
Mounjaro
Mounjaro is a brand name of the active drug Tirzepatide that is used to help lower blood sugar levels in type 2 diabetes with the added benefit of weight loss 1, 2, 3, 4, 5. Mounjaro has also been shown to help with weight loss and maintain the lost weight in clinical trials when combined with diet and exercise 6. The reported mean weight reductions of up to 22.9% after nearly 3.5 years of treatment with tirzepatide 7. Current clinical data have shown that tirzepatide is highly efficacious in improving HbA1c levels and reducing body weight 8.
Mounjaro (tirzepatide) is a once-weekly subcutaneous injection that can be self-administered and should be used alongside dietary changes and exercise. The most commonly reported side effects of Mounjaro (tirzepatide) in clinical trials are gastrointestinal problems such as nausea, vomiting, constipation, indigestion (dyspepsia), and stomach (abdominal) pain, diarrhea and decreased appetite 5. Mounjaro (tirzepatide) may also cause serious side effects including inflammation of the pancreas (pancreatitis), low blood sugar (hypoglycemia), allergic reactions, kidney failure, severe stomach problems, and complications of diabetes-related eye disease (diabetic retinopathy) 5. The side effect of hypoglycemia was generally low in Mounjaro (tirzepatide) single therapy trials but increased when used with insulin or sulfonylureas. Mounjaro (tirzepatide) injection site reactions, including pain, redness, and swelling, were commonly reported but typically mild in severity. Approximately 5-10% of patients discontinued Mounjaro (tirzepatide) due to side effects in clinical trials, with higher discontinuation rates (up to 25% in some studies) at the highest doses (15 mg), and lower rates (around 5%) at lower doses (5 mg). The discontinuation rate is dose-dependent, with gastrointestinal side effects being the primary reason for stopping the medication.
In studies with rats, Mounjaro (tirzepatide) caused thyroid tumors, including thyroid cancer 5. It is not known if Mounjaro (tirzepatide) will cause thyroid tumors, or a type of thyroid cancer called medullary thyroid carcinoma (a rare type of thyroid cancer that originates from the parafollicular C cells, which produce calcitonin) in people.
Mounjaro (tirzepatide) is in a class of medications called incretin mimetics. Mounjaro (tirzepatide) works by activating two gut hormone receptors, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptors, to manage blood sugar 9. Mounjaro (tirzepatide) works by helping your pancreas to release the right amount of insulin when your blood sugar levels are high. Insulin helps move sugar from your blood into your body tissues where it is used for energy. Mounjaro (tirzepatide) injection also slows the emptying of your stomach and may increase fullness to decrease appetite and food intake causing weight loss in some people when combined with diet and exercise.
Mounjaro (tirzepatide) received FDA approval to improve blood sugar control in adults with type 2 diabetes on May 13, 2022 10, 11, 12. Mounjaro (tirzepatide) is currently used as a second-line type 2 diabetes medication similar to glucagon-like peptide-1 (GLP-1) drugs, such as semaglutide (Ozempic, Rybelsus), and is administered once weekly via subcutaneous injection with incremental dosage adjustments. Mounjaro (tirzepatide) is not approved for the treatment of type 1 diabetes mellitus and has not undergone studies in people with pancreatitis.
Mounjaro (tirzepatide) injection is used:
- To control blood sugar levels in certain people with type 2 diabetes (condition in which blood sugar is too high because the body does not make or use insulin normally)..
- To treat obstructive sleep apnea (a condition where breathing is stopped for short times while sleeping) in adults with obesity.
- To assist with weight loss when combined with diet and exercise in certain people who are obese or overweight and have weight-related medical problems
There is no Mounjaro generic. The 2 different brands of tirzepatide (Mounjaro and Zepbound) are made by Eli Lilly but are FDA-approved for different conditions.
- Mounjaro (tirzepatide): Specifically approved for type 2 diabetes management in adults.
- Zepbound (tirzepatide): Designated for weight loss treatment in adults.
Mounjaro (tirzepatide) injection comes in clear, colorless to slightly yellow solution (liquid) available in pre-filled single-dose pens of the following strengths 10:
- 2.5 mg/0.5 mL
- 5 mg/0.5 mL
- 7.5 mg/0.5 mL
- 10 mg/0.5 mL
- 12.5 mg/0.5 mL
- 15 mg/0.5 mL
The recommended starting dosage of Mounjaro (tirzepatide) is 2.5 mg injected subcutaneously (into the fatty tissue layer just under the skin) in the abdomen, thigh, or upper arm once a week with or without meals at any time of day 10. The 2.5 mg dosage is for treatment initiation and is not intended for blood sugar control 10.
- Administer Mounjaro (tirzepatide) once weekly, any time of day, with or without meals.
- Inject Mounjaro (tirzepatide) subcutaneously in the abdomen, thigh, or upper arm.
- Rotate injection sites with each dose.
- Inspect Mounjaro (tirzepatide) visually before use. It should appear clear and colorless to slightly yellow. Do not use Mounjaro (tirzepatide) if particulate matter or discoloration is seen.
- When using Mounjaro (tirzepatide) with insulin, administer as separate injections and never mix. It is acceptable to inject Mounjaro (tirzepatide) and insulin in the same body region, but the injections should not be adjacent to each other.
Use Mounjaro (tirzepatide) exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Your doctor will probably start you on a low dose of Mounjaro (tirzepatide) and gradually increase your dose, not more than once every 4 weeks.
The recommended starting dosage of Mounjaro (tirzepatide) is 2.5 mg injected subcutaneously (into the fatty tissue layer just under the skin) in the abdomen, thigh, or upper arm once a week with or without meals at any time of day 10. The 2.5 mg dosage is for treatment initiation and is not intended for blood sugar control 10.
- After 4 weeks, increase the dosage to 5 mg injected subcutaneously once weekly.
- If additional blood sugar control is needed, increase the dosage in 2.5 mg increments after at least 4 weeks on the current dose.
- The maximum dosage of Mounjaro (tirzepatide) is 15 mg injected subcutaneously once weekly.
- If a dose is missed, instruct patients to administer Mounjaro (tirzepatide) as soon as possible within 4 days (96 hours) after the missed dose. If more than 4 days have passed, skip the missed dose and administer the next dose on the regularly scheduled day. In each case, patients can then resume their regular once weekly dosing schedule.
The day of weekly administration can be changed, if necessary, as long as the time between the 2 doses is at least 3 days (72 hours).
Mounjaro (tirzepatide) controls type 2 diabetes but does not cure it. It may take 4 weeks or longer before you feel the full benefit of Mounjaro (tirzepatide). Continue to take Mounjaro (tirzepatide) even if you feel well. Do not stop taking Mounjaro (tirzepatide) without talking to your doctor.
You will be shown how to use the injection pen or vial by your doctor or nurse. You will also be given instructions how to use Mounjaro (tirzepatide). This will tell you how to inject it. Read it carefully. Ask your pharmacist or doctor if you have any questions about how to inject Mounjaro (tirzepatide).
Mounjaro (tirzepatide) can be injected in the abdomen, thigh or upper arm. Rotate injection sites with each dose.
You may change the day of the week you inject Mounjaro (tirzepatide) as long as at least 3 days have passed between doses.
You may administer insulin in the same area as Mounjaro (tirzepatide) but they should not be given right next to each other. Also, you should not mix Mounjaro (tirzepatide) and insulin in the same injection.
Always look at the Mounjaro (tirzepatide) solution before you inject it. It should be clear, colorless to slightly yelow and free of particles. Do not use Mounjaro (tirzepatide) if it is colored (except slightly yellow), cloudy, frozen, or contains solid particles, or if the expiration date on the pen has passed.
Never reuse needles and never share needles or pens. Always remove the needle right after you inject your dose. Dispose of needles in a puncture-resistant container. Ask your doctor or pharmacist how to dispose of the puncture resistant container.
Figure 1. Tirzepatide chemical structure
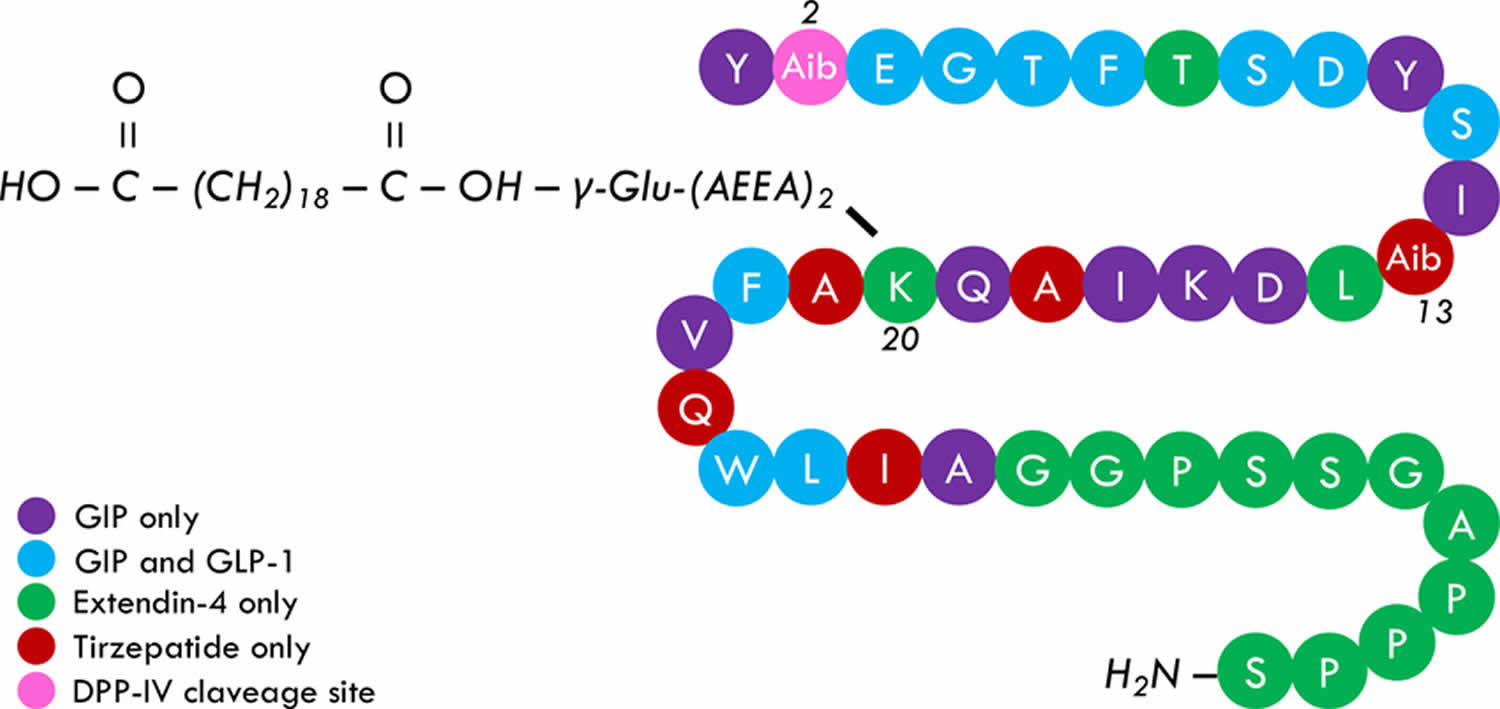
Footnotes: Tirzepatide primary structure. Tirzepatide is a 39-peptide containing different native and not-native incretins fragments, including glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), and Extendin-4 (and glucagon, not shared). Alpha aminobutyric acid is placed in positions 2 and 13 and provides tirzepatide an intrinsic resistance to dipeptidyl-peptidase 4 (DPP-IV) attack and more structural stability, respectively. A 20-carbon fatty acid, namely eicosanedioic acid, is linked to Glu. A 2xAdo unit is attached to the lysine residue in position 20 and allows tirzepatide to be bound to albumin, consequently increasing its half-life to five days. It is currently debated whether the acylation may also increase receptor bounding stability, hypothetically affecting the pharmacological potency of tirzepatide.
[Source 13 ]Mounjaro (Tirzepatide) injection may may increase the risk that you will develop thyroid tumors, including a type of thyroid cancer. Mounjaro (Tirzepatide) injection caused thyroid tumors in rats. It is not known if this medication increases the risk of tumors in humans. Tell your doctor if you or anyone in your family has or ever had thyroid cancer or a condition called Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) syndrome (a rare genetic condition that causes tumors to develop in multiple endocrine glands, primarily the thyroid and adrenal glands. It is caused by a mutation in the RET gene and is inherited in an autosomal dominant pattern). If so, your doctor will probably tell you not to use tirzepatide injection. If you experience any of the following symptoms, call your doctor immediately: lump or swelling in your neck, hoarseness, trouble swallowing, or shortness of breath.
Keep all appointments with your doctor and the laboratory. Your doctor may order certain tests to check your body’s response to tirzepatide.
You will be given the Medication Guide when you begin treatment with tirzepatide and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions. Talk to your doctor about the risk of taking tirzepatide.
Mounjaro safety
Before taking Mounjaro (tirzepatide):
- tell your doctor or pharmacist if you are allergic to this medication, any part of this medication, or any other medications, foods or substances. Tell your doctor or pharmacist about the allergy and what symptoms you had.
- tell your doctor and pharmacist what prescription and nonprescription medications, vitamins, nutritional supplements, and herbal products you are taking or plan to take while using tirzepatide injection. Your doctor may need to change the doses of your medications or monitor you carefully for side effects.
- tell your doctor if you have or have ever had pancreas or kidney disease, stomach problems such as difficulty digesting food, or history of diabetic retinopathy.
- if you are having surgery, including dental surgery, tell the doctor or dentist that you are taking tirzepatide.
- tell your doctor if you are pregnant, plan to become pregnant, or are breast-feeding. If you become pregnant while taking tirzepatide, call your doctor immediately. You should know that tirzepatide may decrease the effectiveness of hormonal contraceptives (birth control pills, patches, rings, and injections). Your doctor may suggest you use another type of birth control for 4 weeks after starting tirzepatide and for 4 weeks after each dose change.
- this medication may cause changes in your blood sugar. Signs and symptoms of low blood sugar may include dizziness or lightheadedness, irritability, sweating, hunger, drowsiness, shakiness, weakness, headache, fast heart rate and feeling jittery. You should know the symptoms of low blood sugar and what to do if you have these symptoms.
- Pancreatitis: Has been reported in clinical trials. Discontinue promptly if pancreatitis is suspected.
- Low blood sugar (hypoglycemia) with concomitant use of insulin secretagogues or insulin: Concomitant use with an insulin secretagogue (a class of drugs used to treat type 2 diabetes by stimulating the pancreas to release more insulin, which helps lower blood sugar e.g., sulfonylureas like glipizide and glyburide and meglitinides such as repaglinide and nateglinide) or insulin
may increase the risk of hypoglycemia, including severe hypoglycemia. Reducing dose of insulin secretagogue or insulin may be necessary. - Hypersensitivity Reactions: Hypersensitivity reactions have been reported. Discontinue Mounjaro (tirzepatide) if suspected.
- Acute Kidney Injury (Acute Kidney Failure): Monitor kidney function in patients with kidney impairment reporting severe adverse gastrointestinal reactions.
- Severe Gastrointestinal Disease: Mounjaro (tirzepatide) use may be associated with gastrointestinal adverse reactions, sometimes severe. Has not been studied in patients with severe gastrointestinal disease and is not recommended in these patients.
- Diabetic Retinopathy Complications in patients with a history of diabetic retinopathy: Has not been studied in patients with non-proliferative diabetic retinopathy requiring acute therapy, proliferative diabetic retinopathy, or diabetic macular edema. Monitor patients with a history of diabetic retinopathy for progression.
- Acute Gallbladder Disease: Has occurred in clinical trials. If cholelithiasis (gallstones) is suspected, gallbladder studies and clinical follow-up are indicated.
Thyroid C-Cell Tumors
In both sexes of rats, tirzepatide caused a dose-dependent and treatment-duration-dependent increase in the incidence of thyroid C-cell tumors (adenomas and carcinomas) in a 2-year study at clinically relevant plasma exposures 10. It is unknown whether Mounjaro (Tirzepatide) causes thyroid C-cell tumors, including medullary thyroid carcinoma (a rare type of thyroid cancer that originates from the parafollicular C cells, which produce calcitonin), in humans as human relevance of tirzepatide-induced rodent thyroid C-cell tumors has not been determined.
Mounjaro (Tirzepatide) is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (a rare type of thyroid cancer that originates from the parafollicular C cells, which produce calcitonin) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (a rare genetic condition that causes tumors to develop in multiple endocrine glands, primarily the thyroid and adrenal glands. It is caused by a mutation in the RET gene and is inherited in an autosomal dominant pattern). People using Mounjaro (tirzepatide) are warned regarding the potential risk for medullary thyroid carcinoma with the use of Mounjaro (Tirzepatide) and are informed regarding symptoms of thyroid tumors (e.g., a mass in the neck, difficulty swallowing, shortness of breath, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of medullary thyroid carcinoma in people taking Mounjaro (tirzepatide). Such monitoring may increase the risk of unnecessary procedures, due to the low test specificity for serum calcitonin and a high background incidence of thyroid disease. Significantly elevated serum calcitonin values may indicate medullary thyroid carcinoma and patients with medullary thyroid carcinoma usually have calcitonin values >50 ng/L. If serum calcitonin is measured
and found to be elevated, the patient should be further evaluated. Patients with thyroid nodules noted on physical examination or neck imaging should also be further evaluated.
Pancreatitis
Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists 10. In clinical studies, 14 events of acute pancreatitis were confirmed by adjudication in 13 Mounjaro-treated patients (0.23 patients per 100 years of exposure) versus 3 events in 3 comparator-treated patients (0.11 patients per 100 years of exposure) 10. Mounjaro (Tirzepatide) has not been studied in patients with a prior history of pancreatitis. It is unknown if patients with a history of pancreatitis are at higher risk for development of pancreatitis on Mounjaro.
After initiation of Mounjaro, observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain, sometimes radiating to the back and which may or may not be accompanied by vomiting). If pancreatitis is suspected, discontinue Mounjaro (tirzepatide) and initiate appropriate management.
Hypersensitivity Reactions
Hypersensitivity reactions have been reported with Mounjaro (tirzepatide) in clinical trials (e.g., urticaria and eczema) and were sometimes severe 10. If hypersensitivity reactions occur, discontinue use of Mounjaro (tirzepatide); treat promptly per standard of care, and monitor until signs and symptoms resolve. Do not use in patients with a previous serious hypersensitivity reaction to tirzepatide or any of the excipients in Mounjaro (tirzepatide).
Anaphylaxis (a severe, life-threatening allergic reaction that must be treated as a medical emergency) and angioedema (a condition where small blood vessels leak fluid into the tissues under the skin, causing swelling in different parts of the body such as your face, lips, tongue, or throat) have been reported with GLP-1 receptor agonists 10. Use caution in patients with a history of angioedema or anaphylaxis with a GLP-1 receptor agonist because it is unknown whether such patients will be predisposed to these reactions with Mounjaro (tirzepatide) 10.
Acute Kidney Injury
Mounjaro (tirzepatide) has been associated with gastrointestinal adverse reactions, which include nausea, vomiting, and diarrhea 10. These events may lead to dehydration, which if severe could cause acute kidney injury (acute kidney failure). In patients treated with GLP-1 receptor agonists, there have been post-marketing reports of acute kidney injury and worsening of chronic kidney failure, which may sometimes require hemodialysis. Some of these events have been reported in patients without known underlying kidney disease. A majority of the reported events occurred in patients who had experienced nausea, vomiting, diarrhea, or dehydration. Monitor kidney function when initiating or escalating doses of Mounjaro (tirzepatide) in patients with kidney impairment reporting severe gastrointestinal adverse reactions 10.
Severe Gastrointestinal Disease
Use of Mounjaro (tirzepatide) has been associated with gastrointestinal adverse reactions, sometimes severe 10. Mounjaro (tirzepatide) has not been studied in patients with severe gastrointestinal disease, including severe gastroparesis (a disorder where the stomach empties too slowly, causing symptoms like nausea, vomiting, bloating, and abdominal pain), and is therefore not recommended in these patients.
Hypoglycemia
Patients receiving Mounjaro (tirzepatide) in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea or other concomitantly administered insulin secretagogue or insulin. Inform patients using these concomitant medications of the risk of hypoglycemia and educate them on the signs and symptoms of hypoglycemia.
Diabetic Retinopathy
Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Mounjaro (tirzepatide) has not been studied in patients with non-proliferative diabetic retinopathy requiring acute therapy, proliferative diabetic retinopathy, or diabetic macular edema. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy.
Acute Gallbladder Disease
Acute events of gallbladder disease such as cholelithiasis (gallstones) or cholecystitis (inflammation of the gallbladder) have been reported in GLP-1 receptor agonist trials and postmarketing. In Mounjaro (tirzepatide) placebo-controlled clinical trials, acute gallbladder disease (cholelithiasis, biliary colic, and cholecystectomy) was reported by 0.6% of Mounjaro-treated patients and 0% of placebo-treated patients. If cholelithiasis (gallstones) is suspected, gallbladder diagnostic studies and appropriate clinical follow-up are indicated.
Drug-Drug Interactions
- People using other glucagon-like peptide-1 (GLP-1) agents, such as semaglutide (Ozempic or Wegovy) or liraglutide (Saxenda, Victoza or Xultophy), should not be prescribed Mounjaro (tirzepatide). Patients on insulin therapy can be initiated on Mounjaro (tirzepatide) therapy and cautiously have the insulin dose decreased to minimize the risk of hypoglycemia 14.
- The efficacy of oral hormonal contraceptives (oral birth control pills) is decreased, so women should be advised to use non-oral contraceptive methods (non-oral birth control pills) or add a barrier contraceptive for 4 weeks after initiation and each dose escalation with tirzepatide.
- Mounjaro (tirzepatide) delays gastric emptying, impacting the absorption of concurrently administered oral medications. This is particularly significant in those with preexisting delayed gastric emptying, as it can worsen these symptoms. Caution is advised when using oral medications dependent on threshold concentrations or with a narrow therapeutic index and tirzepatide 15.
Mounjaro contraindication
Mounjaro (Tirzepatide) is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (a rare type of thyroid cancer that originates from the parafollicular C cells, which produce calcitonin) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (a rare genetic condition that causes tumors to develop in multiple endocrine glands, primarily the thyroid and adrenal glands. It is caused by a mutation in the RET gene and is inherited in an autosomal dominant pattern). People using Mounjaro (tirzepatide) are warned regarding the potential risk for medullary thyroid carcinoma with the use of Mounjaro (Tirzepatide) and are informed regarding symptoms of thyroid tumors (e.g., a mass in the neck, difficulty swallowing, shortness of breath, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of medullary thyroid carcinoma in people taking Mounjaro (tirzepatide). Such monitoring may increase the risk of unnecessary procedures, due to the low test specificity for serum calcitonin and a high background incidence of thyroid disease. Significantly elevated serum calcitonin values may indicate medullary thyroid carcinoma and patients with medullary thyroid carcinoma usually have calcitonin values >50 ng/L. If serum calcitonin is measured
and found to be elevated, the patient should be further evaluated. Patients with thyroid nodules noted on physical examination or neck imaging should also be further evaluated.
Mounjaro mechanism of action
Tirzepatide is a synthetic polypeptide and dual agonist for the glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptors 13, 2, 16. Tirzepatide comprises 39 amino acids and is an analog of the gastric inhibitory polypeptide. Functionally, tirzepatide stimulates insulin release from the pancreas and reduces high blood sugar level. In addition, tirzepatide also increases the levels of adiponectin. Therefore, tirzepatide leads to significantly improved blood sugar control and weight reduction in patients with type 2 diabetes.
Glucose-Dependent Insulinotropic Polypeptide (GIP) is a gastrointestinal polypeptide composed of 42 amino acids secreted by K cells in the duodenum and jejunum mucosae 13. Glucagon-Like Peptide 1 (GLP-1) comprises 31 amino acids and is secreted at the level of L cells in the terminal ileum and colonic mucosae 17. Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptors belong to the seven transmembrane G protein-coupled receptors and are abundantly expressed on the human beta-cell membrane 18, 19. Glucose-dependent insulinotropic polypeptide receptor (GIPR) has also been found on human α-, δ- and γ-cells, while GPL-1 receptor (GLP-1R) is expressed in a minority of human α- and δ-cells. Glucose-dependent insulinotropic polypeptide receptor (GIPR) has also been identified in human subcutaneous and visceral white adipose tissue and cultured osteoblasts. GPL-1 receptor (GLP-1R) is moderately expressed in several brain areas in non-human primates, such as the nucleus accumbens, substantia nigra, and the amygdala, thus playing a role in regulating food intake 13. A weak expression of both receptors has been described in human cardiomyocytes (including sino-atrial node), intestine, pneumocytes, isolated endothelial cells, and seminiferous tubules in mice 18, 19.
Basal glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) concentrations are very low during fasting but increase significantly after meal ingestion 13. Glucose-dependent insulinotropic polypeptide (GIP) release is more evident after carbohydrates and lipids consumption 20, while glucagon-like peptide-1 (GLP-1) release is enhanced by amino acids such as glutamine 18. GLP-1 release appears to be biphasic 21. The first phase of GLP-1 release occurs 10-15 minutes after meal intake. It is probably mediated by neuroendocrine mechanisms that include brainstem vagal stimulation (an anticipatory mechanism), mechanical stretching of the stomach and duodenum due to food transit, GIP release, and gastrin-related peptide from gastric and duodenal mucosae that, in turn, activate vagal efferences to distal intestine. The intestinal transit stimulates the second wave of GLP-1 release throughout L-cells in the distal intestine 21. Glucose-dependent insulinotropic polypeptide (GIP) release occurs rapidly after meal intake and persists over time (up to four hours), with a serum and intestinal peak of concentration two hours later 22.
Insulin suppresses glucose-dependent insulinotropic polypeptide (GIP) secretion resulting from negative feedback, while several cytokines, including interleukins 1 and 6, enhance GIP and GLP-1 release 18, 19. Dipeptidyl-peptidase 4 (DPP-IV) activity is particularly intense, and the enzyme degrades both GIP and GLP-1 a few minutes after their release. Therefore, native GIP and GLP-1 have a short half-life (2-5 minutes), and almost all the action of these incretins takes place in the intestine and the portal vein system. However, a small amount (5-10%) of both incretins reaches the systemic circulation, where GIP and GLP-1 may carry out their pleiotropic effects (e.g., cardiovascular level). Therefore, a large amount of circulating GLP-1 is represented by its inactive peptide GLP-1 with a null or mild antagonistic effect compared to the intact GLP-1 19, 23.
A small amount of GLP-1 originates in the pancreas after the local breakdown of its precursor pro-glucagon. Both systemic and locally originated GLP-1 reach pancreatic islets and regulate insulin, glucagon, and somatostatin secretion 18. Both GIP and GLP-1 enhance insulin secretion in a glucose-dependent manner. Hyperglycemia is a permissive factor to GIP and GLP-1 action as the more the glucose concentration, the great the magnitude of ß-cells membrane depolarization and vice versa 18.
The underlying mechanisms by which GLP-1 suppresses glucagon secretion are still debated and include: 1) a direct GLP-1-mediated suppression of glucagon release, but this hypothesis appears controversial especially considering human α-cells that do not express GLP-1R; 2) an indirect effect due to GLP-1-mediated insulin release; 3) an indirect effect due to GLP-1-mediate somatostatin release 18, 19, 22, 24. GIP enhances glucagon secretion, and this action is directly mediated by GIPR agonism (via intracellular Protein Kinase A pathway) since glucose-dependent insulinotropic polypeptide receptor (GIPR) is abundantly expressed on human α-cells 18, 19. This effect was described in experimental conditions in response to hypoglycemia and euglycemia but not hyperglycemia, suggesting that GIP probably does not contribute to hyperglucagonemia in type 2 diabetes 18, 19.
The incretin effect (the phenomenon where oral glucose leads to a significantly greater insulin release compared to the same amount of glucose given intravenously due to the gut-derived hormones called incretins, primarily glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1)) is dampened in different metabolic conditions such as for overweight or obesity, insulin resistance, impaired glucose tolerance, and type 2 diabetes, in which both incretin secretion and effect are disturbed 22. A GIP resistance has been described in type 2 diabetes due to diminished glucose-dependent insulinotropic polypeptide receptor (GIPR) expression or accelerated glucose-dependent insulinotropic polypeptide receptor (GIPR) clearance. Higher or inappropriately normal levels of GIP are detected in type 2 diabetes patients also during the fast, and the fine regulation of insulin and glucagon release in response to different glycemic levels is problematic. On the other side, GLP-1 response is preserved in type 2 diabetes, but GLP-1 secretion in response to meal consumption weakens over time, making GLP-1-based therapy an effective strategy to manage hyperglycemia as replacement therapy 18, 25, 26.
Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) exhibit extra glycemic effects. GLP-1 slows gastric and duodenal emptying, delays meal digestion, and reduces postprandial glycemic excursion, which, in turn, is an essential target of glycemic control in type 2 diabetes 21. GLP-1 regulates gastrointestinal motility by several mechanisms that include direct activation of vagal efferences (peripheral pathway), cerebral regulation (central pathway), and modulation of local myenteric ganglion activity that controls circular muscle movement, such in a way to reduce evocated peristaltic bustle 21. In addition, GLP-1 reduces food intake by modulating the activity of cerebral areas involved in appetite control, such as the area postrema, amygdala, nucleus accumbens, and substantia nigra 18. The role of GIP in regulating food intake appears controversial. Mechanistic studies revealed that glucose-dependent insulinotropic polypeptide receptor (GIPR) is expressed in cerebral areas that regulate food intake, such as the area postrema, arcuate, and paraventricular nuclei and GIPR expression overlaps GLP-1R expression 27. GIP signaling is expected to directly induce the activation of anorexigenic areas or facilitate GLP-1 action 27. Conversely, GIP seems not to affect gastrointestinal motility when administered in physiologic and supraphysiologic doses 18, 28, and no evidence, to date, has been provided for GIP to facilitate GLP-1-induced gastric empty delay 18, . Incretins could reduce intestinal water resorption, and this mechanism is responsible for diarrhea, a well-recognized adverse effect of GLP-1 receptor agonists (GLP-1RAs).
Glucose-dependent insulinotropic polypeptide (GIP) increases insulin sensibility of white adipose tissue, consequently improving lipid storage and ameliorating lipid profile (mainly triglycerides) and skeletal muscle 18. GIP-mediated actions appear to be additional than those exerted by GLP-1, which improves insulin sensibility in the liver 18.
Glucose-dependent insulinotropic polypeptide (GIP) may stimulate osteoblast activity and bone remodeling, thus providing a possible reduction of fracture risk as similarly observed with GLP-1.
Other effects have been described for GLP-1 (and possibly GIP, with scantier evidence), including anti-inflammatory and vasoactive proprieties 29.
Tirzepatide is an unbalanced dual agonist of glucose-dependent insulinotropic polypeptide receptor (GIPR) and GLP-1 receptor (GLP-1R). Preclinical trials demonstrated that Tirzepatide (LY3298176) exhibited for GIPR the same affinity as native GIP and a five-fold weaker affinity for GLP-1R than the native GLP-1 30. The potency of tirzepatide for glucose-dependent insulinotropic polypeptide receptor (GIPR) is similar to GIP and thirteen-fold lower for GLP-1R than GLP-1 30. The potency of tirzepatide for GLP-1 receptor (GLP-1R) was also inferior compared to Semaglutide 30. In in vitro studies, Tirzepatide stimulated beta-cells response more efficiently than observed with GIP and GLP-1 alone. Also, in vivo, Tirzepatide enhanced insulin secretion by acting on both GIPR and GLP-1R 30.
The dual agonist ability of tirzepatide decreases hyperglycemia significantly more than GLP-1 agonist agents and reduces the patient’s appetite 31. Among patients without type 2 diabetes, administering tirzepatide 5 to 15 mg once weekly for managing obesity led to significant reductions in body weight, ranging from 16.5% to 22.4% over 72 weeks 4. Statistical analysis performed after a study’s data has been collected on fasting biomarkers indicated that tirzepatide exhibited more significant improvements in markers of insulin sensitivity and beta-cell function 32.
Pharmacokinetics
- Absorption: Tirzepatide has a bioavailability of approximately 80%. The time it takes to reach peak serum levels can range from 8 to 72 hours.
- Distribution: The mean steady-state volume of distribution of tirzepatide is approximately 10.3 L. Tirzepatide is highly bound to plasma albumin (99%).
- Metabolism: When injected, the peptide structure undergoes proteolytic cleavage. In addition, the C20 fatty diacid composition undergoes beta-oxidation and amide hydrolysis. Being a modified polypeptide, tirzepatide undergoes metabolism into individual amino acids in various tissues, including the liver 2.
- Elimination: Tirzepatide has a half-life of 5 days, facilitating weekly dosing, and is cleared in urine and feces as metabolites 33.
Mounjaro uses
Mounjaro (Tirzepatide) is US Food and Drug Administration (FDA) approved as an add-on to diet and exercise to improve blood sugar control in adults with type 2 diabetes. Mounjaro (tirzepatide) is currently used as a second-line type 2 diabetes medication and is administered once weekly via subcutaneous injection with incremental dosage adjustments 34, 35.
Current clinical data demonstrated that Mounjaro (tirzepatide) is superior to placebo in improving hemoglobin A1c (HbA1c) levels. The SURPASS-5 clinical trial showed a minus 2.11% reduction in HbA1c levels at 5 mg per week dosing, compared to minus 0.86% with a placebo. At the highest dose of 15 mg per week, Mounjaro (tirzepatide) led to a minus 2.34% reduction in HbA1c. This was demonstrated over 40 weeks. A weight reduction of 5.4 kg was seen with 5 mg of Mounjaro (tirzepatide) dosing, and a 10.5 kg reduction was observed with 15 mg dosing. This dose-dependent correlation with weight loss is similar to another GLP-1 medication called semaglutide (Wegovy) injection used for weight loss management 8.
The results of the SURPASS trials demonstrate that tirzepatide yields clinically significant improvements in blood sugar control and weight loss when compared with other GLP-1 receptor agonists (semaglutide and dulaglutide), insulin degludec, and insulin glargine 4, 8. Consequently, the American Diabetes Association (ADA) categorizes tirzepatide as a highly effective therapy for achieving blood sugar control and weight loss 36, 37.
Comparatively, tirzepatide works similarly to GLP-1 medications (semaglutide and dulaglutide) but with greater efficacy. Given the weight loss properties and lack of liver toxicity, it is likely to have an indirect role in the treatment of nonalcoholic fatty liver disease 2. However, further research is needed before the use is approved for metabolic dysfunction-associated fatty liver disease 38.
Mounjaro for weight loss
Tirzepatide can also be used as an injection for weight loss to treat obesity. A brand name for tirzepatide used for weight management is Zepbound 39, 40. Zepbound (tirzepatide) is an FDA-approved medicine used for weight loss and weight management in adults to help you lose weight and keep weight off, and it is also used for obstructive sleep apnea (OSA) with obesity 39, 40.
Zepbound (tirzepatide) is FDA-approved for chronic weight management in adults with 39, 40:
- Obesity with a body mass index (BMI) of 30 kg/m² or greater)
- OR
- Overweight with a body mass index (BMI) of 27 kg/m² or greater and also have at least one weight-related comorbid condition such as high blood pressure (hypertension), high cholesterol (dyslipidemia), type 2 diabetes mellitus, obstructive sleep apnea (OSA), or cardiovascular disease.
Zepbound (tirzepatide) works by reducing your appetite and making you feel full more quickly and for a longer period of time, so you eat less and lose weight. Zepbound (tirzepatide) for weight loss and sleep apnea is given as a once-weekly injection under the skin and should be used together with diet and exercise.
When Zepbound was used for weight loss patients lost an average of 48 lbs, or 20.9% of their body weight, compared to 7.1 lb, or 3.1%, for a placebo over 72 weeks in a clinical study.
When Zepbound was used for obstructive sleep apnea 42% of adults had no sleep apnea or mild, non-symptomatic obstructive sleep apnea after 1 year of treatment, compared to 16% using placebo 41. Zepbound obstructive sleep apnea patients also had an average weight loss of 45 lbs (18% of their body weight).
Zepbound (tirzepatide) injection comes in: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, or 15 mg per 0.5 mL in single-dose pen.
The recommended starting dosage of Zepbound (tirzepatide) injection is 2.5 mg injected subcutaneously in the abdomen, thigh, or upper arm once weekly at any time of day, with or without meals.
- After 4 weeks, increase to 5 mg injected subcutaneously once weekly.
- Increase the dosage in 2.5 mg increments after at least 4 weeks on the current dose.
- The recommended maintenance dosages are 5 mg, 10 mg, or 15 mg injected subcutaneously once weekly.
- Consider treatment response and tolerability when selecting the maintenance dosage.
- The maximum Zepbound (tirzepatide) injection dosage is 15 mg subcutaneously once weekly.
- Rotate injection sites with each dose.
Mounjaro dosage
Mounjaro (tirzepatide) injection comes in clear, colorless to slightly yellow solution (liquid) available in pre-filled single-dose pens of the following strengths 10:
- 2.5 mg/0.5 mL
- 5 mg/0.5 mL
- 7.5 mg/0.5 mL
- 10 mg/0.5 mL
- 12.5 mg/0.5 mL
- 15 mg/0.5 mL
The recommended starting dosage of Mounjaro (tirzepatide) is 2.5 mg injected subcutaneously (into the fatty tissue layer just under the skin) in the abdomen, thigh, or upper arm once a week with or without meals at any time of day 10. The 2.5 mg dosage is for treatment initiation and is not intended for blood sugar control 10.
- After 4 weeks, increase the dosage to 5 mg injected subcutaneously once weekly.
- If additional blood sugar control is needed, increase the dosage in 2.5 mg increments after at least 4 weeks on the current dose.
- The maximum dosage of Mounjaro (tirzepatide) is 15 mg injected subcutaneously once weekly.
- If a dose is missed, instruct patients to administer Mounjaro (tirzepatide) as soon as possible within 4 days (96 hours) after the missed dose. If more than 4 days have passed, skip the missed dose and administer the next dose on the regularly scheduled day. In each case, patients can then resume their regular once weekly dosing schedule.
The day of weekly administration can be changed, if necessary, as long as the time between the 2 doses is at least 3 days (72 hours).
What should I do if I forget a dose?
Inject the missed dose as soon as you remember it within 4 days after the missed dose. However, if more than 4 days have passed, skip the missed dose and continue your regular dosing schedule. Do not inject two doses within 3 days of each other.
Liver impairment
According to the manufacturer’s product information, no dosage adjustment of Mounjaro (tirzepatide) is suggested for patients with liver impairment.
Kidney impairment
No dosage adjustment of Mounjaro (tirzepatide) is suggested for patients with kidney impairment. However, tirzepatide is associated with gastrointestinal adverse drug reactions, including nausea, vomiting, and diarrhea, leading to dehydration, which may cause acute kidney injury. Use with caution in patients prone to dehydration.
Pregnancy
Available information on tirzepatide use in pregnant women is inadequate to evaluate for a drug-related risk of congenital disabilities and adverse maternal or fetal outcomes. Animal reproduction studies have shown higher occurrences of external, visceral, and skeletal malformations when exposed to tirzepatide. Potential risks exist to the fetus if ingested during pregnancy. Hence, tirzepatide should only be prescribed to pregnant patients of childbearing age when the benefits outweigh the potential risks and after a thorough discussion of the teratogenic effects. Clinicians should also discuss the decreased efficacy of oral contraceptives and offer non-oral methods for at least 4 weeks after beginning tirzepatide.
The product label for tirzepatide states the use of this medication might change the way oral contraceptives (birth control pills used to prevent pregnancy) are absorbed by the body. This might increase the chance of pregnancy, even if the oral birth control is taken correctly and consistently. The product label suggests women using oral contraceptives switch to a non-oral birth control or add a barrier method of contraception (like condoms) for 4 weeks after starting the medication and for 4 weeks after each increase in dose. If you are taking this medication, talk with your doctor about non-oral birth control and all your options for preventing a pregnancy.
Breastfeeding
No information exists on tirzepatide in animal or human milk or its effects on the breastfed infant. Tirzepatide is a large molecule with high molecular weight. Accordingly, the milk concentration is likely less, and absorption is unlikely because it is presumably partially destroyed in the infant’s gastrointestinal tract 42, 43. Preliminary evidence indicates that tirzepatide is barely detectable in breastmilk with doses up to 5 mg 42, 43. If a mother requires tirzepatide, it is not a reason to discontinue breastfeeding. Until more data become available, tirzepatide should be used with caution during breastfeeding, especially while nursing a newborn or preterm infant 42, 43. Clinicians should consider the developmental and health benefits of breastfeeding, the mother’s need for tirzepatide, and the potential adverse impacts on the breastfed infant.
Children
Tirzepatide has not been established as safe and effective for children.
Elderly
For older patients, in a collective analysis of 7 clinical trials, 30.1% were aged 65 or older, with 4.1% aged 75 or older. While safety and efficacy were comparable to younger counterparts, acknowledging heightened sensitivity in older patients remains crucial.
How to Use Mounjaro
Mounjaro (tirzepatide) injection comes in clear, colorless to slightly yellow solution (liquid) available in pre-filled single-dose pens of the following strengths 10:
- 2.5 mg/0.5 mL
- 5 mg/0.5 mL
- 7.5 mg/0.5 mL
- 10 mg/0.5 mL
- 12.5 mg/0.5 mL
- 15 mg/0.5 mL
The recommended starting dosage of Mounjaro (tirzepatide) is 2.5 mg injected subcutaneously (into the fatty tissue layer just under the skin) in the abdomen, thigh, or upper arm once a week with or without meals at any time of day 10. The 2.5 mg dosage is for treatment initiation and is not intended for blood sugar control 10.
- Administer Mounjaro (tirzepatide) once weekly, any time of day, with or without meals.
- Inject Mounjaro (tirzepatide) subcutaneously in the abdomen, thigh, or upper arm.
- Rotate injection sites with each dose.
- Inspect Mounjaro (tirzepatide) visually before use. It should appear clear and colorless to slightly yellow. Do not use Mounjaro (tirzepatide) if particulate matter or discoloration is seen.
- When using Mounjaro (tirzepatide) with insulin, administer as separate injections and never mix. It is acceptable to inject Mounjaro (tirzepatide) and insulin in the same body region, but the injections should not be adjacent to each other.
Use Mounjaro (tirzepatide) exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Your doctor will probably start you on a low dose of Mounjaro (tirzepatide) and gradually increase your dose, not more than once every 4 weeks.
Mounjaro (tirzepatide) controls diabetes but does not cure it. It may take 4 weeks or longer before you feel the full benefit of Mounjaro (tirzepatide). Continue to take Mounjaro (tirzepatide) even if you feel well. Do not stop taking Mounjaro (tirzepatide) without talking to your doctor.
You will be shown how to use the injection pen or vial by your doctor or nurse. You will also be given instructions how to use Mounjaro (tirzepatide). This will tell you how to inject it. Read it carefully. Ask your pharmacist or doctor if you have any questions about how to inject Mounjaro (tirzepatide).
Mounjaro (tirzepatide) can be injected in the abdomen, thigh or upper arm. Rotate injection sites with each dose.
You may change the day of the week you inject Mounjaro (tirzepatide) as long as at least 3 days have passed between doses.
You may administer insulin in the same area as Mounjaro (tirzepatide) but they should not be given right next to each other. Also, you should not mix Mounjaro (tirzepatide) and insulin in the same injection.
Always look at the Mounjaro (tirzepatide) solution before you inject it. It should be clear, colorless to slightly yelow and free of particles. Do not use Mounjaro (tirzepatide) if it is colored (except slightly yellow), cloudy, frozen, or contains solid particles, or if the expiration date on the pen has passed.
Never reuse needles and never share needles or pens. Always remove the needle right after you inject your dose. Dispose of needles in a puncture-resistant container. Ask your doctor or pharmacist how to dispose of the puncture resistant container.
Mounjaro side effects
Mounjaro (tirzepatide) common side effects include nausea, vomiting, diarrhea, decreased appetite, constipation, indigestion, abdominal pain, heartburn, fatigue, injection site reactions, headache, and low blood sugar (in people with type 2 diabetes). Stomach or gastrointestinal side effects are common but tend to be mild and clear up in a few weeks in most people and will not interfere with long-term treatment. Stomach side effects can be more common with higher doses.
The most common gastrointestinal side effect is nausea, which occurs in 12% to 22% of people taking Mounjaro (tirzepatide) at therapeutic doses, according to clinical trials.
- Others include diarrhea (12% to 16%), vomiting (6% to 9%), decreased appetite (5% to 11%), constipation (6% to 7%), indigestion (4% to 7%), abdominal pain (4% to 6%), and injection site reactions (3.2%).
- These side effects occurred at rates higher than in placebo-treated groups (receiving an inactive treatment).
- These Mounjaro (Tirzepatide) side effects occurred in 4% or more of type 2 diabetes patients taking tirzepatide in pooled placebo-controlled clinical trials.
Some side effects can be serious. If you experience any of these symptoms or those listed in the IMPORTANT WARNING section, stop taking Mounjaro (tirzepatide) and see your doctor immediately:
- Stomach pain that will not go away and may radiate to your back with or without vomiting
- Swelling of your face, throat, or around your mouth or eyes; hives; rash; itching; trouble swallowing or breathing; dizziness; or a rapid heartbeat.
The side effect of hypoglycemia was generally low in Mounjaro (tirzepatide) single therapy trials but increased when used with insulin or sulfonylureas. Injection site reactions, including pain, redness, and swelling, were commonly reported but typically mild in severity.
Mounjaro (tirzepatide) may cause other side effects. See your doctor if you have any unusual problems while taking Mounjaro (tirzepatide).
Approximately 5-10% of patients discontinued Mounjaro (tirzepatide) due to side effects in clinical trials, with higher discontinuation rates (up to 25% in some studies) at the highest doses (15 mg), and lower rates (around 5%) at lower doses (5 mg). The discontinuation rate is dose-dependent, with gastrointestinal side effects being the primary reason for stopping the medication.
Timeline for common Mounjaro (tirzepatide) side effects:
- Week 1-2: Peak intensity of gastrointestinal symptoms
- Week 3-4: Gradual improvement begins
- Week 4-8: Most patients experience a significant reduction in side effects
- After 8 weeks: Side effects are typically minimal or resolved.
Mounjaro overdose
Patients who overdose on tirzepatide should be monitored for any changes in clinical status. As tirzepatide has a long half-life, , which is approximately 5 days, patients who overdose on tirzepatide may require prolonged monitoring 44. Clinicians should contact poison control; consultation with a toxicologist may be necessary. No current antidote for tirzepatide overdose exists, and supportive care is most beneficial 4.
Patients with acute pancreatitis present with abdominal pain, serum lipase >3 upper limit of normal, and evidence of acute pancreatitis on imaging. American Gastroenterological Association guidelines recommend goal-directed fluid management for patients with acute pancreatitis 45.
- Hoofnagle JH. Weight Loss Agents. [Updated 2025 Jul 1]. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548929[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Tirzepatide. [Updated 2025 Jun 27]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK581694[↩][↩][↩][↩]
- Tirzepatide injection. https://medlineplus.gov/druginfo/meds/a622044.html[↩]
- Farzam K, Patel P. Tirzepatide. [Updated 2024 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK585056[↩][↩][↩][↩]
- Drug Trials Snapshots: MOUNJARO. https://www.fda.gov/drugs/drug-approvals-and-databases/drug-trials-snapshots-mounjaro[↩][↩][↩][↩]
- Aronne LJ, Horn DB, le Roux CW, Ho W, Falcon BL, Gomez Valderas E, Das S, Lee CJ, Glass LC, Senyucel C, Dunn JP; SURMOUNT-5 Trial Investigators. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. N Engl J Med. 2025 Jul 3;393(1):26-36. https://www.nejm.org/doi/full/10.1056/NEJMoa2416394[↩]
- Jastreboff AM, le Roux CW, Stefanski A, Aronne LJ, Halpern B, Wharton S, Wilding JPH, Perreault L, Zhang S, Battula R, Bunck MC, Ahmad NN, Jouravskaya I; SURMOUNT-1 Investigators. Tirzepatide for Obesity Treatment and Diabetes Prevention. N Engl J Med. 2025 Mar 6;392(10):958-971. https://www.nejm.org/doi/full/10.1056/NEJMoa2410819[↩]
- Dahl D, Onishi Y, Norwood P, Huh R, Bray R, Patel H, Rodríguez Á. Effect of Subcutaneous Tirzepatide vs Placebo Added to Titrated Insulin Glargine on Glycemic Control in Patients With Type 2 Diabetes: The SURPASS-5 Randomized Clinical Trial. JAMA. 2022 Feb 8;327(6):534-545. doi: 10.1001/jama.2022.0078[↩][↩][↩]
- Coskun T, Sloop KW, Loghin C, Alsina-Fernandez J, Urva S, Bokvist KB, Cui X, Briere DA, Cabrera O, Roell WC, Kuchibhotla U, Moyers JS, Benson CT, Gimeno RE, D’Alessio DA, Haupt A. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Mol Metab. 2018 Dec;18:3-14. doi: 10.1016/j.molmet.2018.09.009[↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215866s000lbl.pdf[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- https://www.fda.gov/drugs/novel-drug-approvals-fda/new-drug-therapy-approvals-2022[↩]
- https://www.fda.gov/media/164429/download[↩]
- Lisco G, De Tullio A, Disoteo O, De Geronimo V, Piazzolla G, De Pergola G, Giagulli VA, Jirillo E, Guastamacchia E, Sabbà C, Triggiani V. Basal insulin intensification with GLP-1RA and dual GIP and GLP-1RA in patients with uncontrolled type 2 diabetes mellitus: A rapid review of randomized controlled trials and meta-analysis. Front Endocrinol (Lausanne). 2022 Sep 8;13:920541. doi: 10.3389/fendo.2022.920541[↩][↩][↩][↩][↩]
- Kroopnick JM, Davis SN. The role of Recent Pharmacotherapeutic Options on the Management of Treatment Resistant Type 2 Diabetes. Expert Opin Pharmacother. 2022 Aug;23(11):1259-1271. doi: 10.1080/14656566.2022.2089021[↩]
- Krauss Z, Hintz A, Fisk R. Tirzepatide: Clinical review of the “twincretin” injectable. Am J Health Syst Pharm. 2023 Jul 7;80(14):879-888. doi: 10.1093/ajhp/zxad080[↩]
- Dutta D, Surana V, Singla R, Aggarwal S, Sharma M. Efficacy and safety of novel twincretin tirzepatide a dual GIP and GLP-1 receptor agonist in the management of type-2 diabetes: A Cochrane meta-analysis. Indian J Endocrinol Metab. 2021 Nov-Dec;25(6):475-489. doi: 10.4103/ijem.ijem_423_21[↩]
- Seino Y, Fukushima M, Yabe D. GIP and GLP-1, the two incretin hormones: Similarities and differences. J Diabetes Investig (2010) 1(1-2):8–23. doi: 10.1111/j.2040-1124.2010.00022.x[↩]
- Nauck MA, Quast DR, Wefers J, Pfeiffer AFH. The evolving story of incretins (GIP and GLP-1) in metabolic and cardiovascular disease: A pathophysiological update. Diabetes Obes Metab (2021) 23 Suppl 3:5–29. doi: 10.1111/dom.14496[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Andersen DB, Holst JJ. Peptides in the regulation of glucagon secretion. Peptides (2022) 148:170683. doi: 10.1016/j.peptides.2021.170683[↩][↩][↩][↩][↩][↩][↩]
- Wolfe MM, Zhao KB, Glazier KD, Jarboe LA, Tseng CC. Regulation of glucose-dependent insulinotropic polypeptide release by protein in the rat. Am J Physiol Gastrointest Liver Physiol (2000) 279(3):G561–6. doi: 10.1152/ajpgi.2000.279.3.G561[↩]
- Dailey MJ, Moran TH. Glucagon-like peptide 1 and appetite. Trends Endocrinol Metab (2013) 24(2):85–91. doi: 10.1016/j.tem.2012.11.008[↩][↩][↩][↩]
- Tseng CC, Jarboe LA, Wolfe MM. Regulation of glucose-dependent insulinotropic peptide gene expression by a glucose meal. Am J Physiol (1994) 266(5 Pt 1):G887–91. doi: 10.1152/ajpgi.1994.266.5.G887[↩][↩][↩]
- Frías JP, Davies MJ, Rosenstock J, Pérez Manghi FC, Fernández Landó L, Bergman BK, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med (2021) 385(6):503–15. doi: 10.1056/NEJMoa2107519[↩]
- El K, Campbell JE. The role of GIP in α-cells and glucagon secretion. Peptides (2020) 125:170213. doi: 10.1016/j.peptides.2019.170213[↩]
- Zhang Y, Parajuli KR, Fava GE, Gupta R, Xu W, Nguyen LU, et al. GLP-1 receptor in pancreatic α-cells regulates glucagon secretion in a glucose-dependent bidirectional manner. Diabetes (2019. 2020) 6869(2):267–8. doi: 10.2337/db20-er02c[↩]
- Ahrén B. Incretin dysfunction in type 2 diabetes: clinical impact and future perspectives. Diabetes Metab (2013) 39(3):195–201. doi: 10.1016/j.diabet.2013.03.001[↩]
- Adriaenssens AE, Biggs EK, Darwish T, Tadross J, Sukthankar T, Girish M, et al. Glucose-dependent insulinotropic polypeptide receptor-expressing cells in the hypothalamus regulate food intake. Cell Metab (2019) 30(5):987–96.e6. doi: 10.1016/j.cmet.2019.07.013[↩][↩]
- Meier JJ, Goetze O, Anstipp J, Hagemann D, Holst JJ, Schmidt WE, et al. Gastric inhibitory polypeptide does not inhibit gastric emptying in humans. Am J Physiol Endocrinol Metab (2004) 286(4):E621–5. doi: 10.1152/ajpendo.00499.2003[↩]
- Nauck MA, Meier JJ. Incretin hormones: Their role in health and disease. Diabetes Obes Metab (2018) 20 Suppl 1:5–21. doi: 10.1111/dom.13129[↩]
- Coskun T, Sloop KW, Loghin C, Alsina-Fernandez J, Urva S, Bokvist KB, et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Mol Metab (2018) 18:3–14. doi: 10.1016/j.molmet.2018.09.009[↩][↩][↩][↩]
- Sun B, Willard FS, Feng D, Alsina-Fernandez J, et al. Structural determinants of dual incretin receptor agonism by tirzepatide. Proc Natl Acad Sci U S A. 2022 Mar 29;119(13):e2116506119. doi: 10.1073/pnas.2116506119[↩]
- Thomas MK, Nikooienejad A, Bray R, Cui X, Wilson J, Duffin K, Milicevic Z, Haupt A, Robins DA. Dual GIP and GLP-1 Receptor Agonist Tirzepatide Improves Beta-cell Function and Insulin Sensitivity in Type 2 Diabetes. J Clin Endocrinol Metab. 2021 Jan 23;106(2):388-396. doi: 10.1210/clinem/dgaa863[↩]
- Bucheit J, Ayers J, Pamulapati L, Browning A, Sisson E. A Novel Dual Incretin Agent, Tirzepatide (LY3298176), for the Treatment of Type 2 Diabetes Mellitus and Cardiometabolic Health. J Cardiovasc Pharmacol. 2022 Aug 1;80(2):171-179. doi: 10.1097/FJC.0000000000001299[↩]
- Tirzepatide (Mounjaro) for type 2 diabetes. Med Lett Drugs Ther. 2022 Jul 11;64(1654):105-107. https://secure.medicalletter.org/TML-article-1654a[↩]
- Collins L, Costello RA. Glucagon-Like Peptide-1 Receptor Agonists. [Updated 2024 Feb 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551568[↩]
- Gao L, Lee BW, Chawla M, Kim J, Huo L, Du L, Huang Y, Ji L. Tirzepatide versus insulin glargine as second-line or third-line therapy in type 2 diabetes in the Asia-Pacific region: the SURPASS-AP-Combo trial. Nat Med. 2023 Jun;29(6):1500-1510. doi: 10.1038/s41591-023-02344-1[↩]
- Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, Rosas SE, Del Prato S, Mathieu C, Mingrone G, Rossing P, Tankova T, Tsapas A, Buse JB. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022 Nov 1;45(11):2753-2786. doi: 10.2337/dci22-0034[↩]
- Valenzuela-Vallejo L, Guatibonza-García V, Mantzoros CS. Recent guidelines for Non-Alcoholic Fatty Liver disease (NAFLD)/ Fatty Liver Disease (FLD): Are they already outdated and in need of supplementation? Metabolism. 2022 Nov;136:155248. doi: 10.1016/j.metabol.2022.155248[↩]
- FDA Approves New Medication for Chronic Weight Management. https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management[↩][↩][↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217806s000lbl.pdf[↩][↩][↩]
- Malhotra A, Bednarik J, Chakladar S, Dunn JP, Weaver T, Grunstein R, Fietze I, Redline S, Azarbarzin A, Sands SA, Schwab RJ, Bunck MC. Tirzepatide for the treatment of obstructive sleep apnea: Rationale, design, and sample baseline characteristics of the SURMOUNT -OSA phase 3 trial. Contemp Clin Trials. 2024 Jun;141:107516. doi: 10.1016/j.cct.2024.107516[↩]
- Drugs and Lactation Database (LactMed®) [Internet]. Bethesda (MD): National Institute of Child Health and Human Development; 2006-. Tirzepatide. [Updated 2025 Sep 15]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK581488[↩][↩][↩]
- Tirzepatide (Mounjaro®, Zepbound®). https://mothertobaby.org/fact-sheets/tirzepatide[↩][↩][↩]
- Min T, Bain SC. The Role of Tirzepatide, Dual GIP and GLP-1 Receptor Agonist, in the Management of Type 2 Diabetes: The SURPASS Clinical Trials. Diabetes Ther. 2021 Jan;12(1):143-157. doi: 10.1007/s13300-020-00981-0[↩]
- Crockett SD, Wani S, Gardner TB, Falck-Ytter Y, Barkun AN; American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology. 2018 Mar;154(4):1096-1101. doi: 10.1053/j.gastro.2018.01.032[↩]





{kind=link}