Contents
Chronic abdominal pain
Chronic abdominal pain is defined as abdominal pain that is present for more than 3 months either continuously or intermittently 1, 2. Chronic abdominal pain may be present all the time or it may come and go referred to as “recurrent abdominal pain” or “intermittent abdominal pain”. Chronic abdominal pain typically occurs prior to puberty, with two peaks of frequency. The first peak occurs between 5 to 7 years of age, with equal frequency in boys and girls and in 5 to 8% of children. The second peak, occurring in nearly 25%, occurs between 8 and 12 years of age and is far more common in girls. Chronic abdominal pain is one of the most frequent complaints in children and adolescents with prevalence rates ranging from 0.3% to 19% in Western countries 3, 4. The child often has a family history of functional bowel disease such as irritable bowel syndrome (IBS) 5. About 2% of adults, predominantly women, have chronic abdominal pain (a much higher percentage of adults have some type of chronic gastrointestinal symptoms, including non-ulcer dyspepsia and various bowel disturbances) 1.
Chronic abdominal pain is mostly considered functional 6, 7, 8, 9, 10. Functional abdominal pain is defined as continuous abdominal pain with no known underlying biochemical or structural pathology to explain the symptoms 11, 12, 13. Patients with functional abdominal pain may present complaining of indigestion (dyspepsia), non-specific or shifting abdominal pain, nausea or other gastrointestinal signs 14. However, in up to 45% of cases, organic abnormalities are found 15, 16. Lactose and fructose malabsorption are frequently reported in children suffering from chronic abdominal pain 17, 18, 19, 20, 21.
Chronic abdominal pain potential causes include:
- Lactose intolerance
- Bowel obstruction
- Constipation
- Celiac disease
- Cholecystitis (inflammation of the gall bladder)
- Choledocholithiasis (passage of gall stones through the bile duct)
- Colitis (infection or inflammation of the colon)
- Diverticulitis (inflammation of pouches that form in the colon)
- Food allergy
- Food intolerance
- Food sensitivity
- Irritable bowel syndrome (IBS)
- Inflammatory bowel disease (IBD)
- Peptic ulcer disease
- Enteritis (infections of the small bowel, Crohn’s disease)
- Gastritis
- Hiatus hernia with gastroesophageal reflux
- Chronic hepatitis
- Hepatitis B
- Hepatitis C
- Nonalcoholic steatohepatitis (NASH)
- Nonalcoholic Fatty Liver Disease (NAFLD)
- Alcohol-related liver disease
- Cancer
- Colon cancer or colorectal cancer
- Gastric cancer
- Pancreatic cancer
- Ovarian cancer
- Ovarian cyst
- Congenital genitourinary anomalies
- Urinary calculi, urolithiasis or nephrolithiasis
- Endometriosis
- Pelvic Inflammatory Disease (PID)
- Familial Mediterranean Fever (FMF)
- Menopause
- Chronic cholecystitis
- Pancreatitis
- Acute pancreatitis
- Chronic pancreatitis
- Pancreatic pseudocyst
- Parasitic infestation especially giardiasis
- Granulomatous enterocolitis
- Intestinal tuberculosis
- Postoperative adhesive bands
- Acute porphyria
- Cannabis use (cannabis hyperemesis syndrome)
- Chronic abdominal wall pain (anterior cutaneous nerve entrapment syndrome)
- Functional abdominal pain
- Abdominal epilepsy
- Vascular problems:
- Mesenteric ischemia (blocked arteries or veins e.g., mesenteric artery stenosis, mesenteric venous thrombosis)
- Abdominal aortic aneurysm (swelling of the main artery in the belly)
With so many organs and structures in the abdomen, it can be hard for your doctor to be absolutely sure about the cause of your problem. Your doctor will ask you several questions and then examine you carefully. Your doctor will assess whether your abdominal pain requires surgery or admission to hospital. Your doctor may perform further tests and sometimes you may be referred to another doctor to help find the cause of the problem. Most patients with abdominal pain can be diagnosed and treated successfully. See your physician and appropriate specialists if you have persistent or severe abdominal pain.
Nearly all patients with chronic abdominal pain have had a prior medical investigations that did not yield a diagnosis after history, physical, and basic testing. According to the pediatric ROME IV classification, chronic abdominal pain is referred to as functional abdominal pain disorder if it cannot be attributed to another medical condition after appropriate medical evaluation 22, 23. Patients with chronic abdominal pain who do not respond to medical treatment and have no evidence of other organic disease on laboratory, radiologic, and endoscopic examination make gastroenterologists wonder whether the abdominal pain has originated from a functional or an organic cause 8.
Chronic abdominal pain treatment depends on the underlying cause. If a cause is known, treating the underlying cause is the first step. When a cause is not found (idiopathic), treatment focuses on helping people return to normal daily activities and minimizing discomfort. These measures may include:
- Lessening stress and anxiety with medications, relaxation techniques, biofeedback, hypnosis, or other methods
- Relieving pain with medications
- High-fiber diet or fiber supplements
- Reducing muscle spasms in the digestive tract with medications or peppermint oil
Figure 1. Chronic abdominal pain causes
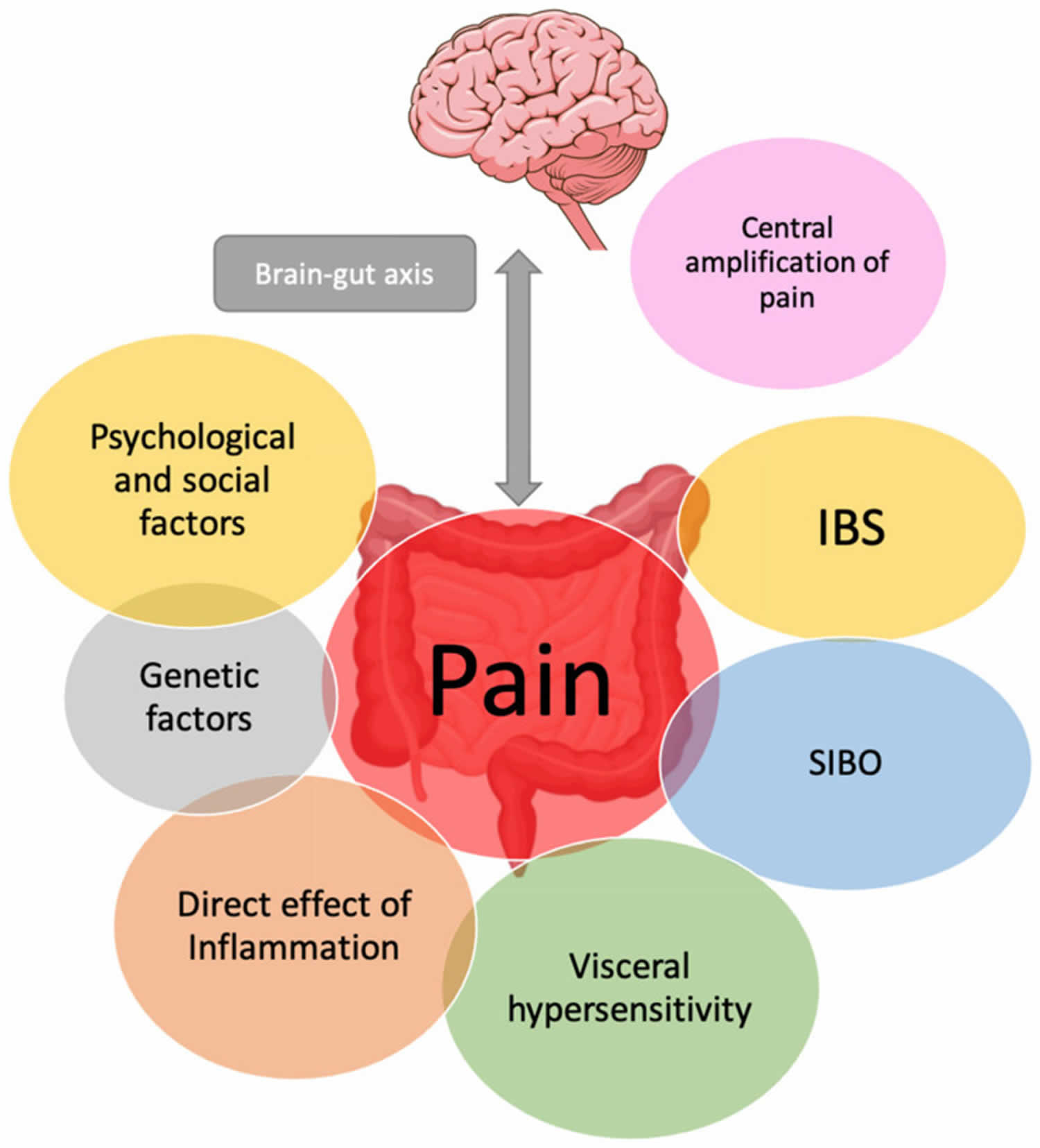
Footnote: Mechanisms of chronic abdominal pain mechanisms and contributing factors implicated in inflammatory bowel disease (IBD).
Abbreviations: IBS = irritable bowel syndrome; SIBO = Small intestinal bacterial overgrowth.
[Source 24 ]Get medical help right away or call your local emergency number if you:
- Have severe pain
- Have pain and vomiting
- Have pain and vomiting blood
- Have pain lasting for several hours
- Are currently being treated for cancer
- Are unable to pass stool, especially if you are also vomiting
- Are vomiting blood or have blood in your stool (especially if bright red, maroon or dark, tarry black)
- Have chest, neck, or shoulder pain
- Have sudden, sharp abdominal pain
- Have pain in, or between, your shoulder blades with nausea
- Have tenderness in your belly, or your belly is rigid and hard to the touch
- Are pregnant or could be pregnant
- Had a recent accident or injury to your abdomen
- Have difficulty breathing
- Burning sensation when you urinate or frequent urination
- Diarrhea for more than 5 days
- Blood in your urine
- Unable to pass urine
- Fever, over 100°F (37.7°C) for adults or 100.4°F (38°C) for children, with pain
- Prolonged poor appetite
- Prolonged vaginal bleeding
- Unexplained weight loss
- Persistent nausea and vomiting
- Pain in your scrotum if you are a male
- Skin that appears discolored
- Severe tenderness when you touch your abdomen
- Swelling of your abdomen
- Become pale and clammy
- Are concerned about your pain
What is functional chronic abdominal pain?
Functional chronic abdominal pain is real pain that exists for more than six months and occurs with no evidence of a specific physical disorder. Functional chronic abdominal pain is also not related to body functions such as menstrual periods, bowel movements, or eating, a drug, or a toxin. Functional abdominal pain can be severe and typically interferes with a person’s life. For example, irritable bowel syndrome (IBS) is a functional bowel disorder that causes chronic abdominal pain and altered bowel habits 25, 26, 27. Another example of functional bowel disorder is centrally mediated abdominal pain syndrome, is a similar but less common disorder that does not cause altered bowel habits.
Exactly what causes functional chronic abdominal pain is unknown. But the nerves of the digestive tract may become oversensitive to sensations.
Chronic abdominal pain causes
The specific cause of chronic abdominal pain is often difficult to determine because there are many reasons why you may have pain in your abdomen. With so many organs and structures in your abdomen, it can be hard for a doctor to be absolutely sure about the cause of your problem. Abdominal pain may not come from the abdomen. Some surprising causes include heart attacks and pneumonia, conditions in the pelvis or groin, some skin rashes like shingles, and problems with stomach muscles like a strain. The pain may occur along with problems in passing urine or with bowel motions, or period problems. Furthermore, in some individuals, chronic abdominal pain has no identifiable cause. Although the exact cause is unknown, nerve signals or chemicals secreted by the gut or brain may cause the gut to be more sensitive to triggers that normally do not cause significant pain (such as stretching, gas bloating or stress). Because of this change in bowel function, this type of abdominal pain is often referred to as “functional abdominal pain.”
Conditions that may cause chronic abdominal pain include:
- Gastrointestinal causes:
- Celiac disease
- Functional dyspepsia
- Chronic pancreatitis
- Gastroesophageal reflux disease (GERD)
- Gallstones
- Gastritis (inflammation of the stomach lining)
- Hiatal hernia
- Inflammatory bowel disease (IBD) such as Crohn’s disease and ulcerative colitis
- Inguinal hernia (a condition in which tissue bulges through a weak spot in the muscles of the abdomen and can descend into the scrotum.)
- Irritable bowel syndrome (IBS)
- Peptic ulcer
- Urogenital causes:
- Neoplasms (abnormal tissue growth), cysts, varicoceles (enlarged veins in the scrotum), prostatitis (a prostate gland disorder), interstitial cystitis (bladder pain syndrome) and chronic pelvic pain. As well as this, chronic abdominal pain can also arise following a vasectomy procedure.
- Gynaecological causes:
- Adhesions (scar-like tissue)
- Endometriosis
- Ovarian cysts
- Mittelschmerz (ovulation pain)
- Pelvic inflammatory disease (PID)
- Pelvic congestion syndrome (enlarged pelvic veins)
- Polycystic ovary syndrome
- In addition, chronic abdominal pain can also develop after hysterectomy, Caesarean and cancer treatment procedures.
- Neurological causes: Chronic abdominal pain can be caused by fibromyalgia, chronic abdominal pain that is felt by the brain’s somatosensory cortex, nerve entrapment within the abdominal cavity (such as, chronic abdominal wall pain or anterior cutaneous nerve entrapment syndrome) and myofascial pain syndromes (such as, amplified musculoskeletal pain syndromes) that affect muscles and soft tissues.
- Metabolic causes: Chronic abdominal pain can occur due to porphyria (disorders that affects the skin and the nerves), diabetic retinopathy and alcohol intake.
- Psychological causes: Chronic abdominal pain has been associated with PTSD, anxiety, depression and personality disorders, due to the impact of psychological distress on gut health.
- Musculoskeletal causes:
- Strained or pulled abdominal muscle
- Sacroiliac joint pain in the lower back, hip pain, symphysis pubic dysfunction (pain in the pelvic joints) and spinal pathologies.
- Hematological causes:
- Sickle cell anemia
- Mast cell activation syndrome
- Hereditary angioedema
- Angioedema
- Acute hepatic porphyria
- Familial Mediterranean fever
- Cardiovascular causes:
- Angina (reduced blood flow to the heart)
- Chronic mesenteric ischemia
- Median arcuate ligament syndrome (MALS)
- Splanchnic artery aneurysm
- Subacute mesenteric venous thrombosis
- Food allergy and food sensitivity
- Functional causes: Chronic abdominal pain can also present without an apparent cause. Diagnostic tests may later reveal the cause to be functional dyspepsia, irritable bowel syndrome or functional abdominal pain syndrome.
Causes of progressive abdominal pain include:
- Cancer
- Crohn’s disease
- Enlarged spleen (splenomegaly)
- Gallbladder cancer
- Hepatitis
- Kidney cancer
- Lead poisoning
- Liver cancer
- Non-Hodgkin’s lymphoma
- Pancreatic cancer
- Stomach cancer
- Tubo-ovarian abscess, which is a pus-filled pocket involving a fallopian tube and an ovary.
- Uremia (buildup of waste products in your blood)
Chronic abdominal pain signs and symptoms
Chronic abdominal pain symptoms vary from patient to patient, and may change with each episode. Chronic abdominal pain is vague pain located around the umbilicus (belly button). However, the pattern or location of abdominal pain is not always predictable with this condition. The pain may occur suddenly, or slowly increase in severity. The pain may be constant or may increase and decrease in severity.
Some children with chronic abdominal pain may experience indigestion (discomfort in your upper abdomen) or upper abdominal pain associated with nausea, vomiting and/or a feeling of fullness after just a few bites. Chronic abdominal pain can also be accompanied by involuntary features such as pallor, nausea, dizziness, headache and fatigue.
The most common chronic abdominal pain symptoms include:
- Sharp or dull pain
- Severe pain that causes you to become sweaty, cry or bend over in pain
- Pain that lasts a few minutes or hours
- Pain in the belly button area or anywhere in the belly
- Pain that may or may not be related to eating
- Pain that occurs any time of the day or night
- Abdominal pain that occurs with vomiting, headaches, or pain in the arms or legs
- Not being hungry like usual or skipping meals, usually without losing weight
Symptoms that require a doctor’s immediate attention include a high fever, loss of appetite or weight, pain that awakens the person, blood in stool or urine, jaundice, severe nausea and vomiting, difficulty swallowing, and swelling of the legs or abdomen.
Chronic abdominal pain diagnosis
The diagnosis of abdominal pain has five components depending on your age. The five components include medical history, a physical examination, laboratory testing, results of imaging studies and response to empiric therapy:
- Medical History. To diagnose abdominal pain, doctors and healthcare professionals are likely to ask you the following questions:
- Location, intensity, character and duration of the pain, time of day or night that pain occurs
- Appetite, diet, satiety, nausea, reflux, vomiting
- Stool pattern, consistency, completeness of evacuation
- Review of systems: weight loss, growth or pubertal delay, fever, rash
- Medications and nutritional interventions
- Family history,
- Travel history,
- Interference with school, work, play, peer relations and family dynamics
- Physical examination
- Weight, height, growth velocity, pubertal stage, blood pressure
- Complete physical examination
- Objective abdominal findings: location, rebound, mass, psoas sign
- Liver, spleen and renal size, ascites, flank pain
- A rectal exam to check for hidden blood or other problems
- A check of the penis and scrotum
- A pelvic exam to check for problems in the womb (uterus), fallopian tubes and ovaries, and a pregnancy test
- Stool testing for occult blood
- Laboratory tests. If tests are needed, these may include:
- Complete blood count with differential, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Urinalysis and urine culture to look for a urine infection or blood (if there is a kidney stone)
- Laboratory tests individualized according to indication
- Stool testing and culture for polymorphonuclear leukocytes, parasites, Giardia antigen
- Serum chemistry profile, serum amylase and serum lipase level
- Pregnancy test, cultures for sexually transmitted diseases
- Breath hydrogen test: lactose, fructose
- Serologic testing for amebae, Helicobacter pylori
- An ECG (an electrical tracing of the heart) to rule out a heart attack
- Imaging studies individualized according to indication
- Abdominal and pelvic sonography
- Upper gastrointestinal contrast study with small bowel testing, abdominal computed tomography
- Upper endoscopy – an examination where a flexible tube with a light and video camera at the tip is used to examine some internal organs without the need for surgery. Different names are used depending on which organ is being looked at for examples, small-bowel capsule endoscopy, video capsule endoscopy, colonoscopy and laparoscopy
- Empiric interventions
- Patient and parent education
- Symptom diary of pain, bowel pattern, diet and associated features, response to intervention
- Constipation investigated as a factor
- Dietary interventions, including adjusted fiber intake, reduced lactose intake, reduced juice intake
- Trial of peptic management
Chronic abdominal pain treatment
The management of chronic abdominal pain depends on the underlying cause. If a cause is known, treating the underlying cause is the first step. When a cause is not found (idiopathic), treatment focuses on helping people return to normal daily activities, resuming a normal diet and minimizing discomfort. These measures may include:
- Lessening stress and anxiety with medications, relaxation techniques, biofeedback, hypnosis, or other methods
- Relieving pain with medications
- High-fiber diet or fiber supplements
- Reducing muscle spasms in the digestive tract with medications or peppermint oil
These additional steps may help prevent some types of abdominal pain:
- Drink plenty of water each day.
- Eat small meals more frequently.
- Exercise regularly.
- Limit foods that produce gas.
- Make sure that your meals are well-balanced and high in fiber. Eat plenty of fruits and vegetables.
The goal of managing chronic abdominal pain is to provide a satisfactory quality of life through education, medical interventions and better coping skills and support. Some individual may benefit from medications, if chronic abdominal pain is significantly limiting the daily routine and quality of life. These medications include anti-spasmodic medicines, muscle relaxants and neuropathic agents. A patient may also benefit from low doses of medicines called tricyclic antidepressants (used at much higher doses to treat depression), which can be excellent pain relievers for some people. DO NOT take any medicine without talking to your healthcare professional.
Some psychological treatments that help people cope with functional abdominal pain and other stressors include behavioral therapy, relaxation exercises and hypnosis.
- Chronic Abdominal Pain and Recurrent Abdominal Pain. https://www.msdmanuals.com/en-au/professional/gastrointestinal-disorders/symptoms-of-gastrointestinal-disorders/chronic-abdominal-pain-and-recurrent-abdominal-pain[↩][↩]
- Apley J. Recurrent abdominal pain. Br J Clin Pract. 1959;13:586–7.[↩]
- Chitkara D.K., Rawat D.J., Talley N.J. The Epidemiology of Childhood Recurrent Abdominal Pain in Western Countries: A Systematic Review. Am. J. Gastroenterol. 2005;100:1868–1875. doi: 10.1111/j.1572-0241.2005.41893.x[↩]
- Ramchandani P.G., Hotopf M., Sandhu B., Stein A., Team A.S. The epidemiology of recurrent abdominal pain from 2 to 6 years of age: Results of a large, population-based study. Pediatrics. 2005;116:46–50. doi: 10.1542/peds.2004-1854[↩]
- Hyams JS, Di Lorenzo C, Saps M, Shulman R, Staiano A, van Tilburg M. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology. 2016;150:1456–1468. e2. doi: 10.1053/j.gastro.2016.02.015[↩]
- Posovszky C, Roesler V, Becker S, Iven E, Hudert C, Ebinger F, Calvano C, Warschburger P. Roles of Lactose and Fructose Malabsorption and Dietary Outcomes in Children Presenting with Chronic Abdominal Pain. Nutrients. 2019 Dec 16;11(12):3063. doi: 10.3390/nu11123063[↩]
- Xue M, Chen X, Shi L, Si J, Wang L, Chen S. Small-bowel capsule endoscopy in patients with unexplained chronic abdominal pain: a systematic review. Gastrointest Endosc. 2015 Jan;81(1):186-93. https://doi.org/10.1016/j.gie.2014.04.062[↩]
- Kim W, Lee B, Yoo A, Kim S, Joo M, Park JJ. Predictors of Positive Video Capsule Endoscopy Findings for Chronic Unexplained Abdominal Pain: Single-Center Retrospective Study and Meta-Analysis. Diagnostics (Basel). 2021 Nov 16;11(11):2123. doi: 10.3390/diagnostics11112123[↩][↩]
- Gijsbers CF, Benninga MA, Schweizer JJ, Kneepkens CM, Vergouwe Y, Büller HA. Validation of the Rome III criteria and alarm symptoms for recurrent abdominal pain in children. J Pediatr Gastroenterol Nutr. 2014 Jun;58(6):779-85. doi: 10.1097/MPG.0000000000000319[↩]
- Helgeland H, Flagstad G, Grøtta J, Vandvik PO, Kristensen H, Markestad T. Diagnosing pediatric functional abdominal pain in children (4-15 years old) according to the Rome III Criteria: results from a Norwegian prospective study. J Pediatr Gastroenterol Nutr. 2009 Sep;49(3):309-15. doi: 10.1097/MPG.0b013e31818de3ab[↩]
- Clouse RE, Mayer EA, Aziz Q, Drossman DA, Dumitrascu DL, Mönnikes H, Naliboff BD. Functional abdominal pain syndrome. Gastroenterology. 2006 Apr;130(5):1492-7. doi: 10.1053/j.gastro.2005.11.062[↩]
- Banez GA. Chronic abdominal pain in children: what to do following the medical evaluation. Curr Opin Pediatr. 2008 Oct;20(5):571-5. doi: 10.1097/MOP.0b013e32830c6ef1[↩]
- Grover M, Drossman DA. Functional abdominal pain. Curr Gastroenterol Rep. 2010 Oct;12(5):391-8. doi: 10.1007/s11894-010-0125-0[↩]
- MacVicar E, Insch P, Summers F, Bruce D, Ramsay G. Quantitative Assessment of Secondary Healthcare Utilisation by Patients With Functional Abdominal Pain. Cureus. 2022 May 19;14(5):e25145. doi: 10.7759/cureus.25145[↩]
- Stordal K., Nygaard E.A., Bentsen B. Organic abnormalities in recurrent abdominal pain in children. Acta Paediatr. 2001;90:638–642. doi: 10.1111/j.1651-2227.2001.tb02426.x[↩]
- Gijsbers C.F., Schweizer J.J., Buller H.A. Protozoa as a cause of recurrent abdominal pain in children. J. Pediatr. Gastroenterol. Nutr. 2013;57:603–606. doi: 10.1097/MPG.0b013e31829f1bc0[↩]
- Lebenthal E., Rossi T.M., Nord K.S., Branski D. Recurrent abdominal pain and lactose absorption in children. Pediatrics. 1981;67:828–832.[↩]
- Garg N., Basu S., Singh P., Kumar R., Sharma L., Kumar P. Prevalence of abnormal lactose breath hydrogen tests in children with functional abdominal pain. Indian J. Gastroenterol. 2017;36:179–183. doi: 10.1007/s12664-017-0750-8[↩]
- Gomara R.E., Halata M.S., Newman L.J., Bostwick H.E., Berezin S.H., Cukaj L., See M.C., Medow M.S. Fructose intolerance in children presenting with abdominal pain. J. Pediatr. Gastroenterol. Nutr. 2008;47:303–308. doi: 10.1097/MPG.0b013e318166cbe4[↩]
- Wintermeyer P., Baur M., Pilic D., Schmidt-Choudhury A., Zilbauer M., Wirth S. Fructose malabsorption in children with recurrent abdominal pain: Positive effects of dietary treatment. Klin. Padiatr. 2012;224:17–21. doi: 10.1055/s-0031-1279747[↩]
- Dabritz J., Muhlbauer M., Domagk D., Voos N., Hennebohl G., Siemer M.L., Foell D. Significance of hydrogen breath tests in children with suspected carbohydrate malabsorption. BMC Pediatr. 2014;14:59. doi: 10.1186/1471-2431-14-59[↩]
- Di Lorenzo C., Nurko S. Rome IV Pediatric Functional Gastrointestinal Disorders—Disorders of Gut-Brain Interaction. 1st ed. The Rome Foundation; Raleigh, NC, USA: 2016.[↩]
- Hyams J.S., Di Lorenzo C., Saps M., Shulman R.J., Staiano A., van Tilburg M. Functional Disorders: Children and Adolescents. Gastroenterology. 2016 doi: 10.1053/j.gastro.2016.02.015[↩]
- Wils P, Caron B, D’Amico F, Danese S, Peyrin-Biroulet L. Abdominal Pain in Inflammatory Bowel Diseases: A Clinical Challenge. J Clin Med. 2022 Jul 22;11(15):4269. doi: 10.3390/jcm11154269[↩]
- Lacy BE, Pimentel M, Brenner DM, Chey WD, Keefer LA, Long MD, Moshiree B. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. Am J Gastroenterol. 2021 Jan 1;116(1):17-44. https://journals.lww.com/ajg/fulltext/2021/01000/acg_clinical_guideline__management_of_irritable.11.aspx[↩]
- Ford AC, Lacy BE, Talley NJ. Irritable Bowel Syndrome. N Engl J Med. 2017 Jun 29;376(26):2566-2578. doi: 10.1056/NEJMra1607547[↩]
- Drossman DA, Hasler WL. Rome IV-Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology. 2016 May;150(6):1257-61. doi: 10.1053/j.gastro.2016.03.035[↩]





{kind=link}