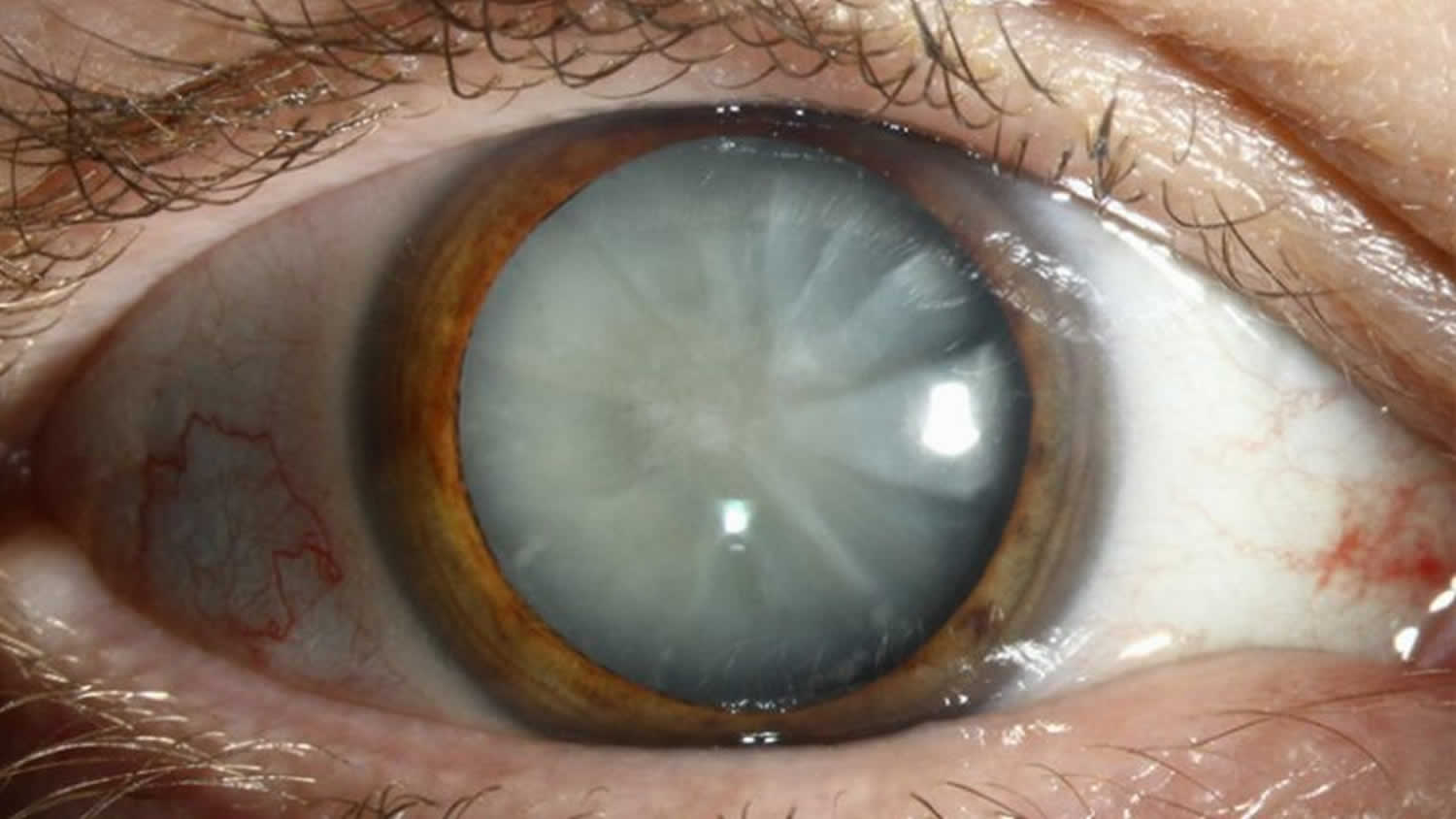
Figure 9. Keratoconus
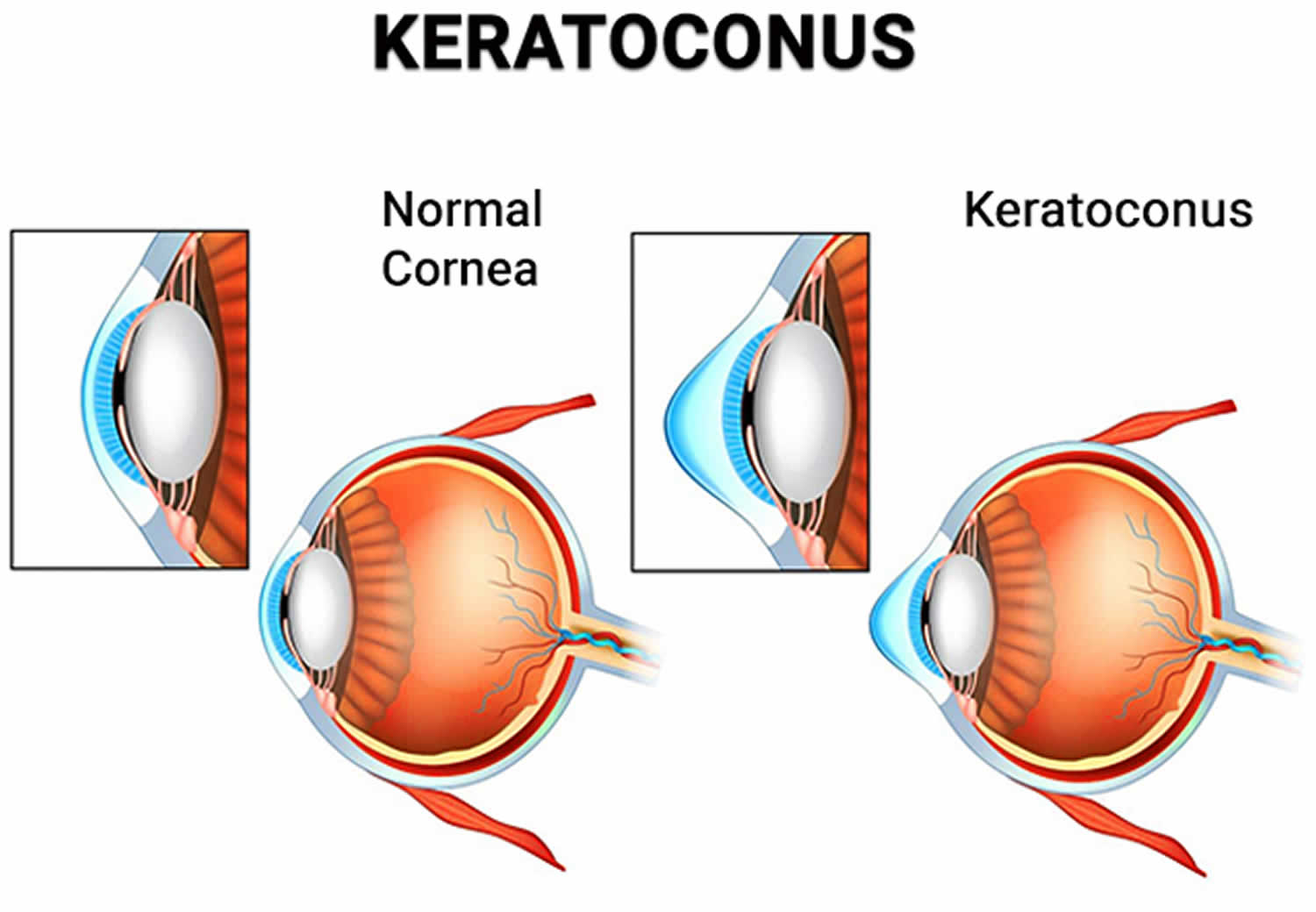
Footnote: Keratoconus is a degenerative eye disorder in which your cornea thins and stretches near the center, loses its shape and eventually bulges outward to form a cone shape. These physical changes come on gradually; in fact, they may start with just the loss of collagen in your eye. The misshapen cornea distorts your vision and requires immediate medical attention by a licensed ophthalmologist. A cone-shaped cornea may also cause sensitivity to light and doesn’t offer adequate protection for your eye.
[Source 49 ]Figure 10. Herpes simplex keratitis
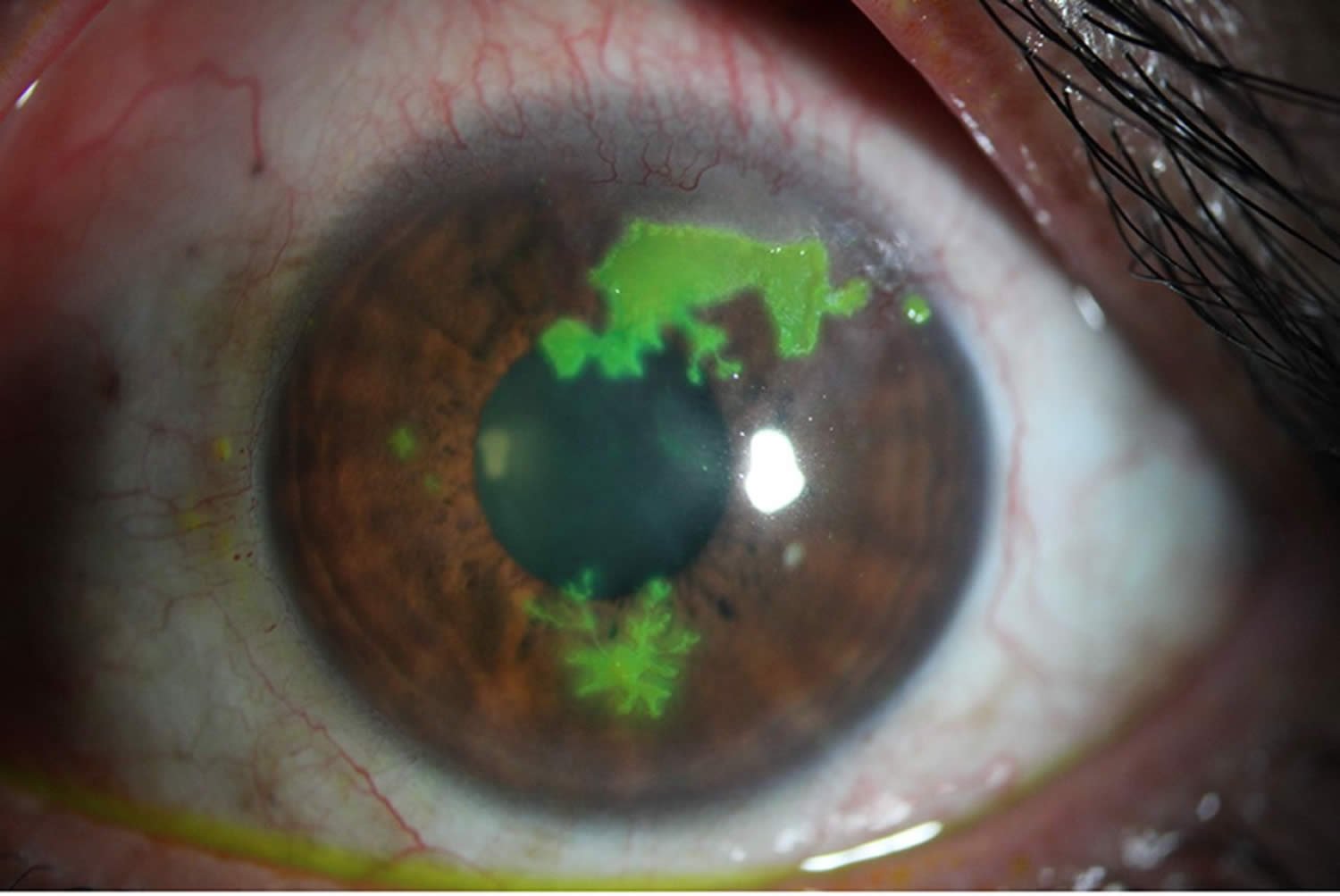
Footnotes: Slit-lamp photograph showing three phases of lesions: epithelial dots (9 o’clock), dendritic pattern (6 o’clock) and a geographic epithelial keratitis (12–2 o’clock), suggesting herpes simplex virus epithelial keratitis.
[Source 50 ]Atopic conjunctivitis diagnosis
A diagnosis of atopic keratoconjunctivitis is made by history and examination. Examination findings are similar to those seen in simple allergic conjunctivitis. However, in atopic keratoconjunctivitis, there are additional chronic inflammatory changes to the ocular surface, such as corneal scarring and neovascularization. Changes to the eyelids, particularly the lower lid, and peri-orbital skin can range from mild atopy to lichenification (skin thickening, hyperpigmentation and exaggerated skin lines caused by sudden itching and excessive rubbing and scratching) 51.
Although allergy testing may help pinpoint the specific allergens, it is usually not necessary since the types of allergens that usually cause conjunctivitis are very common, like grass, weed, and tree pollens. Eye drop treatments are the same no matter what allergen is causing the reaction.
Physical examination
- Eyelids and periorbita: The eyelids and periorbital skin will almost always show evidence of eczematous dermatitis (erythematous, thickened dry skin with blistered patches). Eyelid findings include tylosis (thickening of the tarsal border of the eyelid) with crusting and scaling 23. Meibomian gland disease is very common in patients with AKC. Other lid findings often encountered are ectropion, trichiasis and madarosis.
- Conjunctiva: The conjunctiva is hyperemic and edematous, with prominent tarsal papillae (papillary conjunctivitis). Mucoid discharge is often present. Severe conjunctival disease can result in scarring and symblepharon. Horner-Trantas dots may or may not be present.
- Cornea: Corneal involvement is frequent and can range from punctate epithelial erosions to ulcers and even perforation. Peripheral vascularization and pannus are common 52.
- Anterior Segment: Anterior and posterior subcapsular cataracts are common.
Diagnostic testing
Diagnostic procedures and lab tests can aid in diagnosis and assessing severity of atopic keratoconjunctivitis. Many of these tests require equipment not readily available to most ophthalmologists.
Serum IgE and skin prick testing is non-specific, but can be helpful in establishing that a patient has atopic disease 53. IgE levels in tears have been shown to correlate with clinical severity of allergic eye disease 54.
Brush cytology, which involves taking scrapings from the tarsal conjunctiva, can quantify levels of inflammatory cells such as eosinophils and neutrophils. It has been show to correlate with the amount of corneal damage 55.
Confocal scanning laser microscopy has been described as a less invasive means of evaluating the ocular surface of atopic keratoconjunctivitis patients by identification of inflammatory cell densities 33. A significant correlation was found between the extent of inflammation as determined via brush cytology and that found by in vivo confocal microscopy 56.
Conjunctival biopsy is rarely used to assist in diagnosing atopic keratoconjunctivitis. Histology of atopic keratoconjunctivitis typically shows proliferation of goblet cells, invasion of eosinophils and mast cells into the epithelium as well as mononuclear cell infiltrate in the substantia propria 34. Conjunctival epithelium of atopic keratoconjunctivitis patients shows increased levels of T cells, T-helper cells, macrophages and dendritic cells 57.
Atopic keratoconjunctivitis differential diagnosis
Atopic keratoconjunctivitis differential diagnosis include 3:
- Vernal keratoconjunctivitis
- Seasonal allergic conjunctivitis
- Giant papillary conjunctivitis
- Phlyctenular keratoconjunctivitis. Phlyctenular keratoconjunctivitis is a nodular inflammation of the cornea or conjunctiva that results from a hypersensitivity reaction to a foreign antigen 58.
- Toxic conjunctivitis
- Viral conjunctivitis
- Infections conjunctivitis (especially trachoma)
- Adult blepharitis. Blepharitis refers to inflammatory disease processes of the eyelid(s). Blepharitis often is associated with systemic diseases, such as rosacea, atopy, and seborrheic dermatitis, as well as eye diseases, such as dry eye syndromes, chalazion, trichiasis, ectropion and entropion, infectious or other inflammatory conjunctivitis, and keratitis 59.
- Ocular rosacea.
Clinically, atopic keratoconjunctivitis is very similar to vernal keratoconjunctivitis (VKC), and there is controversy regarding classification of the two diseases. It has been proposed that vernal keratoconjunctivitis is a childhood form of atopic keratoconjunctivitis that evolves into atopic keratoconjunctivitis in adulthood. However, vernal keratoconjunctivitis can be present without signs of atopic disease. Vernal keratoconjunctivitis is generally regarded to end at puberty, and disease severity can fluctuate with seasons. Giant papillary reaction is more common in vernal keratoconjunctivitis. Atopic disease is typically a year-round condition (perennial). Though atopic keratoconjunctivitis peaks in adults, it can be present in childhood.
Atopic conjunctivitis treatment
Consulting with cornea specialist, dermatologists and allergists can help determine the most successful management. The primary goal in managing allergic conjunctivitis, including vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis, is to avoid exposure to the allergen that triggers the allergic response.
If the allergen is known, steps can be taken to minimize exposure to it or, in some cases, get rid of it completely. For example, someone with an allergy to:
- House dust mites may find that minimisation measures such as removing carpet, using dust mite covers for pillows and mattresses, use of hypoallergenic bedding and washing bedding in hot water are enough to reduce symptoms.
- Animal dander may find the best option is to remove the animal or a pet from the house altogether, particularly if symptoms are severe.
- Use of air filtering devices, and dietary changes in cases of food sensitivity.
Mild to moderate symptoms of allergic conjunctivitis usually respond well to simple home treatments such as bathing eyes with cold water, ice packs and cold water compresses. Non-medicated eye drops can also help to lubricate the eye and gently flush allergens from the surface. More severe symptoms will usually require treatment with medication.
In some cases, eye patching may be required, and prevent complications that lead to vision loss. It is also important to balance this with limiting side effects of treatment.
Cold compresses, saline, and cold artificial tears or ointments are useful because they alleviate inflammation and discomfort and dilute the allergen, especially in acute allergic conjunctivitis 6, 12, 13. Recent studies demonstrate the additive effect on the pharmacology of topical agents when combined with cold compresses and artificial tears 12. Other treatments such as eating probiotics like mandarin orange yogurt or antagonists of the prostaglandin D2 receptor 2 have shown promising results in clinical trials, decreasing the symptoms of patients with rhino-conjunctivitis 12, 13.
Maintaining good eyelid hygiene is also essential to prevent and treat staphylococcal blepharitis.
For patients with dry and fissured skin around the eyes, using a moisturizing cream such as E45 can help keep the skin hydrated and improve comfort.
A bandage contact lens may be recommended as part of the treatment plan for persistent epithelial defects. The bandage contact lens can protect the cornea and promote the healing of the corneal defect 60.
Medications for atopic keratoconjunctivitis
Topical therapy
Mild atopic keratoconjunctivitis can be treated similarly to other allergic eye disease, with emphasis placed on hand hygiene, cold compresses, and topical mast cells stabilizers (olopatadine 0.1% or lodoxamide 0.1%) and antihistamines (azelastine 0.05%) 3. While almost all patients will require more intensive treatment, these are vital to efficacious treatment. Corticosteroid drops and ointments are commonly employed in the treatment of atopic keratoconjunctivitis, especially to achieve control of exacerbations and breakthrough inflammation 3. Steroid therapy should be tapered as quickly as possible while avoiding rebound inflammation 3. Calcineurin inhibitors (cyclosporine and tacrolimus) are an effective steroid-sparing therapy 3. Calcineurin is an enzyme involved in the activation of T cells, a key player in atopic keratoconjunctivitis. Tacrolimus is available as a 0.03% and 0.1% topical ointment for dermatologic use (Protopic). It has been used off- label for treatment of ophthalmic diseases 61. Topical cyclosporine is available commercially in a 0.05% eye drop preparation (Restasis). Topical calcineurin inhibitors are safe and generally well tolerated, with stinging and eyelid skin maceration being the most common side effects 62. A recent meta-analysis demonstrated the efficacy of topical immunomodulators in treating atopic keratoconjunctivitis 63.
Oral Medications
Oral antihistamines are routinely used in atopic disease. Oral steroids and cyclosporine are generally reserved for severe/recalcitrant disease or for treatment of dermatologic disease and are often employed in conjunction with the patient’s dermatologist 3. Prolonged treatment with oral steroids is avoided due to unacceptable side effects. Systemic cyclosporine, given at dose of 5mg/kg per day has been shown helpful in inducing remission of severe atopic disease 64, 65. Once remission is obtained, frequency can be decreased to as little as every 5th day. Patients on systemic cyclosporine need regular monitoring of renal function, liver function, blood counts, and blood pressure.
Additional therapy
Zaouali et al 66 reported improvement of symptoms and clinical features of atopic keratoconjunctivitis with injection of supratarsal triamcinolone acetonide. Punctal occlusion can useful for concomitant dry eye.
Medical follow up
Patients with atopic keratoconjunctivitis require close, long- term follow up for development of vision threatening complications and medication side effects such as cataract formation and intraocular pressure elevation associated with steroid usage.
Surgery for atopic keratoconjunctivitis
Amniotic membrane transplantation has been shown to be very effective for persistent corneal epithelial defects 67.
Tectonic keratoplasty may be necessary for patients with severe corneal thinning or perforations. Penetrating keratoplasty (PK) may be indicated for corneal opacities or severe ulceration and thinning.
Patients with atopic keratoconjunctivitis are at increased risk of cataract formation (especially anterior and posterior subcapsular), independent of steroid exposure. Postoperative care and final visual outcomes are impacted by ongoing ocular surface disease.
Eyelid surgery may be necessary for correction of trichiasis, ectropion or entropion 39.
Surgical follow up
Penetrating keratoplasty in atopic keratoconjunctivitis patients is associated with higher rate of postoperative complications such as graft rejection, cataracts and glaucoma 67. Additionally, penetrating keratoplasty is not curative for atopic keratoconjunctivitis; these patients continue to have severe ocular surface disease that can affect viability of the corneal graft. Despite these complications, penetrating keratoplasty can provide significant improvements in visual acuity. One study looking at long term success of penetrating keratoplasty in atopic keratoconjunctivitis found a 50% failure rate in primary penetrating keratoplasty, with the primary causes of graft failure being rejection and stromal ulceration 39.
Atopic conjunctivitis prognosis
Atopic keratoconjunctivitis (AKC) may result in decreased vision or blindness from corneal complications, such as chronic superficial punctate keratitis, persistent epithelial defects, corneal scarring or thinning, keratoconus, cataracts, and symblepharon formation 39.
Complications result from persistent surface keratopathy, corneal scarring or thinning, keratoconus, cataracts, and symblepharon formation. In addition, medical treatment with corticosteroids can further promote the development of cataracts, glaucoma, and secondary corneal infections.
Proper preventive measures, prompt effective treatment of exacerbations, and well-timed elective surgical intervention can reduce the incidence of poor vision and blindness 68.
Patients should be observed every few days or weeks until the ocular surface disease is stable 68. Moreover, when medically treating patients with steroids or immunosuppressants, a regular interval survey for drug-related side effects and complications is indicated 68.
- Patel N, Venkateswaran N, Wang Z, Galor A. Ocular involvement in atopic disease: a review. Curr Opin Ophthalmol. 2018;29:576–581. doi: 10.1097/ICU.0000000000000532[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Bielory L, Schoenberg D. Emerging therapeutics for ocular surface disease. Curr Allergy Asthma Rep. 2019;28:19–16. doi: 10.1007/s11882-019-0844-8[↩][↩][↩]
- Atopic Keratoconjunctivitis. https://eyewiki.org/Atopic_Keratoconjunctivitis[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Atopic Keratoconjunctivitis (AKC). https://www.umkelloggeye.org/conditions-treatments/atopic-keratoconjunctivitis[↩][↩][↩]
- Baudouin C, Liang H, Bremond-Gignac D, Hamard P, Hreiche R, Creuzot-Garcher C, et al. CCR4 and CCR5 expression in conjunctival specimens as differential markers of T(H)1/T(H)2 in ocular surface disorders. J Allergy Clin Immunol. (2005) 116:614–9. 10.1016/j.jaci.2005.05.033[↩]
- Fauquert JL, Jedrzejczak-Czechowicz M, Rondon C, Calder V, Silva D, Kvenshagen BK, Callebaut I, Allegri P, Santos N, Doan S, Perez Formigo D, Chiambaretta F, Delgado L, Leonardi A Interest Group on Ocular Allergy (IGOA) from the European Academy of Allergy and Clinical Immunology. Conjunctival allergen provocation test : guidelines for daily practice. Allergy. 2016;72:43–54. doi: 10.1111/all.12986[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Atopic dermatitis. https://dermnetnz.org/topics/atopic-dermatitis[↩][↩]
- La Rosa M, Lionetti E, Reibaldi M, Russo A, Longo A, Leonardi S, Tomarchio S, Avitabile T, Reibaldi A. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013;39:18. doi: 10.1186/1824-7288-39-18[↩][↩]
- Leonardi A. Vernal keratoconjunctivitis: pathogenesis and treatment. Prog Retin Eye Res. 2002;21:319–339. doi: 10.1016/s1350-9462(02)00006-x[↩]
- Baab S, Le PH, Gurnani B, et al. Allergic Conjunctivitis. [Updated 2024 Jan 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448118[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Berger WE, Granet DB, Kabat AG. Diagnosis and management of allergic conjunctivitis in pediatric patients. Allergy Asthma Proc. 2017;38:16–27. doi: 10.2500/aap.2017.38.4003[↩]
- Leonardi A, Bogacka E, Fauquert JL, Kowalski ML, Groblewska A, Jedrzejczak-Czechowicz M, Doan S, Marmouz F, Demoly P, Delgado L. Ocular allergy: recognizing and diagnosing hypersensitivity disorders of the ocular surface. Allergy. 2012;67:1327–1337. doi: 10.1111/all.12009[↩][↩][↩][↩][↩][↩][↩]
- O’Brien TP. Allergic conjunctivitis: an update on diagnosis and management. Curr Opin Allergy Clin Immunol. 2013;13:543–549. doi: 10.1097/ACI.0b013e328364ec3a[↩][↩][↩]
- Dupuis P, Prokopich CL, Hynes A, Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin Immunol. 2020;16:5. doi: 10.1186/s13223-020-0403-9[↩][↩]
- Hoy SM. Ciclosporin Ophthalmic Emulsion 0.1%: A Review in Severe Dry Eye Disease. Drugs. 2017;77:1909–1916. doi: 10.1007/s40265-017-0834-x[↩]
- Bielory L, Schoenberg D. Ocular allergy: update on clinical trials. Curr Opin Allergy Clin Immunol. 2010;19:495–502. doi: 10.1097/ACI.0000000000000564[↩]
- Amparo F, Dastjerdi MH, Okanobo A, Ferrari G, Smaga L, Hamrah P, Jurkunas U, Schaumberg DA, Dana R. Topical interleukin 1 receptor antagonist for treatment of dry eye disease: a randomized clinical trial. JAMA Ophthalmol. 2013;131:715–723. doi: 10.1001/jamaophthalmol.2013.195[↩]
- Tauber J, Karpecki P, Latkany R, Luchs J, Martel J, Sall K, Raychaudhuri A, Smith V, Semba CP; OPUS-2 Investigators. Lifitegrast Ophthalmic Solution 5.0% versus Placebo for Treatment of Dry Eye Disease: Results of the Randomized Phase III OPUS-2 Study. Ophthalmology. 2015;122:2423–2431. doi: 10.1016/j.ophtha.2015.08.001[↩]
- Iyer G, Agarwal S, Srinivasan B. Outcomes and Rationale of Excision and Mucous Membrane Grafting in Palpebral Vernal Keratoconjunctivitis. Cornea. 2018;37:172–176. doi: 10.1097/ICO.0000000000001421[↩]
- Nishiwaki-Dantas MC, Dantas PE, Pezzutti S, Finzi S. Surgical resection of giant papillae and autologous conjunctival graft in patients with severe vernal keratoconjunctivitis and giant papillae. Ophthalmic Plast Reconstr Surg. 2000;16:438–442. doi: 10.1097/00002341-200011000-00007[↩]
- Guo P, Kheirkhah A, Zhou WW, Qin L, Shen XL. Surgical resection and amniotic membrane transplantation for treatment of refractory giant papillae in vernal keratoconjunctivitis. Cornea. 2013;32:816–820. doi: 10.1097/ICO.0b013e31826a1e53[↩]
- Jabbehdari S, Starnes TW, Kurji KH, Eslani M, Cortina MS, Holland EJ, Djalilian AR. Management of advanced ocular surface disease in patients with severe atopic keratoconjunctivitis. Ocul Surf. 2019;17:303–309. doi: 10.1016/j.jtos.2018.12.002[↩]
- Brémond-Gignac D, Nischal KK, Mortemousque B, Gajdosova E, Granet DB, Chiambaretta F. Atopic Keratoconjunctivitis in Children: Clinical Features and Diagnosis. Ophthalmology. 2016 Feb;123(2):435-437. doi: 10.1016/j.ophtha.2015.07.012[↩][↩]
- Villegas BV, Benitez-Del-Castillo JM. Current Knowledge in Allergic Conjunctivitis. Turk J Ophthalmol. 2021 Feb 25;51(1):45-54. doi: 10.4274/tjo.galenos.2020.11456[↩][↩]
- Aboobacker S, Harris BW, Limaiem F. Lichenification. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537332[↩]
- Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016 Mar 12;387(10023):1109-1122. doi: 10.1016/S0140-6736(15)00149-X[↩]
- Mehta JS, Chen WL, Cheng ACK, Cung LX, Dualan IJ, Kekunnaya R, Khaliddin N, Kim TI, Lam DK, Leo SW, Manurung F, Tesavibul N, Bremond-Gignac D. Diagnosis, Management, and Treatment of Vernal Keratoconjunctivitis in Asia: Recommendations From the Management of Vernal Keratoconjunctivitis in Asia Expert Working Group. Front Med (Lausanne). 2022 Aug 1;9:882240. doi: 10.3389/fmed.2022.882240[↩]
- Atopy. https://dermnetnz.org/topics/atopy[↩][↩]
- Gupta J, Johansson E, Bernstein JA, Chakraborty R, Khurana Hershey GK, Rothenberg ME, Mersha TB. Resolving the etiology of atopic disorders by using genetic analysis of racial ancestry. J Allergy Clin Immunol. 2016 Sep;138(3):676-699. doi: 10.1016/j.jaci.2016.02.045[↩]
- Stone KD, Prussin C, Metcalfe DD. IgE, mast cells, basophils, and eosinophils. J Allergy Clin Immunol. 2010 Feb;125(2 Suppl 2):S73-80. doi: 10.1016/j.jaci.2009.11.017[↩]
- Enríquez-de-Salamanca A, Calder V, Gao J, Galatowicz G, García-Vázquez C, Fernández I, Stern ME, Diebold Y, Calonge M. Cytokine responses by conjunctival epithelial cells: an in vitro model of ocular inflammation. Cytokine. 2008 Oct;44(1):160-7. doi: 10.1016/j.cyto.2008.07.007[↩]
- Metz DP, Hingorani M, Calder VL, Buckley RJ, Lightman SL. T-cell cytokines in chronic allergic eye disease. J Allergy Clin Immunol. 1997 Dec;100(6 Pt 1):817-24. doi: 10.1016/s0091-6749(97)70279-3[↩]
- Hu Y, Adan ES, Matsumoto Y, Dogru M, Fukagawa K, Takano Y, Tsubota K, Fujishima H. Conjunctival in vivo confocal scanning laser microscopy in patients with atopic keratoconjunctivitis. Mol Vis. 2007 Aug 10;13:1379-89.[↩][↩]
- Chen JJ, Applebaum DS, Sun GS, Pflugfelder SC. Atopic keratoconjunctivitis: A review. J Am Acad Dermatol. 2014 Mar;70(3):569-75. doi: 10.1016/j.jaad.2013.10.036[↩][↩][↩][↩]
- Chen JJ, Applebaum DS, Sun GS, Pflugfelder SC. Atopic keratoconjunctivitis: a review. J Am Acad Dermatol. 2014;70:569–575. doi: 10.1016/j.jaad.2013.10.036[↩]
- Takamura E, et al. Japanese guideline for allergic conjunctival diseases. Allergol Int. 2011;60:191–203. doi: 10.2332/allergolint.11-RAI-0335[↩]
- Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66 Suppl 1:8-16. doi: 10.1159/000370220[↩][↩]
- Dom S, Droste JH, Sariachvili MA, Hagendorens MM, Oostveen E, Bridts CH, Stevens WJ, Wieringa MH, Weyler JJ. Pre- and post-natal exposure to antibiotics and the development of eczema, recurrent wheezing and atopic sensitization in children up to the age of 4 years. Clin Exp Allergy. 2010 Sep;40(9):1378-87. doi: 10.1111/j.1365-2222.2010.03538.x[↩]
- Power WJ, Tugal-Tutkun I, Foster CS. Long-term follow-up of patients with atopic keratoconjunctivitis. Ophthalmology. 1998 Apr;105(4):637-42. doi: 10.1016/S0161-6420(98)94017-9[↩][↩][↩][↩][↩]
- Vaidyanathan U, Hopping GC, Liu HY, Somani AN, Ronquillo YC, Hoopes PC, Moshirfar M. Persistent Corneal Epithelial Defects: A Review Article. Med Hypothesis Discov Innov Ophthalmol. 2019 Fall;8(3):163-176.[↩]
- Liu A, Manche EE. Bilateral posterior subcapsular cataracts associated with long-term intranasal steroid use. J Cataract Refract Surg. 2011 Aug;37(8):1555-8. doi: 10.1016/j.jcrs.2011.05.020[↩]
- Wang T, Moinuddin O, Abuzaitoun R, Hwang M, Besirli C, Wubben TJ, Zacks DN. Retinal Detachment After Endophthalmitis: Risk Factors and Outcomes. Clin Ophthalmol. 2021 Apr 13;15:1529-1537. doi: 10.2147/OPTH.S302757[↩]
- Hanet MS, Zimpfer A, Lepper S, Seitz B. Keratoconus-like tomographic changes in a case of recurrent interstitial keratitis. J Ophthalmic Inflamm Infect. 2018 Mar 7;8(1):4. doi: 10.1186/s12348-018-0146-7[↩]
- Garrity JA, Liesegang TJ. Ocular complications of atopic dermatitis. Can J Ophthalmol. 1984 Feb;19(1):21-4.[↩]
- Easty D, Entwistle C, Funk A, Witcher J. Herpes simplex keratitis and keratoconus in the atopic patient. A clinical and immunological study. Trans Ophthalmol Soc U K (1962). 1975 Jul;95(2):267-76.[↩]
- Kallen C, Reinhard T, Schilgen G, Cartsburg O, Böcking A, Auw-Hädrich C, Sundmacher R. Atopische KeratokonjunktivitisWahrscheinlich ein Risikofaktor für die Entstehung von Bindehautkarzinomen [Atopic keratoconjunctivitis: probably a risk factor for the development of conjuntival carcinoma]. Ophthalmologe. 2003 Oct;100(10):808-14. German. doi: 10.1007/s00347-003-0809-z[↩]
- Heinz C, Fanihagh F, Steuhl KP. Squamous cell carcinoma of the conjunctiva in patients with atopic eczema. Cornea. 2003 Mar;22(2):135-7. doi: 10.1097/00003226-200303000-00011[↩]
- Different Types of Cataracts. https://insighteye.com.au/different-types-cataracts/[↩]
- Keratoconus. https://www.vrmny.com/conditions/keratoconus/[↩]
- Prakash G, Avadhani K, Srivastava D. The three faces of herpes simplex epithelial keratitis: a steroid-induced situation. BMJ Case Rep. 2015 Apr 2;2015:bcr2014209197. doi: 10.1136/bcr-2014-209197[↩]
- Azari AA, Arabi A. Conjunctivitis: A Systematic Review. J Ophthalmic Vis Res. 2020 Aug 6;15(3):372-395. doi: 10.18502/jovr.v15i3.7456[↩]
- Guglielmetti S, Dart JK, Calder V. Atopic keratoconjunctivitis and atopic dermatitis. Curr Opin Allergy Clin Immunol. 2010 Oct;10(5):478-85. doi: 10.1097/ACI.0b013e32833e16e4[↩]
- Correale CE, Walker C, Murphy L, Craig TJ. Atopic dermatitis: a review of diagnosis and treatment. Am Fam Physician. 1999 Sep 15;60(4):1191-8, 1209-10. https://www.aafp.org/pubs/afp/issues/1999/0915/p1191.html[↩]
- Inada N, Shoji J, Kato H, Kiely S, Mulyanto, Sawa M. Clinical evaluation of total IgE in tears of patients with allergic conjunctivitis disease using a novel application of the immunochromatography method. Allergol Int. 2009 Dec;58(4):585-9. doi: 10.2332/allergolint.09-OA-0101[↩]
- Takano Y, Fukagawa K, Dogru M, Asano-Kato N, Tsubota K, Fujishima H. Inflammatory cells in brush cytology samples correlate with the severity of corneal lesions in atopic keratoconjunctivitis. Br J Ophthalmol. 2004 Dec;88(12):1504-5. doi: 10.1136/bjo.2004.047167[↩]
- Wakamatsu TH, Tanaka M, Satake Y, Dogru M, Fukagawa K, Igarashi A, Fujishima H. Eosinophil cationic protein as a marker for assessing the efficacy of tacrolimus ophthalmic solution in the treatment of atopic keratoconjunctivitis. Mol Vis. 2011 Apr 13;17:932-8. https://pmc.ncbi.nlm.nih.gov/articles/PMC3084241/[↩]
- Foster CS, Rice BA, Dutt JE. Immunopathology of atopic keratoconjunctivitis. Ophthalmology. 1991 Aug;98(8):1190-6. doi: 10.1016/s0161-6420(91)32154-7[↩]
- Phlyctenular Keratoconjunctivitis. https://eyewiki.org/Phlyctenular_Keratoconjunctivitis[↩]
- Gaddie IB, Donnenfeld ED, Karpecki P, Vollmer P, Berdy GJ, Peterson JD, Simmons B, Edell ARP, Whitson WE, Ciolino JB, Baba SN, Holdbrook M, Trevejo J, Meyer J, Yeu E; Saturn-2 Study Group. Lotilaner Ophthalmic Solution 0.25% for Demodex Blepharitis: Randomized, Vehicle-Controlled, Multicenter, Phase 3 Trial (Saturn-2). Ophthalmology. 2023 Oct;130(10):1015-1023. doi: 10.1016/j.ophtha.2023.05.030[↩]
- Putnam CM. Diagnosis and management of blepharitis: an optometrist’s perspective. Clin Optom (Auckl). 2016 Aug 8;8:71-78. doi: 10.2147/OPTO.S84795[↩]
- Al-Amri AM. Long-term follow-up of tacrolimus ointment for treatment of atopic keratoconjunctivitis. Am J Ophthalmol. 2014 Feb;157(2):280-6. doi: 10.1016/j.ajo.2013.10.006[↩]
- González-López JJ, López-Alcalde J, Morcillo Laiz R, Fernández Buenaga R, Rebolleda Fernández G. Topical cyclosporine for atopic keratoconjunctivitis. Cochrane Database Syst Rev. 2012 Sep 12;(9):CD009078. doi: 10.1002/14651858.CD009078.pub2[↩]
- Erdinest N, Noyman DBE, London N, Lavy I, Levinger N, Landau D, Solomon A, Morad Y, Naroo SA. Applications of topical immunomodulators enhance clinical signs of vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis (AKC): a meta-analysis. Int Ophthalmol. 2024 Mar 24;44(1):157. doi: 10.1007/s10792-024-03097-7[↩]
- Munro CS, Levell NJ, Shuster S, Friedmann PS. Maintenance treatment with cyclosporin in atopic eczema. Br J Dermatol. 1994 Mar;130(3):376-80. doi: 10.1111/j.1365-2133.1994.tb02936.x[↩]
- Salek MS, Finlay AY, Luscombe DK, Allen BR, Berth-Jones J, Camp RD, Graham-Brown RA, Khan GK, Marks R, Motley RJ, et al. Cyclosporin greatly improves the quality of life of adults with severe atopic dermatitis. A randomized, double-blind, placebo-controlled trial. Br J Dermatol. 1993 Oct;129(4):422-30. doi: 10.1111/j.1365-2133.1993.tb03170.x[↩]
- Zaouali S, Kahloun R, Attia S, Jelliti B, Trigui M, Yahia SB, Messaoud R, Khairallah M. Supratarsal injection of triamcinolone acetonide and childhood allergic keratoconjunctivitis. Int Ophthalmol. 2012 Apr;32(2):99-106. doi: 10.1007/s10792-011-9421-4[↩]
- Koçluk Y, Yalniz-Akkaya Z, Burcu A, Örnek F. Atopic keratoconjunctivitis: long-term results of medical treatment and penetrating keratoplasty. Arq Bras Oftalmol. 2016 Nov-Dec;79(6):376-379. doi: 10.5935/0004-2749.20160107[↩][↩]
- Atopic Keratoconjunctivitis (AKC). https://emedicine.medscape.com/article/1194480-overview[↩][↩][↩]




{kind=link}