Contents
- Ataxia telangiectasia
- Ataxia telangiectasia cause
- Ataxia telangiectasia symptoms
- Neurological problems
- Immunodeficiency (weakened immune system)
- Lung disease
- Cancers
- Radiation sensitivity
- Feeding and swallowing problems
- Poor growth
- Delayed pubertal development or gonadal dysgenesis
- Insulin-resistant diabetes
- Hair and skin problems
- Sleep problems
- Cognitive problems
- Muscoloskeletal problems
- Older patients with ataxia telangiectasia
- Other problems
- Ataxia telangiectasia diagnosis
- Ataxia telangiectasia differential diagnosis
- Ataxia telangiectasia treatment
- Ataxia telangiectasia prognosis
- Ataxia telangiectasia life expectancy
Ataxia telangiectasia
Ataxia-telangiectasia also known as Louis-Bar syndrome, cerebello-oculocutaneous telangiectasia, immunodeficiency with ataxia telangiectasia or ATM is a rare autosomal recessive inherited childhood multi-system disorder that affects the part of your brain that controls motor movement (intended movement of muscles) and speech 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. Ataxia telangiectasia also affects your nervous system, immune system, and other body systems. Symptoms usually begins in early childhood before age 5.
Ataxia-telangiectasia is characterized by progressive difficulty with coordinating movements (ataxia) beginning in early childhood, usually before age 5 12, 13. Ataxia telangiectasia generally presents at 12 to 18 months of age with an unsteadiness of gait due to cerebellar ataxia 1. Affected children typically develop difficulty walking, problems with balance and hand coordination, involuntary jerking movements (chorea), muscle twitches (myoclonus), and disturbances in nerve function (peripheral neuropathy) that gradually develop and often worsen. The ataxia gradually worsens and by the age of 10 years children are unable to walk and require wheelchair assistance. People with ataxia-telangiectasia also have slurred speech (dysarthria), trouble moving their eyes to look side-to-side (oculomotor apraxia), difficulty swallowing (dysphagia), choreoathetosis [rapid (chorea) or slow (athetosis) involuntary movements of the fingers or toes], involuntary muscle contractions that cause repetitive or twisting movements (dystonia) and tremor. The majority do not have severe cognitive impairment (intellectual disability) in childhood, although progressive cognitive impairment has been reported over time 14, 15. Small clusters of enlarged blood vessels called telangiectasias, which occur in the eyes mostly in the bulbar conjunctiva and on the surface of the skin develops (but can sometimes be found in other organs such as the bladder) at 3–4 years of age, are also characteristic of ataxia telangiectasia. Immunological deficits make individuals with ataxia telangiectasia more prone to recurrent infections, particularly sinus and lung infections with progressive deterioration of lung function. Increased risk of cancers such as leukaemia, lymphoma, and solid tumors further impact lifespan with life expectancy generally limited to 20–30 years of age in people with classic ataxia telangiectasia also called classical ataxia telangiectasia (the severe form with early-onset and rapidly progressing neurodegeneration) 1, 16.
Ataxia telangiectasia symptoms include:
- Ataxia (lack of coordination of movement)
- Unsteady walking and lack of balance
- Unintentional movement, such as tremor or jerky movement (myoclonus)
- Slurred speech
- Difficulty swallowing
- Difficulty coordinating eye movement
- Tiny, red “spider veins” or visible small linear red blood vessels (broken capillaries) called telangiectasias, on your eyes, ears, or cheeks
- Frequent lung infections
- Delayed physical and sexual development
- Increased sensitivity to ionizing radiation (such as X-rays or gamma rays)
- Diabetes
- Premature graying of the hair
- Fatigue
Ataxia-telangiectasia occurs in 1 in 40,000 to 1 in 100,000 people worldwide 17, 18. Ataxia telangiectasia is caused by mutations in the ATM (ataxia-telangiectasis mutated) gene located on chromosome 11q22-23 (long arm of the chromosome 11) 19, 20, 6, 21, 22. The ATM gene provides instructions for making ATM protein (a serine/threonine kinase) that is located primarily in the nucleus of cells, where it helps control the rate at which cells grow and divide and is involved in DNA repair 23, 10. ATM protein also plays an important role in the normal development and activity of several body systems, including the nervous system and the immune system. Additionally, the ATM protein assists cells in recognizing damaged or broken DNA strands. DNA can be damaged by agents such as toxic chemicals or radiation. Breaks in DNA strands also occur naturally when chromosomes exchange genetic material during cell division. The ATM protein coordinates DNA repair by activating enzymes that fix the broken strands. Efficient repair of damaged DNA strands helps maintain the stability of the cell’s genetic information. Because of its central role in cell division and DNA repair, the ATM protein is of great interest in cancer research.
The severity, disease course and rate of progression of the ataxia telangiectasia affects the average lifespan and ataxia telangiectasia life expectancy varies greatly. Ataxia-telangiectasia is a multi-system disease that affects a variety of body systems ranging from classic ataxia telangiectasia (the severe form) and variant ataxia telangiectasia (the milder form) 9. The classical ataxia telangiectasia is caused by biallelic deleterious ATM mutations, which lead to a total loss of ATM protein, while majority of patients with milder variant ataxia telangiectasia (atypical ataxia-telangiectasia) carry at least one missense or leaky splice site mutation (still producing the protein with residual function or kinase activity) 24. Moreover, some reports suggest that besides residual ATM kinase activity, other factors such as modifying genes and environmental factors might be involved in the presentation of milder phenotypes of ataxia telangiectasia 25.
Classic ataxia telangiectasia or classical ataxia telangiectasia is characterized by early childhood onset of progressive neurological signs and symptoms initially with cerebellar ataxia, followed typically by extrapyramidal involvement and peripheral sensorimotor neuropathy, immunodeficiency (associated with abnormalities of humoral immunity, cellular immunity, or combined immune deficiency), lung disease (resulting from recurrent lung infections, immune deficiency, aspiration, interstitial lung disease, and neurologic abnormalities), autoimmune or other chronic inflammatory diseases, increased serum alpha-fetoprotein (AFP) levels, radiosensitivity and increased risk of cancer 9. Most children are usually wheelchair-bound by age 10 years and die in the second decade of life due to cancers, lung disease, infections or respiratory failure 26, 27, 28.
Variant ataxia telangiectasia or atypical ataxia-telangiectasia patients have a significantly milder late-onset disease course 9. While cerebellar ataxia can be absent, extrapyramidal movement disorders are common (typically dystonia and dystonic tremor) and most individuals have manifestations of axonal sensorimotor polyneuropathy 9. In contrast to classic ataxia telangiectasia, immune function is generally normal, chest infections are not increased, and lung disease is not a major feature. Adults with variant ataxia telangiectasia or atypical ataxia-telangiectasia often do not have ocular telangiectasia 29. Therefore, the absence of ocular telangiectasia does not exclude the diagnosis of ataxia-telangiectasia. However, risk of developing cancers is increased in adults with variant ataxia telangiectasia, particularly in premenopausal females who have an increased risk of developing breast cancer and blood cancers (leukemia). People who have a later onset variant ataxia telangiectasia has a significantly milder disease course typically survive into their 50s 30, 24, 31. However, people with classic ataxia telangiectasia life expectancy is significantly reduced due to cancer, lung disease, and infections 9.
Ataxia telangiectasia individuals tend to have high amounts of a protein called alpha-fetoprotein (AFP) in their blood 32, 33. The level of alpha-fetoprotein (AFP) is normally increased in the bloodstream of pregnant women, but it is unknown why individuals with ataxia-telangiectasia have elevated alpha-fetoprotein (AFP) or what effects it has in these individuals.
People with ataxia-telangiectasia often have a weakened immune system, and many develop chronic lung infections. Some children with ataxia telangiectasia have an increased risk of developing diabetes and cancers, most frequently lymphoma and leukemia (acute lymphoblastic leukemia). Although it affects the brain, people with ataxia telangiectasia usually have normal or high intelligence. However, disturbances in cerebellar as well as non-cerebellar brain areas and networks may result in intellectual disability 9. Affected individuals are also very sensitive to the effects of ionizing radiation (x-ray and gamma ray), including medical x-rays and can result in severe side effects from such treatments.
Because ataxia telangiectasia is so rare, doctors may not be familiar with the symptoms or criteria for making a diagnosis 17. The late appearance of telangiectasia may also be a barrier to diagnosis 17. A diagnosis of ataxia telangiectasia can usually be made by the combination of clinical features and specific laboratory abnormalities. A variety of abnormal laboratory findings occur in most people with ataxia telangiectasia, but not all abnormalities are seen in all patients. These abnormalities are 17:
- Elevated and slowly increasing serum alpha-fetoprotein (AFP) levels after two years of age
- Low serum levels of immunoglobulins (IgA, IgG, IgG subclasses, IgE) and lymphopenia (particularly affecting T-lymphocytes)
- Spontaneous and X-ray induced chromosomal breaks and rearrangements in cultured lymphocytes and fibroblasts
- Reduced survival of cultured lymphocytes and fibroblasts after exposure to ionizing radiation 34
- Cerebellar atrophy detected by MRI
- The diagnosis of ataxia telangiectasia can be confirmed by the absence or deficiency of ATM protein and/or ATM kinase activity in cultured cell lines established from lymphocytes or skin biopsies 35, 36 or the identification of pathological mutations in the ATM gene. These more specialized tests are not always needed, but are particularly helpful if an individual’s symptoms are atypical. As whole exome sequencing becomes standard clinical practice for individuals with unusual and/or unexplained symptoms, it is likely that more people with mild forms of ataxia telangiectasia will be diagnosed 37.
There is no cure for ataxia telangiectasia and currently there’s no way to slow the progression. Treatment is symptomatic and supportive, such as physical therapy to help maintain flexibility and speech therapy to teach children how to control breathing. Additionally, high-dose vitamins, antioxidants, and gamma-globulin injections to strengthen the immune system.
Figure 1. Ataxia telangiectasia
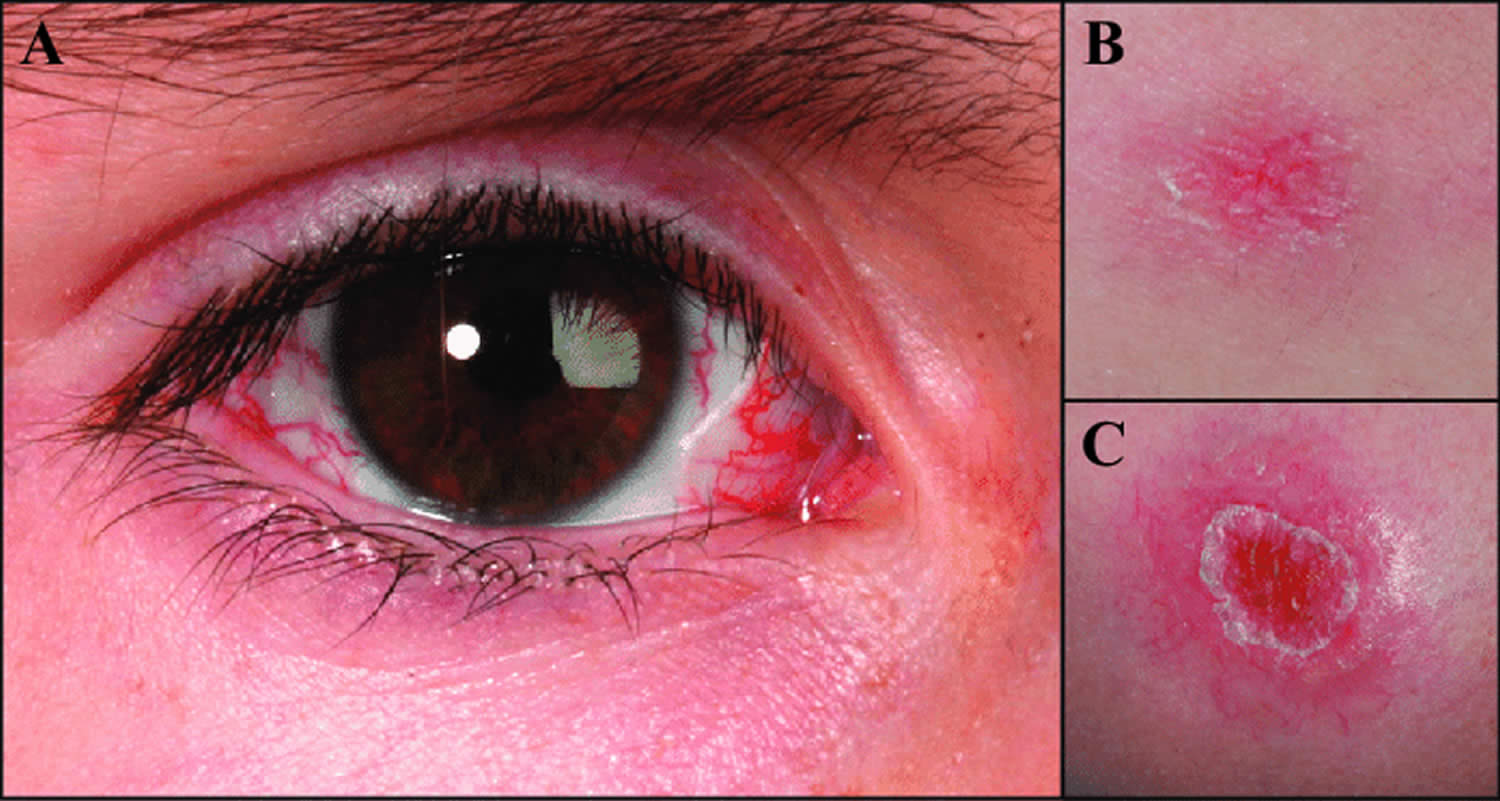
Footnotes: Clinical appearance of ataxia telangiectasia. (A) Telangiectasia visible in the eye of a female patient with ataxia telangiectasia. (B) Telangiectasia on the skin of the same patient. (C) Telangiectasia accompanied with scaling of the skin.
[Source 38 ]Figure 2. Eye telangiectasia in a person with ataxia telangiectasia

Footnotes: A man in early adolescence, born out of consanguineous marriage, presented with progressive gait unsteadiness and recurrent sinopulmonary and soft tissue infections for 5 years. On examination, he had bulbar conjunctival telangiectasia, oculomotor apraxia, bilateral cerebellar signs and bilateral, horizontal, coarse, gaze evoked nystagmus. Eye conjunctival telangiectasia do not bleed usually and they are sometimes misdiagnosed as chronic conjunctivitis. MRI of the brain revealed diffuse cerebellar atrophy. Laboratory investigations revealed elevated serum alfa-fetoprotein with a decreased serum IgA level. The patient was diagnosed with ataxia telangiectasia, which was confirmed with whole genome sequencing.
[Source 39 ]Classic ataxia telangiectasia vs Variant ataxia telangiectasia
| Classic ataxia telangiectasia | Variant ataxia telangiectasia | |
|---|---|---|
| Neurological Manifestations | Neurological deficits are typically observed during the toddler years resulting in wheelchair dependency around the age of 10. | Individuals have more mild neurological deficits in childhood with slower age-related neurodegeneration. The predominant neurological symptoms or symptoms to present first may be myoclonus, dystonia, choreoathetosis or tremor with ataxia appearing later 40, 41, 42. Oculomotor apraxia may also appear later or not at all 43. |
| Immunodeficiencies | Roughly two-thirds of people with classic ataxia telangiectasia suffer from some type of immunodeficiency and/or lymphopenia. | Immunodeficiencies do occur, but are less common. |
| Pulmonary Disease | Relatively common. | Less common. |
| Cancer | Although cancers in these individuals tend to occur at a younger age and are often lymphoid in nature, cancers in older individuals do occur and include both hematopoietic and non-hematopoietic cancers. | Cancers tend to appear later in life and include a higher proportion of non-hematopoietic cancers. The diagnosis of cancer can precede the diagnosis of ataxia telangiectasia. |
Who gets ataxia-telangiectasia?
Ataxia-telangiectasia may occur in any race or sex. Reported rates of incidence range from 1 in 40,000 to 1 in 100,000 births. The incidence of ataxia-telangiectasia is significantly higher when parents are consanguineous (a union between two individuals who are related as second cousins or closer), for example in the Bedouin population.
Ataxia telangiectasia cause
Ataxia telangiectasia is caused by mutations in the ataxia-telangiectasia mutated (ATM) gene located on chromosome 11q22-23 (long arm of the chromosome 11) 19, 20, 6, 21, 22. The ATM gene provides instructions for making ATM protein (a serine/threonine kinase) that is located primarily in the nucleus of cells, where it helps control the rate at which cells grow and divide and is involved in DNA repair 23, 10. This protein also plays an important role in the normal development and activity of several body systems, including the nervous system and the immune system. Additionally, the ATM protein assists cells in recognizing damaged or broken DNA strands. DNA can be damaged by agents such as toxic chemicals or radiation. Breaks in DNA strands also occur naturally when chromosomes exchange genetic material during cell division. The ATM protein coordinates DNA repair by activating enzymes that fix the broken strands. Efficient repair of damaged DNA strands helps maintain the stability of the cell’s genetic information. Because of its central role in cell division and DNA repair, the ATM protein is of great interest in cancer research.
Mutations in the ATM gene reduce or eliminate the function of the ATM protein. Without this protein, cells become unstable and die. Cells in the part of the brain involved in coordinating movements (the cerebellum) are particularly affected by loss of the ATM protein. The loss of these brain cells causes some of the movement problems characteristic of ataxia-telangiectasia. Mutations in the ATM gene also prevent cells from responding correctly to DNA damage, which allows breaks in DNA strands to accumulate and can lead to the formation of cancerous tumors.
Cells without any functional ATM protein are hypersensitive to radiation and do not respond normally to DNA damage. Instead of activating DNA repair, the altered ATM protein allows variants to accumulate in other genes, which may cause cells to grow and divide in an uncontrolled way. This kind of unregulated cell growth can lead to the formation of cancerous tumors. In addition, ATM gene variants can allow cells to die inappropriately, particularly affecting cells in a part of the brain involved in coordinating movements (the cerebellum). This loss of brain cells causes the movement problems characteristic of ataxia-telangiectasia.
Ataxia telangiectasia inheritance
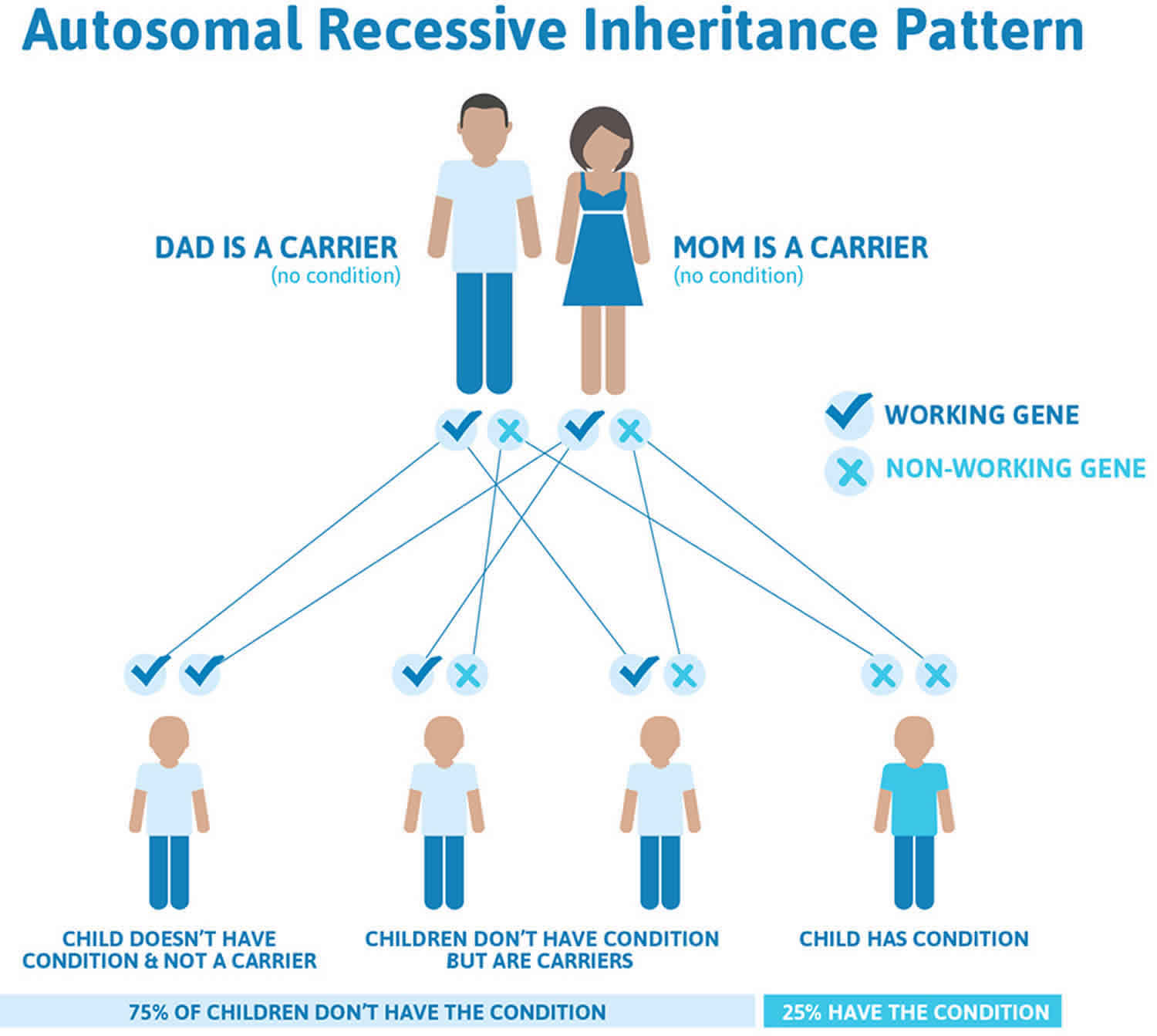
Ataxia-telangiectasia is inherited in an autosomal recessive pattern, which means both copies of the ATM gene in each cell have mutations 44. Most often, the parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but do not show signs and symptoms of the condition (see Figure 2). About 1 percent of the United States population carries one altered copy and one normal copy of the ATM gene in each cell. These individuals are called carriers. Although ATM gene mutation carriers do not have ataxia-telangiectasia, they are more likely than people without an ATM gene mutation to develop cancer; female carriers are particularly at risk for developing breast cancer. Carriers of a mutation in the ATM gene also may have an increased risk of heart disease.
If you are born to parents who both carry the same ATM gene, you have a 25% (1 in 4) chance of inheriting the ATM gene from both parents and developing ataxia-telangiectasia (see Figure 3). You have a 50% (1 in 2) chance of inheriting one variant ATM gene. This would make you ATM gene mutation carrier.
In other words, for a child born to a couple who both carry the ATM gene mutation (but do not have signs of disease), the expected outcome for each pregnancy is:
- A 25% chance that the child is born with two normal genes (healthy)
- A 50% chance that the child is born with one normal and one variant gene (carrier, without disease)
- A 25% chance that the child is born with two variant genes (at risk for the disease)
Figure 3. Ataxia-telangiectasia autosomal recessive inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://findageneticcounselor.nsgc.org) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://www.acmg.net/ACMG/Directories.aspx) has a searchable database of medical genetics clinic services in the United States.
Ataxia telangiectasia symptoms
Ataxia telangiectasia presents differently in each individual. There is high variability between people with ataxia telangiectasia and even siblings with ataxia telangiectasia. Not every child gets every symptom. Children with ataxia-telangiectasia appear normal at birth and it is not until they learn to walk at one or two years of age that symptoms become apparent. The severity of the signs and symptoms is variable. Ataxia (impaired balance or coordination that causes clumsy movements) results from the progressive degeneration of a part of the brain called the cerebellum, that gradually leads to a general lack of muscle control. By age 10 or 11 years most children will need a wheelchair not because their muscles are too weak, but because they cannot control them. Because of the worsening ataxia, children with ataxia telangiectasia lose their ability to write and speech also becomes slowed and slurred. Even reading eventually becomes impossible as eye movements become difficult to control.
Signs and symptoms of progressive neurological impairment include:
- An unsteady walk
- Abnormal, jerking clown-like movements
- Poor limb coordination
- Slow and slurred speech
- Dull, sad, inattentive facial features
- Growth delay
- Learning difficulties in one-third of patients.
The second major clinical sign and symptom of ataxia-telangiectasia is the development of telangiectasia or tiny red “spider” veins which appear in the corners of the eyes or on the surface of the ears and cheeks exposed to sunlight. These usually do not occur until the child is between 3 and 5 years and may not even be apparent until adolescence. The prominent blood vessels first appear around the corners of eyes and then spread to the ears and cheeks. Although these telangiectasia are seemingly harmless, their unique appearance together with ataxia is what led to naming this disease “ataxia-telangiectasia”.
People with ataxia-telangiectasia also have a weakened immune system or immunodeficiency, which makes them vulnerable to recurrent sinus and bronchial infections. In many patients, these infections can become life threatening. Because of low levels of immunoglobulins (IgG, IgA, IgM or IgG subclasses), the natural infection fighting agents in the blood, children with ataxia telangiectasia are highly susceptible to lung infections that do not respond to typical antibiotic treatments. For these ataxia telangiectasia patients, the combination of a weakened immune system and the progressive ataxia can ultimately lead to pneumonia as a common cause of death.
People with ataxia-telangiectasia are also at greater risk of getting cancers. Children with ataxia telangiectasia tend to develop cancers of the blood system almost 1,000 times more frequently than the general population. Lymphoma and leukemia are particularly common types of cancer, although the frequencies of most cancers are also increased.
Another aspect of ataxia telangiectasia is an extreme sensitivity to radiation, which means that ataxia telangiectasia patients cannot tolerate the standard levels of therapeutic radiation or radiomimetic drugs (chemotherapy drugs that work in a way that is similar to radiation therapy) usually given to cancer patients.
Other features of ataxia-telangiectasia that may affect some children are diabetes mellitus, premature graying of the hair, difficulty swallowing causing choking and/or drooling and slowed growth. Even though ataxia telangiectasia is a multi-system disorder, most individuals with ataxia telangiectasia are very socially aware and socially skilled.
Neurological problems
The onset of this ataxia marks the beginning of progressive degeneration of a part of the brain, known as the cerebellum, that gradually leads to a general lack of muscle control, and eventually confines the patient to a wheelchair. The first indications of ataxia in ataxia telangiectasia usually occur during the toddler years. Children with ataxia telangiectasia start walking at the typical age (about 12 months) but may not then improve much from their initial wobbly gait. Often they have problems standing or sitting still and tend to sway backward or from side to side. They often appear to have better balance when they run or walk quickly in comparison to when they walk slowly or stand in one place.
During the primary school years, children with typical forms of ataxia telangiectasia will seek assistance to walk and then start using a wheelchair, at first for long distances but eventually in place of all walking.
During school years, children have increasing difficulty with reading because of impaired coordination of eye movement. At the same time, fine motor functions (writing, coloring, eating with utensils, brushing of teeth and hair) may deteriorate. Most of these neurological problems stop progressing after the age of about 12-16 years.
Difficulties with speech articulation and phonation are often apparent in preschool years and may or may not worsen over time. Children often prefer not to speak in public or unfamiliar places but communicate more with family and friends.
Involuntary movements may start at any age and worsen over time. These extra movements can take many forms, including:
- Chorea (small jerks of the hands and feet that look like fidgeting)
- Athetosis (slower twisting movements of the upper body)
- Dystonia (adoption of stiff and twisted postures)
- Myoclonic jerks (occasional uncontrolled jerks)
- Tremors (various rhythmic movements with attempts at coordinated action)
Immunodeficiency (weakened immune system)
About two-thirds of people with ataxia telangiectasia have abnormalities of the immune system detected by the laboratory, but not all of them cause symptoms. The most common laboratory
abnormalities are:
- Low levels of one or more classes of immunoglobulins (IgG, IgA, IgM, or IgG subclasses)
- Impaired antibody responses to vaccines or infections
- Low numbers of lymphocytes (especially T-lymphocytes) in the blood
Immunodeficiency is one of the factors that can predispose people with ataxia telangiectasia to develop frequent infections of the upper (colds, sinusitus, and ear infections) and lower (bronchitis and pneumonia) respiratory tract.
Typically, the pattern of immunodeficiency seen in a child with ataxia telangiectasia by age 5 will be the same pattern seen throughout that person’s life. However, 10 to 20% of people with ataxia telangiectasia will have immunologic function deteriorate as they get older. It is worthwhile to reassess immune function if problems with infections become more severe at any age.
Additionally, if infections are in the lungs, assessing the person’s swallowing is important as swallowing incoordination may cause aspiration into the lungs leading to infections.
People with ataxia telangiectasia have an increased risk of developing autoimmune or chronic inflammatory diseases. This risk is probably a secondary effect of their immunodeficiency and not a direct effect of the lack of ATM protein. The most common examples of such disorders in ataxia telangiectasia include immune thrombocytopenia (ITP), arthritis, and vitiligo.
Lung disease
Respiratory symptoms and lung complications are common. Recurrent or chronic respiratory symptoms during the first few years of life can adversely affect lung function later in life. Children and adults with ataxia telangiectasia are at increased risk for a decline in lung function during respiratory illnesses, after anesthesia for a surgical procedure, and during treatment for cancers.
Chronic lung disease develops in more than 25 percent of people with ataxia telangiectasia. Three major types of lung disease can develop:
- Recurrent or chronic sinopulmonary infections and bronchiectasis, a condition in which bronchial tubes are permanently damaged, resulting in recurrent lower airway infections. These problems may be caused or made worse by immunodeficiency and aspiration.
- Inability to clear mucus because of ineffective cough and swallowing dysfunction. Difficulty taking deep breaths and an ineffective cough can make it difficult to clear oral and bronchial secretions. This can lead to prolonged respiratory symptoms following common viral respiratory illnesses.
- Restrictive interstitial lung disease or pulmonary fibrosis causes a small number of individuals to have decreased pulmonary reserve, trouble breathing, a need for supplemental oxygen and chronic cough in the absence of lung infections. Recurrent injury to the lungs caused by chronic infections or aspiration may cause lung fibrosis and scarring. The damage may be worsened because of inadequate tissue repair in ATM-deficient cells.
Some children and adults with ataxia telangiectasia have more than one type of lung disease at the same time. Many people will develop swallowing problems as they age which increases their risk of coughing, wheezing, or aspiration and other types of lung injury.
Lung disease may impair sleep efficiency in people with ataxia telangiectasia. This can cause fatigue with detrimental effects on many aspects of health. Sleep studies or polysomnography can help detect breathing problems such as upper airway obstruction, hypoxia and/or hypercarbia. If found, these conditions can be treated with supplemental oxygen alone or with non-invasive ventilation using CPAP (continuous positive airway pressure) or BiPAP (bilevel positive airway pressure). Recently an association has been reported between higher systemic levels of the proinflammatory cytokines interleukin 6 (IL6) and interleukin 8 (IL8) and lower lung function in children and young adults with ataxia telangiectasia. These findings suggest that inflammation may play a role in impairing lung function in people with ataxia telangiectasia.
Cancers
People with ataxia telangiectasia have a highly increased incidence (approximately 25% lifetime risk) of cancers 45, 46. Lymphomas and leukemias most often occur in people with classic ataxia telangiectasia less than 20 years of age, but adults are susceptible to both lymphoid tumors and a variety of solid tumors including breast, liver, gastric and esophageal carcinomas 17. An extensive analysis of the types of cancers that occur in both the classic and atypical ataxia telangiectasia has been performed on combined cohorts from the UK and the Netherlands 45.
Carriers, those who have one mutated copy of the ATM gene, such as the parents of a person with ataxia telangiectasia, are generally healthy 17. However, a systematic meta-analysis found that ATM mutation carriers have a reduced lifespan due to cancer (breast and gastrointestinal tract) and ischemic heart disease 47.
In particular, a mutated ATM gene is considered a moderate risk or moderate penetrance breast cancer susceptibility gene 48, 49. Female carriers are considered to have an approximately 2.3 fold increased risk for the development of breast cancer compared to the general population 49, 50, 51. A 2016 meta-analysis found the cumulative risk of breast cancer in mutated ATM gene carriers to be approximately 6% by age 50 and approximately 30% by age 80 52. Standard breast cancer surveillance, including monthly breast self-exams and mammography at the usual schedule for age, is recommended unless an individual has other risk factors (e.g., family history of breast cancer).
There is as yet no way to predict which individuals with ataxia telangiectasia will develop cancer, and unlike surveillance for many solid tumors (e.g. mammography, colonoscopy, PSA levels), there are no accepted methods to provide surveillance for lymphomas and leukemias. Hematopoietic cancer must be considered as a diagnostic possibility whenever potential symptoms (e.g. persistent swollen lymph nodes, unexplained fever) arise.
Radiation sensitivity
People with ataxia telangiectasia have an increased sensitivity to ionizing radiation (X-rays and gamma rays), which can be toxic to cells (cytotoxic). X-ray exposure should be limited to times when it is medically necessary for diagnostic purposes. Radiation therapy for cancer or any other reason is generally harmful for individuals with ataxia telangiectasia and should be performed only in rare circumstances and at reduced doses 53, 54. Although ataxia telangiectasia cells in culture have an altered DNA damage response to other genotoxic agents (e.g. ultraviolet [UV] light) 55, 56, individuals with ataxia telangiectasia do not have an increased incidence of skin cancer and can cope normally with sun exposure, so there is no need for special precautions for exposure to sunlight 17.
Feeding and swallowing problems
Feeding and swallowing (deglutition) may become difficult for people with ataxia telangiectasia as they age 57. Involuntary movements can make self-feeding difficult and result in messy or excessively prolonged mealtimes. In general, meals longer than 30 minutes may be stressful, interfere with other daily activities, and compromise hydration and nutritional intake.
Difficulty swallowing (dysphagia) is common in ataxia telangiectasia and typically appears during the second decade of life because of the neurological changes which interfere with the coordination of mouth and pharynx movements necessary for safe and efficient swallowing 57. Coordination problems involving the mouth may make chewing difficult and increase the duration of meals. Problems involving the pharynx may cause aspiration of liquid, food, and saliva. Difficulty swallowing (dysphagia) with concomitant silent aspiration may cause lung problems because of impaired clearance of food or liquids from the airway.
Difficulty swallowing (dysphagia) also can result in nutritional compromise because the process of eating becomes slow and difficult. Some people with ataxia telangiectasia stop eating or reduce their intake at meals because of frustration or fatigue with the process. Insufficient caloric intake may compromise growth in children and weight maintenance in older persons, contributing to lower body mass indices (BMI) in comparison to healthy, age-matched individuals 58, 59, 60, 61, 62. Poor nutrition may exaggerate the presentation of neurologic disability. Abnormal respiratory-swallowing coupling has been associated with an increased risk for aspiration and may signify swallowing problems prior to the development of nutritional and pulmonary sequelae in ataxia telangiectasia 63.
Warning signs of a problem with swallowing in people ataxia telangiectasia 17:
- Choking or coughing when eating or drinking
- Poor weight gain during ages of expected growth or weight loss at any age
- Excessive drooling
- Mealtimes longer than 40–45 min, on a regular basis
- Foods or drinks previously enjoyed are now refused or difficult
- Chewing problems
- Increase in the frequency or duration of breathing or respiratory problems
- Increase in lung infections
Poor growth
Poor growth is a common feature of ataxia telangiectasia 17. Nutritional compromise, infections and altered growth factor and hormone levels have been proposed to contribute to this growth impairment 64, 65. A study of endocrine abnormalities in an Israeli cohort of patients with ataxia telangiectasia demonstrated that growth impairment was present in infancy, prior to the onset of neurological symptoms and the nutritional problems commonly seen as children age. This study also showed that impaired growth was more prominent in females than males, and that this difference is apparent at an age before gonadotropins begin to affect growth rates 66.
Delayed pubertal development or gonadal dysgenesis
Infertility is often described as a facet of ataxia telangiectasia 17. In humans it may be more accurate to describe the reproductive abnormalities as gonadal atrophy or dysgenesis causing delayed pubertal development and early menopause 17. Abnormalities in gonadal development and function appear to be more prominent in females than males 66. Pregnancies in people with mild forms of ataxia telangiectasia has been reported 67, but not in anyone with the classic ataxia telangiectasia 17.
Insulin-resistant diabetes
A minority of patients with ataxia telangiectasia suffer from insulin resistant diabetes which typically appears as a late event during disease progression 17. Reduced insulin sensitivity and abnormal blood sugar levels (low or high blood sugar) may be observed in individuals with ataxia telangiectasia who do not have diabetes 68.
Hair and skin problems
Ataxia telangiectasia can cause features of early aging such as premature graying of the hair 69. People with ataxia telangiectasia can also have an increased prevalence of vitiligo, and warts that can be extensive and difficult to treat 70.
Sleep problems
Interestingly, unlike other neuromotor disorders, such as Duchenne Muscular Dystrophy, overnight polysomnography (sleep study) has not identified regular sleep-related gas exchange abnormalities in patients with ataxia telangiectasia. The majority of subjects studied were noted to have decreased sleep efficiency which has been associated with chronic disease states 71. Sleep efficiency refers to the percentage of time a person sleeps, in relation to the amount of time a person spends in bed. The percentage is calculated by dividing Total Sleep Time by Total Time in bed. Normal sleep efficiency is considered to be 80% or greater. For example, if a person spends 8 hours in bed (from 10 p.m. to 6 a.m), at least 6.4 hours or more should be spent sleeping to achieve an 80% or greater sleep efficiency. Most healthy and young adults have sleep efficiencies above 90%. adolescents who are wheelchair-bound with ataxia telangiectasia have mean sleep efficiency of 72.6% with a mean apnea hypopnea index (AHI) of 0.7 events/hr 71.
Cognitive problems
Very few neuropsychological studies have been performed in individuals with ataxia telangiectasia. One study performed in 2000 demonstrated deficits in the judgement of duration (i.e. the “judgement of explicit time intervals” or perceptual timing) 72.
Subsequent studies demonstrated that certain cognitive deficits appear relatively early in ataxia telangiectasia, then become broader and more profound during later stages of the disease 73, 74. In these studies specific impairments were observed in intellectual functioning, nonverbal memory, verbal abstract reasoning and calculation, and executive function. Pronounced deficits in perceptual timing were also observed; however language functioning was not impaired and “expressive language” was noted as a strength in children with ataxia telangiectasia, even during later stages of the disease. The cognitive impairments seen in ataxia telangiectasia have been found to be characteristic of Cerebellar Cognitive Affective Syndrome (CCAS) 75, 76.
Muscoloskeletal problems
Acquired deformity of the feet is common in people with ataxia telangiectasia (unpublished observations) and compounds the difficulty individuals have with walking due to impaired coordination 17. Scoliosis also occurs 77, but is relatively uncommon. Occasionally, individuals with ataxia telangiectasia develop contractures of the fingers, most often because of inflammatory connective tissue disease, but sometimes from neuropathy.
Older patients with ataxia telangiectasia
Certain problems occur with an unexpectedly high frequency in patients with ataxia telangiectasia who survive into their 20s and beyond.
Problems observed in aging or older people with ataxia telangiectasia 17:
- Ballistic, retropulsive or jerky movements
- Sensory and motor neuropathy
- Brain telangiectasia (observed by MRI)
- Restrictive lung disease
- Elevated cholesterol and triglyceride levels
- Glucose intolerance and diabetes
- Liver abnormalities (e.g. fatty liver; non-alcoholic cirrhosis; elevated serum transaminases)
- Changes in the types of cancers (there is an increased incidence for both lymphoid and solid tumors)
- Osteoporosis/osteopenia and low vitamin D levels
- Postural scoliosis and progressive foot deformities
- Gastroesophageal reflux (especially if reflux was an issue in infanthood)
- Early menopause
- Depression
- Aging parents and caregivers
Of particular note, liver abnormalities such as elevated serum transaminase levels, fatty liver disease and non-alcoholic cirrhosis including fibrotic changes have been observed as people with ataxia telangiectasia age, as have elevated triglyceride and cholesterol levels 66, 78, 79.
The spectrum of cancer is also different in older individuals with classic ataxia telangiectasia, as there is an increased risk for the development of both lymphoid cancers and solid tumors in ataxia telangiectasia over the age of 20 17.
Other problems
Some people with ataxia telangiectasia suffer from bladder and/or bowel incontinence that results from difficulties with transfers rather than due peripheral neuropathy 17. Some individuals also go through a period of recurrent vomiting which appears to be more prevalent in the mornings. This transient but repeated vomiting may correlate with the development of eye movement abnormalities, as people can have a sensation of motion sickness or dizziness with head movement 17. This symptom can be treated with drugs for motion sickness and usually resolves in a period of months, possibly as the eye movement abnormalities become more severe 80.
Ataxia telangiectasia diagnosis
Ataxia telangiectasia diagnosis depends on clinical suspicion with the combination of neurologic clinical features (ataxia, abnormal control of eye movement, and postural instability) with one or more of the following which may vary in their appearance: telangiectasia, frequent sinus and lung infections and specific laboratory abnormalities (e.g. IgA deficiency, lymphopenia especially affecting T lymphocytes and increased alpha-fetoprotein (AFP) levels).
The most important features of ataxia telangiectasia are 80:
- Neurological symptoms, particularly progressive cerebellar ataxia. This is normally apparent from an early age, often when children first start to sit or stand and is often manifested in a wobbly gait or swaying while sitting or standing. Although the age when they start to walk is normal, they remain unsteady, as if they had only just achieved this milestone. Unlike ataxia due to cerebral palsy, the problems will worsen over time with chorea, dystonia, and tremor.
- Abnormalities of the eye movements. Movements normally become restricted and following objects becomes difficult.
- Telangiectasia in the whites of the eyes or other areas of the face and ears, though this may not occur until 4 or 5 years of age.
- Recurrent sinus and lung infections, although these only affect around 50% of children with ataxia telangiectasia.
- Laboratory tests may also show an elevated serum alpha-fetoprotein (AFP) level and immunological deficiencies, particularly low levels of T cells and B cells and of one or more classes of immunoglobulin, most commonly IgA.
Because not all children develop in the same manner or at the same rate, the diagnosis of ataxia telangiectasia may not be made until the early school years when the neurologic symptoms (impaired gait, hand incoordination, abnormal eye movements), and the telangiectasia appear or become worse 17.
Ataxia telangiectasia diagnostic test
A diagnosis of ataxia telangiectasia can be confirmed by the finding of an absence or deficiency of the ATM protein or its kinase activity in cultured cell lines, and/or identification of the pathological mutations in the ATM gene.
Ataxia telangiectasia diagnosis is backed up by:
- Cytogenetic analysis (examination of chromosomes in a sample of tissue, blood, bone marrow, or amniotic fluid to look for changes in chromosomes) may help confirm the diagnosis. When a clinical diagnosis of ataxia telangiectasia has been made or there is a reasonable clinical suspicion of ataxia telangiectasia, genetic confirmation should be obtained by identifying the ATM mutations present.
- A diagnosis of ataxia telangiectasia is normally confirmed by the following laboratory tests:
- Chromosomal radiosensitivity test on peripheral blood lymphocytes
- Western blot on lymphoblastoid cell line to look at ATM protein expression and its kinase activity
- ATM gene mutation analysis
- If the previous tests show no abnormalities, expression of hMRE11 protein and aprataxin will be examined, to check for ataxia telangiectasia-like disorder and AOA1
As part of the diagnostic process, the following tests on a lithium heparin blood sample are carried out 80:
- A chromosomal radiosensitivity analysis is carried out on the blood lymphocytes, as sensitivity to ionising radiation is a characteristic of ataxia telangiectasia.
- A lymphoblastoid cell line (LCL) is made from the blood sample and a Western blot carried out to look for loss of ATM protein.
- If these two tests indicate the likelihood of ataxia telangiectasia, the whole of the patient’s ATM gene is sequenced in order to identify both mutations.
- If the Western blot reveals some residual ATM protein activity, as the result, for example, of a missense, or leaky splice-site mutation, an activity assay is also carried out to determine whether the ATM protein has some activity. There is a strong phenotype-genotype correlation in ataxia telangiectasia and patients with some residual ataxia telangiectasia kinase activity generally have a milder clinical course.
Ideally all these tests should be undertaken because, for example, some patients have no measurable increase in chromosomal radiosensitivity, and yet the western blot shows up a greatly reduced level of ATM protein. This is because the ATM present has some activity that is effective in reducing chromosome damage. Similarly some ataxia telangiectasia patients have normal levels of ATM protein on a western blot, but the radiosensitivity assay will indicate a lot of chromosome damage. This is because the mutant ATM protein expressed has no kinase activity. These laboratory tests are usually made available to the doctors at the specialist ataxia telangiectasia centers, as well as to the physician requesting the confirmation.
Immunologic evaluation
About two-thirds of people with ataxia telangiectasia have abnormalities of the immune system 70, 81. The most common abnormalities are low levels of one or more classes of immunoglobulin (IgG, IgA, IgM or IgG subclasses), failure to make antibodies in response to vaccines or infections, and lymphopenia, especially affecting T-lymphocytes. There are reduced numbers of new B cells leaving the bone marrow and new T cells leaving the thymus 82, reduced proportions of naive B and T cells, and reduced antigen receptor repertoire 81. A small percentage of people with ataxia telangiectasia also may have elevated levels of IgM in combination with IgG and/or IgA deficiency. When this is the presenting symptom in infant- or childhood, the diagnosis of ataxia telangiectasia can be confused with that of hyper-IgM syndrome 83. In the majority of individuals with ataxia telangiectasia, the immunologic abnormalities do not deteriorate over time, but approximately 10% will develop more severe problems most often with humoral immunity (humoral immunity produces antibodies by B lymphocytes) 70, 84.
All individuals with ataxia telangiectasia should have at least one comprehensive immunologic evaluation that measures:
- Levels of serum immunoglobulins (IgG, IgA, and IgM)
- Antibody responses to T-dependent (e.g., Pneumococcal conjugate such as Prevnar, Hemophilus influenzae b, tetanus) and T-independent (23-valent pneumococcal polysaccharide) vaccines
- Number and type of lymphocytes in the blood (CD4 and CD8 T-lymphocytes and B-lymphocytes)
If results show significant abnormalities of the immune system, an allergist or immunologist or infectious disease specialist will be able to discuss various treatment options, which might include the use of gamma globulin, prophylactic antibiotics and minimized exposure to infection.
Most people with ataxia telangiectasia have low lymphocyte counts in the blood, often specifically affecting a certain kind of lymphocyte called the CD4 T-cell. This seldom causes problems except for a tendency to have chronic or recurrent viral infections of the skin such as warts and molluscum contagiosum. Treatment for low CD4 cell number is seldom required but should be considered if a person with ataxia telangiectasia is treated with corticosteroid drugs such as prednisone for longer than a few weeks or is treated with chemotherapy for cancer. Under those circumstances, antibiotics may be recommended to prevent infections caused by a specific group of germs (opportunistic pathogens).
Sometimes vaccines can overcome various infections. Vaccines against common bacterial respiratory pathogens such as Hemophilus influenzae, pneumococci, and influenza virus are commercially available and often help to boost antibody responses, even in individuals with low immunoglobulin levels.
If vaccines do not work and the person with ataxia telangiectasia continues to have problems with infections, gamma globulin therapy (IV or subcutaneous infusions of antibodies collected from typical individuals) may help.
Neuroimaging findings
The neuropathological hallmark of ataxia telangiectasia is diffuse degeneration or atrophy of the cerebellar vermis and hemispheres, involving Purkinje cells and, to a lesser extent, granule neurons 17. Various neuropathological abnormalities (e.g. neuronal changes, gliosis and vascular changes) have also been observed in the cerebrum, brain stem and spinal cord 85, 86.
For the majority of people with ataxia telangiectasia, neuroimaging studies in the toddler years and early child years are normal 87. As the disease progresses, MRI studies support the pathological finding of variable, progressive and diffuse cerebellar atrophy 85. Between patients it is notable that the magnitude of volume loss correlates poorly with clinical features 17.
In addition to cerebellar atrophy, MRI studies have demonstrated cerebral, white matter abnormalities in older patients, including hemosiderin deposits and deep cerebral telangiectatic vessels, as well as degenerative changes in white matter corticomotor tracts extending from the cerebellum in younger patients with ataxia telangiectasia 88, 89, 90.
Magnetic resonance spectroscopy (MRS) studies to measure the levels of various brain metabolites have also been performed for ataxia telangiectasia, although with somewhat conflicting results 91, 92. Lin et al. 91 found decreased levels of all analyzed metabolites (N-acetyl aspartate [NAA], choline [Cho], and creatine [Cr]) in the cerebellar vermis with a trend towards decreased metabolite levels in the cerebellar hemispheres, whereas Wallis et al. 92 observed increased levels of Cho in the cerebellum of adults with ataxia telangiectasia.
A positron emission tomography (PET) study to measure brain glucose metabolism in individuals with ataxia telangiectasia has also been performed 93. Due to the radiation exposure inherent in PET imaging, participants in this study were restricted to 18 years of age or older. Although glucose metabolism was uniformly reduced in the cerebellum of patients with ataxia telangiectasia, increased metabolism observed in the globus pallidus was associated with decreased motor performance. Additional imaging studies are warranted; however, these results suggest that deep brain stimulation (DBS) targeting the pallidus may be a therapeutic option for ataxia telangiectasia 93.
Pre-implantation genetic diagnosis, antenatal diagnosis and carrier identification
Pre-implantation genetic diagnosis (PGD) can avoid the birth of an affected child. Pre-implantation genetic diagnosis (PGD) has been performed successfully for parents who have an affected child (or children) with ataxia telangiectasia, and at least two case reports appear in the literature 94, 95.
Antenatal diagnosis and carrier detection can be cost effectively performed in families if the ATM mutations in an affected child have been identified. Antenatal diagnosis can also be performed using haplotype analysis if an unambiguous diagnosis has been made for the affected child. In this case, DNA polymorphisms within and around the ATM gene can be utilized even if the pathogenic mutations are not known.
Carrier testing in the general population, i.e. attempting to identify disease causing mutations in the ATM gene of an unrelated individual (for example, the spouse of a known ataxia telangiectasia carrier), presents significant challenges 17. The ATM gene is extremely large and often contains polymorphisms which do not affect protein function. Clinicians cannot always predict if a specific variant will or will not cause disease 17.
Ataxia telangiectasia differential diagnosis
There are several other disorders with similar symptoms or laboratory features that physicians may consider when diagnosing ataxia telangiectasia 44. The three most common disorders that are sometimes confused with ataxia telangiectasia are: cerebral palsy, congenital ocular motor apraxia and Friedreich’s ataxia. Each of these can be distinguished from ataxia telangiectasia by the neurologic exam and clinical history 17.
There are also other rare disorders that can be confused with ataxia telangiectasia, either because of similar clinical features, a similarity of some laboratory features, or both. These include: ataxia oculomotor apraxia type 1 (AOA1), ataxia oculomotor apraxia type 2 (AOA2, also known as SCAR1), ataxia telangiectasia like disorder (ATLD) and Nijmegen breakage syndrome (NBS) 17.
Differentiation of these disorders is often possible with clinical features and selected laboratory tests. In cases where the distinction is unclear, DNA sequencing and/or protein assays (e.g. western blots or kinase assays to detect abnormal protein levels or activity) can be used to help make a definitive diagnosis 17.
Cerebral palsy
Cerebral palsy (CP) describes any non-progressive disorder of motor function stemming from malformation or early damage to the brain 96. Because most children suffering from ataxia telangiectasia have stable neurologic symptoms for the first 4 to 5 years of life, a misdiagnosis of cerebral palsy is not uncommon 86. However, milestones that have been accomplished and neurologic functions that have developed do not deteriorate in cerebral palsy as they often do in children with ataxia telangiectasia in the late pre-school years 17. In addition, most children with cerebral palsy manifest regional or diffuse spasticity in a pattern not seen in ataxia telangiectasia 17.
Those rare individuals that manifest a static disorder characterized by predominantly cerebellar features have been labeled as having “ataxic cerebral palsy” (a term of uncertain nosology) 17. Most individuals in this group do not begin walking at a normal age; however most children with ataxia telangiectasia do, although they often “wobble” from the start. Children with ataxia caused by cerebral palsy will not manifest the laboratory abnormalities associated with ataxia telangiectasia.
Congenital ocular motor apraxia
Congenital ocular motor apraxia (COMA; Cogan OMA) is a rare disorder of delayed development of visual saccades 97. Congenital ocular motor apraxia arises early and improves with time, whereas in ataxia telangiectasia similar saccadic difficulties worsen over time, typically in early school years 17.
Friedreich’s Ataxia
Friedreich’s Ataxia is the most common genetic cause of ataxia in children and the most prevalent autosomal recessive cerebellar ataxia 44. In Friedreich’s ataxia, ataxia typically appears between 10 and 15 years of age, and differs from ataxia telangiectasia by the absence of telangiectasia and oculomotor apraxia (trouble moving their eyes to look side-to-side), the early absence of tendon reflexes, a normal AFP, the frequent presence of scoliosis, and abnormal features on the EKG. Friedreich’s ataxia and ataxia telangiectasia also differ with regards to proprioception. Individuals with Friedreich’s ataxia manifest difficulty standing in one place that is much enhanced by closure of the eyes (positive Romberg sign). This is not characteristic of ataxia telangiectasia, even though those with ataxia telangiectasia may have greater difficulty standing in one place with their eyes open 86.
Ataxia-telangiectasia-like disorder (ATLD)
Ataxia-telangiectasia-like disorder (ATLD) is caused by mutations to the MRE11 gene and produces symptoms very similar to those of ataxia telangiectasia, especially neurological symptoms. Progression of symptoms seems to be somewhat slower than in classic ataxia telangiectasia.
Ataxia-oculomotor apraxia type 1 (AOA1)
Ataxia-oculomotor apraxia type 1 (AOA1) is caused by mutations to the APTX gene which produces a protein called Aprataxin. Like ataxia telangiectasia, it usually develops in childhood, and causes a similar range of movement and visual problems. However there are usually no associated immunological problems and telangiectasias do not appear to develop.
Ataxia-oculomotor apraxia type 2 (AOA2)
Ataxia-oculomotor apraxia type 2 (AOA2) has a range of symptoms similar to those of ataxia-oculomotor apraxia type 1 (AOA1), however it tends to develop later, typically in late adolescence or early teens. Ataxia-oculomotor apraxia type 2 (AOA2) is the result of mutations on the SETX gene. Ataxia-oculomotor apraxia type 2 (AOA2) seems to be a little more common than ataxia-oculomotor apraxia type 1 (AOA1).
Ataxia telangiectasia treatment
There is no cure for ataxia-telangiectasia. Currently no treatment exists to slow down the progression of the disease. The management of ataxia-telangiectasia is aimed at treating symptoms as they arise, preventing complications and most importantly providing support and education to both patients and their families. This may include physiotherapy, speech therapy, and antibiotics for infection.
Death typically occurs in early or middle adolescence, usually from bronchopulmonary infection, less frequently from malignancy, or from a combination of both. The median age at death in ataxia-telangiectasia is reported to be approximately 20 years. The longest reported survival is 34 years.
Neurologic management
There is no treatment known to slow or stop the progression of the neurologic deficits associated with ataxia telangiectasia. Physical, occupational and speech therapies as well as exercise may help maintain function but will not slow the course of neurodegeneration. Therapeutic exercises should not be used to the point of fatigue and should not interfere with activities of daily life.
Certain anti-Parkinson and anti-epileptic drugs may be useful in the management of symptoms. Commonly prescribed drugs include trihexyphenidyl (Artane), amantadine 98, baclofen and BOTOX injections. Less commonly prescribed drugs that also may be beneficial include clonazepam 99, gabapentin and pregabalin (Lyrica) 87. Various drugs, (e.g. Riluzole), have shown improvement in other cerebellar disorders 100. Nicotinamide riboside, a form of vitamin B3, at 25 mg/kg/day (maximum dose of 900 mg/day), has significantly reduced ataxia scores (i.e., improved the motor disorder) in a single trial with 24 individuals with both classic and variant ataxia telangiectasia 101.
The effectiveness of pharmacotherapy in movement disorders in ataxia telangiectasia is low to moderate. Only a few non-randomized studies have investigated the treatment of movement disorders in individuals with ataxia telangiectasia specifically 102, 103, 101, 104, 105, 106. However, to date, their efficacy and the features of motor impairment that would best be targeted in ataxia telangiectasia are not known. All drugs should be prescribed by a neurologist familiar with the assessment and treatment of individuals with movement disorders.
Dystonia, the most troublesome movement disorder in ataxia telangiectasia, can vary in distribution and severity and varies among affected individuals.
- Focal dystonia. As in individuals with torticollis, botulinum toxin A (Botox) is the treatment of first choice.
- Generalized dystonia. Anticholinergic drugs and GABA mimetics can be helpful.
- Generalized, dopa-responsive dystonia. A trial with levodopa may be useful in some individuals 107.
- Deep brain stimulation (DBS) of the globus pallidus pars interna, described to date in two individuals with ataxia telangiectasia and dystonia, had conflicting results 108.
Respiratory management
Recognizing and treating causes of chronic lung disease can minimize sickness and delay onset of respiratory symptoms 109. To slow or prevent the development of chronic lung disease in ataxia telangiectasia, early intervention for respiratory symptoms is recommended. Pulmonary function testing should be performed in all children starting at 6 years of age and continued on an annual basis 17. Although pulmonary function tests can be difficult to perform in this population due to bulbar weakness and delayed initiation of inspiratory breaths, studies have demonstrated that with adjustments to the technique, reproducible spirometry can be performed in most people with ataxia telangiectasia 110, 111, 109.
Given the complexity of the respiratory complications of ataxia telangiectasia, it is strongly recommended that all children are cared for by a respiratory pediatrician in the local tertiary regional center.
General high quality respiratory care is essential includes avoidance of environmental tobacco smoke and full immunisation, including annual influenza immunization.
In people with chronic or persistent respiratory symptoms unresponsive to therapy, consideration should be given to lung imaging to diagnose unsuspected bronchiectasis, fibrosis, interstitial lung disease and tumors of the chest 17. Low dose chest and sinus CT are currently available which can minimize exposure to ionizing radiation 109. Alternatively, magnetic resonance imaging (MRI) can be used in people with ataxia telangiectasia to identify lung abnormalities 112. However, use of MRI may require anesthesia in younger patients.
No current evidence supports respiratory muscle training and/or cough augmentation but should be considered in an individual child if there is a weak or discoordinate cough.
The major respiratory complications of ataxia telangiectasia are:
- Acute and chronic respiratory tract infection, with the risk of bronchiectasis, related to immunodeficiency and poor secretion clearance
- Aspiration syndromes, related to incoordinated swallowing, which can lead to bronchiectasis
- Scoliosis, especially in adolescence
- Respiratory muscle weakness
- Interstitial lung disease (ILD) (much more rarely)
- Restrictive and obstructive lung disease may develop after chemotherapy treatment for cancers.
Infection
Liberal use of antibiotics should be considered in people with ataxia telangiectasia who have persistent upper and lower respiratory tract symptoms 17. As with cystic fibrosis (CF), people with ataxia telangiectasia who are colonized with or who intermittently grow bacteria from their respiratory secretions are more likely to develop bronchiectasis and have more frequent respiratory exacerbations triggered by respiratory viral illnesses 17.
Administration of antibiotics should be considered when children and adults have prolonged respiratory symptoms (greater than 7 days) following a respiratory illness, including those that begin with a viral illness 17. Antibiotic treatment also should be considered in children with chronic coughs that are productive of mucus, those who do not respond to aggressive pulmonary clearance techniques and in children with muco-purulent secretions from the sinuses or chest 17. Examination of respiratory secretions by induced sputum or bronchoscopy may direct antibiotic therapy to treat lower respiratory tract infections and prevent the development of bronchiectasis.
There is no data to recommend, or otherwise, prophylactic antibiotics, but most children are recommended prophylactic azithromycin by the immunologists. There are no data on the microbiology of ataxia telangiectasia lung disease but experience in one of the biggest clinics suggests that H influenzae, M catarrhalis, Strep pneumoniae, Staph aureus and occasionally Pseudomonas are the main pathogens when the culture is positive.
Experts recommend additional antibiotics under the following circumstances:
- Any increase in respiratory symptoms, especially chronic productive cough, irrespective of whether there are any abnormalities heard with the stethoscope. Culture of respiratory secretions
should be performed, and airway clearance techniques reviewed. Blind treatment with oral antibiotics should be commenced, guided by previous cultures. If there are no previous results which are helpful, then blind treatment with amoxicillin-clavulanic acid or another antibiotic which covers H Influenzae, M Catarrhalis, Strep pneumoniae and Staph aureus should be given. Experts recommend the use of high doses (formulary ‘serious infection’ dose) for 2-4 weeks continuing until the child has returned to baseline for at least 7 days especially when the family feels that the child is more or less returned to baseline. Antibiotics can be changed depending on the culture results. - Any positive culture should be treated with 2-4 weeks of an appropriate oral antibiotic as above, even if the child is asymptomatic
- If the response to oral antibiotics is inadequate, or if the child is very unwell, admission for intravenous antibiotics and intensive airway clearance is mandated. Choice of intravenous antibiotics will depend on cultures or best guess. Isolation of Pseudomonas aeruginosa should be treated with a cystic fibrosis (CF)-protocol eradication regime, for example three weeks oral ciprofloxacin and three months nebulised colistin.
- In a child with a chronic productive cough despite trials of antibiotics, especially if culture negative, consideration should be given to induced sputum sample or fibreoptic bronchoscopy and
bronchoalveolar lavage (BAL) to obtain material for culture. Opportunistic infections are rare in ataxia telangiectasia but, if suspected, early fibreoptic bronchoscopy and bronchoalveolar lavage (BAL) is mandated - Children with ataxia telangiectasia are also prone to sinusitis and otitis media, and these should also be treated with prolonged courses of antibiotics.
Reversible airflow obstruction
Documentation of an acute response to bronchodilators is not uncommon and ataxia telangiectasia does not protect a child from also developing asthma. There is no evidence that prescribing inhaled corticosteroids (ICS) to children with ataxia telangiectasia and reversible airflow obstruction but no risk factors for asthma, is beneficial 80. It is suggested that if a trial of inhaled corticosteroid is contemplated, it should be for a finite period with definite end-points, before the child is committed to long-term therapy. It should be noted that there is increasing evidence that inhaled corticosteroids may increase the risk of airway infection in other contexts, and hence there is a reason for caution for long-term use 80.
Aspiration
Suspicion should be aroused if there are symptoms such as cough during eating, or failure to swallow saliva. The expertise of an experienced speech and language therapist should be sought. If the child has an unsafe swallow, gastrostomy or jejunostomy feeding is advised. A videofluoroscopy with limited radiation exposure should be required if there is suspicion of silent aspiration 80. Enteral feeding is also mandated if the child, while not actually having an unsafe swallow, takes such a long time to eat that nutrition is not maintained 80.
Interstitial lung disease
Interstitial lung disease is rare, but should be suspected if the child has a persistent dry cough, breathlessness, persistent crackles in the absence of respiratory infection, or oxygen desaturation 80. The evidence base for an investigation pathway is even scantier, but since the treatment is with high dose oral corticosteroids, most would advocate obtaining a tissue diagnosis. This would involve a limited low dose CT scan followed by video-assisted thoracoscopic surgery (VATS) or open lung biopsy. Such evidence as exists suggests that early treatment with oral corticosteroids is most beneficial, so diagnosis and treatment should be aggressively pursued at an early stage 80.
Immune problems
All individuals with ataxia telangiectasia should have at least one comprehensive immunologic evaluation that measures the number and type of lymphocytes in the blood (T-lymphocytes and B-lymphocytes), the levels of serum immunoglobulins (IgG, IgA, and IgM) and antibody responses to T-dependent (e.g., tetanus, Hemophilus influenzae b) and T-independent (23-valent pneumococcal polysaccharide) vaccines. For the most part, the pattern of immunodeficiency seen in an ataxia telangiectasia patient early in life (by age five) will be the same pattern seen throughout the lifetime of that individual 70, 84. Therefore, tests of immune function need not be repeated unless that individual develops more problems with infection. If infections are occurring in the lung, it is also important to investigate the possibility of dysfunctional swallow with aspiration.
Antibody deficiency
Immunological abnormalities observed in ataxia telangiectasia include deficiencies of immunoglobulin classes A (IgA) and E (IgE) and occasionally immunoglobulin G (IgG), with a tendency to
high IgM levels. Occasionally a picture of hyper IgM syndrome has been described 113. There is poor responsiveness to pneumococcal polysaccharide vaccine (PPV) but fairly good responses to pneumococcal conjugate vaccine (PCV). Reduced lymphocyte numbers affecting T and B cells but not NK cells is also seen. Amongst T cells, the naïve CD4 CD45 RA population seems to be most depressed and T cells bearing gamma delta T cell receptors may be increased. Spectratyping of T cell receptor repertoires show some abnormal skewing of different V beta families in some individuals. Studies of functional T cell responses have shown very variable results with reduced T cell proliferative responses in some individuals.
In common with other immunodeficiency states associated with poor T cell immunity, autoimmune phenomena may occur. Vitiligo is the most common. Autoimmune haemolytic anemia has been described as a problem in the small number of ataxia telangiectasia patients with a very severe immunodeficiency. Non-infective granulomatous skin disease is a particularly difficult condition to treat. The cause of this is uncertain. Searches for triggering microbes are usually negative.
Problems with low immunity can sometimes be overcome by immunization. Vaccines against common bacterial respiratory pathogens such as Hemophilus influenzae, pneumococci and influenza viruses are commercially available and often help to boost antibody responses, even in individuals with low immunoglobulin levels. If the individual continues to have problems with infections, gamma globulin therapy (IV or subcutaneous infusions) may be of benefit. The need for additional immunizations (especially with pneumococcal and influenza vaccines), antibiotics to provide prophylaxis from infections, and/or gamma globulin therapy should be determined by an expert in the field of immunodeficiency or infectious diseases.
In people with ataxia telangiectasia who have low levels of IgA, further testing should be performed to determine if the IgA level is low or completely absent. If IgA is absent, there is a slight, albeit debatable, increase in the risk for a transfusion reaction. “Medical Alert” bracelets are not necessary, but the family and primary physician should be aware that if there is an elective surgery requiring red cell transfusion, the cells should be washed to decrease the risk of an allergic reaction.
The decision to commence immunoglobulin in ataxia telangiectasia is generally taken on clinical grounds because of recurrent infections usually associated with a low IgG level. About 15% of individuals with ataxia telangiectasia will require Immunoglobulin replacement. Standard dosages are used but since ataxia telangiectasia patients are very unlikely to be completely IgG deficient,
and endogenous production is likely to continue, monitoring of trough IgG levels is less useful in determining dosages than in other antibody-deficient patients. Subcutaneous administration has shown to be both efficacious and acceptable to patients on replacement therapy.
Gammopathy/elevated immunoglobulin levels
A small number of people with ataxia telangiectasia develop an abnormality in which one or more types of immunoglobulin are increased far beyond the normal range. In a few cases, the immunoglobulin levels can be increased so much that it causes hyperviscosity 114. Therapy for this problem must be tailored to the specific abnormality found and its severity.
Lymphopenia
Many people with ataxia telangiectasia have low lymphocyte counts in the blood (lymphopenia). This problem seems to be relatively stable with age, but seldom causes susceptibility to opportunistic infections. The one exception is that problems with chronic or recurrent warts and molluscum contagiosum are relatively common 70.
The number and function of T-lymphocytes should be re-evaluated if a person with ataxia telangiectasia is treated with corticosteroid drugs such as prednisone for longer than a few weeks or is treated with chemotherapy for cancer. If lymphocyte counts are low in people taking those types of drugs, the use of prophylactic antibiotics is recommended to prevent opportunistic infections 17.
Vaccination
If antibody function is normal, all routine childhood immunizations including live viral vaccines (measles/mumps/rubella (MMR) and varicella-zoster virus (VZV) vaccines) should be given, except for those with profound lymphopenia. The MMR (measles/mumps/rubella) vaccine may be related to the development of chronic skin sores called granulomas in a very small number of people with ataxia telangiectasia 115. Chronic cutaneous granulomas occur in less than 10% of people with ataxia telangiectasia. These lesions have not been associated with an identifiable pathogen or other cause 116, but can on occasion be painful, bleed, or erode down to muscle or bone. Treatments have included high potency topical corticosteroids and/or cyclosporine A for small superficial lesions 17. More extensive granulomas may respond to combination therapy (e.g. topical steroids plus IV gamma globulin therapy) 117, systemic inhibitors of tumor necrosis factor (TNF-alpha) 118 or direct injection of steroids into the site of the granulomatous lesions 119.
Severe varicella infection in patients with ataxia telangiectasia can occur but most patients contracting the infection have a mild illness. Nevertheless, there is the risk of severe infection and varicella encephalitis which, as it most commonly affects the cerebellum, will exacerbate the neurological condition 17. Varicella-zoster virus (VZV) vaccine is therefore recommended in all cases that have not already contracted the natural disease (chickenpox). The exception would be those rare cases with very profound T cell lymphopaenia (CD3 count of <500) in whom there would be concerns of vaccine-associated disease.
Experts recommend special attention to vaccines that can prevent influenza (the “flu”) and some forms of pneumonia. Annual influenza vaccination is recommended for all ataxia telangiectasia patients since influenza may be particularly problematic not only for those with immunodeficiency but also in those with neurological disease. Experts also recommend giving influenza vaccine to ataxia telangiectasia sufferers who are on immunoglobulin replacement therapy 80. The rational for this is that administered immunoglobulin will not contain antibodies against new antigenic variants
of influenza. Furthermore, even those ataxia telangiectasia patients on immunoglobulin are likely to have some retained ability to mount an antibody response.
Vaccine recommendations for ataxia telangiectasia 17:
- If a person with ataxia telangiectasia does not need gamma globulin replacement therapy, he/she should receive all standard childhood vaccines.
- The individual with ataxia telangiectasia and all household members should receive the influenza (flu) vaccine every fall.
- People with ataxia telangiectasia who are less than two years old should receive three doses of a pneumococcal conjugate vaccine (Prevnar) given at two month intervals.
- People older than two years who have not previously been immunized with pneumococcal conjugate vaccine (Prevnar) should receive two doses of Prevnar.
- At least 6 months after the last pneumococcal conjugate vaccine (Prevnar) has been given, and after the child is at least two years old, the 23-valent pneumococcal vaccine (Pneumovax23) should be administered. Immunization with the 23-valent pneumococcal vaccine (Pneumovax23) should be repeated approximately every five years after the first dose.
Pneumococcal disease is a serious bacterial infection caused by Streptococcus pneumoniae bacteria or pneumococcus that commonly live in the nose and throat and cause both mild (ear infections) and serious infections (pneumonia).
There are 2 types of pneumococcal vaccines used in the United States 120, 121:
- Pneumococcal conjugate vaccines (PCVs). A conjugate vaccine is a type of vaccine that joins a protein to an antigen (in the case of pneumococcal vaccines, the protein is connected to unique polysaccharides [long chains of sugar molecules] from the surface of each of the pneumococcal serotypes). The conjugate vaccines have the polysaccharides for different serotypes attached (or conjugated) to a carrier protein. The protein helps improve the quality of the immune system response to the vaccine compared to the response to an unconjugated polysaccharide (PPV). Immune response to pneumococcal conjugate vaccine (PCV) is a T-cell dependent response that produces memory B-cells and reduces carriage of the bacteria in the respiratory track. Pneumococcal conjugate vaccines (PCVs) are given to children younger than 5 years old and to older children who need it. Vaccine providers also give pneumococcal conjugate vaccines (PCVs) to adults 65 years or older and other adults who need it.
- Pneumococcal polysaccharide vaccine (PPV). A polysaccharide vaccine is a type of vaccine that is composed of long chains of sugar molecules called polysaccharides, that resemble the surface of certain serotypes of pneumococcal bacteria in order to help the immune system mount a response. The immune response to the Pneumovax23 (PPSV23) vaccine is a T-cell independent immune response but does not reduce bacterial carriage. Vaccine providers may give Pneumovax23 (PPSV23) to children 2 through 18 years old with certain medical conditions. Vaccine providers give it to adults who receive PCV15 (Vaxneuvance). They also may give it to adults who have received an earlier vaccine called PCV13 (Prevnar 13). PCV13 (Prevnar 13) is FDA-licensed and may still be available in some clinics. PCV13 (Prevnar 13) is no longer routinely recommended; however, CDC guidance allows for its use as previously recommended in situations where PCV15, PCV20, or PCV21 is indicated but unavailable and the alternative is that the patient would not be vaccinated 125.
- PPSV23 (Pneumovax23) helps protect against 23 types of Streptococcus pneumoniae bacteria 126. Following the 2022 changes to the pneumococcal vaccination schedule for adults, PPSV23 (Pneumovax23) is no longer recommended alone, however PPSV23 (Pneumovax23) is recommended for adults following PCV13 (Prevnar 13) or PCV15 (Vaxneuvance) vaccination. PPSV23 (Pneumovax23) is not recommended for people who have previously received a PCV20 (Prevnar 20) or PCV21 (Capvaxive) vaccination.
Each of these vaccines helps protect against specific serotypes, or strains of Streptococcus pneumoniae bacteria. The number at the end of the vaccine name tells how many serotypes the pneumococcal vaccine includes.
The Centers for Disease Control and Prevention (CDC) recommends routine pneumococcal vaccination for all children younger than 5 years old 127.
Administer a 4-dose pneumococcal conjugate vaccine series (PCV15 [Vaxneuvance] or PCV20 [Prevnar 20]), 1 dose at each of the following ages 127:
- 2 months
- 4 months
- 6 months
- with a booster at age 12 through 15 months
Catch-up guidance
Vaccinate children younger than 5 years of age who miss their shots or start the pneumococcal conjugate vaccine series later than recommended. The number of doses recommended and the intervals between doses will depend on the child’s age when vaccination begins. Otherwise healthy children who fall behind should be given catch-up vaccination through age 59 months; if they have certain underlying medical conditions they should be given catch-up vaccination through age 71 months.
Children may be at increased risk for febrile seizures if a pneumococcal conjugate vaccine is administered with inactivated influenza vaccine. However, clinicians may give either pneumococcal conjugate vaccine at the same time as an influenza vaccine.
Currently, no data from clinical trials are available for co-administration of Pneumovax23 (PPSV23) with other childhood vaccines during the same visit.
Side effects of pneumonia vaccine
Redness, swelling, pain, or tenderness where the pneumonia vaccine is given, and fever, loss of appetite, fussiness (irritability), feeling tired, headache, muscle aches, joint pain, and chills can happen after pneumococcal conjugate vaccination (PCV) 128.
Young children may be at increased risk for seizures caused by fever after a pneumococcal conjugate vaccine (PCV) if it is administered at the same time as inactivated influenza vaccine. Ask your doctor for more information.
People sometimes faint after medical procedures, including vaccination. Tell your doctor if you feel dizzy or have vision changes or ringing in the ears. As with any medicine, there is a very remote chance of a vaccine causing a severe allergic reaction, other serious injury, or death 128.
An allergic reaction could occur after the vaccinated person leaves the clinic. If you see signs of a severe allergic reaction (hives, swelling of the face and throat, difficulty breathing, a fast heartbeat,
dizziness, or weakness), call your local emergency services number and get the person to the nearest hospital. For other signs that concern you, see your doctor.
Cancer management
The lifetime risk of developing a cancer in ataxia telangiectasia is around 22% in the UK. T and B cell leukemias and lymphomas can occur but leukemias are more common. Carcinomas and brain tumors also occur. The special problems of managing cancer in the context of ataxia telangiectasia are sufficiently complicated that treatment should be performed only in academic oncology centers and after consultation with physicians who have specific expertise in ataxia telangiectasia. For example, standard cancer treatment regimens need to be modified to avoid the use of radiation therapy and radiomimetic drugs, as these are particularly cytotoxic for people with ataxia telangiectasia 129. The use of cyclophosphamide must be monitored very carefully because it has been associated with severe hemorrhage from telangiectasia that develop in the bladder 130. Even with treatment modifications, for some individuals with ataxia telangiectasia and advanced stage cancers toxicity may still pose significant problems 131.
There are two reports in the literature of successful bone marrow transplants (BMTs) for the treatment of T-cell acute lymphoblastic leukemia (T-ALL) and non-Hodgkin lymphoma in individuals with ataxia telangiectasia 132, 133. However, the use of bone marrow transplant (BMT) for the treatment of blood cancers (leukemias) associated with ataxia telangiectasia is an area of active discussion.
Eye and vision problems
Eye muscle surgery can correct the strabismus that is common in people with ataxia telangiectasia and help improve quality of life 17. Drugs that may improve other eye abnormalities, such as 4-amino pyridine for nystagmus and vestibular deficits 134, have not been rigorously prescribed or tested in patients with ataxia telangiectasia.
Musculoskeletal problems
Early treatment of foot deformities may slow their progression. Bracing or surgical correction sometimes improves stability at the ankle sufficient to enable an individual to walk with support, or bear weight during assisted standing transfers from one seat to another. Severe scoliosis is relatively uncommon, but probably does occur more often than in those without ataxia telangiectasia. Spinal fusion is only rarely indicated.
Endocrine problems
Young adults with ataxia telangiectasia may develop insulin-resistant diabetes mellitus and high cholesterol 135, 136, which can be treated following protocols for the general population. However, the shortened life expectancy of individuals with classic ataxia telangiectasia can result in the decision not to treat high cholesterol levels, since treatment will not have any expected clinical consequences 9.
In females with gonadal failure (in case of primary or secondary amenorrhea), estrogen supplementation can prevent osteoporosis 65.
Growth hormone treatment may be an option for children with severe growth failure 137.
Most children with ataxia telangiectasia have difficulty in school because of a delay in response time to visual, verbal or other cues, dysarthria, oculomotor apraxia and impaired fine motor control 17. Despite these problems, children with ataxia telangiectasia often enjoy school if proper accommodations to their disability can be made. The decision about the need for special education classes or extra help in regular classes is highly influenced by the local resources available. Decisions about proper educational placement should be revisited as often as circumstances warrant. Despite their many neurologic impairments, most individuals with ataxia telangiectasia are very socially aware and socially skilled, and benefit from sustained peer relationships developed at school 17. Some individuals are able to function quite well despite their disabilities and a few have graduated from college 17.
Many of the problems encountered will benefit from special attention, as problems are often related more to “input and output” issues than to intellectual impairment 17. Problems with eye movement control make it difficult for people with ataxia telangiectasia to read, yet most fully understand the meaning and nuances of text that is read to them. Delays in speech initiation and lack of facial expression make it seem that they do not know the answers to questions. Reduction of the skilled effort needed to answer questions, and an increase of the time available to respond, is often rewarded by real accomplishment. It is important to recognize that intellectual disability is not regularly a part of the clinical picture of ataxia telangiectasia although school performance may be suboptimal because of the many difficulties in reading, writing, and speech. Children with ataxia telangiectasia are often very conscious of their appearance, and strive to appear normal to their peers and teachers.
Life within the ataxic body can be tiring. The enhanced effort needed to maintain appearances and increased energy expended in abnormal tone and extra movements all contribute to physical and mental fatigue 17. As a consequence, for some a shortened school day yields real benefits.
General recommendations for the education and socialization of children with ataxia telangiectasia 17:
- All children with ataxia telangiectasia need special attention to the barriers they experience in school. In the United States, this takes the form of a formal IEP (Individualized Education Program).
- Children with ataxia telangiectasia tend to be excellent problem solvers. Their involvement in how to best perform tasks should be encouraged.
- Speech-language pathologists may facilitate communication skills that enable persons with ataxia telangiectasia to get their messages across (using key words vs. complete sentences) and teach strategies to decrease frustration associated with the increased time needed to respond to questions (e.g., holding up a hand) and inform others about the need to allow more time for responses. Traditional speech therapies that focus on the production of specific sounds and strengthening of the lip and tongue muscles are rarely helpful.
- Classroom aides may be appropriate, especially to help with scribing, transportation throughout the school, mealtimes and toileting. The impact of an aide on peer relationships should be monitored carefully.
- Physical therapy is useful to maintain strength and general cardiovascular health. Horseback therapy and exercises in a swimming pool are often well-tolerated and fun for people with ataxia telangiectasia. However, no amount of practice will slow the cerebellar degeneration or improve neurologic function. Exercise to the point of exhaustion should be avoided.
- Hearing is normal throughout life. Books on tape may be a useful adjunct to traditional school materials.
- Early use of computers (preschool) with word completion software should be encouraged.
- Practicing coordination (e.g. balance beam or cursive writing exercises) is not helpful.
- Occupational therapy is helpful for managing daily living skills.
- Allow rest time, shortened days, reduced class schedule, reduced homework, modified tests as necessary.
- Like all children, those with ataxia telangiectasia need to have goals to experience the satisfaction of making progress.
- Social interactions with peers are important, and should be taken into consideration for class placement. For everyone, long-term peer relationships can be one of the most rewarding parts of life; for those with ataxia telangiectasia establishing these connections in school years can be helpful.
Genetic counseling
Genetic counseling can provide education for families regarding the feasibility and potential consequences of genetic testing for ataxia telangiectasia in siblings and other family members. Genetic counseling can also help with the interpretation of test results.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://findageneticcounselor.nsgc.org) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://www.acmg.net/ACMG/Directories.aspx) has a searchable database of medical genetics clinic services in the United States.
Surveillance
To monitor existing signs and symptoms of ataxia telangiectasia, the individual’s response to supportive care, and the emergence of new signs and symptoms, the evaluations summarized in Table 1 are recommended.
Note the recommended surveillance is the same for individuals with classic ataxia telangiectasia and variant ataxia telangiectasia, with the exception that individuals who do not have evidence of lung disease at the time of the initial diagnosis do not require annual screening for pulmonary disease.
Table 1. Ataxia-telangiectasia recommended surveillance
| System/Concern | Evaluation | Frequency/Timing |
|---|---|---|
| Neurologic | Eval by neurologist for response to therapy for existing findings & development of new findings If child has severe/profound intellectual disability, seek additional cause. | Annually More frequently if problems are present or suspected |
| Educational needs | Screening for cognitive functioning & any speech-language issues | Before becoming school age; once school age, annually More frequently if problems are present or suspected |
| Behavior | Monitoring for social-emotional development | When starting kindergarten & again when entering secondary school |
| Activity of daily living/Musculoskeletal | By PT, OT, &/or rehab specialist | Per rehab team |
| Dysarthria/Communication | By speech-language pathologist | Per treating speech-language pathologist |
| Oculomotor problems | By ophthalmologist | Only if indicated |
| Immunodeficiency | By immunologist (immunoglobulin levels, white blood cell count) | Annually More frequently if problems are present or suspected |
| Infection | By immunologist | |
| Pulmonary disease | By pulmonologist Lung function testing (by spirometry) | Annually for persons w/evidence of disease at time of initial diagnosis More frequently if problems are present or suspected |
| Increased susceptibility to malignancy | Clinical assessment for signs/symptoms of leukemia &/or lymphoma incl for lymphadenopathy & unexplained fever | Annually |
| Blood count & smear, immunoglobulin levels, M protein, lactate dehydrogenase, IgM | Annually More frequently if problems are present or suspected Immediate referral to oncologist if malignancy is diagnosed or suspected | |
| Ultrasound exam of abdomen in adulthood | Annually | |
| Breast MRI in females | Annually starting at age 25 yrs More frequently if problems are present or suspected | |
| Endocrine abnormalities | Assess length/height in children. | Annually in childhood More frequently if problems are present or suspected |
| Assess age-appropriate pubertal development. | Annually More frequently if problems are present or suspected | |
| Diabetes screening: urinalysis, fasting blood glucose concentration, hemoglobin A1c | Annually in adults More frequently if problems are present or suspected | |
| Feeding/Nutrition | By speech-language pathologist/nutritionist | Annually More frequently if problems are present or suspected |
| Family support & resources | All health care providers should pay attention to the well-being of persons w/A-T & their families. | At each visit |
Ataxia telangiectasia prognosis
Historically, individuals with ataxia telangiectasia succumbed to their disease in childhood or the teenage years 17. However, the average life expectancy for individuals with ataxia telangiectasia has improved and continues to improve with advances in care. In 2006, the average life expectancy was reported to be approximately 25 years 138. The two most common causes of death are chronic lung disease (about one-third of cases) and cancer (about one-third of cases) 17.
Ataxia telangiectasia life expectancy
The severity of the ataxia telangiectasia affects the average lifespan and ataxia telangiectasia life expectancy varies greatly. While the rarity of ataxia telangiectasia makes it difficult to evaluate, the most recent and authoritative paper suggests a median survival age of around 25 years 139. Ataxia-telangiectasia is a continuum ranging from classic ataxia telangiectasia (the severe form) and variant ataxia telangiectasia (the milder form) 9. People who have a later onset variant ataxia telangiectasia has a significantly milder disease course typically survive into their 50s. However, people with classic ataxia telangiectasia life expectancy is significantly reduced due to cancer, lung disease, nonspecific pulmonary failure and infections 9, 140. While there is no published evidence, many patients with mild variant ataxia telangiectasia are known to be living into their 40s and 50s and some even into their 60s in
the UK 80. Around 22% of people with ataxia telangiectasia die of cancer. The majority of other deaths are likely to be due to lung disease 141.
- Petley E, Yule A, Alexander S, Ojha S, Whitehouse WP. The natural history of ataxia-telangiectasia (A-T): A systematic review. PLoS One. 2022 Mar 15;17(3):e0264177. doi: 10.1371/journal.pone.0264177[↩][↩][↩]
- Moeini Shad T, Yazdani R, Amirifar P, Delavari S, Heidarzadeh Arani M, Mahdaviani SA, Sadeghi-Shabestari M, Aghamohammadi A, Rezaei N, Abolhassani H. Atypical Ataxia Presentation in Variant Ataxia Telangiectasia: Iranian Case-Series and Review of the Literature. Front Immunol. 2022 Jan 14;12:779502. doi: 10.3389/fimmu.2021.779502[↩]
- Schon K, van Os NJH, Oscroft N, Baxendale H, Scoffings D, Ray J, Suri M, Whitehouse WP, Mehta PR, Everett N, Bottolo L, van de Warrenburg BP, Byrd PJ, Weemaes C, Willemsen MA, Tischkowitz M, Taylor AM, Hensiek AE. Genotype, extrapyramidal features, and severity of variant ataxia-telangiectasia. Ann Neurol. 2019 Feb;85(2):170-180. doi: 10.1002/ana.25394[↩]
- Gupta AS, Luddy AC, Khan NC, Reiling S, Thornton JK. Real-life Wrist Movement Patterns Capture Motor Impairment in Individuals with Ataxia-Telangiectasia. Cerebellum. 2023 Apr;22(2):261-271. doi: 10.1007/s12311-022-01385-5[↩]
- Khan M, Cassidy E, Parkin T, Wallace A, Carter B, Paton J, Donohue K, Mitchell S, Quin G, McNarry N, Hartley H, Bailey H, Whitehouse W, Medd R, Zahidi A, McMullan M, Bunn L. The Care and Management of Children and Young People with Ataxia Telangiectasia Provided by Nurses and Allied Health Professionals: a Scoping Review. Cerebellum. 2024 Apr;23(2):722-756. doi: 10.1007/s12311-023-01555-z[↩]
- Jackson T.J., Chow G., Suri M., Byrd P., Taylor M. R., Whitehouse W. P., Longitudinal analysis of the neurological features of ataxia-telangiectasia. Developmental Medicine & Child Neurology, 2016. 58(7): p. 690–7. doi: 10.1111/dmcn.13052[↩][↩][↩]
- Ataxia Telangiectasia. https://www.ninds.nih.gov/health-information/disorders/ataxia-telangiectasia[↩]
- Rothblum-Oviatt C., et al., Ataxia telangiectasia: a review. Orphanet Journal Of Rare Diseases, 2016. 11(1): p. 159. doi: 10.1186/s13023-016-0543-7[↩]
- Veenhuis S, van Os N, Weemaes C, et al. Ataxia-Telangiectasia. 1999 Mar 19 [Updated 2023 Oct 5]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK26468[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Ataxia-telangiectasia. https://medlineplus.gov/genetics/condition/ataxia-telangiectasia[↩][↩][↩]
- Ataxia – telangiectasia. https://medlineplus.gov/ency/article/001394.htm[↩]
- Lavin MF, Gueven N, Bottle S, Gatti RA. Current and potential therapeutic strategies for the treatment of ataxia-telangiectasia. Br Med Bull. 2007;81–82:129–147. doi: 10.1093/bmb/ldm012[↩]
- Nissenkorn A, Ben-Zeev B. Ataxia telangiectasia. Handb Clin Neurol. 2015;132:199-214. doi: 10.1016/B978-0-444-62702-5.00014-7[↩]
- Vinck A., Verhagen M. M., Gerven Mv, de Groot I. J., Weemaes C. M., Maassen B. A, et al., Cognitive and speech-language performance in children with ataxia telangiectasia. Developmental neurorehabilitation, 2011. 14(5): p. 315–22. doi: 10.3109/17518423.2011.603368[↩]
- Hoche F., et al., The Cerebellar Cognitive Affective Syndrome in Ataxia-Telangiectasia. Cerebellum, 2019. 18(2): p. 225–244. doi: 10.1007/s12311-018-0983-9[↩]
- Claes K, Depuydt J, Taylor AMR, Last JI, Baert A, Schietecatte P, et al.. Variant Ataxia Telangiectasia: Clinical and Molecular Findings and Evaluation of Radiosensitive Phenotypes in a Patient and Relatives. Neuromolecular Med (2013) 15:447–57. doi: 10.1007/s12017-013-8231-4[↩]
- Rothblum-Oviatt C, Wright J, Lefton-Greif MA, McGrath-Morrow SA, Crawford TO, Lederman HM. Ataxia telangiectasia: a review. Orphanet J Rare Dis. 2016 Nov 25;11(1):159. doi: 10.1186/s13023-016-0543-7[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Swift M, Morrell D, Cromartie E, Chamberlin AR, Skolnick MH, Bishop DT. The incidence and gene frequency of ataxia-telangiectasia in the United States. Am J Hum Genet. 1986 Nov;39(5):573-83. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1684065/pdf/ajhg00147-0017.pdf[↩]
- Savitsky K, Sfez S, Tagle DA, Ziv Y, Sartiel A, Collins FS, Shiloh Y, Rotman G. The complete sequence of the coding region of the ATM gene reveals similarity to cell cycle regulators in different species. Hum Mol Genet. 1995 Nov;4(11):2025-32. doi: 10.1093/hmg/4.11.2025[↩][↩]
- Gatti RA, et al. Localization of an ataxia-telangiectasia gene to chromosome 11q22-23. Nature. 1988;336(6199):577–80. doi: 10.1038/336577a0[↩][↩]
- Chaudhary MW, Al-Baradie RS. Ataxia-Telangiectasia: Future Prospects. Appl Clin Genet (2014) 7:159. doi: 10.2147/TACG.S35759[↩][↩]
- Ambrose M, Gatti RA. Pathogenesis of Ataxia-Telangiectasia: The Next Generation of ATM Functions. Blood (2013) 121:4036–45. doi: 10.1182/blood-2012-09-456897[↩][↩]
- ATM gene. https://medlineplus.gov/genetics/gene/atm[↩][↩]
- Verhagen MM, Last JI, Hogervorst FB, Smeets DF, Roeleveld N, Verheijen F, et al.. Presence of ATM Protein and Residual Kinase Activity Correlates With the Phenotype in Ataxia-Telangiectasia: A Genotype–Phenotype Study. Hum Mutat (2012) 33:561–71. doi: 10.1002/humu.22016[↩][↩]
- Rothblum-Oviatt C, Wright J, Lefton-Greif MA, McGrath-Morrow SA, Crawford TO, Lederman HM. Ataxia Telangiectasia: A Review. Orphanet J rare Dis (2016) 11:159. doi: 10.1186/s13023-016-0543-7[↩]
- Amirifar P, Ranjouri MR, Yazdani R, Abolhassani H, Aghamohammadi A. Ataxia-Telangiectasia: A Review of Clinical Features and Molecular Pathology. Pediatr Allergy Immunol (2019) 30:277–88. doi: 10.1111/pai.13020[↩]
- Micol R, Slama LB, Suarez F, Le Mignot L, Beauté J, Mahlaoui N, et al.. Morbidity and Mortality From Ataxia-Telangiectasia are Associated With ATM Genotype. J Allergy Clin Immunol (2011) 128:382–389. e1. doi: 10.1016/j.jaci.2011.03.052[↩]
- Moeini Shad T, Ranjouri M, Amirifar P. Clinical Manifestations in Iranian Ataxia Telangiectasia Patients. Immunol Genet J (2020) 3:29–40. doi: 10.22034/igj.2020.224536.1034[↩]
- Petley E, Yule A, Alexander S, et al. The natural history of ataxia-telangiectasia (A-T): a systematic review. PLoS One 2022;17:e0264177. doi:10.1371/journal.pone.0264177[↩]
- Verhagen M, Abdo W, Willemsen M, Hogervorst F, Smeets D, Hiel J, et al.. Clinical Spectrum of Ataxia-Telangiectasia in Adulthood. Neurology (2009) 73:430–7. doi: 10.1212/WNL.0b013e3181af33bd[↩]
- van Os NJ, Jansen AF, van Deuren M, Haraldsson A, van Driel NT, Etzioni A, et al.. Ataxia-Telangiectasia: Immunodeficiency and Survival. Clin Immunol (2017) 178:45–55. doi: 10.1016/j.clim.2017.01.009[↩]
- Chun HH, Gatti RA. Ataxia-telangiectasia, an evolving phenotype. DNA Repair (Amst). 2004 Aug-Sep;3(8-9):1187-96. doi: 10.1016/j.dnarep.2004.04.010[↩]
- Taylor AM, Byrd PJ. Molecular pathology of ataxia telangiectasia. J Clin Pathol. 2005 Oct;58(10):1009-15. doi: 10.1136/jcp.2005.026062[↩]
- Sun X, et al. Early diagnosis of ataxia-telangiectasia using radiosensitivity testing. J Pediatr. 2002;140(6):724–31. doi: 10.1067/mpd.2002.123879[↩]
- Chun HH, et al. Improved diagnostic testing for ataxia-telangiectasia by immunoblotting of nuclear lysates for ATM protein expression. Mol Genet Metab. 2003;80(4):437–43. doi: 10.1016/j.ymgme.2003.09.008[↩]
- Taylor AM, Byrd PJ. Molecular pathology of ataxia telangiectasia. J Clin Pathol. 2005;58(10):1009–15. doi: 10.1136/jcp.2005.026062[↩]
- Bower, M., Diagnostic Yield of a Targeted Next Generation Sequencing Approach in a Young Adult Population: High Frequency of Recessive Ataxias and Implentation of a Next Generation Sequencing Copy-Number Variation Algorithm. 5th Ataxia Investigators Meeting (AIM 2014), Las Vegas, NV, March 18–21, 2014[↩]
- Knoch J, Kamenisch Y, Kubisch C, Berneburg M. Rare hereditary diseases with defects in DNA-repair. Eur J Dermatol. 2012 Jul-Aug;22(4):443-55. doi: 10.1684/ejd.2012.1654[↩]
- Chakraborty U, Chandra A, Dasgupta S. Eye in ataxia telangiectasia. BMJ Case Rep. 2023 Oct 5;16(10):e256865. https://casereports.bmj.com/content/16/10/e256865.long[↩]
- Saunders-Pullman R, et al. Variant ataxia-telangiectasia presenting as primary-appearing dystonia in Canadian Mennonites. Neurology. 2012;78(9):649–57. doi: 10.1212/WNL.0b013e3182494d51[↩]
- Churchyard A, Stell R, Mastaglia FL. Ataxia telangiectasia presenting as an extrapyramidal movement disorder and ocular motor apraxia without overt telangiectasia. Clin Exp Neurol. 1991;28:90-6.[↩]
- Termsarasab P, Yang AC, Frucht SJ. Myoclonus in ataxia-telangiectasia. Tremor Other Hyperkinet Mov (N Y). 2015 Mar 13;5:298. doi: 10.7916/D88P5Z9X[↩]
- Verhagen MM, et al. Presence of ATM protein and residual kinase activity correlates with the phenotype in ataxia-telangiectasia: a genotype-phenotype study. Hum Mutat. 2012;33(3):561–71. doi: 10.1002/humu.22016[↩]
- Anheim M, Tranchant C, Koenig M. The autosomal recessive cerebellar ataxias. N Engl J Med. 2012;366(7):636–46. doi: 10.1056/NEJMra1006610[↩][↩][↩]
- Reiman A, et al. Lymphoid tumours and breast cancer in ataxia telangiectasia; substantial protective effect of residual ATM kinase activity against childhood tumours. Br J Cancer. 2011;105(4):586–91. doi: 10.1038/bjc.2011.266[↩][↩]
- Suarez F, et al. Incidence, presentation, and prognosis of malignancies in ataxia-telangiectasia: a report from the French national registry of primary immune deficiencies. J Clin Oncol. 2015;33(2):202–8. doi: 10.1200/JCO.2014.56.5101[↩]
- van Os NJ, et al. Health risks for ataxia-telangiectasia mutated heterozygotes: a systematic review, meta-analysis and evidence-based guideline. Clin Genet. 2016;90(2):105–17. doi: 10.1111/cge.12710[↩]
- Hollestelle A, et al. Discovering moderate-risk breast cancer susceptibility genes. Curr Opin Genet Dev. 2010;20(3):268–76. doi: 10.1016/j.gde.2010.02.009[↩]
- Economopoulou P, Dimitriadis G, Psyrri A. Beyond BRCA: new hereditary breast cancer susceptibility genes. Cancer Treat Rev. 2015 Jan;41(1):1-8. doi: 10.1016/j.ctrv.2014.10.008[↩][↩]
- Thompson D, et al. Cancer risks and mortality in heterozygous ATM mutation carriers. J Natl Cancer Inst. 2005;97(11):813–22. doi: 10.1093/jnci/dji141[↩]
- Renwick A, et al. ATM mutations that cause ataxia-telangiectasia are breast cancer susceptibility alleles. Nat Genet. 2006;38(8):873–5. doi: 10.1038/ng1837[↩]
- Marabelli M, Cheng SC, Parmigiani G. Penetrance of ATM gene mutations in breast cancer: A meta-analysis of different measures of risk. Genet Epidemiol. 2016;40(5):425–31. doi: 10.1002/gepi.21971[↩]
- Hart RM, et al. Radiotherapeutic management of medulloblastoma in a pediatric patient with ataxia telangiectasia. Int J Radiat Oncol Biol Phys. 1987;13(8):1237–40. doi: 10.1016/0360-3016(87)90200-8[↩]
- DeWire MD, et al. Radiation therapy and adjuvant chemotherapy in a patient with a malignant glioneuronal tumor and underlying ataxia telangiectasia: a case report and review of the literature. J Clin Oncol. 2013;31(1):e12–4. doi: 10.1200/JCO.2011.40.1430[↩]
- Hannan MA, et al. Deficiency in the repair of UV-induced DNA damage in human skin fibroblasts compromised for the ATM gene. Carcinogenesis. 2002;23(10):1617–24. doi: 10.1093/carcin/23.10.1617[↩]
- Shiloh Y. ATM: expanding roles as a chief guardian of genome stability. Exp Cell Res. 2014;329(1):154–61. doi: 10.1016/j.yexcr.2014.09.002[↩]
- Lefton-Greif MA, et al. Oropharyngeal dysphagia and aspiration in patients with ataxia-telangiectasia. J Pediatr. 2000;136(2):225–31. doi: 10.1016/S0022-3476(00)70106-5[↩][↩]
- Boder E, Sedgwick R. Ataxia telangiectasia: a review of 101 cases, in little club clinics in developmental medicine No. 8. London: Heinemann Books; 1963. pp. 110–118.[↩]
- Moin M, et al. Ataxia-Telangiectasia in Iran: Clinical and Laboratory Features of 104 Patients. Pediatr Neurol. 2007;37(1):21–28. doi: 10.1016/j.pediatrneurol.2007.03.002[↩]
- Schubert R, Reichenbach J, Zielen S. Growth factor deficiency in patients with ataxia telangiectasia. Clin Exp Immunol. 2005;140(3):517–9. doi: 10.1111/j.1365-2249.2005.02782.x[↩]
- Kieslich M, et al. Extracerebellar MRI-lesions in ataxia telangiectasia go along with deficiency of the GH/IGF-1 axis, markedly reduced body weight, high ataxia scores and advanced age. Cerebellum. 2010;9(2):190–7. doi: 10.1007/s12311-009-0138-0[↩]
- Woods CG, Taylor AM. Ataxia telangiectasia in the British Isles: the clinical and laboratory features of 70 affected individuals. Q J Med. 1992 Feb;82(298):169-79.[↩]
- Lefton-Greif MA, et al. Assessment of impaired coordination between respiration and deglutition in children and young adults with ataxia telangiectasia. Dev Med Child Neurol. 2016;58(10):1069–75. doi: 10.1111/dmcn.13156[↩]
- Voss S, et al. Growth retardation and growth hormone deficiency in patients with Ataxia telangiectasia. Growth Factors. 2014;32(3–4):123–9. doi: 10.3109/08977194.2014.939805[↩]
- Ehlayel M, Soliman A, De Sanctis V. Linear growth and endocrine function in children with ataxia telangiectasia. Indian J Endocrinol Metab. 2014 Nov;18(Suppl 1):S93-6. doi: 10.4103/2230-8210.145079[↩][↩]
- Nissenkorn A, et al. Endocrine abnormalities in ataxia telangiectasia: findings from a national cohort. Pediatr Res. 2016;79(6):889–94. doi: 10.1038/pr.2016.19[↩][↩][↩]
- Worth PF, et al. Very mild presentation in adult with classical cellular phenotype of ataxia telangiectasia. Mov Disord. 2013;28(4):524–8. doi: 10.1002/mds.25236[↩]
- Connelly PJ, et al. Recessive mutations in the cancer gene Ataxia Telangiectasia mutated (ATM), at a locus previously associated with metformin response, cause dysglycaemia and insulin resistance. Diabet Med. 2016;33(3):371–5. doi: 10.1111/dme.13037[↩]
- Crawford TO. Ataxia telangiectasia. Semin Pediatr Neurol. 1998;5(4):287–94. doi: 10.1016/S1071-9091(98)80007-7[↩]
- Nowak-Wegrzyn A, et al. Immunodeficiency and infections in ataxia-telangiectasia. J Pediatr. 2004;144(4):505–11. doi: 10.1016/j.jpeds.2003.12.046[↩][↩][↩][↩][↩]
- McGrath-Morrow SA, et al. Polysomnographic values in adolescents with ataxia telangiectasia. Pediatr Pulmonol. 2008;43(7):674–9. doi: 10.1002/ppul.20838[↩][↩]
- Mostofsky SH, et al. Judgment of duration in individuals with ataxia-telangiectasia. Dev Neuropsychol. 2000;17(1):63–74. doi: 10.1207/S15326942DN1701_04[↩]
- Vinck A, et al. Cognitive and speech-language performance in children with ataxia telangiectasia. Dev Neurorehabil. 2011;14(5):315–22. doi: 10.3109/17518423.2011.603368[↩]
- Hoche F, et al. Cognitive phenotype in ataxia-telangiectasia. Pediatr Neurol. 2014;51(3):297–310. doi: 10.1016/j.pediatrneurol.2014.04.027[↩]
- Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain. 1998;121(Pt 4):561–79. doi: 10.1093/brain/121.4.561[↩]
- Hoche F, et al. The cerebellar cognitive affective syndrome (CCAS) in children with ataxia telangiectasia (A-T) Orlando: Ataxia Investigators Meeting, National Ataxia Foundation; 2016.[↩]
- Gatti R, Perlman S, et al. Ataxia-telangiectasia. In: Pagon RA, Pagon RA, et al., editors. GeneReviews(R) Seattle: University of Washington; 1993.[↩]
- Weiss B, et al. Liver disease in pediatric patients with ataxia telangiectasia: a novel report. J Pediatr Gastroenterol Nutr. 2016;62(4):550–5. doi: 10.1097/MPG.0000000000001036[↩]
- Andrade IG, et al. Risk of atherosclerosis in patients with ataxia telangiectasia. Ann Nutr Metab. 2015;66(4):196–201. doi: 10.1159/000430790[↩]
- Ataxia-Telangiectasia in Children: Guidance on Diagnosis and Clinical Care. https://atsociety.org.uk/wp-content/uploads/2017/10/A-T_Clinical_Guidance_Document_Final.pdf[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Driessen GJ, et al. Antibody deficiency in patients with ataxia telangiectasia is caused by disturbed B- and T-cell homeostasis and reduced immune repertoire diversity. J Allergy Clin Immunol. 2013;131(5):1367–1375. doi: 10.1016/j.jaci.2013.01.053[↩][↩]
- Kraus M, et al. Disturbed B and T cell homeostasis and neogenesis in patients with ataxia telangiectasia. J Clin Immunol. 2014;34(5):561–72. doi: 10.1007/s10875-014-0044-1[↩]
- Noordzij JG, et al. Ataxia-telangiectasia patients presenting with hyper-IgM syndrome. Arch Dis Child. 2009;94(6):448–9. doi: 10.1136/adc.2008.149351[↩]
- Chopra C, et al. Immune deficiency in Ataxia-Telangiectasia: a longitudinal study of 44 patients. Clin Exp Immunol. 2014;176(2):275–82. doi: 10.1111/cei.12262[↩][↩]
- Sahama I, et al. Radiological imaging in ataxia telangiectasia: a review. Cerebellum. 2014;13(4):521–30. doi: 10.1007/s12311-014-0557-4[↩][↩]
- Boder E. Ataxia-telangiectasia: an overview. Kroc Found Ser. 1985;19:1-63.[↩][↩][↩]
- Hoche F, et al. Neurodegeneration in ataxia telangiectasia: what is new? What is evident? Neuropediatrics. 2012;43(3):119–29. doi: 10.1055/s-0032-1313915[↩][↩]
- Lin DD, et al. Cerebral abnormalities in adults with ataxia-telangiectasia. AJNR Am J Neuroradiol. 2014;35(1):119–23. doi: 10.3174/ajnr.A3646[↩]
- Sahama I, et al. Altered corticomotor-cerebellar integrity in young ataxia telangiectasia patients. Mov Disord. 2014;29(10):1289–98. doi: 10.1002/mds.25970[↩]
- Sahama I, et al. Motor pathway degeneration in young ataxia telangiectasia patients: a diffusion tractography study. Neuroimage Clin. 2015;9:206–15. doi: 10.1016/j.nicl.2015.08.007[↩]
- Lin DD, et al. Proton MR spectroscopic imaging in ataxia-telangiectasia. Neuropediatrics. 2006;37(4):241–6. doi: 10.1055/s-2006-924722[↩][↩]
- Wallis LI, Griffiths PD, Ritchie SJ, Romanowski CA, Darwent G, Wilkinson ID. Proton spectroscopy and imaging at 3T in ataxia-telangiectasia. AJNR Am J Neuroradiol. 2007 Jan;28(1):79-83. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8134102[↩][↩]
- Volkow ND, et al. Brain glucose metabolism in adults with ataxia-telangiectasia and their asymptomatic relatives. Brain. 2014;137(Pt 6):1753–61. doi: 10.1093/brain/awu092[↩][↩]
- Hellani A, et al. Pregnancy after preimplantation genetic diagnosis for ataxia telangiectasia. Mol Hum Reprod. 2002;8(8):785–8. doi: 10.1093/molehr/8.8.785[↩]
- Verlinsky Y, et al. Preimplantation diagnosis for immunodeficiencies. Reprod Biomed Online. 2007;14(2):214–23. doi: 10.1016/S1472-6483(10)60790-0[↩]
- Herskind A, Greisen G, Nielsen JB. Early identification and intervention in cerebral palsy. Dev Med Child Neurol. 2015;57(1):29–36. doi: 10.1111/dmcn.12531[↩]
- Salman MS, Ikeda KM. The syndrome of infantile-onset saccade initiation delay. Can J Neurol Sci. 2013;40(2):235–40. doi: 10.1017/S0317167100013792[↩]
- Nissenkorn A, et al. Movement disorder in ataxia-telangiectasia: treatment with amantadine sulfate. J Child Neurol. 2013;28(2):155–60. doi: 10.1177/0883073812441999[↩]
- van Egmond ME, et al. Myoclonus in childhood-onset neurogenetic disorders: The importance of early identification and treatment. Eur J Paediatr Neurol. 2015;19(6):726–9. doi: 10.1016/j.ejpn.2015.07.003[↩]
- Romano S, et al. Riluzole in patients with hereditary cerebellar ataxia: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2015;14(10):985–91. doi: 10.1016/S1474-4422(15)00201-X[↩]
- Veenhuis SJG, van Os NJH, Janssen AJWM, van Gerven MHJC, Coene KLM, Engelke UFH, Wevers RA, Tinnevelt GH, Ter Heine R, van de Warrenburg BPC, Weemaes CMR, Roeleveld N, Willemsen MAAP. Nicotinamide Riboside Improves Ataxia Scores and Immunoglobulin Levels in Ataxia Telangiectasia. Mov Disord. 2021 Dec;36(12):2951-2957. doi: 10.1002/mds.28788[↩][↩]
- van Os NJH, Jansen AFM, van Deuren M, Haraldsson A, van Driel NTM, Etzioni A, van der Flier M, Haaxma CA, Morio T, Rawat A, Schoenaker MHD, Soresina A, Taylor AMR, van de Warrenburg BPC, Weemaes CMR, Roeleveld N, Willemsen MAAP. Ataxia-telangiectasia: Immunodeficiency and survival. Clin Immunol. 2017 May;178:45-55. doi: 10.1016/j.clim.2017.01.009[↩]
- Zannolli R, Buoni S, Betti G, Salvucci S, Plebani A, Soresina A, Pietrogrande MC, Martino S, Leuzzi V, Finocchi A, Micheli R, Rossi LN, Brusco A, Misiani F, Fois A, Hayek J, Kelly C, Chessa L. A randomized trial of oral betamethasone to reduce ataxia symptoms in ataxia telangiectasia. Mov Disord. 2012 Sep 1;27(10):1312-6. doi: 10.1002/mds.25126[↩]
- Shaikh AG, Marti S, Tarnutzer AA, Palla A, Crawford TO, Zee DS, Straumann D. Effects of 4-aminopyridine on nystagmus and vestibulo-ocular reflex in ataxia-telangiectasia. J Neurol. 2013 Nov;260(11):2728-35. doi: 10.1007/s00415-013-7046-4[↩]
- Leuzzi V, Micheli R, D’Agnano D, Molinaro A, Venturi T, Plebani A, Soresina A, Marini M, Ferremi Leali P, Quinti I, Pietrogrande MC, Finocchi A, Fazzi E, Chessa L, Magnani M. Positive effect of erythrocyte-delivered dexamethasone in ataxia-telangiectasia. Neurol Neuroimmunol Neuroinflamm. 2015 Apr 9;2(3):e98. doi: 10.1212/NXI.0000000000000098[↩]
- Nissenkorn A, Hassin-Baer S, Lerman SF, Levi YB, Tzadok M, Ben-Zeev B. Movement disorder in ataxia-telangiectasia: treatment with amantadine sulfate. J Child Neurol. 2013 Feb;28(2):155-60. doi: 10.1177/0883073812441999[↩]
- Charlesworth G, Mohire MD, Schneider SA, Stamelou M, Wood NW, Bhatia KP. Ataxia telangiectasia presenting as dopa-responsive cervical dystonia. Neurology. 2013 Sep 24;81(13):1148-51. doi: 10.1212/WNL.0b013e3182a55fa2[↩]
- Georgiev D, Mehta D, Zacharia A, Vinke RS, Milabo C, Candelario J, Tripoliti E, Hyam JA, Zrinzo L, Hariz M, O’Riordan S, Foltynie T, Limousin P. Bilateral Deep Brain Stimulation of the Globus Pallidus Pars Interna in a Patient with Variant Ataxia-Telangiectasia. Mov Disord Clin Pract. 2016 Jan 21;3(4):405-408. doi: 10.1002/mdc3.12287[↩]
- McGrath-Morrow SA, et al. Evaluation and management of pulmonary disease in ataxia-telangiectasia. Pediatr Pulmonol. 2010;45(9):847–59. doi: 10.1002/ppul.21277[↩][↩][↩]
- McGrath-Morrow S, et al. Pulmonary function in adolescents with ataxia telangiectasia. Pediatr Pulmonol. 2008;43(1):59–66. doi: 10.1002/ppul.20738[↩]
- McGrath-Morrow SA, et al. Pulmonary function in children and young adults with ataxia telangiectasia. Pediatr Pulmonol. 2014;49(1):84–90. doi: 10.1002/ppul.22760[↩]
- Montella S, et al. Non invasive assessment of lung disease in ataxia telangiectasia by high-field magnetic resonance imaging. J Clin Immunol. 2013;33(7):1185–91. doi: 10.1007/s10875-013-9933-y[↩]
- Ataxia-Telangiectasia in Children: Guidance on Diagnosis and Clinical Care. https://atsociety.org.uk/wp-content/uploads/2017/10/ataxia telangiectasia_Clinical_Guidance_Document_Final.pdf[↩]
- Sadighi Akha AA, et al. Oligo-/monoclonal gammopathy and hypergammaglobulinemia in ataxia-telangiectasia. A study of 90 patients. Medicine (Baltimore) 1999;78(6):370–81. doi: 10.1097/00005792-199911000-00002[↩]
- CARING FOR PEOPLE WITH ATAXIA-TELANGIECTASIA. https://atcp.org/wp-content/uploads/2023/04/Caring-For-People-With-A-T_Handbook_10-22.pdf[↩]
- Chiam LY, et al. Cutaneous granulomas in ataxia telangiectasia and other primary immunodeficiencies: reflection of inappropriate immune regulation? Dermatology. 2011;223(1):13–9. doi: 10.1159/000330335[↩]
- Privette ED, et al. Healing of granulomatous skin changes in ataxia-telangiectasia after treatment with intravenous immunoglobulin and topical mometasone 0.1% ointment. Pediatr Dermatol. 2014;31(6):703–7. doi: 10.1111/pde.12411[↩]
- Mitra A, et al. Infliximab in the treatment of a child with cutaneous granulomas associated with ataxia telangiectasia. J Am Acad Dermatol. 2011;65(3):676–7. doi: 10.1016/j.jaad.2010.06.060[↩]
- Pinzon-Charry A, Kimble R, Peake J. Intralesional steroids for the treatment of cutaneous granulomas in ataxia telangiectasia [abstract] Intern Med J. 2013;43(Suppl S4):25.[↩]
- About Pneumococcal Vaccines. https://www.cdc.gov/vaccines/vpd/pneumo/hcp/about-vaccine.html[↩]
- Types of Pneumococcal Vaccines. https://www.cdc.gov/pneumococcal/vaccines/types.html[↩]
- VAXNEUVANCE. https://www.fda.gov/vaccines-blood-biologics/vaccines/vaxneuvance[↩]
- PREVNAR 20. https://www.fda.gov/vaccines-blood-biologics/vaccines/prevnar-20[↩]
- CAPVAXIVE. https://www.fda.gov/vaccines-blood-biologics/capvaxive[↩]
- Centers for Disease Control and Prevention (CDC). Licensure of 13-valent pneumococcal conjugate vaccine for adults aged 50 years and older. MMWR Morb Mortal Wkly Rep. 2012 Jun 1;61(21):394-5. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6121a3.htm[↩]
- PNEUMOVAX 23 – Pneumococcal Vaccine, Polyvalent. https://www.fda.gov/vaccines-blood-biologics/vaccines/pneumovax-23-pneumococcal-vaccine-polyvalent[↩]
- Pneumococcal Vaccine Recommendations. https://www.cdc.gov/pneumococcal/hcp/vaccine-recommendations/index.html[↩][↩]
- Pneumococcal Conjugate Vaccine: What You Need to Know. https://www.cdc.gov/vaccines/hcp/vis/vis-statements/pcv.pdf[↩][↩]
- Schoenaker MHD, et al. Treatment of acute leukemia in children with ataxia telangiectasia (A-T). Eur. J. Med. Genet. 2016;27. doi:10.1016/j.ejmg.2016.05.012[↩]
- Lavin MF, et al. Current and potential therapeutic strategies for the treatment of ataxia-telangiectasia. Br Med Bull. 2007;81–82:129–47. doi: 10.1093/bmb/ldm012[↩]
- Sandlund JT, et al. Pilot study of modified LMB-based therapy for children with ataxia-telangiectasia and advanced stage high grade mature B-cell malignancies. Pediatr Blood Cancer. 2014;61(2):360–2. doi: 10.1002/pbc.24696[↩]
- Ussowicz M, et al. Long-term survival after allogeneic-matched sibling PBSC transplantation with conditioning consisting of low-dose busilvex and fludarabine in a 3-year-old boy with ataxia-telangiectasia syndrome and ALL. Bone Marrow Transplant. 2013;48(5):740–1. doi: 10.1038/bmt.2012.207[↩]
- Beier R, et al. Allogeneic-matched sibling stem cell transplantation in a 13-year-old boy with ataxia telangiectasia and EBV-positive non-Hodgkin lymphoma. Bone Marrow Transplant. 2016;51(9):1271–4. doi: 10.1038/bmt.2016.93[↩]
- Shaikh AG, et al. Effects of 4-aminopyridine on nystagmus and vestibulo-ocular reflex in ataxia-telangiectasia. J Neurol. 2013;260(11):2728–35. doi: 10.1007/s00415-013-7046-4[↩]
- Andrade IGA, Costa-Carvalho BT, da Silva R, Hix S, Kochi C, Suano-Souza FI, Sarni ROS. Risk of Atherosclerosis in Patients with Ataxia Telangiectasia. Ann Nutr Metab. 2015;66(4):196-201. doi: 10.1159/000430790[↩]
- Donath H, Hess U, Kieslich M, Theis M, Ohlenschläger U, Schubert R, Woelke S, Zielen S. Diabetes in Patients With Ataxia Telangiectasia: A National Cohort Study. Front Pediatr. 2020 Jul 9;8:317. doi: 10.3389/fped.2020.00317[↩]
- Woelke S, Pommerening H, Kieslich M, Schubert R, Zielen S. Growth hormone treatment in patients with ataxia telangiectasia. Growth Factors. 2017 Jun;35(2-3):125-130. doi: 10.1080/08977194.2017.1367681[↩]
- Crawford TO, et al. Survival probability in ataxia telangiectasia. Arch Dis Child. 2006;91(7):610–1. doi: 10.1136/adc.2006.094268[↩]
- Crawford TO, Skolasky RL, Fernandez R, Rosquist KJ, Lederman HM. Survival probability in ataxia telangiectasia. Arch Dis Child. 2006 Jul;91(7):610-1. doi: 10.1136/adc.2006.094268[↩]
- Perlman S, Becker-Catania S, Gatti RA. Ataxia-telangiectasia: diagnosis and treatment. Semin Pediatr Neurol. 2003 Sep;10(3):173-82. doi: 10.1016/s1071-9091(03)00026-3[↩]
- McGrath-Morrow SA, Gower WA, Rothblum-Oviatt C, Brody AS, Langston C, Fan LL, Lefton-Greif MA, Crawford TO, Troche M, Sandlund JT, Auwaerter PG, Easley B, Loughlin GM, Carroll JL, Lederman HM. Evaluation and management of pulmonary disease in ataxia-telangiectasia. Pediatr Pulmonol. 2010 Sep;45(9):847-59. doi: 10.1002/ppul.21277[↩]





{kind=link}