Contents
- In-vitro fertilization
- In vitro fertilization clinic near me
- In vitro fertilization risks
- In-vitro fertilization contraindications
- In-vitro fertilization process
- In-vitro fertilization success rates
- In-vitro fertilization cost
- When to end IVF treatment?
In-vitro fertilization
In vitro fertilization also called “IVF” is the most common type of assisted reproductive technology (ART) which is a complex series of treatments, procedures and techniques to treat infertility. Infertility is defined as no becoming pregnant after 12 months of unprotected sexual intercourse in women less than 35 or six months in women 35 years or older 1. IVF also can be used to prevent passing on genetic problems to a child. In vitro fertilization (IVF) is a treatment for infertility or genetic problems. IVF is the most effective type of fertility treatment that involves the handling of eggs or embryos and sperm. Together, this group of treatments is called assisted reproductive technology (ART). “In vitro” is Latin for “in glass”, “in a test tube”, “culture dish” or elsewhere outside a living organism. During in-vitro fertilization (IVF), mature eggs are collected from your ovaries and fertilized by sperm in a petri dish. Then a procedure is done to place one or more of the fertilized eggs, called embryos, in a uterus, which is where babies develop. One full cycle of in-vitro fertilization (IVF) takes about 2 to 3 weeks. Sometimes these steps are split into different parts and the process can take longer.
Dr. Robert Edwards and Dr. Patrick Steptoe reported the first “test tube baby” from IVF in July 1978 in England 2. In 2010, Dr. Robert Edwards was awarded the Nobel Prize in Medicine for his pioneering work in the development of in vitro fertilization to help couples overcome infertility 3. IVF now accounts for 1.6% and 4.5% of all live births in the United States and Europe, respectively 4. Initially developed as a way to bypass irreparable tubal disease, IVF is now widely applied for the treatment of infertility due to a variety of causes, including endometriosis, male factor, and unexplained infertility 5. Women who cannot use their own eggs (oocytes) due to primary ovarian insufficiency (POI) or age-related decline in oocyte number can now become successfully pregnant utilizing donor egg IVF.
IVF can be done using a couple’s own eggs and sperm. Or it may involve eggs, sperm or embryos from a known or unknown donor. In some cases, a gestational carrier — someone who has an embryo implanted in the uterus — might be used. Women who don’t have a working uterus or for whom pregnancy poses a serious health risk might choose IVF using another woman to carry the pregnancy. The person is called a gestational carrier. In this case, your eggs are fertilized with sperm, but the embryos that result are placed in the gestational carrier’s uterus.
Your chances of having a healthy baby using IVF depend on many factors, such as your age and the cause of your infertility. What’s more, IVF involves getting procedures that can be time-consuming, expensive and invasive. If more than one embryo is placed in the uterus, it can result in a pregnancy with more than one baby. This is called a multiple pregnancy.
Before you have IVF to treat infertility, you and your partner might be able to try other treatment options that involve fewer or no procedures that enter your body. For example, fertility drugs can help your ovaries make more eggs. And a procedure called intrauterine insemination (IUI) places sperm directly in the uterus near the time when an ovary releases an egg called ovulation. Intrauterine insemination (IUI) is an infertility treatment that is sometimes referred to as “artificial insemination”. During intrauterine insemination (IUI), specially prepared sperm are inserted into the woman’s uterus. Intrauterine insemination (IUI) may be recommended for couples in which the male has close to normal sperm count and motility (movement) and the ability to produce a semen sample in the office (or, under some circumstances, at home) and the woman has open, functioning fallopian tubes.
Sometimes, IVF is offered as a main treatment for infertility in people over the age of 40. It also can be done if you have certain health conditions. For example, IVF may be an option if you or your partner has:
- Fallopian tube damage or blockage. Eggs move from the ovaries to the uterus through the fallopian tubes. If both tubes get damaged or blocked, that makes it hard for an egg to be fertilized or for an embryo to travel to the uterus.
- Ovulation disorders. If ovulation doesn’t happen or doesn’t occur often, fewer eggs are available to be fertilized by sperm.
- Endometriosis. This condition happens when tissue that’s like the lining of the uterus grows outside of the uterus. Endometriosis often affects the ovaries, uterus and fallopian tubes.
- Uterine fibroids. Fibroids are tumors in the uterus. Most often, they’re not cancer. They’re common in people in their 30s and 40s. Fibroids can cause a fertilized egg to have trouble attaching to the lining of the uterus.
- Previous surgery to prevent pregnancy. An operation called tubal ligation involves having the fallopian tubes cut or blocked to prevent pregnancy for good. If you wish to conceive after tubal ligation, IVF may help. It might be an option if you don’t want or can’t get surgery to reverse tubal ligation.
- Issues with sperm. A low number of sperm or unusual changes in their movement, size or shape can make it hard for sperm to fertilize an egg. If medical tests find issues with sperm, a visit to an infertility specialist might be needed to see if there are treatable problems or other health concerns.
- Unexplained infertility. This is when tests can’t find the reason for someone’s infertility.
- A genetic disorder. If you or your partner is at risk of passing on a genetic disorder to your child, your health care team might recommend getting a procedure that involves IVF. It’s called preimplantation genetic testing. After the eggs are harvested and fertilized, they’re checked for certain genetic problems. Still, not all of these disorders can be found. Embryos that don’t appear to contain a genetic problem can be placed in the uterus.
- A desire to preserve fertility due to cancer or other health conditions. Cancer treatments such as radiation or chemotherapy can harm fertility. If you’re about to start treatment for cancer, IVF could be a way to still have a baby in the future. Eggs can be harvested from their ovaries and frozen for later use. Or the eggs can be fertilized and frozen as embryos for future use.
Your reproductive endocrinologist (a doctor who specializes in managing infertility) can help you understand how IVF works, what the risks are and whether it’s right for you.
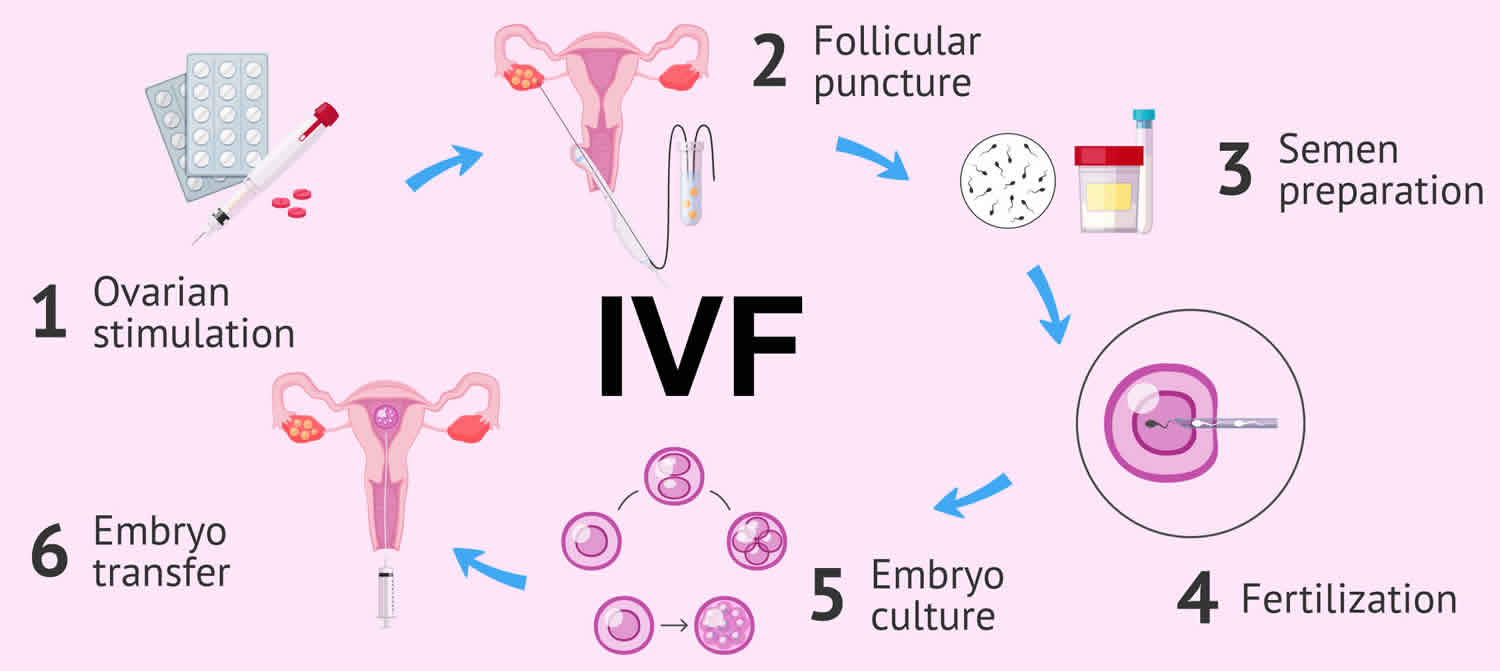
Figure 1. In vitro fertilization (IVF)
What causes infertility in men?
Infertility in men can be caused by disruption of testicular or ejaculatory function, as well as by hormonal and genetic disorders. It is typically evaluated by a semen analysis, complete medical history, and physical examination. This assessment helps determine if and how male factors are contributing to infertility. A semen analysis assesses the number (concentration), motility (movement), and morphology (shape) of sperm. The results are then evaluated by a specialist. If semen is found to be slightly abnormal, it does not necessarily mean that a man is infertile.
Disruption of testicular or ejaculatory function. Some conditions that can disrupt testicular or ejaculatory function include the following:
- Varicocele is a condition in which the veins in the testicles are enlarged, which may affect the number or shape of the sperm.
- Trauma to the testes may affect sperm production and result in lower number of sperm.
- Unhealthy habits, such as heavy alcohol use, smoking, anabolic steroid use, and illicit drug use, may decrease sperm production.
- Cancer treatment involving the use of certain types of chemotherapy, radiation, or surgery to remove one or both testicles may affect sperm production or the ability of sperm to fertilize an egg.
- Medical conditions such as diabetes, cystic fibrosis, certain types of autoimmune disorders, and certain types of infections may cause testicular failure.
Hormonal disorders. Improper function of the hypothalamus or pituitary glands are hormonal disorders that can cause infertility. These glands produce hormones that maintain normal testicular function. Too much of these hormones, especially prolactin, can result in infertility. Other conditions that damage or impair the hypothalamus or the pituitary gland may also result in low or no sperm production.
Examples of hormonal disorders include:
- Malignant (cancerous) pituitary tumors
- Congenital adrenal hyperplasia (CAH)
- Exposure to too much estrogen
- Exposure to too much testosterone
- Cushing’s syndrome
- Chronic use of medications called glucocorticoids
Genetic disorders. Genetic conditions can cause no sperm or low numbers of sperm to be produced.
Examples of genetic disorders include:
- Klinefelter’s syndrome
- Y-chromosome microdeletion
- Myotonic dystrophy
Men’s fertility is also known to decline with:
- Age. Couples in which the male partner is 40 or older are more likely to report difficulty conceiving.
- Having overweight or obesity.
- Smoking.
- Excessive use of alcohol or drug use (such as opioids or marijuana).
- A history of trauma to the testes.
- Exposure to testosterone, radiation, certain medicines, or certain environmental toxins.
- Frequent exposure of the testes to high temperatures.
What causes infertility in women?
Women need functioning ovaries, fallopian tubes, and a uterus to get pregnant. Conditions affecting any one of these organs can contribute to female infertility 7.
Disruption of ovarian function. A woman’s menstrual cycle is on average 28 days long. Regular, predictable periods that occur every 21 to 35 days likely reflect ovulation. A woman with irregular periods is likely not ovulating. Ovulation can be predicted by using an ovulation test or blood test. Disruption in ovarian function may be caused by several conditions and calls for an evaluation by a health care provider. No single test is a perfect predictor of fertility, but there are tests for common markers of ovarian function. These include follicle-stimulating hormone (FSH), anti-müllerian hormone (AMH), and antral follicle count (AFC) tests. Some conditions that may cause issues related to ovarian function include the following:
- Polycystic ovary syndrome (PCOS) is the most common cause of infertility. PCOS is a condition that causes women to not ovulate, or to ovulate irregularly.
- Diminished ovarian reserve is a condition where there are fewer eggs remaining in the ovaries than expected at a specific age. Diminished ovarian reserve can be due to congenital, medical, surgical, or unexplained causes.
- Impaired function of the hypothalamus and pituitary glands can affect ovarian function. If impaired, these glands can cause too much of the hormones that maintain normal ovarian function to be produced.
- Functional hypothalamic amenorrhea (FHA) is a condition that can affect ovarian function. It can be caused by excessive exercise, weight loss, or stress, or by a combination of these factors.
- Primary ovarian insufficiency (POI) is sometimes referred to as premature menopause. It occurs when a woman’s ovaries fail before age 40.
Fallopian tube obstruction. Fallopian tubes can be evaluated by various methods, including with a hysterosalpingogram or by chromopertubation. Hysterosalpingogram is an X-ray of the uterus and fallopian tubes. These images are used to see if dye moves freely through the fallopian tubes indicating they are open. Chromopertubation is similar to a hysterosalpingogram but is done in the operating room at the time of a laparoscopy. This test is used to evaluate if the fallopian tubes are open and to assess if they are dilated.
Risk factors for fallopian tube obstruction include:
- History of pelvic infection
- Ruptured appendix
- Gonorrhea
- Chlamydia
- Endometriosis
- Prior abdominal surgery
Abnormalities of the uterus. The uterus may be evaluated by transvaginal ultrasound to look for various problems. A sonohystogram or hysteroscopy may also be performed to evaluate the uterine environment.
Problems that affect the physical characteristics of the uterus include:
- Intrauterine adhesions
- Endometrial polyps
- Adenomyosis
- Congenital anomalies of the uterus
- Fibroids
Women’s fertility is also known to decline with:
- Age. Fertility declines with age primarily because egg quality declines over time. Older women also have fewer eggs left, and they are more likely to have health conditions that can cause fertility problems. Aging also increases a woman’s chances of miscarriage and of having a child with a genetic abnormality.
- Smoking.
- Excessive alcohol use.
- Having overweight, obesity, or low body weight.
- Extreme weight gain or loss.
- Excessive physical or emotional stress that results in amenorrhea (absent periods).
Should we have genetic testing?
Preimplantation genetic testing (PGT) is a technique in which one or more cells is taken from an egg or embryo (fertilized egg) for testing to provide information about the genetic make-up of the rest of the cells in that embryo. In order to use preimplantation genetic testing (PGT), couples must undergo in vitro fertilization (IVF), where the eggs (oocytes) are removed from a woman’s body and mixed with her partner’s sperm in a laboratory. The embryos which are created can be tested on Day 3 after egg harvest and then implanted back into the uterus on Day 5. Alternatively, the embryos can be frozen after the cells are removed for testing and implanted in a subsequent menstrual cycle.
Patients with many inherited familial diseases can have their embryos tested to determine its genetic make-up. Specifically, this would include patients with a history of single-gene disorders such as cystic fibrosis or sickle cell anemia and patients with a history of sex-linked disorders such as Duchenne muscular dystrophy and Fragile X syndrome. In addition, even families in search of a bone marrow donor may be able to use preimplantation genetic testing (PGT) to bring a child into the world that can provide matching stem cells for an affected sibling.
Other patients may also decide to use genetic screening. For some patients with recurrent pregnancy loss, severe male factor infertility, advanced reproductive age or recurrent IVF treatment failures, genetic screening may be used. Genetic screening is different than other types of genetic testing because the testing is looking for any abnormality instead of a specific disease, and as a result is associated with higher rates of false results. At this time, the American Society for Reproductive Medicine considers genetic screening for this indication experimental. If you are uncertain about genetic testing for you, speak with your doctor about whether preimplantation genetic testing is right for you.
In vitro fertilization clinic near me
The links below contain all practicing members of American Society for Reproductive Medicine (ASRM) and Society for Assisted Reproductive Technology (SART). Find an IVF Clinic near you here:
https://www.sartcorsonline.com/members/Search
https://www.reproductivefacts.org/find-a-health-professional/
In vitro fertilization risks
In vitro fertilization (IVF) raises your chances of certain health problems. From short term to longer term, these risks include:
- Stress. IVF can be draining for the body, mind and finances. Support from counselors, family and friends can help you and your partner through the ups and downs of infertility treatment.
- Complications from the procedure to retrieve eggs. After you take medicines to spur the growth of sacs in the ovaries that each contain an egg, a procedure is done to collect the eggs. This is called egg retrieval. Ultrasound images are used to guide a long, thin needle through the vagina and into the sacs, also called follicles, to harvest the eggs. The needle could cause bleeding, infection or damage to the bowel, bladder or a blood vessel. Risks are also linked with medicines that can help you sleep and prevent pain during the procedure, called anesthesia.
- Ovarian hyperstimulation syndrome (OHSS). This is a condition in which the ovaries become swollen and painful. It can be caused by receiving shots of fertility medicines, such as human chorionic gonadotropin (hCG), to trigger ovulation. In mild cases, women experience mild belly pain, bloating, upset stomach, nausea, vomiting and diarrhea. Symptoms often last up to a week. If you become pregnant, your symptoms might last a few weeks. In more severe cases, fluid builds up in your abdomen called ascites with severe abdominal pain and possible pleural effusion (build-up of fluid between the tissues that line the lungs and the chest), which may lead to shortness of breath and hypoxia. Patients may show signs of low blood volume (hypovolemia), low urine output (oliguria), elevated creatinine due to kidney failure, increased liver enzymes due to liver injury, high white blood cell count (leukocytosis) and electrolyte abnormalities. Increase in the concentration of blood cells (hemoconcentration) will increase youre risk of blood clot forming inside your blood vessels (thromboembolism). In critical cases, acute kidney failure and disseminated intravascular coagulation (DIC) may result in death. Rarely, some people get a worse form of ovarian hyperstimulation syndrome that also can cause rapid weight gain and shortness of breath. The World Health Organization (WHO) estimates the incidence of severe ovarian hyperstimulation syndrome (OHSS) to be 0.2 to 1% of all stimulation cycles 8.
- Miscarriage. The rate of miscarriage for people who conceive using IVF with fresh embryos is similar to that of people who conceive naturally — about 15% for pregnant people in their 20s to over 50% for those in their 40s. The rate rises with the pregnant person’s age.
- Ectopic pregnancy. Ectopic pregnancy is a pregnancy in which the fertilized egg implants in a location outside of the uterus usually in the fallopian tube, the ovary or the abdominal cavity. The embryo can’t survive outside the uterus, and there’s no way to continue the pregnancy. A small percentage of people who use IVF will have an ectopic pregnancy.
- Multiple pregnancy. IVF raises the risk of having more than one baby. Becoming pregnant with multiple babies carries higher risks of pregnancy-related high blood pressure and diabetes, early labor and delivery, low birth weight, and birth defects than does pregnancy with a single baby.
- Birth defects. The age of the mother is the main risk factor for birth defects, no matter how the child is conceived. But assisted reproductive technologies such as IVF are linked with a slightly higher risk of a baby being born with heart issues, digestive problems or other conditions. More research is needed to find out if it’s IVF that causes this raised risk or something else.
- Premature delivery and low birth weight. Research suggests that IVF slightly raises the risk that the baby will be born early or with a low birth weight.
- Cancer. Some early studies suggested that certain medicines used to stimulate egg growth might be linked with getting a specific type of ovarian tumor. But more-recent studies do not support these findings. There doesn’t seem to be a significantly higher risk of breast, endometrial, cervical or ovarian cancer after IVF.
In-vitro fertilization contraindications
There are no absolute contraindications to IVF. However, IVF should not be performed in women who have a significant risk of being sick and dying due to pregnancy if IVF were successful 5. Some examples of these high-risk conditions include but are not limited to Marfan syndrome, New York Heart Association (NYHA) class 3 or 4 heart failure, Eisenmenger syndrome, severe valvular stenosis, pulmonary hypertension, or coarctation of the aorta. For women with these significant medical issues who desire a biological child, they can undergo IVF with egg aspiration, fertilization with their partner’s sperm, but the embryos will be transferred to a gestational carrier.
In-vitro fertilization process
During in vitro fertilization (IVF), eggs and sperm from the couple are incubated together in a laboratory to produce an embryo. A doctor then places the embryo into the woman’s uterus, where it may implant and result in a successful pregnancy.
Both men and women can contribute to infertility. Pregnancy is the result of a process that has many steps. To get pregnant:
- A woman’s body must release an egg from one of her ovaries.
- A man’s sperm must join with the egg along the way (fertilize).
- The fertilized egg must go through a fallopian tube toward the uterus.
- The embryo must attach to the inside of the uterus (implantation).
Infertility may result from a problem with any or several of these steps.
To get started, you’ll want to find a reputable fertility clinic. If you live in the United States, the Centers for Disease Control and Prevention (CDC) and the Society for Assisted Reproductive Technology provide information online about clinics’ individual pregnancy and live birth rates. A fertility clinic’s success rate depends on many things. These include the ages and medical issues of people they treat, as well as the clinic’s treatment approaches. When you talk with a representative at a clinic, also ask for detailed information about the costs of each step of the procedure.
Before you start a cycle of IVF using your own eggs and sperm, you and your partner will likely need various screening tests. These include 9:
- Ovarian reserve testing. This involves getting blood tests to find out how many eggs are available in your body. This is also called egg supply. The results of the blood tests, often used together with an ultrasound of the ovaries, can help predict how your ovaries will respond to fertility medicines. The woman’s ovarian reserve is evaluated using either cycle day three follicle-stimulating hormone (FSH) and estradiol (E2), anti-Mullerian hormone (AMH), or antral follicle count. If the woman is determined to have poor ovarian reserve based on any of these values, she can still pursue IVF but may need to consider the use of donor oocytes.
- Semen analysis. Semen is the fluid that contains sperm. An analysis of it can check the amount of sperm, their shape and how they move. This testing may be part of an initial fertility evaluation. Or it might be done shortly before the start of an IVF treatment cycle.
Infectious disease screening. You and your partner will both be screened for diseases such as HIV. - Practice embryo transfer. This test doesn’t place a real embryo in the uterus. It may be done to figure out the depth of your uterus. It also helps determine the technique that’s most likely to work well when one or more actual embryos are inserted.
- Uterine exam. The inside lining of the uterus is checked before you start IVF. This might involve getting a test called sonohysterography. Fluid is sent through the cervix into the uterus using a thin plastic tube. The fluid helps make more-detailed ultrasound images of the uterine lining. Or the uterine exam might include a test called hysteroscopy. A thin, flexible, lighted telescope is inserted through the vagina and cervix into the uterus to see inside it. Uterine cavity issues such as endometrial polyps or fibroids, adhesions, or septa may interfere with embryo implantation.
- Infectious disease screening for HIV, hepatitis B, and hepatitis C and syphilis is recommended for both partners.
Before you begin a cycle of IVF, think about some key questions, including 9:
- How many embryos will be transferred? The number of embryos placed in the uterus often is based on age and the number of eggs collected. Since the rate of fertilized eggs attaching to the lining of uterus is lower for older people, usually more embryos are transferred — except for people who use donor eggs from a young person, genetically tested embryos or in certain other cases. Most fertility specialists follow specific guidelines to prevent a multiple pregnancy with triplets or more. In some countries, legislation limits the number of embryos that can be transferred. Make sure you and your fertility specialist agree on the number of embryos that will be placed in the uterus before the transfer procedure.
- What will you do with any extra embryos? Extra embryos can be frozen and stored for future use for many years. Not all embryos will survive the freezing and thawing process, but most will. Having frozen embryos can make future cycles of IVF less expensive and less invasive. Or you might be able to donate unused frozen embryos to another couple or a research facility. You also might choose to discard unused embryos. Make sure you feel comfortable making decisions about extra embryos before they are created.
- How will you handle a multiple pregnancy? If more than one embryo is placed in your uterus, IVF can cause you to have a multiple pregnancy. This poses health risks for you and your babies. In some cases, a surgery called fetal reduction can be used to help a person deliver fewer babies with lower health risks. Getting fetal reduction is a major decision with ethical, emotional and mental risks.
- Have you thought through the risks linked with using donor eggs, sperm or embryos, or a gestational carrier? A trained counselor with expertise in donor issues can help you understand the concerns, such as the legal rights of the donor. You also may need an attorney to file court papers to help you become legal parents of an embryo that’s developing in the uterus.
After the above IVF preparations are completed,
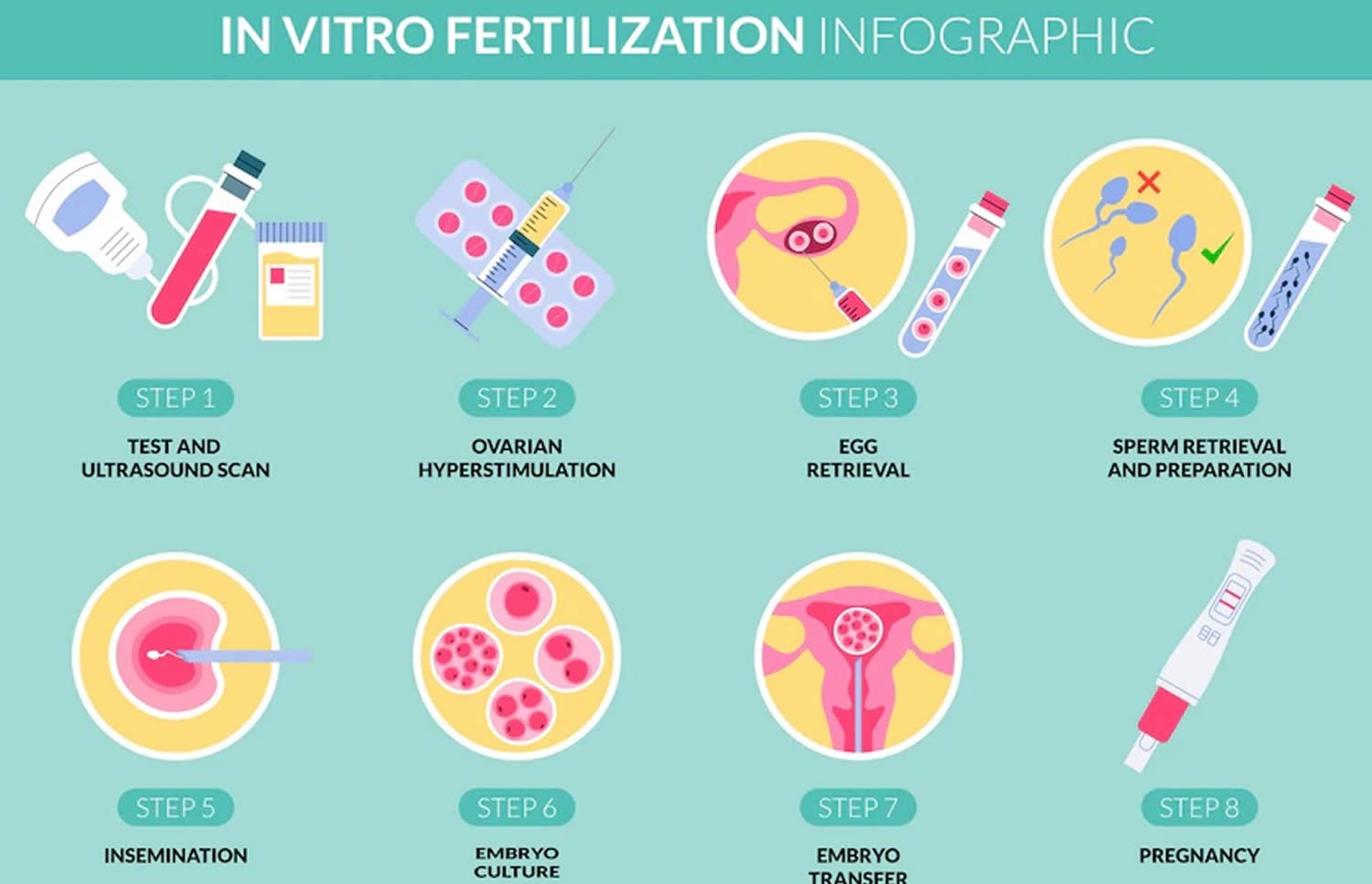
The steps of IVF go as follows:
- Ovarian stimulation. Ovarian stimulation also known as treatment to make mature eggs, ovulation induction, stimulation of egg maturation or superovulation, a woman takes medication to stimulate the ovaries to make many mature eggs at one time. These medications are given by injection for 8 to 14 days. A doctor closely monitors the development of the eggs using transvaginal ultrasound and blood tests to assess follicle growth and estrogen production by the ovaries. When the eggs are mature—as determined by the size of the ovarian follicles and the level of estrogen—an injection of the hormone human chorionic gonadotropin (hCG) initiates the ovulation process. A doctor takes out (egg retrieval) the eggs 34 to 36 hours after the human chorionic gonadotropin (hCG) injection.
- Egg Retrieval. Egg retrieval is the process used to remove the eggs from the ovaries so they can be fertilized. The procedure is performed in a doctor’s office as an outpatient procedure. A mild sedative and painkiller are often used during the procedure, and it normally takes about 30 minutes. The steps for egg retrieval are as follows:
- An ultrasound probe is inserted into the vagina to visualize the ovaries and the follicles, which contain the eggs.
- A needle is inserted through the wall of the vagina to the ovaries. Generally, ultrasound is used to guide the placement of the needle.
- Suction is used to pull the eggs from the ovaries into the needle.
- Fertilization. A man provides a semen sample. If the sperm are healthy, they are centrifuged to concentrate them and reduce the volume, placed in a dish with the egg, and left overnight in an incubator. Fertilization usually occurs on its own. However, sometimes sperm are not able to fertilize the egg on their own. When this is the case, a single sperm is injected into an egg using a needle. This process is called intracytoplasmic sperm injection (ICSI). About 60% of IVF in the Unites States is performed with ICSI 10. The pregnancy rate is about the same for IVF using natural fertilization or intracytoplasmic sperm injection (ICSI). If sperm cannot fertilize the egg without assistance, couples should consider genetic testing. Genetic testing can determine whether the sperm have chromosome problems that might cause development problems in the resulting embryos. Embryos that develop from IVF are placed into the uterus 1 to 6 days after retrieval.
- Embryo Transfer. Embryo transfer is performed in a doctor’s office. Embryo transfer procedure is normally painless, but some women may experience cramping. A doctor inserts a long, thin tube through the vagina and into the uterus and injects the embryo into the uterus. The embryo should implant into the lining of the uterus 6 to 10 days after retrieval. Sometimes the embryos are frozen and thawed at a later date for embryo transfer. This is often done when fresh embryos fail to implant or when a woman wants to preserve her eggs in order to become pregnant years later. Women either time implantation with their ovulation cycle or receive estrogen and progesterone medications to prepare their uterine linings for implantation.
Evaluation before IVF
Before starting IVF, each patient is evaluated to help maximize her chances for success and a healthy pregnancy. Good preconception health is essential to achieving pregnancy with IVF. Chronic medical conditions such as diabetes, high blood pressure and asthma should be well controlled before attempting to conceive. In addition, women planning an IVF cycle should optimize their weight. Obesity has been associated with infertility, a reduced chance of success with IVF, and an increase in the risk of miscarriage and preterm birth. Your doctor can help you determine your ideal weight and refer you to appropriate resources for weight management.
Blood tests
Prior to starting IVF, the woman’s blood type should be verified, and she should be screened for conditions that could affect the health of a pregnancy. Documentation of immunity to rubella (German measles) and varicella (chicken pox) may also require a blood test. Vaccination can be offered before pregnancy if immunity is not present. The patient and her partner will also be tested for:
Female
- HIV
- Hepatitis B antigen
- Hepatitis C antibody
- RPR (rapid plasma reagin) a screening test for syphilis
- Pap smear
- Blood group, Rh, and antibody screen
Male
- HIV
- Hepatitis B antigen
- Hepatitis C antibody
- RPR (rapid plasma reagin) a screening test for syphilis
- Complex semen analysis, antisperm antibodies, and strict morphology
If you are an egg donor, several additional tests are required. These include blood testing for evidence of previous or current cytomegalovirus (CMV infection), a genetic consultation to evaluate your family medical history, and a psychological screening interview.
An option for couples to consider is Universal Genetic Carrier Screening. This testing offers the additional advantages of identifying before pregnancy couples at risk of having children with genetic diseases. They can then be offered appropriate testing to optimize patient education, counseling, and options for achieving pregnancy. Couples at risk of having children with specific genetic diseases can be counseled about the disease inheritance and course and offered referral for potential interventions, such as preimplantation genetic testing (PGT).
Ovarian Reserve Testing
As women age they have a decreased ability to conceive and an increased risk of miscarriage. The reproductive potential of the ovaries, termed ovarian reserve, represents the number of eggs (oocytes) available for potential fertilization at that point in time and may be assessed by blood tests or ultrasound. The presence of decreased ovarian reserve predicts future response to ovarian stimulation. The results of ovarian reserve tests should be considered in the context of the patient’s age. Ovarian reserve tests are good predictors of response to ovarian stimulation, but poor results do not necessarily predict inability to achieve a live birth.
- Anti-Mullerian Hormone Test (AMH): AMH levels remain relatively stable throughout the menstrual cycle and can be assessed on any day of the menstrual cycle. An AMH value less than 1.0 can predict a low response to stimulation.
- Day 2-5 Levels of Follicle-Stimulating Hormone (FSH), and Estradiol (E2): Follicle stimulating hormone (FSH) values greater than 10 IU/L are associated with a less robust response to ovarian stimulation. Estradiol (E2) serves as an aid for interpreting FSH results. Basal estradiol levels typically should be less than 60–80 pg/mL; elevated estradiol levels may have a suppressive effect on FSH levels and may be indicative of decreased ovarian reserve.
- Ultrasonographic assessment of the antral follicle count: determines the number of follicles that measure 2–10 mm in both ovaries. Low antral follicle count may be defined as fewer than 5–7 follicles and is associated with poor response to ovarian stimulation. However, antral follicle count is a relatively poor predictor of future ability to become pregnant.
Semen analysis
A semen analysis should be reviewed. Changes in sperm quality may occur over time that could affect IVF success. Semen parameters can help determine whether standard insemination of eggs or intracytoplasmic sperm injection (ICSI) may be advised.
Uterus exam
The uterus is usually evaluated prior to an IVF. Three methods can be used: a hysterosalpingogram, a saline infusion sonohysterography or a hysteroscopy.
Prior to IVF, a trial or “mock” transfer may be done. The purpose of this procedure is to determine the length and direction of the uterus. This enables the physician to anticipate any difficulties with the embryo transfer.
Ovarian stimulation (treatment to make mature eggs)
The cycle of IVF begins with ovarian stimulation. The start of an IVF cycle begins by using man-made hormones to help the ovaries to make eggs — rather than the single egg that usually develops each month. Multiple eggs are needed because some eggs won’t fertilize or develop correctly after they’re combined with sperm. One cycle of IVF can take about 2 to 3 weeks. More than one cycle may be needed.
During ovarian stimulation, also known as treatment to make mature eggs, ovulation induction or superovulation, “fertility drugs” or “medications for inducing ovulation” are used to stimulate multiple eggs to grow in the ovaries rather than the single egg that normally develops each month. Several medications are used in a typical IVF cycle. These medicines belong to several categories and each are an important part of a stimulated cycle. The types and amount of medications used vary according to the medication protocol prescribed by your physician.
Certain medicines may be used to:
- Stimulate the ovaries. You might receive shots of hormones called gonadotropins that help more than one egg develop at a time. The shot may contain a follicle-stimulating hormone (FSH), a luteinizing hormone (LH) or both.
- Help eggs mature. A hormone called human chorionic gonadotropin (hCG) or other medicines, can help the eggs ripen and get ready to be released from their sacs, called follicles, in the ovaries.
- Delay ovulation. These medicines prevent the body from releasing the developing eggs too soon.
- Prepare the lining of the uterus. You might start to take supplements of the hormone progesterone on the day of the procedure to collect your eggs. Or you might take these supplements around the time an embryo is placed in the uterus. They improve the odds that a fertilized egg attaches to the lining of your uterus.
Medications for Ovarian Stimulation
- Human menopausal gonadotropin (hMG)
- Follicle-stimulating hormone (FSH)
- Luteinizing hormone (LH) (used in conjunction with FSH)
- Human chorionic gonadotropin (hCG)
- Clomiphene citrate
- Letrozole
Medications to Prevent Premature Ovulation
- Gonadatropin-releasing hormone (GnRH) agonists
- GnRH antagonists
Multiple protocols have been utilized, including no stimulation to various levels of ovarian stimulation using clomiphene citrate, letrozole, and exogenous gonadotropins (follicle-stimulating hormone [FSH] and luteinizing hormone [LH]). In IVF cycles, gonadotropin-releasing hormone (GnRH) analogs are utilized to eliminate the woman’s luteinizing hormone (LH) surge allowing the physicians to time egg retrieval. Follicular growth is monitored by transvaginal ultrasonography, and blood levels of estradiol (E2) help determine any indicated changes in the stimulation protocol.
In natural cycle IVF, the egg is retrieved before the mid-cycle luteinizing hormone (LH) surge occurs, or a GnRH antagonist (GnRHant) is used to prevent the release of luteinizing hormone (LH). When the lead follicle reaches a mature size, human chorionic gonadotropin (hCG) is given as a substitute for the LH surge. The pregnancy rate is about 8% per cycle with a 21% cumulative rate after three cycles, with rates as high as 44% in couples with male factor infertility. Natural cycle IVF is not commonly performed because of the lower clinical pregnancy rate 11.
Ovarian stimulation is done in the vast majority of IVF cycles so that approximately 10 to 20 eggs are retrieved. There are two main protocols: long luteal GnRH agonist (GnRHa) or a GnRH antagonist (GnRHant) cycle.
- The long luteal GnRH agonist (GnRHa) protocol begins with the administration of 0.1 mg GnRH agonist (GnRHa) daily starting on cycle-day 21 in the preceding month. This turns off the pituitary secretion of LH (and FSH) during the ovarian stimulation, and the GnRH agonist (GnRHa)is continued until the human chorionic gonadotropin (hCG) injection. Gonadotropins are injected at doses ranging from 75 to 450 IU daily starting on cycle day 2 with dose adjustments based on follicular development and estradiol levels. The human chorionic gonadotropin (hCG) injection is administered when at least three follicles reach 18 mm in size.
- The GnRH antagonist (GnRHant) protocol entails the administration of daily gonadotropins (75 to 450 IU) starting on cycle day 2 or 3. The GnRH antagonist (GnRHant) is started to block the endogenous luteinizing hormone (LH) surge when the lead follicular diameter reaches 14 mm or on the sixth day of ovarian stimulation. When at least three follicles reach, 18 mm hCG is administered.
The minimal stimulation protocol utilizes clomiphene citrate, a selective estrogen receptor modulator (SERM), or letrozole, an aromatase inhibitor, with or without gonadotropins 5. When decreasing or eliminating gonadotropin stimulation, the cost is reduced. The minimal stimulation protocol is gaining more support as studies have found that while the live birth rate is slightly decreased compared to the long GnRH agonist (GnRHa) protocol (49% vs. 63%), there are significantly lower rates of ovarian hyperstimulation syndrome (OHSS) and multiple pregnancies 12, 13.
Your doctor decides which medicines to use and when to use them.
Most often, you’ll need 1 to 2 weeks of ovarian stimulation before your eggs are ready to be collected with the egg retrieval procedure. To figure out when the eggs are ready, you may need:
- Vaginal ultrasound, an imaging exam of the ovaries to track the developing follicles. Those are the fluid-filled sacs in the ovaries where eggs mature.
- Blood tests, to check on how you respond to ovarian stimulation medicines. Estrogen levels often rise as follicles develop. Progesterone levels remain low until after ovulation.
Sometimes, IVF cycles need to be canceled before the eggs are collected. Reasons for this include:
- Not enough follicles develop.
- Ovulation happens too soon.
- Too many follicles develop, raising the risk of ovarian hyperstimulation syndrome (OHSS).
- Other medical issues happen.
If your cycle is canceled, your doctor might recommend changing medicines or the amounts or doses you take. This might lead to a better response during future IVF cycles. Or you may be advised that you need an egg donor.
Gonadotropin releasing hormone (GnRH) Agonists
Gonadotropin releasing hormone (GnRH) is a hormone produced in the brain (hypothalamus) that indirectly stimulates ovarian function. Gonadotropin releasing hormone (GnRH) causes the anterior pituitary gland to release other hormones (luteinizing hormone [LH] and follicle-stimulating hormone [FSH]). Agonists of GnRH are synthetic forms of this hormone which do not directly induce follicle development or ovulation but which have become very important in ART therapy.
GnRH agonists such as Leuprolide (Lupron®) initially stimulate the anterior pituitary gland to release all the stored gonadotropins (LH and FSH -the hormones that normally stimulate ovarian function). Over the course of a week to 10 days, GnRH analogs suppress the production of any new LH and FSH. This effect appears to prevent the ovaries from receiving mixed signals from the patient’s own LH and FSH and from the medications that are administered to stimulate follicle development. The result for many patients is a more synchronized development of mature eggs (oocytes).
There are several advantages to using GnRH agonists:
- They make ovarian stimulation easier to regulate, since the patient’s own hormone production (luteinizing hormone [LH] and follicle-stimulating hormone [FSH]) is suppressed.
- Patients who are treated with GnRH agonists tend to produce a greater proportion of mature eggs than patients who do not receive them.
- GnRH agonists markedly decrease the risk of cycle cancellation for most patients. Prior to their use, 20-50 percent of IVF cycles were canceled because patients would have a premature luteinizing hormone (LH) surge with spontaneous ovulation. Using GnRH agonists, the risk of cycle cancellation is less than 5 percent.
- Ovarian function can be suspended with GnRH agonists for variable periods of time if necessary, which allows for flexibility in cycle scheduling.
GnRH agonists Dosage and Monitoring
The GnRH agonist used most commonly is leuprolide acetate (Lupron®). Lupron® is not US Food and Drug Adminstration (FDA) approved for use in IVF treatment but has been used successfully in IVF for 20 years. Lupron® must be injected to be active. In ART therapy, a formulation of Lupron® is used, which can be injected just under the skin, in a manner similar to insulin injections for diabetes therapy.
The usual dosage of Lupron® is 0.1 or 0.2 ml daily as a single injection. Menstruation usually occurs four to 10 days later. During the time of actual ovarian stimulation, the dosage of Lupron® is halved (e.g., 0.1 ml to 0.05 ml daily). Lupron is usually administered until the day of human chorionic gonadotropin (hCG) administration. Some patients, because of their history or condition, are treated with a different dosage or schedule of Lupron®.
In some protocols, a GnRH analog can be used to trigger ovulation of mature follicles in place of human chorionic gonadotropin (hCG). This is usually reserved for patients with a risk of ovarian hyperstimulation.
Another GnRH analog used in ART therapy is nafarelin acetate (Synarel®). Synarel® is administered as a nasal spray. The usual starting dose is two sprays twice a day. The timing of administration is identical to Lupron®. The dosage of Synarel® is usually halved (e.g., from two sprays twice a day to one spray twice a day) when ovarian stimulation is begun.
Gonadotropin releasing hormone (GnRH) Antagonists
Gonadotropin releasing hormone (GnRH) Antagonists also called “anti- gonadotropin-releasing hormones” bind to the receptor for gonoadotropin releasing hormone on the anterior pituitary gland, preventing the natural luteinizing hormone (LH) surge and ovulation. This is important to the success of an IVF cycle, when premature ovulation could reduce the number of eggs retrieved.
Gonadotropin releasing hormone (GnRH) Antagonists such as cetrorelix acetate (Cetrotide®) and ganirelix acetate (Antagon®) are started later in the cycle than leuprolide acetate (Lupron®) and directly and immediately inhibit luteinizing hormone (LH) and follicle-stimulating hormone (FSH) production. Protocols that use GnRH Antagonists may require fewer injections. Ultrasound measurements of follicular growth are used to determine when to start these medicines.
Gonadotropins
To increase likelihood of pregnancy through ART, multiple eggs must be produced. This is accomplished through the administration of gonadotropins, hormonal medications that directly stimulate the ovaries. Stimulation can be achieved with a variety of drug regimens. Gonadotropin medications come in several forms; Repronex® (menotropins for injection) and Menopur® (menotropins for injection) are a combination of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). They replace a woman’s own LH and FSH which are normally produced by the anterior pituitary gland. Bravelle®, Follistim® AQ Cartridge for use with Follistim Pen®, Follistim® AQ Vial, Gonal-F®, and Gonal-F® RFF Pen are preparations that contain only FSH. Follistim® AQ Cartridge for use with Follistim Pen®, Follistim® AQ Vial, Gonal-F®, and Gonal-F® RFF Pen are recombinant products which are made by genetically engineered cells. This process ensures uniform purity and potency. Because the dose of hormones that are used in ART is greater than what the body normally produces, the ovaries typically develop more than one oocyte as occurs in a natural cycle.
Gonadotropins act directly on the ovary to stimulate the growth of follicles (the structures in the ovaries which contain eggs). Granulosa cells within the follicles grow and develop which cause the follicles to enlarge and fill with follicular fluid. These developing follicles can be counted and measured using transvaginal ultrasound. As the follicles grow, they produce increasing amounts of estrogen, which can be measured with a laboratory blood test. Some physicians prefer one formulation or another. Your doctor can discuss this with you in more detail.
Gonadotropins Dosage and Monitoring
Gonadotropins are packaged in vials containing 37.5, 75 or 150 International Units (IU). Follistim AQ Pens and Gonal-F RFF Pens are packaged in pre-mixed injectable pens. Multi-dose vials of some medications are also available. Dosage may vary depending on the patient’s history. Patients will then have regularly scheduled transvaginal ultrasound examinations and serum estradiol tests. The dose of gonadotropins is then determined by the result of the ultrasound and estradiol tests. Most women require between seven to 10 days of gonadotropin therapy.
Bravelle®, and Repronex® are administered subcutaneously or by intramuscular injection, usually into the muscles of the buttocks. Gonal-F,® Follistim,® Follistim AQ Pens, and Gonal-F RFF Pens are administered subcutaneously, like an insulin or allergy shot.
Human Chorionic Gonadotropin (hCG)
Human chorionic gonadotropin (hCG) is an injectable medication that is administered to complete egg maturation. Human chorionic gonadotropin is structurally similar to the LH that is produced by a woman’s pituitary gland. It acts on the ovary in a manner similar to a woman’s own LH. Human chorionic gonadotropin, like LH, stimulates the final maturation of the oocytes in the follicle. It also stimulates progesterone production from the ovary after egg retrieval. This progesterone is important to prepare the uterus for implantation of the embryo.
Human chorionic gonadotropin (hCG) Dosage and Administration
Human chorionic gonadotropin (hCG) are Profasi®, Ovidrel®, Novarel®,and Pregnyl® can be administered several different ways. The commonly administered dose is a single injection of 10,000 units. Once hCG is administered, ovulation usually occurs in approximately 36 to 40 hours. Therefore oocyte retrieval is routinely scheduled at 34-36 hours after hCG. This helps ensure maximal egg maturity, which is important for fertilization and embryo development. Occasionally, several doses of 2,500 units (usually every three days) are administered after egg retrieval to stimulate progesterone production. If your response to stimulation is particularly exuberant, the dose of hCG can be reduced to 5,000 units in an attempt to reduce the risk of ovarian hyperstimulation syndrome.
It typically takes 8-10 days for single injection of 10,000 units of hCG to be cleared from the blood stream. As hCG is the same hormone that is produced by a developing pregnancy, patients should not have a blood or urine pregnancy test sooner than 10 days following the hCG injection. If a pregnancy test is performed earlier, it may measure the hCG that was given by injection rather than measure hCG produced by a pregnancy.
What if I don’t respond to the drugs for ovarian stimulation?
A response to ovarian stimulation depends on a number of different factors, the most important include available eggs, appropriate hormone levels, proper administration of any medications and lifestyle/environmental factors. In order to respond to ovarian stimulation, a woman must have eggs available to respond; this is sometimes referred to as ovarian reserve. If a woman has diminished ovarian reserve (identified by a high blood levels of follicle stimulation hormone (FSH), low blood levels of anti Müllerian hormone (AMH) or a low antral follicle count on ultrasound), she may not have as robust (or any) response to ovarian stimulation. For these patients, an alternate stimulation protocol may be tried or donated eggs may be used (from a woman known or unknown to the patient).
It is possible that a woman does have the necessary eggs but lacks the appropriate pituitary hormones to respond. In this case, using a different medication- one which may contain both follicle stimulation hormone (FSH) and luteinizing hormone (LH) may allow for an optimal response. Lifestyle factors can also affect a woman’s response to ovarian stimulation. Optimizing your weight, diet and stress and cessation of use of tobacco, alcohol and recreational substances can also improve a response to ovarian stimulation. Speak to your doctor regarding improving your particular response to ovarian stimulation.
Egg retrieval
Egg retrieval is the procedure to collect the eggs from one or both of your ovaries. It takes place in your doctor’s office or a clinic. The procedure is done 34 to 36 hours after the final shot of fertility medicine human chorionic gonadotropin (hCG) and before ovulation.
- Before egg retrieval, you’ll be given medicine to help you relax and keep you from feeling pain.
- An ultrasound device is placed into your vagina to find follicles, which are the sacs in the ovaries that each contain an egg. Then a thin needle is inserted into an ultrasound guide to go through the vagina and into the follicles to collect the eggs. This process is called transvaginal ultrasound aspiration.
- If your ovaries can’t be reached through the vagina this way, an ultrasound of the stomach area may be used to guide the needle through the stomach and into the ovaries.
- The eggs are removed from the follicles through a needle connected to a suction device. Multiple eggs can be removed in about 20 minutes.
- After the procedure, you may have cramping and feelings of fullness or pressure.
- Mature eggs are placed in a liquid that helps them develop. Eggs that appear healthy and mature will be mixed with sperm to attempt to create embryos. But not all eggs are able to be fertilized with success.
Egg retrieval is usually accomplished by transvaginal ultrasound aspiration, a minor surgical procedure that can be performed in the doctor’s office or an outpatient center. Some form of pain medication is generally administered. An ultrasound probe is inserted into the vagina to identify the follicles, and a needle is guided through the vagina and into the follicles.
The eggs are aspirated (removed) from the follicles through the needle connected to a suction device. Removal of multiple eggs can usually be completed in less than 30 minutes. Some women experience cramping on the day of the retrieval, but this sensation usually subsides by the next day. Feelings of fullness and/or pressure may last for several weeks following the procedure because the ovaries remain enlarged. In some circumstances, one or both ovaries may not be accessible by transvaginal ultrasound. Laparoscopy may then be used to retrieve the eggs using a small telescope placed in the umbilicus.
Do I need donor eggs?
The main limitation to human reproduction is the natural loss of healthy eggs as a woman ages. At birth, a woman is born with her total reserve of eggs and no more are created. Over her lifetime, waves of healthy eggs degenerate through a natural process called atresia so that by her mid thirties, women begin to see a greater difficulty to achieve a pregnancy and a higher chance of chromosome abnormally affected children. By her early forties, the majority of women experience infertility and eventually a loss of reproductive capacity. This is due to the eventual loss of her remaining healthy eggs. Egg donation, like sperm donation, is a means to realize parenthood when the loss of gametes (i.e., egg or sperm) occurs. This may be due to the natural process of aging or may occur prematurely from other disease states or because of medical treatments for cancer, for example. When gametes are depleted, replacement by egg donation is a wonderful option to enable one to become a parent. There are many young women who want to help others overcome infertility. They serve as egg donors by expressing interest and then going through a rigorous screening process to ensure they are appropriate candidates. Typically, they provide a detailed health history of themselves and genetic history of their ancestors. Medical and psychological evaluations are performed, in addition to Food and Drug Administration (FDA) mandated infectious disease testing. Once a patient has chosen to pursue egg donation, the process typically involves coordination of their two menstrual cycles so that the eggs may be retrieved, fertilization by the sperm of the patient’s partner and transfer into the patient’s womb can occur during the same month. The egg donor treatment cycles rate among the highest success in assisted reproduction.
Sperm retrieval
If you’re using your partner’s sperm, a semen sample needs to be collected at your doctor’s office or clinic the morning of egg retrieval. Or sperm can be collected ahead of time and frozen. Most often, the semen sample is collected through masturbation. Other methods can be used if a person can’t ejaculate or has no sperm in the semen. For example, a procedure called testicular aspiration uses a needle or surgery to collect sperm directly from the testicle. Sperm from a donor also can be used. Sperm are separated from the semen fluid in the lab.
Fertilization
After the eggs are retrieved, they are examined in the laboratory for maturity and quality. Mature eggs are placed in an IVF culture medium and transferred to an incubator to await fertilization by the sperm.
Sperm is separated from semen usually obtained by masturbation or in a special condom used during intercourse. Alternatively, sperm may be obtained from the testicle, epididymis, or vas deferens from men whose semen is void of sperm either due to an obstruction or lack of production.
Two common methods can be used to try to fertilize eggs with sperm:
- Conventional insemination. Healthy sperm and mature eggs are mixed and kept in a controlled environment called an incubator.
- Intracytoplasmic sperm injection (ICSI). A single healthy sperm is injected right into each mature egg. Often, ICSI is used when semen quality or number is an issue. Or it might be used if fertilization attempts during prior IVF cycles didn’t work.
In certain situations, other procedures may be recommended before embryos are placed in the uterus. These include:
- Assisted hatching. About 5 to 6 days after fertilization, an embryo “hatches” from the thin layer that surrounds it, called a membrane. This lets the embryo attach to the lining of the uterus. If you’re older and you want to get pregnant, or if you have had past IVF attempts that didn’t work, a technique called assisted hatching might be recommended. With assisted hatching a hole is made in the embryo’s membrane just before the embryo is placed in the uterus. This helps the embryo hatch and attach to the lining of the uterus. Assisted hatching is also useful for eggs or embryos that were frozen, as that process can harden the membrane.
- Preimplantation genetic testing (PGT). Embryos are allowed to develop in the incubator until they reach a stage where a small sample can be removed. The sample is tested for certain genetic diseases or the correct number of threadlike structures of DNA, called chromosomes. There are usually 46 chromosomes in each cell. Embryos that don’t contain affected genes or chromosomes can be transferred to the uterus. Preimplantation genetic testing can lower the chances that a parent will pass on a genetic problem. It can’t get rid of the risk completely. Prenatal testing may still be recommended during pregnancy.
Do I need intracytoplasmic sperm injection (ICSI)?
The purpose of intracytoplasmic sperm injection (ICSI) is to assist the fertilization process when a man’s sperm count is abnormal. Whether it is because the number of motile sperm is very low or the morphology is excessively poor, the intracytoplasmic sperm injection (ICSI) technique involves the delivery of a single sperm into a single egg. Most clinics will recommend ICSI if there is a fear that poor fertilization may occur by traditional IVF where sperm are merely added to the egg culture dish. Accordingly, efforts are made to assess sperm by function or morphology to help determine those most likely to require ICSI. It is best to discuss this option with your doctor prior to treatment.
What if my eggs don’t fertilize?
Most eggs will fertilize when they are placed in a culture dish with several thousand normal sperm. This process is called “in vitro fertilization” or “IVF”. When there are not enough normal functioning sperm for IVF, fertilization will usually occur after a single live sperm is injected into each egg, termed “intracytoplasmic sperm injection” or “ICSI”. On rare occasions, fertilization does not occur even with ICSI, presumably because of a problem inherent to either eggs or sperm. In these cases, the use of donor sperm or donor eggs will usually result in fertilization. Your fertility specialist and IVF laboratory personnel will help you determine which approach is most likely to result in egg fertilization.
Assisted hatching
Assisted hatching is a micromanipulation procedure in which a hole is made in the zona pellucida just prior to embryo transfer to facilitate hatching of the embryo. Although assisted hatching has not been demonstrated definitively to improve live birth rates, assisted hatching may be used for older women or couples who have had unsuccessful prior IVF attempts. There is no clear benefit of assisted hatching to improve pregnancy or live birth rates in other groups of IVF patients.
Preimplantation genetic testing (PGT)
Preimplantation genetic testing (PGT) also called preimplantation genetic diagnosis (PGD) is performed at some centers to screen for inherited diseases. In preimplantation genetic testing (PGT), one or two cells are removed from the developing embryo and tested for a specific genetic disease. Embryos that do not have the gene associated with the disease are selected for transfer to the uterus.
Preimplantation genetic testing (PGT) procedures require specialized equipment and experience together with IVF (in a couple who may otherwise not need IVF to conceive). Some couples, especially those who are carriers of genetic diseases, consider embryo screening beneficial in reducing the risk of having an affected child. While preimplantation genetic testing (PGT) can reduce the likelihood of conceiving a pregnancy with an affected child, it cannot eliminate the risk. Confirmation with chorionic villus sampling (CVS), amniocentesis, or other testing is still necessary.
Embryo transfer
The next step in the IVF process is the embryo transfer. Embryo transfer is a procedure to place one or more embryos in your uterus, is done at your doctor’s office or a clinic. Embryo transfer often takes place 2 to 6 days after eggs are collected.
- You might be given a mild sedative to help you relax. The procedure is often painless, but you might have mild cramping.
- Embryos are transferred under transabdominal ultrasound guidance into the uterus by a long, thin, flexible tube called a catheter is placed into your vagina, through the cervix and into the uterus.
- A syringe that contains one or more embryos in a small amount of fluid is attached to the end of the catheter.
- Using the syringe, the embryo or embryos are placed into the uterus.
- The embryo(s) are placed 1 to 2 cm from the uterine fundus. After the transfer, the catheter is checked under the microscope to ensure no embryos are retained in the catheter and that all embryos were successfully placed in the uterus.
The number of embryos transferred will depend on the embryo stage, embryo quality, maternal age, and patient preference. Since each embryo has a fair probability of implantation and development, the number of embryos to be transferred should be determined for each patient, taking into account the odds of achieving a pregnancy based on the number of embryos transferred weighed against the risk of multiple pregnancy. The American Society for Reproductive Medicine recommends no more than two embryos to be transferred in women 37 years-old or less, no more than three embryos in 38 to 40 year-olds as well as in women 41 to 42 years of age 14. A higher number of cleavage stage embryos can be transferred due to the lower likelihood of successful implantation; no more than two embryos in women < 35 years of age, no more than three embryos in women 35 to 37 years of age, no more than four embryos in women 38 to 40 and in women 41 to 42 years of age, five or fewer embryos. These guidelines have been effective in helping US ART programs maintain their high success rates while significantly decreasing the number of high-order multiple pregnancies (triplets and higher). The reproductive endocrinologist or embryologist will discuss this with you prior to the transfer.
To optimize embryo implantation and a continuing pregnancy, progesterone supplementation is initiated on the day of egg retrieval or embryo transfer. Excess good quality embryos are cryopreserved for future use.
If the procedure works, an embryo will attach to the lining of your uterus about 6 to 10 days after egg retrieval.
After the embryo transfer, you can get back to your usual daily routine. Your ovaries may still be enlarged, so vigorous activities or sex might cause discomfort. Ask your doctor how long you should stay away from these activities.
Typical side effects of embryo transfer include:
- Passing a small amount of clear or bloody fluid shortly after the procedure. This is due to the swabbing of the cervix before the embryo transfer.
- Breast tenderness due to high estrogen levels.
- Mild bloating.
- Mild cramping.
- Constipation.
Call your doctor if you have moderate or severe pain, or heavy bleeding from the vagina after the embryo transfer. You’ll likely to need to get checked for complications such as infection, twisting of an ovary and ovarian hyperstimulation syndrome (OHSS).
Should I have my IVF center perform Assisted Hatching on my embryos before transfer?
In vivo hatching of the embryo is a critical component of the physiologic events culminating in implantation. Conversely, the failure to hatch may be one of the many factors limiting human reproductive efficiency. The clinical application of assisted hatching has been proposed as one approach toward the enhancement of implantation and pregnancy rates following in vitro fertilization (IVF). The assisted hatching procedure entails the creation of a gap in the outer area of the embryo called the zona. This is done either by drilling with an acid medium, by laser, or by using a piezomicromanipulator. Success rates following the use of assisted hatching in different ART programs have varied considerably. Well-designed studies suggest that assisted hatching might best be used in patients > 38 years old or with multiple prior failed IVF cycles.
How many embryos should I have transferred back?
The objective of infertility treatment should be the birth of a single, healthy child. Many of the treatment options presented to infertile couples, however, are associated with high risks of multiple births. Moreover, many couples view multiple gestation as desirable and are unaware of the risks they pose to both mother and babies. Couples should understand these potential risks before starting treatment.
The ability to limit the number of embryos or eggs transferred is an effective approach to limit multiple pregnancies. The Society for Assisted Reproductive Technology and the American Society for Reproductive Medicine have published guidelines recommending an optimal number of embryos for transfer based on patient age, embryo quality, and other criteria. In the United States, the decision regarding the number of embryos to transfer is made jointly by the doctor and the patients. This decision should be based upon the best interests of the patient and the future offspring. However, in England no more than three embryos may be transferred in most circumstances. In Canada, a recent Royal Commission recommended the transfer of a maximum of three embryos.
The ultimate goal is to achieve a high pregnancy rate while transferring a single embryo. Recent laboratory improvements have allowed programs to transfer two embryos while maintaining acceptable pregnancy rates. Eventually, the transfer of one embryo will resolve the issues surrounding multiple pregnancies.
Some clinics see more than the average number of patients with difficult infertility problems. Some clinics are willing to offer assisted reproductive technology (ART) to most potential users, even those who have a low probability of success. Others discourage such patients or encourage them to use donor eggs, a practice that results in higher success rates among older women. Clinics that accept a higher percentage of women who previously have had multiple unsuccessful ART cycles will generally have lower success rates than clinics that do not. In contrast, clinics that offer ART procedures to patients who might have become pregnant with less technologically advanced treatment will have higher success rates than clinics that do not.
What is the difference between a day 3 and day 5 transfer?
Usually embryos are transferred on day 3 or 5. The day of transfer depends on embryo quantity quality, patient characteristics, and laboratory practices. You should discuss this decision with your doctor.
What are my options if I decide not to use my stored embryos?
If you have stored embryos that you have decided not to transfer into your uterus to attempt pregnancy, you have four options for their final disposition. First, you can donate your embryos to another woman with fertility problems that you don’t know so that she can attempt pregnancy through a process called “anonymous embryo donation”. Second, you can donate your embryos to another woman that you do know so that she can attempt pregnancy though a process called “directed embryo donation”. Third, you can donate your embryos for laboratory research to help improve pregnancy rates for infertile couples in the future. Finally, you can ask that your embryos be thawed and discarded. In both of these last two situations, your embryos will not be transferred into another person and no child will be born as a result.
Embryos Freezing
Extra embryos remaining after the embryo transfer may be frozen or cryopreserved for future transfer. Embryos Freezing or cryopreservation makes future ART cycles simpler, less expensive, and less invasive than the initial IVF cycle, since the woman does not require ovarian stimulation or egg retrieval. Once frozen, embryos may be stored for prolonged periods, and live births have been
reported using embryos that have been frozen for almost 20 years. However, not all embryos survive the freezing and thawing process, and the live birth rate is lower with cryopreserved embryo transfer. Couples should decide if they are going to cryopreserve extra embryos before undergoing IVF.
There are two methods used to cryopreserve embryos: conventional (slow) freezing and “vitrification” or fast freezing. Your center will determine which method is best to use based on their experience and the developmental stage at which the embryos are frozen. Although some reports claim that fast freezing (vitrification) may have higher success rates after thawing or warming, this is not the case at all centers.
It should also be noted that more and more ART centers are cryopreserving eggs (oocytes) prior to fertilization. This is done most commonly in young women who are about to undergo treatments or procedures that may affect their future fertility, such as chemotherapy for cancer. However, it is also used for couples who do not wish to freeze embryos because of concerns over their survival during freezing and thawing or the dilemma of what to do with remaining embryos after they have completed their families. Clinic success rates may vary.
Finally, it should be noted that although there are theoretical risks, freezing of sperm, eggs, and embryos is very safe. There have been no documented cases of infectious disease transmission, nor do the risks of birth defects, chromosomal anomalies, or pregnancy complications appear to be increased compared with using fresh sperm, eggs, or embryos.
IVF Results
At least 12 days after egg retrieval, you get a blood test to find out whether you’re pregnant.
- If you’re pregnant, you’ll likely be referred to an obstetrician or other pregnancy specialist for prenatal care.
- If you’re not pregnant, you’ll stop taking progesterone and likely get your period within a week. Call your doctor if you don’t get your period or if you have unusual bleeding. If you’d like to try another cycle of IVF, your doctor might suggest steps you can take to improve your chances of getting pregnant next time.
The chances of giving birth to a healthy baby after using IVF depend on various factors, including:
- Maternal age. The younger you are, the more likely you are to get pregnant and give birth to a healthy baby using your own eggs during IVF. Often, people age 40 and older are counseled to think about using donor eggs during IVF to boost the chances of success.
- Embryo status. Transfer of embryos that are more developed is linked with higher pregnancy rates compared with less-developed embryos. But not all embryos survive the development process. Talk with your doctor about your specific situation.
- Reproductive history. People who’ve given birth before are more likely to be able to get pregnant using IVF than are people who’ve never given birth. Success rates are lower for people who’ve already tried IVF multiple times but didn’t get pregnant.
- Cause of infertility. Having an average supply of eggs raises your chances of being able to get pregnant using IVF. People who have severe endometriosis are less likely to be able to get pregnant using IVF than are those who have infertility without a clear cause.
- Lifestyle factors. Smoking can lower the chance of success with IVF. Often, people who smoke have fewer eggs retrieved during IVF and may miscarry more often. Obesity also can lower the chances of getting pregnant and having a baby. Use of alcohol, drugs, too much caffeine and certain medicines also can be harmful.
Talk with your doctor about any factors that apply to you and how they may affect your chances of a successful pregnancy.
In-vitro fertilization success rates
Success rates after IVF vary and depend on many factors. They can include the clinic or IVF center performing the IVF procedure, the infertility diagnosis, and the age of the woman undergoing the procedure. The woman’s age is especially important. To find your chance of having a baby using in vitro fertilization (IVF), which is the most common type of Assisted Reproductive Technology (ART), you can use the free IVF Success Estimator tool. This tool uses data from the 453 United States fertility clinics in operation in 2021. This information is calculated based on the experiences of women and couples with similar characteristics. However, the IVF Success Estimator tool does have some limitations. The estimates are based on available data which may not be representative of your specific experience. For example, the IVF Success Estimator tool can generate estimates only for people ranging from age 20 to 50 years. If you are younger than 20 or older than 50 years of age and attempt to enter your true age, the tool will be unable to provide an estimate and you will be directed to enter a value between 20 and 50. You may choose to enter the value that is closest to your true age for an estimation. Available data to generate estimates are similarly limited to specific ranges for height and weight. Additionally, this the IVF Success Estimator tool does not provide medical advice, diagnosis, or treatment. You still need to speak with your doctor about your specific treatment plan and potential for success.
It is also important to understand the definitions of pregnancy rates and live birth rates. For example, a pregnancy rate of 40% does not mean that 40% of women took babies home. Pregnancy does not always result in live birth. A biochemical pregnancy is a pregnancy confirmed by blood or urine tests but not visible on ultrasound, because the pregnancy stops developing before it
is far enough along to be seen on ultrasound. A clinical pregnancy is one in which the pregnancy is seen with ultrasound, but stops developing sometime afterwards. Therefore, when comparing the “pregnancy” rates of different clinics, it is important to know which type of pregnancy is being compared. Most couples are more concerned with a clinic’s live birth rate, which is the probability of delivering a live baby per IVF cycle started. Pregnancy rates, and more importantly live birth rates, are influenced by a number of factors, especially the woman’s age.
According to the 2022 Society for Assisted Reproductive Technology live births rates per intended egg retrieval (all embryo transfers) by age group were as follows:
Women <35 years:
- Live births: 43.1%
- Singleton (percentage of live births): 95.7%
- Twins (percentage of live births): 4.2%
- Triplets (percentage of live births): 0%
Women 35-37 years:
- Live births: 31%
- Singleton (percentage of live births): 96%
- Twins (percentage of live births): 3.9%
- Triplets (percentage of live births): 0.1%
Women 38-40 years:
- Live births: 19%
- Singleton (percentage of live births): 95.7%
- Twins (percentage of live births): 4.3%
- Triplets (percentage of live births): 0%
Women 41-42 years:
- Live births: 9.4%
- Singleton (percentage of live births): 96.3%
- Twins (percentage of live births): 3.7%
- Triplets (percentage of live births): 0%
Women >42 years:
- Live births: 3.2%
- Singleton (percentage of live births): 96.9%
- Twins (percentage of live births): 3.1%
- Triplets (percentage of live births): 0%
In-vitro fertilization cost
Costs for an IVF vary from clinic to clinic. Including procedures, imaging, bloodwork, and medications, a single cycle can cost $15,000 to $30,000 or more. Note this is merely an approximation. Some people go through more than one IVF cycle, which can multiply treatment expenses. On average, the medication costs for a single IVF cycle can range from $3,000 to $6,000 per cycle. These are rough estimates, and the actual costs can differ based on individual circumstances, medication choices, and insurance coverage. Additional expenses may include loss of wages from time missed at work and expenses incurred due to travel and/or accommodations. In addition, the medications utilized in in-vitro fertilization (IVF) procedures (gonadotropins, hCG, GnRH analogs, or GnRH antagonists) are very expensive. All of these factors must be considered in determining the financial feasibility of participation in an in-vitro fertilization (IVF) program.
Do insurance plans cover infertility treatment?
The degree of services covered depends on where you live and the type of insurance plan you have. Many insurance companies do offer coverage for the various stages of the evaluation and treatment of infertility. Exactly what is covered often varies from insurer to insurer, and from policy to policy. Some insurers will only cover the examination and testing to determine the cause of infertility, while others will cover treatment and medications. The kind of treatment that is covered also varies. For example, some policies may cover intrauterine insemination (IUI) when used in conjunction with medication to boost ovulation, but may not cover in vitro fertilization (IVF) where as others may cover both. Fourteen states currently have laws that require insurers to either cover or offer to cover some form of infertility diagnosis and treatment. Those states are Arkansas, California, Connecticut, Hawaii, Illinois, Maryland, Massachusetts, Montana, New Jersey, New York, Ohio, Rhode Island, Texas and West Virginia. However, the laws vary greatly in their scope of what is and is not required to be covered. For more information about the specific laws for each of those states, please call your state’s Insurance Commissioner’s office or to learn about pending insurance legislation in your state, please contact your State Representatives.
It is also important to study your policy to determine if, and to what extent, you may be covered. Many fertility practices have financial counselors to help you through this, to answer your questions about your insurance benefits and to work with the insurer to determine what is covered.
Whether or not you live in a state with an infertility insurance law, you may want to consult with your employer’s director of human resources to determine the exact coverage your plan provides. Another good source of assistance is RESOLVE, an infertility patient advocacy and information organization.
When to end IVF treatment?
Studies indicate that the chance for pregnancy in consecutive IVF cycles remains similar in up to 4 cycles. However, many other factors should be considered when determining the appropriate endpoint in therapy, including financial and psychological factors. Members of the IVF team can help couples decide when to stop treatment and discuss other options such as egg and/or sperm donation or adoption, if appropriate. Your doctor, support groups, and other couples undergoing infertility treatment can provide valuable support and guidance.
- Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2013 Jan;99(1):63. doi: 10.1016/j.fertnstert.2012.09.023[↩]
- Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978 Aug 12;2(8085):366. doi: 10.1016/s0140-6736(78)92957-4[↩]
- Zhao Y, Brezina P, Hsu CC, Garcia J, Brinsden PR, Wallach E. In vitro fertilization: four decades of reflections and promises. Biochim Biophys Acta. 2011 Sep;1810(9):843-52. doi: 10.1016/j.bbagen.2011.05.001[↩]
- Sunderam S, Kissin DM, Crawford SB, Folger SG, Boulet SL, Warner L, Barfield WD. Assisted Reproductive Technology Surveillance – United States, 2015. MMWR Surveill Summ. 2018 Feb 16;67(3):1-28. doi: 10.15585/mmwr.ss6703a1[↩]
- Choe J, Shanks AL. In Vitro Fertilization. [Updated 2023 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562266[↩][↩][↩]
- In-Vitro Fertilization (IVF). https://www.yashodahealthcare.com/blogs/in-vitro-fertilization-ivf/[↩]
- Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet Gynecol. 2019 Jun;133(6):e377-e384. doi: 10.1097/AOG.0000000000003271[↩]
- Binder H, Dittrich R, Einhaus F, Krieg J, Müller A, Strauss R, Beckmann MW, Cupisti S. Update on ovarian hyperstimulation syndrome: Part 1–Incidence and pathogenesis. Int J Fertil Womens Med. 2007 Jan-Feb;52(1):11-26.[↩]
- In vitro fertilization (IVF). https://www.mayoclinic.org/tests-procedures/in-vitro-fertilization/about/pac-20384716[↩][↩]
- American Society for Reproductive Medicine. (2015). Assisted reproductive technologies: A guide for patients. http://www.fertilityanswers.com/wp-content/uploads/2016/04/assisted-reproductive-technologies-booklet.pdf[↩]
- Pelinck MJ, Vogel NE, Arts EG, Simons AH, Heineman MJ, Hoek A. Cumulative pregnancy rates after a maximum of nine cycles of modified natural cycle IVF and analysis of patient drop-out: a cohort study. Hum Reprod. 2007 Sep;22(9):2463-70. doi: 10.1093/humrep/dem164[↩]
- Zhang JJ, Merhi Z, Yang M, Bodri D, Chavez-Badiola A, Repping S, van Wely M. Minimal stimulation IVF vs conventional IVF: a randomized controlled trial. Am J Obstet Gynecol. 2016 Jan;214(1):96.e1-8. doi: 10.1016/j.ajog.2015.08.009[↩]
- Shrestha D, La X, Feng HL. Comparison of different stimulation protocols used in in vitro fertilization: a review. Ann Transl Med. 2015 Jun;3(10):137. doi: 10.3978/j.issn.2305-5839.2015.04.09[↩]
- Practice Committee of the American Society for Reproductive Medicine. Electronic address: [email protected]; Practice Committee of the Society for Assisted Reproductive Technology. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril. 2017 Apr;107(4):901-903. https://doi.org/10.1016/j.fertnstert.2017.02.107[↩]





 process and procedure. What are the risks & success rates of assisted in vitro fertilization (IVF). How much does IVF cost?){kind=link}