Contents
Mediastinal fibrosis
Mediastinal fibrosis also known as fibrosing mediastinitis or sclerosing mediastinitis, is a rare disease that causes fibrous tissue (scar tissue) and inflammation to build up in your mediastinum (middle portion of the chest, situated between the lungs) and hilar areas (the wedge-shaped regions at the center of each lung that allow for the passage of blood vessels, nerves, and bronchi) of your chest causing narrowing and obstruction of important chest structures, including pulmonary arteries, pulmonary veins, the superior vena cava (SVC), airways/bronchi, or the esophagus (foodpipe) 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13. Your mediastinum is the middle portion of your thoracic cavity between your lungs, extending from the base of your neck (from your first rib and sternum) to the diaphragm (Figure 4). Your mediastinum contains your heart (pericardial cavity, peri- = around; -cardial = heart, a fluid-filled space that surrounds your heart), the major blood vessels connected to your heart and lungs, the trachea (windpipe) and bronchi, the esophagus (foodpipe), the thymus, and lymph nodes but not your lungs. Your right and left lungs are on either side of the mediastinum. Mediastinal fibrosis or fibrosing mediastinitis primarily presents in younger patients and this slowly progressive disease has been associated with a high mortality if it affects both lungs.
There are 2 recognized subtypes of mediastinal fibrosis:
- Post-histoplasma fibrosing mediastinitis also called histoplasmosis fibrosing mediastinitis. Post-histoplasma fibrosing mediastinitis is thought to represent an abnormally prolonged and robust immune reaction to a remote infection with the soil-based fungus called Histoplasma capsulatum, perhaps related to ongoing reaction to residual fungal antigens found within lymph nodes regions of the central chest 14, 15. However, post-histoplasma fibrosing mediastinitis is a rare complication of pulmonary histoplasmosis occurring in less than 1% of cases 6.
- Histoplasmosis is a lung infection caused by breathing in Histoplasma capsulatum, the most common endemic parasitic fungus in the United States 16, 17, 18, 19. Histoplasma capsulatum fungus resides in soil and thrives when specific conditions with respect to acidity, temperature, nitrogen content, and humidity are present, resulting in large geographic areas of endemicity, most notably along the Mississippi and Ohio River valleys. It also occasionally causes disease in Central and South America. Histoplasma capsulatum fungus also spreads in bird and bat droppings that mix in soil. In the United States, the fungus mainly lives in the central and eastern states. Histoplasma species are also found in Europe, Asia, Africa, and Australia, though histoplasmosis is less prevalent in these regions. It also flourishes in soil fertilized by bird droppings and is found in bat guano; chicken houses and caves or bridge underpasses contaminated with guano are notorious sources of Histoplasma capsulatum infection. In urban settings, most exposure is probably related to soil disruption leading to fungal spores becoming airborne. The inhaled fungus typically causes a limited, asymptomatic infection. A minority of people will experience nonspecific upper respiratory or flu-like symptoms, with progressive pneumonia requiring antifungal treatment being uncommon. Histoplasmosis is often misdiagnosed or diagnosed late because the symptoms are similar to more common pneumonias caused by bacteria or viruses. Histoplasmosis can develop into a long-term lung infection, specifically among people with weakened immune systems. In rare cases, it can spread to other parts of the body, including the brain and spinal cord (meningitis). Disseminated or systemic histoplasmosis is rare and most often observed in those who are severely immunocompromised. In endemic areas in the United States, nearly all persons are exposed/infected in childhood. It is not known why some individuals develop an excessively exuberant immune response to the Histoplasma capsulatum fungus, leading to the excessive scarring and obstruction of blood vessels or airways that characterizes fibrosing mediastinitis 15. Fungal yeast forms have been observed to persist within mediastinal lymph nodes; these specimens almost never grow in culture, indicating they most likely represent long-dead fungus, but the continued presence of fungal antigens within or around these fungal forms may stimulate an ongoing immune response in some individuals. Calcification of formerly infected lymph nodes is typical but may require years to develop. Calcifications are also frequently observed within the abnormal mediastinal tissue of post-histoplasma fibrosing mediastinitis.
- Histoplasmosis is a lung infection caused by breathing in Histoplasma capsulatum, the most common endemic parasitic fungus in the United States 16, 17, 18, 19. Histoplasma capsulatum fungus resides in soil and thrives when specific conditions with respect to acidity, temperature, nitrogen content, and humidity are present, resulting in large geographic areas of endemicity, most notably along the Mississippi and Ohio River valleys. It also occasionally causes disease in Central and South America. Histoplasma capsulatum fungus also spreads in bird and bat droppings that mix in soil. In the United States, the fungus mainly lives in the central and eastern states. Histoplasma species are also found in Europe, Asia, Africa, and Australia, though histoplasmosis is less prevalent in these regions. It also flourishes in soil fertilized by bird droppings and is found in bat guano; chicken houses and caves or bridge underpasses contaminated with guano are notorious sources of Histoplasma capsulatum infection. In urban settings, most exposure is probably related to soil disruption leading to fungal spores becoming airborne. The inhaled fungus typically causes a limited, asymptomatic infection. A minority of people will experience nonspecific upper respiratory or flu-like symptoms, with progressive pneumonia requiring antifungal treatment being uncommon. Histoplasmosis is often misdiagnosed or diagnosed late because the symptoms are similar to more common pneumonias caused by bacteria or viruses. Histoplasmosis can develop into a long-term lung infection, specifically among people with weakened immune systems. In rare cases, it can spread to other parts of the body, including the brain and spinal cord (meningitis). Disseminated or systemic histoplasmosis is rare and most often observed in those who are severely immunocompromised. In endemic areas in the United States, nearly all persons are exposed/infected in childhood. It is not known why some individuals develop an excessively exuberant immune response to the Histoplasma capsulatum fungus, leading to the excessive scarring and obstruction of blood vessels or airways that characterizes fibrosing mediastinitis 15. Fungal yeast forms have been observed to persist within mediastinal lymph nodes; these specimens almost never grow in culture, indicating they most likely represent long-dead fungus, but the continued presence of fungal antigens within or around these fungal forms may stimulate an ongoing immune response in some individuals. Calcification of formerly infected lymph nodes is typical but may require years to develop. Calcifications are also frequently observed within the abnormal mediastinal tissue of post-histoplasma fibrosing mediastinitis.
- Idiopathic mediastinal fibrosis. Idiopathic mediastinal fibrosis is very rare and is associated with immunoglobulin G4 (IgG4)-related disease, tuberculosis, sarcoidosis, ANCA vasculitis, systemic lupus erythematosus (SLE), previous radiation to the mediastinum, certain drugs (e.g. methysergide, cabergoline and bromocriptine) and rare histiocytic disorders (a group of rare diseases that occur when there is an overproduction of histiocytes [a type of white blood cells] that can lead to organ failure and tumors e.g., Langerhans cell histiocytosis, juvenile xanthogranuloma, Erdheim-Chester disease, hemophagocytic lymphohistiocytosis, Rosai-Dorfman disease, certain kinds of leukemia and malignant tumors) 20, 21, 22, 23. Tuberculosis is considered the second leading cause of mediastinal fibrosis, especially in nonendemic areas of histoplasmosis 24. The hallmarks immunoglobulin G4 (IgG4)-related disease are dense lymphoplasmacytic infiltrations with a predominance of IgG4-positive plasma cells in the affected tissue, associated with a degree of fibrosis that has a distinguished “storiform” pattern and is often characterized by obliterative phlebitis and an increased number of eosinophils with elevated serum concentrations of IgG4 8. Unfortunately, measuring immunoglobulin G4 (IgG4) in serum has not been clinically relevant as it has not shown correlation with the presence of disease or its severity 7, 21.
- Idiopathic fibrosing mediastinitis may present with one of two main radiological patterns – focal or diffuse disease 20. Focal fibrosing mediastinitis usually involves the right mediastinum, hilar and subcarinal region 25. The diffuse type can extend to the soft-tissue structures of the neck, posterior mediastinum and the lung.
- Idiopathic fibrosing mediastinitis is progressive when left untreated and can be staged as follows 26, 23:
- Stage 1 lesions are characterized by oedematous fibromyxoid tissue associated with an inflammatory reaction, thin-walled vessels, and lacking cellular atypia and necrosis.
- Stage 2 lesions are poorly demarcated lesions consisting of haphazardly arranged hyaline material encircling and infiltrating mediastinal structures with minimal inflammatory reaction.
- Stage 3 lesions are obliterative, which involve mediastinal structures, and are characterised by acellular dense collagen and occasional lymphoid aggregates. Spindle cells and inflammatory cells are absent. Dystrophic calcification is commonly seen.
- The majority of patients with idiopathic fibrosing mediastinitis will experience symptoms and exhibit signs of compression of mediastinal structures, which include pulmonary arterial or venous narrowing, superior vena cava obstruction, and airway narrowing 27.
Both subtypes of mediastinal fibrosis are rare.
Mediastinal fibrosis or fibrosing mediastinitis symptoms typically do not develop until the disease has progressed to the point of causing severe compromise of blood flow within an affected vessel (e.g., pulmonary arteries, pulmonary veins, the superior vena cava [SVC]) or air flow within an affected central airway (bronchi) 28, 10. Thin-walled blood vessels with low intraluminal pressure, such as superior vena cava (SVC) and less frequently, the pulmonary arteries, are especially subjected to compression by mediastinal masses resulting in increased intravascular pressure. Due to its extended course through the mediastinum, the right pulmonary artery is more susceptible to mediastinal processes compared to the left pulmonary artery 29. The build-up of scar tissue (fibrosis) usually occurs very slowly (1 mm/year approximately), though more rapid growth has been observed occasionally. Symptoms may appear suddenly, even though the process has progressed slowly for years, once a critical limitation of blood/air flow occurs. The growth of mediastinal scar tissue itself causes no symptoms.
The diagnosis of mediastinal fibrosis can be very challenging. There is no definitive diagnostic test and tissue biopsies are typically complicated and risky. CT and MR imaging are crucial in both diagnosing and treating fibrosing mediastinitis 30 . These imaging techniques play a key role in helping doctor identify and manage cases of mediastinal fibrosis effectively.
Fibrosing mediastinitis can have an unpredictable course, with both spontaneous remission or exacerbation of symptoms being reported.
Several treatment strategies for mediastinal fibrosis have been described including medical, surgical and non- surgical interventions. Since fungal antigens are thought to play a role in the pathogenesis of mediastinal fibrosis, antifungal therapy has been used as part of the medical treatment but has not shown efficacy and is not currently recommended 6.
Idiopathic mediastinal fibrosis is usually a progressive disease with no evidence-based therapeutic options 31, 32. Oral corticosteroids are the most commonly used medical treatment and have been associated with variable success. Other potentially efficacious therapies include tamoxifen, methotrexate and mycophenolate mofetil 33, 34, 35, 36. Rituximab has also been shown to be associated with a favourable therapeutic response in patients with progressive and refractory disease 37. The combination of corticosteroids and methotrexate has been reported to provide resolution of symptoms and improvement of hemodynamic parameters related to pulmonary hypertension 32. Surgical biopsy should be performed in patients with poor response to therapy. Surgical resection is curative in localized disease and may ameliorate symptoms. A complete resection may require vascular and airway reconstruction, which is associated with high morbidity and mortality. Patients with bilateral mediastinal involvement, extensive fibrosis, calcifications and collateral vessels are generally not suitable for surgery 38. Symptomatic patients can also be treated with local therapies directed towards re-establishing patency of occluded airways, pulmonary arteries or superior vena cava 39.
Figure 1. Mediastinal fibrosis types
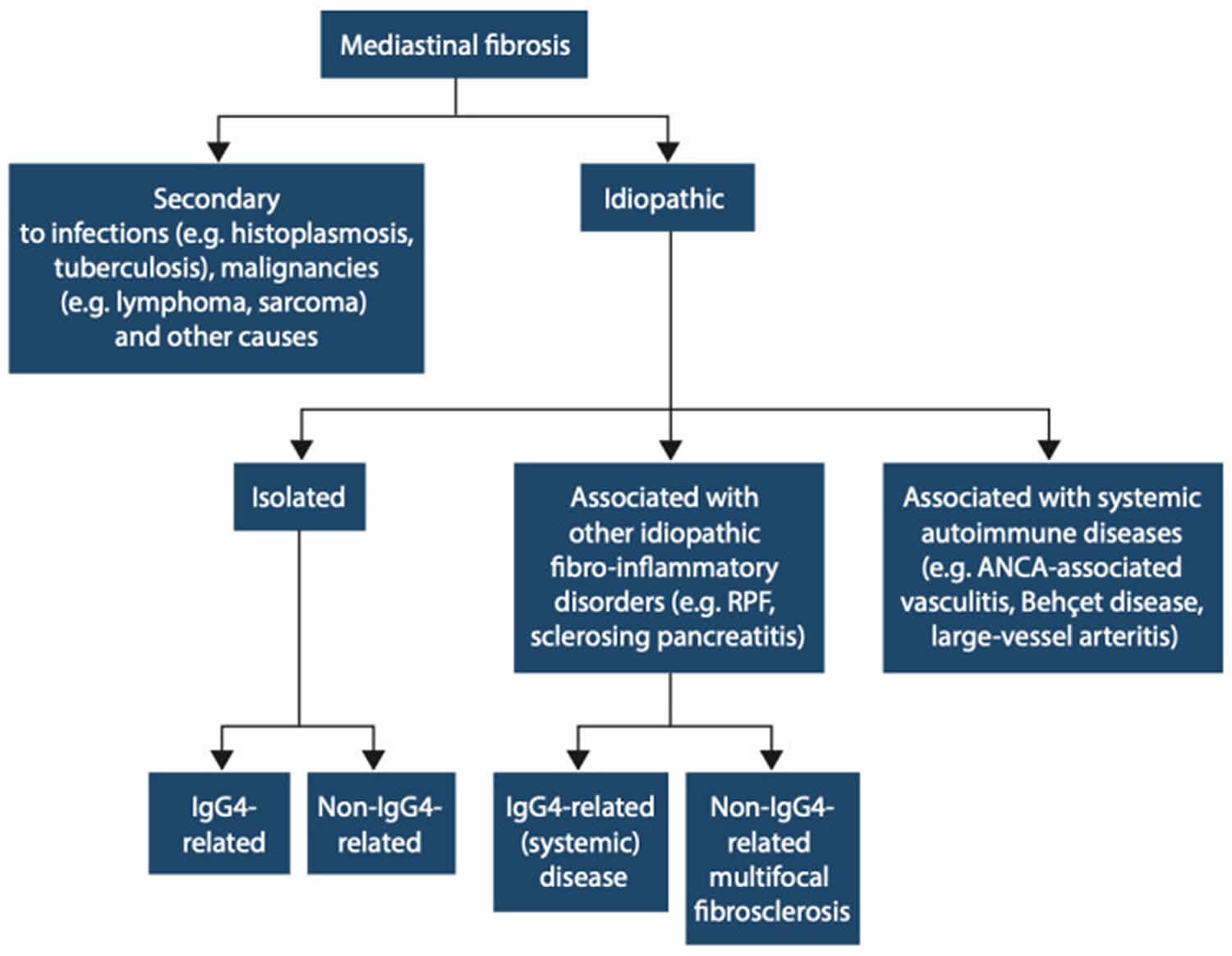
Abbreviations: ANCA = antineutrophil cytoplasmic antibodies; RPF = retroperitoneal fibrosis
[Source 20 ]Figure 2. Fibrosing mediastinitis
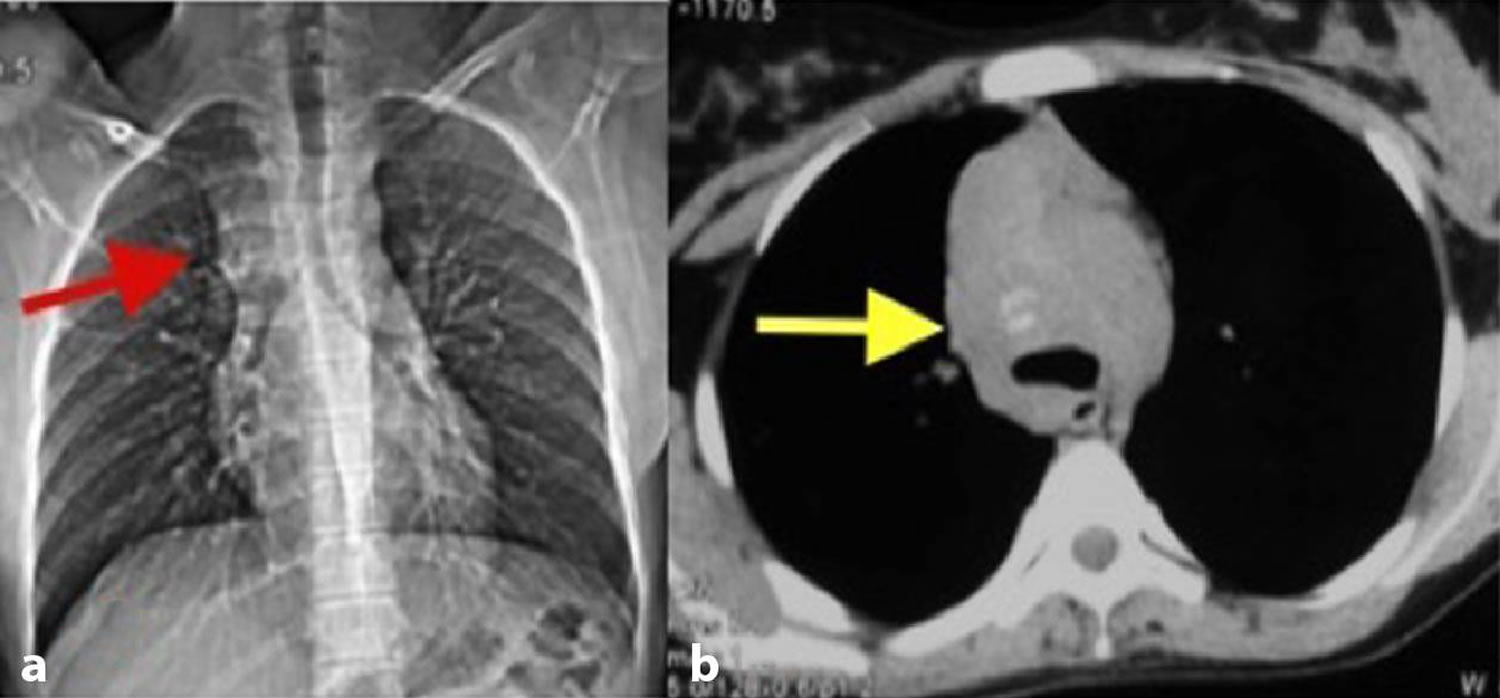
Footnotes: A young female who presented with complaints of breathlessness, occasional cough and diffuse chest pain for 3 months. (a) Chest X-ray reveals widening of the superior mediastinum (red arrow) and (b) an axial non-contrast CT scan of the chest in the mediastinal window shows an ill-defined mass with faint amorphous calcification (yellow arrow).
[Source 40 ]Figure 3. Fibrosing mediastinitis
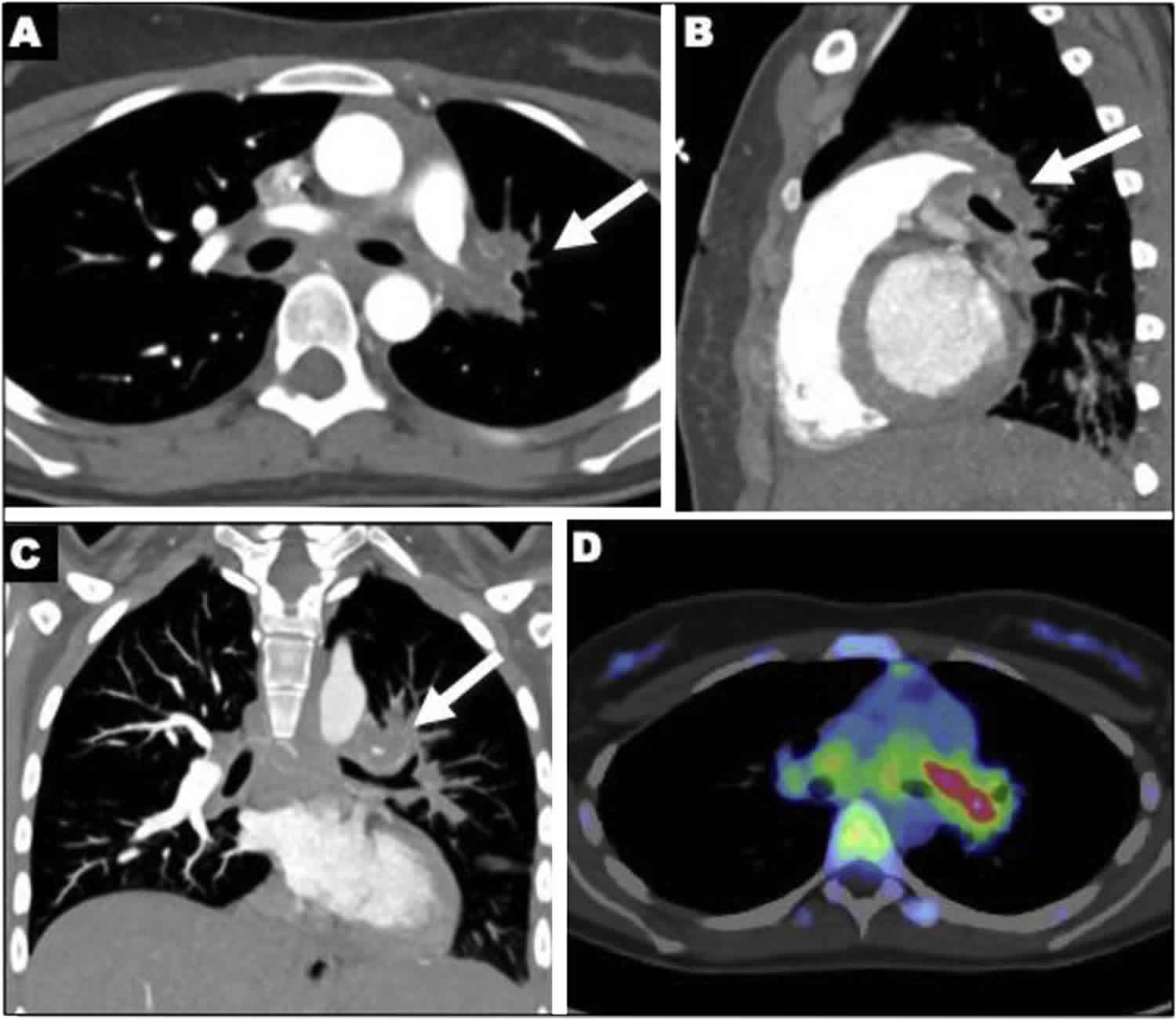
Footnotes: Fibrosing mediastinitis in a 19-year-old female with ulcerative colitis, treated with vedolizumab, developed progressive cough, shortness of breath, and left pleuritic chest pain. Contrast-enhanced computed tomography of chest (CT). Axial (A), sagittal (B) and coronal images (C) demonstrate an occluded left pulmonary artery (arrows) with tissue density encasing the vessel, and extending from the mediastinum to the hilar region. Positive emission tomography (PET) CT axial image the level of the left pulmonary artery (D) shows increased metabolic activity in the left hilum.
[Source 2 ]Figure 4. Histoplasma capsulatum
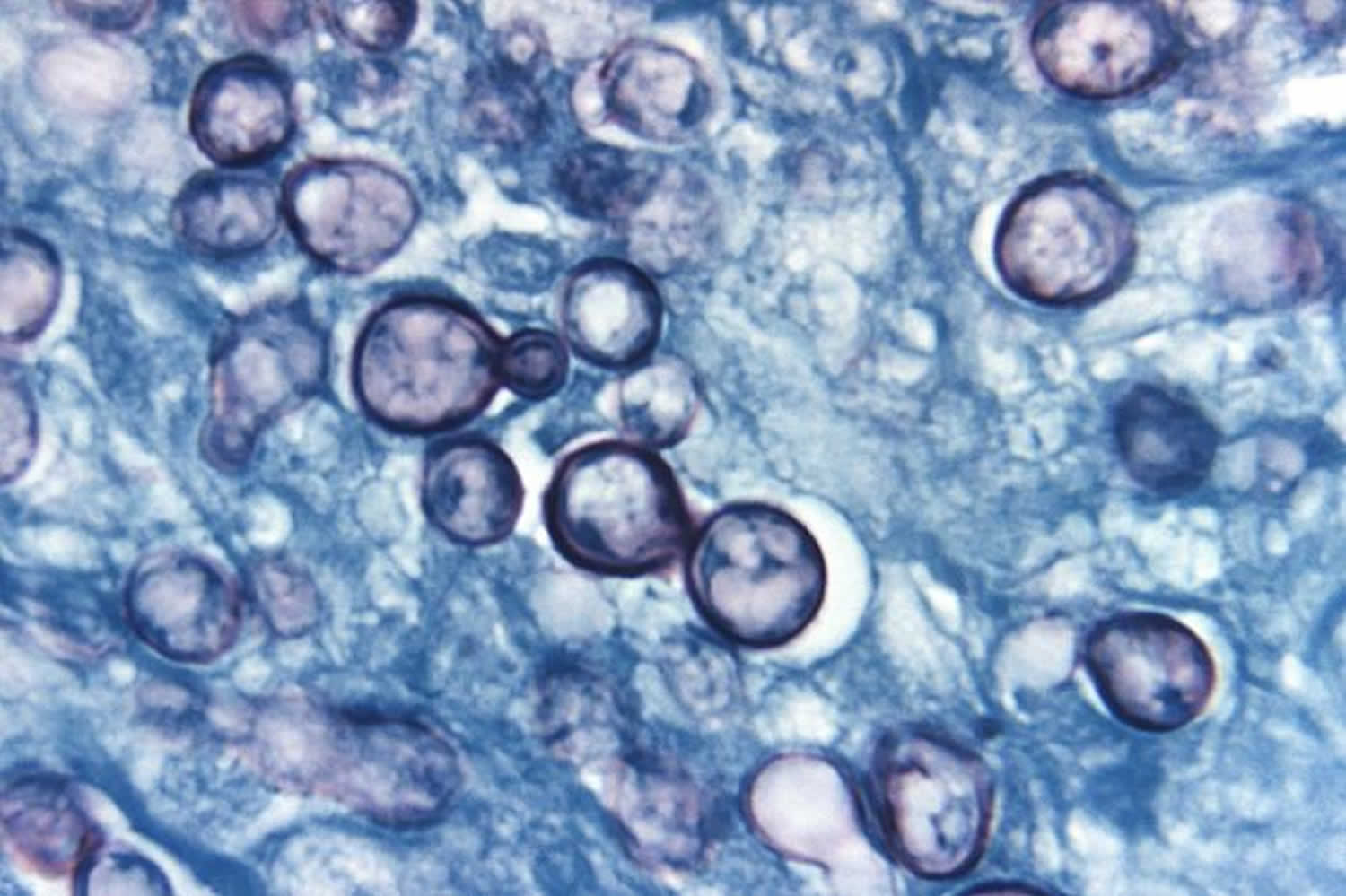
Footnotes: This is a photomicrograph of a methenamine silver stained tissue sample, extracted from a patient with a case of histoplasmosis, due to the fungal organism, Histoplasma capsulatum var. duboisii. Note the presence of typical yeast cells, some of which were undergoing replication by budding.
[Source 41 ]Chest anatomy
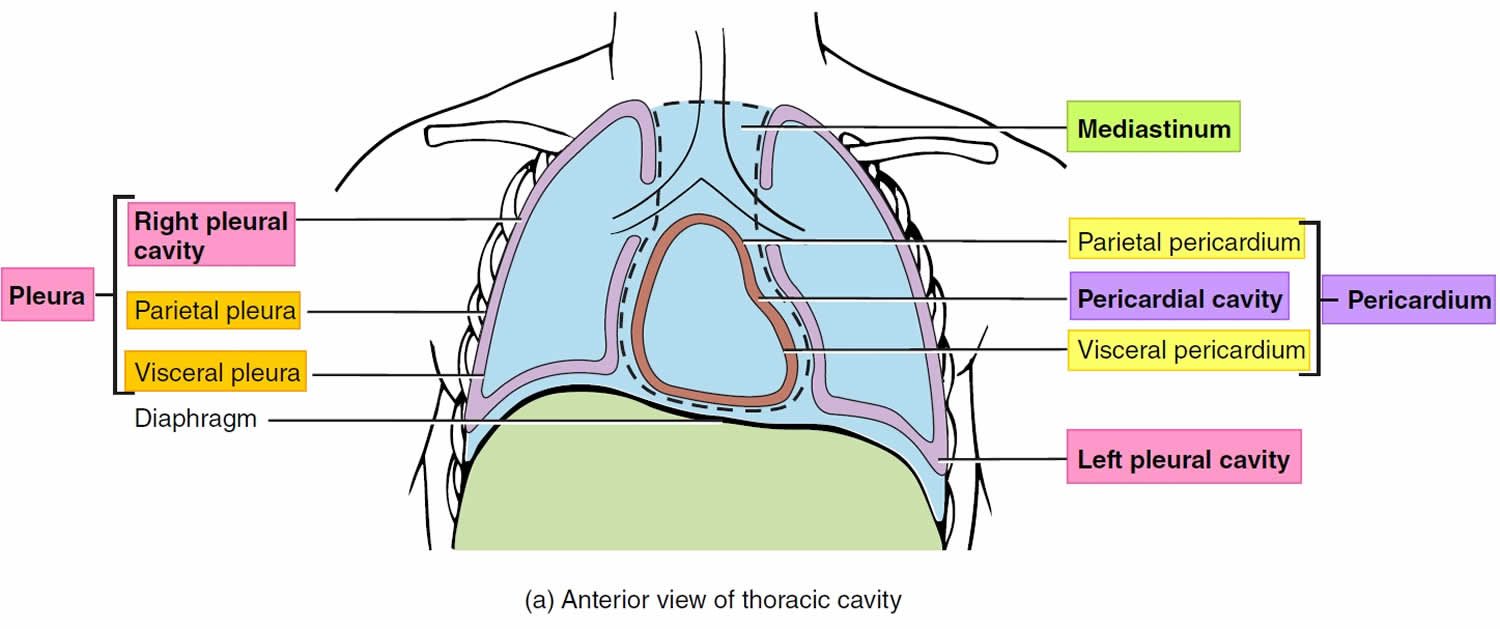
Your chest cavity also called the thoracic cavity is formed by the ribs, the muscles of the chest, the sternum (breastbone), and the thoracic portion of the vertebral column. Within your thoracic cavity are 3 smaller cavities: (a) 2 pleural cavities (fluid-filled spaces one around each lung), your left pleural cavity (holds your left lung) and your right pleural cavity (holds your right lung) and (b) a central portion of your thoracic cavity between your lungs called the mediastinum (media- = middle; -stinum = partition). The mediastinum is the central portion of your thoracic cavity between your lungs, extending from the base of your neck (from your first rib and sternum) to the diaphragm. The mediastinum contains your heart (pericardial cavity, peri- = around; -cardial = heart, a fluid-filled space that surrounds your heart), the major blood vessels connected to your heart and lungs, the trachea (windpipe) and bronchi, the esophagus (foodpipe), the thymus, and lymph nodes but not your lungs. Your right and left lungs are on either side of the mediastinum. The diaphragm is a dome-shaped muscle that separates the thoracic cavity from the abdominopelvic cavity.
Your mediastinum is divided into several parts, which researchers call compartments. The traditional or classical model divides your mediastinum into four parts:
- Superior mediastinum: The top part, located superior to (above) your heart.
- Anterior mediastinum: The part anterior to (in front of) your heart, between your heart and your sternum (breastbone).
- Middle mediastinum: The part that contains your heart.
- Posterior mediastinum: The part posterior to (behind) your heart.
A membrane is a thin, pliable tissue that covers, lines, partitions, or connects internal organs (viscera). One example is a slippery, double-layered membrane associated with body cavities that does not open directly to the exterior called a serous membrane. Serous membrane covers your internal organs (viscera) within the thoracic and abdominal cavities and also lines the walls of the thorax and abdomen. The parts of a serous membrane are (1) the parietal layer (outer layer), a thin epithelium that lines the walls of the cavities, and (2) the visceral layer (inner layer), a thin epithelium that covers and adheres to the viscera within the cavities. Between the two layers is a potential space that contains a small amount of lubricating fluid (serous fluid). The fluid allows the internal organs (viscera) to slide somewhat during movements, such as when the lungs inflate and deflate during breathing.
Within the right and left sides of your thoracic cavity (chest cavity), the compartments that contain your lungs, on either side of the mediastinum, are lined with a membrane called the parietal pleura (outer serous membrane) lining the inside of your rib cage (parietal pleura lines the chest wall) and covering the superior surface of the diaphragm. A similar membrane, called the visceral pleura (inner serous membrane), clings to the surface of your lungs forming the external surface of your lung. The visceral (inner) and parietal (outer) pleural membranes are separated only by a thin film of watery fluid called serous fluid, which is secreted by the parietal and visceral pleural membranes. Although no actual space normally exists between the parietal (outer) and visceral (inner) pleural membranes, the potential space between them is called the pleural cavity. The parietal pleura (outer membrane) and visceral pleura (inner membrane) slide with little friction across the cavity walls as your lungs move, expand and collapse during respiration.
Your respiratory system includes the trachea, the right and left lungs and their lobes, and the bronchi. Oxygen (O2) is inhaled into your lungs and passes through the alveoli (the tiny air sacs at the end of the bronchioles) and into your bloodstream, where it travels to the tissues throughout the body.
Figure 5. Chest anatomy

Figure 6. Thoracic cavity
Footnote: The black dashed lines indicate the borders of the mediastinum.
Figure 7. Thoracic cavity transverse section
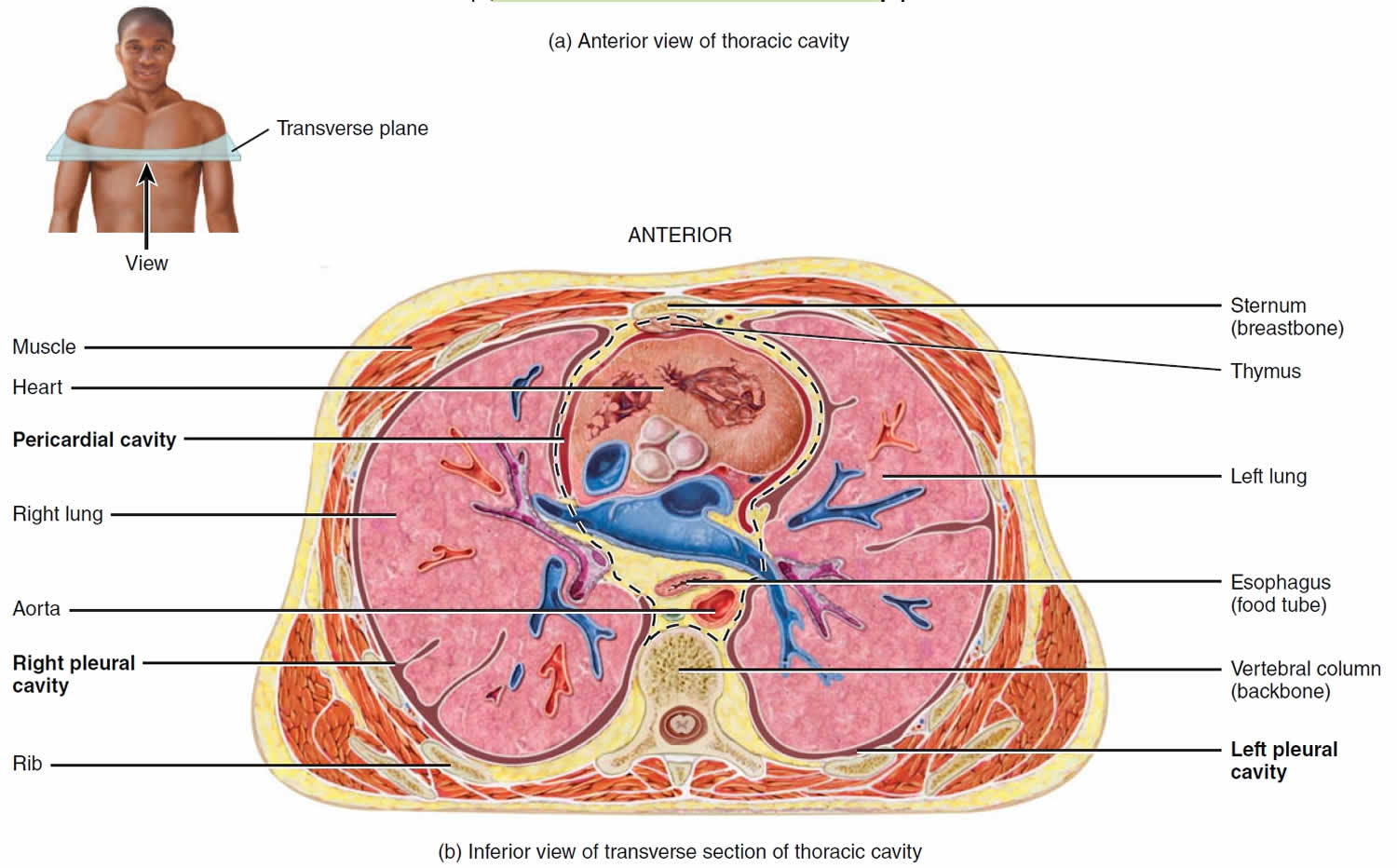
Figure 8. Mediastinum
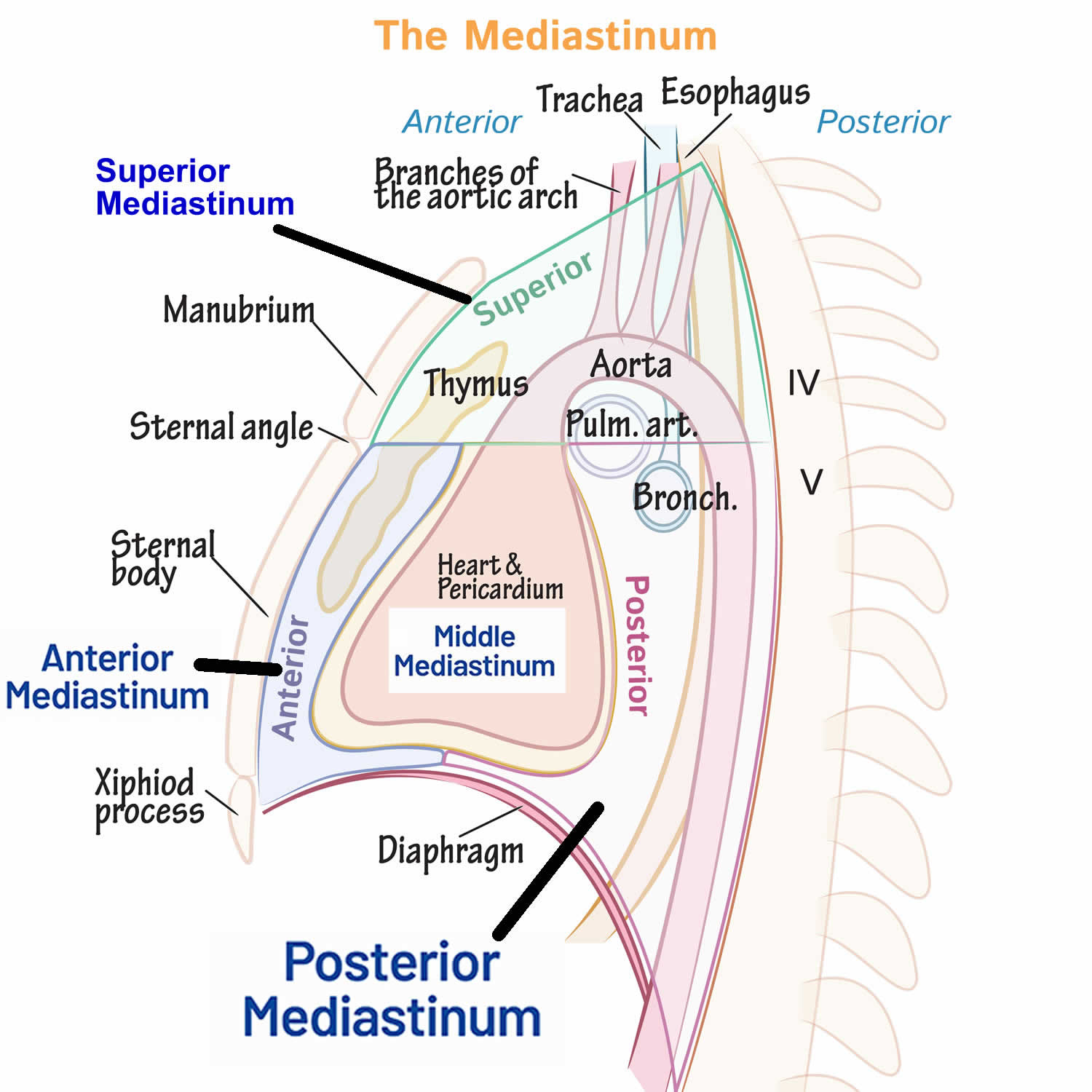
Figure 9. Human heart anatomy

Mediastinal fibrosis causes
In the majority of patients, mediastinal fibrosis or fibrosing mediastinitis is triggered by the body’s abnormal excessive immune reaction to prior exposure to Histoplasma capsulatum fungus found in soil in endemic areas, most notably along the Mississippi and Ohio River valleys in the United States 17, 14. In the United States, the fungus mainly lives in the central and eastern states 42. The Histoplasma capsulatum fungus resides in the soil, becomes airborne when the soil is disturbed, and is subsequently inhaled. Histoplasma is also associated with bird and bat droppings, the former of which do not appear to become infected by the fungus but may carry the fungus on their feathers, while the gastrointestinal tracts of the latter may become colonized with the fungus 42. Histoplasmosis does not spread between people or between people and pets (cats and dogs) 42. After the Histoplasma spores enter the lungs, the person’s body temperature allows the spores to transform into yeast. The yeast can then travel to lymph nodes and can spread to other parts of the body through the bloodstream. Outbreaks of histoplasmosis are not common. Of the few that have been reported, most occurred after events that disturb soil contaminated with bird or bat droppings.
Certain groups of people are at higher risk for getting histoplasmosis and for more severe infections, including people who 43:
- Have HIV/AIDS.
- Receive an organ transplant.
- Take medications such as corticosteroids or TNF-inhibitors.
- Are exposed to large amounts of the fungus such as:
- Outdoor workers
- Construction workers
- Farmers, especially if handling or cleaning up after chickens.
Adults over the age of 55 and infants are more at risk for histoplasmosis 43.
It is possible to get histoplasmosis more than once, but it is usually milder after the first infection 43. The body’s immune system that built up to fight the first infection offers some protection.
People with weakened immune systems may not fully fight off histoplasmosis after their first infection even if they feel better. It can remain hidden in the body for months or years and later cause symptoms again (relapse of infection).
Of the entire population who are exposed to Histoplasma, only a tiny fraction (far fewer than 1%) develop the excessive response to the fungal infection that is the basis of post-histoplasma fibrosing mediastinitis. Of the many millions of people with repeated exposures to Histoplasma while living in endemic areas, the vast majority never develop symptomatic histoplasmosis, and far fewer go on to develop post-histoplasma fibrosing mediastinitis. It is estimated that there are only a few hundred cases of post-histoplasma fibrosing mediastinitis in the United States. At Vanderbilt University Medical Center, a referral center for this condition in an endemic area, approximately 10 new cases have been evaluated annually over the last few decades. Post-histoplasma fibrosing mediastinitis is seen only in individuals who lived in an endemic region sometime during their life. Idiopathic mediastinal fibrosis is believed to be even rarer, with an estimated several dozen cases known in the United States.
Idiopathic mediastinal fibrosis is not related to histoplasmosis. Idiopathic mediastinal fibrosis has been reported in the setting of autoimmune diseases, tuberculosis, sarcoidosis, systemic lupus erythematosus (SLE), Behcet disease, ANCA-associated vasculitides including granulomatosis with polyangiitis (a rare autoimmune disorder that causes inflammation of blood vessels. It can affect the lungs, kidneys, nose, sinuses, and ears and can damage vital organs), immunoglobulin G4 (IgG4)-related disease, rheumatic fever, previous mediastinal radiation therapy, severe viral infections of Coxsackie B virus, treatment with methysergide maleate (an ergot-derived serotonin antagonists previously used in the treatment of migraine) or trauma 44, 5, 45, 46. Idiopathic mediastinal fibrosis can occur in association with other idiopathic fibroinflammatory disorders at sites outside the chest, including retroperitoneal fibrosis, sclerosing cholangitis, Riedel thyroiditis (a rare inflammatory disease of the thyroid that causes the thyroid to harden and become fibrous), pseudotumor of the orbit, and rare histiocytic disorders (a group of rare diseases that occur when there is an overproduction of histiocytes [a type of white blood cells] that can lead to organ failure and tumors e.g., Langerhans cell histiocytosis, juvenile xanthogranuloma, Erdheim-Chester disease, hemophagocytic lymphohistiocytosis, Rosai-Dorfman disease, certain kinds of leukemia and malignant tumors) and others many of which are now recognized as other manifestations of systemic IgG4-related disease 47. Tuberculosis is considered the second leading cause of mediastinal fibrosis, especially in nonendemic areas of histoplasmosis 24.
Mediastinal fibrosis signs and symptoms
Mediastinal fibrosis signs and symptoms varies depending on which of the intrathoracic structures are compromised. Mediastinal fibrosis or fibrosing mediastinitis symptoms typically do not develop until the disease has progressed to the point of causing severe compromise of blood flow within an affected vessel (e.g., pulmonary arteries, pulmonary veins, the superior vena cava [SVC]) or air flow within an affected central airway (bronchi). Pulmonary, bronchial vasculature, superior vena cava (SVC), and esophageal compression can occur in up to 47%, 26%, 19% and 2% of cases, respectively 6, 32. The build-up of scar tissue (fibrosis) usually occurs very slowly (1 mm/year approximately), though more rapid growth has been observed occasionally. Symptoms may appear suddenly, even though the process has progressed slowly for years, once a critical limitation of blood/air flow occurs. The growth of mediastinal scar tissue itself causes no symptoms.
Typically, people with post-histoplasma mediastinal fibrosis were originally exposed or infected with Histoplasma capsulatum fungus as children but the symptoms begin in most patients in the third or fourth decade of life. No evidence suggests an association with specific ancestry or gender. Patients may present with shortness of breath (dyspnea), fatigue or loss of stamina, cough with blood (hemoptysis) or without, chronic chest (pleuritic) pain, recurrent pulmonary infections or pneumonias, difficulty swallowing (dysphagia), or swelling of the arms and face. These symptoms most commonly occur because there is an obstruction or critical narrowing of one of the main blood vessels in the chest, such as the superior vena cava (the vein which returns blood from the head, neck, and arms the heart), pulmonary arteries, and/or pulmonary veins. Superior vena cava syndrome (SVCS), characterized by face and arm swelling due to obstruction of the superior vena cava (SVC), is a common symptom. Some patients do not develop superior vena cava syndrome (SVCS) despite having obstruction of the superior vena cava (SVC) because collateral alternative veins sometimes visible on the anterior chest enlarge sufficiently to bypass the superior vena cava (SVC) as it becomes slowly obstructed and successfully return blood to the heart. Cough and shortness of breath are the most common symptoms when obstruction of a central airway occurs (bronchi). Pulmonary venous obstruction usually presents with shortness of breath, coughing blood, or sometimes collection of fluid in the space between the lung and the chest wall (pleural effusion). Symptoms can be present for years before diagnosis.
Patients with idiopathic mediastinal fibrosis are usually young and present with symptoms related to obstruction of vital mediastinal structures, such as the esophagus, airways, pulmonary arteries or veins and central systemic veins 20. The most common presenting complaints include cough, shortness of breath, coughing up blood (hemoptysis) and pleuritic chest pain 48. Hemoptysis can affect up to 20% of patients and has several potential causes in patients with fibrosing mediastinitis 49. Airway obstruction with a post-obstructive necrotizing pneumonia, invasion of a bronchus by fibrous tissue, and pulmonary hypertension from pulmonary vascular compression are the most common clinically encountered mechanisms. Obstruction of the pulmonary arteries, in particular, may lead to extensive anastomoses with intercostal or bronchial arteries, which increases the risk for massive hemoptysis 50. They may also have fibrosis or inflammation elsewhere in the body which may cause symptoms at those other sites.
Mediastinal fibrosis complications
Mediastinal fibrosis complications may include:
- Superior vena cava compression/obstruction/thrombosis
- Pulmonary hypertension 51
- Esophageal compression
- Airway stenosis/obstruction 52
- Mediastinal perivascular pseudoaneurysms, bulges in an artery that’s contained by the tissue around it 53
Mediastinal fibrosis diagnosis
The diagnosis of mediastinal fibrosis can be very challenging. There is no definitive diagnostic test and tissue biopsies are typically complicated and risky. Diagnosing either form of mediastinal fibrosis is best accomplished by chest CT, a scan that shows the abnormal tissue in the mediastinum. The characteristic appearance of a mediastinal abnormality on chest CT scan in a person who has lived in a region with endemic histoplasmosis can definitively diagnose post-histoplasma mediastinal fibrosis in many cases, especially when assessed by a chest specialist or radiologist with expertise in this disease.
A chest CT scan enhanced with intravenous contrast is often necessary to highlight any vascular narrowing which may be present. Non-enhanced chest CT scans are also useful for definitively identifying calcifications within the abnormal mediastinal tissue, which are characteristic of post-histoplasma mediastinal fibrosis. A perfusion nuclear medicine scan might also be performed to quantify the degree of reduction in blood flow to parts of the lung by vascular narrowing. Magnetic resonance angiography (MRA) of the heart or cardiac MRI (cMRI) can be helpful in special circumstances, especially to better evaluate the pulmonary veins where they enter the left atrium, which are commonly affected by mediastinal fibrosis.
The chest CT scan might also demonstrate one or more nodules within lung tissue, which may also have internal calcifications. These lung nodules often represent the initial focus of inhaled Histoplasma infection within the lungs. Calcifications within the spleen (an immune organ which also helps respond to Histoplasma infection) or, less commonly, the liver, are often also seen. There may be signs of infarction of the lung in patients with complete obstruction of blood flow into or out of a region of the lung, including thickening of septal membranes within the lung or scattered opacities.
In situations where definitive diagnosis is not possible based on the CT scan alone, which most commonly occurs when characteristic internal calcifications within the mediastinal abnormality are absent, Histoplasma serologies are often helpful. This test detects antibodies responding to Histoplasma, and is positive in most but not all cases of post-histoplasma mediastinal fibrosis. Ideally, an assay which detects Histoplasma antibodies by both complement fixation and immunodiffusion should be used. Histoplasma antigen testing, which detects proteins shed by living Histoplasma organisms, is invariably negative in mediastinal fibrosis. Lack of calcifications within a lesion otherwise meeting radiographic criteria for mediastinal fibrosis often also prompts serological evaluation for conditions known to be associated with idiopathic mediastinal fibrosis, including IgG4-related disease and granulomatosis with polyangiitis.
Occasionally, biopsy of abnormal mediastinal tissue is required to exclude malignancy such as a lymphoma, especially if the CT scan shows that the abnormal tissue lacks internal calcifications characteristic of a post-Histoplasma syndrome. This can be accomplished via bronchoscopy using linear endobronchial ultrasound guidance to obtain transbronchial needle aspiration samples of the lesion, via CT-guided transthoracic needle biopsy, or surgical biopsy via thoracotomy or mediastinoscopy. Of note, bronchoscopic biopsy should be approached with caution if the lesion is most likely a mediastinal granuloma based on radiographic appearance, as transbronchial sampling of these lesions via the non-sterile airways can contaminate them with bacteria and lead to an infection requiring surgical intervention. Given this, and the fact that the primary alternative diagnosis in many such cases is lymphoma, which tends to require a large surgical biopsy specimen for definitive characterization, surgical biopsy is often preferred to distinguish between mediastinal granuloma and lymphoma. Intra-operative recognition of an encapsulated mediastinal granuloma also permits marsupialization of the lesion via resection of the free wall of the mediastinal granuloma capsule during the same procedure, which is the therapeutic operation of choice for this condition.
An 18-fludeoxyglucose (FDG)-positron emission tomography (PET) scan may show evidence of radiotracer uptake in active inflammatory areas; however, owing to variable fludeoxyglucose (FDG) avidity, it is not routinely used for the evaluation of granulomatous fibrosing mediastinitis 54, 55.
Diagnosis may be delayed for years because symptoms are not specific or characteristic findings are not recognized on scans. Erroneous initial diagnoses include asthma, pneumonia, chronic obstructive lung disease, pulmonary embolism with lung infarction, and, in cases involving compromise of the pulmonary veins, mitral stenosis with congestive heart failure. The current widespread use of CT of the chest has greatly improved detection and diagnosis of mediastinal fibrosis.
Mediastinal fibrosis treatment
There is no standard therapy for either form of mediastinal fibrosis. The natural history of idiopathic mediastinal fibrosis is not known, but there are reports of individual patients who improve after treatment with drugs directed at the underlying cause. There are also some cases of spontaneous improvement in idiopathic mediastinal fibrosis, which has not been seen in post-histoplasma mediastinal fibrosis. Reports of individual patients with idiopathic mediastinal fibrosis due to various underlying diseases describe use of the following drugs: prednisone, tamoxifen, non-steroid anti-inflammatory medication such as indomethacin, and immunosuppressants such as azathioprine or cyclosporin 56, 57, 58, 59. Data is not available about the effectiveness of these treatments, and most reports are individual cases, so it is not possible to be sure whether a favorable response was actually caused by the treatment.
There are no known effective medical therapies for post-histoplasma mediastinal fibrosis. Antifungal therapies and corticosteroids have not demonstrated benefit. A single small study involving three patients with mediastinal fibrosis exhibiting metabolic overactivity within the abnormal fibrotic tissue (as evidenced by intense uptake of 18 fluorodeoxyglucose [FDG] on positron emission tomography [PET] scan) demonstrated decrease in the metabolic activity and some decrease in the size of the mediastinal abnormalities after treatment with rituximab. This work has not been duplicated in a larger study or studied in a clinical trial, so it remains unclear if rituximab represents an effective treatment.
Medical treatments can help address some of the symptoms and complications caused by fibrosing mediastinitis. When fluid retention occurs related to vascular obstructions, patients are treated with diuretic therapy. Antibiotics can be used to treat complications such as pneumonia. Regular exercise is beneficial for heart and muscle function, and is encouraged for all patients as tolerated.
Given the lack of effective medical therapies for post-histoplasma mediastinal fibrosis, a mechanical approach has been used to address narrowings caused by mediastinal fibrosis. When blood vessels carrying blood to or from the lungs are blocked, pulmonary arterial and/or pulmonary venous catheterization with stenting of the affected vessel(s) to prop them open can be done to restore more normal blood flow 60. Stenting can also be used to address narrowing of the superior vena cava if it is causing symptoms of superior vena cava syndrome (SVCS) including arm or neck swelling, headaches 61, 62, 63, 64, 65. These vascular stenting procedures are typically performed by interventional radiologists or interventional cardiologists. When airways are narrowed by scar tissue, airway stents can be placed via bronchoscopy to hold these airways open. This is generally used as a last resort, as these stents may also promote airway inflammation by foreign body reaction or friction with airway mucosa, which sometimes leads to worsened inflammatory airway narrowing.
If the scar tissue of mediastinal fibrosis is localized, surgical resection has been used rarely, but is high risk and appropriate for very few patients. This is not a preferred method of treatment and should only be used in the most extreme cases due to a high level of morbidity and mortality associated with surgery in this condition. Surgical intervention should only be considered at specialized centers with extensive experience in managing mediastinal fibrosis.
Finally, patients with mediastinal fibrosis can cough up blood (hemoptysis). This may happen via several mechanisms, including an increase in blood pressure in the pulmonary circulation due to pulmonary venous obstruction or narrowing (“pseudo-mitral stenosis”), or the creation of more fragile arterial collateral vessels to bypass obstructed pulmonary arteries which can rupture in the airways. The latter, which generally results in a larger degree of bleeding and is occasionally life-threatening, can be addressed via angiography to identify the aberrant vessel(s) which can then be selectively embolized. The former is generally self-limited but recurrent episodes can be a significant nuisance and lead to repeated hospitalizations. Inhaled tranexamic acid can be used to shorten these episodes.
Mediastinal fibrosis prognosis
The prognosis of mediastinal fibrosis depends on the subtype, post-histoplasma mediastinal fibrosis versus idiopathic mediastinal fibrosis, and the extent of involvement of mediastinal structures 10. Idiopathic mediastinal fibrosis has not been well studied due to its extreme rarity, but existing data suggests it is rarely life threatening. Post-histoplasma mediastinal fibrosis affects one lung in approximately 80% of affected individuals and both lungs in the remaining 20%. Progressive one sided disease often leads to the loss of function of that lung, sometimes referred to as “autoamputation”. With a remaining healthy lung, life expectancy tends to be normal. Chest pain from blood vessel narrowing, intermittent coughing up of blood (hemoptysis), fluid collecting outside of the affected lung (pleural effusion) and intermittent pneumonias may continue to affect some individual with one sided disease.
The early mortality rate when fibrosing mediastinitis affects both lungs is up to 30% 66, 67, 68. Recognition of bilateral disease should lead to careful consideration of vascular stenting when vascular narrowing(s) are present. This is associated with symptomatic improvement in most patients and may improve survival in those with both lungs affected. Vascular stenting may also be considered in unilateral disease associated with refractory chest discomfort or pleural effusion.
- Fibrosing Mediastinitis. https://rarediseases.org/rare-diseases/fibrosing-mediastinitis[↩]
- Argueta F, Villafuerte D, Castaneda-Nerio J, Peters J, Restrepo C. Successful management of fibrosing mediastinitis with severe vascular compromise: Report of two cases and literature review. Respir Med Case Rep. 2019 Dec 14;29:100987. doi: 10.1016/j.rmcr.2019.100987[↩][↩]
- Rajput AK, Rajan KE, Vardhan V, Tewari SC, Borcar JM. MEDIASTINAL FIBROSIS. Med J Armed Forces India. 2000 Jan;56(1):82-84. doi: 10.1016/S0377-1237(17)30106-5[↩]
- Seferian A., Steriade A., Jais X., Planche O., Savale L., Parent F., et al. (2015). Pulmonary hypertension complicating fibrosing mediastinitis. Medicine 94:e1800 10.1097/MD.0000000000001800[↩]
- Rossi G. M., Emmi G., Corradi D., Urban M. L., Maritati F., Landini F., et al. (2016). Idiopathic mediastinal fibrosis: a systemic immune-mediated disorder. A case series and a review of the literature. Clin. Rev. Allergy Immunol. 52 446–459. 10.1007/s12016-016-8584-1[↩][↩]
- Peikert T., Colby T.V., Midthun D.E., Pairolero P.C., Edell E.S., Schroeder D.R., Specks U. Fibrosing mediastinitis: clinical presentation, therapeutic outcomes, and adaptive immune response. Medicine (Baltim.) 2011 Nov;90(6):412–423. doi: 10.1097/MD.0b013e318237c8e6[↩][↩][↩][↩]
- Strock S.B., Mason W., Loyd J.E. Further progress in understanding fibrosing mediastinitis. Am. J. Respir. Crit. Care Med. 2015 Sep 15;192(6):767–768. doi: 10.1164/rccm.201505-0964LE[↩][↩]
- Khalid M, Weheba I, Abdelsayed A, Zeitouni LM, Saleemi S, Al Mutairy E, Hassan S. Superior vena cava stenting in IgG4-associated mediastinal fibrosis. Ann Saudi Med. 2020 Mar-Apr;40(2):155-158. doi: 10.5144/0256-4947.2020.155[↩][↩]
- Ezzahi M, Ennasery Z, Malih SE, Akammar A, Bouardi NE, Haloua M, Alaoui Lamrani MY, Boubbou M, Serraj M, Maaroufi M, Smahi M, Bouchra A, Alami B. Mediastinal fibrosis as a late and fatal complication of treated tuberculosis mimicking a neoplastic process in a 34-year-old man. Radiol Case Rep. 2023 Sep 23;18(12):4287-4293. doi: 10.1016/j.radcr.2023.09.001[↩]
- Hu Y, Qiu J-X, Liao J-P, Zhang H, Jin Z, Wang G-Fa. Clinical manifestations of fibrosing mediastinitis in Chinese patients. Chinese Med J. 2016;129(22):2697–2702. doi: 10.4103/0366-6999.193457[↩][↩][↩]
- Chaanoun K, Haouassia FE, Zaghba N, Benjelloun H, Yassine N. Idiopathic Mediastinal Fibrosis: A Study of a Case Using CT and Bronchoscopic Imaging. Cureus. 2024 Mar 1;16(3):e55344. doi: 10.7759/cureus.55344[↩]
- Urschel HC, Patel AN, Razzuk MA, et al. Chronic mediastinitis. In: Patterson GA, Cooper JD, Deslauriers J, et al., eds. Pearson’s Thoracic and Esophageal Surgery (Vol 1). 3rd ed. Philadelphia, PA: Churchill Livingstone Elsevier; 2008:1532–1536.[↩]
- Patil PL, Salkar HR. Idiopathic mediastinal fibrosis presenting as mediastinal compression syndrome. Indian J Med Sci. 2005 Jun;59(6):268-71.[↩]
- Barros N, Wheat JL, Hage C. Pulmonary Histoplasmosis: A Clinical Update. J Fungi (Basel). 2023 Feb 10;9(2):236. doi: 10.3390/jof9020236[↩][↩]
- Takanashi S., Akiyama M., Suzuki K., Otomo K., Takeuchi T. IgG4-related fibrosing mediastinitis diagnosed with computed tomography-guided percutaneous needle biopsy: two case reports and a review of the literature. Medicine (Baltim.) 2018 Jun;97(22) doi: 10.1097/MD.0000000000010935[↩][↩]
- Histoplasmosis. https://www.cdc.gov/histoplasmosis/about[↩]
- Akram SM, Koirala J. Histoplasmosis. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448185[↩][↩]
- Valentin LI, Kuban JD, Ramanathan R, Whigham CJ. Endovascular Treatment of Bilateral Pulmonary Artery Stenoses and Superior Vena Cava Syndrome in a Patient with Advanced Mediastinal Fibrosis. Tex Heart Inst J. 2016 Jun 1;43(3):249-51. doi: 10.14503/THIJ-15-5091[↩]
- Gustafson MR, Moulton MJ. Fibrosing mediastinitis with severe bilateral pulmonary artery narrowing: RV-RPA bypass with a homograft conduit. Tex Heart Inst J. 2012;39(3):412-5. https://pmc.ncbi.nlm.nih.gov/articles/PMC3368482[↩]
- Manyeruke FD, Perumal R, Symons G, Mottay L. Idiopathic fibrosing mediastinitis. Afr J Thorac Crit Care Med. 2021 Jun 23;27(2):10.7196/AJTCCM.2021.v27i2.064. doi: 10.7196/AJTCCM.2021.v27i2.064[↩][↩][↩][↩]
- Peikert T, Shrestha B, Aubry MC, Colby TV, Ryu JH, Sekiguchi H, Smyrk TC, Specks U, Yi ES. Histopathologic Overlap between Fibrosing Mediastinitis and IgG4-Related Disease. Int J Rheumatol. 2012;2012:207056. doi: 10.1155/2012/207056[↩][↩]
- Oka S, Uramoto H, Yamada S, Tanaka F. Sclerosing mediastinitis of unknown origin: Report of a case. Int J Surg Case Rep. 2015;10:5–7. doi: 10.1016/j.ijscr.2015.03.013[↩]
- Flieder DB, Suster S, Moran CA. Idiopathic fibroinflammatory (fibrosing/sclerosing) lesions of the mediastinum: a study of 30 cases with emphasis on morphologic heterogeneity. Mod Pathol. 1999 Mar;12(3):257-64.[↩][↩]
- Mole TM, Glover J, MN1021193 Sheppard Sclerosing mediastinitis: a report on 18 cases. Thorax. 1995;50(3):280–283. doi: 10.1136/thx.50.3.280[↩][↩]
- Devaraj A, Griffin N, Nicholson AG, Padley SPG. Computed tomography findings in fibrosing mediastinitis. Clin Radiol. 2007;62(8):781–786. doi: 10.1016/j.crad.2007.03.002[↩]
- Rossi GM, Emmi G, Corradi D, et al. Idiopathic mediastinal fibrosis: A systemic immune-mediated disorder. A case series and a review of the literature. Clin Rev Allergy Immunol. 2017;52(3):446–459. doi: 10.1007/s12016-016-8584-1[↩]
- Lindholm KE, de Groot P, Moran CA. Fibrosing/sclerosing lesions of the mediastinum: A review. Adv Anat Pathol. 2019;26(4):235–240. doi: 10.1097/pap.0000000000000223[↩]
- Sherrick A. D., Brown L. R., Harms G. F., Myers J. L. (1994). The radiographic findings of fibrosing mediastinitis. Chest 106 484–489. 10.1378/chest.106.2.484[↩]
- Su J, Simonsen U, Carlsen J, Mellemkjaer S. Pulmonary Artery Occlusion and Mediastinal Fibrosis in a Patient on Dopamine Agonist Treatment for Hyperprolactinemia. Front Pharmacol. 2017 Jul 20;8:492. doi: 10.3389/fphar.2017.00492[↩]
- Rossi SE, McAdams HP, Rosado-de-Christenson ML, Franks TJ, Galvin JR. Fibrosing mediastinitis. Radiographics. 2001;21(3):737–757. doi: 10.1148/radiographics.21.3.g01ma17737[↩]
- Westerly B.D., Johnson G.B., Maldonado F., Utz J.P., Specks U., Peikert T. Targeting B lymphocytes in progressive fibrosing mediastinitis. Am. J. Respir. Crit. Care Med. 2014 Nov 1;190(9):1069–1071. doi: 10.1164/rccm.201407-1258LE[↩]
- Joury A.U., Al Boukai A.A., Kashour T.S. Severe fibrosing mediastinitis with atypical presentation: effective control with novel therapeutic approach. Ann. Thorac. Med. 2017 Jul-Sep;12(3):209–212. doi: 10.4103/atm.ATM_47_17[↩][↩][↩]
- Li Y, Meng X, Wang Y, Yang Y, Lu X. Fibrosing mediastinitis with pulmonary hypertension as a complication of pulmonary vein stenosis: A case report and review of the literature. Medicine. 2018;97(4):e9694. doi: 10.1097/md.0000000000009694[↩]
- Ikeda K, Nomori H, Mori T, et al. Successful steroid treatment for fibrosing mediastinitis and sclerosing cervicitis. Ann Thorac Surg. 2007;83(3):1199–1201. doi: 10.1016/j.athoracsur.2006.09.034[↩]
- Ichimura H, Ishikawa S, Yamamoto T, et al. Effectiveness of steroid treatment for hoarseness caused by idiopathic fibrosing mediastinitis: Report of a case. Surg Today. 2006;36(4):382–384. doi: 10.1007/s00595-005-3161-x[↩]
- Joury AU, Boukai AAA, Kashour TS. Severe fibrosing mediastinitis with atypical presentation: Effective control with novel therapeutic approach. Ann Thorac Med. 2017;12(3):209. doi: 10.4103/atm.atm_47_17[↩]
- Wu Z, Jarvis H, Howard LS, Wright C, Kon OM. Post-tuberculous fibrosing mediastinitis: A review of the literature. BMJ Open Respir Res. 2017;4(1):e000174. doi: 10.1136/bmjresp-2016-000174[↩]
- Westerly BD, Johnson GB, Maldonado F, Utz JP, Specks U, Peikert T. Targeting B lymphocytes in progressive fibrosing mediastinitis. Am J Respir Crit Care Med. 2014;190(9):1069. doi: 10.1164/rccm.201407-1258le[↩]
- Sinha D, Kundaragi NG, Kale SK, Sharma S. Fibrosing mediastinitis mimicking as chronic pulmonary thromboembolism. BJR Case Rep. 2019;6(1):20190049. doi: 10.1259/bjrcr.20190049[↩]
- Jain N, Chauhan U, Puri SK, Agrawal S, Garg L. Fibrosing mediastinitis: when to suspect and how to evaluate? BJR Case Rep. 2016 Jan 19;2(1):20150274. doi: 10.1259/bjrcr.20150274[↩]
- Histoplasma capsulatum. https://phil.cdc.gov/Details.aspx?pid=4221[↩]
- How People Get Histoplasmosis. https://www.cdc.gov/histoplasmosis/causes/index.html[↩][↩][↩]
- Reducing Risk for Histoplasmosis. https://www.cdc.gov/histoplasmosis/prevention/index.html[↩][↩][↩]
- Graham J. R., Suby H. I., LeCompte P. R., Sadowsky N. L. (1966). Fibrotic disorders associated with methysergide therapy for headache. N. Engl. J. Med. 274 359–368. 10.1056/NEJM196602172740701[↩]
- Kanne JP., Mohammed T-LH. Fibrosing mediastinitis associated with Behçet’s disease: CT findings. Clin Radiol. 2007;62(11):1124–1126. doi: 10.1016/j.crad.2007.07.007[↩]
- Bahler C, Hammoud Z, Sundaram C. Mediastinal fibrosis in a patient with idiopathic retroperitoneal fibrosis. Interact CardioVasc Thorac Surg. 2008;7(2):336–338. doi: 10.1510/icvts.2007.166033[↩]
- Clinton Bahler, Zane Hammoud, Chandru Sundaram, Mediastinal fibrosis in a patient with idiopathic retroperitoneal fibrosis, Interactive CardioVascular and Thoracic Surgery, Volume 7, Issue 2, April 2008, Pages 336–338, https://doi.org/10.1510/icvts.2007.166033[↩]
- Worrell JA, Donnelly EF, Martin JB, Bastarache JA, Loyd JE. Computed tomography and the idiopathic form of proliferative fibrosing mediastinitis. J Thorac Imaging. 2007;22(3):235–240. doi: 10.1097/01.rti.0000213589.29472.18[↩]
- Peikert TD, Colby TV, Midthun DE, et al. Fibrosing mediastinitis: Clinical presentation, therapeutic outcomes and adaptive immune response. Medicine. 2011;90(6):412–423. doi: 10.1097/md.0b013e318237c8e6[↩]
- Schade MA, Mirani NM. Fibrosing mediastinitis: An unusual cause of pulmonary symptoms. J Gen Intern Med. 2013;28(12):1677. doi: 10.1007/s11606-013-2528-8[↩]
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M; ESC Scientific Document Group. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016 Jan 1;37(1):67-119. doi: 10.1093/eurheartj/ehv317[↩]
- Carrana SH, Buckley JR, Rosado-de-Christenson ML, Martínez-Jiménez S, Muñoz P, Borsa JJ. Multimodality Imaging of Focal and Diffuse Fibrosing Mediastinitis. Radiographics. 2019 May-Jun;39(3):651-667. doi: 10.1148/rg.2019180143[↩]
- Tabotta F, Ferretti GR, Prosch H, Boussouar S, Brun AL, Roos JE, Ebner L, Letovanec I, Brauner M, Beigelman-Aubry C. Imaging features and differential diagnoses of non-neoplastic diffuse mediastinal diseases. Insights Imaging. 2020 Oct 15;11(1):111. doi: 10.1186/s13244-020-00909-z[↩]
- Takalkar AM, Bruno GL, Makanjoula AJ, El-Haddad G, Lilien DL, Payne DK. A Potential Role for F-18 FDG PET/CT in Evaluation and Management of Fibrosing Mediastinitis. Clin Nucl Med. 2007 Sep;32(9):703-6. doi: 10.1097/RLU.0b013e318125035b[↩]
- McNeeley MF, Chung JH, Bhalla S, Godwin JD. Imaging of granulomatous fibrosing mediastinitis. AJR Am J Roentgenol. 2012 Aug;199(2):319-27. doi: 10.2214/AJR.11.7319[↩]
- Dunn EJ, Ulicny KS, Jr, Wright CB, Gottesman L. Surgical implications of sclerosing mediastinitis: a report of six cases and review of the literature. Chest. 1990;97(2):338–346. doi: 10.1378/chest.97.2.338[↩]
- Loyd JE, Tillman BF., Atkinson JB., Des Prez RM. Mediastinal fibrosis complicating histoplasmosis. Medicine. 1988;67(5):295–310. doi: 10.1097/00005792-198809000-00002[↩]
- Mathisen DJ, Grillo HC. Clinical manifestation of mediastinal fibrosis and histoplasmosis. Ann Thorac Surg. 1992;54:1053Y1057. doi: 10.1016/0003-4975(92)90069-g[↩]
- Urschel HC, Jr, Razzuk MA, Netto GJ, Disiere J, Chung SY. Sclerosing mediastinitis: improved management with histoplasmosis titer and ketoconazole. Ann Thorac Surg. 1990;50:215Y221. doi: 10.1016/0003-4975(90)90737-q[↩]
- Bardet J, Fabre D, Brenot P, Watkins C, Fadel E. Kissing Stents for Superior Vena Cava Syndrome Due to Mediastinal Fibrosis. Open J Cardiovasc Surg. 2018 May 29;10:1179065218771900. doi: 10.1177/1179065218771900[↩]
- Breault S, Doenz F, Jouannic AM, Qanadli SD. Percutaneous endovascular management of chronic superior vena cava syndrome of benign causes : long-term follow-up. Eur Radiol. 2017 Jan;27(1):97-104. doi: 10.1007/s00330-016-4354-y[↩]
- Sfyroeras GS, Antonopoulos CN, Mantas G, Moulakakis KG, Kakisis JD, Brountzos E, Lattimer CR, Geroulakos G. A Review of Open and Endovascular Treatment of Superior Vena Cava Syndrome of Benign Aetiology. Eur J Vasc Endovasc Surg. 2017 Feb;53(2):238-254. doi: 10.1016/j.ejvs.2016.11.013[↩]
- Rizvi AZ, Kalra M, Bjarnason H, Bower TC, Schleck C, Gloviczki P. Benign superior vena cava syndrome: stenting is now the first line of treatment. J Vasc Surg. 2008 Feb;47(2):372-80. doi: 10.1016/j.jvs.2007.09.071[↩]
- Johansen M, Hoyer M, Kleiman M. Transcatheter treatment of SVC syndrome from histoplasmosis-related mediastinal fibrosis in a 9-year old male. Catheter Cardiovasc Interv. 2013 Nov 1;82(5):E708-11. doi: 10.1002/ccd.24883[↩]
- O’Sullivan GJ, Mhuircheartaigh JN, Ferguson D, Delappe E, O’Riordan C, Browne AM. Isolated pharmacomechanical thrombolysis plus primary stenting in a single procedure to treat acute thrombotic superior vena cava syndrome. J Endovasc Ther. 2010 Feb;17(1):115-23. doi: 10.1583/09-2940.1[↩]
- Murphy JC, Johnston N, Spence MS. A pressing matter–mediastinal fibrosis with near obliteration of the pulmonary arteries. Catheter Cardiovasc Interv. 2013;81(6):1079–83. doi: 10.1002/ccd.24561[↩]
- Thiessen R, Matzinger FR, Seely J, Aina R, Macleod P. Fibrosing mediastinitis: successful stenting of the pulmonary artery. Can Respir J. 2008;15(1):41–4. doi: 10.1155/2008/835921[↩]
- Rossi SE, McAdams HP, Rosado-de-Christenson ML, Franks TJ, Galvin JR. Fibrosing mediastinitis. Radiographics. 2001;21(3):737–57. doi: 10.1148/radiographics.21.3.g01ma17737[↩]





{kind=link}