Contents
- Constrictive pericarditis
- What is the pericardium?
- Constrictive pericarditis types
- Constrictive pericarditis cause
- Constrictive pericarditis pathophysiology
- Constrictive pericarditis signs and symptoms
- Constrictive pericarditis diagnosis
- Constrictive pericarditis differential diagnosis
- Constrictive pericarditis management
- Constrictive pericarditis prognosis
Constrictive pericarditis
Constrictive pericarditis also called restrictive pericarditis is a chronic (long-term) condition that causes the pericardium or the pericardial sac (a double-walled sac containing serous fluid that surrounds your heart and helps your heart function properly) to thicken and stiffen, making it difficult for your heart to pump blood 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. This interferes with your heart’s pumping ability and can lead to severe problems like heart failure. Constrictive pericarditis is usually a chronic (long-term) problem, but it is treatable in most cases, especially with early diagnosis.
The pericardium is a fluid-filled membrane with two layers (inner layer called visceral pericardium and outer layer called parietal pericardium) that surrounds your heart (see Figures 1 and 2 below). Part of your pericardium’s job is to hold your heart in place. There’s also a layer of fluid inside the pericardium between it and your heart. That fluid helps cushion your heart and protect it from injury. Under normal circumstances, the pericardium is flexible and stretchy. That means your heart doesn’t have any trouble expanding to fill up with blood between heartbeats. However, when you have constrictive pericarditis the pericardium is stiffer and thicker than normal. This makes it hard for your heart to expand properly as it should when it beats. When your heart can’t expand enough to fill up with blood, it struggles to pump enough to meet your body’s needs. To compensate, blood backs up behind your heart and the filling pressures increase, which leads to heart failure and other symptoms of heart failure.
Constrictive pericarditis symptoms may include shortness of breath (dyspnea) that develops slowly and gets worse over time, fatigue or general feeling of weakness or being sick, swelling in your legs and ankles (edema), swelling of your abdomen (ascites) and weakness.
Constrictive pericarditis is most likely to happen to people who have a history of heart surgery, radiation therapy around their heart, or idiopathic (idiopathic means “unknown” cause) or viral pericarditis. In developing countries, tuberculosis (TB) is the most common cause. Constrictive pericarditis is two to three times more likely to happen to men than women. Constrictive pericarditis is also extremely rare in children.
Constrictive pericarditis is a rare condition overall. It happens to about 9% of people with acute pericarditis, and acute pericarditis accounts for about 5% of all chest pain-related emergency room visits. In a 2019 report of annual trends of patients admitted to US hospitals with constrictive pericarditis from 2005 to 2014, investigators found a stable prevalence of 9-10 cases per million admissions 12. There appears to be a male predominance, with some studies report a male-to-female ratio of 3:1. No racial predilection exists for constrictive pericarditis. Between 2005 and 2014, patients with constrictive pericarditis who underwent pericardiectomy were younger, more likely to be male, and had fewer comorbidities than those who received medical management 12.
Constrictive pericarditis has multiple possible causes and in many cases, no causes or etiology can be found (idiopathic). All forms of pericarditis may eventually lead to constrictive pericarditis.
Common causes of constrictive pericarditis may include:
- Idiopathic (unknown cause). Constrictive pericarditis can happen for unknown reasons. Doctors often assume these cases happen because of a viral infection or group unknown and viral causes together for statistical reasons.
- Infection (bacterial or viral). In developing countries, constrictive pericarditis are usually cause by bacterial infections, especially tuberculosis (constrictive pericarditis happens in 20% to 30% of tuberculosis-related cases of pericarditis) 13. In developed countries, viral infections are more likely to cause constrictive pericarditis with 40% to 60% of total cases.
- Medical procedures and treatments. Pericardial thickening or scarring can happen after heart surgery, radiation therapy for cancer or as a side effect of some medications.
Less common causes of constrictive pericarditis include:
- Immune system conditions or connective tissue disorders. Examples of these conditions include lupus, systemic lupus erythematosus (SLE), scleroderma, rheumatoid arthritis or Sjögren’s syndrome.
- Heart and circulatory problems. This includes heart attacks or other conditions that affect the major blood vessels closest to your heart.
- Trauma. Injuries to your chest either blunt impacts or penetration injuries like knife or bullet wounds can cause inflammation that leads to scar tissue formation around your heart sac.
- Cancer. This includes either cancer of the pericardium itself or cancer from somewhere else in your body e.g. mesothelioma.
Constrictive pericarditis is sometimes difficult to diagnose, especially when the symptoms aren’t severe or when you have other conditions with similar or related symptoms. Your heart doctor (cardiologist) can diagnose constrictive pericarditis based on a combination of your symptoms, your medical history, a physical examination and diagnostic tests. However, the diagnostic challenge lies in distinguishing constrictive pericarditis from restrictive cardiomyopathy (a rare heart disease that occurs when the heart muscle becomes stiff and doesn’t relax properly, preventing the heart from filling with blood and pumping effectively).
The diagnosis of constrictive pericarditis is challenging as there are currently no standard echocardiographic diagnostic criteria 4. If a doctor or cardiologist suspects you have constrictive pericarditis, the following tests may be performed:
- Testing for tuberculosis (TB).
- Electrocardiogram (ECG or EKG). An electrocardiogram is a quick and painless test that records the electrical signals in the heart. It can show how the heart is beating. Sticky patches called electrodes with wires attach to the chest and sometimes the arms or legs. The wires connect to a monitor, which prints or displays results. There are no specific signs of constrictive pericarditis on ECG which may reveal nonspecific ST changes and low voltage. Advanced and long-standing cases may show atrial fibrillation (AF) secondary to elevated atrial pressures.
- Chest X-ray. A chest X-ray can show changes in the size and shape of the heart. It can tell if the heart is enlarged.
- Echocardiogram. Sound waves create images of the moving heart. An echocardiogram shows how well the heart is pumping blood. It also can see any fluid buildup in the tissue surrounding the heart. The test can tell if the sac surrounding the heart affects the way the heart fills with blood or pumps blood.
- Heart computerized tomography (CT) scan. Cardiac CT scans use X-rays to create images of the heart and chest. The test can be used to look for heart thickening that may be a sign of constrictive pericarditis.
- Heart magnetic resonance imaging (MRI). This test uses magnetic fields and radio waves to create detailed images of the heart. A cardiac MRI scan can show thickening, inflammation or other changes in the thin tissue surrounding the heart.
- Left and right heart catheterization.
Constrictive pericarditis is usually treatable. In most cases, curing constrictive pericarditis involves two main principles:
- Relieving pressure on your heart happens because the pericardium can’t stretch.
- Treating underlying causes or related symptoms.
Most of the time, constrictive pericarditis treatment involves the following:
- Surgery. Pericardiectomy, which removes all of the pericardium, usually offers the best chance to treat constrictive pericarditis successfully. You don’t need your pericardium to survive, and many people return to their normal lives without any difficulty or long-term effects.
- Potential complications from surgery include:
- Heart failure.
- Irregular heart rhythms (arrhythmias).
- Infections and sepsis.
- Death.
- Potential complications from surgery include:
- Medication. Depending on the underlying cause and symptoms, different medications can help treat constrictive pericarditis symptoms directly or try to cure it by stopping whatever is causing it to happen. In some cases, medications are enough to treat constrictive pericarditis, avoiding the need for surgery, or they can help manage symptoms for people who can’t have surgery.
The most common medications for the treatment of constrictive pericarditis include:
- Diuretics (water pills). There are several categories of diuretics. All diuretics help your kidneys remove extra fluid from your body.
- Non-steroidal anti-inflammatory drugs (NSAIDs). Non-steroidal anti-inflammatory drugs (NSAIDs) help reduce inflammation and relieve pain. Examples of these include ibuprofen or naproxen.
- Steroids also called corticosteroids. Steroids are a man-made version of hormones normally produced by your adrenal glands which are 2 small glands found above the kidneys. Steroids are anti-inflammatory medicines that reduce redness and swelling (inflammation). This can help with inflammatory conditions.
- Cause-specific medications. Examples of these include antibiotics for bacterial infections like tuberculosis.
Figure 1. Pericardium
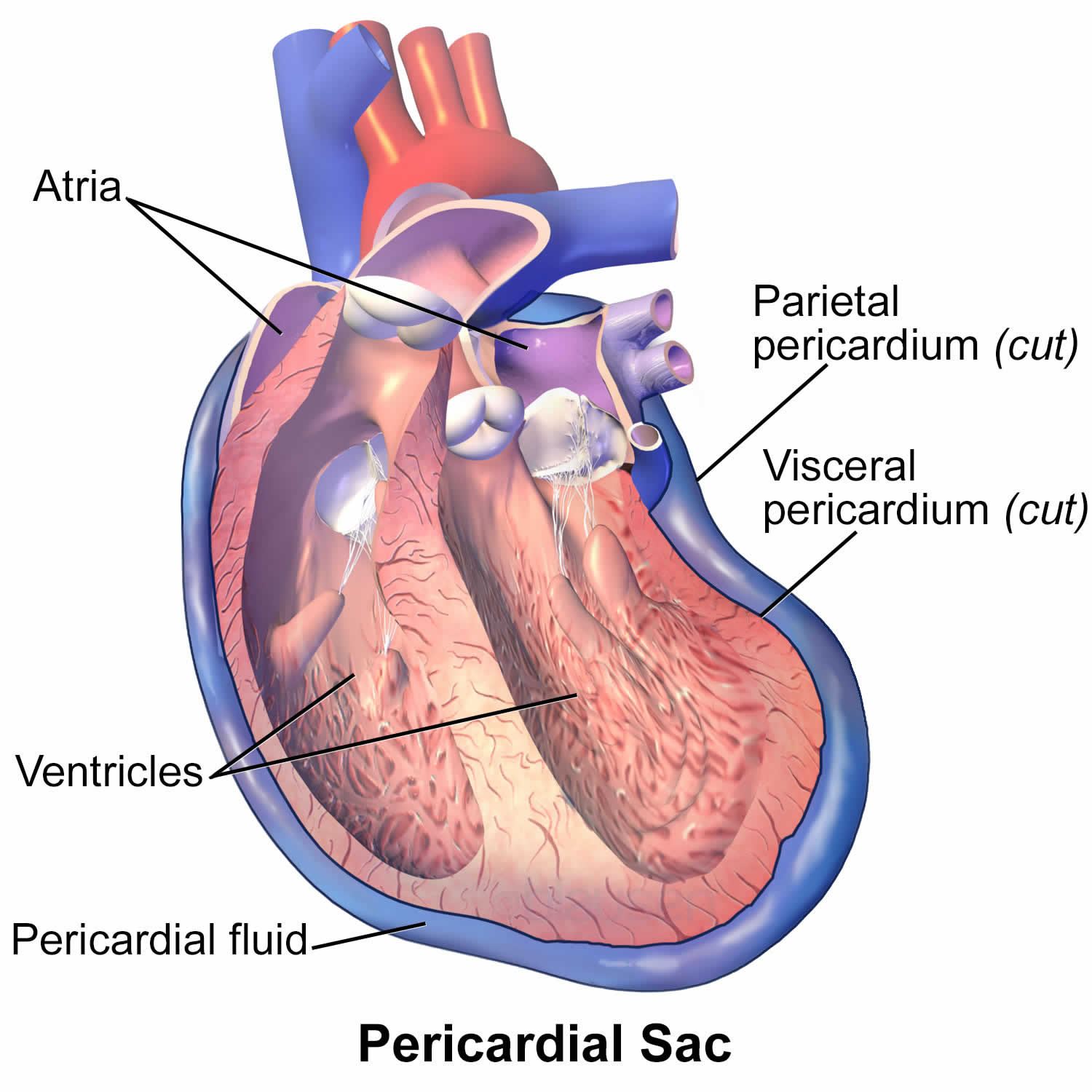
Figure 2. Heart wall layers
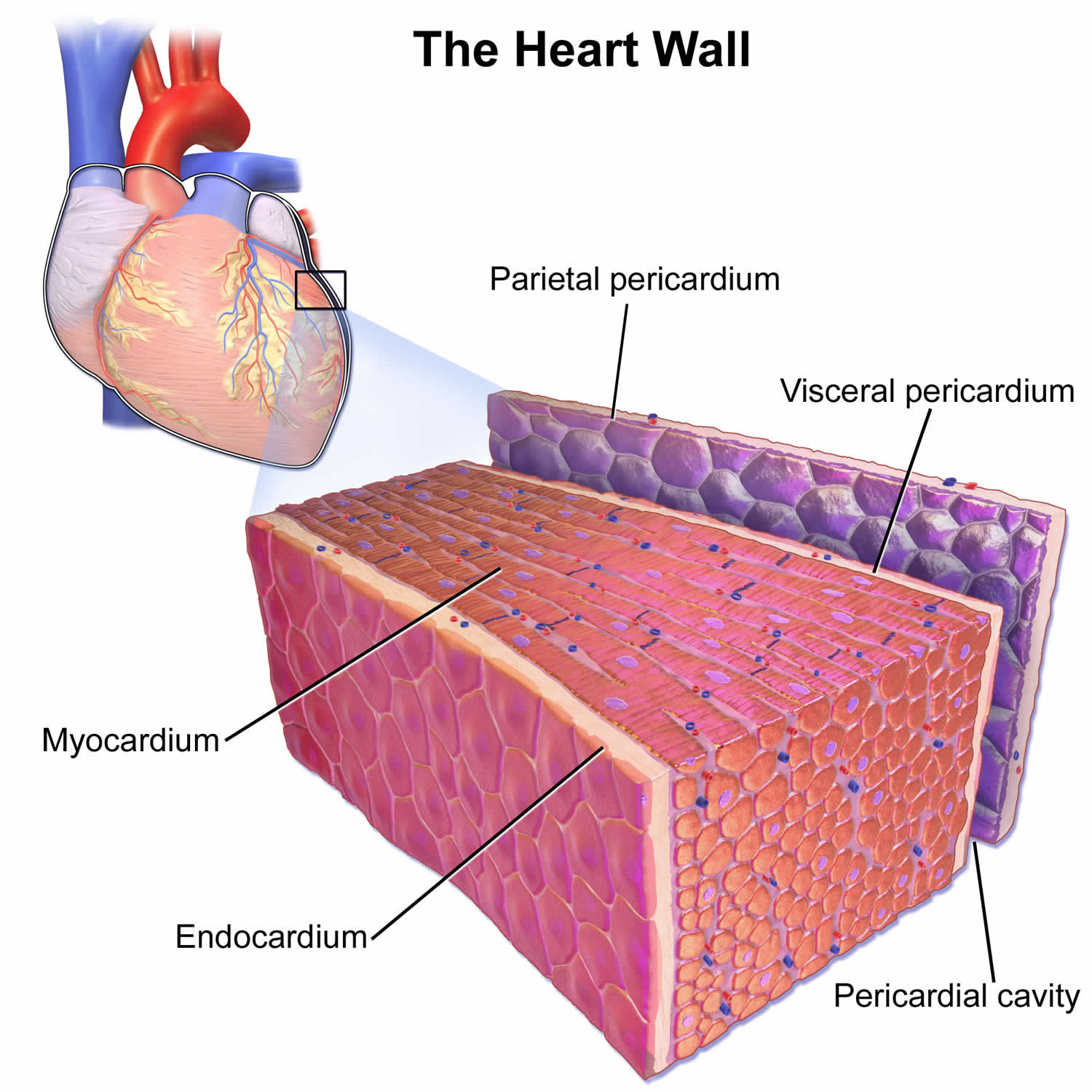
Figure 3. Constrictive pericarditis
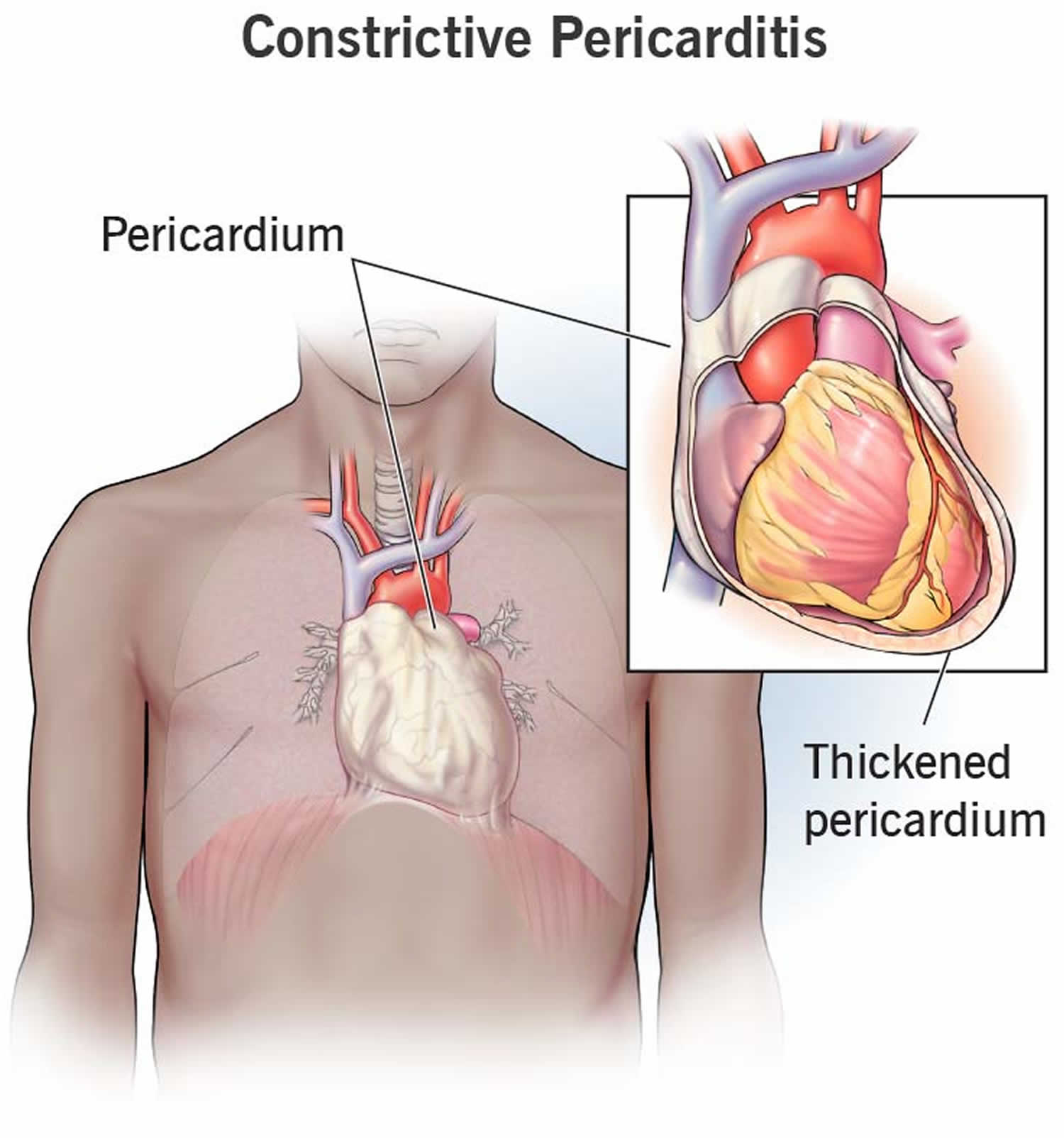
Figure 4. Constrictive pericarditis echocardiography
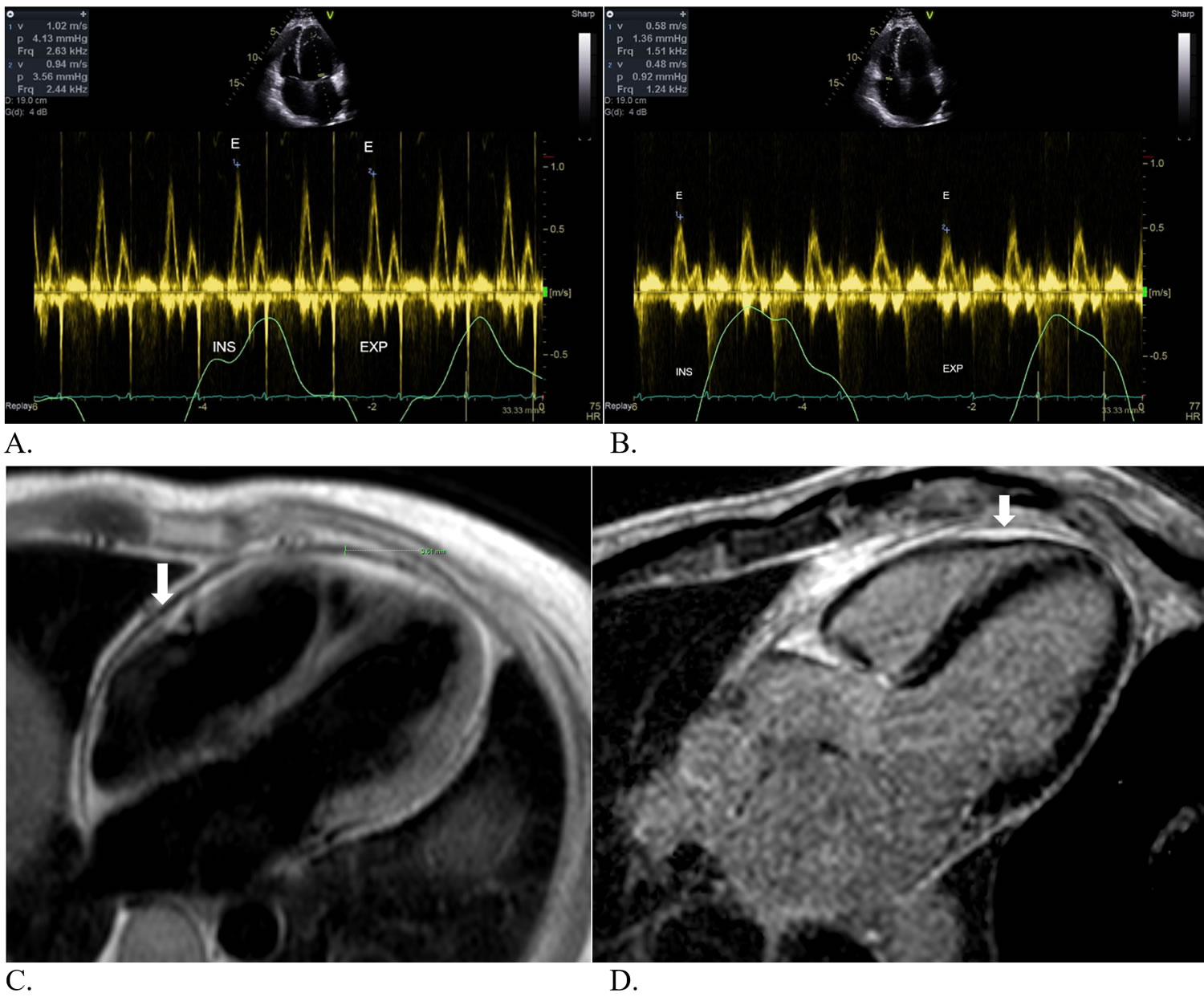
Footnotes: (A) Mild variation of mitral inflow Doppler. (B) Mild variation of tricuspid inflow Doppler. (C) Mild pericardial thickening on axial black blood images. (D) Delayed pericardial enhancement, particularly around the right ventricle (arrow). Patient is a 47-year-old male with a past medical history significant for hypertension and obesity who presents to clinic with shortness of breath, swelling of both lower extremities and abdomen as well as intermittent low-grade fevers. Prior to clinic presentation (8 months prior), he was seen at an outside health care facility where he underwent an extensive work-up including computed tomography (CT) of his chest/abdomen/pelvis as well as echocardiogram. He was found to have a small pericardial effusion at that time. He was also found to have an elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). He was ultimately diagnosed with viral pericarditis and treated with colchicine, ibuprofen, and oral Lasix. He was monitored locally and was found to have improving inflammatory markers but unfortunately had worsening volume overload and was admitted to his local hospital with decompensated heart and renal failure. He underwent a right heart catheterization during this admission revealing elevated right and left sided intra-cardiac filling pressures with a preserved cardiac index. His pericardial effusion was found to be enlarging for which he underwent a pericardial window with 400 cc of fluid drained. Tissue biopsy from the pericardium revealed chronic fibrous constrictive pericarditis and chronic lymphocytic pericarditis. At that time he was diuresed to euvolemia and discharged home with a 6-month prednisone taper. Colchicine and ibuprofen were discontinued due to renal failure. His symptoms significantly improved while taking prednisone. Unfortunately, his symptoms recurred after finishing the prednisone for which he presented to Cleveland Clinic for a second opinion.
[Source 14 ]Figure 5. Constrictive pericarditis echocardiogram
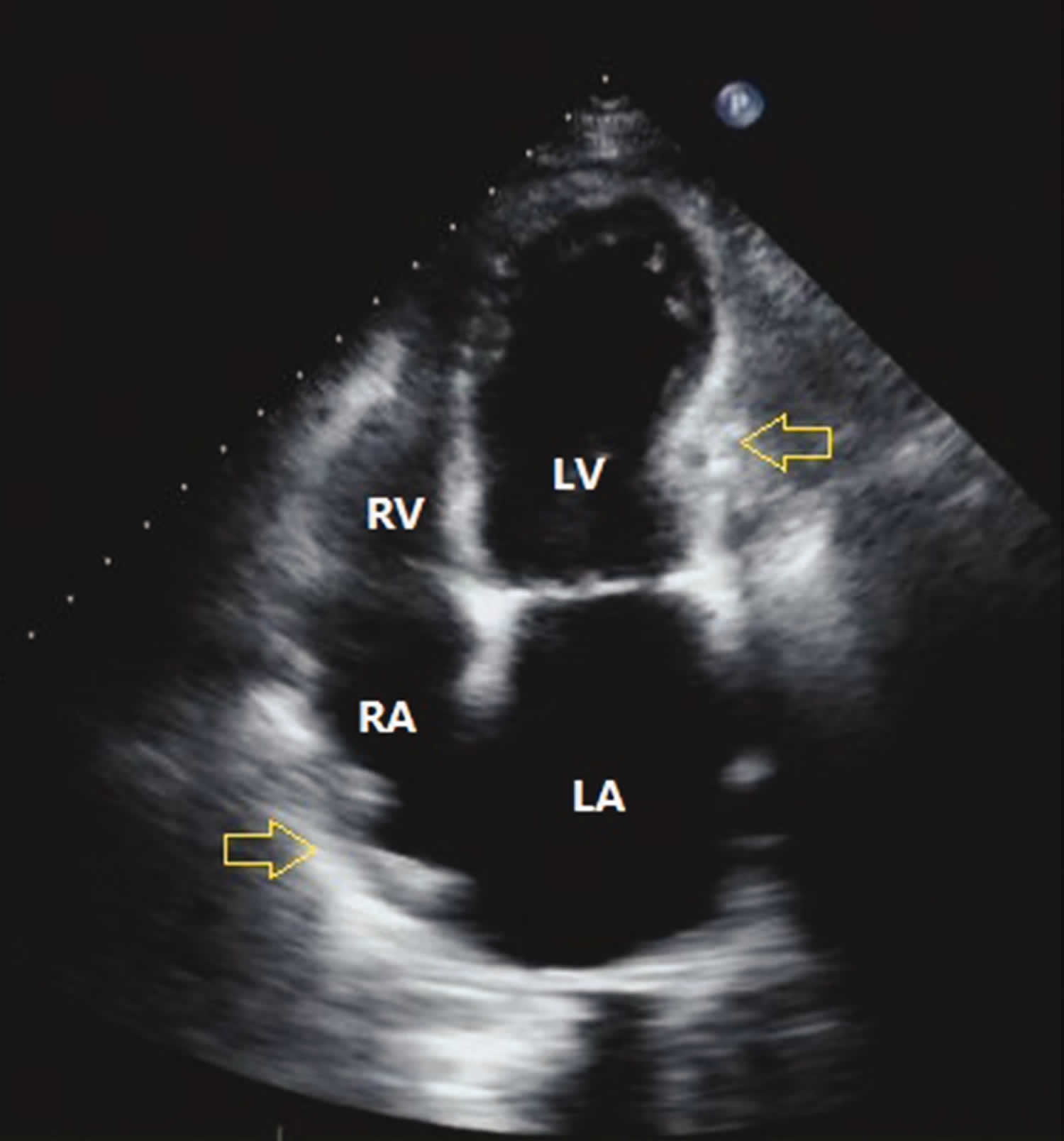
Footnote: Pericardial calcification (yellow arrow) and the resulting abnormal cardiac morphology in a patient with constrictive pericarditis.
Abbreviations: CP = constrictive pericarditis; RV = right ventricle; LV = left ventricle; RA = right atrium; LA = left atrium.
[Source 4 ]Figure 6. Constrictive pericarditis M-mode echocardiography
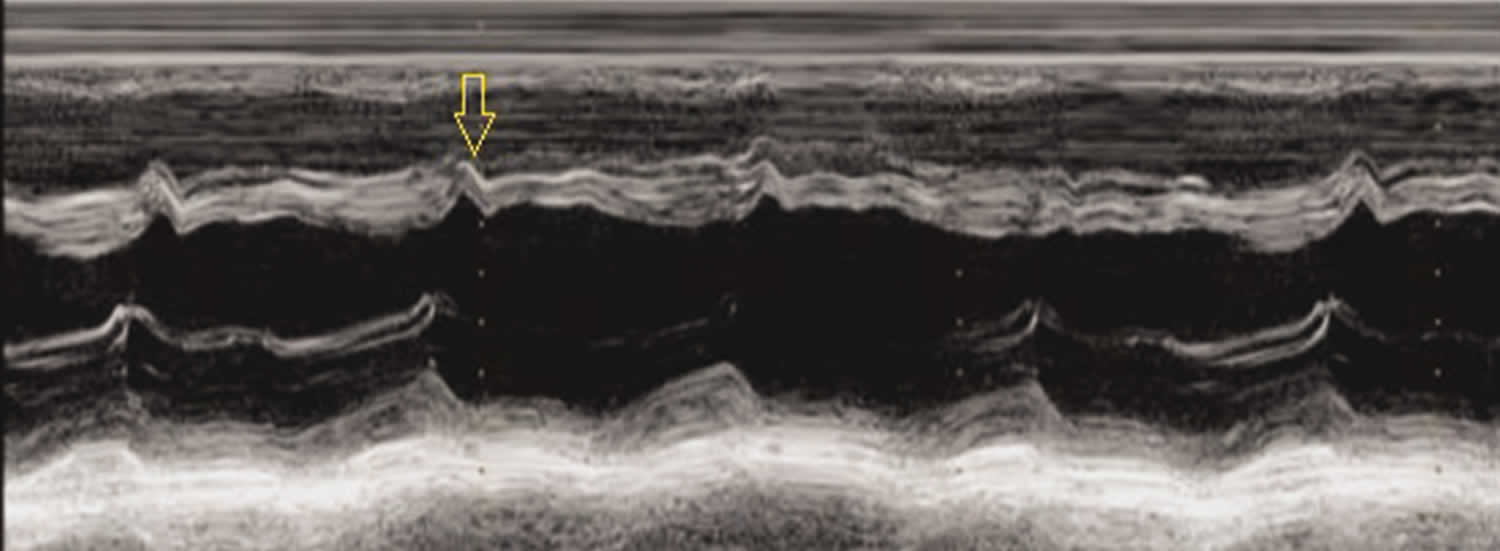
Footnote: M-mode echocardiography of a patient with constrictive pericarditis. An obvious V-shaped cut (yellow arrow) is seen.
[Source 4 ]Figure 7. Constrictive pericarditis doppler echocardiography
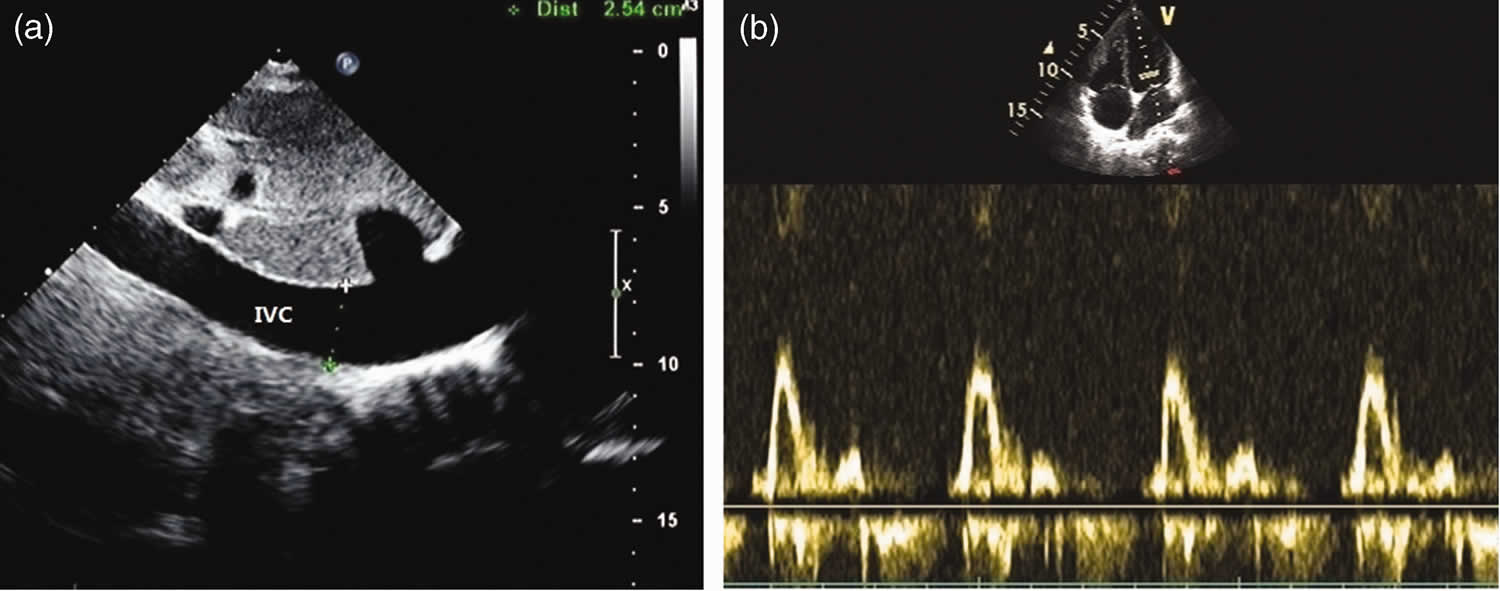
Footnotes: Restrictive ventricular diastolic filling pattern in a patient with constrictive pericarditis; (a) dilated IVC (2.5 cm) in the subxiphoid view and (b) mitral inflow wave: E/A: 3.6, DT: 71 ms.
Abbreviations: CP = constrictive pericarditis; IVC = inferior vena cava; E/A = early (E) velocity to atrial (A) wave ratio; DT = deceleration time; V = ventricle.
[Source 4 ]Figure 8. Constrictive pericarditis echocardiography
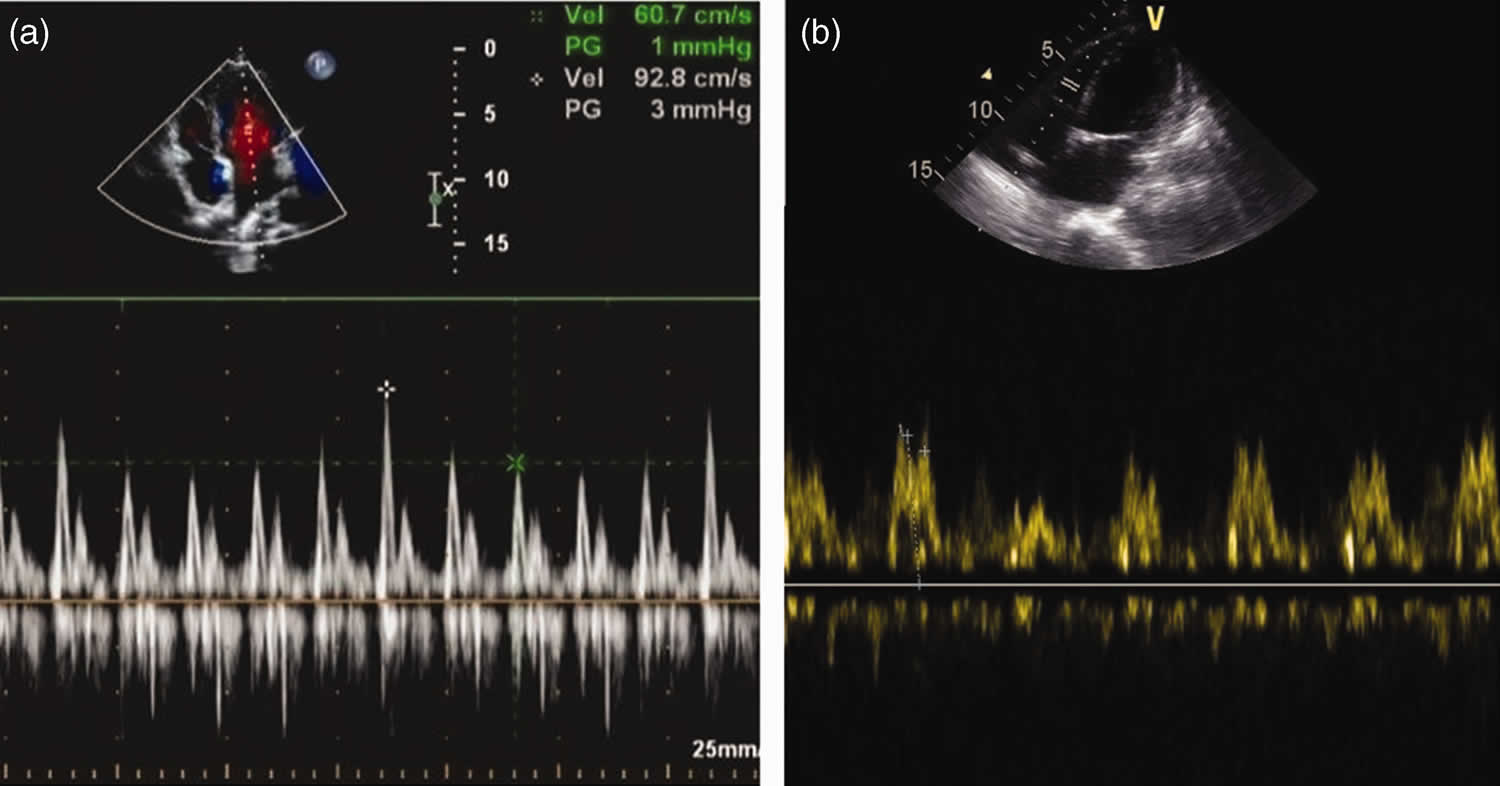
Footnotes: Mitral and tricuspid inflow pulse waves in patients with constrictive pericarditis. (a) The variability rates in expiration and inspiration were 34% (mitral inflow) and (b) 40% (tricuspid inflow) respectively.
Abbreviations: Vel = velocity; PG = pressure gradient; V = ventricle.
[Source 4 ]Get medical care right away if you have new symptoms of chest pain. Many of the symptoms of pericarditis are like those of other heart and lung conditions. It’s important to be thoroughly checked by a doctor if you have any type of chest pain.
Many of the symptoms of constrictive pericarditis also happen with life-threatening medical emergencies. Because of that, you should get medical care immediately if you have any of the following symptoms:
- Shortness of breath (dyspnea).
- Chest pain.
- Dizziness or feeling lightheaded.
- Fainting or passing out.
Is constrictive pericarditis contagious?
No. While constrictive pericarditis can happen because of infections (some of which are potentially contagious), constrictive pericarditis isn’t contagious on its own.
How common is constrictive pericarditis?
Approximately 9% of patients with acute pericarditis from any cause go on to develop constrictive pericarditis 15. The true frequency is dependent on the incidence of the specific causes of pericarditis, but given that acute pericarditis is clinically diagnosed in only 1 in 1000 hospital admissions, the frequency of a diagnosis of constrictive pericarditis is likely to be less than 1 in 10,000 admissions.
In a 2019 report of annual trends of patients admitted to US hospitals with constrictive pericarditis from 2005 to 2014, investigators found a stable prevalence of 9-10 cases per million admissions 12.
Although data for children are lacking for epidemiologic analysis, it is clear that constrictive pericarditis is rare in adults and even more rare in children. In all age groups, constrictive pericarditis prevalence is increased among patients who are hospitalized and among patients who have undergone heart surgery. Constrictive pericarditis cases have been reported in persons aged 8 to 70 years. Predilection is likely reflective of the underlying disease. Historical studies suggest a median age of 45 years, whereas more recent studies suggest a median age of 61 years (possibly reflecting ongoing demographic changes).
How can I prevent or reduce my risk of constrictive pericarditis?
Constrictive pericarditis happens unpredictably, so it’s not possible to prevent it. The only thing you can do to reduce your risk of developing constrictive pericarditis is to avoid situations that might lead to developing it. One example is getting bacterial infections treated quickly rather than delaying care. Another is for medical personnel to limit radiation damage to your pericardium if you receive radiation therapy.
How long does constrictive pericarditis last, and when can I resume my usual routine and activities?
How long constrictive pericarditis lasts depends on the type, cause and treatments you receive. In some cases, constrictive pericarditis goes away on its own or with medication only. That usually takes a few weeks to a few months. The more severe the case or cause, the longer it usually takes for you to recover.
What is the pericardium?
The pericardium is a tough fibroelastic fluid-filled sac or membrane that covers your heart from all sides except at the cardiac root (top of your heart) where the major blood vessels join your heart and the bottom where only the serous pericardium exists to cover the upper surface of the central tendon of the diaphragm (a muscle that separates your chest cavity from your abdomen and helps with breathing).
Your pericardium has 2 main layers:
- Fibrous pericardium: This is the tough, outermost layer of your pericardium. It’s made of connective tissue that prevents your heart from expanding too much. It attaches to your major blood vessels at the top of your heart and to the central tendon of your diaphragm at the bottom of your heart. At the front of your chest, ligaments connect this layer to your breastbone.
- Serous pericardium: This is the inner layer of your pericardium. It’s actually made of two layers, described below. Your serous pericardium produces pericardial fluid that lubricates your heart as it beats.
- Your serous pericardium is made of two layers:
- Parietal (outer) layer of the serous pericardium: This is the outer layer that’s firmly attached to your fibrous pericardium. There’s no space between them.
- Visceral (inner) layer of the serous pericardium: This is the innermost layer of your pericardium. It directly covers your heart and the roots of your great vessels. The portion that covers your heart is also known as your epicardium.
- Your serous pericardium is made of two layers:
The pericardial cavity is the space between the two layers of your serous pericardium. This space holds your pericardial fluid. Usually, approximately 50 mL of fluid (plasma ultrafiltrate) is present in the intrapericardial space to minimize friction during cardiac motion 16. Both of parietal and visceral serous pericardium layers function in lubricating your heart to prevent friction during heart activity.
Constrictive pericarditis types
Constrictive pericarditis has a few different subtypes:
- Acute constrictive pericarditis. Acute constrictive pericarditis type happens when scarring of the pericardium happens quickly, usually over a matter of days.
- Subacute constrictive pericarditis. Subacute constrictive pericarditis type is like acute constrictive pericarditis, but the symptoms aren’t as severe.
- Effusive constrictive pericarditis. Effusive constrictive pericarditis subtype causes pericardial effusion, a buildup of fluid inside the pericardium that can put too much pressure on your heart. That causes cardiac tamponade, where your heart can’t beat because fluid buildup takes up more and more space. Eventually, your heart stops because of the pressure from fluid around it. Effusive constriction happens when elevated filling pressures in the heart remain even after draining the extra fluid.
- Transient constrictive pericarditis. Transient constrictive pericarditis type usually involves acute pericarditis that turns into inflammatory constrictive pericarditis. This is treatable with anti-inflammatory medications.
- Occult constrictive pericarditis. In medicine, the term “occult” means “hidden”. This type of constrictive pericarditis carries that name because it’s hard to detect. Finding and diagnosing occult constrictive pericarditis usually happens by accident when running other tests.
Constrictive pericarditis cause
Constrictive pericarditis is the result of scarring of the pericardium and that your pericardium is stiffer or thicker than normal, consequently with loss of the normal elasticity of the pericardial sac, leading to restriction in ventricular filling. This stiffening of the pericardium can happen for several reasons, including:
- Infections. In developing countries, constrictive pericarditis are usually cause by bacterial infections, especially tuberculosis (constrictive pericarditis happens in 20% to 30% of tuberculosis-related cases of pericarditis). In developed countries, viral infections are more likely to cause constrictive pericarditis.
- Tuberculosis is the leading cause of constrictive pericarditis in developing nations but represents only a minority of causes in the United States and other developed countries. Tuberculous constrictive pericarditis is also known as “heart with shell”17. Tuberculous pericarditis has a high morbidity and mortality rate 18. Tuberculous constrictive pericarditis is secondary to exudative pericarditis and is usually caused by Mycobacterium tuberculosis bacteria 19. Tuberculous pericarditis is characterized by pericardial thickening, adhesion, fibrosis and calcification, which can impair diastolic function and lead to poor circulation. Surgical intervention is the most appropriate treatment for tuberculous constrictive pericarditis if the patient shows continuous clinical evidence after antituberculous therapy 20
. Pericardiectomy is the standard treatment for tuberculous constrictive pericarditis 21. - Bacterial infections that lead to purulent pericarditis are also declining in frequency. In the past, purulent pericarditis associated with pneumococcal pneumonia was the most common presentation of a bacterial source. However, the widespread use of antibiotics has drastically changed the frequency and spectrum of purulent pericarditis such that the most common presentation now occurs following cardiac surgery. It should be noted that the progression from acute pericarditis to constrictive pericarditis can occur more rapidly after bacterial pericarditis (e.g, ≤6 months in some cases). An increasing number of Gram-positive organisms, including multiple resistant strains of Staphylococci, may be isolated. Group A and B Streptococci and Gram-negative rods (eg, Pseudomonas species, Escherichia coli, and Klebsiella species) have also been documented.
- Although the absolute number of tuberculous and bacterial pericarditis cases are decreasing, it must be recognized that these processes remain closely associated with constrictive pericarditis. A prospective analysis determined that the incidence of constrictive pericarditis was 0.76 cases per 1,000 person-years after acute idiopathic/viral pericarditis but 31.7 cases per 1,000 person-years for acute tuberculous pericarditis and 52.7 cases per 1,000 person-years for purulent pericarditis 22.
- Viral pathogens that can cause constrictive pericarditis include coxsackievirus, hepatitis virus, adenovirus, and echovirus 15.
- Fungal infections are an uncommon source of constrictive pericarditis in patients who are immunocompetent. Nocardia species can be causative organisms, especially in endemic areas such as the Ohio Valley. Aspergillus, Candida, and Coccidioides species are important pathogens in patients infected with HIV and in other immunocompromised hosts.
- Tuberculosis is the leading cause of constrictive pericarditis in developing nations but represents only a minority of causes in the United States and other developed countries. Tuberculous constrictive pericarditis is also known as “heart with shell”17. Tuberculous pericarditis has a high morbidity and mortality rate 18. Tuberculous constrictive pericarditis is secondary to exudative pericarditis and is usually caused by Mycobacterium tuberculosis bacteria 19. Tuberculous pericarditis is characterized by pericardial thickening, adhesion, fibrosis and calcification, which can impair diastolic function and lead to poor circulation. Surgical intervention is the most appropriate treatment for tuberculous constrictive pericarditis if the patient shows continuous clinical evidence after antituberculous therapy 20
- Heart and circulatory problems. This includes heart attacks or other conditions that affect the major blood vessels closest to your heart.
- Trauma. Injuries to your chest either blunt impacts or penetration injuries like knife or bullet wounds can cause inflammation that leads to scar tissue formation around your heart sac.
- Immune system conditions or connective tissue disorders. Examples of these conditions include lupus, systemic lupus erythematosus (SLE), scleroderma, rheumatoid arthritis or Sjögren’s syndrome.
- Medical procedures and treatments. Pericardial thickening or scarring can happen after heart surgery, radiation therapy for cancer or as a side effect of some medications.
- Radiation therapy. The long-term effects of thoracic and mediastinal radiation therapy as used in the treatment of blood, breast, lung and other cancers are increasingly being recognized. The common features of radiation-induced heart complications stem from microcirculation injury with endothelial damage, capillary rupture, and platelet adhesion. This sets up an inflammatory response, which may either resolve or organize to form adhesions between the visceral pericardium and the parietal pericardium. This cascade potentially leads to constriction. Generally, radiation-induced constrictive pericarditis presents 5-10 years after radiation therapy and is more likely to present with an associated pericardial effusion. In a study by Bertog et al 23, the median time between radiation and pericardiectomy was 11 years, with a broad range of 2-30 years. These findings were consistent with those of other previous studies.
- Heart surgery. Any operative or invasive procedure in which the pericardium is opened, manipulated, or damaged may invoke an inflammatory response, leading to constrictive pericarditis (postpericardiotomy syndrome). The most common example is constrictive pericarditis in the setting of previous coronary artery bypass grafting (CABG) when only part of the pericardium is resected.
- Medications. Procainamide and hydralazine have been reported to cause constrictive pericarditis through a drug-induced lupuslike syndrome. Methysergide therapy also has been implicated as a cause of constrictive pericarditis.
- Constrictive pericarditis after implantation of an epicardial pacemaker or automated implantable cardiac defibrillator is a rare but reported phenomenon.
- In rare instances, constrictive pericarditis may occur after sclerotherapy for esophageal varices.
- Cancer. This includes either cancer of the pericardium itself or cancer from somewhere else in your body e.g. mesothelioma. Breast cancer and lung cancer and lymphomas are the metastatic malignancies most commonly associated with constrictive pericarditis. Other cancers that involve the pericardium with relative frequency include melanoma and mesothelioma.
- Uremia. Uremia is a buildup of waste products in your blood that occurs as a result of untreated kidney failure. Uremia occurs when your kidneys no longer filter properly. Uremia is likely to occur when a person is in the final stage of chronic kidney disease. Uremia with long-term hemodialysis can lead to constrictive pericarditis and is usually associated with a pericardial effusion.
- Mulibrey nanism is a very rare autosomal recessive genetic disorder that is characterized by multiple abnormalities, including dwarfism, constrictive pericarditis, abnormal fundi, and fibrous dysplasia of the long bones 24. Mulibrey is an acronym for MUscles, LIver, BRain, and EYes relating to the original clinical description of the disease. Nanism refers to the short stature (dwarfism) often observed in patients with this disorder. Mulibrey nanism is caused by a mutation in the TRIM37 gene. The growth delay usually begins before birth. Non-inflammatory constrictive pericarditis involving fibrotic overgrowth of the sac surrounding the heart is a common feature with a major impact on prognosis. Overgrowth of heart muscle walls (hypertrophy) may add to circulatory problems (congestive heart failure) in these patients as they get older. Short height and facial differences are commonly present. Radiologic findings include slender long bones with thick cortex, narrow medullary channel and fibrous dysplasia, J-shaped sella turcica and a small thoracic cage. The liver is usually enlarged. Additionally, fibrous tissue may build up on the interior of the lungs (pulmonary fibrosis) causing difficulty breathing. Weak muscle tone (hypotonia) is another symptom. The clinical presentation is very variable.
- Chylopericardium is a rare cause of constrictive pericarditis.
- Idiopathic. Constrictive pericarditis can happen for unknown reasons. Doctors often assume these cases happen because of a viral infection or group unknown and viral causes together for statistical reasons. Reports by many authors indicate that a high percentage of idiopathic cases of constrictive pericarditis may be related to previously recognized or unrecognized viral pericarditis 25.
The top 3 causes of constrictive pericarditis are idiopathic (presumably viral), cardiothoracic surgery, and radiation therapy, which, according to one study, are responsible for 46%, 37%, and 9% of cases of constrictive pericarditis, respectively (in patients who underwent surgical therapy of their constriction) 23.
Constrictive pericarditis pathophysiology
In constrictive pericarditis, the easily expandable, thin parietal and visceral pericardial linings become inflamed, thickened, and fused during healing of an acute episode of fibrinous or serofibrinous pericarditis or resorption of chronic pericardial effusion. The granulation tissue gradually contracts over time and encases the heart and may get calcified. This rigid thickened pericardium limits the ventricular filling as the elastic limit of the diseased pericardium is much lesser than that of a normal pericardium. Ventricular filling in early diastole is not affected and is only impeded when the elastic limit of the pericardium is reached in contrast to cardiac tamponade where the ventricular filling is impeded throughout the diastole. This results in decreased end diastolic volume and decreased stroke volume and cardiac output. The thickened and scarred pericardium prevents the normal inspiratory decrease in intrathoracic pressure from being transferred to the heart chambers 2. Venous return to the heart becomes limited, and ventricular filling is reduced, with associated inability to maintain adequate preload. Filling pressures of the heart tend to become equal in both the ventricles and the atria.
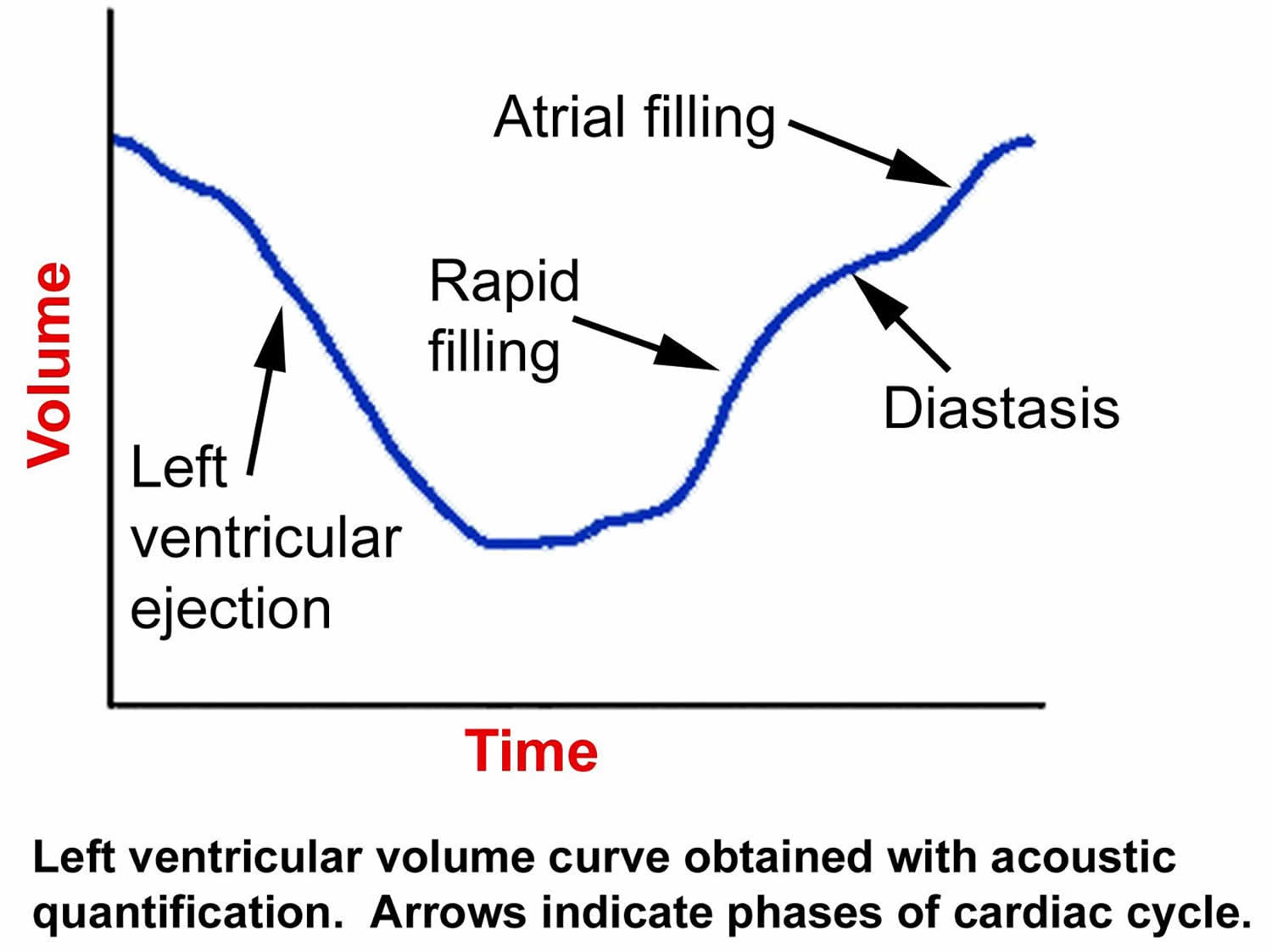
Since the myocardium is unaffected, early ventricular filling during the first third of diastole is unimpeded. After early diastole, the stiff pericardium affects flow and hemodynamics. Accordingly, the ventricular pressure initially decreases rapidly (producing a steep Y descent on right atrial pressure waveform tracings) and then increases abruptly to a level that is sustained until systole (the “dip-and-plateau waveform” or “square root sign” seen on right or left ventricular pressure waveform tracings) 26.
The preservation of myocardial function in early diastole aids in distinguishing constrictive pericarditis from restrictive cardiomyopathy 27. Systolic function is rarely affected until late in the course of the disease, presumably secondary to infiltrative processes that affect the myocardium, atrophy, or scarring or fibrosis of the myocardium from the overlying adjacent pericardial disease 27.
Experimental models indicated that a change in volume-elasticity curves (see Figure 9 below) was the fundamental pathophysiologic change associated with constrictive pericarditis. During development of the constriction, right and left ventricular diastolic pressure increased, and stroke volume decreased. A small increase in volume resulted in a considerable increase in end-diastolic pressure.
Symptoms consistent with congestive heart failure (CHF), especially right-sided heart failure, develop as a result of the inability of the heart to increase stroke volume 28. Over time, cardiac output gradually becomes inadequate, at first with exercise and then at rest.
The clinical symptoms and classic hemodynamic findings of constrictive pericarditis can be explained by the early rapid diastolic filling and elevation, with eventual equalization of the diastolic pressures in all of the cardiac chambers. This restricts late diastolic filling, leading to venous engorgement and decreased cardiac output, all secondary to a confining pericardium.
Figure 9. Constrictive pericarditis left ventricular volume curve
Constrictive pericarditis signs and symptoms
Constrictive pericarditis signs and symptoms include:
- Shortness of breath (dyspnea).
- Chest pain.
- Fatigue.
- Dizziness.
- Swelling especially in the abdomen and lower legs from fluid buildup.
- Loss of muscle mass.
- Loss of appetite and feeling full even when eating very little.
Early on in the course of constrictive pericarditis, patients may present with symptoms secondary to a reduction in cardiac output rather than those due to elevated filling pressures. These early symptoms include fatigue and shortness of breath on exertion (exertional dyspnea), commonly referred to as “out of puff” on mild exercise.
Once the filling pressures become significantly elevated, and systemic venous pressure rises, signs of overt right heart failure develop. Abdominal complaints are secondary to either ascites (accumulation of fluid in the peritoneal cavity, causing abdominal swelling) or congestive hepatomegaly (enlarged liver).
Constrictive pericarditis diagnosis
Constrictive pericarditis is very hard to diagnose as there is no single diagnostic test that can provide a definitive diagnosis or evidence of constrictive pericarditis. To diagnose constrictive pericarditis, your heart doctor will examine you and asks questions about your symptoms and medical history. Your doctor will also listen to your heart using a device called a stethoscope.
Direct questioning, particularly for a prior history of pericarditis, is relevant in any patient presenting with constrictive pericarditis.
On physical examination, the jugular venous pressure (JVP) is usually elevated, however, may be normal in early constrictive pericarditis. The level of the jugular venous pressure (JVP) may only become visible with the patient in an upright position, and it is therefore imperative to evaluate it with the patient standing when the diagnosis is suspected. Avoid examining the patient only in the supine position, because jugular venous pressure (JVP) may be above the angle of the jaw and inadvertently mistaken for normal.
Kussmaul’s sign: Kussmaul’s sign is a condition where the jugular venous pressure (JVP) increases during inhalation, instead of decreasing as normal. It’s a sign of right heart dysfunction and can be seen in some heart diseases. Kussmaul’s sign is observed in only 21% of constrictive pericarditis cases and is therefore not a sensitive sign, because this sign is also observed in patients with right ventricular failure, restrictive cardiomyopathy, right ventricular infarction, and tricuspid stenosis—although, notably, not in patients with cardiac tamponade.
Sinus tachycardia is common while the blood pressure (BP) is normal or low, depending on the stage of the disease process.
The apical impulse is often impalpable, and the patient may have distant or muffled heart sounds. A friction rub is usually not found.
A pericardial knock, which corresponds with the sudden cessation of ventricular filling early in diastole, occurs in approximately half the cases. It is usually heard along the left sternal border and may be mistaken for an S3 gallop. However, a knock is of higher frequency than an S3 gallop and occurs slightly earlier in diastole.
A cardiac murmur is typically not present unless concomitant valvular heart disease or a fibrous band that constricts the right ventricular outflow tract is present.
Pulsus paradoxus: Pulsus paradoxus also known as a paradoxical pulse is a condition where your blood pressure (BP) drops abnormally when you inhale. Pulsus paradoxus may be seen in approximately 20% of constrictive pericarditis patients. If present, it rarely exceeds 10 mm Hg unless a concomitant pericardial effusion with an abnormally elevated pressure exists.
Hepatomegaly with prominent hepatic pulsations can be detected in as many as 70% of patients. Other signs that result from chronic hepatic congestion include ascites, spider angiomata, and palmar erythema, which can contribute to the common but erroneous diagnosis of primary liver disease.
Tests to diagnose pericarditis or rule out conditions that may cause similar symptoms may include:
- Testing for tuberculosis (TB).
- Blood tests. Blood tests usually are done to check for signs of a heart attack, inflammation, infection or to confirm or rule out immune system conditions.
- Electrocardiogram (ECG or EKG). An electrocardiogram is a quick and painless test that records the electrical signals in the heart. It can show how the heart is beating. Sticky patches called electrodes with wires attach to the chest and sometimes the arms or legs. The wires connect to a monitor, which prints or displays results. There are no specific signs of constrictive pericarditis on ECG which may reveal nonspecific ST changes and low voltage. Advanced and long-standing cases may show atrial fibrillation (AF) secondary to elevated atrial pressures.
- Chest X-ray. A chest X-ray can show changes in the size and shape of the heart. It can tell if the heart is enlarged.
- Echocardiogram. Sound waves create images of the moving heart. An echocardiogram shows how well the heart is pumping blood. It also can see any fluid buildup in the tissue surrounding the heart. The test can tell if the sac surrounding the heart affects the way the heart fills with blood or pumps blood.
- Heart computerized tomography (CT) scan. Cardiac CT scans use X-rays to create images of the heart and chest. The test can be used to look for heart thickening that may be a sign of constrictive pericarditis.
- Heart magnetic resonance imaging (MRI). This test uses magnetic fields and radio waves to create detailed images of the heart. A cardiac MRI scan can show thickening, inflammation or other changes in the thin tissue surrounding the heart.
- Left and right heart catheterization. Cardiac catheterization can be used to measure how much blood your heart pumps out per minute (cardiac output). Cardiac catheterization is the only way to measure directly the pressure of blood in each chamber of your heart and in the major blood vessels going from your heart to your lungs. In cardiac catheterization, a thin catheter (a small, flexible, hollow plastic tube) is inserted into an artery or vein in your neck, arm, or groin/upper thigh through a puncture made with a needle. A local anesthetic is given to numb the insertion site. The catheter is then threaded through the major blood vessels and into the chambers of your heart and/or into the coronary arteries. The procedure is done in the hospital and takes 40 to 60 minutes. Various small instruments can be advanced through the tube to the tip of the catheter. They include instruments to measure the pressure of blood in each heart chamber and in blood vessels connected to the heart, to view or take ultrasound images of the interior of blood vessels, to take blood samples from different parts of the heart, or to remove a tissue sample from inside the heart for examination under a microscope (biopsy).
Transthoracic echocardiography as well as frontal and lateral chest radiography with adequate technical characteristics are recommended in all patients with suspected constrictive pericarditis.
Computed tomography (CT) scanning and/or cardiac magnetic resonance imaging (CMRI) are indicated as second-level imaging techniques to assess calcifications (CT scanning), pericardial thickness, and degree and extension of pericardial involvement. Myocardial fibrosis or atrophy seen on CT or MRI is associated with a poor surgical outcome.
Right-sided heart cardiac catheterization provides direct assessment of cardiac filling pressures and can be invaluable in diagnosing constriction, helping to correlate physical examination findings with quantitative data. Ventricular pressure waveform typically demonstrates a steep Y descent after systole, followed by rapid diastolic filling (during early diastole) until a plateau is reached. There is little additional filling of the ventricle despite atrial contraction. This corresponds to a normally compliant ventricle opening and rapid filling initially until the stiff pericardium impedes late diastolic filling (forming the so-called “dip-and-plateau” sign).
Echocardiography
The American College of Cardiology and the European Society of Cardiology guidelines recommend the use of echocardiography (transthoracic echocardiography) for diagnosis of constrictive pericarditis and any other pericardial disease 29. Two-dimensional echocardiography may show increased pericardial thickness without or without calcification. Two-dimensional echocardiography may also reveal dilatation of the inferior vena cava with the absence of inspiratory collapse. A sharp halt in diastolic filling may be seen along with the abrupt transient movement of intraventricular septum towards the right side which is also known as septal bounce 30, 31, 32.
The M mode is very important to rule out constrictive pericarditis. The following features are frequently seen in constrictive pericarditis and An absence these features on M mode makes the diagnosis of constrictive pericarditis very unlikely.
- Posterior motion of ventricular septum on early diastole in inspiration
- Absence of increase in systemic venous return with inspiration
- Premature opening of the pulmonic valve due to higher right ventricular diastolic pressure compared to pulmonary arterial pressure
Doppler ECHO is used to evaluate hemodynamics of the disease and may reveal the following:
- Abnormal passive filling of the ventricles in early diastole
- Increase in diastolic flow velocity across the tricuspid valve during inspiration and decrease during expiration
- Exaggerated reduction in flow velocity in the pulmonary veins and across the mitral valve in inspiration and a leftward shift of ventricular septum
Constrictive pericarditis differential diagnosis
Constrictive pericarditis has similar signs and symptoms to other conditions such as restrictive cardiomyopathy and cardiac tamponade. Your cardiologist will need to rule out these conditions when making a diagnosis.
- Restrictive cardiomyopathy also called idiopathic restrictive cardiomyopathy or infiltrative cardiomyopathy is a rare heart disease that causes the heart muscle to become stiff and unable to relax. This makes it difficult for the heart to fill with blood, which can lead to heart failure
- Cardiac tamponade: Cardiac tamponade is a life-threatening condition that occurs when fluid builds up around the heart, preventing it from pumping properly. This is a medical emergency that requires immediate treatment.
- Congestive heart failure from a number of causes, including pressure-overload and myocardial, valvular, or atherosclerotic disease, must be excluded.
- Right-sided valvular abnormalities such as tricuspid stenosis or tricuspid regurgitation that increase venous pressure, often have similar findings to constriction on physical examination. Echocardiography should readily identify these conditions.
- Right-sided atrial tumors, such as myxomas, can mimic constriction by compressing the tricuspid valve. These are very rare and can be distinguished with echocardiography.
- Superior vena cava syndrome and nephrotic syndrome can produce gross edema and ascites. Laboratory and imaging data should differentiate these from constriction.
- Sarcoidosis, amyloidosis, and hemochromatosis are the most commonly encountered infiltrative processes that lead to restrictive physiology.
- Cardiac fibrosis is another cause of restrictive cardiomyopathy that is becoming more frequent as cardiac patients with more common disorders live longer.
- HIV infections and AIDS.
Constrictive pericarditis management
Constrictive pericarditis is usually treatable. In most cases, curing constrictive pericarditis involves two main principles:
- Relieving pressure on your heart happens because the pericardium can’t stretch.
- Treating underlying causes or related symptoms.
Most of the time, constrictive pericarditis treatment involves the following:
- Surgery. Pericardiectomy, which removes all of the pericardium, usually offers the best chance to treat constrictive pericarditis successfully. You don’t need your pericardium to survive, and many people return to their normal lives without any difficulty or long-term effects.
- Potential complications from surgery include:
- Heart failure.
- Irregular heart rhythms (arrhythmias).
- Infections and sepsis.
- Death.
- Potential complications from surgery include:
- Medication. Depending on the underlying cause and symptoms, different medications can help treat constrictive pericarditis symptoms directly or try to cure it by stopping whatever is causing it to happen. In some cases, medications are enough to treat constrictive pericarditis, avoiding the need for surgery, or they can help manage symptoms for people who can’t have surgery.
The most common medications for the treatment of constrictive pericarditis include:
- Diuretics (water pills). There are several categories of diuretics. All diuretics help your kidneys remove extra fluid from your body.
- Non-steroidal anti-inflammatory drugs (NSAIDs). Non-steroidal anti-inflammatory drugs (NSAIDs) help reduce inflammation and relieve pain. Examples of these include ibuprofen or naproxen.
- Steroids also called corticosteroids. Steroids are a man-made version of hormones normally produced by your adrenal glands which are 2 small glands found above the kidneys. Steroids are anti-inflammatory medicines that reduce redness and swelling (inflammation). This can help with inflammatory conditions.
- Cause-specific medications. Examples of these include antibiotics for bacterial infections like tuberculosis.
The general management of constrictive pericarditis is shown in Figure 10 below 33, 34, 29, 23, 35. The primary goal in constrictive pericarditis is to improve heart function and it is crucial that the primary cause be identified and managed accordingly. The definitive cure for constrictive pericarditis is primarily surgical in the form of complete pericardiectomy, where feasible 36, 37, 38, 39. Pericardiectomy typically leads to rapid hemodynamic and symptomatic improvements in most patients; however, in a subset of patients, particularly those with left ventricular systolic dysfunction, advanced New York Heart Association (NYHA) functional class, concomitant myocardial disease and also comorbidities, symptoms may persist after surgery. Medical management, such as careful observation or symptomatic treatment, has been suggested in less severe cases; however, this option remains controversial.
Diuretics have been used in the early stages of the disease to improve pulmonary and systemic congestion. However, diuretics should be used cautiously as any drop in intravascular volume may lead to a significant drop in cardiac output. A strict fluid restriction and low sodium diet may be recommended in some patients. It is important to anticipate complications which may arise due to failure for early diagnose of constrictive pericarditis or improper management of constriction, as well as complications related to the primary etiology of constriction or related to any existing pathology.
Figure 10. Constrictive pericarditis treatment algorithm
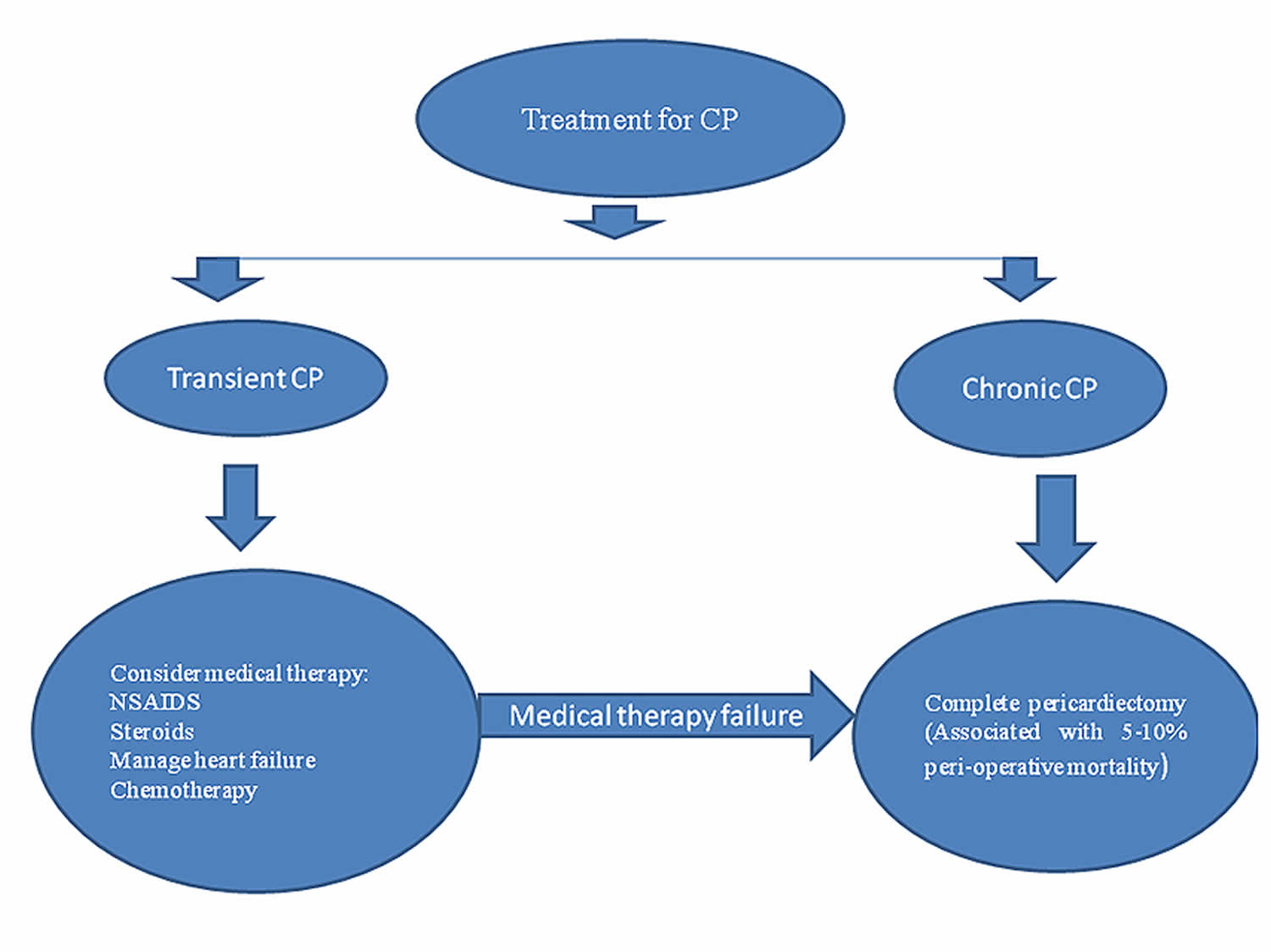
Abbreviations: ASA = aspirin; CP = constrictive pericarditis; CRP = C-reactive protein; CT = computed tomography; ESR = erythrocyte sedimentation rate; MRI = magnetic resonance imaging; NSAIDS = non-steroidal anti-inflammatory drugs; WCC = white cell count
[Source 40 ]Medical therapy
In the majority of cases, medical therapy is deemed ineffective unless there is prominent evidence suggestive of an inflammatory component which makes cardiac magnetic resonance imaging very important in the detection of pericardial enhancement as part of the initial diagnostic modalities in patients suspected of pericardial disease, in particular constrictive pericarditis 40. The management of constrictive pericarditis differs from that of acute pericarditis, where the use of non-steroidal anti-inflammatory agents (NSAIDs), cyclooxygenase (COX)-2 inhibitors, colchicine, corticosteroids, or a combined therapy may be beneficial 33, 34, 29, 23, 35. Although reports have documented the benefit of optimal medical therapy for acute pericarditis, constriction may still develop over time after the initial insult. As a result, these patients need a close and regular follow-up, where echocardiography will be one non-invasive imaging modality to evaluate the patient, in addition to other modalities. Transient constrictive pericarditis has been described, so those individuals with the diagnosis of constriction who are medically stable may be given a trial of conservative treatment for a period of two to three months (using NSAIDs and/or steroids) 33, 34, 29, 23, 35. This should only be considered in individuals with optimized volume status and controlled symptoms.
The following specific treatment modalities should be considered for each of the special situations highlighted.
- Subacute constrictive pericarditis may respond to steroids if treated before pericardial fibrosis develops.
- Diuretics, particularly loop diuretics, are the mainstay to relieve congestion and to optimise clinical volume status; however, they may decrease preload to the point of reducing cardiac output and thus require closer monitoring.
- Any other medications used to treat patients with constrictive pericarditis should be specifically directed to the underlying etiology of the pericardial disease.
- Any therapy directed towards the causative disease, e.g., antituberculosis therapy, is appropriate.
- Constrictive pericarditis-related complications require their own specific therapy as appropriate, e.g., atrial arrhythmias.
- In general, beta-blockers and calcium channel blockers should be avoided, because the sinus tachycardia that commonly occurs in constriction has a compensatory function, maintaining cardiac output in the setting of fixed stroke volume (secondary to fixed diastolic filling).
- Patients with advanced cardiac symptoms related to constriction may derive little benefit from surgery, as these are often the high surgical risk group.
Pericardiectomy
A pericardiectomy is a surgical procedure that removes part or all of the pericardium. Pericardiectomy is usually done to treat constrictive pericarditis, a condition where the pericardium becomes inflamed and stiff. Pericardiectomy was first performed and reported in 1913, and is regarded as a curative measure for constrictive pericarditis 37, 39. Although partial pericardiectomy has been recommended in some patients, complete pericardiectomy remains the definitive therapy and a potential cure in most constrictive pericarditis patients 35, 36. If pericardiectomy is performed earlier in the course of constrictive pericarditis, when the pericardium is less calcified and no element of myocardium fibrosis/dysfunction or advanced heart failure is evidenced, the outcomes are generally acceptably good. However, some judgement must be exercised because patients who are in NYHA Class I or early NYHA Class II may be clinically stable for many years. Pericardiectomy may not be recommended very early on during the course of the disease or in patients with advanced disease (Class IV symptoms), when the surgical risk is high. The surgical risk in patients with advanced diseases or those with LV systolic dysfunction is very high, with an estimated 40% to 60% perioperative mortality rate 41.
Partial pericardiectomy or less invasive options (i.e., pericardial window) should be considered whenever fluid reaccumulates, becomes loculated or biopsy material is required in the setting of a large or recurrent pericardial effusion, particularly in effusive constriction. This approach should also be considered in patients with advanced disease, myocardial dysfunction or anticipated heart failure, particularly in those at high risk of acute ventricular dilatation after surgery, with subsequent acute heart failure (right ventricular failure [RVF]).
Pericardiectomy can be a long, horrendous and often technically complex procedure, requiring extensive surgical experience. The two recommended standard approaches are via an anterolateral thoracotomy and median sternotomy 41, 36, 37. Pericardial decortication should be as extensive as possible, especially at the diaphragmatic-ventricular contact regions. An excimer laser is recommended and should be considered, particularly when severe adhesions occur between the pericardium and epicardium to prevent perioperative mediastinal bleeding and maintain haemodynamic stability throughout the surgical procedure. Complications related to pericardiectomy may include excessive bleeding, atrial and ventricular arrhythmias, ventricular wall ruptures, phrenic nerve injury and even constrictive pericarditis recurrence.
In the recent past, published reports have indicated that the surgical mortality is estimated to range between 5 and 15%, with one of the reports indicating a 30-day perioperative mortality of 6.1% 41, 33, 23. Furthermore, other studies have demonstrated a perioperative mortality of between 5% and 10%, and a further increased later mortality rate of up to 70% in the same study population; however, these poorer outcomes were also exacerbated by other comorbidity factors 41, 23. Generally, poor prognostic markers associated with these detrimental outcomes include progressive heart failure or advanced heart failure symptoms (NYHA III-IV), sepsis, renal failure, respiratory failure, arrhythmia, prior mediastinal radiotherapy as the primary cause of constriction, and other concomitant severe comorbidities 33. Reports have indicated that an estimated 80% to 90% of constrictive pericarditis patients who undergo a successful pericardiectomy, particularly in the hands of extensive expertise, achieve significant symptomatic improvement to NYHA Class I or II postoperatively and live potentially normal or near normal lives afterwards 42.
Although symptomatic improvement is evident after pericardiectomy, evidence of abnormal diastolic filling patterns often persist for months. These can be correlated with symptoms or clinical status 43. Furthermore, reports have indicated that a significant number of patients, in excess of 60% of constrictive pericarditis patients, demonstrate complete normalisation or resolution of cardiac haemodynamics after pericardiectomy 41, 33, 23. Although some patients improve with time, persistent diastolic filling abnormalities tended to occur in those who had a longer history of preoperative symptoms, supporting the view that early operation is advisable in symptomatic patients 43. Those patients who have symptoms that persist even after successful pericardiectomy may have a mixed constrictive-restrictive picture or so-called constrictive cardiomyopathy, which warrants thorough clinical and imaging modalities including advanced echocardiographic parameters, cardiac computed tomography scan or even cardiac magnetic resonance 33, 23.
One study reported 58 constrictive pericarditis patients who underwent total pericardiectomy and were then followed up for a total of four to five years after surgery 44. About 30% of these patients had persistently severe heart failure symptoms during the follow-up period after pericardiectomy; some had persistent evidence of a restrictive or constrictive pattern 41, 33, 23, 34. The overall assumption was that the persistent symptoms could be related to the restrictive or constrictive changes demonstrated in most of their Doppler signals 41, 33, 23, 34.
Constrictive pericarditis prognosis
The prognosis (outlook) for constrictive pericarditis depends on the cause, the severity of your condition, the treatments involved and any other health conditions you might have 45. Your cardiologist is the best person to tell you what to expect from constrictive pericarditis and your likely outlook (prognosis). Life expectancy is reduced in untreated children and in patients with relatively acute onset of symptoms.
Because constrictive pericarditis often happens alongside severe or deadly conditions, the outlook is often negative. This is especially true when it happens because of radiation therapy or when you also have:
- Advanced kidney disease or kidney failure.
- Heart failure.
- Liver disease.
- Pulmonary hypertension.
Because of the risks, the best outcomes usually happen with early diagnosis and treatment, but it is potentially fatal if left untreated. Undiagnosed patients with constrictive pericarditis can have a 90% mortality 45. Good outcomes are also more likely with the transient type of constrictive pericarditis. One study showed postpericardiectomy survival rates of 71% and 52% at 5 and 10 years, respectively. Even so, about 5% to 10% of those who undergo surgery don’t survive (hospitals that specialize in heart care tend to have better outcomes). However, constrictive pericarditis is potentially curable if diagnosed early and most people recover and do well. Between 2005 and 2014, in-hospital mortality for patients with constrictive pericarditis was 7.3% for those who underwent pericardiectomy and 6.8% for those who received medical management 12.
Nearly 80% of the people who have surgery for constrictive pericarditis live at least five years, and nearly 60% live at least 10 years. Long-term survival after pericardiectomy depends on the underlying cause 45. Of common causes, idiopathic constrictive pericarditis has the best prognosis (88% survival at 7 years), followed by constriction due to cardiac surgery (66% at 7 years). The worst postpericardiectomy prognosis occurs in postradiation constrictive pericarditis (27% survival at 7 years), probably as a reflection of confounding comorbidities. Occasionally, the cause of the constriction may cause coincident myocardial dysfunction.
With surgical treatment, the long-term outcomes of patients with constrictive pericarditis have been shown to be independently less favorable with advanced age, poor renal function, abnormal left ventricular systolic function, high pulmonary artery systolic pressure, lower serum sodium level, worsening NYHA classification, and, as noted above, radiation therapy as the cause of the constrictive pericarditis 23, 46 The degree of pericardial calcification has shown no effect on survival.
- Syed, F., Schaff, H. & Oh, J. Constrictive pericarditis—a curable diastolic heart failure. Nat Rev Cardiol 11, 530–544 (2014). https://doi.org/10.1038/nrcardio.2014.100[↩]
- Yadav NK, Siddique MS. Constrictive Pericarditis. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459314[↩][↩]
- Welch TD. Constrictive pericarditis: diagnosis, management and clinical outcomes. Heart 2018;104:725-731. https://doi.org/10.1136/heartjnl-2017-311683[↩]
- Li J, Li R, Cheng G, et al. A case series of constrictive pericarditis and suggested echocardiographic diagnostic criteria. Journal of International Medical Research. 2022;50(11). doi:10.1177/03000605221134468[↩][↩][↩][↩][↩][↩]
- Birtolo LI, Shahini E. Constrictive Pericarditis and Protein-Losing Enteropathies: Exploring the Heart-Gut Axis. J Clin Med. 2024 Aug 30;13(17):5150. doi: 10.3390/jcm13175150[↩]
- Chang SA, Oh JK. Constrictive Pericarditis: A Medical or Surgical Disease? J Cardiovasc Imaging. 2019 Jul;27(3):178-186. doi: 10.4250/jcvi.2019.27.e28[↩]
- Restelli D, Carerj ML, Bella GD, Zito C, Poleggi C, D’Angelo T, Donato R, Ascenti G, Blandino A, Micari A, Mazziotti S, Minutoli F, Baldari S, Carerj S. Constrictive Pericarditis: An Update on Noninvasive Multimodal Diagnosis. J Cardiovasc Echogr. 2023 Oct-Dec;33(4):161-170. doi: 10.4103/jcecho.jcecho_61_23[↩]
- Khan I. A Review of the Surgical Treatment for Constrictive Pericarditis. ARYA Atheroscler. 2023 Jul;19(4):57-66. doi: 10.48305/arya.2023.41472.2882[↩]
- Bhattad PB, Jain V. Constrictive Pericarditis: A Commonly Missed Cause of Treatable Diastolic Heart Failure. Cureus. 2020 May 8;12(5):e8024. doi: 10.7759/cureus.8024[↩]
- Okyere I, Okyere P, Ameyaw E, Brenu SG, Tamatey M, Agyemang Yeboah F. Pericardiectomy for constrictive pericarditis in a resource constraint setting. Kardiochir Torakochirurgia Pol. 2021 Sep;18(3):165-172. doi: 10.5114/kitp.2021.109390[↩]
- Ren Y. The clinical value of P-wave terminal force in lead V1 in evaluating pericardial thickness in tuberculous constrictive pericarditis. J Cardiothorac Surg. 2024 Feb 12;19(1):89. doi: 10.1186/s13019-024-02526-z[↩]
- Mori M, Mullan CW, Bin Mahmood SU, Yousef S, Pelletier KJ, Mangi AA, Geirsson A. US National Trends in the Management and Outcomes of Constrictive Pericarditis: 2005-2014. Can J Cardiol. 2019 Oct;35(10):1394-1399. doi: 10.1016/j.cjca.2019.05.015[↩][↩][↩][↩]
- Zhu P, Mai M, Wu R, et al. Pericardiectomy for constrictive pericarditis: single-center experience in China. J Cardiothorac Surg. 2015;10:34. doi: 10.1186/s13019-015-0237-6[↩]
- Constrictive Pericarditis: A Spectrum of Disease Manifestations and Management. https://www.acc.org/Education-and-Meetings/Patient-Case-Quizzes/2021/09/27/12/02/Constrictive-Pericarditis[↩]
- Griffin BP, Topol EJ. Pericardial Disease. Manual of Cardiovascular Medicine. 2nd ed. Philadelphia, Pennsylvania: Lippincott Williams and Wilkins; 2004. 372-396.[↩][↩]
- Shabetai R. Constrictive pericarditis. Shabetai R, ed. The Pericardium. New York, NY: Grune & Stratton; 1981.[↩]
- Rajesh G, Raju D, Krishnan MN. Shelled heart: tuberculous constrictive pericarditis. Heart Asia. 2013 doi: 10.1136/heartasia-2013-010363[↩]
- Meybeck A, Pasquet A, Senneville E. Immunotherapy for tuberculous pericarditis. N Engl J Med. 2014;371:2532. doi: 10.1056/NEJMc1413185[↩]
- Gary T, Aamir A, Francisco A, Sanjay P, Raphael CE, Vassilis V. Tuberculous constrictive pericarditis. Res Cardiovasc Med. 2015;4:290–292. doi: 10.5812/cardiovascmed.29614[↩]
- Syed FF, Mayosi BM. A modern approach to tuberculous pericarditis. Prog Cardiovasc Dis. 2007;50(3):218–236. doi: 10.1016/j.pcad.2007.03.002[↩]
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. 2004;25(7):587–610. doi: 10.1016/j.ehj.2004.02.002[↩]
- Imazio M, Brucato A, Maestroni S, Cumetti D, Belli R, Trinchero R, Adler Y. Risk of constrictive pericarditis after acute pericarditis. Circulation. 2011 Sep 13;124(11):1270-5. doi: 10.1161/CIRCULATIONAHA.111.018580[↩]
- Bertog SC, Thambidorai SK, Parakh K, Schoenhagen P, Ozduran V, Houghtaling PL, Lytle BW, Blackstone EH, Lauer MS, Klein AL. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004 Apr 21;43(8):1445-52. doi: 10.1016/j.jacc.2003.11.048[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Mulibrey Nanism. https://rarediseases.org/rare-diseases/mulibrey-nanism/[↩]
- Constrictive Pericarditis Etiology. https://emedicine.medscape.com/article/157096-overview#a5[↩]
- Shabetai R. Pericardial Disease: etiology, pathophysiology, clinical recognition, and treatment. New York NY: Churchill Livingstone; 1995. 1024-35.[↩]
- Constrictive Pericarditis Pathophysiology. https://emedicine.medscape.com/article/157096-overview#a4[↩][↩][↩]
- Higano ST, Azrak E, Tahirkheli NK, Kern MJ. Hemodynamic rounds series II: hemodynamics of constrictive physiology: influence of respiratory dynamics on ventricular pressures. Catheter Cardiovasc Interv. 1999 Apr;46(4):473-86. doi: 10.1002/(SICI)1522-726X(199904)46:4<473::AID-CCD21>3.0.CO;2-W[↩]
- Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, Maisch B, Mayosi B, Pavie A, Ristic AD, Sabaté Tenas M, Seferovic P, Swedberg K, Tomkowski W; ESC Scientific Document Group. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015 Nov 7;36(42):2921-2964. doi: 10.1093/eurheartj/ehv318[↩][↩][↩][↩]
- Pessinaba S, Sonhaye L, Agbétiafa M, Wossinu Quacoe M, Aloumon M, Yayehd K, Amadou L, d’Alméida R, Damorou F. La péricardite chronique constrictive, une véritable gangue calcifiée réalisant un goulot d’étranglement médio-ventriculaire : à propos d’un cas [The chronic constrictive pericarditis, a real calcified gangue realizing a mid-ventricular bottleneck: A case report]. Ann Cardiol Angeiol (Paris). 2019 Apr;68(2):125-128. French. doi: 10.1016/j.ancard.2018.07.001[↩]
- Imazio M. Dieci quesiti in tema di pericardite costrittiva [Ten questions about constrictive pericarditis]. G Ital Cardiol (Rome). 2018 Jul-Aug;19(7):412-419. Italian. doi: 10.1714/2938.29537[↩]
- Mukai-Yatagai N, Haruki N, Kinugasa Y, Ohta Y, Ishibashi-Ueda H, Akasaka T, Kato M, Ogawa T, Yamamoto K. Assessment of myocardial fibrosis using T1-mapping and extracellular volume measurement on cardiac magnetic resonance imaging for the diagnosis of radiation-induced cardiomyopathy. J Cardiol Cases. 2018 Jun 30;18(4):132-135. doi: 10.1016/j.jccase.2018.06.001[↩]
- Ling LH, Oh JK, Schaff HV, Danielson GK, Mahoney DW, Seward JB, Tajik AJ. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation. 1999 Sep 28;100(13):1380-6. doi: 10.1161/01.cir.100.13.1380[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Cho YH, Schaff HV. Surgery for pericardial disease. Heart Fail Rev. 2013 May;18(3):375-87. doi: 10.1007/s10741-012-9338-7[↩][↩][↩][↩][↩]
- Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010 Jun;85(6):572-93. doi: 10.4065/mcp.2010.0046[↩][↩][↩][↩]
- Tiruvoipati R, Naik RD, Loubani M, Billa GN. Surgical approach for pericardiectomy: a comparative study between median sternotomy and left anterolateral thoracotomy. Interact Cardiovasc Thorac Surg. 2003 Sep;2(3):322-6. doi: 10.1016/S1569-9293(03)00074-4[↩][↩][↩]
- GLENN F, DIETHELM AG. Surgical treatment of constrictive pericarditis. Ann Surg. 1962 Jun;155(6):883-93. doi: 10.1097/00000658-196206000-00008[↩][↩][↩]
- Srivastava AK, Ganjoo AK, Misra B, Chaterjee T, Kapoor A, Pandey CM. Subtotal Pericardiectomy via Sternotomy for Constrictive Pericarditis. Asian Cardiovascular and Thoracic Annals. 2000;8(2):134-136. doi:10.1177/021849230000800210[↩]
- Bassem R, Hèla BJ, Bassem J, Nada T, Taieb C, Ahmed E, Iheb S, Samir K, Sayda M, Imed F. Unusual Presentation of a Primary Pericardial Malignant Mesothelioma: Constrictive Pericarditis A Case Report and Review of the Literature. J Tumor Diag Rep. 2015;1:104. https://www.longdom.org/open-access/unusual-presentation-of-a-primary-pericardial-malignant-mesotheliomaconstrictive-pericarditis-a-case-report-and-review-of-the-lite-jtdr-1000004.pdf[↩][↩]
- Constrictive pericarditis: prevention and treatment. https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-15/Constrictive-pericarditis-prevention-and-treatment [↩][↩]
- Depboylu BC, Mootoosamy P, Vistarini N, Testuz A, El-Hamamsy I, Cikirikcioglu M. Surgical Treatment of Constrictive Pericarditis. Tex Heart Inst J. 2017 Apr 1;44(2):101-106. doi: 10.14503/THIJ-16-5772[↩][↩][↩][↩][↩][↩][↩]
- Biçer M, Özdemir B, Kan İ, Yüksel A, Tok M, Şenkaya I. Long-term outcomes of pericardiectomy for constrictive pericarditis. J Cardiothorac Surg. 2015 Nov 27;10:177. doi: 10.1186/s13019-015-0385-8[↩]
- Syed FF, Schaff HV, Oh JK. Constrictive pericarditis–a curable diastolic heart failure. Nat Rev Cardiol. 2014 Sep;11(9):530-44. doi: 10.1038/nrcardio.2014.100. Epub 2014 Jul 29. Erratum in: Nat Rev Cardiol. 2015 Dec;12(12):682. doi: 10.1038/nrcardio.2015.162[↩][↩]
- Shabetai R. The pericardium. Norwell (MA): Kluwer Academic Publishers; 2003. p.1-50.[↩]
- Liu VC, Fritz AV, Burtoft MA, Martin AK, Greason KL, Ramakrishna H. Pericardiectomy for Constrictive Pericarditis: Analysis of Outcomes. J Cardiothorac Vasc Anesth. 2021 Dec;35(12):3797-3805. doi: 10.1053/j.jvca.2021.02.020[↩][↩][↩]
- Kleynberg RL, Kleynberg VM, Kleynberg LM, Farahmandian D. Chronic constrictive pericarditis in association with end-stage renal disease. Int J Nephrol. 2011;2011:469602. doi: 10.4061/2011/469602[↩]





{kind=link}