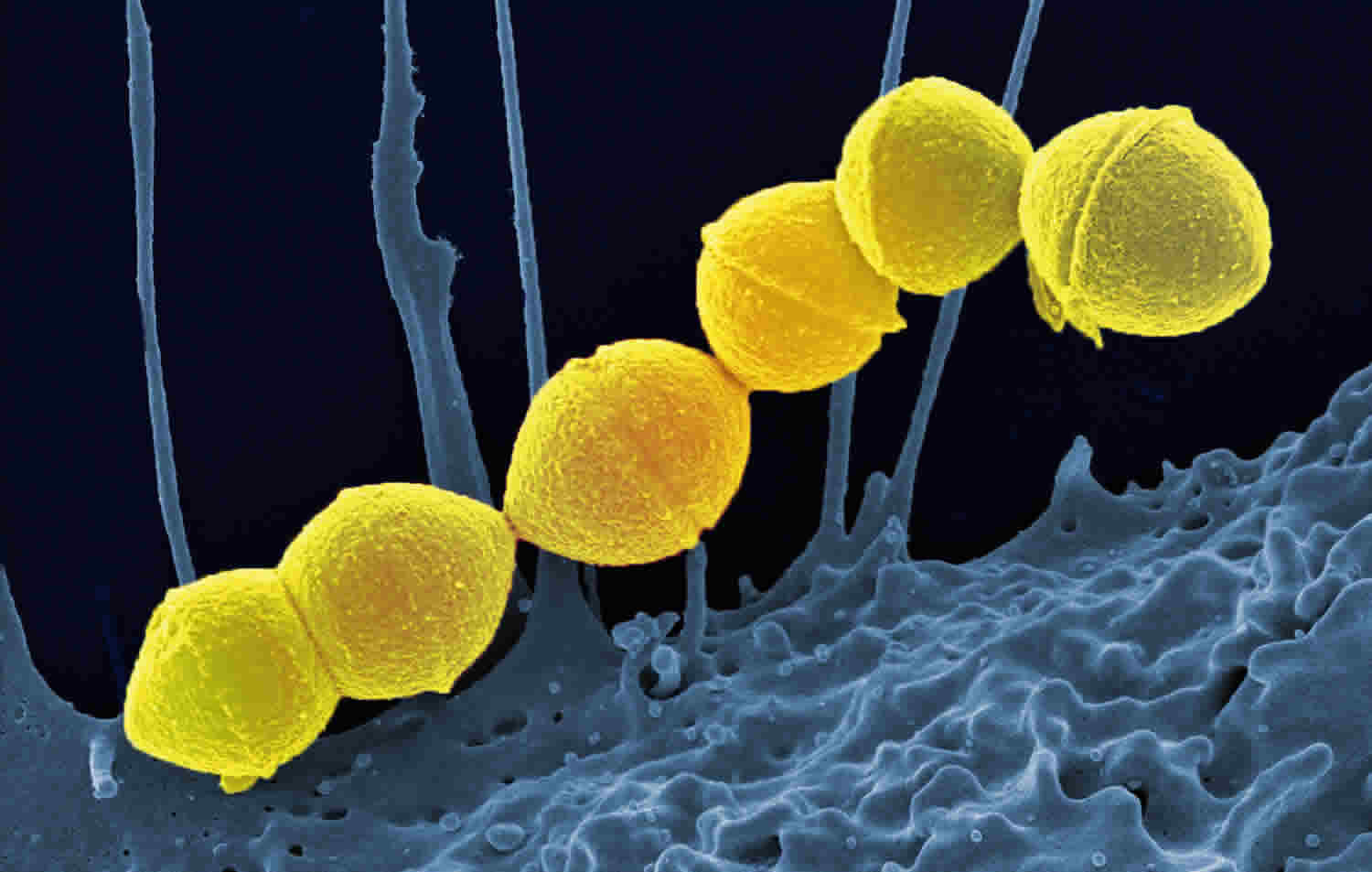
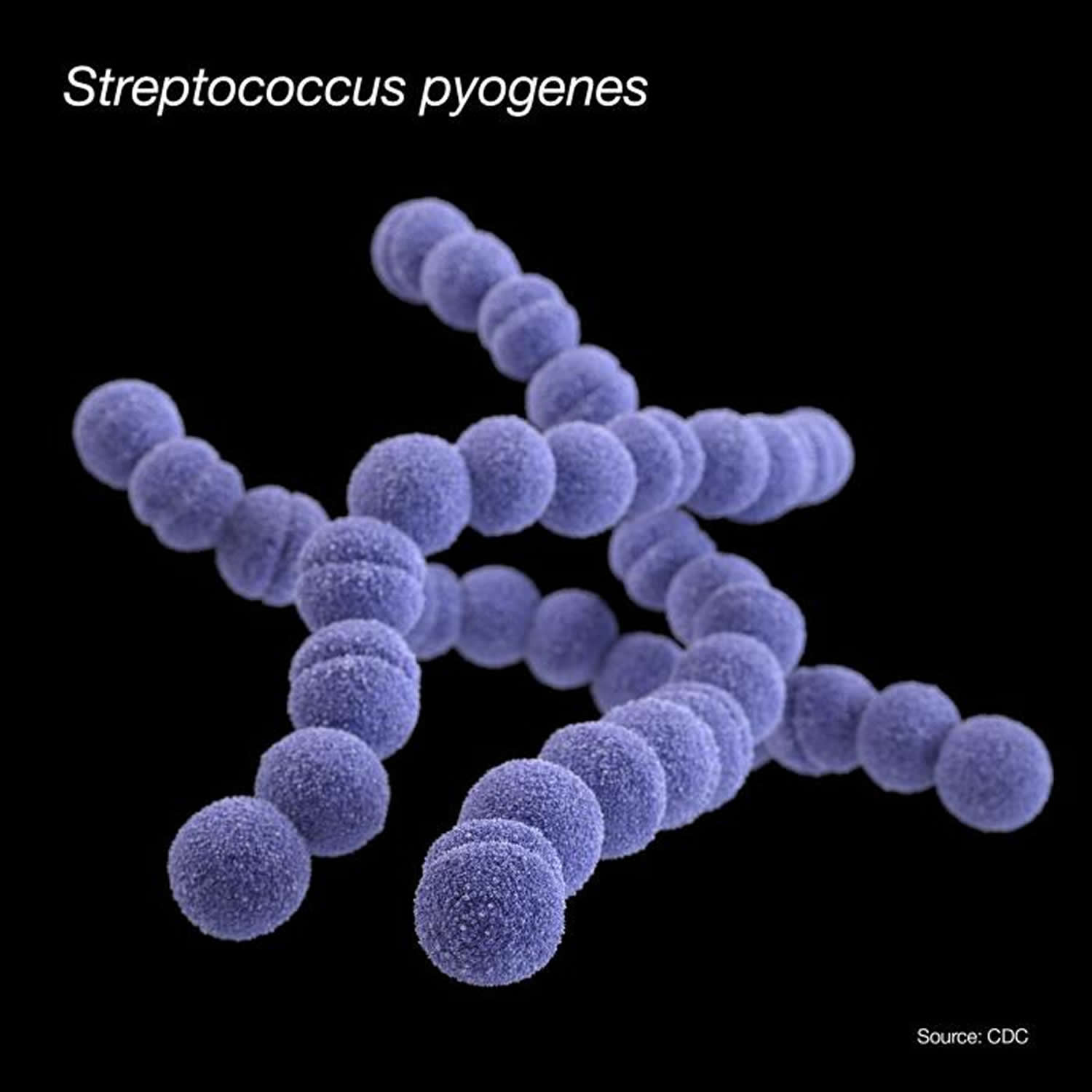
Streptococcus pyogenes
Streptococcus pyogenes also called group A Streptococcus (GAS) or Group A beta hemolytic streptococcus (GABHS) is a species of Gram-positive beta-hemolytic aerobic bacteria in the genus Streptococcus belonging to Lancefield group A antigen that causes a wide variety of diseases in humans ranging from mild localized infections to life-threatening invasive infections 1, 2, 3, 4, 5.
Streptococcus pyogenes are Gram-positive cocci that grow in chains. Streptococcus pyogenes exhibit beta-hemolysis (complete hemolysis) when grown on blood agar plates. Streptococcus pyogenes belong to group A in the Lancefield classification system for beta-hemolytic Streptococcus and thus are called group A streptococci.
Streptococcus pyogenes cause a wide range of illnesses collectively called group A strep infections. Some group A strep infections, like strep throat (pharyngitis) and skin infection (impetigo), are less serious. However, they are very common in children and can sometimes lead to serious complications. Invasive (severe) disease, like necrotizing fasciitis, is less common but can be deadly.
Invasive group A streptococcal infections may manifest as any of several clinical syndromes, including pneumonia, bacteremia (bacteria in the bloodstream) in association with skin infection (e.g., cellulitis, erysipelas, or infection of a surgical or nonsurgical wound), deep soft-tissue infection (e.g., myositis or necrotizing fasciitis), endocarditis, meningitis, peritonitis, osteomyelitis, septic arthritis, postpartum sepsis (i.e., puerperal fever), neonatal sepsis, and nonfocal bacteremia.
Streptococcus pyogenes symptoms vary with the organ infected but commonly include fever, sore throat, swollen neck glands, and fatigue. Other signs can include a red and sandpaper-like rash, a “strawberry tongue” or symptoms of a skin infection like cellulitis or impetigo. More severe symptoms can include headache, nausea, vomiting, and severe muscle aches.
- Strep Throat:
- Sudden sore throat, especially with pain when swallowing
- Fever
- White or yellow spots on the tonsils or throat
- Swollen, tender lymph nodes in the neck
- Fatigue
- Loss of appetite
- Scarlet Fever (a complication of strep throat):
- A fine, red rash that feels like sandpaper and starts on the chest and abdomen
- Flushed face with paleness around the mouth
- A red, bumpy “strawberry tongue”
- Skin peeling on fingers and toes after the rash fades
- Invasive Group A Strep (iGAS):
- Fever
- Severe muscle aches
- Nausea and vomiting
- Shortness of breath
- Severe headache
- Cellulitis: Redness, swelling, and warmth at the site of a skin wound
- Impetigo: Itchy, reddish rash that can form fluid-filled blisters which break and form a crusty, honey-colored scab often appears around the mouth and nose
Complication of group A beta-hemolytic streptococci infections may include acute rheumatic fever and post streptococcal glomerulonephritis.
Streptococcus pyogenes diagnosis typically involves a rapid antigen test on a throat swab, which provides a quick result 6, 7. A positive result is definitive, but a negative result in children and adolescents should be confirmed with a throat culture, which is the “gold standard” for diagnosis 6, 7. Other methods include blood cultures for invasive infections or serologic tests to diagnose past infections like rheumatic fever.
Streptococcus pyogenes diagnostic methods
- Rapid antigen detection test (RADT): A swab from the throat is used to quickly detect Streptococcus pyogenes antigens. A positive result is immediate and accurate. The rapid antigen detection test (RADT) has a sensitivity of approximately 85% in children, although variability exists, while its specificity is stable at 95% 8. Due to the high specificity of the rapid antigen detection test (RADT) in children, antibiotic therapy is recommended without the need for further throat culture to distinguish infection from carriage. If the rapid antigen detection test (RADT) result is negative, treatment decisions depend on national guidelines 8. In the United States, however, in adults, due to the low general rate of Streptococcus pyogenes pharyngitis and corresponding low pretest probability, a negative RADT does not require confirmatory culture. A negative rapid swab result confers an extremely low post-test probability of group A beta-hemolytic streptococci infection 9, 10. For other sites of infection, whether superficial or deep (such as skin, blood, wound, or lung), performing a Gram stain and cultures are the appropriate diagnostic methods. Polymerase chain reaction (PCR) can also be used to identify specific group A beta-hemolytic streptococci strains, particularly in complicated cases 11.
- Throat culture: Throat culture (i.e., a swab rubbed on both tonsillar pillars, avoiding the lips and tongue) is the “gold standard” for confirming a strep infection. A throat swab is sent to a lab and cultured on a blood agar plate, which facilitates the easy identification of beta-hemolytic colonies. Group A Streptococcus (GAS) grows easily on sheep blood agar and is catalase- and oxidase-negative. Confirmatory identification is achieved through Lancefield grouping and, more recently, techniques such as matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) 12, 13. However, culture results typically take 24 hours or longer, which delays critical information needed for treatment, isolation, and epidemiological purposes.
- Molecular tests: Nucleic acid amplification tests (NAATs) or other molecular methods can be used to detect Streptococcus pyogenes from various specimens, including throat swabs, blood, or other body fluids.
- Serologic tests: These are used for retrospective diagnosis of post-streptococcal diseases, such as acute rheumatic fever or glomerulonephritis, by detecting antibodies to streptococcal antigens. These are not useful for diagnosing an acute infection.
- Other specimens: For invasive infections, samples from sterile sites like blood, cerebrospinal fluid, or joint fluid can be tested via culture or molecular methods. For skin infections, an aspirate from the edge of the lesion may be used.
- Bacitracin susceptibility: Streptococcus pyogenes can be differentiated from other non-group A beta-hemolytic streptococci by their increased sensitivity to bacitracin. The bacitracin test, along with the Lancefield antigen A test, is used for greater specificity in the identification of Streptococcus pyogenes, since other beta-hemolytic strains of streptococci may contain the group A antigen are resistant to bacitracin. The bacitracin test is also used to distinguish Streptococcus pyogenes from other beta-hemolytic streptococci that are PYR-positive, such as S. iniae and S. porcinus. To perform a bacitracin susceptibility test, it is important to make a subculture of the strain to be tested on a sheep blood agar plate (SBA), since placing the bacitracin disc on a primary plate could give variable results. The strain being tested is streaked with several individual colonies of a pure culture on an SBA agar plate and a disk containing 0.04 U of bacitracin is placed on the SBA plate. After overnight incubation at 35°C in 5% CO2, a zone of inhibition surrounding the disc indicates the susceptibility of the strain. It is noteworthy that bacitracin-resistant strains of S. pyogenes have been observed in a number of European countries; however, bacitracin resistance has not yet been reported in the US to date 14, 15, 16.
Treatment for Streptococcus pyogenes involves antibiotics, with the specific medication and duration depending on the infection’s location and severity. Common options include oral penicillin or amoxicillin for less severe infections like strep throat, while intravenous (IV) antibiotics like vancomycin or clindamycin are used for severe or invasive infections. Penicillin continues to be the gold standard for group A beta-hemolytic streptococci treatment 17. For patients with penicillin allergies, macrolides (e.g, erythromycin) and lincosamides (e.g, clindamycin) are notable alternatives 18. However, resistance to these antibiotics has increased in the past decade, with variable prevalence of resistant group A beta-hemolytic streptococci strains worldwide 19. While reports of antibiotic resistance to penicillins and increased minimal inhibitory concentrations (MICs) to penicillin and cephalosporins have emerged primarily due to mutations in the peptidoglycan synthetic enzyme pbp2x gene, resistance rates remain low 20.
A full course of antibiotics must be completed to prevent complications and reduce the spread of bacteria, even if you start feeling better. You should see your doctor if your symptoms don’t improve after 48 hours of antibiotic treatment.
Infection control:
- You should stay home from school, work, or daycare for at least 24 hours after starting antibiotic treatment to prevent the spread of infection.
Prophylactic antibiotics:
- Doctors may recommend a course of antibiotics for close contacts of individuals with invasive group A streptococcal infections to reduce their risk of becoming ill.
Streptococcus pyogenes treatment based on infection type
- Streptococcal pharyngitis (strep throat): Oral antibiotics such as penicillin or amoxicillin are commonly prescribed for 10 days.
- Streptococcus pyogenes skin infections (e.g., impetigo, cellulitis): A semi-synthetic penicillinase-resistant penicillin is often used. For patients with severe skin infections, intravenous antibiotics may be required initially, followed by oral medication, and in some cases, surgical debridement of necrotic tissue.
- Invasive group A streptococcal disease (iGAS): These severe infections require urgent treatment, often in a hospital, with intravenous antibiotics such as vancomycin or clindamycin. Other supportive therapies and intensive care may also be needed.
Figure 1. Streptococcus pyogenes
How Streptococcus pyogenes bacteria spread
Streptococcus pyogenes or group A Streptococcus (group A strep bacteria) are very contagious. Some people infected with group A strep bacteria don’t have symptoms or seem sick. They can still spread the bacteria to others. Generally, people spread Streptococcus pyogenes bacteria to others through respiratory droplets or direct contact. Rarely group A strep bacteria can spread through food that isn’t handled properly.
Respiratory droplets
Group A strep bacteria often live in the nose and throat. People who are infected spread the bacteria by talking, coughing, or sneezing. This creates respiratory droplets that contain the bacteria.
People can get sick if they:
- Breathe in respiratory droplets that contain Streptococcus pyogenes bacteria
- Touch their mouth or nose after touching something with those droplets on it
- Use the same plate, utensils, or glass as someone infected with Streptococcus pyogenes bacteria. Once washed, plates, utensils, and glasses are safe for others to use.
Direct contact
People can also spread group A strep bacteria from infected sores on their skin. Other people can get sick if they touch those sores or come into contact with fluid from the sores. Once the sores heal, Streptococcus pyogenes bacteria aren’t usually able to spread to other people.
Streptococcus pyogenes causes
Streptococcus pyogenes or group A Streptococcus (group A strep bacteria) can cause a wide range of infections, including pharyngitis (strep throat), scarlet fever, and skin infections like impetigo, cellulitis, and erysipelas. More serious conditions can result, such as necrotizing fasciitis, toxic shock syndrome, and post-infective complications like rheumatic fever and glomerulonephritis. These infections are contagious and spread through respiratory droplets, direct contact, or contaminated surfaces.
Common infections
- Pharyngitis (strep throat): A sore throat with symptoms like difficulty swallowing, headache, and swollen tonsils.
- Scarlet fever: A red rash that often accompanies strep throat.
- Skin infections:
- Impetigo: An itchy, oozing sore that forms a yellow crust.
- Cellulitis: A deeper skin infection causing red, hot, swollen, and painful skin, often on the face or legs.
- Erysipelas: A more superficial skin infection with a raised, sharply defined red border.
Severe and invasive infections
- Necrotizing fasciitis: A severe “flesh-eating disease” where bacteria destroy skin and other tissues, which can be fatal if not contained quickly.
- Streptococcal toxic shock syndrome (STSS): A serious condition caused by toxins that leads to low blood pressure, organ failure, difficulty breathing, and other severe symptoms.
- Pneumonia: An infection of the lungs.
- Meningitis: An infection of the membranes surrounding the brain and spinal cord.
- Septicemia (blood infection): The bacteria spread to the bloodstream, which can be life-threatening.
Post-infective complications
- Acute rheumatic fever: An inflammatory disease that can affect the heart, joints, and brain, often after strep throat.
- Rheumatic heart disease: Permanent damage to the heart’s valves from acute rheumatic fever.
- Acute glomerulonephritis: A kidney disorder that can occur after a Streptococcus infection.
Streptococcus pyogenes disease
Streptococcus pyogenes or group A Streptococcus (group A strep bacteria) can cause many different types of infections that range from minor to serious. Streptococcus pyogenes bacteria can also cause inflammatory diseases. The following are some, but not all, of the conditions associated with Streptococcus pyogenes bacteria.
Minor infections
The following infections caused by group A strep bacteria are generally mild:
Impetigo
Impetigo, also known as school sores, is a common, highly contagious bacterial skin infection caused by Staphylococcus aureus (common) or Streptococcus pyogenes bacteria (group A beta hemolytic streptococci [GABHS]). Impetigo appears as red sores, often around the nose and mouth, that quickly develop into fluid-filled blisters that may ooze, burst, and form a characteristic yellowish or “honey-colored” crust. The infection can be treated with prescription antibiotic ointments like mupirocin or oral antibiotics, which can clear it up faster than it would on its own and help prevent its spread. It is important to complete the entire course of medication.
Impetigo affects the superficial layers of the epidermis. Impetigo can be classified into non-bullous also known as ‘school sores’ caused by either Staphylococcus aureus, Streptococcus pyogenes, or both bacteria conjointly and bullous impetigo caused by Staphylococcus aureus which produces exfoliative toxins (exfoliatins A and B). Ecthyma is a deep form of impetigo causing deeper erosions of the skin into the dermis.
Impetigo is most common in young children but can occur at any age. It is usually transmitted through direct contact.
Impetigo risk factors include:
- Skin conditions: atopic dermatitis, contact dermatitis, scabies, chickenpox
- Skin trauma: lacerations, insect bites, thermal burns, abrasions
- Immunosuppression
- Warm, humid climate
- Poor hygiene
- Crowded environments.
Non-bullous impetigo symptoms most commonly found on the face or extremities but skin on any part of the body can be involved:
- Initial sores: Red sores that are often clustered around the nose and mouth. On darker skin tones, these may appear purple, brown, or gray.
- Blisters: The sores quickly form blisters that may be filled with pus.
- Crusts: Blisters can ooze and burst, leaving behind a thick, yellowish, or “honey-colored” crust.
- Other locations: The sores can also appear on the trunk, arms, legs, and diaper area.
- “Kissing lesions” arise where two skin surfaces are in contact.
- Itching: The sores may be mildly irritating. Avoid scratching the sores. Wash bedding, towels, and clothing that come into contact with the sores.
Patients are typically otherwise well; they may experience some itching and enlarged or swollen lymph nodes (lymphadenopathy).
Impetigo complications may include:
- Wider spread infection: cellulitis, lymphangitis, and bacteraemia.
- Staphylococcal scalded skin syndrome.
- Scarlet fever.
- Post-streptococcal glomerulonephritis (PSGN): a rare, acute renal condition following infection with Streptococcus pyogenes (group A streptococcus). This is due to a type III hypersensitivity reaction and presents 2–6 weeks post-skin infection.
- Streptococcal toxic shock syndrome (STSS): a rare complication causing diffuse erythematous rash, hypotension, and pyrexia.
- Postinflammatory pigmentation.
- Scarring, particularly with ecthyma.
Impetigo is usually a clinical diagnosis based on the features described above. A skin swab for culture and sensitivity may be beneficial if the impetigo is recurrent, widespread or there is concern of MRSA (methicillin-resistant Staphylococcus aureus) infection. Nasal swabs should be carried out in recurrent infection as they can identify staphylococcal nasal carriage which requires specific management. Rarely a biopsy may be indicated if the diagnosis is unclear in particular for bullous impetigo or if it is refractory to treatment.
Impetigo is treated with topical antibiotics. Topical antibiotics such as fusidic acid (first-line) or mupirocin (often reserved for possible MRSA infection) are effective in treating non-bullous impetigo, however, their use may not be recommended in some countries due to bacterial resistance. For localized non-bullous impetigo, application of antiseptic 2–3 times per day for 5–7 days is recommended (e.g. hydrogen peroxide 1% cream or povidone — iodine 10% ointment). Topical antibiotics can be considered when antiseptic treatment has not worked or is not appropriate (e.g. impetigo around the eyes).
Scarlet fever
Scarlet fever also known as scarlatina is a bacterial infection caused by Streptococcus pyogenes (group A streptococcus bacteria) that develops in some people who have strep throat, fever, and a characteristic bright red, sandpaper-like rash (tiny pinkish-red spots) that covers most of your body. The rash typically starts on your neck and chest before spreading to the rest of your body, often leaving red lines in skin folds. Scarlet fever almost always includes a sore throat and a high fever. Additional symptoms of scarlet fever include a flushed face with a pale ring around the mouth, and a “strawberry tongue” with a white coating at first. Scarlet fever is treated with antibiotics, such as penicillin, for a 10-day course.
Scarlet fever is most common in children 5 to 15 years of age. Scarlet fever most often occurs after a strep throat infection. Although scarlet fever was once considered a serious childhood illness, antibiotic treatments have made it less threatening. Still, if left untreated, scarlet fever can result in more-serious conditions that affect the heart, kidneys and other parts of the body.
Scarlet fever affects people who have recently had a sore throat (strep throat) or school sores (impetigo) caused by the group A streptococcus bacteria. A toxin released by the streptococcal bacteria causes the rash of scarlet fever. The infection spreads from person to person by droplets released when an infected person coughs or sneezes. Scarlet fever germs spread more easily among people in close contact, such as family members, child-care groups or classmates. The incubation period (the time between exposure and illness) is usually 2 to 4 days.
The signs and symptoms that give scarlet fever its name include:
- Red rash. The rash looks like a sunburn and feels like sandpaper. It typically begins on the face or neck and spreads to the trunk, arms and legs. Pushing on the reddened skin makes it turn pale.
- Red lines. The folds of skin around the groin, armpits, elbows, knees and neck usually become a deeper red than the other areas with the rash.
- Flushed face. The face may appear flushed with a pale ring around the mouth.
- Strawberry tongue. The tongue generally looks red and bumpy, and it’s often covered with a white coating early in the disease.
Signs and symptoms of scarlet fever also include:
- Fever of 100.4 F (38 °C) or higher, often with chills
- Very sore and red throat, sometimes with white or yellowish patches
- Difficulty swallowing
- Enlarged glands in the neck (lymph nodes) that are tender to the touch
- Nausea or vomiting
- Belly (abdominal) pain
- Headache and body aches
The rash and the redness in the face and tongue usually last about a week. After these signs and symptoms have gone away, the skin affected by the rash often peels.
If scarlet fever goes untreated, the group A streptococcus bacteria may spread to the:
- Tonsils
- Skin
- Blood
- Middle ear
- Sinuses
- Lungs
- Heart
- Kidneys
- Joints
- Muscles
Rarely, scarlet fever can lead to rheumatic fever, a serious inflammatory disease that can affect the heart, joints, nervous system and skin.
A possible relationship has been suggested between Strep infection and a rare condition called pediatric autoimmune neuropsychiatric disorder associated with group A streptococci (PANDAS). Children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococci (PANDAS) experience worsened symptoms of neuropsychiatric conditions, such as obsessive-compulsive disorder or tic disorders, with strep. This relationship currently remains unproved and controversial.
Diagnosis of scarlet fever is often suspected from the characteristic history and physical examination. Diagnosis is supported by throat swab taken from the posterior pharynx or tonsils. The following methods may be used (check local guidelines):
- Bacterial culture (gold standard)
- Rapid molecular tests (e.g, nucleic acid amplification test; NAAT)
- Rapid antigen detection tests (RADTs).
Blood tests for anti-deoxyribonuclease B (anti-DNase B) and antistreptolysin-O (ASO) titers may also be helpful.
A rapid strep test can identify the bacteria quickly, usually during your child’s appointment. If the rapid test is negative, but your doctor still thinks strep bacteria is the cause of your child’s illness, a strep throat culture can be done. It can take longer to get the results of this test.
Tests for the strep bacteria are important because a number of conditions can cause the signs and symptoms of scarlet fever, and these illnesses may require different treatments. If there are no strep bacteria, then some other factor is causing the illness.
Once a streptococcal infection is confirmed, a course of antibiotics is prescribed, usually penicillin, for up to 10 days. A 10-day course of oral antibiotics is typically recommended. Recommended antibiotic regimens include penicillin V or amoxicillin for 10 days, which is administered by mouth 21. An alternative treatment for group A streptococcal pharyngitis is a single intramuscular dose of penicillin G benzathine, particularly for patients who may not complete the full course of oral antibiotics 21, 9. Macrolides or clindamycin can be used for patients allergic to penicillin, although local resistance patterns should be considered 21.
It is very important that the full antibiotic course is taken to ensure all the infection is cleared, to reduce the risk of complications. If your child doesn’t follow the antibiotic treatment guidelines, the antibiotic treatment may not completely eliminate the infection, which can increase your child’s risk of developing complications.
In some situations a single dose of penicillin may be given by intramuscular injection. Patients allergic to penicillin may be treated with an alternative antibiotic, such as erythromycin.
Additional treatments include:
- Ibuprofen (Advil, Children’s Motrin, others) or acetaminophen (paracetamol) when necessary for fever, headache or throat pain. Check with your child’s doctor about the right dosage.
- Eating soft foods and drinking plenty of cool liquids, particularly if the throat is very painful.
- Oral antihistamines and emollients to relieve the itch of rash.
- Keep fingernails short on young children to prevent them from damaging the skin.
The fever usually improves within 12-24 hours after starting antibiotics and most patients recover after 4-5 days with clearing of skin symptoms over several weeks.
Your child can return to school after having taken antibiotics for at least 12 hours and no longer having a fever.
The prognosis for scarlet fever today is excellent, a significant improvement from the early 20th century 22. This progress is primarily attributed to the introduction of antibiotics and advances in rapid diagnosis. Once treatment begins, patients can usually resume regular activities 24 hours after their fever resolves. However, if left untreated, the condition may worsen, increasing the risk of complications related to group A streptococcal infection.
For most patients who receive prompt treatment, the prognosis is excellent. Recovery typically occurs within 3 to 6 days, although skin symptoms may persist for 14 to 21 days. In some cases, the infection can recur. With the advent of antibiotics, the mortality rate for scarlet fever is now less than 1%. Morbidity is primarily associated with complications such as glomerulonephritis, rheumatic fever, sinusitis, and other infections, although these complications are rare 23, 24
Strep throat
Strep throat is a bacterial infection of your throat caused by Streptococcus pyogenes or group A Streptococcus bacteria, which leads to a sore throat, fever, painful swallowing, and swollen neck glands. Strep throat is an infection in your throat and tonsils (the lymph nodes in the back of your mouth). With strep throat, your tonsils become very inflamed. This inflammation typically affects the surrounding area of your throat as well, which causes a sore throat (pharyngitis).
If untreated, strep throat can cause complications, such as kidney inflammation or rheumatic fever. Strep throat rarely causes more serious illnesses such as rheumatic fever, a disease that can lead to painful and inflamed joints, a specific type of rash, or cause permanent damage to your heart and heart valves. Therefore, it’s important to see a doctor for a prompt diagnosis and treatment. With proper treatment, your strep throat should resolve within seven to 10 days. If you or your child has signs or symptoms of strep throat, see your doctor for prompt testing and treatment. Treatment typically involves antibiotics prescribed by a doctor, and symptoms can be relieved by rest, staying hydrated, and gargling with warm salt water.
Strep throat is most common in school-aged children between the ages of 5 and 15, but it affects people of all ages including your siblings, parents, teachers and other caregivers that have direct contact with a school-aged child.
Streptococcal bacteria are contagious. Streptococcal bacteria can spread through droplets when someone with the infection coughs or sneezes, or through shared food or drinks. You can also pick up Streptococcal bacteria from a doorknob or other surface and transfer them to your nose, mouth or eyes.
Several factors can increase your risk of strep throat infection:
- Young age. Strep throat occurs most commonly in children.
- Time of year. Although strep throat can occur anytime, it tends to circulate in winter and early spring. Strep bacteria flourish wherever groups of people are in close contact.
Strep throat usually causes throat pain and difficulty swallowing. Signs and symptoms of strep throat can include:
- Throat pain that usually comes on quickly
- Painful swallowing
- Red and swollen tonsils, sometimes with white patches or streaks of pus
- Tiny red spots on the area at the back of the roof of the mouth (soft or hard palate) called petechiae
- Swollen, tender lymph nodes in your neck
- Fever
- Headache
- Rash
- Nausea or vomiting, especially in younger children
- Body aches
If you have strep throat, your throat and tonsils may appear red, sore and swollen. You may also have white patches, spots or streaks of pus on your throat and tonsils. In addition, you may develop tiny, red spots on the roof of your mouth called petechiae.
It’s possible for you or your child to have many of these signs and symptoms but not have strep throat. The cause of these signs and symptoms could be a viral infection or some other illness. That’s why your doctor generally tests specifically for strep throat.
It’s also possible for you to be exposed to a person who carries strep but shows no symptoms.
Strep throat can lead to serious complications.
Strep bacteria may spread, causing infection in:
- Tonsils
- Sinuses
- Skin
- Blood
- Middle ear
Strep infection may lead to inflammatory illnesses, including:
- Scarlet fever, a streptococcal infection characterized by a prominent rash
- Inflammation of the kidney (post-streptococcal glomerulonephritis)
- Rheumatic fever, a serious inflammatory condition that can affect the heart, joints, nervous system and skin
- Poststreptococcal reactive arthritis, a condition that causes inflammation of the joints
- Abscesses: Pockets of pus (abscesses) can form around your tonsils.
- Guttate psoriasis: A skin condition that causes small, red and scaly teardrop-shaped spots to develop on your arms, legs and torso.
- Invasive streptococcal infection: An infection that can occur when bacteria enter your tissue. It can be life-threatening, with conditions occurring such as streptococcal toxic shock syndrome, necrotizing fasciitis and other severe infections. This can ultimately lead to rapid decline and death.
A possible relationship has been suggested between strep infection and a rare condition called pediatric autoimmune neuropsychiatric disorder associated with group A streptococci (PANDAS). Children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococci (PANDAS) experience worsened symptoms of neuropsychiatric conditions, such as obsessive-compulsive disorder or tic disorders, with strep. This relationship currently remains unproved and controversial.
If you think you may have strep throat, you should see a doctor. Your doctor will conduct a physical exam, look for signs and symptoms of strep throat, and probably order one or more of the following tests:
- Rapid antigen test. Your doctor may perform a rapid antigen test on a swab sample from your throat. This test can detect strep bacteria in minutes by looking for substances (antigens) in the throat. If the test is negative but your doctor still suspects strep, he or she might do a throat culture.
- A rapid strep test takes about 20 minutes. If the test is positive (the swab contained Streptococcus bacteria), you have strep throat. If the test is negative (no signs of Streptococcus on the swab), you may not have strep throat. However, your doctor may send the throat swab to a laboratory to double-check the results with a throat culture.
- Molecular (polymerase chain reaction or PCR) test. This test is also done using a swab sample from your throat.
- Throat culture. A sterile swab is rubbed over the back of the throat and tonsils to get a sample of the secretions. It’s not painful, but it may cause gagging. The sample is then cultured in a laboratory for the presence of bacteria, but results can take as long as two days. It takes one to two days to see if Streptococcus bacteria grow from it. Throat cultures can sometimes find bacteria that rapid strep tests miss.
Strep throat treatment includes antibiotics. If your doctor diagnoses you or your child with strep throat, your doctor will likely prescribe an oral antibiotic. Penicillin and amoxicillin are common antibiotics doctors use to treat strep throat. If you’re allergic to penicillin, your doctor can prescribe another antibiotic. If taken within 48 hours of the onset of the illness, antibiotics reduce the duration and severity of symptoms, as well as the risk of complications and the likelihood that infection will spread to others. See your doctor if there’s no improvement after taking antibiotics for 48 hours.
Your doctor may give you an antibiotic shot, or he/she may prescribe an antibiotic in either pill or liquid form. You’ll usually take the pills or liquid for 10 days. Follow your doctor’s instructions. You should take all of the medication, even if you feel better. The bacteria can still be alive even if you’re feeling well.
Children taking an antibiotic who feel well and don’t have a fever often can return to school or child care when they’re no longer contagious — usually 24 hours after beginning treatment. But be sure to finish all the medicine. Stopping early can lead to recurrences and serious complications, such as rheumatic fever or kidney inflammation.
Symptom relievers
To relieve throat pain and reduce fever, try over-the-counter pain relievers, such as ibuprofen (Advil, Motrin IB, others) or acetaminophen (Tylenol, others). Use caution when giving aspirin to children or teenagers. Though aspirin is approved for use in children older than age 3, children and teenagers recovering from chickenpox or flu-like symptoms should never take aspirin. This is because aspirin has been linked to Reye’s syndrome, a rare but potentially life-threatening condition, in such children.
Drink soothing liquids like warm tea or cool drinks, and eat soft foods. Gargle with warm salt water to ease your sore throat.
You should start to feel better within a day or two of beginning an antibiotic. Most symptoms of strep throat should be gone within seven to 10 days.
Untreated, Strep throat can lead to more serious illnesses, so it’s important to start on antibiotics immediately.
Serious infections
Three infections caused by group A strep bacteria can be very serious and even deadly:
Cellulitis
Cellulitis is a bacterial infection of the skin and the subcutaneous tissue beneath it, most commonly caused by Staphylococcus aureus and Streptococcus pyogenes bacteria 25, 26, 27. Cellulitis typically appears as a red, warm, swollen, and tender area on your skin, often accompanied by fever and chills if severe. Fever may occur, and regional lymph nodes may enlarge in more serious infections. Cellulitis diagnosis is by appearance; cultures may help, but treatment with antibiotics should not be delayed pending those results, as it can spread to other parts of the body if left untreated. Prognosis is excellent with timely treatment.
The most common causes of cellulitis are 27:
- Streptococcus pyogenes
- Staphylococcus aureus
Less common causes of cellulitis are 27:
- Group B streptococci (e.g, Streptococcus agalactiae) in older adults with diabetes
- Gram-negative bacilli (e.g, Haemophilus influenzae) in children
- Pseudomonas aeruginosa in patients with diabetes or neutropenia, hot tub or spa users, and patients who are hospitalized
- Animal bites may result in cellulitis and are often caused by several types of microorganisms; Pasteurella multocida is often the cause in cat bites, and Pasteurella or Capnocytophaga species are typically responsible in dog bites.
- Immersion injuries in fresh water may result in cellulitis caused by Aeromonas hydrophila. Immersion injuries in warm salt water may result in cellulitis caused by Vibrio vulnificus.
In general, people cannot catch cellulitis from others. Patients who are immunocompromised may become infected by opportunistic organisms, including gram-negative bacteria such as Proteus, Serratia, Enterobacter, or Citrobacter, anaerobic bacteria, and Helicobacter and Fusarium species. Mycobacteria may rarely cause cellulitis.
Cellulitis is most often caused by Streptococcus pyogenes (group A beta-hemolytic streptococci) or Staphylococcus aureus. The skin barrier is usually compromised. Skin conditions like eczema, psoriasis, scabies, acne or surgical wounds. A foreign object in the skin, like glass or metal can also cause cellulitis.
Streptococcus pyogenes (group A beta-hemolytic streptococci) cause diffuse, rapidly spreading infection because enzymes produced by the organism (streptokinase, DNase, hyaluronidase) break down cellular components that would otherwise contain and localize the inflammation.
Staphylococcal cellulitis is typically more localized and usually occurs in open wounds or cutaneous abscesses.
Anyone can get cellulitis, but some factors can increase the risk of getting this infection. Risk factors include skin abnormalities (e.g, cuts, scrapes, abrasions, ulceration, fungal infection, other skin barrier compromise due to preexisting skin disease), which are common among patients with chronic venous insufficiency or lymphedema (a chronic condition causing swelling due to a compromised lymphatic system, which fails to properly drain lymph fluid). Scars from saphenous vein removal for cardiac or vascular surgery are common sites for recurrent cellulitis, especially if athlete’s foot (tinea pedis) is present. Frequently, no predisposing condition or site of entry is evident.
The following risk factors allow bacteria to get through your skin 26:
- Chickenpox and shingles
- Chronic skin conditions like athlete’s foot and eczema (dermatitis)
- Injection drug use
- Injuries that break the skin. Injuries that break the skin can include cuts, ulcers, bites, puncture wounds, tattoos, and piercings.
- Having diabetes or poor circulation.
For many people who get cellulitis, experts don’t know how the bacteria get into the body.
Other factors that increase risk for cellulitis include being overweight and chronic edema. Chronic edema is when limbs, like feet, legs, hands, or arms, stay swollen. Lymphedema and a coronary artery bypass graft (CABG) are two conditions that can cause chronic edema. Lymphedema happens when the lymphatic system doesn’t drain the way that it should. As part of the body’s immune system, the lymphatic system moves fluid containing infection-fighting cells throughout the body. A coronary artery bypass graft (CABG) includes removing a healthy vein from the leg and connecting it to the coronary artery. This surgery helps to improve blood flow to the heart.
Cellulitis can appear anywhere on the body, but it’s most common on your feet and legs. Cellulitis is typically unilateral; stasis dermatitis closely mimics cellulitis but is usually bilateral.
Generally, skin affected by cellulitis is:
- Painful
- Red
- Swollen
- Tender to the touch
- Warm
Skin affected by cellulitis is a spreading area of skin that is red, swollen, warm, and tender. The skin may look pitted, like the peel of an orange also called Peau d’orange. Blisters may appear on the affected skin. Swollen glands (lymph nodes) near the affected area. Some people may also develop fever and chills, feeling unwell, general body aches.
Most cellulitis is nonpurulent 27. However, cellulitis sometimes is accompanied by one or more pustules, furuncles, or abscesses with or without purulent drainage or exudate and is referred to as purulent 27.
Seek medical attention immediately if the red area of the skin spreads quickly or you develop a fever or chills.
Without prompt diagnosis and treatment, cellulitis could lead to several complications.
Complications from cellulitis are uncommon but can include serious infections:
- Bacteremia (bloodstream infection). If the bacterial infection reaches the bloodstream, it could lead to bacteremia. Bacteremia is diagnosable by obtaining blood cultures in patients who exhibit systemic symptoms. Your doctor should obtain identification and susceptibilities from the blood cultures and tailor antibiotics accordingly 28.
- Endocarditis (a serious infection of the inner lining of the heart, most often affecting the heart valves). Failure to identify and treat bacteremia from cellulitis can lead to endocarditis, an infection of the inner lining (endocardium) of the heart.
- Osteomyelitis (bone infection). If cellulitis moves from the deep dermis and subcutaneous tissue to the bone, it can lead to osteomyelitis.
- Suppurative arthritis (bacterial infection in a joint)
Cellulitis can cause thrombophlebitis (swelling and inflammation in a vein due to a blood clot), often in your legs.
Patients who have cellulitis along with two or more SIRS (Systemic Inflammatory Response Syndrome) criteria if at least two of the following four are present: fever over 100.4 degrees F (>38 °C), high respiratory rate over 20 breaths per minute (tachypnea), high heart rate over 90 beats per minute (tachycardia) or abnormal white cell count (over 12,000 or under 4,000, or more than 10% immature cells) get diagnosed with sepsis.
Cellulitis that leads to bacteremia, endocarditis, or osteomyelitis will require a longer duration of antibiotics and possibly surgery 29.
Doctors typically diagnose cellulitis by looking at the affected skin during a physical examination. Blood or other lab tests aren’t usually needed.
- Blood cultures are useful to detect or rule out bacteremia in patients who are immunocompromised and in patients who have signs of systemic infection (e.g, fever and leukocytosis).
- Culture of involved tissue may be required in patients who are immunocompromised if they are not responding to empiric therapy or if blood cultures do not isolate an organism as well as in patients with cellulitis at the site of certain injuries (eg, animal bite wounds, penetrating injuries).
- Skin and wound cultures (when wounds are present) are generally not indicated in cellulitis because they rarely identify the infecting organism.
Abscess should be ruled out based on clinical findings, although bedside ultrasonography may be useful.
Contact dermatitis and stasis dermatitis (a skin condition affecting the lower legs, caused by poor circulation [venous insufficiency], which leads to blood pooling and increased pressure) are often misdiagnosed as cellulitis, thus leading to unnecessary antibiotic use. Contact dermatitis can often be differentiated by the presence of itching, limitation of lesions to the site of contact, absence of systemic signs, and sometimes unilateral location. Stasis dermatitis can sometimes be differentiated by features of dermatitis itself (e.g, scaling, eczematous findings, lichenification), evidence of venous stasis, and bilateral location. Other disorders to consider include cutaneous T-cell lymphoma, nummular dermatitis, and tinea infection.
Doctors treat cellulitis with antibiotics. They can be oral antibiotics (medicine taken by mouth) or intravenous (IV) antibiotics (medicine given directly into a vein).
- Doctors use oral antibiotics to treat most cellulitis infections. IV antibiotics can be used to treat more serious infections.
Keeping the affected limb (arm or leg) elevated can help decrease swelling (edema) and speed up recovery. Wet dressings relieve local discomfort. Compression therapy can help prevent repeat episodes of leg cellulitis in patients with recurrent cellulitis who have chronic lower extremity edema.
Antibiotics
Antibiotics are the treatment of choice, and selection is based on the presence or absence of purulence and other risk factors for serious and/or resistant infection 30. Antibiotic treatments are usually not given for a fixed interval but are continued until there is satisfactory clinical response—but typically for not less than 1 week.
Nonpurulent, uncomplicated cellulitis
For most patients with cellulitis not containing pus (nonpurulent cellulitis), empiric therapy effective against both Streptococcus pyogenes and Staphylococcus aureus is used.
Oral therapy is usually adequate for mild infections, typically with dicloxacillin 250 mg or cephalexin 500 mg 4 times a day. In patients allergic to penicillin, clindamycin 300 to 450 mg 3 times a day is an alternative.
Patients with mild cellulitis caused by mammalian bites can be treated as outpatients with amoxicillin/clavulanic acid 875/125 mg orally every 12 hours. In patients allergic to penicillin, clindamycin 300 to 450 mg 3 times a day plus either an oral fluoroquinolone (eg, ciprofloxacin 500 mg every 12 hours) or double-strength sulfamethoxazole/trimethoprim (800 mg sulfamethoxazole/160 mg trimethoprim) orally 2 times a day may be used.
Cellulitis that develops after exposure to fresh or brackish water should be treated with a 1st-generation cephalosporin such as cephalexin 500 mg orally 4 times a day or cefazolin 1 g IV every 8 hours in addition to a fluoroquinolone. If cellulitis develops after exposure to brackish or salt water, doxycycline 100 mg orally 2 times a day should also be added.
Likely infecting organisms tend to be similar in brackish and fresh water (e.g, Vibrio species, Aeromonas species, Shewanella species, Erysipelothrix rhusiopathiae, Mycobacterium marinum, Streptococcus iniae).
Cellulitis can recur in patients with risk factors such as tinea pedis, obesity, venous insufficiency, edema, and atopic dermatitis. These disorders should be identified and treated to decrease the likelihood of recurrent cellulitis. Prophylactic antibiotics such as benzathine penicillin 1.2 million units IM monthly or penicillin V or erythromycin 250 mg orally 2 times a day for 1 to 12 months may be considered for patients who have 3 to 4 episodes of cellulitis per year despite treatment of risk factors. Patients taking prophylactic antibiotics should be assessed regularly to monitor for adverse effects and efficacy of treatment. Antibiotics should be continued until risk factors also have been managed. If these regimens prove unsuccessful, tissue culture may be required.
Methicillin-resistant Staphylococcus aureus (MRSA) and purulent or complicated cellulitis
Purulent cellulitis and other risk factors predispose to complicated serious (i.e, deeper, invasive, systemic) infection. Affected patients should receive coverage for methicillin-resistant Staphylococcus aureus (MRSA).
Risk factors for MRSA and complicated infection include the following 27:
- Penetrating trauma
- Surgical wounds
- Recent hospitalization or nursing home exposure
- Illicit IV drug use
- Proximity of infection to an implanted medical device such as a prosthetic joint
- Previous MRSA infection
- Known nasal colonization with MRSA
Clinical features suggestive of serious infection:
Clinical features suggestive of MRSA or complicated infection (high-risk symptoms) include the following 27:
- Pain disproportionate to physical findings
- Bleeding into the skin (cutaneous hemorrhage)
- Bullae
- Skin sloughing
- Skin anesthesia
- Rapid progression
- Tissue gas
- Signs of systemic toxicity (fever or hypothermia, tachycardia, hypotension, delirium)
For suspected MRSA without features suggesting complicated infection, empiric outpatient treatment is reasonable using double-strength sulfamethoxazole/trimethoprim (800 mg sulfamethoxazole/160 mg trimethoprim) orally 2 times a day, doxycycline 100 mg orally 2 times a day, linezolid 600 mg orally 2 times a day, or clindamycin 300 to 450 mg orally 3 times a day (however, resistance to clindamycin is becoming more prevalent) 27.
Patients who have more serious infections, with high-risk symptoms with suspected or confirmed MRSA, or whose oral therapy failed are hospitalized and typically are given one of the following 27:
- Vancomycin 15 mg/kg IV every 12 hours (drug of choice; see Antibiotic resistance)
- Linezolid 600 mg IV every 12 hours for 10 to 14 days, usually for highly resistant MRSA
- Daptomycin 4 to 6 mg/kg IV once/day
- Teicoplanin 6 mg/kg IV every 12 hours for 2 doses, followed by 3 or 6 mg/kg IV or IM once a day to achieve targeted trough concentration (mechanism of action similar to that of vancomycin; commonly used outside the United States to treat MRSA)
The use of alternative medications for severe acute bacterial skin and skin structure infection with S. aureus (including MRSA) are based on availability, ease of administration, adverse effect profile, and cost. Alternatives include:
- Linezolid or tedizolid (IV or oral)
- Delafloxacin (IV or oral)
- Omadacycline (IV or oral)
- Ceftaroline and ceftobiprole (which is only available in Canada and Europe) (IV)
- Dalbavancin, oritavancin, and telavancin (IV)
Cellulitis in a patient with neutropenia requires broad-spectrum antibiotic coverage. Vancomycin plus cefepime or meropenem is recommended until blood culture results are available to guide therapy. Tissue culture should be strongly considered for identification of the causative organism because of the increased risk of fungal infection. Culture should be considered for patients who are immunocompromised if they are not responding to empiric therapy or if blood cultures do not isolate an organism and for patients with cellulitis at the site of certain injuries (eg, animal bite wounds, penetrating injuries).
Most cellulitis resolves quickly with the correct antibiotic therapy, patients can expect to notice an improvement in signs and symptoms within 48 hours 25. There is approximately an 18% failure rate with initial antibiotic treatment 31. Local abscesses occasionally form, requiring incision and drainage. Serious but rare complications include severe necrotizing subcutaneous infection and bacteremia with metastatic foci of infection.
Recurrences in the same area are common, sometimes causing serious damage to the lymphatics, chronic lymphatic obstruction, and lymphedema. Annual recurrence of cellulitis occurs in about 8 to 20% of patients, with overall reoccurrence rates reaching as high as 49% 29, 32. Recurrence is preventable with prompt treatment of cuts or abrasions, proper hand hygiene, as well as effectively treating any underlying comorbidities.
Necrotizing fasciitis
Necrotizing fasciitis also called “flesh-eating disease” is a rare and serious bacterial infection that can be fatal if not treated promptly. Necrotizing fasciitis is a medical emergency that requires prompt attention. There are many types of bacteria that can cause the “flesh-eating disease” called necrotizing fasciitis, but experts believe Streptococcus pyogenes (group A Streptococcus bacteria) are the most common cause. Symptoms include severe pain, swelling, fever, and skin that becomes red, purple, or black. People with necrotizing fasciitis need immediate hospital care, antibiotics, and surgery. Treatment requires immediate hospital care involving intravenous antibiotics and surgery to remove dead tissue, and in some cases, amputation may be necessary.
There are two subtypes of necrotizing soft-tissue infection (flesh-eating disease):
- Type 1 necrotizing soft-tissue infection
- Type 1 necrotizing soft-tissue infection, typically involving the trunk (the central part of the human body) and perineum (the area of skin and tissue between the anus and the genitals [scrotum in males, vulva in females]), results from an infection caused by multiple types of microorganisms usually including Streptococcus pyogenes and a mixture of aerobic and anaerobic bacteria (e.g, Bacteroides species) 33. These organisms typically extend to subcutaneous tissue from a contiguous ulcer or infection, or after trauma 33. Streptococci can arrive from a remote site of infection via the bloodstream. Perineal involvement also called Fournier’s gangrene is usually a complication of recent surgery, perirectal abscess, periurethral gland infection, or retroperitoneal infection resulting from perforated abdominal viscera. Patients with diabetes are at particular risk of type 1 necrotizing soft-tissue infection. Type 1 infections often produce gas in the soft tissue, making its signs and symptoms similar to that of gas gangrene (clostridial myonecrosis), which is a soft-tissue infection is caused by a single type of microorganism 34.
- Type 2 necrotizing soft-tissue infection
- Type 2 necrotizing soft-tissue infection is caused by a single type of microorganism and is most commonly caused by group A beta-hemolytic streptococci (Streptococcus pyogenes); Staphylococcus aureus is the second most common pathogen 33. Patients tend to be younger with few documented health problems but may have a history of IV illicit drug use, trauma, or recent surgery 33. The infection has the potential for rapid local spread and systemic complications such as toxic shock. A subgroup of type 2 necrotizing soft-tissue infection usually occurs with aquatic injuries sustained in warmer coastal areas. Vibrio vulnificus is the usual pathogen 33.
Streptococcus pyogenes or group A Streptococcus (group A strep bacteria) cause necrotizing fasciitis, often through a wound, cut, or insect bite. The most common cause is Group A Streptococcus (the same bacteria that causes strep throat), but other bacteria can also be responsible. Most cases of necrotizing fasciitis occur randomly. Necrotizing fasciitis can develop quickly and is more common in people with weakened immune systems, advanced age, or chronic illnesses like diabetes. However, less serious group A strep infections can turn into necrotizing fasciitis and these bacteria are contagious.
Necrotizing soft-tissue infection causes tissue ischemia by widespread blockage of small subcutaneous vessels. Small subcutaneous blood vessel blockage results in skin infarction and necrosis, which facilitates the growth of obligate anaerobes (eg, Bacteroides) while promoting anaerobic metabolism by facultative organisms (eg, Escherichia coli), resulting in gangrene 33. Anaerobic metabolism produces hydrogen and nitrogen, relatively insoluble gases that may accumulate in subcutaneous tissues 33.
Risk factors for necrotizing soft-tissue infection 33:
Although it’s rare, anyone can get necrotizing fasciitis. Some conditions that weaken the immune system can increase the risk for necrotizing fasciitis. Most people who get necrotizing fasciitis have other health factors that may lower their body’s ability to fight infections. Conditions that weaken the body’s immune system include:
- Cancer
- Cirrhosis (scarring) of the liver
- Diabetes
- Kidney disease
Injuries that break the skin. People with an open wound (break in the skin) are at increased risk for necrotizing fasciitis. The bacteria most commonly enter the body through a break in the skin, which can include:
- Burns
- Cuts and scrapes
- Insect bites
- Puncture wounds (including those due to intravenous [IV] drug use)
- Surgical wounds
However, people can also get necrotizing fasciitis after blunt trauma (an injury that doesn’t break the skin).
Necrotizing fasciitis spreads very quickly.
- Early symptoms can include 35:
- A red, warm, or swollen area of skin that spreads quickly and hot to the touch
- Fever and flu-like symptoms (nausea, vomiting, diarrhea)
- Severe pain disproportionate to any visible injury, including beyond the area that’s red, warm, or swollen
See your doctor right away if you have these symptoms, particularly after an injury or surgery. Even though other illnesses can cause symptoms like these, people shouldn’t delay getting medical care.
- Later symptoms can include 35:
- Changes in the color of the skin
- Swelling and blisters filled with dark fluid
- Diarrhea or nausea
- Dizziness
- Fatigue (tiredness)
- Pus or oozing from the infected area
- Ulcers, blisters, or black spots on the skin
- Skin that turns purple, gray, or black as tissue dies (necrosis)
- General feeling of being unwell
Necrotizing fasciitis complications
Necrotizing fasciitis can lead to:
- Organ failure
- Sepsis (a life-threatening condition caused by the body’s extreme, damaging response to an infection)
- Shock (a life-threatening medical emergency where the body isn’t getting enough blood flow, which deprives organs of oxygen)
Necrotizing fasciitis can also result in life-long complications from loss of limbs or severe scarring due to surgically removing infected tissue. Recent data show how deadly necrotizing fasciitis can be. Even with treatment, about 20% to 30% people died from the infection 36. Old age, underlying medical problems, delayed diagnosis and therapy, and insufficient surgical debridement worsen prognosis.
Testing and diagnosis
There are many infections that look similar to necrotizing fasciitis in the early stages, which can make diagnosis difficult. In addition to looking at the injury or infection, doctors can diagnose necrotizing fasciitis with:
- Biopsies (taking tissue samples)
- Bloodwork for signs of infection and muscle damage
- Imaging (CT scan, MRI, ultrasound) of the damaged area
However, it’s important to start treatment as soon as possible. Therefore, your doctor may not wait for test results if they think a patient might have necrotizing fasciitis.
Treatment of necrotizing soft-tissue infection
Necrotizing fasciitis is a very serious illness that requires hospital care. Antibiotics and surgery are typically necessary.
- Surgical debridement
- Treatment of early necrotizing soft-tissue infection and clostridial myonecrosis is primarily surgical, which should not be delayed by diagnostic studies. It is crucial to surgically remove all dead and infected tissue. This may involve removing large amounts of tissue or, in severe cases, lead to amputation.
- Since necrotizing fasciitis can spread rapidly, patients often must get surgery quickly. It’s not unusual for someone with necrotizing fasciitis to end up needing multiple surgeries. In serious cases, the patient may need a blood transfusion.
- Evidence of bullae, ecchymosis, fluctuance, crepitus, and systemic spread of infection requires immediate surgical exploration and debridement. The initial incision should be extended until an instrument or finger can no longer separate the skin and subcutaneous tissue from the deep fascia. The most common error is insufficient surgical intervention; repeat operation every 1 to 2 days, with further incision and debridement as needed, should be carried out routinely. Negative-pressure wound therapy also called vacuum-assisted closure (VAC), which applies suction to the wound, has been used as an adjunct for care between debridements.
- Intravenous antibiotics
- To try to stop the infection, doctor give antibiotics directly into a vein (IV), which allows medicine to flow into a vein. Sometimes, however, antibiotics can’t reach all the infected areas because the bacteria have killed too much tissue and reduced blood flow. When this happens, doctors must surgically remove the dead tissue.
- IV antibiotics are add-ons, usually including 2 or more medications. An empiric regimen should include antibiotics effective against aerobic and anaerobic organisms. Current recommendations from the Infectious Diseases Society of America (IDSA) suggest vancomycin, linezolid, or daptomycin combined with piperacillin/tazobactam, a carbapenem, ceftriaxone plus metronidazole, or a fluoroquinolone plus metronidazole. Antibiotic coverage should be narrowed based on blood and tissue culture results once they become available.
- Amputation if necessary. Amputation of an extremity may be necessary.
- IV fluids may be needed in large volumes before and after surgery.
- IV immune globulin has been suggested as adjunctive therapy for streptococcal toxic shock syndrome with necrotizing soft-tissue infection.
- Doctors may also perform other procedures like blood transfusions or plastic surgery to help close wounds.
Streptococcal toxic shock syndrome
Streptococcal toxic shock syndrome (STSS) also called Streptococcus pyogenes toxic shock syndrome is a life-threatening bacterial illness caused by group A beta-hemolytic streptococci (GABHS) infection associated with shock and organ failure that requires immediate medical attention. Initial symptoms of Streptococcal toxic shock syndrome (STSS) often appear flu-like, including fever, nausea, and aching muscles, but can quickly progress to more severe signs like dangerously low blood pressure, rapid heart and breathing rates, confusion, and organ failure. Treatment involves aggressive care, such as intensive care, IV antibiotics, and supportive therapies like intravenous fluids, with high-dose intravenous immunoglobulins sometimes used to improve outcomes. Streptococcal toxic shock syndrome is similar to that caused by Staphylococcus aureus, but mortality is higher (20 to 60%) despite aggressive therapy 37. Mortality rate for streptococcal toxic shock syndrome (STSS) is approximately 28% in children 38 and up to 45% in adults 34, and highest in patients presenting with necrotizing fasciitis. In addition, Streptococcus pyogenes bacteremia is frequently present, and 50% or more cases are associated with deep soft tissue streptococcal infections such as necrotizing fasciitis or erysipelas (a superficial bacterial skin infection that is characterized by a sharply defined, raised, red rash), neither is common with staphylococcal toxic shock syndrome 34. Patients are usually otherwise healthy children or adults. Primary infections in skin and soft tissue are more common than in other sites. In contrast to staphylococcal toxic shock syndrome, streptococcal toxic shock syndrome is more likely to cause acute respiratory distress syndrome (ARDS) and less likely to cause a typical cutaneous reaction.
Streptococcal toxic shock syndrome (STSS) can occur in anyone but is associated with factors that break the skin’s surface, including:
- Minor cuts or injuries
- Surgical procedures
- Viral infections (eg, varicella)
- Use of nonsteroidal anti-inflammatory drugs (NSAIDs)
- Diabetes
- Alcohol use disorder
- Age (children and older adults)
Symptoms of Streptococcal toxic shock syndrome (STSS) include:
- Early symptoms: High fever, nausea, vomiting, and muscle aches.
- Severe symptoms:
- Dangerously low blood pressure (hypotension)
- Rapid heart rate (tachycardia) and rapid breathing (tachypnea)
- Rash that can be flat and widespread or develop into peeling skin, particularly on the palms and soles
- Confusion or disorientation
- Organ failure (kidney, liver)
Onset of toxic shock syndrome is sudden, with 39:
- Fever (39 to 40.5° C, which remains elevated)
- Low blood pressure (hypotension) (systolic blood pressure < 90 mm Hg for adults or less than the fifth percentile for age in children; it can be refractory)
- A diffuse widespread red rash (erythroderma) that includes a macular (flat, red) component (especially on the palms and soles, 1 to 2 weeks after onset)
- Involvement of at least 3 other organ systems (eg, gastrointestinal, muscular, mucous membrane, renal, hepatic, hematologic, central nervous system)
Streptococcal toxic shock syndrome commonly causes acute respiratory distress syndrome, bleeding disorder, and liver damage and is more likely to cause high fever, malaise, rapid heart rate (tachycardia), rapid breathing (tachypnea) and severe pain at the site of a soft-tissue infection 40. Kidney impairment is frequent and common in Streptococcal toxic shock syndrome 37.
Although less severe cases of staphylococcal toxic shock syndrome are fairly common, severe cases of toxic shock syndrome may progress within 48 hours to fainting (syncope), tissue necrosis, shock, disseminated intravascular coagulation (a serious and life-threatening disorder where abnormal blood clotting occurs throughout the body’s blood vessels), multisystem organ failure, and death 37.
Treatment of Streptococcal toxic shock syndrome (STSS) 37:
- Patients suspected of having toxic shock syndrome should be hospitalized immediately, often in an Intensive Care Unit (ICU), due to its rapid progression and treated intensively. Tampons, diaphragms, and other foreign bodies suspected to be contributing to the infection should be removed at once.
- Antibiotics: Intravenous (IV) antibiotics are a cornerstone of treatment to control the bacterial infection. Empiric antibiotic therapy (eg, beta-lactams or vancomycin, daptomycin, or ceftaroline (if MRSA proven or suspected) plus protein inhibitors (clindamycin or linezolid) pending culture results.
- Pending culture results, clindamycin or linezolid (to suppress toxin production) plus vancomycin, daptomycin, linezolid (if clindamycin used), or ceftaroline should be used; these antibiotics are empiric choices that cover the most likely etiologic organisms. If a pathogen is isolated on culture, the antibiotic regimen is adjusted as needed, as for the following:
- For group A streptococci: Clindamycin or linezolid plus a beta-lactam
- For methicillin-susceptible S. aureus (MSSA): Clindamycin plus oxacillin or nafcillin
- For methicillin-resistant Staphylococcus aureus (MRSA): Vancomycin or daptomycin plus clindamycin or linezolid, depending on the susceptibility
- Antibiotics given during the acute illness may eradicate pathogen foci and prevent recurrences. Passive immunization to toxic shock syndrome toxins with IV immune globulin (IVIg) has been helpful in severe cases of both types of toxic shock syndrome and lasts for weeks, but the disease may not induce active immunity, so recurrences are possible. It may reduce mortality from staphylococcal toxic shock syndrome, especially when coadministered with clindamycin 41.
- Pending culture results, clindamycin or linezolid (to suppress toxin production) plus vancomycin, daptomycin, linezolid (if clindamycin used), or ceftaroline should be used; these antibiotics are empiric choices that cover the most likely etiologic organisms. If a pathogen is isolated on culture, the antibiotic regimen is adjusted as needed, as for the following:
- Supportive care: This includes IV fluids to help with low blood pressure and medications to support failing organs. Fluids and electrolytes are replaced to prevent or treat hypovolemia, hypotension, and shock. Because fluid loss into tissues can occur throughout the body (because of systemic capillary leak syndrome and hypoalbuminemia), subsequent shock may be profound and resistant. Aggressive fluid resuscitation and circulatory, ventilatory, and/or hemodialysis support are sometimes required.
- Immunoglobulins: High-dose IV immunoglobulin (IVIg) may be administered to help neutralize the toxins.
- Surgery: In some cases, surgery may be needed to remove the source of the infection. Suspected primary sites should be decontaminated thoroughly. Decontamination includes:
- Reinspection and irrigation of surgical wounds, even if they appear healthy
- Repeated debridement of devitalized tissues
- Irrigation with normal saline of potential naturally colonized sites (sinuses, vagina)
If a test for seroconversion of the serum antibody responses to TSST-1 in acute- and convalescent-phase paired sera is negative, women who have had staphylococcal toxic shock syndrome may have a genetically higher risk of toxic shock syndrome due to associations with HLA class II genes 42. Such women (with higher genetic risks and negative seroconversion) should refrain from using tampons and menstrual cups, cervical caps, contraceptive sponges, intrauterine devices, diaphragms, and pessaries. Advising all women, regardless of TSST-1 antibody status, to change tampons or other vaginally inserted materials frequently or use napkins instead and to avoid hyperabsorbent tampons seems prudent.
In cases of S. aureus nasal carriage, topical mupirocin may be used. In cases of extra-nasal colonization, bathing with additional chlorhexidine antiseptic for 1 week is warranted.
Inflammatory diseases
Long-term health issues related to group A strep bacteria include:
- Post-streptococcal glomerulonephritis (PSGN)
- Rheumatic fever
Both are thought to be caused by an immune response to an earlier group A strep infection. As the body’s defense system, the immune system is important in fighting off infections. But the immune system can mistakenly attack healthy parts of the body and cause damage.
Post-streptococcal glomerulonephritis
Post-streptococcal glomerulonephritis (PSGN) is a kidney disease that can occur after a Streptococcus pyogenes (group A Streptococcus) infection, such as a sore throat or skin infection like impetigo. It happens when your immune system’s response to the bacteria damages your kidneys’ glomeruli (filters). Symptoms often include swelling (edema), high blood pressure, and dark or reddish-brown urine. While often mild and self-limiting, especially in children, treatment focuses on managing symptoms and may include antibiotics for the original infection, a low-salt diet, and medication for blood pressure and swelling.
Most post-streptococcal glomerulonephritis (PSGN) cases are caused by nephritogenic strains of group A beta-hemolytic streptococci, most notably type 12 which causes pharyngitis and type 49 which causes impetigo 43. A latency period (the time between exposure to the infection and the appearance of symptoms or effects) of 6 to 21 days between infection and glomerulonephritis onset is typical, but latency may extend up to 6 weeks 43.
Latent period
- Following group A strep throat: post-streptococcal glomerulonephritis (PSGN) occurs after a latent period of approximately 10 days.
- Following streptococcal skin infections: post-streptococcal glomerulonephritis (PSGN) occurs up to 3 weeks later.
There are no known risk factors specific for post-streptococcal glomerulonephritis (PSGN). Post-streptococcal glomerulonephritis (PSGN) is more common in children, particularly pre-school and early school aged children. However, it can also occur in adults.
Risk factors for post-streptococcal glomerulonephritis (PSGN) are the same as for the preceding infection:
- Risk factors for strep throat
- Risk factors for skin infections
There’s insufficient evidence to determine if antibiotic therapy can prevent post-streptococcal glomerulonephritis 44, 45.
The clinical features of acute glomerulonephritis include:
- Fluid retention (edema). Fluid retention (edema), particularly in the face (especially the eyes in the morning), hands, feet, and abdomen.
- High blood pressure (hypertension). High blood pressure, which can range from mild to severe.
- Protein in urine (proteinuria). Foamy or bubbly urine due to excess protein.
- Macroscopic blood in urine (hematuria), with urine appearing dark, reddish-brown or cola-colored urine due to blood.
- Oliguria or anuria: Decreased urine output or no urine output.
- Complaints of lethargy, generalized weakness, or anorexia
Other signs and symptoms post-streptococcal glomerulonephritis (PSGN) may include:
- Fatigue and malaise
- Nausea and vomiting
- Headaches
- Abdominal pain
- Fever
- Malaise
More severe signs and complications post-streptococcal glomerulonephritis (PSGN):
- Shortness of breath from fluid buildup in the lungs (pulmonary edema)
- Confusion, seizures, or coma (hypertensive encephalopathy)
- Joint pain
- Rashes
- Chest pain or palpitations
Laboratory tests usually reveal:
- Mild normocytic normochromic anemia
- Slight hypoproteinemia
- Elevated blood urea nitrogen (BUN) and creatinine
- Elevated erythrocyte sedimentation rate (ESR)
- Low total hemolytic complement and C3 complement
Patients usually have decreased urine output. Urine examination often reveals protein (usually <3 grams per day) and hemoglobin with red blood cell casts.
Subclinical cases of post-streptococcal glomerulonephritis (PSGN) with only microscopic hematuria and decreased complement levels can occur 46. Some individuals may have symptoms that are mild enough to not come to medical attention.
Clinical history and findings with evidence of a preceding group A strep infection should inform a post-streptococcal glomerulonephritis diagnosis.
Evidence of preceding group A strep infection can include:
- Isolation of group A strep from the throat
- Isolation of group A strep from skin lesions
- Elevated streptococcal antibodies
Treatment of post-streptococcal glomerulonephritis focuses on managing hypertension and edema.
Patients should receive penicillin (preferably penicillin G benzathine) to eradicate any remaining group A strep. This will help prevent spread of the bacteria to other people.
The prognosis of post-streptococcal glomerulonephritis in children is very good. More than 90% of children make a full recovery. Adults with post-streptococcal glomerulonephritis are more likely to have a worse outcome due to residual kidney function impairment. Debilitated adults, the mortality rate can be as high as 30%, as a consequence of a cardiovascular complication 47.
The long-term prognosis of post-streptococcal glomerulonephritis, as related to the development of chronic kidney disease, is also different in children and in adults. In a recent study of a specific outbreak of post-streptococcal glomerulonephritis that resulted from the consumption of cheese contaminated with Streptococcus zooepidemicus and that affected mostly adults, there was an alarming incidence of chronic renal disease: impaired renal function was found in 30% of the patients after 2 years of follow-up (10% of them in chronic dialysis therapy) 48. A recent 20-year follow-up of the patients with post-streptococcal glomerulonephritis predominantly adult patients (mean age 56.6 years), found 72% hypertensives, 44.7% with eGFR <60ml/min/m², 18.6% with a urinary protein/creatinine ratio >150mg/g and 53% had chronic kidney disease (low eGFR and/or increased proteinuria) 49.
In a particular subgroup of adult patients with acute post-streptococcal glomerulonephritis that had massive proteinuria as the initial manifestation of the disease, the long-term prognosis was especially severe, with an incidence of chronic renal failure as high as 77% 50. The worse prognosis in adults has been attributed to age-related impairment of the Fc-receptor function of the mononuclear phagocyte system 51. Deficiency of the complement factor H-related protein 5 (CFHR5) has also been proposed as a factor that may result in a predisposition to the development of chronic renal disease 52. In addition, a study from the Mayo Clinic found abnormalities in the alternative pathway of complement (mutations in complement factor H or in CFHR5, and/or C3 Nef) in 10 of 11 patients with atypical postinfectious glomerulonephritis. The patients had persistent microscopic hematuria and proteinuria, plus subepithelial “humps” and, in most cases, C3-dominant deposits on renal biopsy 53.
Rheumatic fever
Rheumatic fever is an inflammatory condition caused by an abnormal autoimmune response to an untreated Group A Streptococcus infection, such as strep throat (streptococcal pharyngitis 54, 55, 56, 57. Rheumatic fever can lead to a variety of symptoms affecting your joints (arthritis), brain (chorea), skin (subcutaneous nodules, erythema marginatum), and heart (carditis), with the potential for long-term damage to heart valves, a condition known as rheumatic heart disease. Rheumatic fever diagnosis is based on applying the Revised Jones criteria to information gleaned from history, examination, and laboratory testing. Treatment includes aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids during severe carditis, and antibiotics to eradicate residual streptococcal infection and to prevent future episodes, with the goal of preventing or limiting heart damage.
Rheumatic fever is more common in children than adults:
- Most common: School-age children (5 through 15 years old)
- Rare: Children younger than 3 years old and adults
- Someone who had rheumatic fever is more likely to get it again if they get another group A strep infection.
- If someone with rheumatic fever is still infected with group A strep bacteria, they can spread the bacteria to others. Group A strep bacteria are contagious.
A first episode of acute rheumatic fever can occur at any age but occurs most often between 5 years and 15 years of age, which are the peak years of age for strep throat (streptococcal pharyngitis) 54. Acute rheumatic fever is uncommon before 3 years and after 21 years 54. However, preceding symptomatic pharyngitis is recognized in only about two thirds of patients with acute rheumatic fever 54.
Approximately 470,000 new cases of acute rheumatic fever and 233,000 attributable deaths due to acute rheumatic fever or rheumatic heart disease are reported yearly 58. Worldwide, acute rheumatic fever incidence ranges from 8 to 51/100,000, with lowest rates (< 10 per 100,000) in North America and Western Europe and highest rates (> 10 per 100,000) in Eastern Europe, the Middle East, Asia, Africa, Australia, and New Zealand 59, 60, 61, 62, 56. The attack rate (percentage of patients with untreated group A streptococcal pharyngitis who develop acute rheumatic fever) varies from < 1.0% to 3.0% 54. Higher attack rates occur with certain streptococcal M protein serotypes and a stronger host immune response likely resulting from as-yet-uncharacterized genetic tendencies 54.
In patients with a prior episode of acute rheumatic fever, the rate of recurrence of acute rheumatic fever in untreated group A streptococcal pharyngitis approaches 50%, underscoring the importance of long-term antistreptococcal prophylaxis 54. Incidence has declined in most developed countries but remains high in resource-poor parts of the world, especially parts with aboriginal or native populations, such as Alaskan Native, Canadian Inuit, Native American, Australian Aboriginal, and Maori New Zealander, where incidence is as high as 50 to 250 per 100,000 54. However, the continued occurrence in the United States of local outbreaks of acute rheumatic fever suggest that more rheumatogenic strains of streptococci are still present in the United States 54.
The prevalence of chronic rheumatic heart disease is uncertain because criteria are not standardized and autopsy is not done routinely, but it is estimated that worldwide there are ≥ 39 million patients with rheumatic heart disease, resulting in about 300,000 deaths annually 54.
Rheumatic fever can develop about 1 to 5 weeks after a group A strep infection.
Common symptoms of rheumatic fever can include:
- Arthritis (painful, tender joints). Arthritis is most common in the knees, ankles, elbows, and wrists.
- Chorea (jerky, uncontrollable body movements)
- Fatigue (tiredness)
- Fever
Uncommon rheumatic fever symptoms:
- Subcutaneous nodules (painless lumps) near joints. Subcutaneous nodules, which occur most frequently on the extensor surfaces of large joints (eg, knees, elbows, wrists), usually coexist with arthritis and carditis. Fewer than 10% of children with acute rheumatic fever have nodules. Ordinarily, the nodules are painless and transitory and respond to treatment of joint or heart inflammation.
- Rash with pink rings and a clear center also known as erythema marginatum. Erythema marginatum is a serpiginous, flat or slightly raised, nonscarring, and painless rash. Fewer than 6% of children have this rash. The rash usually appears on the trunk and proximal extremities but not the face. It sometimes lasts < 1 day. Its appearance is often delayed after the inciting streptococcal infection; it may appear with or after the other manifestations of rheumatic inflammation.
Heart-related symptoms
Symptoms of rheumatic fever can also include symptoms of congestive heart failure:
- Chest pain
- Fast heartbeat
- Shortness of breath
Heart failure caused by the combination of inflammation of the heart (carditis) and heart valve dysfunction may cause shortness of breath (dyspnea) without rattling sound (rales), nausea and vomiting, a right upper quadrant or epigastric ache, and a hacking, nonproductive cough. Marked lethargy and fatigue may be early signs and symptoms of heart failure.
In addition, someone with rheumatic fever can have:
- Inflammation of the heart (carditis) can occur alone or in combination with pericardial rub, heart murmurs, an enlarged heart, or heart failure. In the first episode of acute rheumatic fever, carditis occurs in about 50 to 70%. Patients may have high fever, chest pain, or both; fast heartbeat (tachycardia) is common, especially during sleep. In about 50% of cases, heart damage (ie, persistent heart valve dysfunction) occurs much later. Although the carditis of acute rheumatic fever is considered to be a pancarditis (involving the endocardium, myocardium, and pericardium), inflammation of heart valves (valvulitis) is the most consistent feature of acute rheumatic fever, and if it is not present, the diagnosis should be reconsidered. The diagnosis of inflammation of heart valves (valvulitis) has classically been made by listening to your heart for murmurs, but subclinical cases (ie, valvular dysfunction not manifested by heart murmurs but recognized on echocardiography and Doppler studies) may occur in up to 18% of cases of acute rheumatic fever.
- A new heart murmur. Heart murmurs are common and, although usually evident early, may not be heard at initial examination; in such cases, repeated clinical examinations as well as echocardiography are recommended to determine the presence of carditis. Mitral valve regurgitation is characterized by an apical pansystolic blowing murmur radiating to the axilla. The soft diastolic blow at the left sternal border of aortic valve regurgitation, and the presystolic murmur of mitral stenosis, may be difficult to detect. Murmurs often persist indefinitely. If no worsening occurs during the next 2 to 3 weeks, new signs and symptoms of carditis seldom follow. Acute rheumatic fever typically does not cause chronic, smoldering carditis. Scars left by acute valvular damage may contract and change, and secondary hemodynamic difficulties may develop in the myocardium without persistence of acute inflammation.
- An enlarged heart
- Fluid around the heart
If rheumatic fever is not treated promptly, rheumatic heart disease may occur. Rheumatic heart disease weakens the valves between the chambers of the heart. Severe rheumatic heart disease can require heart surgery and result in death.
Sydenham chorea is a neurological disorder in children caused by an autoimmune reaction to a Streptococcus infection, leading to sudden, involuntary, jerky movements of the face, limbs, and trunk. Chorea consists of rapid and irregular jerking movements that may begin in the hands but often becomes generalized, involving the feet and face. Other symptoms include muscle weakness, emotional disturbances like irritability and obsessiveness, and difficulties with speech, handwriting, and concentration. Sydenham chorea occurs in about 10 to 30% of children. It may develop along with other signs and symptoms of rheumatic fever, but frequently arises after the signs and symptoms of rheumatic fever have subsided (often months after the acute streptococcal infection) and therefore may be overlooked as an indicator of acute rheumatic fever. Onset of chorea is typically insidious and may be preceded by inappropriate laughing or crying.
Characteristic findings include fluctuating grip strength (milkmaid’s grip), tongue fasciculations or tongue darting (the tongue cannot protrude without darting in and out), facial grimacing, and explosive speech with or without tongue clucking. Associated motor symptoms include loss of fine motor control, and weakness and hypotonia (that can be severe enough to be mistaken for paralysis).
Previously undiagnosed obsessive-compulsive behavior may be unmasked in many patients.
Sydenham chorea treatment focuses on preventing recurrent infections with long-term antibiotics and managing symptoms with medication and supportive therapies.
Table 1. Revised Jones Criteria for diagnosing Acute Rheumatic Fever
| Low-Risk Population | Moderate- and High-Risk Populations | |
|---|---|---|
| Major Criteria | Carditis (clinical or subclinical) | Carditis (clinical or subclinical) |
| Polyarthritis | Monoarthritis, polyarthritis, or polyarthralgia | |
| Chorea | Chorea | |
| Subcutaneous nodules | Subcutaneous nodules | |
| Erythema marginatum | Erythema marginatum | |
| Minor Criteria | Polyarthralgia | Monoarthralgia |
| Fever ≥101.5 °F (38.5 °C) | Fever ≥100.4 °F (38 °C) | |
| ESR >60 mm/hr or CRP >3.0 mg/dL | ESR >30 mm/hr or CRP >3.0 mg/dL | |
| ECG with prolonged PR interval | ECG with prolonged PR interval |
Footnotes: ESR = erythrocyte sedimentation rate; CRP = C-reactive protein.
* Diagnosis of acute rheumatic fever requires 2 major or 1 major and 2 minor manifestations and evidence of group A streptococcal infection (elevated or rising antistreptococcal antibody titer [e.g, antistreptolysin O, anti-DNase B], positive throat culture, or positive rapid antigen test in a child with clinical manifestations suggestive of streptococcal pharyngitis).
† Carditis can be clinical and/or subclinical. Subclinical carditis is defined by strict echocardiographic criteria.
‡ Polyarthralgia is not used for diagnosis if polyarthritis is a major criterion for the patient.
§ PR interval is adjusted for age and is not used for diagnosis if carditis is a major criterion for the patient 63
[Source 55 ]Rheumatic fever diagnosis
There’s no single test used to diagnose rheumatic fever. Instead, doctor can look for signs of illness and check your medical history. Your doctor can also use many tests, including:
- Blood test to look for antibodies of a recent group A strep infection
- Echocardiography or echo (to see the heart muscle working)
- Electrocardiogram or EKG (a test of how well the heart is working)
- Throat swab to look for a group A strep infection
Diagnosis of a first episode of acute rheumatic fever is based on the Revised Jones criteria (see Table 1 Revised Jones Criteria for a First Episode of Acute Rheumatic Fever).
Initial diagnosis in any risk population requires the following:
- 2 major criteria, or
- 1 major and 2 minor criteria
The diagnosis of a recurrent episode of acute rheumatic fever requires the following:
- 2 major criteria, or
- 1 major and 2 minor criteria, or
- 3 minor criteria
The modified Jones criteria were designed for the evaluation of acute rheumatic fever rather than for a possible recurrence. A presumptive diagnosis of acute rheumatic fever may be made without using the Revised Jones Criteria in patients presenting with Sydenham chorea or carditis months after group A Streptococcus infection. These cases require further evaluation with an echocardiogram. A possible case can be defined as patients who meet the criteria for an initial infection but lack evidence of preceding group A Streptococcus infection. Patients with 1 major and 1 minor criteria with evidence of a preceding group A Streptococcus infection are also labeled as possible cases of acute rheumatic fever 64. However, if patients have a reliable past history of acute rheumatic fever or rheumatic heart disease and also have documented group A Streptococcus infection, the modified Jones criteria may be used to establish the presence of a recurrence.
A preceding group A Streptococcus infection is suggested by a recent history of pharyngitis and is confirmed by 1 or more of the following:
- Positive throat culture
- Increased or preferably rising antistreptolysin O titer (ASO titer) or antideoxyribonuclease B (Anti-DNase B) antibody titer
Positive rapid group A Streptococcus antigen test in a child with clinical manifestations suggestive of streptococcal pharyngitis
Recent scarlet fever is highly suggestive. Throat cultures and rapid strep antigen tests are often negative by the time acute rheumatic fever manifests, whereas titers of antistreptolysin O and anti-DNase B typically peak 3 to 6 weeks after group A Streptococcus pharyngitis. About 80% of children with acute rheumatic fever have a significantly elevated antistreptolysin O titer; if an anti-DNase B antibody level is also done, the percentage with confirmed group A Streptococcus infection is higher, especially if acute and convalescent samples are tested.
Joint aspiration may be needed to exclude other causes of arthritis (eg, infection). The joint fluid is usually cloudy and yellow, with an elevated white blood cell (WBC) count composed primarily of neutrophils; culture is negative. Complement levels are usually normal or slightly decreased, compared with decreased levels in other inflammatory arthritides.
ECG is done during the initial evaluation. Serum cardiac marker levels are obtained; normal cardiac troponin I levels exclude prominent myocardial damage. ECG abnormalities such as PR prolongation do not correlate with other evidence of carditis. Only 35% of children with acute rheumatic fever have a prolonged PR interval; higher-degree heart block may occur but is uncommon. Other ECG abnormalities may be due to pericarditis, enlargement of ventricles or atria, or arrhythmias.
Echocardiography can detect evidence of carditis even in patients without apparent murmurs and is recommended for all patients with confirmed or suspected acute rheumatic fever. Echocardiography is also used to detect subclinical carditis in patients with apparently isolated Sydenham chorea and to monitor the status of patients with recurrences of carditis or chronic rheumatic heart disease. However, not all echocardiographic abnormalities represent rheumatic carditis; isolated trivial valvar regurgitation or trivial pericardial effusion may be a nonspecific finding.
To maintain specificity, echocardiographic and Doppler results should meet the following criteria for acute rheumatic carditis 65:
- Doppler flow criteria:
- Pathologic mitral regurgitation: Must be seen in at least 2 views, and have a jet length ≥ 2 cm in at least 1 view, a peak velocity of > 3 m/second, and a pansystolic jet in at least 1 envelope
- Pathologic aortic regurgitation: Must be seen in at least 2 views, and have a jet length ≥ 1 cm in at least 1 view, a peak velocity of > 3 m/second, and a pandiastolic jet in at least 1 envelope
- Echocardiographic morphologic criteria:
- Pathologic mitral valve morphologic changes include annular dilation, chordal elongation or rupture with flail leaflet, anterior (or less commonly posterior) leaflet tip prolapse, or beading/nodularity of leaflet tips.
- Pathologic aortic valve morphologic changes include irregular or focal leaflet thickening, coaptation defect, restricted leaflet motion, or leaflet prolapse.
Chest x-rays are not routinely done but can detect cardiomegaly, a common manifestation of carditis in acute rheumatic fever.
Biopsy of a subcutaneous nodule can aid in early diagnosis, especially when other major clinical manifestations are absent.
ESR and serum CRP are sensitive but not specific. The ESR is typically > 60 mm/hour. CRP is typically > 3 mg/dL (> 30 mg/L) and often > 7 mg/dL (> 70 mg/L); because it rises and falls faster than ESR, a normal CRP may confirm that inflammation is resolving in a patient with prolonged ESR elevation after acute symptoms have subsided. In the absence of carditis, ESR usually returns to normal within 3 months. Evidence of acute inflammation, including ESR, usually subsides within 5 months in uncomplicated carditis. The WBC count reaches 12,000 to 20,000/mcL (12 to 20 × 109/L) and may go higher with corticosteroid therapy.
The differential diagnosis includes JIA (especially systemic JIA and, less so, polyarticular JIA), Lyme disease, reactive arthritis, arthropathy of sickle cell disease, leukemia or other cancer, systemic lupus erythematosus, embolic bacterial endocarditis, serum sickness, Kawasaki disease, drug reactions, and gonococcal arthritis. These are frequently distinguished by history or specific laboratory tests. The absence of an antecedent Streptococcus pyogenes infection, the diurnal variation of the fever, evanescent rash, and prolonged symptomatic joint inflammation usually distinguish systemic juvenile idiopathic arthritis (JIA) from acute rheumatic fever.
The primary goals of rheumatic fever treatment are eradication of group A streptococcal infection, relief of acute symptoms, suppression of inflammation, and prophylaxis against future infection to prevent recurrent heart disease. For general management, patients should limit their activities if they have symptoms of arthritis, chorea, or heart failure. In the absence of carditis, no physical restrictions are needed after the initial episode subsides. In asymptomatic patients with carditis, strict bed rest has no proven value, despite its traditional usage.
Antibiotic treatment
Although poststreptococcal inflammation is well developed by the time acute rheumatic fever is detected, a 10-day course of oral penicillin or amoxicillin, or a single injection of penicillin G benzathine, is used to eradicate any lingering organisms and prevent reinfection. For specific regimens, see treatment of streptococcal pharyngitis. Antibiotic prophylaxis is continued as described below.
Aspirin and anti-inflammatory medications
Aspirin controls fever and pain and should be given to all patients with arthritis and/or mild carditis. Although aspirin has been used for many decades, there are surprisingly few data from controlled trials to define the optimal dosing schedule. Most experts would give children and adolescents 15 to 25 mg/kg orally 4 times a day (to a maximum daily dose of 4 to 6 g) for 2 to 4 weeks and then taper the dose over another 4 weeks. Symptomatic acute rheumatic fever responds dramatically to aspirin. If no improvement is seen after 24 to 48 hours of high-dose aspirin therapy, the diagnosis of acute rheumatic fever should be reconsidered. Salicylate toxicity is the limiting factor to aspirin therapy and is manifested by tinnitus, headache, or hyperpnea; it may not appear until after 1 week of therapy. Salicylate levels are measured only to manage toxicity. Enteric-coated, buffered, or complex salicylate molecules provide no advantage.
For patients with minimal to mild carditis, there are no controlled data to suggest that adding prednisone to aspirin therapy speeds resolution of illness or prevents rheumatic heart disease.
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been reported in small trials to be effective; naproxen (7.5 to 10 mg/kg orally 2 times a day) is the most studied. However, other nonsteroidal anti-inflammatory drugs (NSAIDs) have few advantages over aspirin, especially in the first week of therapy when salicylism is uncommon. Acetaminophen is not effective for symptoms of acute rheumatic fever.
Oral prednisone is recommended instead of aspirin for patients with moderate to severe carditis (as judged by a combination of clinical findings, presence of cardiac enlargement, and possibly by severely abnormal echocardiography results). If inflammation is not suppressed after 2 days or for severe heart failure, an IV corticosteroid pulse of methylprednisolone succinate (30 mg/kg IV once a day, maximum 1 g/day, for 3 successive days) may be given. Oral corticosteroids typically are given for 2 to 4 weeks and then tapered over another 2 to 3 weeks. Aspirin should be started during the corticosteroid taper and continued for 2 to 4 weeks after the corticosteroid has been stopped. Aspirin dose is the same as above. Inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein may be used to monitor disease activity and response to treatment.
Recurrences of mild cardiac inflammation (indicated by fever or chest pain) may subside spontaneously; aspirin or corticosteroids should be resumed if recurrent symptoms last longer than a few days or if heart failure is uncontrolled by standard management (eg, diuretics, angiotensin-converting enzyme inhibitors, beta-blockers, inotropic agents).
Antibiotic prophylaxis
Antistreptococcal prophylaxis should be maintained continuously after the initial episode of acute rheumatic fever to prevent recurrences. Antibiotics taken orally are slightly less effective as those given by injection. However, with the oral route, painful injections are avoided, and clinic visits and observation for postinjection reactions are not needed.
The optimal duration of antistreptococcal prophylaxis is uncertain. Children without carditis should receive prophylaxis for 5 years or until age 21 (whichever is longer). The American Heart Association and the American Academy of Pediatrics both recommend that patients with carditis without evidence of residual heart damage receive prophylaxis for 10 years or until age 21 (whichever is longer) 66. Children with carditis and evidence of residual heart damage should receive prophylaxis for > 10 years; many experts recommend that such patients continue prophylaxis indefinitely or, alternatively, until age 40. Prophylaxis should be life long in all patients with severe valvular disease who have close contact with young children because young children have a high rate of GAS carriage.
The standard regimen for prophylaxis against recurrent group A Streptococcus infection is penicillin G benzathine IM every 3 to 4 weeks. In parts of the world with high acute rheumatic fever endemicity, IM prophylaxis every 3 weeks is superior to every 4 weeks. Alternatives (eg, for patients unwilling to receive injections) are penicillin V or sulfadiazine or sulfisoxazole orally every day. For patients who are proved to be allergic to penicillin and sulfa, alternatives are erythromycin or azithromycin orally every day.
The American Heart Association no longer recommends that patients with known or suspected rheumatic valvular disease take short-term antibiotic prophylaxis against bacterial endocarditis for dental or oral surgical procedures unless they have an indwelling prosthetic valve 66.
Risk factors for serious Streptococcus pyogenes infections
Some people are generally at increased risk of getting a serious Streptococcus pyogenes or group A strep infection:
- Viral infections, like flu or chickenpox, can increase this risk.
- Medical conditions that can increase the risk for getting a serious group A strep infection include:
- Cancer
- Chronic heart, kidney, liver, or lung disease
- Diabetes
- Immunocompromising condition (having a weakened immune system)
- Obesity
- Wounds or skin disease
Other groups at increased risk for getting a serious Streptococcus pyogenes or group A strep infection include:
- American Indian, Alaska Native, Native Hawaiian, and Pacific Island populations
- People aged 65 years or older
- People who inject drugs or who are experiencing homelessness
- Residents of long-term care facilities.
Crowded conditions can increase the risk of getting strep throat, scarlet fever, or impetigo. Thus, these settings can increase the risk for rheumatic fever if those infections aren’t treated properly. These settings include:
- Daycare centers and schools
- Detention or correctional facilities
- Homeless shelters
- Military training facilities.
Streptococcus pyogenes prevention
People can get infected with Streptococcus pyogenes or group A Streptococcus (group A strep bacteria) more than once. There’s no vaccine to prevent group A strep infections.
Group A strep prevention activities vary by disease, but generally focus on three important goals 67:
- Limit exposure and spread of bacteria
- Treat group A strep infections
- Use preventive antibiotics when appropriate
Limit exposure and spread of Streptococcus pyogenes bacteria
Many daily healthy habits can help prevent Streptococcus pyogenes infections:
- Care for fungal infections
- Clean and care for wounds
- Cover coughs and sneezes
- Wash glasses, utensils, and plates after someone who’s sick uses them
- Wash hands often
Take extra measures for impetigo:
- Wash body and hair often with soap and clean, running water
- Wash the clothes, linens, and towels of anyone with impetigo every day
- Don’t share clothes, linens, or towels with anyone who has impetigo.
After items (dishes, linens) have been washed, they’re safe for others to use.
Wound care
- Step 1: Wash hands with soap and water or use an alcohol-based hand rub if washing isn’t possible.
- Step 2: Clean all minor cuts and injuries that break the skin (like blisters and scrapes) with soap and water.
- Step 3: After cleaning, cover draining or open wounds with clean, dry bandages until they heal.
Protect wounds and infections
If you have an open wound or skin infection, avoid spending time in:
- Hot tubs
- Natural bodies of water (e.g., lakes, rivers, oceans)
- Swimming pools
Treat infections
Take antibiotics, if prescribed. Antibiotics treat the infection and help prevent serious complications, like rheumatic fever. They also prevent Streptococcus pyogenes bacteria from spreading to others.
Use preventive antibiotics when appropriate. Close contacts of someone with a group A strep infection generally don’t get antibiotics to prevent them from getting sick. People who live together are examples of close contacts. However, rheumatic fever and serious infections are important exceptions.
Rheumatic fever
Preventive antibiotics help protect people with rheumatic fever from getting it again. They may need preventive antibiotics over a period of many years (often until 21 years old). Preventive antibiotics can include daily antibiotics by mouth or a shot into the muscle every few weeks.
Serious infections
Three infections caused by group A strep bacteria can be very serious and even deadly:
- Cellulitis
- Necrotizing fasciitis
- Streptococcal toxic shock syndrome
For patients with a serious infection, doctors may give antibiotics to close contacts if they:
- Are 65 years or older
- Have other factors that increase their risk of getting a serious group A strep infection
Streptococcus pyogenes symptoms
Symptoms of Streptococcus pyogenes infection vary depending on the infection site but commonly include fever, sore throat, swollen neck glands, and fatigue. Other signs can include a red and sandpaper-like rash, a “strawberry tongue” or symptoms of a skin infection like cellulitis or impetigo. More severe symptoms can include headache, nausea, vomiting, and severe muscle aches.
- Strep Throat:
- Sudden sore throat, especially with pain when swallowing
- Fever
- White or yellow spots on the tonsils or throat
- Swollen, tender lymph nodes in the neck
- Fatigue
- Loss of appetite
- Scarlet Fever (a complication of strep throat):
- A fine, red rash that feels like sandpaper and starts on the chest and abdomen
- Flushed face with paleness around the mouth
- A red, bumpy “strawberry tongue”
- Skin peeling on fingers and toes after the rash fades
- Invasive Group A Strep (iGAS):
- Fever
- Severe muscle aches
- Nausea and vomiting
- Shortness of breath
- Severe headache
- Cellulitis: Redness, swelling, and warmth at the site of a skin wound
- Impetigo: Itchy, reddish rash that can form fluid-filled blisters which break and form a crusty, honey-colored scab often appears around the mouth and nose
Streptococcus pyogenes diagnosis
Streptococcus pyogenes diagnosis typically involves a rapid antigen test on a throat swab, which provides a quick result 6, 7. A positive result is definitive, but a negative result in children and adolescents should be confirmed with a throat culture, which is the “gold standard” for diagnosis 6, 7. Other methods include blood cultures for invasive infections or serologic tests to diagnose past infections like rheumatic fever.
Streptococcus pyogenes diagnostic methods
- Rapid antigen detection test (RADT): A swab from the throat is used to quickly detect Streptococcus pyogenes antigens. A positive result is immediate and accurate. The rapid antigen detection test (RADT) has a sensitivity of approximately 85% in children, although variability exists, while its specificity is stable at 95% 8. Due to the high specificity of the rapid antigen detection test (RADT) in children, antibiotic therapy is recommended without the need for further throat culture to distinguish infection from carriage. If the rapid antigen detection test (RADT) result is negative, treatment decisions depend on national guidelines 8. In the United States, however, in adults, due to the low general rate of Streptococcus pyogenes pharyngitis and corresponding low pretest probability, a negative RADT does not require confirmatory culture. A negative rapid swab result confers an extremely low post-test probability of group A beta-hemolytic streptococci infection 9, 10. For other sites of infection, whether superficial or deep (such as skin, blood, wound, or lung), performing a Gram stain and cultures are the appropriate diagnostic methods. Polymerase chain reaction (PCR) can also be used to identify specific group A beta-hemolytic streptococci strains, particularly in complicated cases 11.
- Throat culture: Throat culture (i.e., a swab rubbed on both tonsillar pillars, avoiding the lips and tongue) is the “gold standard” for confirming a strep infection. A throat swab is sent to a lab and cultured on a blood agar plate, which facilitates the easy identification of beta-hemolytic colonies. Group A Streptococcus (GAS) grows easily on sheep blood agar and is catalase- and oxidase-negative. Confirmatory identification is achieved through Lancefield grouping and, more recently, techniques such as matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) 12, 13. However, culture results typically take 24 hours or longer, which delays critical information needed for treatment, isolation, and epidemiological purposes.
- Molecular tests: Nucleic acid amplification tests (NAATs) or other molecular methods can be used to detect Streptococcus pyogenes from various specimens, including throat swabs, blood, or other body fluids.
- Serologic tests: These are used for retrospective diagnosis of post-streptococcal diseases, such as acute rheumatic fever or glomerulonephritis, by detecting antibodies to streptococcal antigens. These are not useful for diagnosing an acute infection.
- Other specimens: For invasive infections, samples from sterile sites like blood, cerebrospinal fluid, or joint fluid can be tested via culture or molecular methods. For skin infections, an aspirate from the edge of the lesion may be used.
- Bacitracin susceptibility: Streptococcus pyogenes can be differentiated from other non-group A beta-hemolytic streptococci by their increased sensitivity to bacitracin. The bacitracin test, along with the Lancefield antigen A test, is used for greater specificity in the identification of Streptococcus pyogenes, since other beta-hemolytic strains of streptococci may contain the group A antigen are resistant to bacitracin. The bacitracin test is also used to distinguish Streptococcus pyogenes from other beta-hemolytic streptococci that are PYR-positive, such as S. iniae and S. porcinus. To perform a bacitracin susceptibility test, it is important to make a subculture of the strain to be tested on a sheep blood agar plate (SBA), since placing the bacitracin disc on a primary plate could give variable results. The strain being tested is streaked with several individual colonies of a pure culture on an SBA agar plate and a disk containing 0.04 U of bacitracin is placed on the SBA plate. After overnight incubation at 35°C in 5% CO2, a zone of inhibition surrounding the disc indicates the susceptibility of the strain. It is noteworthy that bacitracin-resistant strains of S. pyogenes have been observed in a number of European countries; however, bacitracin resistance has not yet been reported in the US to date 14, 15, 16.
Streptococcus pyogenes treatment
Treatment for Streptococcus pyogenes involves antibiotics, with the specific medication and duration depending on the infection’s location and severity. Common options include oral penicillin or amoxicillin for less severe infections like strep throat, while intravenous (IV) antibiotics like vancomycin or clindamycin are used for severe or invasive infections. Penicillin continues to be the gold standard for group A beta-hemolytic streptococci treatment 17. For patients with penicillin allergies, macrolides (e.g, erythromycin) and lincosamides (e.g, clindamycin) are notable alternatives 18. However, resistance to these antibiotics has increased in the past decade, with variable prevalence of resistant group A beta-hemolytic streptococci strains worldwide 19. While reports of antibiotic resistance to penicillins and increased minimal inhibitory concentrations (MICs) to penicillin and cephalosporins have emerged primarily due to mutations in the peptidoglycan synthetic enzyme pbp2x gene, resistance rates remain low 20.
A full course of antibiotics must be completed to prevent complications and reduce the spread of bacteria, even if you start feeling better. You should see your doctor if your symptoms don’t improve after 48 hours of antibiotic treatment.
Infection control:
- You should stay home from school, work, or daycare for at least 24 hours after starting antibiotic treatment to prevent the spread of infection.
Prophylactic antibiotics:
- Doctors may recommend a course of antibiotics for close contacts of individuals with invasive group A streptococcal infections to reduce their risk of becoming ill.
Streptococcus pyogenes treatment based on infection type
- Streptococcal pharyngitis (strep throat): Oral antibiotics such as penicillin or amoxicillin are commonly prescribed for 10 days.
- Streptococcus pyogenes skin infections (e.g., impetigo, cellulitis): A semi-synthetic penicillinase-resistant penicillin is often used. For patients with severe skin infections, intravenous antibiotics may be required initially, followed by oral medication, and in some cases, surgical debridement of necrotic tissue.
- Invasive group A streptococcal disease (iGAS): These severe infections require urgent treatment, often in a hospital, with intravenous antibiotics such as vancomycin or clindamycin. Other supportive therapies and intensive care may also be needed.
Streptococcus pyogenes prognosis
Generally, simple, noninvasive group A beta-hemolytic streptococci infections have low morbidity and mortality rates, with patients experiencing good outcomes 18. However, more invasive and severe group A beta-hemolytic streptococci infections carry significant morbidity and mortality. Invasive group A streptococcal (iGAS) infections are associated with more severe conditions, such as necrotizing fasciitis also called “flesh-eating disease” and streptococcal toxic shock syndrome (STSS) also called streptococcus pyogenes toxic shock syndrome, have a higher risk of ICU admission compared to other group A beta-hemolytic streptococci strains. Streptococcal toxic shock syndrome has a mortality rate of 5% to 10%, particularly in patients at the extremes of age or those with preexisting conditions. Mortality rate for streptococcal toxic shock syndrome (STSS) is approximately 28% in children 38 and up to 45% in adults 34, and highest in patients presenting with necrotizing fasciitis. When necrotizing fasciitis occurs alongside streptococcal toxic shock syndrome (STSS), the mortality rate can reach up to 60% 68, 69.
- Kanwal S, Vaitla P. Streptococcus Pyogenes. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554528[↩]
- Streptococcal Infections. https://www.msdmanuals.com/professional/infectious-diseases/gram-positive-cocci/streptococcal-infections[↩]
- Streptococcal Infections. https://www.msdmanuals.com/home/infections/bacterial-infections-gram-positive-bacteria/streptococcal-infections[↩]
- Streptococcus pyogenes. https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases/streptococcus-pyrogenes[↩]
- Brouwer, S., Rivera-Hernandez, T., Curren, B.F. et al. Pathogenesis, epidemiology and control of Group A Streptococcus infection. Nat Rev Microbiol 21, 431–447 (2023). https://doi.org/10.1038/s41579-023-00865-7[↩]
- Spellerberg B, Brandt C. Laboratory Diagnosis of Streptococcus pyogenes (group A streptococci) 2016 Feb 10. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes : Basic Biology to Clinical Manifestations [Internet]. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2016-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK343617[↩][↩][↩][↩]
- Wessels MR. Streptococcus pyogenes Pharyngitis and Scarlet Fever. 2022 Sep 5 [Updated 2022 Oct 4]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. 2nd edition. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2022 Oct 8. Chapter 22. Available from: https://www.ncbi.nlm.nih.gov/books/NBK587104[↩][↩][↩][↩]
- Cohen JF, Bertille N, Cohen R, Chalumeau M. Rapid antigen detection test for group A streptococcus in children with pharyngitis. Cochrane Database Syst Rev. 2016 Jul 4;7(7):CD010502. doi: 10.1002/14651858.CD010502.pub2[↩][↩][↩][↩]
- Schroeder BM. Diagnosis and management of group A streptococcal pharyngitis. Am Fam Physician. 2003 Feb 15;67(4):880, 883-4. https://www.aafp.org/pubs/afp/issues/2003/0215/p880.html[↩][↩][↩]
- Stevens DL. Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment. Emerg Infect Dis. 1995 Jul-Sep;1(3):69-78. https://pmc.ncbi.nlm.nih.gov/articles/instance/2626872/pdf/8903167.pdf[↩][↩]
- Liu D, Hollingshead S, Swiatlo E, Lawrence ML, Austin FW. Rapid identification of Streptococcus pyogenes with PCR primers from a putative transcriptional regulator gene. Res Microbiol. 2005 May;156(4):564-7. doi: 10.1016/j.resmic.2005.01.010[↩][↩]
- Gera K, McIver KS. Laboratory growth and maintenance of Streptococcus pyogenes (the Group A Streptococcus, GAS). Curr Protoc Microbiol. 2013 Oct 2;30:9D.2.1-9D.2.13. doi: 10.1002/9780471729259.mc09d02s30[↩][↩]
- Wang J, Zhou N, Xu B, Hao H, Kang L, Zheng Y, Jiang Y, Jiang H. Identification and cluster analysis of Streptococcus pyogenes by MALDI-TOF mass spectrometry. PLoS One. 2012;7(11):e47152. doi: 10.1371/journal.pone.0047152[↩][↩]
- Malhotra-Kumar S, Wang S, Lammens C, Chapelle S, Goossens H. Bacitracin-resistant clone of Streptococcus pyogenes isolated from pharyngitis patients in Belgium. J Clin Microbiol. 2003 Nov;41(11):5282-4. doi: 10.1128/JCM.41.11.5282-5284.2003[↩][↩]
- Mihaila-Amrouche L, Bouvet A, Loubinoux J. Clonal spread of emm type 28 isolates of Streptococcus pyogenes that are multiresistant to antibiotics. J Clin Microbiol. 2004 Aug;42(8):3844-6. doi: 10.1128/JCM.42.8.3844-3846.2004[↩][↩]
- James L, McFarland RB. An epidemic of pharyngitis due to a nonhemolytic group A streptococcus at lowry air force base. N Engl J Med. 1971 Apr 8;284(14):750-2. doi: 10.1056/NEJM197104082841403[↩][↩]
- Yu D, Zheng Y, Yang Y. Is There Emergence of β-Lactam Antibiotic-Resistant Streptococcus pyogenes in China? Infect Drug Resist. 2020 Jul 14;13:2323-2327. doi: 10.2147/IDR.S261975[↩][↩]
- Newberger R, Hollingshead CM. Group A Streptococcal Infections. [Updated 2025 Jan 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559240[↩][↩][↩]
- Rafei R, Al Iaali R, Osman M, Dabboussi F, Hamze M. A global snapshot on the prevalent macrolide-resistant emm types of Group A Streptococcus worldwide, their phenotypes and their resistance marker genotypes during the last two decades: A systematic review. Infect Genet Evol. 2022 Apr;99:105258. doi: 10.1016/j.meegid.2022.105258[↩][↩]
- Macris MH, Hartman N, Murray B, Klein RF, Roberts RB, Kaplan EL, Horn D, Zabriskie JB. Studies of the continuing susceptibility of group A streptococcal strains to penicillin during eight decades. Pediatr Infect Dis J. 1998 May;17(5):377-81. doi: 10.1097/00006454-199805000-00006[↩][↩]
- Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012 Nov 15;55(10):1279-82. doi: 10.1093/cid/cis847. Erratum in: Clin Infect Dis. 2014 May;58(10):1496. Dosage error in article text.[↩][↩][↩]
- Pardo S, Perera TB. Scarlet Fever. [Updated 2025 Feb 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507889[↩]
- Wang HC, Lau CI, Lin CC, Chang A, Kao CH. Group A Streptococcal Infections Are Associated With Increased Risk of Pediatric Neuropsychiatric Disorders: A Taiwanese Population-Based Cohort Study. J Clin Psychiatry. 2016 Jul;77(7):e848-54. doi: 10.4088/JCP.14m09728[↩]
- Yung CF, Thoon KC. A 12 year outbreak of scarlet fever in Singapore. Lancet Infect Dis. 2018 Sep;18(9):942. doi: 10.1016/S1473-3099(18)30464-X[↩]
- Brown BD, Hood Watson KL. Cellulitis. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549770[↩][↩]
- About Cellulitis. https://www.cdc.gov/group-a-strep/about/cellulitis.html[↩][↩]
- Cellulitis. https://www.msdmanuals.com/professional/dermatologic-disorders/bacterial-skin-infections/cellulitis[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. J Infect. 2012 Feb;64(2):148-55. doi: 10.1016/j.jinf.2011.11.004[↩]
- Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37. doi: 10.1001/jama.2016.8825[↩][↩]
- Brindle R, Williams OM, Barton E, Featherstone P. Assessment of Antibiotic Treatment of Cellulitis and Erysipelas: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019 Sep 1;155(9):1033-1040. doi: 10.1001/jamadermatol.2019.0884[↩]
- Obaitan I, Dwyer R, Lipworth AD, Kupper TS, Camargo CA Jr, Hooper DC, Murphy GF, Pallin DJ. Failure of antibiotics in cellulitis trials: a systematic review and meta-analysis. Am J Emerg Med. 2016 Aug;34(8):1645-52. doi: 10.1016/j.ajem.2016.05.064[↩]
- Richmond JM, Harris JE. Immunology and skin in health and disease. Cold Spring Harb Perspect Med. 2014 Dec 1;4(12):a015339. doi: 10.1101/cshperspect.a015339[↩]
- Necrotizing Soft-Tissue Infection. https://www.msdmanuals.com/professional/dermatologic-disorders/bacterial-skin-infections/necrotizing-soft-tissue-infection[↩][↩][↩][↩][↩][↩][↩][↩]
- Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. N Engl J Med. 2017 Dec 7;377(23):2253-2265. doi: 10.1056/NEJMra1600673[↩][↩][↩][↩]
- About Necrotizing Fasciitis. https://www.cdc.gov/group-a-strep/about/necrotizing-fasciitis.html[↩][↩]
- Hua C, Urbina T, Bosc R, Parks T, Sriskandan S, de Prost N, Chosidow O. Necrotising soft-tissue infections. Lancet Infect Dis. 2023 Mar;23(3):e81-e94. doi: 10.1016/S1473-3099(22)00583-7[↩]
- Toxic Shock Syndrome (TSS). https://www.msdmanuals.com/professional/infectious-diseases/gram-positive-cocci/toxic-shock-syndrome-tss[↩][↩][↩][↩]
- Adalat S, Dawson T, Hackett SJ, Clark JE; In association with the British Paediatric Surveillance Unit. Toxic shock syndrome surveillance in UK children. Arch Dis Child. 2014 Dec;99(12):1078-82. doi: 10.1136/archdischild-2013-304741[↩][↩]
- Lappin E, Ferguson AJ. Gram-positive toxic shock syndromes. Lancet Infect Dis. 2009 May;9(5):281-90. doi: 10.1016/S1473-3099(09)70066-0[↩]
- Atchade E, De Tymowski C, Grall N, Tanaka S, Montravers P. Toxic Shock Syndrome: A Literature Review. Antibiotics (Basel). 2024 Jan 18;13(1):96. doi: 10.3390/antibiotics13010096[↩]
- Parks T, Wilson C, Curtis N, Norrby-Teglund A, Sriskandan S. Polyspecific Intravenous Immunoglobulin in Clindamycin-treated Patients With Streptococcal Toxic Shock Syndrome: A Systematic Review and Meta-analysis. Clin Infect Dis. 2018 Oct 15;67(9):1434-1436. doi: 10.1093/cid/ciy401[↩]
- Weiss S, Holtfreter S, Meyer TC, Schmiedeke F, Cammann C, Dörr M, Felix SB, Grabe HJ, Homuth G, Kohler C, Mahncke C, Michalik S, Nauck M, Friedrich N, Samietz S, Völzke H, Völker U, Bröker BM. Toxin exposure and HLA alleles determine serum antibody binding to toxic shock syndrome toxin 1 (TSST-1) of Staphylococcus aureus. Front Immunol. 2023 Sep 4;14:1229562. doi: 10.3389/fimmu.2023.1229562[↩]
- Postinfectious Glomerulonephritis (PIGN). https://www.msdmanuals.com/professional/genitourinary-disorders/glomerular-disorders/postinfectious-glomerulonephritis-pign[↩][↩]
- Sainato RJ, Weisse ME. Poststreptococcal Glomerulonephritis and Antibiotics: A Fresh Look at Old Data. Clinical Pediatrics. 2018;58(1):10-12. doi:10.1177/0009922818793345[↩]
- Bateman E, Mansour S, Okafor E, Arrington K, Hong BY, Cervantes J. Examining the Efficacy of Antimicrobial Therapy in Preventing the Development of Postinfectious Glomerulonephritis: A Systematic Review and Meta-Analysis. Infect Dis Rep. 2022 Mar 7;14(2):176-183. doi: 10.3390/idr14020022[↩]
- Rodriguez-Iturbe B, Haas M. Post-Streptococcus pyogenes Glomerulonephritis. 2022 Sep 9 [Updated 2022 Oct 4]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. 2nd edition. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2022 Oct 8. Chapter 27. Available from: https://www.ncbi.nlm.nih.gov/books/NBK587117[↩]
- Melby PC, Musick WD, Luger AM, Khanna R. Poststreptococcal glomerulonephritis in the elderly. Report of a case and review of the literature. Am J Nephrol. 1987;7(3):235-40. doi: 10.1159/000167471[↩]
- Pinto SW, Sesso R, Vasconcelos E, Watanabe YJ, Pansute AM. Follow-up of patients with epidemic poststreptococcal glomerulonephritis. Am J Kidney Dis. 2001 Aug;38(2):249-55. doi: 10.1053/ajkd.2001.26083[↩]
- Pinto SW, do Nascimento Lima H, de Abreu TT, Otoni A, Koch Nogueira PC, Sesso R. Twenty-year Follow-up of Patients With Epidemic Glomerulonephritis due to Streptococcus zooepidemicus in Brazil. Kidney Int Rep. 2022 Jun 30;7(9):2029-2038. doi: 10.1016/j.ekir.2022.06.011[↩]
- Vogl W, Renke M, Mayer-Eichberger D, Schmitt H, Bohle A. Long-term prognosis for endocapillary glomerulonephritis of poststreptococcal type in children and adults. Nephron. 1986;44(1):58-65. doi: 10.1159/000183913[↩]
- Mezzano S, Lopez MI, Olavarria F, Ardiles L, Arriagada A, Elgueta S, Wegman ME, Fuentes C. Age influence on mononuclear phagocyte system Fc-receptor function in poststreptococcal nephritis. Nephron. 1991;57(1):16-22. doi: 10.1159/000186209[↩]
- Vernon KA, Goicoechea de Jorge E, Hall AE, Fremeaux-Bacchi V, Aitman TJ, Cook HT, Hangartner R, Koziell A, Pickering MC. Acute presentation and persistent glomerulonephritis following streptococcal infection in a patient with heterozygous complement factor H-related protein 5 deficiency. Am J Kidney Dis. 2012 Jul;60(1):121-5. doi: 10.1053/j.ajkd.2012.02.329[↩]
- Sethi S, Fervenza FC, Zhang Y, Zand L, Meyer NC, Borsa N, Nasr SH, Smith RJ. Atypical postinfectious glomerulonephritis is associated with abnormalities in the alternative pathway of complement. Kidney Int. 2013 Feb;83(2):293-9. doi: 10.1038/ki.2012.384[↩]
- Rheumatic Fever. https://www.msdmanuals.com/professional/pediatrics/miscellaneous-bacterial-infections-in-infants-and-children/rheumatic-fever[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Chowdhury MDS, Koziatek CA, Tristram D, et al. Acute Rheumatic Fever. [Updated 2025 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK594238[↩][↩]
- Karthikeyan G, Guilherme L. Acute rheumatic fever. Lancet. 2018 Jul 14;392(10142):161-174. doi: 10.1016/S0140-6736(18)30999-1. Epub 2018 Jun 29. Erratum in: Lancet. 2018 Sep 8;392(10150):820. doi: 10.1016/S0140-6736(18)32057-9[↩][↩]
- About Rheumatic Fever. https://www.cdc.gov/group-a-strep/about/rheumatic-fever.html[↩]
- Carapetis JR. Rheumatic heart disease in developing countries. N Engl J Med. 2007 Aug 2;357(5):439-41. doi: 10.1056/NEJMp078039[↩]
- Tibazarwa KB, Volmink JA, Mayosi BM. Incidence of acute rheumatic fever in the world: a systematic review of population-based studies. Heart. 2008 Dec;94(12):1534-40. doi: 10.1136/hrt.2007.141309[↩]
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990-2015. N Engl J Med. 2017 Aug 24;377(8):713-722. doi: 10.1056/NEJMoa1603693[↩]
- Carapetis JR, Beaton A, Cunningham MW, Guilherme L, Karthikeyan G, Mayosi BM, Sable C, Steer A, Wilson N, Wyber R, Zühlke L. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers. 2016 Jan 14;2:15084. doi: 10.1038/nrdp.2015.84[↩]
- Sable C. Update on Prevention and Management of Rheumatic Heart Disease. Pediatr Clin North Am. 2020 Oct;67(5):843-853. doi: 10.1016/j.pcl.2020.06.003[↩]
- Gewitz MH, Baltimore RS, Tani LY, et al: Revision of Jones criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: A scientific statement from the American Heart Association. Circulation 131:1806–1818, 2015. doi: 10.1161/CIR.0000000000000205[↩]
- Scheel A, Beaton AZ, Katzenellenbogen J, Parks T, Miller KM, Cherian T, Van Beneden CA, Cannon JW, Moore HC, Bowen AC, Carapetis JR. Standardization of Epidemiological Surveillance of Acute Rheumatic Fever. Open Forum Infect Dis. 2022 Sep 15;9(Suppl 1):S41-S49. doi: 10.1093/ofid/ofac252[↩]
- Gewitz MH, Baltimore RS, Tani LY, et al. American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation. 2015 May 19;131(20):1806-18. doi: 10.1161/CIR.0000000000000205. Epub 2015 Apr 23. Erratum in: Circulation. 2020 Jul 28;142(4):e65. doi: 10.1161/CIR.0000000000000889[↩]
- Gerber MA, Baltimore RS, Eaton CB, Gewitz M, Rowley AH, Shulman ST, Taubert KA. Prevention of rheumatic fever and diagnosis and treatment of acute Streptococcal pharyngitis: a scientific statement from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, the Interdisciplinary Council on Functional Genomics and Translational Biology, and the Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Academy of Pediatrics. Circulation. 2009 Mar 24;119(11):1541-51. doi: 10.1161/CIRCULATIONAHA.109.191959[↩][↩]
- Preventing Group A Strep Infection. https://www.cdc.gov/group-a-strep/prevention/index.html[↩]
- Schmitz M, Roux X, Huttner B, Pugin J. Streptococcal toxic shock syndrome in the intensive care unit. Ann Intensive Care. 2018 Sep 17;8(1):88. doi: 10.1186/s13613-018-0438-y[↩]
- Stevens DL. Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment. Emerg Infect Dis. 1995 Jul-Sep;1(3):69-78. doi: 10.3201/eid0103.950301[↩]

{kind=link}